winner of resident paper award 2014 - antoniocasella.eu · winner of resident paper award 2014...
TRANSCRIPT

Winner of Resident Paper Award 2014
Benzodiazepines for PTSDA Systematic Review and Meta-Analysis
Objective Although benzodiazepines (BZDs)are commonly used in the treatment of post-traumatic stress disorder (PTSD) no system-atic review or meta-analysis has specificallyexamined this treatment The goal of this studywas to analyze and summarize evidence con-cerning the efficacy of BZDs in treating PTSDMethods The review protocol was undertakenaccording to the principles recommended bythe Preferred Reporting Items for SystematicReviews and Meta-Analyses (PRISMA) state-ment and is registered with the PROSPEROinternational prospective register of systematicreviews (httpwwwcrdyorkacukPROSPEROregistration number CRD42014009318) Twoauthors independently conducted a search ofall relevant articles using multiple electronicdatabases and independently abstracted infor-mation from studies measuring PTSD out-comes in patients using BZDs Eighteen clinicaltrials and observational studies were identi-fied with a total of 5236 participants Outcomeswere assessed using qualitative and quantita-tive syntheses including meta-analysisResults BZDs are ineffective for PTSD treat-ment and prevention and risks associatedwith their use tend to outweigh potentialshort-term benefits In addition to adverseeffects in general populations BZDs are asso-ciated with specific problems in patients withPTSD worse overall severity significantlyincreased risk of developing PTSD with useafter recent trauma worse psychotherapyoutcomes aggression depression and sub-stance use Potential biopsychosocial explan-ations for these results are proposed based onstudies that have investigated BZDs PTSDand relevant animal modelsConclusions The results of this systematicreview suggest that BZDs should be consideredrelatively contraindicated for patients withPTSD or recent trauma Evidence-based treat-ments for PTSD should be favored over BZDs(Journal of Psychiatric Practice 201521281ndash303)
Key Words benzodiazepine sedative traumastress disorder posttraumatic stress disorderpsychopharmacology
The use of benzodiazepines (BZDs) in the treatmentof posttraumatic stress disorder (PTSD) is bothcommon and controversial Although BZDs areprescribed to 30 to 74 of patients with PTSD1ndash2
there is little literaturemdashand no reviews before thisarticlemdashfocusing exclusively on the use of BZDs toprevent or treat PTSD Considering all the servicemembers returning from Afghanistan and Iraq withcombat-related PTSD there is no better time toevaluate this topic than now
Some argue that BZDs are effective symptomatictreatments for the anxiety insomnia and irrita-bility associated with PTSD and they defend theprescription of BZDs for PTSD as necessary fortreatment-resistant patients with severe symp-toms Others contend that BZDs may diminishsubjective anxiety in the short term at the cost ofworsening other features of PTSD such as pro-moting avoidance in the long term They explainthe correlation between BZDs and increasedsymptom severity as the result of BZDs actuallyprolonging and worsening PTSD
JEFFREY GUINA MDSARAH R ROSSETTER MD
BETHANY J DeRHODES MDRAMZI W NAHHAS PhDRANDON S WELTON MD
GUINA Wright State University Department of Psychiatryand Wright-Patterson Air Force Base Medical Center Day-ton OH ROSSETTER Wright State University Departmentof Psychiatry DERHODES Wright State University Depart-ment of Psychiatry and Miami Valley Hospital Dayton OHNAHHAS Wright State University Department of Commun-ity Health WELTON Wright State University Department ofPsychiatry and Veterans Affairs Medical Center Dayton OH
Copyright copy 2015 Wolters Kluwer Health Inc All rightsreserved
Registration PROSPERO international prospective registerof systematic reviews (CRD42014009318 httpwwwcrdyorkacukPROSPERO)
The authors declare no conflicts of interest
Please send correspondence to Jeffrey Guina MD Wright-Patterson Medical Center Mental Health 4881 Sugar MapleDr Wright-Patterson Air Force Base Dayton OH 45433(jeffreyguinawrightedu)
DOI 101097PRA0000000000000091
Journal of Psychiatric Practice Vol 21 No 4 July 2015 281
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Most PTSD practice guidelines pay little attentionto BZDs or caution against their use citing weakevidence risks that outweigh benefits and contra-indication for conditions that are commonly comorbidwith PTSD such as traumatic brain injury (TBI) andsubstance use disorder (SUD) Some guidelines gofurther declaring BZDs contraindicated for combat-related PTSD (Veterans Affairs and Department ofDefense)3 traumatic grief (British National For-mulary)4 and all PTSD (International Society forTraumatic Stress Studies)5
Despite the abundance of articles about PTSDand the frequent prescription of BZDs littleresearch has evaluated the use of BZDs for PTSDIn our literature review we attempted to captureevery available study about BZDs in PTSD toexamine 3 questions
(1) What are the effects of BZDs on the develop-ment of PTSD in trauma patients
(2) What are the effects of BZDs on PTSD-associ-ated outcomes in patients with PTSD
(3) What are the effects of BZDs on PTSD-associ-ated outcomes in trauma patients with andwithout PTSD
METHODS
Study Selection
Studies were included for review using the followingeligibility criteria
(1) Study design clinical trials or observationalstudies
(2) Participants any patient with a history oftrauma assessed for PTSD
(3) Intervention any dose duration or type of BZD(4) Outcomes measured PTSD-associated symptoms
Studies were excluded if they were reviews oranecdotal or if BZDs were not distinguished fromother medications
The authors conducted electronic searches usingPubMed PsycINFO MEDLINE Cochrane Libraryand Google Scholar (all the studies eventuallyselected are available in PubMed) Search parame-ters included all English-language articles pub-lished until June 30 2014 Search terms includedPTSD stress disorder benzodiazepine and the
generic names of the different BZDs For examplethe following search was used in PubMed
((PTSD) OR (stress disorder)) AND ((benzodia-zepine) OR (alprazolam) OR (chlordiazepoxide)OR (clonazepam) OR (clorazepate) OR (diaze-pam) OR (flurazepam) OR (lorazepam) OR(midazolam) OR (oxazepam) OR (temazepam)OR (triazolam))
References in retrieved articles were further scan-ned for additional relevant articles Duplicate articleswere not counted in the total sample of identifiedrecords Abstracts were screened for relevance Full-text articles were retrieved to determine eligibilityTwo authors independently determined eligibility forwhich interobserver agreement was calculated usingpercent agreement and kappa statistics Disagree-ments regarding eligibility were resolved by consensusamong the authors For each eligible study 2 authorsindependently abstracted information concerningstudy characteristics
Data Synthesis
The findings of the selected articles were catego-rized according to levels of scientific evidence basedon clinical practice guidelines from the US Depart-ment of Health and Human Services6
A Multiple double-blind placebo-controlled trialsand a confirmatory meta-analysis (in addition tolevel B of evidence)
B At least 1 double-blind placebo-controlled trial(in addition to level C of evidence)
C Anecdotal reports case series and open trialsin addition to expert endorsement or consensus
D Few case reports without any expert panelendorsement
To evaluate evidence for an association betweenBZDs and PTSD the following 3 null hypotheseswere tested
H1 BZDs are not associated with the develop-ment of PTSD in trauma patientsH2 BZDs are not associated with PTSD-associ-ated symptoms in patients with PTSDH3 BZDs are not associated with PTSD-associ-ated symptoms in trauma patients with andwithout PTSD
282 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
In each case the hypothesis was tested using ameta-analysis carried out in the MetaEasy Exceladd-in (httpwwwstatanalysiscoukmeta-analysishtml) Studies included in the meta-analysis werethose that compared outcomes between a group ofpatients given BZDs and a control group An esti-mate and 95 confidence interval (CI) for thestandardized effect size (ES) was computed for eachoutcome in a study To compute a single effect esti-mate for each study MetaEasy uses the within-study median ES and confidence limits Finally ameta-analysis was used to test each hypothesis afterpooling information over all of the relevant studiesNote that the meta-analysis for H3 is not simplypooling the other 2 meta-analyses but includes allPTSD-related outcomes in addition to ldquoPTSD diag-nosisrdquo which was the only outcome measured in H1
Using a random-effects model (to account for theheterogeneity between studies) we estimated the ESand 95 CI associated with each hypothesis Alltests were 2 sided and at the 005 level ofsignificance
RESULTS
Study Characteristics
The authors reviewed 8422 citations 249 abstractsand 109 full-text articles The selection process isillustrated in Figure 1 using the PRISMA flowdiagram7 with reasons for exclusion The percentagreement (kappa statistic) for eligibilitywas as follows full-text review 899 (κ=063)randomized-controlled trials (RCTs) 991
FIGURE 1 Flow diagram of literature search results from identification to inclusion of studies
Records identified through database searching
(n = 9093) Google Scholar (n = 8392) PubMed (n = 515) PsycINFO (n = 162) MEDLINE (n = 22) Cochrane Library (n = 14)
Records after duplicates removed(n = 8422)
Records screened (n = 249)
Records excluded (n = 140)
Not related to benzodiazepines in PTSD
Full-text articles assessed for eligibility
(n = 109)
Full-text articles excluded (n = 91)
Reviewspractice guidelines (n = 58) No PTSD treatment outcomes (n = 18) Case reportsseries (n = 6) Benzodiazepines not distinguished from
other medications (n = 5) Participants not PTSD or trauma
patients (n = 4)Studies included in qualitative
synthesis (n = 18)
Studies included in meta-analysis
(n = 12)
Additional records identified through other sources
(n = 6) Unique references from
retrieved records
Iden
tifi
cati
on
S
cree
nin
g
Elig
ibili
ty
Incl
ud
ed
PTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 283
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
andObse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Rothb
aum
etal
8Ran
domized
-controlled
trial
103pa
tien
tswith
PTSD
invirtua
lrealityex
posu
retherap
y(sufficien
tda
taformeta-
analysis
was
availableon
lyfor
69pa
tien
ts)
Alprazolam
(025
mgpe
rsession
for5sessions
)
12mo
CAPS
Tho
setakingBZDssign
ificantlymorelike
lyto
have
PTSD
at3mopo
sttrea
tmen
tthan
those
takingplaceb
o(83
compa
redwith48
)No
sign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
sat
anyother
time
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
thech
ange
inPTSD
symptom
sOrbicularis
oculiEMG
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
startleresp
onse
Salivary
cortisol
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
cortisol
leve
ls
Mellm
anet
al9
Ran
domized
-controlled
trial
22recent
physical
trau
mapa
tien
tswithinsomnia
Tem
azep
am(30
mgfor5nigh
tsthen
15mgfor
2nigh
ts)
6wkor
before
starting
nons
tudy
med
ication
CAPS
Tho
setakingBZDsmorelike
lyto
deve
lop
PTSD
than
thosetakingplaceb
o(55
compa
redwith27
)bu
tdifferen
cewas
not
sign
ificant
Sleep
diary
Tho
setakingBZDshad
sign
ificantlyincrea
sed
slee
pdu
ration
onthefirstnightcompa
red
withthosetakingplaceb
oNosign
ificant
differen
cebe
twee
nBZDsan
dplaceb
oon
any
slee
pmea
sure
atan
yother
time
Braun
etal
10Ran
domized
-controlled
trial
10pa
tien
tswith
PTSD
Alprazolam
(15-6
mgdfor
5wk
then
2wk
tape
r)
12wk
PTSD
Scale
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
s
IES
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
sHAM-A
Tho
setakingBZDshad
sign
ificantlyde
crea
sed
anxietycompa
redwiththosetakingplaceb
oHAM-D
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
depr
ession
VAS
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
overallwell-be
ing
Cates
etal
11Ran
domized
-controlled
trial
6pa
tien
tswith
PTSD
Clona
zepa
m(1
mgfor7
nigh
tsthen
2mgfor7nigh
ts
then
1wktape
r)
5wk
CAPS-
adap
ted
slee
pdiary
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oon
anyslee
pmea
sure
orin
nigh
tmares
Gelpinet
al12
Non
rand
omized
-controlled
trial
26recent
physical
trau
mapa
tien
tsAlprazolam
(25
mgd)
orclon
azep
am(27plusmn08mgd)
for1-6mo
6mo
CAPS
Tho
setakingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(69
vs15
)
284 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
IES
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sMIS
SNosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sSCID
Tho
setakingBZDssign
ificantlymorelike
lyto
deve
lopmajor
depr
essive
disord
erthan
those
not
takingBZDs(54
vs0
)Nosign
ificant
differen
cebe
twee
nBZDsan
dnoBZDsin
deve
lopm
entof
phob
ias
alcohol
abusep
anic
disord
eror
dysthym
iaSTAI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
anxiety
BDI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
depr
ession
Hea
rtrate
Tho
setakingBZDshad
decrea
sedhea
rtrate
inthefirstwee
kcompa
redwiththosenot
takingBZDs
butthis
differen
cewas
not
sign
ificantNosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
hea
rtrate
atan
yother
time
Sha
levet
al13
Non
rand
omized
compa
rison
trial
18pa
tien
ts(9
with
PTSD9with
panicdisord
er)
Alprazolam
(205plusmn
069
mgd)
2wk
HAM-A
Nosign
ificantdifferen
cebe
twee
nPTSD
and
panic
disord
erin
prestimulation
anxiety
Orbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
npa
tien
tswithPTSD
andpa
nic
disord
erin
physiologicalmea
suresbe
fore
BZDs
Acoustic
startleresp
onsesin
PTSD
werenot
statisticallydifferen
tbe
fore
andafterBZDs
butthey
weresign
ificantlyde
crea
sedin
patien
tswithpa
nic
disord
erafterBZDs
Zatzicket
al14
Prosp
ective
coho
rt29
31ph
ysical
trau
mapa
tien
tsAny
agen
tdo
se
anddu
ration
12mo
PCL
Tho
sereceivingBZDsbe
fore
injury
sign
ificantlymorelike
lyto
hav
ePTSD
symptom
sthan
thosenot
takingBZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 285
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Shinet
al15
Prosp
ective
coho
rt37
6pa
tien
tswith
PTSD
Any
agen
tdo
se
anddu
ration
5-12
mo
CTS
Tho
sewithahistory
ofag
gression
taking
BZDshad
sign
ificantlyincrea
sedag
gression
compa
