workforce assessment: dhb psychologist workforce · workforce assessment: dhb psychologist...
TRANSCRIPT
Prepared by Kamini Pather
For Strategic Workforce Services
Strategic Workforce Services
Workforce Assessment: DHB Psychologist Workforce
April 2016
Strategic Workforce Services – DHB Psychologists Workforce 1
Copyright C/- Central Region’s Technical Advisory Services Limited (TAS)
PO Box 23 075
Wellington 6140
Phone 04 801 2430
Fax 04 801 6230
www.centraltas.co.nz
© Central Region’s Technical Advisory Services Limited
Copyright Statement
The content of this document is protected by the Copyright Act 1994. The information provided
on behalf of TAS may be reproduced without further permission, subject to the following
conditions.
You must reproduce the information accurately, using the most recent version.
You must not use the material in a manner that is offensive, deceptive or misleading.
You must acknowledge the source and copyright status of the material.
Disclaimer
While care has been used in the processing, analysing and extraction of information to
ensure the accuracy of this report, TAS gives no warranty that the information supplied is
free from error. TAS should not be liable for provision of any incorrect or incomplete
information nor for any loss suffered through the use, directly or indirectly, of any
information, product or service.
Strategic Workforce Services – DHB Psychologists Workforce 2
Contents
Executive Summary ............................................................................................................................ 3
Key findings include: .......................................................................................................................... 3
1. Purpose ........................................................................................................................................... 5
2. Workforce Information ................................................................................................................... 5
3. Current Status of the DHB Psychologists Workforce ...................................................................... 7
3.1 Overall Assessment of the Psychologists Workforce ......................................................... 7
3.2 Rationale ............................................................................................................................. 9
3.3 Summary of the Current Status of the DHB Psychologists Workforce ............................. 10
3.4 Workforce Assessment ..................................................................................................... 11
a) Service Demand ..................................................................................................... 11
b) Supply ..................................................................................................................... 13
c) Operational Flexibility ............................................................................................ 15
d) Operational Capacity .............................................................................................. 16

Strategic Workforce Services – DHB Psychologists Workforce 3
Executive Summary
Current analysis of the DHB Psychologists workforce has resulted in it being classified as a
‘Transitional Occupation’. This classification highlights that service demand is progressively
increasing with some supply issues around the number of Maori and Pacific psychologists
and with particular areas of specialisation. There are emerging sector requirements to
begin looking at alternative models of care and roles for this workforce, as greater flexibility
is required. Some recruitment and retention issues are occurring in areas of specialisation,
minority ethnic groups and particular geographic areas, with longer timeframes for gaining
this workforce. Overall, the Psychologists Workforce within the DHBs remains stable with a
few long standing issues continuing to gain momentum. No significant priorities have been
identified for the DHBs to address through the bargaining strategy.
Key findings include:
Service demand has been increasing and is predicted to continue increasing as primary intervention and integration is prioritised.
Population growth and variegation, the outcome of the Christchurch earthquake and increasing recognition of the value of psychology in health are also impacting on service demand.
There have been significant changes to Mental Health Services, models of care and service delivery. As a result, psychologists are increasingly being required to take on new key roles with significant increases in responsibility.
The DHB Psychologist Workforce has no major distribution or supply issues. However, there are some wider issues with supply, i.e. with Maori and Pacific psychologists, particular areas of specialisation, some geographic areas and the funding of intern placements; rather than the entire workforce. This is resulting in slightly longer timeframes for gaining this workforce.
The demand for specialist practitioners is increasing, particularly in emerging areas such as transgender surgery, transplants, cardiac, renal, neuro injury (stroke), and cancer support services. There is a need for the consideration of options to support long term capability development in the areas of specialisation which are experiencing or are likely to experience supply issues.
It can be challenging recruiting qualified and experienced psychologists for rural areas and a lot of proactive work needs to be done, usually involving longer timeframes. There can also be high turnover where there are solo practitioners, who don’t get a lot of support.
The quality of interns coming through are generally good, however there are concerns around the funding of interns and placement numbers. Some interns are within current FTE budget, while others are partially funded through HWNZ. There

Strategic Workforce Services – DHB Psychologists Workforce 4
have been funding changes which are also having an impact. Clarity needs to be sought from HWNZ.
Supervision requirements mean that trained psychologists are sometimes recruited over interns. While interns are registered as psychologists, they still need to complete their internship and 1500 hours of supervision. It can be difficult to provide supervision, and there is a tension with service delivery. This can make it difficult for interns to get appropriate placements.
Access to training can become a retention issue as funding of Continuing Professional Development (CPD) is negotiated. Training is needed to develop specialist skills, however funding is an issue.
While the DHBs are doing the best they can to support a Maori perspective and effective delivery of service to this group, under representation of Maori in this workforce does create difficulties. Increasing the number of Maori psychologists and support is a significant concern. There are small numbers of Maori going into training. While there have been a few Maori interns coming through, the numbers are very low. There are a range of barriers inhibiting minority groups from entering the profession, including the limited availability of colleagues within the group to support / supervise appropriately. The long training pathway and different perceptions of mental health can also be deterrents and barriers to entry. Changes to Postgraduate funding of student loans has also reduced access. The Kia Ora Hauora Programme may change this over the long term.