redwiththosenot
takingBZDsan
dthosewithou
tahistory
ofag
gression
Kostenet
al16
Prosp
ective
coho
rt37
0pa
tien
tswith
PTSD
inmen
tal
health
trea
tmen
t
Any
agen
tdo
se
anddu
ration
12mo
MIS
STho
setakingBZDshad
sign
ificantlyincrea
sed
PTSD
symptom
sat
baselinecompa
redwith
thosenot
takingBZDs
BSI
Tho
setaking
BZD
sha
dsign
ificantly
increa
sed
anxietyat
baselin
ecompa
redwiththoseno
ttaking
BZD
sNosign
ificant
diffe
rencebe
tween
BZD
san
dno
BZD
sin
chan
gein
anxiety
NVVRS-
derive
dinstru
men
t
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
violen
ceat
baseline
Thosewith
comorbidSUD
takingBZDshad
less
impr
ovem
entin
violen
cecompa
redwith
thosewithcomorbidSUD
not
takingBZDs
butthis
differen
cewas
not
sign
ificant
ASI
Tho
setakingBZDshad
sign
ificantlyincrea
sed
alcohol
use
atba
selinecompa
redwiththose
not
takingBZDs
Nosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
chan
gein
subs
tance
use
orsocial
functioning
Those
withcomorbidSUD
takingBZDshad
less
impr
ovem
entin
subs
tance
use
compa
red
withthosewithcomorbidSUD
not
taking
BZDs
butthis
differen
cewas
not
sign
ificant
Rosen
etal
17Prosp
ective
coho
rt28
3pa
tien
tswith
PTSD
(140
inpr
olon
ged
expo
sure14
3in
presen
t-centered
psycho
therap
ysu
fficien
tda
tafor
meta-an
alysis
was
only
availablefor
143pa
tien
ts)
Any
agen
tdo
se
anddu
ration
6mo
CAPS
Nosign
ificance
differen
cebe
twee
nBZDswith
prolon
gedex
posu
rean
dnoBZDswitheither
therap
yin
PTSD
symptom
sThosetaking
BZDsin
presen
t-centeredps
ychotherap
yhad
sign
ificantlyworse
posttrea
tmen
tmaintenan
ceof
impr
ovem
ents
inPTSD
symptom
scompa
redwithother
grou
psPCL
Inpr
esen
t-centeredtherap
ythosetaking
BZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
sdu
ringps
ychotherap
ycompa
redwiththosenot
takingBZDs
Significance
ofresu
ltsforpr
olon
gedex
posu
rewerenot
determ
inab
ledu
eto
presen
ceof
aninteractionterm
andtheway
theresu
lts
werepr
esen
ted
286 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Jone
set
al18
Prosp
ective
coho
rt23
8recent
trau
mapa
tien
ts(ICU)
Any
agen
tdo
sean
ddu
ration
3mo
PTSS-14
Higher
BZD
dosesin
theIC
Uas
sociated
with
sign
ificantlyincrea
sedPTSD
symptom
s
Sam
uelson
etal
19Prosp
ective
coho
rt22
6recent
trau
ma
patien
ts(ICU)
Midaz
olam
(any
dose
ordu
ration
)
2mo
IES-R
Tho
sereceivingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(68
vs30
)
Bienv
enu
etal
20Prosp
ective
coho
rt18
6recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
3-24
mo
IES-R
Higher
BZD
dosesin
theIC
Unot
associated
withsign
ificantch
ange
sin
therisk
ofde
velopingPTSD
Baran
yiet
al21
Prosp
ective
coho
rt12
6trau
ma
patien
ts(solid-organ
tran
splants)
Any
agen
tdo
se
anddu
ration
Mea
nof
249
mo
PTSS-10
Chronic
BZD
useeither
before
orafter
surgery
associated
withsign
ificantly
increa
sedrisk
ofPTSD
symptom
s
Girardet
al22
Prosp
ective
coho
rt43
recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
6mo
PTSS-10
Greater
BZD
administrationin
theIC
Uas
sociated
withsign
ificantlyincrea
sedrisk
ofde
velopingPTSD
Van
Minne
net
al23
Prosp
ective
coho
rt43
patien
tswith
PTSD
inpr
olon
ged
expo
sure
Daily
useof
any
agen
tor
dose
3mo
PSS-SR
Tho
setakingBZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
san
dmore
drop
outs
compa
redwiththosenot
taking
BZDs
McG
hee
etal
24Retrosp
ective
coho
rt21
1trau
ma
patien
ts(bur
nsrequ
iringsu
rgery)
Midaz
olam
(any
dose
intrao
perative
)
Any
upto
4y
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
risk
ofde
velopingPTSD
Sha
levan
dRog
el-
Fuc
hs25
Cross-section
al18
patien
tswith
PTSD
Clona
zepa
m(27plusmn11mgd)
Not ap
plicab
leOrbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
mag
nitude
orhab
ituationrate
ofacou
stic
startleresp
onses
ASIindicates
Addiction
SeverityIn
dexB
DIBeckDep
ressionIn
ventoryB
SIBrief
Sym
ptom
Inventory
BZDb
enzodiazepineCAPSC
linician-administeredPTSD
Sca
leCTSCon
flicts
Tac
tics
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRatingSca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionIC
U
intensive
care
unitI
ESIm
pact
ofEvent
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDN
VVRSNational
Vietnam
Veteran
sRea
djustmen
tStudy
PCLP
TSD
ChecklistPSS-SRP
TSD
Sym
ptom
Sca
leSelf-repo
rtP
TSSP
osttra
umatic
StressSyn
dromeSca
leP
TSDp
osttra
umatic
stress
disorderS
CID
StructuredClinical
Interview
fortheDSMSTAI
State-Tra
itAnxietyIn
ventoryS
UDsu
bstance
use
disorderVASvisu
alan
alog
scale
Journal of Psychiatric Practice Vol 21 No 4 July 2015 287
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
umaTyp
e(
)
Rothb
aum
etal
8IIraq
andor
Afgha
nistan
veterans
DSM-IVcriteria
forPTSD
dueto
militarytrau
mave
rified
throug
hdischa
rgepa
pers
discon
tinu
edtaking
long
-actingBZD
sfor1moan
dsh
ort-
acting
BZD
sfor2wkbe
fore
screen
ing
stab
ledo
sesof
othe
rps
ycho
trop
icmed
ications
forat
leas
t2wkbe
fore
thestud
ywritten
inform
edconsent
EMed
ically
unstab
leps
ycho
sis
bipo
lardisord
erc
urrent
suicidal
risk
cu
rren
talcoho
lor
drug
depe
nden
ce
preg
nanc
ygluc
ocorticoids
BZD
sch
ronicallyus
edop
ioids
354
Black
50
White
42
Hispa
nic5
Other3
Com
bat10
0
Mellm
anet
al9
IAdm
ittedto
leve
lItrau
macenterr
ecallof
trau
ma
atleas
tmod
erateim
pairmen
tof
slee
pinitiation
ormainten
ance
mee
tfullcriteria
forat
leas
t2PTSD
symptom
clus
ters
inDSM-IVwilling
andab
leto
prov
idewritten
inform
edcons
ent
EIn
toxication
attimeof
trau
ma
braininjurypr
eexisting
psychiatricdisord
ers
3636
Hispa
nic8
2White
9Black
9
MVC68
Assau
lt2
3Acciden
t9
Braun
etal
10I
DSM-III
criteria
forPTSDwilling
andab
leto
prov
ide
written
inform
edconsentfreeof
psycho
trop
icmed
ications
atleas
t2wkbe
fore
stud
yEPhy
sicallyun
healthy
sign
ificant
head
injury
38Com
bat40
MVC30
Acciden
t20
Terrorism
10
Cates
etal
11I
DSM-IV
criteria
forPTSDat
leas
tthrice
wee
klypr
oblems
withslee
pan
dnigh
tmaresw
illing
andab
leto
prov
ide
written
inform
edconsent
Elt
18yold
unstab
lemed
ical
cond
itions
sen
sitivity
toBZD
scu
rren
tBZD
use
subs
tanc
eab
useor
depe
nden
cein
past
4wk
inab
ilityto
attend
regu
larfollow
-upvisitswom
enwho
wereeither
preg
nant
orof
child-be
aringpo
tentialan
dno
tus
ingcontraceptivesde
men
tia
cogn
itivedisord
er
520
Com
bat10
0
Gelpinet
al12
IEmerge
ncyroom
admission
swithatrau
ma
ETak
ingps
ycho
trop
icmed
ications
before
thetrau
ma
coma
head
injuryloss
ofcons
ciou
sness
2946
MVCs
77
Terrorism
19
Acciden
t4
Sha
levet
al13
IDSM-III-R
criteria
forPTSD
orpa
nicdisord
ermed
ication
free
EPsych
osism
ajor
depr
ession
cur
rent
orpa
stsu
bstanc
eor
alcoho
lus
epa
tien
tswithPTSD
withsp
ontane
ouspa
nic
attack
spa
tien
tswithpa
nicdisord
erwithahistoryof
trau
ma
3439
288 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
Zatzicket
al14
I18
-84yold
Eng
lish
-spe
akingor
Spa
nish
-spe
akingpa
tien
ts
arrive
daliveat
hosp
italm
oderateto
seve
reinjuries
Eg
reater
than
oreq
ual
toge65
yoldwithafirstlisted
diag
nosisof
hipfracturem
ajor
burn
strea
tmen
tde
lays
gt24
hincarcerated
attimeof
injury
4135
White
67
Black
16
Hispa
nic13
Other3
Injury10
0
Shinet
al15
I18
-69yold
militaryve
terans
servingin
Vietnam
eraor
laterat
leas
ton
eou
tpatient
VAvisitwithaPTSD
diag
nosis
EN
oPTSD
diag
nosisin
thepr
ior2y
4250
White
65
Black
17
Hispa
nic10
Other3
Kostenet
al16
IDSM-III
criteria
forPTSDmilitaryve
terans
450
White
75
Rosen
etal
17I
femaleve
teranor
active
duty
soldier
DSM-IV
criteria
for
PTSDCAPSscoregt45
EC
oncu
rren
tPTSD
psycho
therap
yothe
rthan
briefvisits
withan
existing
therap
istor
participationin
self-help
grou
psc
hang
ein
psycho
active
med
ications
during
the2mo
before
stud
yrecruitm
entsu
bstanc
ede
pend
ence
notin
remission
forat
leas
t3mo
curren
tps
ycho
ticsymptom
sor
man
iab
ipolar
disord
erpr
ominen
tcu
rren
tsu
icidal
orho
micidal
idea
tion
cogn
itiveim
pairmen
tcu
rren
tinvo
lvem
entin
violen
trelation
shipself-m
utilationwithin
thepa
st6mo
100
White
55
Black
33
Hispa
nic
6Other7
Sex
ual93
Acciden
t82
Disas
ter
72
Com
bat25
Jone
set
al18
Igt18
yold
mecha
nicallyve
ntilated
IC
Uleng
thof
stay
atleas
t48
hEP
rior
PTSDa
dmittedaftersu
icideattemptp
reex
isting
orconc
omitan
tps
ycho
ticillness
reside
sgt30
kmfrom
hosp
ital
unresolved
confus
ionen
rolled
inan
othe
rresearch
stud
y
6138
Life-threaten
ingmed
ical
condition
10
0
Sam
uelson
etal
19I
gt18
yold
mecha
nicallyve
ntilated
ge
neralIC
Uleng
thof
stay
atleas
t24
hEH
eadinjuryps
ycho
ticillness
men
talretard
ation
intoxication
adm
ittedaftersu
icideattempth
earing
spe
ech
disa
bilityno
n-Swed
ishsp
eaking
tran
sferredto
anothe
rho
spitalm
echa
nicallyve
ntilated
atdischa
rge
mecha
nically
ventilated
gt24
hpr
eadm
ission
6348
Life-threaten
ingmed
ical
condition
10
0
Bienv
enuet
al20
IMecha
nicallyve
ntilated
withacutelung
injury
EN
eurologicalsp
ecialtyIC
Upr
eexistingillnesswithalife
expe
ctan
cylt6mo
pree
xistingcogn
itiveim
pairmen
tor
commun
icationlang
uage
barriersn
ofixe
dad
dress
tran
sfer
toastud
ysite
ICU
withpr
eexistingacutelung
injury
gt24
h
45
Life-threaten
ingmed
ical
condition
10
0
Journal of Psychiatric Practice Vol 21 No 4 July 2015 289
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
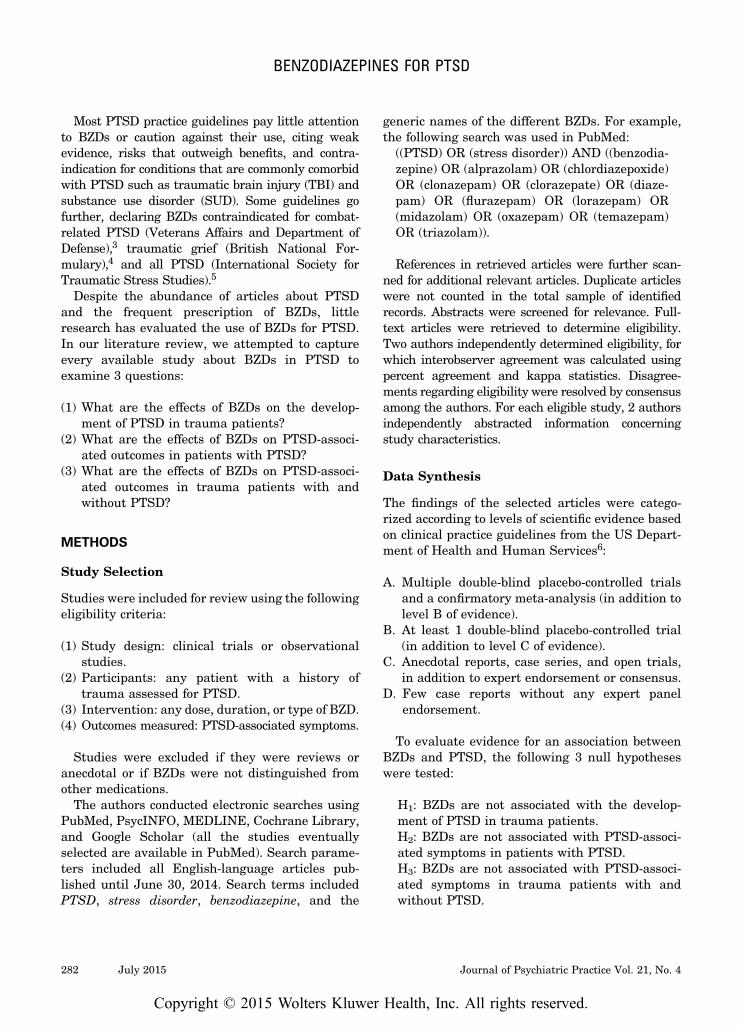
Most PTSD practice guidelines pay little attentionto BZDs or caution against their use citing weakevidence risks that outweigh benefits and contra-indication for conditions that are commonly comorbidwith PTSD such as traumatic brain injury (TBI) andsubstance use disorder (SUD) Some guidelines gofurther declaring BZDs contraindicated for combat-related PTSD (Veterans Affairs and Department ofDefense)3 traumatic grief (British National For-mulary)4 and all PTSD (International Society forTraumatic Stress Studies)5
Despite the abundance of articles about PTSDand the frequent prescription of BZDs littleresearch has evaluated the use of BZDs for PTSDIn our literature review we attempted to captureevery available study about BZDs in PTSD toexamine 3 questions
(1) What are the effects of BZDs on the develop-ment of PTSD in trauma patients
(2) What are the effects of BZDs on PTSD-associ-ated outcomes in patients with PTSD
(3) What are the effects of BZDs on PTSD-associ-ated outcomes in trauma patients with andwithout PTSD
METHODS
Study Selection
Studies were included for review using the followingeligibility criteria
(1) Study design clinical trials or observationalstudies
(2) Participants any patient with a history oftrauma assessed for PTSD
(3) Intervention any dose duration or type of BZD(4) Outcomes measured PTSD-associated symptoms
Studies were excluded if they were reviews oranecdotal or if BZDs were not distinguished fromother medications
The authors conducted electronic searches usingPubMed PsycINFO MEDLINE Cochrane Libraryand Google Scholar (all the studies eventuallyselected are available in PubMed) Search parame-ters included all English-language articles pub-lished until June 30 2014 Search terms includedPTSD stress disorder benzodiazepine and the
generic names of the different BZDs For examplethe following search was used in PubMed
((PTSD) OR (stress disorder)) AND ((benzodia-zepine) OR (alprazolam) OR (chlordiazepoxide)OR (clonazepam) OR (clorazepate) OR (diaze-pam) OR (flurazepam) OR (lorazepam) OR(midazolam) OR (oxazepam) OR (temazepam)OR (triazolam))
References in retrieved articles were further scan-ned for additional relevant articles Duplicate articleswere not counted in the total sample of identifiedrecords Abstracts were screened for relevance Full-text articles were retrieved to determine eligibilityTwo authors independently determined eligibility forwhich interobserver agreement was calculated usingpercent agreement and kappa statistics Disagree-ments regarding eligibility were resolved by consensusamong the authors For each eligible study 2 authorsindependently abstracted information concerningstudy characteristics
Data Synthesis
The findings of the selected articles were catego-rized according to levels of scientific evidence basedon clinical practice guidelines from the US Depart-ment of Health and Human Services6
A Multiple double-blind placebo-controlled trialsand a confirmatory meta-analysis (in addition tolevel B of evidence)
B At least 1 double-blind placebo-controlled trial(in addition to level C of evidence)
C Anecdotal reports case series and open trialsin addition to expert endorsement or consensus
D Few case reports without any expert panelendorsement
To evaluate evidence for an association betweenBZDs and PTSD the following 3 null hypotheseswere tested
H1 BZDs are not associated with the develop-ment of PTSD in trauma patientsH2 BZDs are not associated with PTSD-associ-ated symptoms in patients with PTSDH3 BZDs are not associated with PTSD-associ-ated symptoms in trauma patients with andwithout PTSD
282 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
In each case the hypothesis was tested using ameta-analysis carried out in the MetaEasy Exceladd-in (httpwwwstatanalysiscoukmeta-analysishtml) Studies included in the meta-analysis werethose that compared outcomes between a group ofpatients given BZDs and a control group An esti-mate and 95 confidence interval (CI) for thestandardized effect size (ES) was computed for eachoutcome in a study To compute a single effect esti-mate for each study MetaEasy uses the within-study median ES and confidence limits Finally ameta-analysis was used to test each hypothesis afterpooling information over all of the relevant studiesNote that the meta-analysis for H3 is not simplypooling the other 2 meta-analyses but includes allPTSD-related outcomes in addition to ldquoPTSD diag-nosisrdquo which was the only outcome measured in H1
Using a random-effects model (to account for theheterogeneity between studies) we estimated the ESand 95 CI associated with each hypothesis Alltests were 2 sided and at the 005 level ofsignificance
RESULTS
Study Characteristics
The authors reviewed 8422 citations 249 abstractsand 109 full-text articles The selection process isillustrated in Figure 1 using the PRISMA flowdiagram7 with reasons for exclusion The percentagreement (kappa statistic) for eligibilitywas as follows full-text review 899 (κ=063)randomized-controlled trials (RCTs) 991
FIGURE 1 Flow diagram of literature search results from identification to inclusion of studies
Records identified through database searching
(n = 9093) Google Scholar (n = 8392) PubMed (n = 515) PsycINFO (n = 162) MEDLINE (n = 22) Cochrane Library (n = 14)
Records after duplicates removed(n = 8422)
Records screened (n = 249)
Records excluded (n = 140)
Not related to benzodiazepines in PTSD
Full-text articles assessed for eligibility
(n = 109)
Full-text articles excluded (n = 91)
Reviewspractice guidelines (n = 58) No PTSD treatment outcomes (n = 18) Case reportsseries (n = 6) Benzodiazepines not distinguished from
other medications (n = 5) Participants not PTSD or trauma
patients (n = 4)Studies included in qualitative
synthesis (n = 18)
Studies included in meta-analysis
(n = 12)
Additional records identified through other sources
(n = 6) Unique references from
retrieved records
Iden
tifi
cati
on
S
cree
nin
g
Elig
ibili
ty
Incl
ud
ed
PTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 283
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
andObse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Rothb
aum
etal
8Ran
domized
-controlled
trial
103pa
tien
tswith
PTSD
invirtua
lrealityex
posu
retherap
y(sufficien
tda
taformeta-
analysis
was
availableon
lyfor
69pa
tien
ts)
Alprazolam
(025
mgpe
rsession
for5sessions
)
12mo
CAPS
Tho
setakingBZDssign
ificantlymorelike
lyto
have
PTSD
at3mopo
sttrea
tmen
tthan
those
takingplaceb
o(83
compa
redwith48
)No
sign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
sat
anyother
time
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
thech
ange
inPTSD
symptom
sOrbicularis
oculiEMG
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
startleresp
onse
Salivary
cortisol
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
cortisol
leve
ls
Mellm
anet
al9
Ran
domized
-controlled
trial
22recent
physical
trau
mapa
tien
tswithinsomnia
Tem
azep
am(30
mgfor5nigh
tsthen
15mgfor
2nigh
ts)
6wkor
before
starting
nons
tudy
med
ication
CAPS
Tho
setakingBZDsmorelike
lyto
deve
lop
PTSD
than
thosetakingplaceb
o(55
compa
redwith27
)bu
tdifferen
cewas
not
sign
ificant
Sleep
diary
Tho
setakingBZDshad
sign
ificantlyincrea
sed
slee
pdu
ration
onthefirstnightcompa
red
withthosetakingplaceb
oNosign
ificant
differen
cebe
twee
nBZDsan
dplaceb
oon
any
slee
pmea
sure
atan
yother
time
Braun
etal
10Ran
domized
-controlled
trial
10pa
tien
tswith
PTSD
Alprazolam
(15-6
mgdfor
5wk
then
2wk
tape
r)
12wk
PTSD
Scale
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
s
IES
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
sHAM-A
Tho
setakingBZDshad
sign
ificantlyde
crea
sed
anxietycompa
redwiththosetakingplaceb
oHAM-D
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
depr
ession
VAS
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
overallwell-be
ing
Cates
etal
11Ran
domized
-controlled
trial
6pa
tien
tswith
PTSD
Clona
zepa
m(1
mgfor7
nigh
tsthen
2mgfor7nigh
ts
then
1wktape
r)
5wk
CAPS-
adap
ted
slee
pdiary
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oon
anyslee
pmea
sure
orin
nigh
tmares
Gelpinet
al12
Non
rand
omized
-controlled
trial
26recent
physical
trau
mapa
tien
tsAlprazolam
(25
mgd)
orclon
azep
am(27plusmn08mgd)
for1-6mo
6mo
CAPS
Tho
setakingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(69
vs15
)
284 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
IES
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sMIS
SNosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sSCID
Tho
setakingBZDssign
ificantlymorelike
lyto
deve
lopmajor
depr
essive
disord
erthan
those
not
takingBZDs(54
vs0
)Nosign
ificant
differen
cebe
twee
nBZDsan
dnoBZDsin
deve
lopm
entof
phob
ias
alcohol
abusep
anic
disord
eror
dysthym
iaSTAI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
anxiety
BDI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
depr
ession
Hea
rtrate
Tho
setakingBZDshad
decrea
sedhea
rtrate
inthefirstwee
kcompa
redwiththosenot
takingBZDs
butthis
differen
cewas
not
sign
ificantNosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
hea
rtrate
atan
yother
time
Sha
levet
al13
Non
rand
omized
compa
rison
trial
18pa
tien
ts(9
with
PTSD9with
panicdisord
er)
Alprazolam
(205plusmn
069
mgd)
2wk
HAM-A
Nosign
ificantdifferen
cebe
twee
nPTSD
and
panic
disord
erin
prestimulation
anxiety
Orbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
npa
tien
tswithPTSD
andpa
nic
disord
erin
physiologicalmea
suresbe
fore
BZDs
Acoustic
startleresp
onsesin
PTSD
werenot
statisticallydifferen
tbe
fore
andafterBZDs
butthey
weresign
ificantlyde
crea
sedin
patien
tswithpa
nic
disord
erafterBZDs
Zatzicket
al14
Prosp
ective
coho
rt29
31ph
ysical
trau
mapa
tien
tsAny
agen
tdo
se
anddu
ration
12mo
PCL
Tho
sereceivingBZDsbe
fore
injury
sign
ificantlymorelike
lyto
hav
ePTSD
symptom
sthan
thosenot
takingBZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 285
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Shinet
al15
Prosp
ective
coho
rt37
6pa
tien
tswith
PTSD
Any
agen
tdo
se
anddu
ration
5-12
mo
CTS
Tho
sewithahistory
ofag
gression
taking
BZDshad
sign
ificantlyincrea
sedag
gression
compa
redwiththosenot
takingBZDsan
dthosewithou
tahistory
ofag
gression
Kostenet
al16
Prosp
ective
coho
rt37
0pa
tien
tswith
PTSD
inmen
tal
health
trea
tmen
t
Any
agen
tdo
se
anddu
ration
12mo
MIS
STho
setakingBZDshad
sign
ificantlyincrea
sed
PTSD
symptom
sat
baselinecompa
redwith
thosenot
takingBZDs
BSI
Tho
setaking
BZD
sha
dsign
ificantly
increa
sed
anxietyat
baselin
ecompa
redwiththoseno
ttaking
BZD
sNosign
ificant
diffe
rencebe
tween
BZD
san
dno
BZD
sin
chan
gein
anxiety
NVVRS-
derive
dinstru
men
t
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
violen
ceat
baseline
Thosewith
comorbidSUD
takingBZDshad
less
impr
ovem
entin
violen
cecompa
redwith
thosewithcomorbidSUD
not
takingBZDs
butthis
differen
cewas
not
sign
ificant
ASI
Tho
setakingBZDshad
sign
ificantlyincrea
sed
alcohol
use
atba
selinecompa
redwiththose
not
takingBZDs
Nosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
chan
gein
subs
tance
use
orsocial
functioning
Those
withcomorbidSUD
takingBZDshad
less
impr
ovem
entin
subs
tance
use
compa
red
withthosewithcomorbidSUD
not
taking
BZDs
butthis
differen
cewas
not
sign
ificant
Rosen
etal
17Prosp
ective
coho
rt28
3pa
tien
tswith
PTSD
(140
inpr
olon
ged
expo
sure14
3in
presen
t-centered
psycho
therap
ysu
fficien
tda
tafor
meta-an
alysis
was
only
availablefor
143pa
tien
ts)
Any
agen
tdo
se
anddu
ration
6mo
CAPS
Nosign
ificance
differen
cebe
twee
nBZDswith
prolon
gedex
posu
rean
dnoBZDswitheither
therap
yin
PTSD
symptom
sThosetaking
BZDsin
presen
t-centeredps
ychotherap
yhad
sign
ificantlyworse
posttrea
tmen
tmaintenan
ceof
impr
ovem
ents
inPTSD
symptom
scompa
redwithother
grou
psPCL
Inpr
esen
t-centeredtherap
ythosetaking
BZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
sdu
ringps
ychotherap
ycompa
redwiththosenot
takingBZDs
Significance
ofresu
ltsforpr
olon
gedex
posu
rewerenot
determ
inab
ledu
eto
presen
ceof
aninteractionterm
andtheway
theresu
lts
werepr
esen
ted
286 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Jone
set
al18
Prosp
ective
coho
rt23
8recent
trau
mapa
tien
ts(ICU)
Any
agen
tdo
sean
ddu
ration
3mo
PTSS-14
Higher
BZD
dosesin
theIC
Uas
sociated
with
sign
ificantlyincrea
sedPTSD
symptom
s
Sam
uelson
etal
19Prosp
ective
coho
rt22
6recent
trau
ma
patien
ts(ICU)
Midaz
olam
(any
dose
ordu
ration
)
2mo
IES-R
Tho
sereceivingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(68
vs30
)
Bienv
enu
etal
20Prosp
ective
coho
rt18
6recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
3-24
mo
IES-R
Higher
BZD
dosesin
theIC
Unot
associated
withsign
ificantch
ange
sin
therisk
ofde
velopingPTSD
Baran
yiet
al21
Prosp
ective
coho
rt12
6trau
ma
patien
ts(solid-organ
tran
splants)
Any
agen
tdo
se
anddu
ration
Mea
nof
249
mo
PTSS-10
Chronic
BZD
useeither
before
orafter
surgery
associated
withsign
ificantly
increa
sedrisk
ofPTSD
symptom
s
Girardet
al22
Prosp
ective
coho
rt43
recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
6mo
PTSS-10
Greater
BZD
administrationin
theIC
Uas
sociated
withsign
ificantlyincrea
sedrisk
ofde
velopingPTSD
Van
Minne
net
al23
Prosp
ective
coho
rt43
patien
tswith
PTSD
inpr
olon
ged
expo
sure
Daily
useof
any
agen
tor
dose
3mo
PSS-SR
Tho
setakingBZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
san
dmore
drop
outs
compa
redwiththosenot
taking
BZDs
McG
hee
etal
24Retrosp
ective
coho
rt21
1trau
ma
patien
ts(bur
nsrequ
iringsu
rgery)
Midaz
olam
(any
dose
intrao
perative
)
Any
upto
4y
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
risk
ofde
velopingPTSD
Sha
levan
dRog
el-
Fuc
hs25
Cross-section
al18
patien
tswith
PTSD
Clona
zepa
m(27plusmn11mgd)
Not ap
plicab
leOrbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
mag
nitude
orhab
ituationrate
ofacou
stic
startleresp
onses
ASIindicates
Addiction
SeverityIn
dexB
DIBeckDep
ressionIn
ventoryB
SIBrief
Sym
ptom
Inventory
BZDb
enzodiazepineCAPSC
linician-administeredPTSD
Sca
leCTSCon
flicts
Tac
tics
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRatingSca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionIC
U
intensive
care
unitI
ESIm
pact
ofEvent
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDN
VVRSNational
Vietnam
Veteran
sRea
djustmen
tStudy
PCLP
TSD
ChecklistPSS-SRP
TSD
Sym
ptom
Sca
leSelf-repo
rtP
TSSP
osttra
umatic
StressSyn
dromeSca
leP
TSDp
osttra
umatic
stress
disorderS
CID
StructuredClinical
Interview
fortheDSMSTAI
State-Tra
itAnxietyIn
ventoryS
UDsu
bstance
use
disorderVASvisu
alan
alog
scale
Journal of Psychiatric Practice Vol 21 No 4 July 2015 287
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
umaTyp
e(
)
Rothb
aum
etal
8IIraq
andor
Afgha
nistan
veterans
DSM-IVcriteria
forPTSD
dueto
militarytrau
mave
rified
throug
hdischa
rgepa
pers
discon
tinu
edtaking
long
-actingBZD
sfor1moan
dsh
ort-
acting
BZD
sfor2wkbe
fore
screen
ing
stab
ledo
sesof
othe
rps
ycho
trop
icmed
ications
forat
leas
t2wkbe
fore
thestud
ywritten
inform
edconsent
EMed
ically
unstab
leps
ycho
sis
bipo
lardisord
erc
urrent
suicidal
risk
cu
rren
talcoho
lor
drug
depe
nden
ce
preg
nanc
ygluc
ocorticoids
BZD
sch
ronicallyus
edop
ioids
354
Black
50
White
42
Hispa
nic5
Other3
Com
bat10
0
Mellm
anet
al9
IAdm
ittedto
leve
lItrau
macenterr
ecallof
trau
ma
atleas
tmod
erateim
pairmen
tof
slee
pinitiation
ormainten
ance
mee
tfullcriteria
forat
leas
t2PTSD
symptom
clus
ters
inDSM-IVwilling
andab
leto
prov
idewritten
inform
edcons
ent
EIn
toxication
attimeof
trau
ma
braininjurypr
eexisting
psychiatricdisord
ers
3636
Hispa
nic8
2White
9Black
9
MVC68
Assau
lt2
3Acciden
t9
Braun
etal
10I
DSM-III
criteria
forPTSDwilling
andab
leto
prov
ide
written
inform
edconsentfreeof
psycho
trop
icmed
ications
atleas
t2wkbe
fore
stud
yEPhy
sicallyun
healthy
sign
ificant
head
injury
38Com
bat40
MVC30
Acciden
t20
Terrorism
10
Cates
etal
11I
DSM-IV
criteria
forPTSDat
leas
tthrice
wee
klypr
oblems
withslee
pan
dnigh
tmaresw
illing
andab
leto
prov
ide
written
inform
edconsent
Elt
18yold
unstab
lemed
ical
cond
itions
sen
sitivity
toBZD
scu
rren
tBZD
use
subs
tanc
eab
useor
depe
nden
cein
past
4wk
inab
ilityto
attend
regu
larfollow
-upvisitswom
enwho
wereeither
preg
nant
orof
child-be
aringpo
tentialan
dno
tus
ingcontraceptivesde
men
tia
cogn
itivedisord
er
520
Com
bat10
0
Gelpinet
al12
IEmerge
ncyroom
admission
swithatrau
ma
ETak
ingps
ycho
trop
icmed
ications
before
thetrau
ma
coma
head
injuryloss
ofcons
ciou
sness
2946
MVCs
77
Terrorism
19
Acciden
t4
Sha
levet
al13
IDSM-III-R
criteria
forPTSD
orpa
nicdisord
ermed
ication
free
EPsych
osism
ajor
depr
ession
cur
rent
orpa
stsu
bstanc
eor
alcoho
lus
epa
tien
tswithPTSD
withsp
ontane
ouspa
nic
attack
spa
tien
tswithpa
nicdisord
erwithahistoryof
trau
ma
3439
288 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
Zatzicket
al14
I18
-84yold
Eng
lish
-spe
akingor
Spa
nish
-spe
akingpa
tien
ts
arrive
daliveat
hosp
italm
oderateto
seve
reinjuries
Eg
reater
than
oreq
ual
toge65
yoldwithafirstlisted
diag
nosisof
hipfracturem
ajor
burn
strea
tmen
tde
lays
gt24
hincarcerated
attimeof
injury
4135
White
67
Black
16
Hispa
nic13
Other3
Injury10
0
Shinet
al15
I18
-69yold
militaryve
terans
servingin
Vietnam
eraor
laterat
leas
ton
eou
tpatient
VAvisitwithaPTSD
diag
nosis
EN
oPTSD
diag
nosisin
thepr
ior2y
4250
White
65
Black
17
Hispa
nic10
Other3
Kostenet
al16
IDSM-III
criteria
forPTSDmilitaryve
terans
450
White
75
Rosen
etal
17I
femaleve
teranor
active
duty
soldier
DSM-IV
criteria
for
PTSDCAPSscoregt45
EC
oncu
rren
tPTSD
psycho
therap
yothe
rthan
briefvisits
withan
existing
therap
istor
participationin
self-help
grou
psc
hang
ein
psycho
active
med
ications
during
the2mo
before
stud
yrecruitm
entsu
bstanc
ede
pend
ence
notin
remission
forat
leas
t3mo
curren
tps
ycho
ticsymptom
sor
man
iab
ipolar
disord
erpr
ominen
tcu
rren
tsu
icidal
orho
micidal
idea
tion
cogn
itiveim
pairmen
tcu
rren
tinvo
lvem
entin
violen
trelation
shipself-m
utilationwithin
thepa
st6mo
100
White
55
Black
33
Hispa
nic
6Other7
Sex
ual93
Acciden
t82
Disas
ter
72
Com
bat25
Jone
set
al18
Igt18
yold
mecha
nicallyve
ntilated
IC
Uleng
thof
stay
atleas
t48
hEP
rior
PTSDa
dmittedaftersu
icideattemptp
reex
isting
orconc
omitan
tps
ycho
ticillness
reside
sgt30
kmfrom
hosp
ital
unresolved
confus
ionen
rolled
inan
othe
rresearch
stud
y
6138
Life-threaten
ingmed
ical
condition
10
0
Sam
uelson
etal
19I
gt18
yold
mecha
nicallyve
ntilated
ge
neralIC
Uleng
thof
stay
atleas
t24
hEH
eadinjuryps
ycho
ticillness
men
talretard
ation
intoxication
adm
ittedaftersu
icideattempth
earing
spe
ech
disa
bilityno
n-Swed
ishsp
eaking
tran
sferredto
anothe
rho
spitalm
echa
nicallyve
ntilated
atdischa
rge
mecha
nically
ventilated
gt24
hpr
eadm
ission
6348
Life-threaten
ingmed
ical
condition
10
0
Bienv
enuet
al20
IMecha
nicallyve
ntilated
withacutelung
injury
EN
eurologicalsp
ecialtyIC
Upr
eexistingillnesswithalife
expe
ctan
cylt6mo
pree
xistingcogn
itiveim
pairmen
tor
commun
icationlang
uage
barriersn
ofixe
dad
dress
tran
sfer
toastud
ysite
ICU
withpr
eexistingacutelung
injury
gt24
h
45
Life-threaten
ingmed
ical
condition
10
0
Journal of Psychiatric Practice Vol 21 No 4 July 2015 289
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

In each case the hypothesis was tested using ameta-analysis carried out in the MetaEasy Exceladd-in (httpwwwstatanalysiscoukmeta-analysishtml) Studies included in the meta-analysis werethose that compared outcomes between a group ofpatients given BZDs and a control group An esti-mate and 95 confidence interval (CI) for thestandardized effect size (ES) was computed for eachoutcome in a study To compute a single effect esti-mate for each study MetaEasy uses the within-study median ES and confidence limits Finally ameta-analysis was used to test each hypothesis afterpooling information over all of the relevant studiesNote that the meta-analysis for H3 is not simplypooling the other 2 meta-analyses but includes allPTSD-related outcomes in addition to ldquoPTSD diag-nosisrdquo which was the only outcome measured in H1