There are well qualified overseas trained psychologists being recruited by DHBs, however there is low reliance on this source as there are sufficient numbers of psychologists available locally. There is an identified gap in terms of overseas trained psychologists requiring New Zealand specific cultural training, which the New Zealand Psychologists Board is currently looking to addressing.
Longer term challenges remain around the public/private interface, particularly in relation to loss of experienced staff to private practice and/or a reduction in hours worked for DHBs.
There are also increased pressures in terms of the aging workforce, reducing hours of work and time out for parental leave. These issues also impact on capacity for supervision of interns.
Psychologists need to be responsive to consumer needs. There is a move away from the usual Monday to Friday, 9am to 5pm hours. There is also an increasing need for flexibility around locations.
New technologies are providing some flexibility in the way work is structured and organised, and services are delivered. There is increased use of technology such as online tools for consultations, monitoring and communicating with clients using secure transmission. This seems to work particularly well with the younger age groups.
Strategic Workforce Services – DHB Psychologists Workforce 5
1. Purpose Employment Relations is a key accountability for DHBs and has a significant impact on DHB
outcomes. The Employment Relations Strategy Group (ERSG) has an operational governance role
over Strategic Workforce Services (SWS) ER activity and has mandated a range of advice to ensure
that development of bargaining strategy is well supported.
Operational advice on the DHB employed workforce is developed by the Strategic Workforce
Services team and is complementary to the strategic advice and direction provided by Health
Workforce New Zealand (HWNZ). The intent of the operational advice is to ensure that Bargaining
Strategy Groups have access to accurate information on the current status of the DHB employed
workforce.
This paper provides summary advice to the ERSG and the Bargaining Strategy Group on the current
status of the DHB employed Psychologists Workforce. It is based on the feedback received from
DHBs through the workforce assessment process and workforce information data. This information
is provided for the purpose of informing the development of a bargaining strategy for the
Psychologists MECA – expiry date 31 May 2016.
2. Workforce Information The DHB psychologist workforce comprises 570 FTE (723 people in total) as at 30 September 2015.
Canterbury DHB has the highest FTE of psychologists at 79.1 followed by Auckland DHB with 77.2
FTE.
HWIP trend analysis from 2007 to 2015 demonstrates a steadily increasing number of clinical
psychologists, with an overall FTE increase of 36% over this period. Conversely, over the same period
the Mean FTE has reduced from 0.83 to 0.79 indicating an increasing proportion of part time staff.
The DHB psychologist workforce has an average age of 44.7 years and an average length of service of
6.4 years. The proportion of females to males increased from 74% in 2007 to 79% in 2015. The
turnover rate which is currently 17% has fluctuated between 15-20% for the period 2007 to 2015.
The number of psychologists leaving is extremely small and therefore susceptible to significant
variation. This combined with an increasing length of service and an increase in mean age for both
sexes, suggests a stable and aging workforce.
The majority of psychologists are classified as ‘Other’ ethnicity (87.9%) followed by Asian, Māori and
Pacific groups with ratios of 6.5%, 4.5% and 1.1% respectively. This represents a change from 2007,
when the ethnic composition of the DHB psychologist workforce comprised 94.6% ‘Other’, 2.1%
Asian, 3.3% Māori and 0% Pacific. The difference between workforce ethnicity and population
Strategic Workforce Services – DHB Psychologists Workforce 6
ethnicity proportions indicates negative values, i.e. significant under-representation, of Asian, Māori
and Pacific ethnic groups.
In general employees are 9 to 5 workers with very little overtime and penal payments paid. It is
unknown what percentage are union members.
The key statistics suggest a stable workforce, increasing in size, proportionately more dominant
female representation, with a fluctuating turnover, an increasing proportion of part time staff and
under-representation of minority ethnic groups. A detailed Workforce Information Report is
included at Appendix 1.