Using a random-effects model (to account for theheterogeneity between studies) we estimated the ESand 95 CI associated with each hypothesis Alltests were 2 sided and at the 005 level ofsignificance
RESULTS
Study Characteristics
The authors reviewed 8422 citations 249 abstractsand 109 full-text articles The selection process isillustrated in Figure 1 using the PRISMA flowdiagram7 with reasons for exclusion The percentagreement (kappa statistic) for eligibilitywas as follows full-text review 899 (κ=063)randomized-controlled trials (RCTs) 991
FIGURE 1 Flow diagram of literature search results from identification to inclusion of studies
Records identified through database searching
(n = 9093) Google Scholar (n = 8392) PubMed (n = 515) PsycINFO (n = 162) MEDLINE (n = 22) Cochrane Library (n = 14)
Records after duplicates removed(n = 8422)
Records screened (n = 249)
Records excluded (n = 140)
Not related to benzodiazepines in PTSD
Full-text articles assessed for eligibility
(n = 109)
Full-text articles excluded (n = 91)
Reviewspractice guidelines (n = 58) No PTSD treatment outcomes (n = 18) Case reportsseries (n = 6) Benzodiazepines not distinguished from
other medications (n = 5) Participants not PTSD or trauma
patients (n = 4)Studies included in qualitative
synthesis (n = 18)
Studies included in meta-analysis
(n = 12)
Additional records identified through other sources
(n = 6) Unique references from
retrieved records
Iden
tifi
cati
on
S
cree
nin
g
Elig
ibili
ty
Incl
ud
ed
PTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 283
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
andObse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Rothb
aum
etal
8Ran
domized
-controlled
trial
103pa
tien
tswith
PTSD
invirtua
lrealityex
posu
retherap
y(sufficien
tda
taformeta-
analysis
was
availableon
lyfor
69pa
tien
ts)
Alprazolam
(025
mgpe
rsession
for5sessions
)
12mo
CAPS
Tho
setakingBZDssign
ificantlymorelike
lyto
have
PTSD
at3mopo
sttrea
tmen
tthan
those
takingplaceb
o(83
compa
redwith48
)No
sign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
sat
anyother
time
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
thech
ange
inPTSD
symptom
sOrbicularis
oculiEMG
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
startleresp
onse
Salivary
cortisol
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
cortisol
leve
ls
Mellm
anet
al9
Ran
domized
-controlled
trial
22recent
physical
trau
mapa
tien
tswithinsomnia
Tem
azep
am(30
mgfor5nigh
tsthen
15mgfor
2nigh
ts)
6wkor
before
starting
nons
tudy
med
ication
CAPS
Tho
setakingBZDsmorelike
lyto
deve
lop
PTSD
than
thosetakingplaceb
o(55
compa
redwith27
)bu
tdifferen
cewas
not
sign
ificant
Sleep
diary
Tho
setakingBZDshad
sign
ificantlyincrea
sed
slee
pdu
ration
onthefirstnightcompa
red
withthosetakingplaceb
oNosign
ificant
differen
cebe
twee
nBZDsan
dplaceb
oon
any
slee
pmea
sure
atan
yother
time
Braun
etal
10Ran
domized
-controlled
trial
10pa
tien
tswith
PTSD
Alprazolam
(15-6
mgdfor
5wk
then
2wk
tape
r)
12wk
PTSD
Scale
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
s
IES
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
sHAM-A
Tho
setakingBZDshad
sign
ificantlyde
crea
sed
anxietycompa
redwiththosetakingplaceb
oHAM-D
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
depr
ession
VAS
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
overallwell-be
ing
Cates
etal
11Ran
domized
-controlled
trial
6pa
tien
tswith
PTSD
Clona
zepa
m(1
mgfor7
nigh
tsthen
2mgfor7nigh
ts
then
1wktape
r)
5wk
CAPS-
adap
ted
slee
pdiary
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oon
anyslee
pmea
sure
orin
nigh
tmares
Gelpinet
al12
Non
rand
omized
-controlled
trial
26recent
physical
trau
mapa
tien
tsAlprazolam
(25
mgd)
orclon
azep
am(27plusmn08mgd)
for1-6mo
6mo
CAPS
Tho
setakingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(69
vs15
)
284 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
IES
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sMIS
SNosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sSCID
Tho
setakingBZDssign
ificantlymorelike
lyto
deve
lopmajor
depr
essive
disord
erthan
those
not
takingBZDs(54
vs0
)Nosign
ificant
differen
cebe
twee
nBZDsan
dnoBZDsin
deve
lopm
entof
phob
ias
alcohol
abusep
anic
disord
eror
dysthym
iaSTAI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
anxiety
BDI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
depr
ession
Hea
rtrate
Tho
setakingBZDshad
decrea
sedhea
rtrate
inthefirstwee
kcompa
redwiththosenot
takingBZDs
butthis
differen
cewas
not
sign
ificantNosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
hea
rtrate
atan
yother
time
Sha
levet
al13
Non
rand
omized
compa
rison
trial
18pa
tien
ts(9
with
PTSD9with
panicdisord
er)
Alprazolam
(205plusmn
069
mgd)
2wk
HAM-A
Nosign
ificantdifferen
cebe
twee
nPTSD
and
panic
disord
erin
prestimulation
anxiety
Orbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
npa
tien
tswithPTSD
andpa
nic
disord
erin
physiologicalmea
suresbe
fore
BZDs
Acoustic
startleresp
onsesin
PTSD
werenot
statisticallydifferen
tbe
fore
andafterBZDs
butthey
weresign
ificantlyde
crea
sedin
patien
tswithpa
nic
disord
erafterBZDs
Zatzicket
al14
Prosp
ective
coho
rt29
31ph
ysical
trau
mapa
tien
tsAny
agen
tdo
se
anddu
ration
12mo
PCL
Tho
sereceivingBZDsbe
fore
injury
sign
ificantlymorelike
lyto
hav
ePTSD
symptom
sthan
thosenot
takingBZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 285
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Shinet
al15
Prosp
ective
coho
rt37
6pa
tien
tswith
PTSD
Any
agen
tdo
se
anddu
ration
5-12
mo
CTS
Tho
sewithahistory
ofag
gression
taking
BZDshad
sign
ificantlyincrea
sedag
gression
compa
redwiththosenot
takingBZDsan
dthosewithou
tahistory
ofag
gression
Kostenet
al16
Prosp
ective
coho
rt37
0pa
tien
tswith
PTSD
inmen
tal
health
trea
tmen
t
Any
agen
tdo
se
anddu
ration
12mo
MIS
STho
setakingBZDshad
sign
ificantlyincrea
sed
PTSD
symptom
sat
baselinecompa
redwith
thosenot
takingBZDs
BSI
Tho
setaking
BZD
sha
dsign
ificantly
increa
sed
anxietyat
baselin
ecompa
redwiththoseno
ttaking
BZD
sNosign
ificant
diffe
rencebe
tween
BZD
san
dno
BZD
sin
chan
gein
anxiety
NVVRS-
derive
dinstru
men
t
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
violen
ceat
baseline
Thosewith
comorbidSUD
takingBZDshad
less
impr
ovem
entin
violen
cecompa
redwith
thosewithcomorbidSUD
not
takingBZDs
butthis
differen
cewas
not
sign
ificant
ASI
Tho
setakingBZDshad
sign
ificantlyincrea
sed
alcohol
use
atba
selinecompa
redwiththose
not
takingBZDs
Nosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
chan
gein
subs
tance
use
orsocial
functioning
Those
withcomorbidSUD
takingBZDshad
less
impr
ovem
entin
subs
tance
use
compa
red
withthosewithcomorbidSUD
not
taking
BZDs
butthis
differen
cewas
not
sign
ificant
Rosen
etal
17Prosp
ective
coho
rt28
3pa
tien
tswith
PTSD
(140
inpr
olon
ged
expo
sure14
3in
presen
t-centered
psycho
therap
ysu
fficien
tda
tafor
meta-an
alysis
was
only
availablefor
143pa
tien
ts)
Any
agen
tdo
se
anddu
ration
6mo
CAPS
Nosign
ificance
differen
cebe
twee
nBZDswith
prolon
gedex
posu
rean
dnoBZDswitheither
therap
yin
PTSD
symptom
sThosetaking
BZDsin
presen
t-centeredps
ychotherap
yhad
sign
ificantlyworse
posttrea
tmen
tmaintenan
ceof
impr
ovem
ents
inPTSD
symptom
scompa
redwithother
grou
psPCL
Inpr
esen
t-centeredtherap
ythosetaking
BZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
sdu
ringps
ychotherap
ycompa
redwiththosenot
takingBZDs
Significance
ofresu
ltsforpr
olon
gedex
posu
rewerenot
determ
inab
ledu
eto
presen
ceof
aninteractionterm
andtheway
theresu
lts
werepr
esen
ted
286 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Jone
set
al18
Prosp
ective
coho
rt23
8recent
trau
mapa
tien
ts(ICU)
Any
agen
tdo
sean
ddu
ration
3mo
PTSS-14
Higher
BZD
dosesin
theIC
Uas
sociated
with
sign
ificantlyincrea
sedPTSD
symptom
s
Sam
uelson
etal
19Prosp
ective
coho
rt22
6recent
trau
ma
patien
ts(ICU)
Midaz
olam
(any
dose
ordu
ration
)
2mo
IES-R
Tho
sereceivingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(68
vs30
)
Bienv
enu
etal
20Prosp
ective
coho
rt18
6recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
3-24
mo
IES-R
Higher
BZD
dosesin
theIC
Unot
associated
withsign
ificantch
ange
sin
therisk
ofde
velopingPTSD
Baran
yiet
al21
Prosp
ective
coho
rt12
6trau
ma
patien
ts(solid-organ
tran
splants)
Any
agen
tdo
se
anddu
ration
Mea
nof
249
mo
PTSS-10
Chronic
BZD
useeither
before
orafter
surgery
associated
withsign
ificantly
increa
sedrisk
ofPTSD
symptom
s
Girardet
al22
Prosp
ective
coho
rt43
recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
6mo
PTSS-10
Greater
BZD
administrationin
theIC
Uas
sociated
withsign
ificantlyincrea
sedrisk
ofde
velopingPTSD
Van
Minne
net
al23
Prosp
ective
coho
rt43
patien
tswith
PTSD
inpr
olon
ged
expo
sure
Daily
useof
any
agen
tor
dose
3mo
PSS-SR
Tho
setakingBZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
san
dmore
drop
outs
compa
redwiththosenot
taking
BZDs
McG
hee
etal
24Retrosp
ective
coho
rt21
1trau
ma
patien
ts(bur
nsrequ
iringsu
rgery)
Midaz
olam
(any
dose
intrao
perative
)
Any
upto
4y
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
risk
ofde
velopingPTSD
Sha
levan
dRog
el-
Fuc
hs25
Cross-section
al18
patien
tswith
PTSD
Clona
zepa
m(27plusmn11mgd)
Not ap
plicab
leOrbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
mag
nitude
orhab
ituationrate
ofacou
stic
startleresp
onses
ASIindicates
Addiction
SeverityIn
dexB
DIBeckDep
ressionIn
ventoryB
SIBrief
Sym
ptom
Inventory
BZDb
enzodiazepineCAPSC
linician-administeredPTSD
Sca
leCTSCon
flicts
Tac
tics
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRatingSca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionIC
U
intensive
care
unitI
ESIm
pact
ofEvent
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDN
VVRSNational
Vietnam
Veteran
sRea
djustmen
tStudy
PCLP
TSD
ChecklistPSS-SRP
TSD
Sym
ptom
Sca
leSelf-repo
rtP
TSSP
osttra
umatic
StressSyn
dromeSca
leP
TSDp
osttra
umatic
stress
disorderS
CID
StructuredClinical
Interview
fortheDSMSTAI
State-Tra
itAnxietyIn
ventoryS
UDsu
bstance
use
disorderVASvisu
alan
alog
scale
Journal of Psychiatric Practice Vol 21 No 4 July 2015 287
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
umaTyp
e(
)
Rothb
aum
etal
8IIraq
andor
Afgha
nistan
veterans
DSM-IVcriteria
forPTSD
dueto
militarytrau
mave
rified
throug
hdischa
rgepa
pers
discon
tinu
edtaking
long
-actingBZD
sfor1moan
dsh
ort-
acting
BZD
sfor2wkbe
fore
screen
ing
stab
ledo
sesof
othe
rps
ycho
trop
icmed
ications
forat
leas
t2wkbe
fore
thestud
ywritten
inform
edconsent
EMed
ically
unstab
leps
ycho
sis
bipo
lardisord
erc
urrent
suicidal
risk
cu
rren
talcoho
lor
drug
depe
nden
ce
preg
nanc
ygluc
ocorticoids
BZD
sch
ronicallyus
edop
ioids
354
Black
50
White
42
Hispa
nic5
Other3
Com
bat10
0
Mellm
anet
al9
IAdm
ittedto
leve
lItrau
macenterr
ecallof
trau
ma
atleas
tmod
erateim
pairmen
tof
slee
pinitiation
ormainten
ance
mee
tfullcriteria
forat
leas
t2PTSD
symptom
clus
ters
inDSM-IVwilling
andab
leto
prov
idewritten
inform
edcons
ent
EIn
toxication
attimeof
trau
ma
braininjurypr
eexisting
psychiatricdisord
ers
3636
Hispa
nic8
2White
9Black
9
MVC68
Assau
lt2
3Acciden
t9
Braun
etal
10I
DSM-III
criteria
forPTSDwilling
andab
leto
prov
ide
written
inform
edconsentfreeof
psycho
trop
icmed
ications
atleas
t2wkbe
fore
stud
yEPhy
sicallyun
healthy
sign
ificant
head
injury
38Com
bat40
MVC30
Acciden
t20
Terrorism
10
Cates
etal
11I
DSM-IV
criteria
forPTSDat
leas
tthrice
wee
klypr
oblems
withslee
pan
dnigh
tmaresw
illing
andab
leto
prov
ide
written
inform
edconsent
Elt
18yold
unstab
lemed
ical
cond
itions
sen
sitivity
toBZD
scu
rren
tBZD
use
subs
tanc
eab
useor
depe
nden
cein
past
4wk
inab
ilityto
attend
regu
larfollow
-upvisitswom
enwho
wereeither
preg
nant
orof
child-be
aringpo
tentialan
dno
tus
ingcontraceptivesde
men
tia
cogn
itivedisord
er
520
Com
bat10
0
Gelpinet
al12
IEmerge
ncyroom
admission
swithatrau
ma
ETak
ingps
ycho
trop
icmed
ications
before
thetrau
ma
coma
head
injuryloss
ofcons
ciou
sness
2946
MVCs
77
Terrorism
19
Acciden
t4
Sha
levet
al13
IDSM-III-R
criteria
forPTSD
orpa
nicdisord
ermed
ication
free
EPsych
osism
ajor
depr
ession
cur
rent
orpa
stsu
bstanc
eor
alcoho
lus
epa
tien
tswithPTSD
withsp
ontane
ouspa
nic
attack
spa
tien
tswithpa
nicdisord
erwithahistoryof
trau
ma
3439
288 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
Zatzicket
al14
I18
-84yold
Eng
lish
-spe
akingor
Spa
nish
-spe
akingpa
tien
ts
arrive
daliveat
hosp
italm
oderateto
seve
reinjuries
Eg
reater
than
oreq
ual
toge65
yoldwithafirstlisted
diag
nosisof
hipfracturem
ajor
burn
strea
tmen
tde
lays
gt24
hincarcerated
attimeof
injury
4135
White
67
Black
16
Hispa
nic13
Other3
Injury10
0
Shinet
al15
I18
-69yold
militaryve
terans
servingin
Vietnam
eraor
laterat
leas
ton
eou
tpatient
VAvisitwithaPTSD
diag
nosis
EN
oPTSD
diag
nosisin
thepr
ior2y
4250
White
65
Black
17
Hispa
nic10
Other3
Kostenet
al16
IDSM-III
criteria
forPTSDmilitaryve
terans
450
White
75
Rosen
etal
17I
femaleve
teranor
active
duty
soldier
DSM-IV
criteria
for
PTSDCAPSscoregt45
EC
oncu
rren
tPTSD
psycho
therap
yothe
rthan
briefvisits
withan
existing
therap
istor
participationin
self-help
grou
psc
hang
ein
psycho
active
med
ications
during
the2mo
before
stud
yrecruitm
entsu
bstanc
ede
pend
ence
notin
remission
forat
leas
t3mo
curren
tps
ycho
ticsymptom
sor
man
iab
ipolar
disord
erpr
ominen
tcu
rren
tsu
icidal
orho
micidal
idea
tion
cogn
itiveim
pairmen
tcu
rren
tinvo
lvem
entin
violen
trelation
shipself-m
utilationwithin
thepa
st6mo
100
White
55
Black
33
Hispa
nic
6Other7
Sex
ual93
Acciden
t82
Disas
ter
72
Com
bat25
Jone
set
al18
Igt18
yold
mecha
nicallyve
ntilated
IC
Uleng
thof
stay
atleas
t48
hEP
rior
PTSDa
dmittedaftersu
icideattemptp
reex
isting
orconc
omitan
tps
ycho
ticillness
reside
sgt30
kmfrom
hosp
ital
unresolved
confus
ionen
rolled
inan
othe
rresearch
stud
y
6138
Life-threaten
ingmed
ical
condition
10
0
Sam
uelson
etal
19I
gt18
yold
mecha
nicallyve
ntilated
ge
neralIC
Uleng
thof
stay
atleas
t24
hEH
eadinjuryps
ycho
ticillness
men
talretard
ation
intoxication
adm
ittedaftersu
icideattempth
earing
spe
ech
disa
bilityno
n-Swed
ishsp
eaking
tran
sferredto
anothe
rho
spitalm
echa
nicallyve
ntilated
atdischa
rge
mecha
nically
ventilated
gt24
hpr
eadm
ission
6348
Life-threaten
ingmed
ical
condition
10
0
Bienv
enuet
al20
IMecha
nicallyve
ntilated
withacutelung
injury
EN
eurologicalsp
ecialtyIC
Upr
eexistingillnesswithalife
expe
ctan
cylt6mo
pree
xistingcogn
itiveim
pairmen
tor
commun
icationlang
uage
barriersn
ofixe
dad
dress
tran
sfer
toastud
ysite
ICU
withpr
eexistingacutelung
injury
gt24
h
45
Life-threaten
ingmed
ical
condition
10
0
Journal of Psychiatric Practice Vol 21 No 4 July 2015 289
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
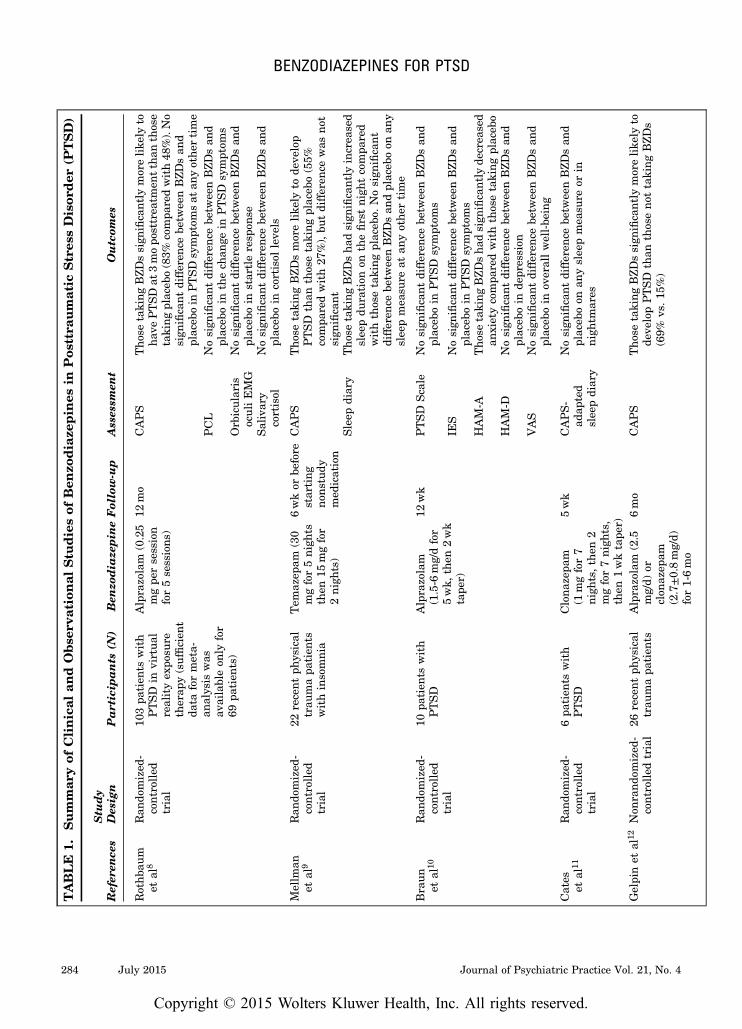
TABLE
1Summar
yof
Clinical
andObse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Rothb
aum
etal
8Ran
domized
-controlled
trial
103pa
tien
tswith
PTSD
invirtua
lrealityex
posu
retherap
y(sufficien
tda
taformeta-
analysis
was
availableon
lyfor
69pa
tien
ts)
Alprazolam
(025
mgpe
rsession
for5sessions
)
12mo
CAPS
Tho
setakingBZDssign
ificantlymorelike
lyto
have
PTSD
at3mopo
sttrea
tmen
tthan
those
takingplaceb
o(83
compa
redwith48
)No
sign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
sat
anyother
time
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
thech
ange
inPTSD
symptom
sOrbicularis
oculiEMG
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
startleresp
onse
Salivary
cortisol
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
cortisol
leve
ls
Mellm
anet
al9
Ran
domized
-controlled
trial
22recent
physical
trau
mapa
tien
tswithinsomnia
Tem
azep
am(30
mgfor5nigh
tsthen
15mgfor
2nigh
ts)
6wkor
before
starting
nons
tudy
med
ication
CAPS
Tho
setakingBZDsmorelike
lyto
deve
lop
PTSD
than
thosetakingplaceb
o(55
compa
redwith27
)bu
tdifferen
cewas
not
sign
ificant
Sleep
diary
Tho
setakingBZDshad
sign
ificantlyincrea
sed
slee
pdu
ration
onthefirstnightcompa
red
withthosetakingplaceb
oNosign
ificant
differen
cebe
twee
nBZDsan
dplaceb
oon
any
slee
pmea
sure
atan
yother
time
Braun
etal
10Ran
domized
-controlled
trial
10pa
tien
tswith
PTSD
Alprazolam
(15-6
mgdfor
5wk
then
2wk
tape
r)
12wk
PTSD
Scale
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
s
IES
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
PTSD
symptom
sHAM-A
Tho
setakingBZDshad
sign
ificantlyde
crea
sed
anxietycompa
redwiththosetakingplaceb
oHAM-D
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
depr
ession
VAS
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oin
overallwell-be
ing
Cates
etal
11Ran
domized
-controlled
trial
6pa
tien
tswith
PTSD
Clona
zepa
m(1
mgfor7
nigh
tsthen
2mgfor7nigh
ts
then
1wktape
r)
5wk
CAPS-
adap
ted
slee
pdiary
Nosign
ificantdifferen
cebe
twee
nBZDsan
dplaceb
oon
anyslee
pmea
sure
orin
nigh
tmares
Gelpinet
al12
Non
rand
omized
-controlled
trial
26recent
physical
trau
mapa
tien
tsAlprazolam
(25
mgd)
orclon
azep
am(27plusmn08mgd)
for1-6mo
6mo
CAPS
Tho
setakingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(69
vs15
)
284 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
IES
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sMIS
SNosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sSCID
Tho
setakingBZDssign
ificantlymorelike
lyto
deve
lopmajor
depr
essive
disord
erthan
those
not
takingBZDs(54
vs0
)Nosign
ificant
differen
cebe
twee
nBZDsan
dnoBZDsin
deve
lopm
entof
phob
ias
alcohol
abusep
anic
disord
eror
dysthym
iaSTAI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
anxiety
BDI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
depr
ession
Hea
rtrate
Tho
setakingBZDshad
decrea
sedhea
rtrate
inthefirstwee
kcompa
redwiththosenot
takingBZDs
butthis
differen
cewas
not
sign
ificantNosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
hea
rtrate
atan
yother
time
Sha
levet
al13
Non
rand
omized
compa
rison
trial
18pa
tien
ts(9
with
PTSD9with
panicdisord
er)
Alprazolam
(205plusmn
069
mgd)
2wk
HAM-A
Nosign
ificantdifferen
cebe
twee
nPTSD
and
panic
disord
erin
prestimulation
anxiety
Orbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
npa
tien
tswithPTSD
andpa
nic
disord
erin
physiologicalmea
suresbe
fore
BZDs
Acoustic
startleresp
onsesin
PTSD
werenot
statisticallydifferen
tbe
fore
andafterBZDs
butthey
weresign
ificantlyde
crea
sedin
patien
tswithpa
nic
disord
erafterBZDs
Zatzicket
al14
Prosp
ective
coho
rt29
31ph
ysical
trau
mapa
tien
tsAny
agen
tdo
se
anddu
ration
12mo
PCL
Tho
sereceivingBZDsbe
fore
injury
sign
ificantlymorelike
lyto
hav
ePTSD
symptom
sthan
thosenot
takingBZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 285
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Shinet
al15
Prosp
ective
coho
rt37
6pa
tien
tswith
PTSD
Any
agen
tdo
se
anddu
ration
5-12
mo
CTS
Tho
sewithahistory
ofag
gression
taking
BZDshad
sign
ificantlyincrea
sedag
gression
compa
redwiththosenot
takingBZDsan
dthosewithou
tahistory
ofag
gression
Kostenet
al16
Prosp
ective
coho
rt37
0pa
tien
tswith
PTSD
inmen
tal
health
trea
tmen
t
Any
agen
tdo
se
anddu
ration
12mo
MIS
STho
setakingBZDshad
sign
ificantlyincrea
sed
PTSD
symptom
sat
baselinecompa
redwith
thosenot
takingBZDs
BSI
Tho
setaking
BZD
sha
dsign
ificantly
increa
sed
anxietyat
baselin
ecompa
redwiththoseno
ttaking
BZD
sNosign
ificant
diffe
rencebe
tween
BZD
san
dno
BZD
sin
chan
gein
anxiety
NVVRS-
derive
dinstru
men
t
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
violen
ceat
baseline
Thosewith
comorbidSUD
takingBZDshad
less
impr
ovem
entin
violen
cecompa
redwith
thosewithcomorbidSUD
not
takingBZDs
butthis
differen
cewas
not
sign
ificant
ASI
Tho
setakingBZDshad
sign
ificantlyincrea
sed
alcohol
use
atba
selinecompa
redwiththose
not
takingBZDs
Nosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
chan
gein
subs
tance
use
orsocial
functioning
Those
withcomorbidSUD
takingBZDshad
less
impr
ovem
entin
subs
tance
use
compa
red
withthosewithcomorbidSUD
not
taking
BZDs
butthis
differen
cewas
not
sign
ificant
Rosen
etal
17Prosp
ective
coho
rt28
3pa
tien
tswith
PTSD
(140
inpr
olon
ged
expo
sure14
3in
presen
t-centered
psycho
therap
ysu
fficien
tda
tafor
meta-an
alysis
was
only
availablefor
143pa
tien
ts)
Any
agen
tdo
se
anddu
ration
6mo
CAPS
Nosign
ificance
differen
cebe
twee
nBZDswith
prolon
gedex
posu
rean
dnoBZDswitheither
therap
yin
PTSD
symptom
sThosetaking
BZDsin
presen
t-centeredps
ychotherap
yhad
sign
ificantlyworse
posttrea
tmen
tmaintenan
ceof
impr
ovem
ents
inPTSD
symptom
scompa
redwithother
grou
psPCL
Inpr
esen
t-centeredtherap
ythosetaking
BZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
sdu
ringps
ychotherap
ycompa
redwiththosenot
takingBZDs
Significance
ofresu
ltsforpr
olon
gedex
posu
rewerenot
determ
inab
ledu
eto
presen
ceof
aninteractionterm
andtheway
theresu
lts
werepr
esen
ted
286 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Jone
set
al18
Prosp
ective
coho
rt23
8recent
trau
mapa
tien
ts(ICU)
Any
agen
tdo
sean
ddu
ration
3mo
PTSS-14
Higher
BZD
dosesin
theIC
Uas
sociated
with
sign
ificantlyincrea
sedPTSD
symptom
s
Sam
uelson
etal
19Prosp
ective
coho
rt22
6recent
trau
ma
patien
ts(ICU)
Midaz
olam
(any
dose
ordu
ration
)
2mo
IES-R
Tho
sereceivingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(68
vs30
)
Bienv
enu
etal
20Prosp
ective
coho
rt18
6recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
3-24
mo
IES-R
Higher
BZD
dosesin
theIC
Unot
associated
withsign
ificantch
ange
sin
therisk
ofde
velopingPTSD
Baran
yiet
al21
Prosp
ective
coho
rt12
6trau
ma
patien
ts(solid-organ
tran
splants)
Any
agen
tdo
se
anddu
ration
Mea
nof
249
mo
PTSS-10
Chronic
BZD
useeither
before
orafter
surgery
associated
withsign
ificantly
increa
sedrisk
ofPTSD
symptom
s
Girardet
al22
Prosp
ective
coho
rt43
recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
6mo
PTSS-10
Greater
BZD
administrationin
theIC
Uas
sociated
withsign
ificantlyincrea
sedrisk
ofde
velopingPTSD
Van
Minne
net
al23
Prosp
ective
coho
rt43
patien
tswith
PTSD
inpr
olon
ged
expo
sure
Daily
useof
any
agen
tor
dose
3mo
PSS-SR
Tho
setakingBZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
san
dmore
drop
outs
compa
redwiththosenot
taking
BZDs
McG
hee
etal
24Retrosp
ective
coho
rt21
1trau
ma
patien
ts(bur
nsrequ
iringsu
rgery)
Midaz
olam
(any
dose
intrao
perative
)
Any
upto
4y
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
risk
ofde
velopingPTSD
Sha
levan
dRog
el-
Fuc
hs25
Cross-section
al18
patien
tswith
PTSD
Clona
zepa
m(27plusmn11mgd)
Not ap
plicab
leOrbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
mag
nitude
orhab
ituationrate
ofacou
stic
startleresp
onses
ASIindicates
Addiction
SeverityIn
dexB
DIBeckDep
ressionIn
ventoryB
SIBrief
Sym
ptom
Inventory
BZDb
enzodiazepineCAPSC
linician-administeredPTSD
Sca
leCTSCon
flicts
Tac
tics
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRatingSca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionIC
U
intensive
care
unitI
ESIm
pact
ofEvent
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDN
VVRSNational
Vietnam
Veteran
sRea
djustmen
tStudy
PCLP
TSD
ChecklistPSS-SRP
TSD
Sym
ptom
Sca
leSelf-repo
rtP
TSSP
osttra
umatic
StressSyn
dromeSca
leP
TSDp
osttra
umatic
stress
disorderS
CID
StructuredClinical
Interview
fortheDSMSTAI
State-Tra
itAnxietyIn
ventoryS
UDsu
bstance
use
disorderVASvisu
alan
alog
scale
Journal of Psychiatric Practice Vol 21 No 4 July 2015 287
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
umaTyp
e(
)
Rothb
aum
etal
8IIraq
andor
Afgha
nistan
veterans
DSM-IVcriteria
forPTSD
dueto
militarytrau
mave
rified
throug
hdischa
rgepa
pers
discon
tinu
edtaking
long
-actingBZD
sfor1moan
dsh
ort-
acting
BZD
sfor2wkbe
fore
screen
ing
stab
ledo
sesof
othe
rps
ycho
trop
icmed
ications
forat
leas
t2wkbe
fore
thestud
ywritten
inform
edconsent
EMed
ically
unstab
leps
ycho
sis
bipo
lardisord
erc
urrent
suicidal
risk
cu
rren
talcoho
lor
drug
depe
nden
ce
preg
nanc
ygluc
ocorticoids
BZD
sch
ronicallyus
edop
ioids
354
Black
50
White
42
Hispa
nic5
Other3
Com
bat10
0
Mellm
anet
al9
IAdm
ittedto
leve
lItrau
macenterr
ecallof
trau
ma
atleas
tmod
erateim
pairmen
tof
slee
pinitiation
ormainten
ance
mee
tfullcriteria
forat
leas
t2PTSD
symptom
clus
ters
inDSM-IVwilling
andab
leto
prov
idewritten
inform
edcons
ent
EIn
toxication
attimeof
trau
ma
braininjurypr
eexisting
psychiatricdisord
ers
3636
Hispa
nic8
2White
9Black
9
MVC68
Assau
lt2
3Acciden
t9
Braun
etal
10I
DSM-III
criteria
forPTSDwilling
andab
leto
prov
ide
written
inform
edconsentfreeof
psycho
trop
icmed
ications
atleas
t2wkbe
fore
stud
yEPhy
sicallyun
healthy
sign
ificant
head
injury
38Com
bat40
MVC30
Acciden
t20
Terrorism
10
Cates
etal
11I
DSM-IV
criteria
forPTSDat
leas
tthrice
wee
klypr
oblems
withslee
pan
dnigh
tmaresw
illing
andab
leto
prov
ide
written
inform
edconsent
Elt
18yold
unstab
lemed
ical
cond
itions
sen
sitivity
toBZD
scu
rren
tBZD
use
subs
tanc
eab
useor
depe
nden
cein
past
4wk
inab
ilityto
attend
regu
larfollow
-upvisitswom
enwho
wereeither
preg
nant
orof
child-be
aringpo
tentialan
dno
tus
ingcontraceptivesde
men
tia
cogn
itivedisord
er
520
Com
bat10
0
Gelpinet
al12
IEmerge
ncyroom
admission
swithatrau
ma
ETak
ingps
ycho
trop
icmed
ications
before
thetrau
ma
coma
head
injuryloss
ofcons
ciou
sness
2946
MVCs
77
Terrorism
19
Acciden
t4
Sha
levet
al13
IDSM-III-R
criteria
forPTSD
orpa
nicdisord
ermed
ication
free
EPsych
osism
ajor
depr
ession
cur
rent
orpa
stsu
bstanc
eor
alcoho
lus
epa
tien
tswithPTSD
withsp
ontane
ouspa
nic
attack
spa
tien
tswithpa
nicdisord
erwithahistoryof
trau
ma
3439
288 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
Zatzicket
al14
I18
-84yold
Eng
lish
-spe
akingor
Spa
nish
-spe
akingpa
tien
ts
arrive
daliveat
hosp
italm
oderateto
seve
reinjuries
Eg
reater
than
oreq
ual
toge65
yoldwithafirstlisted
diag
nosisof
hipfracturem
ajor
burn
strea
tmen
tde
lays
gt24
hincarcerated
attimeof
injury
4135
White
67
Black
16
Hispa
nic13
Other3
Injury10
0
Shinet
al15
I18
-69yold
militaryve
terans
servingin
Vietnam
eraor
laterat
leas
ton
eou
tpatient
VAvisitwithaPTSD
diag
nosis
EN
oPTSD
diag
nosisin
thepr
ior2y
4250
White
65
Black
17
Hispa
nic10
Other3
Kostenet
al16
IDSM-III
criteria
forPTSDmilitaryve
terans
450
White
75
Rosen
etal
17I
femaleve
teranor
active
duty
soldier
DSM-IV
criteria
for
PTSDCAPSscoregt45
EC
oncu
rren
tPTSD
psycho
therap
yothe
rthan
briefvisits
withan
existing
therap
istor
participationin
self-help
grou
psc
hang
ein
psycho
active
med
ications
during
the2mo
before
stud
yrecruitm
entsu
bstanc
ede
pend
ence
notin
remission
forat
leas
t3mo
curren
tps
ycho
ticsymptom
sor
man
iab
ipolar
disord
erpr
ominen
tcu
rren
tsu
icidal
orho
micidal
idea
tion
cogn
itiveim
pairmen
tcu
rren
tinvo
lvem
entin
violen
trelation
shipself-m
utilationwithin
thepa
st6mo
100
White
55
Black
33
Hispa
nic
6Other7
Sex
ual93
Acciden
t82
Disas
ter
72
Com
bat25
Jone
set
al18
Igt18
yold
mecha
nicallyve
ntilated
IC
Uleng
thof
stay
atleas
t48
hEP
rior
PTSDa
dmittedaftersu
icideattemptp
reex
isting
orconc
omitan
tps
ycho
ticillness
reside
sgt30
kmfrom
hosp
ital
unresolved
confus
ionen
rolled
inan
othe
rresearch
stud
y
6138
Life-threaten
ingmed
ical
condition
10
0
Sam
uelson
etal
19I
gt18
yold
mecha
nicallyve
ntilated
ge
neralIC
Uleng
thof
stay
atleas
t24
hEH
eadinjuryps
ycho
ticillness
men
talretard
ation
intoxication
adm
ittedaftersu
icideattempth
earing
spe
ech
disa
bilityno
n-Swed
ishsp
eaking
tran
sferredto
anothe
rho
spitalm
echa
nicallyve
ntilated
atdischa
rge
mecha
nically
ventilated
gt24
hpr
eadm
ission
6348
Life-threaten
ingmed
ical
condition
10
0
Bienv
enuet
al20
IMecha
nicallyve
ntilated
withacutelung
injury
EN
eurologicalsp
ecialtyIC
Upr
eexistingillnesswithalife
expe
ctan
cylt6mo
pree
xistingcogn
itiveim
pairmen
tor
commun
icationlang
uage
barriersn
ofixe
dad
dress
tran
sfer
toastud
ysite
ICU
withpr
eexistingacutelung
injury
gt24
h
45
Life-threaten
ingmed
ical
condition
10
0
Journal of Psychiatric Practice Vol 21 No 4 July 2015 289
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
IES
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sMIS
SNosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
PTSD
symptom
sSCID
Tho
setakingBZDssign
ificantlymorelike
lyto
deve
lopmajor
depr
essive
disord
erthan
those
not
takingBZDs(54
vs0
)Nosign
ificant
differen
cebe
twee
nBZDsan
dnoBZDsin
deve
lopm
entof
phob
ias
alcohol
abusep
anic
disord
eror
dysthym
iaSTAI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
anxiety
BDI
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
depr
ession
Hea
rtrate
Tho
setakingBZDshad
decrea
sedhea
rtrate
inthefirstwee
kcompa
redwiththosenot
takingBZDs
butthis
differen
cewas
not
sign
ificantNosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