Strategic Workforce Services – DHB Psychologists Workforce 7
3. Current Status of the DHB Psychologists Workforce
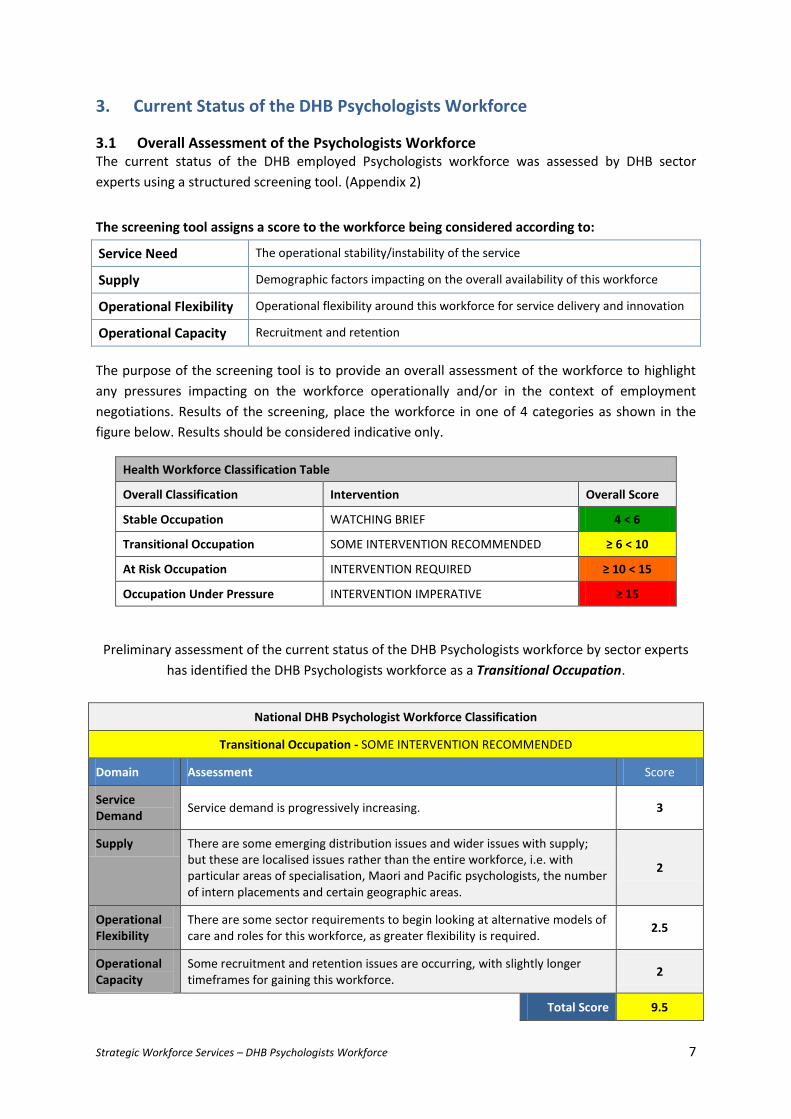
3.1 Overall Assessment of the Psychologists Workforce The current status of the DHB employed Psychologists workforce was assessed by DHB sector
experts using a structured screening tool. (Appendix 2)
The screening tool assigns a score to the workforce being considered according to:
Service Need The operational stability/instability of the service
Supply Demographic factors impacting on the overall availability of this workforce
Operational Flexibility Operational flexibility around this workforce for service delivery and innovation
Operational Capacity Recruitment and retention
The purpose of the screening tool is to provide an overall assessment of the workforce to highlight
any pressures impacting on the workforce operationally and/or in the context of employment
negotiations. Results of the screening, place the workforce in one of 4 categories as shown in the
figure below. Results should be considered indicative only.
Health Workforce Classification Table
Overall Classification Intervention Overall Score
Stable Occupation WATCHING BRIEF 4 < 6
Transitional Occupation SOME INTERVENTION RECOMMENDED ≥ 6 < 10
At Risk Occupation INTERVENTION REQUIRED ≥ 10 < 15
Occupation Under Pressure INTERVENTION IMPERATIVE ≥ 15
Preliminary assessment of the current status of the DHB Psychologists workforce by sector experts
has identified the DHB Psychologists workforce as a Transitional Occupation.
National DHB Psychologist Workforce Classification
Transitional Occupation - SOME INTERVENTION RECOMMENDED
Domain Assessment Score
Service Demand
Service demand is progressively increasing. 3
Supply There are some emerging distribution issues and wider issues with supply; but these are localised issues rather than the entire workforce, i.e. with particular areas of specialisation, Maori and Pacific psychologists, the number of intern placements and certain geographic areas.
2
Operational Flexibility
There are some sector requirements to begin looking at alternative models of care and roles for this workforce, as greater flexibility is required.
2.5
Operational Capacity
Some recruitment and retention issues are occurring, with slightly longer timeframes for gaining this workforce.