hea
rtrate
atan
yother
time
Sha
levet
al13
Non
rand
omized
compa
rison
trial
18pa
tien
ts(9
with
PTSD9with
panicdisord
er)
Alprazolam
(205plusmn
069
mgd)
2wk
HAM-A
Nosign
ificantdifferen
cebe
twee
nPTSD
and
panic
disord
erin
prestimulation
anxiety
Orbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
npa
tien
tswithPTSD
andpa
nic
disord
erin
physiologicalmea
suresbe
fore
BZDs
Acoustic
startleresp
onsesin
PTSD
werenot
statisticallydifferen
tbe
fore
andafterBZDs
butthey
weresign
ificantlyde
crea
sedin
patien
tswithpa
nic
disord
erafterBZDs
Zatzicket
al14
Prosp
ective
coho
rt29
31ph
ysical
trau
mapa
tien
tsAny
agen
tdo
se
anddu
ration
12mo
PCL
Tho
sereceivingBZDsbe
fore
injury
sign
ificantlymorelike
lyto
hav
ePTSD
symptom
sthan
thosenot
takingBZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 285
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Shinet
al15
Prosp
ective
coho
rt37
6pa
tien
tswith
PTSD
Any
agen
tdo
se
anddu
ration
5-12
mo
CTS
Tho
sewithahistory
ofag
gression
taking
BZDshad
sign
ificantlyincrea
sedag
gression
compa
redwiththosenot
takingBZDsan
dthosewithou
tahistory
ofag
gression
Kostenet
al16
Prosp
ective
coho
rt37
0pa
tien
tswith
PTSD
inmen
tal
health
trea
tmen
t
Any
agen
tdo
se
anddu
ration
12mo
MIS
STho
setakingBZDshad
sign
ificantlyincrea
sed
PTSD
symptom
sat
baselinecompa
redwith
thosenot
takingBZDs
BSI
Tho
setaking
BZD
sha
dsign
ificantly
increa
sed
anxietyat
baselin
ecompa
redwiththoseno
ttaking
BZD
sNosign
ificant
diffe
rencebe
tween
BZD
san
dno
BZD
sin
chan
gein
anxiety
NVVRS-
derive
dinstru
men
t
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
violen
ceat
baseline
Thosewith
comorbidSUD
takingBZDshad
less
impr
ovem
entin
violen
cecompa
redwith
thosewithcomorbidSUD
not
takingBZDs
butthis
differen
cewas
not
sign
ificant
ASI
Tho
setakingBZDshad
sign
ificantlyincrea
sed
alcohol
use
atba
selinecompa
redwiththose
not
takingBZDs
Nosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
chan
gein
subs
tance
use
orsocial
functioning
Those
withcomorbidSUD
takingBZDshad
less
impr
ovem
entin
subs
tance
use
compa
red
withthosewithcomorbidSUD
not
taking
BZDs
butthis
differen
cewas
not
sign
ificant
Rosen
etal
17Prosp
ective
coho
rt28
3pa
tien
tswith
PTSD
(140
inpr
olon
ged
expo
sure14
3in
presen
t-centered
psycho
therap
ysu
fficien
tda
tafor
meta-an
alysis
was
only
availablefor
143pa
tien
ts)
Any
agen
tdo
se
anddu
ration
6mo
CAPS
Nosign
ificance
differen
cebe
twee
nBZDswith
prolon
gedex
posu
rean
dnoBZDswitheither
therap
yin
PTSD
symptom
sThosetaking
BZDsin
presen
t-centeredps
ychotherap
yhad
sign
ificantlyworse
posttrea
tmen
tmaintenan
ceof
impr
ovem
ents
inPTSD
symptom
scompa
redwithother
grou
psPCL
Inpr
esen
t-centeredtherap
ythosetaking
BZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
sdu
ringps
ychotherap
ycompa
redwiththosenot
takingBZDs
Significance
ofresu
ltsforpr
olon
gedex
posu
rewerenot
determ
inab
ledu
eto
presen
ceof
aninteractionterm
andtheway
theresu
lts
werepr
esen
ted
286 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Jone
set
al18
Prosp
ective
coho
rt23
8recent
trau
mapa
tien
ts(ICU)
Any
agen
tdo
sean
ddu
ration
3mo
PTSS-14
Higher
BZD
dosesin
theIC
Uas
sociated
with
sign
ificantlyincrea
sedPTSD
symptom
s
Sam
uelson
etal
19Prosp
ective
coho
rt22
6recent
trau
ma
patien
ts(ICU)
Midaz
olam
(any
dose
ordu
ration
)
2mo
IES-R
Tho
sereceivingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(68
vs30
)
Bienv
enu
etal
20Prosp
ective
coho
rt18
6recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
3-24
mo
IES-R
Higher
BZD
dosesin
theIC
Unot
associated
withsign
ificantch
ange
sin
therisk
ofde
velopingPTSD
Baran
yiet
al21
Prosp
ective
coho
rt12
6trau
ma
patien
ts(solid-organ
tran
splants)
Any
agen
tdo
se
anddu
ration
Mea
nof
249
mo
PTSS-10
Chronic
BZD
useeither
before
orafter
surgery
associated
withsign
ificantly
increa
sedrisk
ofPTSD
symptom
s
Girardet
al22
Prosp
ective
coho
rt43
recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
6mo
PTSS-10
Greater
BZD
administrationin
theIC
Uas
sociated
withsign
ificantlyincrea
sedrisk
ofde
velopingPTSD
Van
Minne
net
al23
Prosp
ective
coho
rt43
patien
tswith
PTSD
inpr
olon
ged
expo
sure
Daily
useof
any
agen
tor
dose
3mo
PSS-SR
Tho
setakingBZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
san
dmore
drop
outs
compa
redwiththosenot
taking
BZDs
McG
hee
etal
24Retrosp
ective
coho
rt21
1trau
ma
patien
ts(bur
nsrequ
iringsu
rgery)
Midaz
olam
(any
dose
intrao
perative
)
Any
upto
4y
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
risk
ofde
velopingPTSD
Sha
levan
dRog
el-
Fuc
hs25
Cross-section
al18
patien
tswith
PTSD
Clona
zepa
m(27plusmn11mgd)
Not ap
plicab
leOrbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
mag
nitude
orhab
ituationrate
ofacou
stic
startleresp
onses
ASIindicates
Addiction
SeverityIn
dexB
DIBeckDep
ressionIn
ventoryB
SIBrief
Sym
ptom
Inventory
BZDb
enzodiazepineCAPSC
linician-administeredPTSD
Sca
leCTSCon
flicts
Tac
tics
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRatingSca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionIC
U
intensive
care
unitI
ESIm
pact
ofEvent
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDN
VVRSNational
Vietnam
Veteran
sRea
djustmen
tStudy
PCLP
TSD
ChecklistPSS-SRP
TSD
Sym
ptom
Sca
leSelf-repo
rtP
TSSP
osttra
umatic
StressSyn
dromeSca
leP
TSDp
osttra
umatic
stress
disorderS
CID
StructuredClinical
Interview
fortheDSMSTAI
State-Tra
itAnxietyIn
ventoryS
UDsu
bstance
use
disorderVASvisu
alan
alog
scale
Journal of Psychiatric Practice Vol 21 No 4 July 2015 287
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
umaTyp
e(
)
Rothb
aum
etal
8IIraq
andor
Afgha
nistan
veterans
DSM-IVcriteria
forPTSD
dueto
militarytrau
mave
rified
throug
hdischa
rgepa
pers
discon
tinu
edtaking
long
-actingBZD
sfor1moan
dsh
ort-
acting
BZD
sfor2wkbe
fore
screen
ing
stab
ledo
sesof
othe
rps
ycho
trop
icmed
ications
forat
leas
t2wkbe
fore
thestud
ywritten
inform
edconsent
EMed
ically
unstab
leps
ycho
sis
bipo
lardisord
erc
urrent
suicidal
risk
cu
rren
talcoho
lor
drug
depe
nden
ce
preg
nanc
ygluc
ocorticoids
BZD
sch
ronicallyus
edop
ioids
354
Black
50
White
42
Hispa
nic5
Other3
Com
bat10
0
Mellm
anet
al9
IAdm
ittedto
leve
lItrau
macenterr
ecallof
trau
ma
atleas
tmod
erateim
pairmen
tof
slee
pinitiation
ormainten
ance
mee
tfullcriteria
forat
leas
t2PTSD
symptom
clus
ters
inDSM-IVwilling
andab
leto
prov
idewritten
inform
edcons
ent
EIn
toxication
attimeof
trau
ma
braininjurypr
eexisting
psychiatricdisord
ers
3636
Hispa
nic8
2White
9Black
9
MVC68
Assau
lt2
3Acciden
t9
Braun
etal
10I
DSM-III
criteria
forPTSDwilling
andab
leto
prov
ide
written
inform
edconsentfreeof
psycho
trop
icmed
ications
atleas
t2wkbe
fore
stud
yEPhy
sicallyun
healthy
sign
ificant
head
injury
38Com
bat40
MVC30
Acciden
t20
Terrorism
10
Cates
etal
11I
DSM-IV
criteria
forPTSDat
leas
tthrice
wee
klypr
oblems
withslee
pan
dnigh
tmaresw
illing
andab
leto
prov
ide
written
inform
edconsent
Elt
18yold
unstab
lemed
ical
cond
itions
sen
sitivity
toBZD
scu
rren
tBZD
use
subs
tanc
eab
useor
depe
nden
cein
past
4wk
inab
ilityto
attend
regu
larfollow
-upvisitswom
enwho
wereeither
preg
nant
orof
child-be
aringpo
tentialan
dno
tus
ingcontraceptivesde
men
tia
cogn
itivedisord
er
520
Com
bat10
0
Gelpinet
al12
IEmerge
ncyroom
admission
swithatrau
ma
ETak
ingps
ycho
trop
icmed
ications
before
thetrau
ma
coma
head
injuryloss
ofcons
ciou
sness
2946
MVCs
77
Terrorism
19
Acciden
t4
Sha
levet
al13
IDSM-III-R
criteria
forPTSD
orpa
nicdisord
ermed
ication
free
EPsych
osism
ajor
depr
ession
cur
rent
orpa
stsu
bstanc
eor
alcoho
lus
epa
tien
tswithPTSD
withsp
ontane
ouspa
nic
attack
spa
tien
tswithpa
nicdisord
erwithahistoryof
trau
ma
3439
288 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
Zatzicket
al14
I18
-84yold
Eng
lish
-spe
akingor
Spa
nish
-spe
akingpa
tien
ts
arrive
daliveat
hosp
italm
oderateto
seve
reinjuries
Eg
reater
than
oreq
ual
toge65
yoldwithafirstlisted
diag
nosisof
hipfracturem
ajor
burn
strea
tmen
tde
lays
gt24
hincarcerated
attimeof
injury
4135
White
67
Black
16
Hispa
nic13
Other3
Injury10
0
Shinet
al15
I18
-69yold
militaryve
terans
servingin
Vietnam
eraor
laterat
leas
ton
eou
tpatient
VAvisitwithaPTSD
diag
nosis
EN
oPTSD
diag
nosisin
thepr
ior2y
4250
White
65
Black
17
Hispa
nic10
Other3
Kostenet
al16
IDSM-III
criteria
forPTSDmilitaryve
terans
450
White
75
Rosen
etal
17I
femaleve
teranor
active
duty
soldier
DSM-IV
criteria
for
PTSDCAPSscoregt45
EC
oncu
rren
tPTSD
psycho
therap
yothe
rthan
briefvisits
withan
existing
therap
istor
participationin
self-help
grou
psc
hang
ein
psycho
active
med
ications
during
the2mo
before
stud
yrecruitm
entsu
bstanc
ede
pend
ence
notin
remission
forat
leas
t3mo
curren
tps
ycho
ticsymptom
sor
man
iab
ipolar
disord
erpr
ominen
tcu
rren
tsu
icidal
orho
micidal
idea
tion
cogn
itiveim
pairmen
tcu
rren
tinvo
lvem
entin
violen
trelation
shipself-m
utilationwithin
thepa
st6mo
100
White
55
Black
33
Hispa
nic
6Other7
Sex
ual93
Acciden
t82
Disas
ter
72
Com
bat25
Jone
set
al18
Igt18
yold
mecha
nicallyve
ntilated
IC
Uleng
thof
stay
atleas
t48
hEP
rior
PTSDa
dmittedaftersu
icideattemptp
reex
isting
orconc
omitan
tps
ycho
ticillness
reside
sgt30
kmfrom
hosp
ital
unresolved
confus
ionen
rolled
inan
othe
rresearch
stud
y
6138
Life-threaten
ingmed
ical
condition
10
0
Sam
uelson
etal
19I
gt18
yold
mecha
nicallyve
ntilated
ge
neralIC
Uleng
thof
stay
atleas
t24
hEH
eadinjuryps
ycho
ticillness
men
talretard
ation
intoxication
adm
ittedaftersu
icideattempth
earing
spe
ech
disa
bilityno
n-Swed
ishsp
eaking
tran
sferredto
anothe
rho
spitalm
echa
nicallyve
ntilated
atdischa
rge
mecha
nically
ventilated
gt24
hpr
eadm
ission
6348
Life-threaten
ingmed
ical
condition
10
0
Bienv
enuet
al20
IMecha
nicallyve
ntilated
withacutelung
injury
EN
eurologicalsp
ecialtyIC
Upr
eexistingillnesswithalife
expe
ctan
cylt6mo
pree
xistingcogn
itiveim
pairmen
tor
commun
icationlang
uage
barriersn
ofixe
dad
dress
tran
sfer
toastud
ysite
ICU
withpr
eexistingacutelung
injury
gt24
h
45
Life-threaten
ingmed
ical
condition
10
0
Journal of Psychiatric Practice Vol 21 No 4 July 2015 289
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Shinet
al15
Prosp
ective
coho
rt37
6pa
tien
tswith
PTSD
Any
agen
tdo
se
anddu
ration
5-12
mo
CTS
Tho
sewithahistory
ofag
gression
taking
BZDshad
sign
ificantlyincrea
sedag
gression
compa
redwiththosenot
takingBZDsan
dthosewithou
tahistory
ofag
gression
Kostenet
al16
Prosp
ective
coho
rt37
0pa
tien
tswith
PTSD
inmen
tal
health
trea
tmen
t
Any
agen
tdo
se
anddu
ration
12mo
MIS
STho
setakingBZDshad
sign
ificantlyincrea
sed
PTSD
symptom
sat
baselinecompa
redwith
thosenot
takingBZDs
BSI
Tho
setaking
BZD
sha
dsign
ificantly
increa
sed
anxietyat
baselin
ecompa
redwiththoseno
ttaking
BZD
sNosign
ificant
diffe
rencebe
tween
BZD
san
dno
BZD
sin
chan
gein
anxiety
NVVRS-
derive
dinstru
men
t
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
violen
ceat
baseline
Thosewith
comorbidSUD
takingBZDshad
less
impr
ovem
entin
violen
cecompa
redwith
thosewithcomorbidSUD
not
takingBZDs
butthis
differen
cewas
not
sign
ificant
ASI
Tho
setakingBZDshad
sign
ificantlyincrea
sed
alcohol
use
atba
selinecompa
redwiththose
not
takingBZDs
Nosign
ificantdifferen
cebe
twee
nBZDsan
dnoBZDsin
chan
gein
subs
tance
use
orsocial
functioning
Those
withcomorbidSUD
takingBZDshad
less
impr
ovem
entin
subs
tance
use
compa
red
withthosewithcomorbidSUD
not
taking
BZDs
butthis
differen
cewas
not
sign
ificant
Rosen
etal
17Prosp
ective
coho
rt28
3pa
tien
tswith
PTSD
(140
inpr
olon
ged
expo
sure14
3in
presen
t-centered
psycho
therap
ysu
fficien
tda
tafor
meta-an
alysis
was
only
availablefor
143pa
tien
ts)
Any
agen
tdo
se
anddu
ration
6mo
CAPS
Nosign
ificance
differen
cebe
twee
nBZDswith
prolon
gedex
posu
rean
dnoBZDswitheither
therap
yin
PTSD
symptom
sThosetaking
BZDsin
presen
t-centeredps
ychotherap
yhad
sign
ificantlyworse
posttrea
tmen
tmaintenan
ceof
impr
ovem
ents
inPTSD
symptom
scompa
redwithother
grou
psPCL
Inpr
esen
t-centeredtherap
ythosetaking
BZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
sdu
ringps
ychotherap
ycompa
redwiththosenot
takingBZDs
Significance
ofresu
ltsforpr
olon
gedex
posu
rewerenot
determ
inab
ledu
eto
presen
ceof
aninteractionterm
andtheway
theresu
lts
werepr
esen
ted
286 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Jone
set
al18
Prosp
ective
coho
rt23
8recent
trau
mapa
tien
ts(ICU)
Any
agen
tdo
sean
ddu
ration
3mo
PTSS-14
Higher
BZD
dosesin
theIC
Uas
sociated
with
sign
ificantlyincrea
sedPTSD
symptom
s
Sam
uelson
etal
19Prosp
ective
coho
rt22
6recent
trau
ma
patien
ts(ICU)
Midaz
olam
(any
dose
ordu
ration
)
2mo
IES-R
Tho
sereceivingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(68
vs30
)
Bienv
enu
etal
20Prosp
ective
coho
rt18
6recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
3-24
mo
IES-R
Higher
BZD
dosesin
theIC
Unot
associated
withsign
ificantch
ange
sin
therisk
ofde
velopingPTSD
Baran
yiet
al21
Prosp
ective
coho
rt12
6trau
ma
patien
ts(solid-organ
tran
splants)
Any
agen
tdo
se
anddu
ration
Mea
nof
249
mo
PTSS-10
Chronic
BZD
useeither
before
orafter
surgery
associated
withsign
ificantly
increa
sedrisk
ofPTSD
symptom
s
Girardet
al22
Prosp
ective
coho
rt43
recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
6mo
PTSS-10
Greater
BZD
administrationin
theIC
Uas
sociated
withsign
ificantlyincrea
sedrisk
ofde
velopingPTSD
Van
Minne
net
al23
Prosp
ective
coho
rt43
patien
tswith
PTSD
inpr
olon
ged
expo
sure
Daily
useof
any
agen
tor
dose
3mo
PSS-SR
Tho
setakingBZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
san
dmore
drop
outs
compa
redwiththosenot
taking
BZDs
McG
hee
etal
24Retrosp
ective
coho
rt21
1trau
ma
patien
ts(bur
nsrequ
iringsu
rgery)
Midaz
olam
(any
dose
intrao
perative
)
Any
upto
4y
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
risk
ofde
velopingPTSD
Sha
levan
dRog
el-
Fuc
hs25
Cross-section
al18
patien
tswith
PTSD
Clona
zepa
m(27plusmn11mgd)
Not ap
plicab
leOrbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
mag
nitude
orhab
ituationrate
ofacou
stic
startleresp
onses
ASIindicates
Addiction
SeverityIn
dexB
DIBeckDep
ressionIn
ventoryB
SIBrief
Sym
ptom
Inventory
BZDb
enzodiazepineCAPSC
linician-administeredPTSD
Sca
leCTSCon
flicts
Tac
tics
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRatingSca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionIC
U
intensive
care
unitI
ESIm
pact
ofEvent
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDN
VVRSNational
Vietnam