2
Total Score 9.5
Strategic Workforce Services – DHB Psychologists Workforce 8
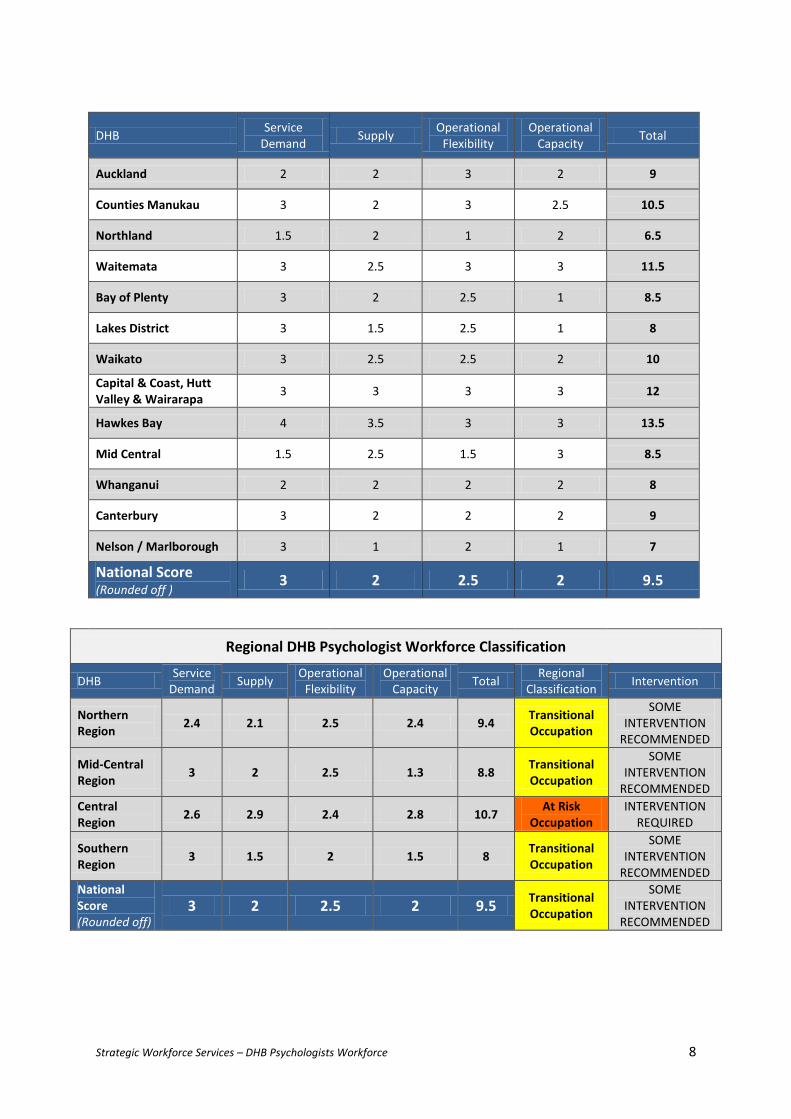
DHB Service
Demand Supply
Operational Flexibility
Operational Capacity
Total
Auckland 2 2 3 2 9
Counties Manukau 3 2 3 2.5 10.5
Northland 1.5 2 1 2 6.5
Waitemata 3 2.5 3 3 11.5
Bay of Plenty 3 2 2.5 1 8.5
Lakes District 3 1.5 2.5 1 8
Waikato 3 2.5 2.5 2 10
Capital & Coast, Hutt Valley & Wairarapa
3 3 3 3 12
Hawkes Bay 4 3.5 3 3 13.5
Mid Central 1.5 2.5 1.5 3 8.5
Whanganui 2 2 2 2 8
Canterbury 3 2 2 2 9
Nelson / Marlborough 3 1 2 1 7
National Score (Rounded off )
3 2 2.5 2 9.5
Regional DHB Psychologist Workforce Classification
DHB Service
Demand Supply
Operational Flexibility
Operational Capacity
Total Regional
Classification Intervention
Northern Region
2.4 2.1 2.5 2.4 9.4 Transitional Occupation
SOME INTERVENTION
RECOMMENDED
Mid-Central Region
3 2 2.5 1.3 8.8 Transitional Occupation
SOME INTERVENTION
RECOMMENDED
Central Region
2.6 2.9 2.4 2.8 10.7 At Risk
Occupation INTERVENTION
REQUIRED
Southern Region
3 1.5 2 1.5 8 Transitional Occupation
SOME INTERVENTION
RECOMMENDED
National Score (Rounded off)
3 2 2.5 2 9.5 Transitional Occupation
SOME INTERVENTION
RECOMMENDED
Strategic Workforce Services – DHB Psychologists Workforce 9
3.2 Rationale The analysis of the Psychologists Workforce within the DHBs has resulted in the classification of a
Transitional Occupation. This classification highlights that service demand is progressively increasing
with some supply issues around the number of Maori and Pacific psychologists and with particular
areas of specialisation. There are emerging sector requirements to begin looking at alternative
models of care and roles for this workforce, as greater flexibility is required. Some recruitment and
retention issues are occurring in areas of specialisation, minority ethnic groups and particular
geographic areas, with longer timeframes for gaining this workforce.
Key findings include:
Service demand has been increasing and is predicted to continue increasing as primary
intervention and integration is prioritised.
Population growth and variegation, the outcome of the Christchurch earthquake and
increasing recognition of the value of psychology in health are also impacting on service
demand.
There have been significant changes to Mental Health Services, models of care and service
delivery. As a result, psychologists are increasingly being required to take on new key roles
with significant increases in responsibility.
The demand for specialist practitioners is also increasing, particularly in emerging areas such
as transgender surgery, transplants, cardiac, renal, neuro injury (stroke), and cancer support
services.
There are also increased pressures in terms of the aging workforce, reducing hours of work
and time out for parental leave. These issues also impact on capacity for supervision of
interns.
The DHB Psychologist Workforce has no major distribution or supply issues. However, there
are some wider issues with supply, i.e. with Maori and Pacific psychologists, particular areas
of specialisation, some geographic areas and the funding of intern placements; rather than
the entire workforce.
Longer term challenges remain around the public/private interface, particularly in relation to
loss of experienced staff to private practice and/or a reduction in hours worked for DHBs.
Some recruitment and retention issues are occurring in areas of specialisation, minority
ethnic groups and some geographic areas, with slightly longer timeframes for gaining this
workforce.
Overall, the Psychologists Workforce within the DHBs remains stable with a few long standing
issues continuing to gain momentum. No significant priorities have been identified for the DHBs to
address through the bargaining strategy.
Strategic Workforce Services – DHB Psychologists Workforce 10
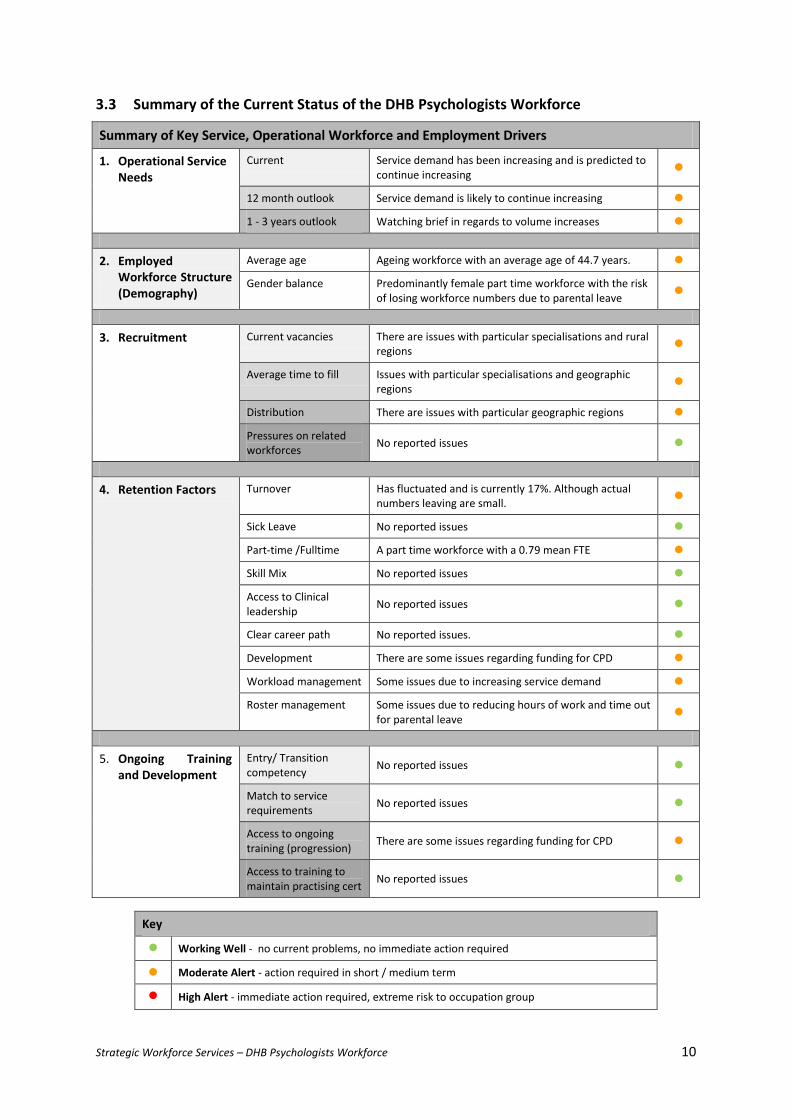
3.3 Summary of the Current Status of the DHB Psychologists Workforce
Summary of Key Service, Operational Workforce and Employment Drivers
1. Operational Service Needs
Current Service demand has been increasing and is predicted to continue increasing
12 month outlook Service demand is likely to continue increasing
1 - 3 years outlook Watching brief in regards to volume increases
2. Employed Workforce Structure (Demography)
Average age Ageing workforce with an average age of 44.7 years.
Gender balance Predominantly female part time workforce with the risk of losing workforce numbers due to parental leave
3. Recruitment Current vacancies There are issues with particular specialisations and rural regions
Average time to fill Issues with particular specialisations and geographic regions
Distribution There are issues with particular geographic regions
Pressures on related workforces
No reported issues
4. Retention Factors Turnover Has fluctuated and is currently 17%. Although actual numbers leaving are small.
Sick Leave No reported issues
Part-time /Fulltime A part time workforce with a 0.79 mean FTE
Skill Mix No reported issues
Access to Clinical leadership
No reported issues
Clear career path No reported issues.
Development There are some issues regarding funding for CPD
Workload management Some issues due to increasing service demand
Roster management Some issues due to reducing hours of work and time out for parental leave
5. Ongoing Training and Development
Entry/ Transition competency
No reported issues
Match to service requirements
No reported issues
Access to ongoing training (progression)
There are some issues regarding funding for CPD
Access to training to maintain practising cert
No reported issues
Key
Working Well - no current problems, no immediate action required
Moderate Alert - action required in short / medium term
High Alert - immediate action required, extreme risk to occupation group

Strategic Workforce Services – DHB Psychologists Workforce 11
3.4 Workforce Assessment
a) Service Demand
Service Demand is about the demands on a particular service and associated workforce, and it
relates to the need for service provision within the environment or context being examined.
Service demand relating to the DHB Psychologist Workforce is progressively increasing.
The following considerations are influencing this:
Population growth and variegation, the outcome of the Christchurch earthquake and
increasing recognition of the value of psychology in health are some of the factors driving
increases in service demand.