Veteran
sRea
djustmen
tStudy
PCLP
TSD
ChecklistPSS-SRP
TSD
Sym
ptom
Sca
leSelf-repo
rtP
TSSP
osttra
umatic
StressSyn
dromeSca
leP
TSDp
osttra
umatic
stress
disorderS
CID
StructuredClinical
Interview
fortheDSMSTAI
State-Tra
itAnxietyIn
ventoryS
UDsu
bstance
use
disorderVASvisu
alan
alog
scale
Journal of Psychiatric Practice Vol 21 No 4 July 2015 287
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
umaTyp
e(
)
Rothb
aum
etal
8IIraq
andor
Afgha
nistan
veterans
DSM-IVcriteria
forPTSD
dueto
militarytrau
mave
rified
throug
hdischa
rgepa
pers
discon
tinu
edtaking
long
-actingBZD
sfor1moan
dsh
ort-
acting
BZD
sfor2wkbe
fore
screen
ing
stab
ledo
sesof
othe
rps
ycho
trop
icmed
ications
forat
leas
t2wkbe
fore
thestud
ywritten
inform
edconsent
EMed
ically
unstab
leps
ycho
sis
bipo
lardisord
erc
urrent
suicidal
risk
cu
rren
talcoho
lor
drug
depe
nden
ce
preg
nanc
ygluc
ocorticoids
BZD
sch
ronicallyus
edop
ioids
354
Black
50
White
42
Hispa
nic5
Other3
Com
bat10
0
Mellm
anet
al9
IAdm
ittedto
leve
lItrau
macenterr
ecallof
trau
ma
atleas
tmod
erateim
pairmen
tof
slee
pinitiation
ormainten
ance
mee
tfullcriteria
forat
leas
t2PTSD
symptom
clus
ters
inDSM-IVwilling
andab
leto
prov
idewritten
inform
edcons
ent
EIn
toxication
attimeof
trau
ma
braininjurypr
eexisting
psychiatricdisord
ers
3636
Hispa
nic8
2White
9Black
9
MVC68
Assau
lt2
3Acciden
t9
Braun
etal
10I
DSM-III
criteria
forPTSDwilling
andab
leto
prov
ide
written
inform
edconsentfreeof
psycho
trop
icmed
ications
atleas
t2wkbe
fore
stud
yEPhy
sicallyun
healthy
sign
ificant
head
injury
38Com
bat40
MVC30
Acciden
t20
Terrorism
10
Cates
etal
11I
DSM-IV
criteria
forPTSDat
leas
tthrice
wee
klypr
oblems
withslee
pan
dnigh
tmaresw
illing
andab
leto
prov
ide
written
inform
edconsent
Elt
18yold
unstab
lemed
ical
cond
itions
sen
sitivity
toBZD
scu
rren
tBZD
use
subs
tanc
eab
useor
depe
nden
cein
past
4wk
inab
ilityto
attend
regu
larfollow
-upvisitswom
enwho
wereeither
preg
nant
orof
child-be
aringpo
tentialan
dno
tus
ingcontraceptivesde
men
tia
cogn
itivedisord
er
520
Com
bat10
0
Gelpinet
al12
IEmerge
ncyroom
admission
swithatrau
ma
ETak
ingps
ycho
trop
icmed
ications
before
thetrau
ma
coma
head
injuryloss
ofcons
ciou
sness
2946
MVCs
77
Terrorism
19
Acciden
t4
Sha
levet
al13
IDSM-III-R
criteria
forPTSD
orpa
nicdisord
ermed
ication
free
EPsych
osism
ajor
depr
ession
cur
rent
orpa
stsu
bstanc
eor
alcoho
lus
epa
tien
tswithPTSD
withsp
ontane
ouspa
nic
attack
spa
tien
tswithpa
nicdisord
erwithahistoryof
trau
ma
3439
288 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
Zatzicket
al14
I18
-84yold
Eng
lish
-spe
akingor
Spa
nish
-spe
akingpa
tien
ts
arrive
daliveat
hosp
italm
oderateto
seve
reinjuries
Eg
reater
than
oreq
ual
toge65
yoldwithafirstlisted
diag
nosisof
hipfracturem
ajor
burn
strea
tmen
tde
lays
gt24
hincarcerated
attimeof
injury
4135
White
67
Black
16
Hispa
nic13
Other3
Injury10
0
Shinet
al15
I18
-69yold
militaryve
terans
servingin
Vietnam
eraor
laterat
leas
ton
eou
tpatient
VAvisitwithaPTSD
diag
nosis
EN
oPTSD
diag
nosisin
thepr
ior2y
4250
White
65
Black
17
Hispa
nic10
Other3
Kostenet
al16
IDSM-III
criteria
forPTSDmilitaryve
terans
450
White
75
Rosen
etal
17I
femaleve
teranor
active
duty
soldier
DSM-IV
criteria
for
PTSDCAPSscoregt45
EC
oncu
rren
tPTSD
psycho
therap
yothe
rthan
briefvisits
withan
existing
therap
istor
participationin
self-help
grou
psc
hang
ein
psycho
active
med
ications
during
the2mo
before
stud
yrecruitm
entsu
bstanc
ede
pend
ence
notin
remission
forat
leas
t3mo
curren
tps
ycho
ticsymptom
sor
man
iab
ipolar
disord
erpr
ominen
tcu
rren
tsu
icidal
orho
micidal
idea
tion
cogn
itiveim
pairmen
tcu
rren
tinvo
lvem
entin
violen
trelation
shipself-m
utilationwithin
thepa
st6mo
100
White
55
Black
33
Hispa
nic
6Other7
Sex
ual93
Acciden
t82
Disas
ter
72
Com
bat25
Jone
set
al18
Igt18
yold
mecha
nicallyve
ntilated
IC
Uleng
thof
stay
atleas
t48
hEP
rior
PTSDa
dmittedaftersu
icideattemptp
reex
isting
orconc
omitan
tps
ycho
ticillness
reside
sgt30
kmfrom
hosp
ital
unresolved
confus
ionen
rolled
inan
othe
rresearch
stud
y
6138
Life-threaten
ingmed
ical
condition
10
0
Sam
uelson
etal
19I
gt18
yold
mecha
nicallyve
ntilated
ge
neralIC
Uleng
thof
stay
atleas
t24
hEH
eadinjuryps
ycho
ticillness
men
talretard
ation
intoxication
adm
ittedaftersu
icideattempth
earing
spe
ech
disa
bilityno
n-Swed
ishsp
eaking
tran
sferredto
anothe
rho
spitalm
echa
nicallyve
ntilated
atdischa
rge
mecha
nically
ventilated
gt24
hpr
eadm
ission
6348
Life-threaten
ingmed
ical
condition
10
0
Bienv
enuet
al20
IMecha
nicallyve
ntilated
withacutelung
injury
EN
eurologicalsp
ecialtyIC
Upr
eexistingillnesswithalife
expe
ctan
cylt6mo
pree
xistingcogn
itiveim
pairmen
tor
commun
icationlang
uage
barriersn
ofixe
dad
dress
tran
sfer
toastud
ysite
ICU
withpr
eexistingacutelung
injury
gt24
h
45
Life-threaten
ingmed
ical
condition
10
0
Journal of Psychiatric Practice Vol 21 No 4 July 2015 289
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

TABLE
1Summar
yof
Clinical
and
Obse
rvat
ional
Stu
diesof
Ben
zodiaze
pin
esin
Pos
ttra
umat
icStres
sDisor
der
(PTSD)(con
tinued
)
Refer
ence
sStu
dy
Design
Particip
ants
(N)
Ben
zodia
zepin
eFollow-up
Assessm
ent
Outcom
es
Jone
set
al18
Prosp
ective
coho
rt23
8recent
trau
mapa
tien
ts(ICU)
Any
agen
tdo
sean
ddu
ration
3mo
PTSS-14
Higher
BZD
dosesin
theIC
Uas
sociated
with
sign
ificantlyincrea
sedPTSD
symptom
s
Sam
uelson
etal
19Prosp
ective
coho
rt22
6recent
trau
ma
patien
ts(ICU)
Midaz
olam
(any
dose
ordu
ration
)
2mo
IES-R
Tho
sereceivingBZDssign
ificantlymorelike
lyto
deve
lopPTSD
than
thosenot
takingBZDs
(68
vs30
)
Bienv
enu
etal
20Prosp
ective
coho
rt18
6recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
3-24
mo
IES-R
Higher
BZD
dosesin
theIC
Unot
associated
withsign
ificantch
ange
sin
therisk
ofde
velopingPTSD
Baran
yiet
al21
Prosp
ective
coho
rt12
6trau
ma
patien
ts(solid-organ
tran
splants)
Any
agen
tdo
se
anddu
ration
Mea
nof
249
mo
PTSS-10
Chronic
BZD
useeither
before
orafter
surgery
associated
withsign
ificantly
increa
sedrisk
ofPTSD
symptom
s
Girardet
al22
Prosp
ective
coho
rt43
recent
trau
ma
patien
ts(ICU)
Any
agen
tdo
se
anddu
ration
6mo
PTSS-10
Greater
BZD
administrationin
theIC
Uas
sociated
withsign
ificantlyincrea
sedrisk
ofde
velopingPTSD
Van
Minne
net
al23
Prosp
ective
coho
rt43
patien
tswith
PTSD
inpr
olon
ged
expo
sure
Daily
useof
any
agen
tor
dose
3mo
PSS-SR
Tho
setakingBZDshad
sign
ificantlyless
impr
ovem
entin
PTSD
symptom
san
dmore
drop
outs
compa
redwiththosenot
taking
BZDs
McG
hee
etal
24Retrosp
ective
coho
rt21
1trau
ma
patien
ts(bur
nsrequ
iringsu
rgery)
Midaz
olam
(any
dose
intrao
perative
)
Any
upto
4y
PCL
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
risk
ofde
velopingPTSD
Sha
levan
dRog
el-
Fuc
hs25
Cross-section
al18
patien
tswith
PTSD
Clona
zepa
m(27plusmn11mgd)
Not ap
plicab
leOrbicularis
oculiEMG
skin
cond
uctanc
ehe
artrate
Nosign
ificantdifferen
cebe
twee
nBZDsan
dno
BZDsin
mag
nitude
orhab
ituationrate
ofacou
stic
startleresp
onses
ASIindicates
Addiction
SeverityIn
dexB
DIBeckDep
ressionIn
ventoryB
SIBrief
Sym
ptom
Inventory
BZDb
enzodiazepineCAPSC
linician-administeredPTSD
Sca
leCTSCon
flicts
Tac
tics
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRatingSca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionIC
U
intensive
care
unitI
ESIm
pact
ofEvent
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDN
VVRSNational
Vietnam
Veteran
sRea
djustmen
tStudy
PCLP
TSD
ChecklistPSS-SRP
TSD
Sym
ptom
Sca
leSelf-repo
rtP
TSSP
osttra
umatic
StressSyn
dromeSca
leP
TSDp
osttra
umatic
stress
disorderS
CID
StructuredClinical
Interview
fortheDSMSTAI
State-Tra
itAnxietyIn
ventoryS
UDsu
bstance
use
disorderVASvisu
alan
alog
scale
Journal of Psychiatric Practice Vol 21 No 4 July 2015 287
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
umaTyp
e(
)
Rothb
aum
etal
8IIraq
andor
Afgha
nistan
veterans
DSM-IVcriteria
forPTSD
dueto
militarytrau
mave
rified
throug
hdischa
rgepa
pers
discon
tinu
edtaking
long
-actingBZD
sfor1moan
dsh
ort-
acting
BZD
sfor2wkbe
fore
screen
ing
stab
ledo
sesof
othe
rps
ycho
trop
icmed
ications
forat
leas
t2wkbe
fore
thestud
ywritten
inform
edconsent
EMed
ically
unstab
leps
ycho
sis
bipo
lardisord
erc
urrent
suicidal
risk
cu
rren
talcoho
lor
drug
depe
nden
ce
preg
nanc
ygluc
ocorticoids
BZD
sch
ronicallyus
edop
ioids
354
Black
50
White
42
Hispa
nic5
Other3
Com
bat10
0
Mellm
anet
al9
IAdm
ittedto
leve
lItrau
macenterr
ecallof
trau
ma
atleas
tmod
erateim
pairmen
tof
slee
pinitiation
ormainten
ance
mee
tfullcriteria
forat
leas
t2PTSD
symptom
clus
ters
inDSM-IVwilling
andab
leto
prov
idewritten
inform
edcons
ent
EIn
toxication
attimeof
trau
ma
braininjurypr
eexisting
psychiatricdisord
ers
3636
Hispa
nic8
2White
9Black
9
MVC68
Assau
lt2
3Acciden
t9
Braun
etal
10I
DSM-III
criteria
forPTSDwilling
andab
leto
prov
ide
written
inform
edconsentfreeof
psycho
trop
icmed
ications
atleas
t2wkbe
fore
stud
yEPhy
sicallyun
healthy
sign
ificant
head
injury
38Com
bat40
MVC30
Acciden
t20
Terrorism
10
Cates
etal
11I
DSM-IV
criteria
forPTSDat
leas
tthrice
wee
klypr
oblems
withslee
pan
dnigh
tmaresw
illing
andab
leto
prov
ide
written
inform
edconsent
Elt
18yold
unstab
lemed
ical
cond
itions
sen
sitivity
toBZD
scu
rren
tBZD
use
subs
tanc
eab
useor
depe
nden
cein
past
4wk
inab
ilityto
attend
regu
larfollow
-upvisitswom
enwho
wereeither
preg
nant
orof
child-be
aringpo
tentialan
dno
tus
ingcontraceptivesde
men
tia
cogn
itivedisord
er
520
Com
bat10
0
Gelpinet
al12
IEmerge
ncyroom
admission
swithatrau
ma
ETak
ingps
ycho
trop
icmed
ications
before
thetrau
ma
coma
head
injuryloss
ofcons
ciou
sness
2946
MVCs
77
Terrorism
19
Acciden
t4
Sha
levet
al13
IDSM-III-R
criteria
forPTSD
orpa
nicdisord
ermed
ication
free
EPsych
osism
ajor
depr
ession
cur
rent
orpa
stsu
bstanc
eor
alcoho
lus
epa
tien
tswithPTSD
withsp
ontane
ouspa
nic
attack
spa
tien
tswithpa
nicdisord
erwithahistoryof
trau
ma
3439
288 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
Zatzicket
al14
I18
-84yold
Eng
lish
-spe
akingor
Spa
nish
-spe
akingpa
tien
ts
arrive
daliveat
hosp
italm
oderateto
seve
reinjuries
Eg
reater
than
oreq
ual
toge65
yoldwithafirstlisted
diag
nosisof
hipfracturem
ajor
burn
strea
tmen
tde
lays
gt24
hincarcerated
attimeof
injury
4135
White
67
Black
16
Hispa
nic13
Other3
Injury10
0
Shinet
al15
I18
-69yold
militaryve
terans
servingin
Vietnam
eraor
laterat
leas
ton
eou
tpatient
VAvisitwithaPTSD
diag
nosis
EN
oPTSD
diag
nosisin
thepr
ior2y
4250
White
65
Black
17
Hispa
nic10
Other3
Kostenet
al16
IDSM-III
criteria
forPTSDmilitaryve
terans
450
White
75
Rosen
etal
17I
femaleve
teranor
active
duty
soldier
DSM-IV
criteria
for
PTSDCAPSscoregt45
EC
oncu
rren
tPTSD
psycho
therap
yothe
rthan
briefvisits
withan
existing
therap
istor
participationin
self-help
grou
psc
hang
ein
psycho
active
med
ications
during
the2mo
before
stud
yrecruitm
entsu
bstanc
ede
pend
ence
notin
remission
forat
leas
t3mo
curren
tps
ycho
ticsymptom
sor
man
iab
ipolar
disord
erpr
ominen
tcu
rren
tsu
icidal
orho
micidal
idea
tion
cogn
itiveim
pairmen
tcu
rren
tinvo
lvem
entin
violen
trelation
shipself-m
utilationwithin
thepa
st6mo
100
White
55
Black
33
Hispa
nic
6Other7
Sex
ual93
Acciden
t82
Disas
ter
72
Com
bat25
Jone
set
al18
Igt18
yold
mecha
nicallyve
ntilated
IC
Uleng
thof
stay
atleas
t48
hEP
rior
PTSDa
dmittedaftersu
icideattemptp
reex
isting
orconc
omitan
tps
ycho
ticillness
reside
sgt30
kmfrom
hosp
ital
unresolved
confus
ionen
rolled
inan
othe
rresearch
stud
y
6138
Life-threaten
ingmed
ical
condition
10
0
Sam
uelson
etal
19I
gt18
yold
mecha
nicallyve
ntilated
ge
neralIC
Uleng
thof
stay
atleas
t24
hEH
eadinjuryps
ycho
ticillness
men
talretard
ation
intoxication
adm
ittedaftersu
icideattempth
earing
spe
ech
disa
bilityno
n-Swed
ishsp
eaking
tran
sferredto
anothe
rho
spitalm
echa
nicallyve
ntilated
atdischa
rge
mecha
nically
ventilated
gt24
hpr
eadm
ission
6348
Life-threaten
ingmed
ical
condition
10
0
Bienv
enuet
al20
IMecha
nicallyve
ntilated
withacutelung
injury
EN
eurologicalsp
ecialtyIC
Upr
eexistingillnesswithalife
expe
ctan
cylt6mo
pree
xistingcogn
itiveim
pairmen
tor
commun
icationlang
uage
barriersn
ofixe
dad
dress
tran
sfer
toastud
ysite
ICU
withpr
eexistingacutelung
injury
gt24
h
45
Life-threaten
ingmed
ical
condition
10
0
Journal of Psychiatric Practice Vol 21 No 4 July 2015 289
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
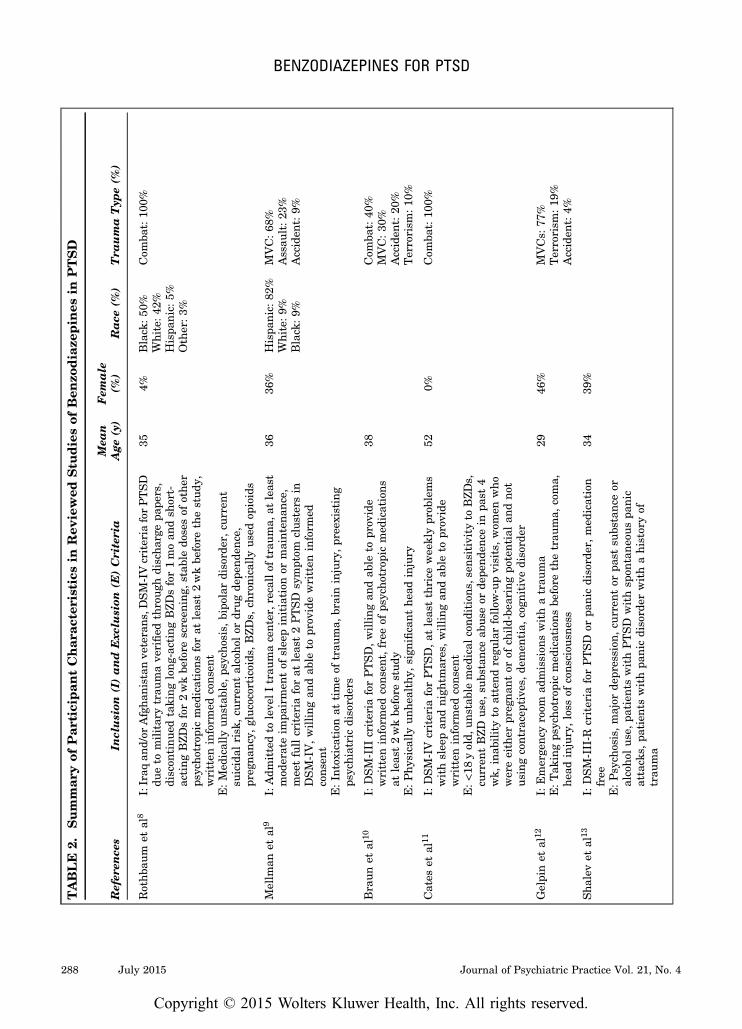
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
umaTyp
e(
)
Rothb
aum
etal
8IIraq
andor
Afgha
nistan
veterans
DSM-IVcriteria
forPTSD
dueto
militarytrau
mave
rified
throug
hdischa
rgepa
pers
discon
tinu
edtaking
long
-actingBZD
sfor1moan
dsh
ort-
acting
BZD
sfor2wkbe
fore
screen
ing
stab
ledo
sesof
othe
rps
ycho
trop
icmed
ications
forat
leas
t2wkbe
fore
thestud
ywritten
inform
edconsent
EMed
ically
unstab
leps
ycho
sis
bipo
lardisord
erc
urrent
suicidal
risk
cu
rren
talcoho
lor
drug
depe
nden
ce
preg
nanc
ygluc
ocorticoids
BZD
sch
ronicallyus
edop
ioids
354
Black
50
White
42
Hispa
nic5
Other3
Com
bat10
0
Mellm
anet
al9
IAdm
ittedto
leve
lItrau
macenterr
ecallof
trau
ma
atleas
tmod
erateim
pairmen
tof
slee
pinitiation
ormainten
ance
mee
tfullcriteria
forat
leas
t2PTSD
symptom
clus
ters
inDSM-IVwilling
andab
leto
prov
idewritten
inform
edcons
ent
EIn
toxication
attimeof
trau
ma
braininjurypr
eexisting
psychiatricdisord
ers
3636
Hispa
nic8
2White
9Black
9
MVC68
Assau
lt2
3Acciden
t9
Braun
etal
10I
DSM-III
criteria
forPTSDwilling
andab
leto
prov
ide
written
inform
edconsentfreeof
psycho
trop
icmed
ications
atleas
t2wkbe
fore
stud
yEPhy
sicallyun
healthy
sign
ificant
head
injury
38Com
bat40
MVC30
Acciden
t20
Terrorism
10
Cates
etal
11I
DSM-IV
criteria
forPTSDat
leas
tthrice
wee
klypr
oblems
withslee
pan
dnigh
tmaresw
illing
andab
leto
prov
ide
written
inform
edconsent
Elt
18yold
unstab
lemed
ical
cond
itions
sen
sitivity
toBZD
scu
rren
tBZD
use
subs
tanc
eab
useor
depe
nden
cein
past
4wk
inab
ilityto
attend
regu
larfollow
-upvisitswom
enwho
wereeither
preg
nant
orof
child-be
aringpo
tentialan
dno
tus
ingcontraceptivesde
men
tia
cogn
itivedisord
er
520
Com
bat10
0
Gelpinet
al12
IEmerge
ncyroom
admission
swithatrau
ma
ETak
ingps
ycho
trop
icmed
ications
before
thetrau
ma
coma
head
injuryloss
ofcons
ciou
sness
2946
MVCs
77
Terrorism
19
Acciden
t4
Sha
levet
al13
IDSM-III-R
criteria
forPTSD
orpa
nicdisord
ermed
ication
free
EPsych
osism
ajor
depr
ession
cur
rent
orpa
stsu
bstanc
eor
alcoho
lus
epa
tien
tswithPTSD
withsp
ontane