There is increasing recognition of the role and value of psychological interventions in
primary care, therefore increasing demand for service. Overall service demand has been
increasing and is predicted to continue increasing as primary intervention and integration is
prioritised. Psychologists are increasingly taking a lead role or multi-disciplinary integrated
approach. While there is an expectation of integrated primary and secondary interventions,
no guidance has been provided on how to achieve this.
Reduced societal stigma about mental health issues in addition to increased publicity and
communication has increased the uptake of psychological services. There seems to be
decreased community resilience.
There have been significant changes to Mental Health Services, models of care and service
delivery. The increasing rate of access for mental health services is leading to a re-
examination of models of care to utilise resources, including psychology resources, in
different ways. As a result, psychologists are being required to take on new key roles, with
significant increases in responsibility.
The value of psychological assessments is also being recognised more, therefore also
contributing to an increase in demand. The scope of the role is broadening and changing.
Psychologists are required to complete more comprehensive assessments of individuals,
contextual and background factors. This is also a workforce development issue in that there
are changing requirements and skills that are needed.
Specialty demand is increasing in terms of the need for specialist practitioners. Areas such
transgender and transplants need pre-surgery psychology assessments. There may be a
need for a centralised resource. Cardiac and renal are also emerging areas. An area where
Psychologists can also have a positive impact is Neuro injury (stroke), i.e. the areas of brain
damage injury and chronic pain. Cancer support services is another new and increasing area
of service demand.
Strategic Workforce Services – DHB Psychologists Workforce 12
Forensics is a growth area which is experiencing an increase in requests for court reports.
This is a significant part of the work that Forensic Psychologists do and requires high levels of
technical competence. Legislative compliance requirements mean that only Forensic
Psychologists and Psychiatrists can write court reports. Youth Forensic is a national service
and which starts on 21 April 2016.
There has been an increase in referrals for both short & long term psychological
interventions, e.g. DBT - currently most community teams run waiting lists. In adult CMHS
there are long waiting lists for psychology input. Some DHBs are using FTE for outsourcing to
move through the short term referrals. This is freeing up the more experienced
psychologists to focus on the prioritised referrals. This involves them working on a
consultancy basis and allocating work appropriately.
There has also been an increase in the acuity and complexity of referrals, requiring specialist
services. As a result of the ‘Stepped care’ approach, psychologists are increasingly working
with clients with complex issues over an extended period of time.
Clients with chronic conditions are living longer and have changed care needs over a longer
extended period. Talking therapies are in common use for long term conditions. There will
be difficulties meeting the needs of this area in the future and if the underlying issues are
not addressed then this will place demand on other areas, e.g. longer term stays. Other
workforces could be used to deliver the therapies with psychologist supervision or on a
consultant basis.
General referrals in the areas of children and adolescents are also growing, with anticipated
increases of 10-14%. Hamilton has experienced more than 100% increase in children and
adolescents referrals in recent years. There are also new regional in-patient services with a
focus on younger clients, i.e. Children and Adolescents. There will be a need to find
increased number of specialists in this area.
The establishment of Children’s Teams under the Vulnerable Children Act 2014, involves
practitioners and professionals in government agencies, iwi and non-government
organisations bringing together existing services for vulnerable children into one
personalised plan for each child and their family/whānau with existing resources. A key aim
is to fast track children into government services such as health. There is also a focus on
targeting resources on priority areas such as the ‘Million dollar babies’. Additionally, FTE is
being assigned to the Children’s Teams which puts pressure on the rest of the team.
As a result of the Ministry of Health targeting access rates for service, within the context of
DHBs being required to do more with less, services are being reorganised. This includes
meeting waitlist targets across all age groups.
There is high demand for rural work due to factors such as high suicide rates in farming
communities, increasing pressures with falling dairy prices, isolation, etc. Rural roles are
often recruited from overseas, mainly South Africa. These recruits generally work out well.

Strategic Workforce Services – DHB Psychologists Workforce 13
However, it was noted that in Tairawhiti which has a strong Maori presence, there have
been some tensions.
ACC related ‘Sensitive Claims’ is a growth area. ACC Special Services Contract with Capital &
Coast and Canterbury DHBs is a one year pilot which utilises the services of Psychologists,
psychiatrists and social workers.
There are also increased pressures in terms of the aging workforce, reducing hours and time
out for parental leave. These issues also impact on capacity for supervision.
Service provision hours are almost exclusively Monday to Friday currently. However, this is
changing in terms of the drive to be more responsive, and is likely to expand to include early
evening and Saturdays, to ensure families are able to attend and participate in family
therapy. Acute care teams are available to provide after hours service.
b) Supply
Supply is about the actual quantity and distribution of a workforce; including current demographics
and the quantity and quality of students / graduates.
There are some emerging distribution issues and wider issues with supply; but these are localised
issues rather than the entire workforce, i.e. with particular areas of specialisation, Maori and
Pacific psychologists, the number of intern placements and certain geographic areas.
The following considerations are influencing this:
There is increasing diversity in the general population. Ideally, the psychologist workforce
should be representative of the general population. However, there are supply issues with
regard to gender and ethnic demographics such that the workforce is not representative of
the wider population, with significant under representation of minority groups. The small
numbers are not meeting demographic needs, since there are insufficient Maori and Pacific
psychologists available.
While the DHBs are doing the best they can to support a Maori perspective and effective
delivery of service to this group, under representation of Maori in this workforce does create
difficulties.
Increasing the number of Maori psychologists and support is a significant concern. There are
small numbers of Maori going into training. While there have been a few Maori interns
coming through, the numbers are very low. There are a range of barriers inhibiting minority
groups from entering the profession, including the limited availability of colleagues within
the group to support / supervise appropriately. The long training pathway and different
perceptions of mental health can also be deterrents and barriers to entry. At a local level
Strategic Workforce Services – DHB Psychologists Workforce 14
there are identifiable barriers such as family pressures, social issues, costs, distance from
training institutes, etc. which are deterring Maori from training as psychologists. Changes to
Postgraduate funding of student loans has also reduced access. The Kia Ora Hauora
Programme may change this over the long term.
While there is sufficient supply available in general psychology, there are increasing
shortages of psychologists in specialised areas and sub-specialties. These are long standing
issues which have escalated in recent years, as referrals for specialty services are increasing
significantly. Some specialist therapeutic models are requiring a special suite of skills and
qualifications, e.g. DBT. There is a tension between specialist vs generalist capability
development. The drive towards specialisation could create a shortage of generalists over
the long term.
There are well qualified overseas trained psychologists being recruited by DHBs, however
there is low reliance on this source as there are sufficient numbers of psychologists available
locally. There is an identified gap in terms of overseas trained psychologists requiring New
Zealand specific cultural training, which the New Zealand Psychologists Board is currently
looking to addressing.
There are fewer male psychologists, which can put pressure on service delivery.
There is an emerging trend of an increased number of fulltime staff reducing their hours in
order to also work in private practice. It is difficult to recruit to cover small FTE gaps. This
increase in part-time hours puts pressure on service delivery.
The quality of interns coming through are generally good, however there are concerns
around the funding of interns and placement numbers. Some interns are within current FTE
budget, while others are partially funded through HWNZ. Clarity needs to be sought from
HWNZ. There have been funding changes which are also having an impact. Some DHBs have
to recruit interns within current FTE. This is resulting in an adhoc reactive approach.
Supervision requirements mean that trained psychologists are recruited over interns. Interns
are usually used to fill vacancies which DHBs may be having difficulty filling. Counties
Manukau has a short term planned approach but this is funding dependent. While interns
are registered as psychologists, they still need to complete their internship and 1500 hours
of supervision. It can be difficult to provide supervision, and there is a tension with service
delivery / demand. It can be difficult for interns to get appropriate placements. Sometimes
Clinical Psychologists need to settle for less than desirable placements.
Intern placements are controlling what comes through the universities. There is a need for
more intern placements otherwise the universities cannot take more students. There are
only 8 partially funded annual placements for DHBs nationally, which is considered
inadequate.
Interns are considered to be very hard workers and a highly skilled/valuable resource. Intern
remuneration is quite high. Some DHBs are debating whether if the salary was lower, more
Strategic Workforce Services – DHB Psychologists Workforce 15
interns could be funded. However, some DHBs consider the remuneration reasonable for
the value interns provide.
c) Operational Flexibility
Operational Flexibility is primarily about substitution of a workforce and the ability for other
workforces to potentially take on the roles involved. It includes specificity of skills and how
specialised particular roles / scopes of practice are in regards to delivery of required care. It is also
about how enabling or limiting a current scope of practice is on workforce utilisation.
There are some sector requirements to begin looking at alternative models of care and roles for
the DHB Psychologist Workforce, as greater flexibility is required.
Considerations include:
This is a relatively small workforce with a long training/education pathway. The training is
prescribed and there is no other entry pathway.
Psychologists are increasingly required to be responsive, consumer focused / centred with
flexibility of approach. While the psychologist workforce comprises specialised roles with
specific qualifications and scope of practice, there are aspects of the role that can be moved
to other roles with appropriate training and support. There are only a few aspects that only
a psychologist can do. Some aspects of treatment can be done by others with appropriate
training and support, e.g. co-facilitation of therapy groups. Ideally, there should be a
stepped model of care to enable more flexibility.
There are requirements in mental health to look at different models of care to meet
increasing need, and this will have an impact on the role of psychology in teams / services.
Changing models of service delivery are looking at taking a multi-disciplinary approach and
breaking down silos. There is an increased focus on looking to increase integration with
primary care, provide shared care, etc.
Some DHBs are using FTE for outsourcing to move through the short term referrals. This is
freeing up the more experienced psychologists to focus on the prioritised referrals. This
involves them working on a consultancy basis and allocating work appropriately. At the
moment the focus is on psychologists managing a workload of mainly acute, but ideally their
workload should comprise a balance of acute and medium care.
The possibility of developing ‘Psychologist Hubs’ is being looked at as a way of getting
people to work smarter. This workforce can be resistant to changes to their way of working.

Strategic Workforce Services – DHB Psychologists Workforce 16
There are increasing requirements for psychologists in areas where they may not have
previously been involved. Increasingly complex issues are coming through, so trying to take
an integrated approach.
There is flexibility in working with other health professions within multi-disciplinary models
of care. There is some tension here due to how the value of the different roles may be
perceived and how the priorities are assessed.
Dialectical Behaviour Therapy (DBT) is a specialist cognitive behavioural treatment
developed for clients with severe emotional problems, who meet criteria for Borderline
Personality Disorder (BPD) or Complex Post-Traumatic Stress Disorder (CPTSD). The goal of
DBT is about building a life worth living. Community DBT can be demanding and often results
in psychologists being the ones responsible for the ‘risky’ interventions.
Some psychologists such CAF Psychologists can only work with people up to the age of 18
years, so while they tend to be flexible, they are restricted by their scope of practice.
Specialisations can reduce service flexibility. Neuropsychology and cognitive assessments are
at the complex end and can only be done by clinical psychologists.
Similarly, Forensic court reports can only be done by Forensic Psychologists. No substitution
is possible. Legislative compliance requirements can restrict operational flexibility and
require a structured approach.
New technologies are providing some flexibility in the way work is structured and organised,
and services are delivered. There is increased use of technology such as online tools for
consultations, monitoring and communicating with clients using secure transmission. This
seems to work particularly well with the younger age groups. The adult sector tends to be
the most challenging.
Psychologists need to be responsive to consumer needs. There is a move away from usual
Monday to Friday, 9am to 5pm hours. There is also an increasing need for flexibility around
locations. The role allows flexibility, however it depends on the individual. There is also
flexibility in the range of therapies and deployment of psychologists.
There is high potential for psychologists to move into psychiatric areas. Substituting
psychologists to pick up some of the work, so less treatment with drugs and more
psychological therapies.
d) Operational Capacity
Operational Capacity is about recruitment and retention of a workforce. It includes availability and
the ability to buy / bring in more of a particular workforce as required.
Strategic Workforce Services – DHB Psychologists Workforce 17
Some recruitment and retention issues are occurring in areas of specialisation, minority ethnic
groups and some geographic areas, with slightly longer timeframes for gaining this workforce.
Considerations include:
It can be challenging recruiting qualified and experienced psychologists and a lot of
proactive work needs to be done. There are longer timeframes involved in sourcing the
limited supply of qualified and experienced staff, particularly for rural areas. There are small
numbers of applicants for advertised roles. Very few applications (maybe 1 or 2) are
received for vacant positions, and mainly from overseas applicants. It does seem however
that recruits with overseas qualifications manage to achieve registration in New Zealand
with relative ease.
Recruiting to rural areas can be difficult, as it involves getting people to move to small towns
without university linkages.
There can be high turnover where there are solo practitioners, who don’t get a lot of
support.
While not highly reliant on overseas qualified psychologists, some DHBs do use them as a
source. Some overseas recruitment is done with the UK, Australia and South Africa being
primary source countries. There has been a decrease in overseas applicants recently.
There is competition between DHBs during recruitment.
Differences in credentialing overseas graduates and placement on salary scales can lead to
movement between DHBs.
There is some difficulty involved in recruiting minority ethnic groups and for cultural
services. There are some but it can take a long time to source people.
There are some retention and recruitment issues relating to specialised areas and roles. It is
harder to recruit for specialised areas or services, especially new and developing specialist
services such as Youth Forensics Services.
Sometimes, due to budgeting issues psychologists have been de-prioritised in terms of
vacancies, leading to time lags in recruitment. The diverse nature of the service and small
FTE numbers in some locations impacts on recruitment timelines.
There are issues with increased movement to private practice, i.e. increasing the hours
worked in private practice and decreasing availability for DHB work. This trend results in
reducing FTE and it is difficult to recruit to fill the gaps created, which challenges service
delivery. There is a potential issue of retaining psychology staff fulltime in DHB settings, as
compared with other non-medical staff, there are many and increasing opportunities for
private practice. There are significant and increasing, numbers of psychologists who have
work split between DHB and private practice. There is a lack of willingness to work fulltime
in the DHB environment, due to the nature of the work. The differences between the private
Strategic Workforce Services – DHB Psychologists Workforce 18
and DHB contexts are hard to overcome, i.e. more exciting opportunities, greater
satisfaction, higher remuneration, greater control over the hours worked, etc.
The high numbers of females means that there are high levels of parental leave and people
not returning from parental leave, which impacts on retention.
The DHBs lose highly skilled psychologists to the Department of Corrections (DoC) due to
higher remunerations on offer. The DoC has no merit progression steps to achieve and this
can be seen as a positive above the merit step remuneration in a DHB context. They are
competing for a limited pool of highly skilled psychologists.
The high cost of living in Auckland impacts on recruitment and retention. The DoC gives a
$2.4K extra allowance to psychologists working in Auckland.
Interns are utilised to cover FTE gaps. Some DHBs are reducing the number of interns,
resulting in people moving into other areas.
Access to training and lead in time can become a retention issue. Funding of Continuing
Professional Development (CPD) is negotiated. Training is needed to develop specialist skills,
however funding is an issue.

Strategic Workforce Services – DHB Psychologists Workforce 19