ouspa
nic
attack
spa
tien
tswithpa
nicdisord
erwithahistoryof
trau
ma
3439
288 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
Zatzicket
al14
I18
-84yold
Eng
lish
-spe
akingor
Spa
nish
-spe
akingpa
tien
ts
arrive
daliveat
hosp
italm
oderateto
seve
reinjuries
Eg
reater
than
oreq
ual
toge65
yoldwithafirstlisted
diag
nosisof
hipfracturem
ajor
burn
strea
tmen
tde
lays
gt24
hincarcerated
attimeof
injury
4135
White
67
Black
16
Hispa
nic13
Other3
Injury10
0
Shinet
al15
I18
-69yold
militaryve
terans
servingin
Vietnam
eraor
laterat
leas
ton
eou
tpatient
VAvisitwithaPTSD
diag
nosis
EN
oPTSD
diag
nosisin
thepr
ior2y
4250
White
65
Black
17
Hispa
nic10
Other3
Kostenet
al16
IDSM-III
criteria
forPTSDmilitaryve
terans
450
White
75
Rosen
etal
17I
femaleve
teranor
active
duty
soldier
DSM-IV
criteria
for
PTSDCAPSscoregt45
EC
oncu
rren
tPTSD
psycho
therap
yothe
rthan
briefvisits
withan
existing
therap
istor
participationin
self-help
grou
psc
hang
ein
psycho
active
med
ications
during
the2mo
before
stud
yrecruitm
entsu
bstanc
ede
pend
ence
notin
remission
forat
leas
t3mo
curren
tps
ycho
ticsymptom
sor
man
iab
ipolar
disord
erpr
ominen
tcu
rren
tsu
icidal
orho
micidal
idea
tion
cogn
itiveim
pairmen
tcu
rren
tinvo
lvem
entin
violen
trelation
shipself-m
utilationwithin
thepa
st6mo
100
White
55
Black
33
Hispa
nic
6Other7
Sex
ual93
Acciden
t82
Disas
ter
72
Com
bat25
Jone
set
al18
Igt18
yold
mecha
nicallyve
ntilated
IC
Uleng
thof
stay
atleas
t48
hEP
rior
PTSDa
dmittedaftersu
icideattemptp
reex
isting
orconc
omitan
tps
ycho
ticillness
reside
sgt30
kmfrom
hosp
ital
unresolved
confus
ionen
rolled
inan
othe
rresearch
stud
y
6138
Life-threaten
ingmed
ical
condition
10
0
Sam
uelson
etal
19I
gt18
yold
mecha
nicallyve
ntilated
ge
neralIC
Uleng
thof
stay
atleas
t24
hEH
eadinjuryps
ycho
ticillness
men
talretard
ation
intoxication
adm
ittedaftersu
icideattempth
earing
spe
ech
disa
bilityno
n-Swed
ishsp
eaking
tran
sferredto
anothe
rho
spitalm
echa
nicallyve
ntilated
atdischa
rge
mecha
nically
ventilated
gt24
hpr
eadm
ission
6348
Life-threaten
ingmed
ical
condition
10
0
Bienv
enuet
al20
IMecha
nicallyve
ntilated
withacutelung
injury
EN
eurologicalsp
ecialtyIC
Upr
eexistingillnesswithalife
expe
ctan
cylt6mo
pree
xistingcogn
itiveim
pairmen
tor
commun
icationlang
uage
barriersn
ofixe
dad
dress
tran
sfer
toastud
ysite
ICU
withpr
eexistingacutelung
injury
gt24
h
45
Life-threaten
ingmed
ical
condition
10
0
Journal of Psychiatric Practice Vol 21 No 4 July 2015 289
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
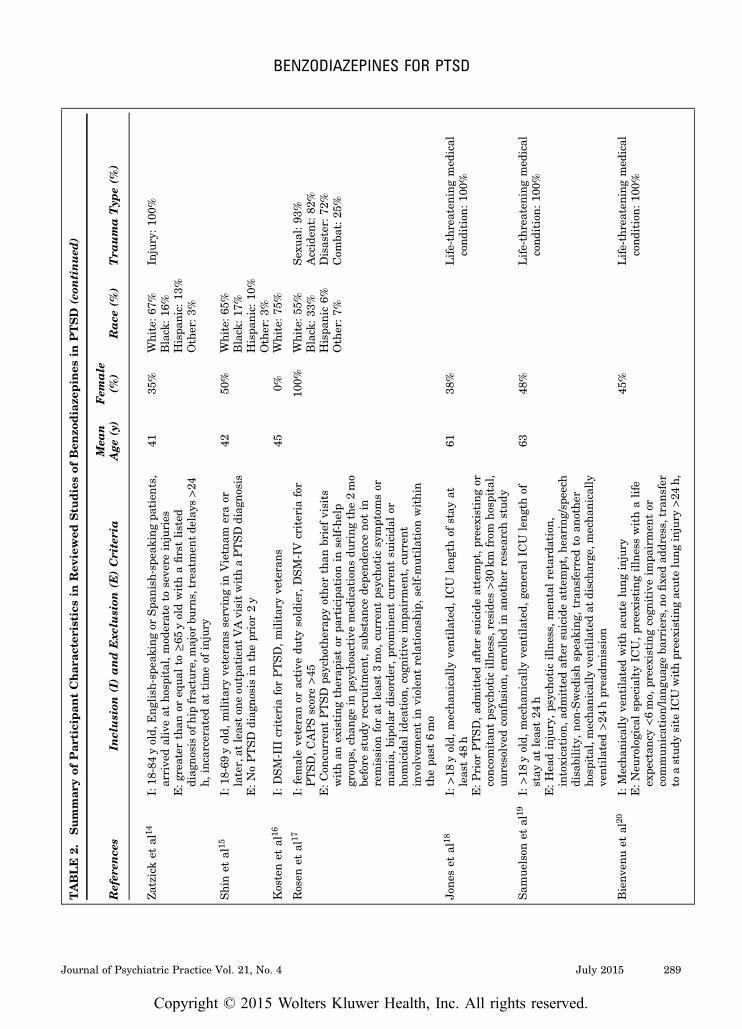
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
Zatzicket
al14
I18
-84yold
Eng
lish
-spe
akingor
Spa
nish
-spe
akingpa
tien
ts
arrive
daliveat
hosp
italm
oderateto
seve
reinjuries
Eg
reater
than
oreq
ual
toge65
yoldwithafirstlisted
diag
nosisof
hipfracturem
ajor
burn
strea
tmen
tde
lays
gt24
hincarcerated
attimeof
injury
4135
White
67
Black
16
Hispa
nic13
Other3
Injury10
0
Shinet
al15
I18
-69yold
militaryve
terans
servingin
Vietnam
eraor
laterat
leas
ton
eou
tpatient
VAvisitwithaPTSD
diag
nosis
EN
oPTSD
diag
nosisin
thepr
ior2y
4250
White
65
Black
17
Hispa
nic10
Other3
Kostenet
al16
IDSM-III
criteria
forPTSDmilitaryve
terans
450
White
75
Rosen
etal
17I
femaleve
teranor
active
duty
soldier
DSM-IV
criteria
for
PTSDCAPSscoregt45
EC
oncu
rren
tPTSD
psycho
therap
yothe
rthan
briefvisits
withan
existing
therap
istor
participationin
self-help
grou
psc
hang
ein
psycho
active
med
ications
during
the2mo
before
stud
yrecruitm
entsu
bstanc
ede
pend
ence
notin
remission
forat
leas
t3mo
curren
tps
ycho
ticsymptom
sor
man
iab
ipolar
disord
erpr
ominen
tcu
rren
tsu
icidal
orho
micidal
idea
tion
cogn
itiveim
pairmen
tcu
rren
tinvo
lvem
entin
violen
trelation
shipself-m
utilationwithin
thepa
st6mo
100
White
55
Black
33
Hispa
nic
6Other7
Sex
ual93
Acciden
t82
Disas
ter
72
Com
bat25
Jone
set
al18
Igt18
yold
mecha
nicallyve
ntilated
IC
Uleng
thof
stay
atleas
t48
hEP
rior
PTSDa
dmittedaftersu
icideattemptp
reex
isting
orconc
omitan
tps
ycho
ticillness
reside
sgt30
kmfrom
hosp
ital
unresolved
confus
ionen
rolled
inan
othe
rresearch
stud
y
6138
Life-threaten
ingmed
ical
condition
10
0
Sam
uelson
etal
19I
gt18
yold
mecha
nicallyve
ntilated
ge
neralIC
Uleng
thof
stay
atleas
t24
hEH
eadinjuryps
ycho
ticillness
men
talretard
ation
intoxication
adm
ittedaftersu
icideattempth
earing
spe
ech
disa
bilityno
n-Swed
ishsp
eaking
tran
sferredto
anothe
rho
spitalm
echa
nicallyve
ntilated
atdischa
rge
mecha
nically
ventilated
gt24
hpr
eadm
ission
6348
Life-threaten
ingmed
ical
condition
10
0
Bienv
enuet
al20
IMecha
nicallyve
ntilated
withacutelung
injury
EN
eurologicalsp
ecialtyIC
Upr
eexistingillnesswithalife
expe
ctan
cylt6mo
pree
xistingcogn
itiveim
pairmen
tor
commun
icationlang
uage
barriersn
ofixe
dad
dress
tran
sfer
toastud
ysite
ICU
withpr
eexistingacutelung
injury
gt24
h
45
Life-threaten
ingmed
ical
condition
10
0
Journal of Psychiatric Practice Vol 21 No 4 July 2015 289
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

TABLE
2Summar
yof
Par
ticipan
tChar
acteristicsin
Rev
iewed
Stu
diesof
Ben
zodiaze
pin
esin
PTSD
(con
tinued
)
Refer
ence
sIn
clusion
(I)and
Exc
lusion
(E)Criteria
Mea
nAge
(y)
Fem
ale
()
Race
()
Tra
uma
Typ
e(
)
gt5dof
mecha
nicalve
ntilationbe
fore
acutelung
injurya
physicianorde
rforno
escalation
ofIC
Ucare
atthetimeof
stud
yeligibility
Baran
yiet
al21
IPatientsreceivingsolid-orga
ntran
splantsan
dIC
Utrea
tmen
t52
31
White
100
Life-threaten
ingmed
ical
condition
10
0
Girardet
al22
IIn
med
ical
orcorona
ryIC
Umecha
nicallyve
ntilated
EN
eurologicaldiseas
eim
pairingcogn
itivefunc
tion
men
tal
retard
ation
nonndash
Eng
lish
spea
king
sens
oryde
ficits
impa
iringcommun
ication
5253
Black
16
Life-threaten
ingmed
ical
condition
10
0
Van
Minne
net
al23
IDSM-III-R
criteria
forPTSD
for3moor
more
3774
Sex
ual22
Violence21
Battering
19
Acciden
t14
MVC13
Other11
McG
heeet
al24
IThe
rmal
injuries
during
militaryde
ploy
men
tssu
rgery
within30
dof
injury
betw
een20
04an
d20
08P
CL
betw
een
2004
and20
08
Com
bat10
0
Sha
levan
dRog
el-
Fuc
hs25
IDSM-III-R
criteria
forPTSDreceivingclon
azep
amor
med
icationfree
EP
anic
disord
ers
ubstan
cede
pend
ence
3511
BZD
indica
tesbenz
odiazepine
CAPSC
linician-administeredPTSD
Sca
leD
SMD
iagn
ostican
dStatistical
Man
ual
ofMen
talDisorders
ICUintensive
care
unit
MVCmotor
vehicle
collisionP
CLPTSD
ChecklistPTSDpo
sttrau
matic
stress
disorderVAVeteran
sAffairs
290 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

(κ=089) nonrandomized clinical trials 100(κ=100) observational studies 977 (κ=063) Thepercent agreement for data abstraction was 761
After excluding ineligible articles 18 studies wereselected for review and are summarized in Table 1
Sample sizes varied from 6 to 2931 with a total of5236 completers Because not every study reportedthe same characteristics the following numberswere calculated using available data for partic-ipants as summarized in Table 2 Participants
TABLE 3 Summary of Outcomes of Reviewed Studies of Benzodiazepines in PTSD
Randomized-controlled
Trials
Double-blind Other
NonrandomizedClinical Trials
ObservationalStudies
Level ofEvidence
Efficacy 1 1 0 0 DAnxiety short term 1 0 0 0 DSleep short term 0 1 0 0 DPTSD core symptoms 0 0 0 0 Ddagger
Long term 0 0 0 0 Ddagger
Inefficacy 2 2 2 12 ADaggerOverall severity 2 1 1 10 ADaggerStartle reflex 1 0 1 1 BPsychotherapy outcomes 1 0 0 2 BDepression 1 0 1 0 BOverall well-being 1 0 0 0 BSleep 0 2 0 0 CNightmares 0 1 0 0 CAnxiety 0 0 1 1 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CSocial functioning 0 0 0 1 C
Worsened outcomes 1 1 1 10 BOverall severity 1 1 1 9 BPsychotherapy outcomes 1 0 0 2 BDepression 0 0 1 0 CAggression 0 0 0 2 CSubstance use 0 0 0 1 CAnxiety 0 0 0 1 C
Note that studies with multiple measures or mixed results are counted more than once and bolded rows summarize the studies inthe areas listed belowThe findings of the selected articles were categorized according to levels of scientific evidence based on clinical practice guidelinesfrom the US Department of Health and Human Services6
A Multiple double-blind placebo-controlled trials and a confirmatory meta-analysis (in addition to level B of evidence)B At least 1 double-blind placebo-controlled trial (in addition to level C of evidence)C Anecdotal reports case series and open trials in addition to expert endorsement or consensusD Few case reports without any expert panel endorsement
No expert consensus supports this findingdaggerNothing but case reports supports this findingDaggerSupported by meta-analysisPTSD indicates posttraumatic stress disorder
Journal of Psychiatric Practice Vol 21 No 4 July 2015 291
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
Rothb
aum
etal
82
3CAPSpo
sttrea
tmen
t35
34minus002
14minus049
34045
052
3CAPS3mo
2923
minus052
97minus107
70001
762
3CAPS6mo
2523
minus057
87minus114
50minus001
242
3CAPS12
mo
2220
minus022
17minus082
73038
382
3PCLpo
sttrea
tmen
t35
34minus013
70minus060
89033
502
3PCL3mo
2923
minus050
31minus105
03004
422
3PCL6mo
2523
minus067
87minus124
50minus011
242
3PCL12
mo
2220
minus031
91minus092
47028
642
3PTSD
posttrea
tmen
t35
34minus001
72minus048
92045
472
3PTSD
3mo
2923
minus077
67minus132
40minus022
952
3PTSD
6mo
2523
minus070
07minus126
70minus013
442
3PTSD
12mo
2220
minus017
63minus078
19042
922
3CAPSpo
sttrea
tmen
tch
ange
3534
minus018
51minus065
71028
69
23
PCLpo
sttrea
tmen
tch
ange
3534
minus020
41minus067
61026
792
3CAPS12
moch
ange
2220
minus002
77minus063
32057
792
3PCL12
moch
ange
2220
minus003
20minus063
76057
352
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus021
29minus076
97034
39
Mellm
anet
al9
13
PTSD
diag
nosis
1111
minus057
74minus141
31025
841
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus057
74minus141
31025
84
3CAPS
1111
minus028
76minus112
34054
813
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus043
25minus126
82040
33
Braun
etal
102
3PTSD
Scale
Intrus
ion
1010
054
33minus033
32141
992
3PTSD
Scale
Avo
idan
ce10
10016
32minus071
33103
982
3HAM-D
1010
002
81minus084
84090
472
3HAM-A
1010
068
08minus019
58155
732
3IE
SIn
trus
ion
1010
052
41minus035
25140
062
3IE
SAvo
idan
ce10
10011
03minus076
63098
682
3VAS
1010
052
17minus035
48139
822
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
052
17minus035
48139
82
Cates
etal
112
3Sleep
onsetpr
oblems
66
113
03minus000
13226
192
3Mid-sleep
awak
ening
66
021
96minus091
20135
122
3Early-m
orning
awak
ening
66
074
58minus038
58187
742
3Difficu
ltyfallingas
leep
66
050
21minus062
95163
37
292 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
Sleep
quan
tity
66
030
16minus083
00143
322
3Sleep
quality
66
041
10minus072
06154
262
3Distressing
drea
ms
freq
uenc
y6
6minus018
51minus131
67094
65
23
Distressing
drea
ms
intens
ity
66
minus013
81minus126
97099
36
23
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
035
63minus077
53148
79
Gelpinet
al12
13
PTSD
diag
nosis
1313
minus129
99minus206
86minus053
111
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus129
99minus206
86minus053
11
3Major
depr
ession
diag
nosis
1313
minus152
75minus229
63minus075
873
Sim
pleph
obia
diag
nosis
1313
043
64minus033
23120
523
Socialph
obia
diag
nosis
1313
024
25minus052
62101
133
Alcoh
olab
usediag
nosis
1313
minus040
82minus117
70036
053
Pan
icdisord
erdiag
nosis
1313
minus040
82minus117
70036
053
Dysthym
ia13
13040
82minus036
05117
703
STAI-State
1313
minus015
11minus091
99061
763
STAI-Trait
1313
minus017
43minus094
31059
453
IESIn
trus
ion
1313
minus029
33minus106
20047
553
IESAvo
idan
ce13
13027
80minus049
08104
683
BDI
1313
minus036
91minus113
79039
963
MIS
S13
13minus046
28minus123
15030
603
HR
1313
037
29minus039
59114
173
Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus023
38minus100
26053
50
Sha
levet
al13
23
HAM-A
99
144
30051
91236
702
3Resting
EMG
99
minus009
74minus102
13082
662
3Bas
eEMG
99
047
04minus045
35139
442
3EMG
1sttone
resp
onse
99
043
04minus049
35135
442
3EMG
15th
tone
resp
onse
99
minus024
95minus117
34067
452
3Mea
nEMG
resp
onse
99
029
52minus062
88121
912
3EMG
resp
onse-TTC
99
minus003
71minus096
11088
682
3Resting
SC
99
037
22minus055
18129
612
3Bas
eSC
99
minus095
85minus188
25minus003
462
3SC
1sttone
resp
onse
99
minus097
37minus189
76minus004
97
Journal of Psychiatric Practice Vol 21 No 4 July 2015 293
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
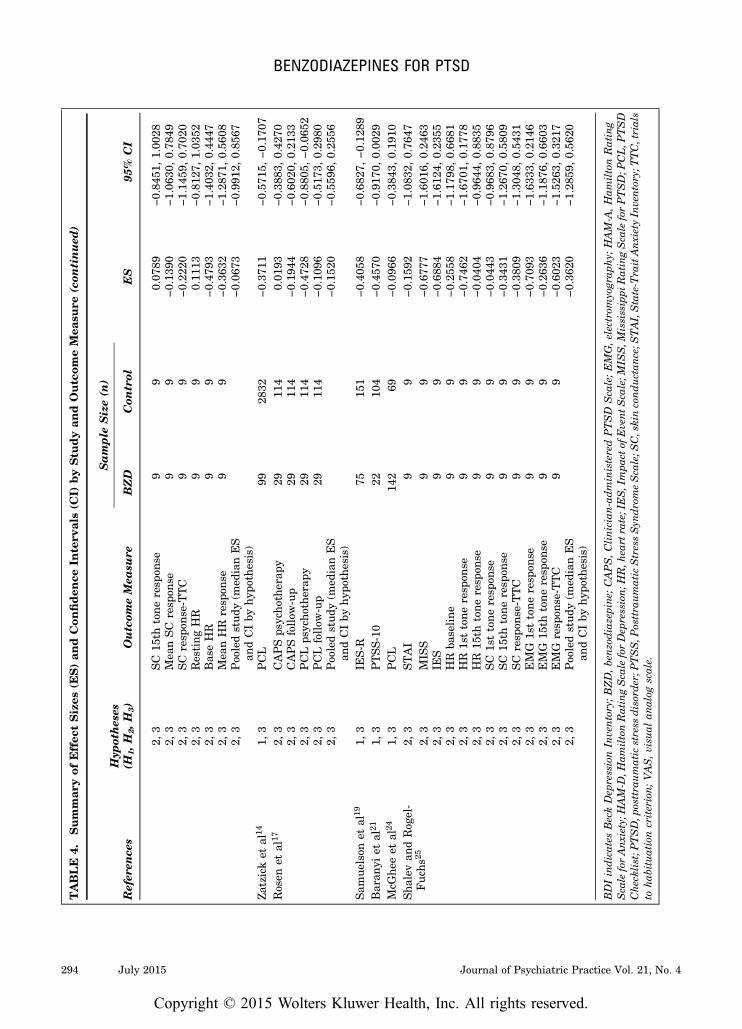
TABLE
4Summar
yof
Effec
tSizes
(ES)an
dCon
fiden
ceIn
terv
als(C
I)byStu
dyan
dOutcom
eMea
sure
(con
tinued
)
Sample
Size(n
)
Refer
ence
sHyp
otheses
(H1H
2H
3)
Outcom
eMea
sure
BZD
Con
trol
ES
95
CI
23
SC
15th
tone
resp
onse
99
007
89minus084
51100
282
3Mea
nSC
resp
onse
99
minus013
90minus106
30078
492
3SC
resp
onse-TTC
99
minus022
20minus114
59070
202
3Resting
HR
99
011
13minus081
27103
522
3Bas
eHR
99
minus047
93minus140
32044
472
3Mea
nHR
resp
onse
99
minus036
32minus128
71056
082
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus006
73minus099
12085
67
Zatzicket
al14
13
PCL
9928
32minus037
11minus057
15minus017
07Rosen
etal
172
3CAPSps
ycho
therap
y29
114
001
93minus038
83042
702
3CAPSfollow
-up
2911
4minus019
44minus060
20021
332
3PCLps
ycho
therap
y29
114
minus047
28minus088
05minus006
522
3PCLfollow
-up
2911
4minus010
96minus051
73029
802
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus015
20minus055
96025
56
Sam
uelson
etal
191
3IE
S-R
7515
1minus040
58minus068
27minus012
89Baran
yiet
al21
13
PTSS-10
2210
4minus045
70minus091
70000
29McG
heeet
al24
13
PCL
142
69minus009
66minus038
43019
10Sha
levan
dRog
el-
Fuc
hs25
23
STAI
99
minus015
92minus108
32076
472
3MIS
S9
9minus067
77minus160
16024
632
3IE
S9
9minus068
84minus161
24023
552
3HR
baseline
99
minus025
58minus117
98066
812
3HR
1sttone
resp
onse
99
minus074
62minus167
01017
782
3HR
15th
tone
resp
onse
99
minus004
04minus096
44088
352
3SC
1sttone
resp
onse
99
minus004
43minus096
83087
962
3SC
15th
tone
resp
onse
99
minus034
31minus126
70058
092
3SC
resp
onse-TTC
99
minus038
09minus130
48054
312
3EMG
1sttone
resp
onse
99
minus070
93minus163
33021
462
3EMG
15th
tone
resp
onse
99
minus026
36minus118
76066
032
3EMG
resp
onse-TTC
99
minus060
23minus152
63032
172
3Poo
ledstud
y(m
edianES
andCIby
hypo
thesis)
minus036
20minus128
59056
20
BDIindicates
BeckDep
ressionIn
ventoryBZDbenzodiazepine
CAPSC
linician-administeredPTSD
Sca
leEMGelectrom
yograp
hy
HAM-A
Ham
iltonRating
Sca
leforAnxiety
HAM-D
Ham
iltonRatingSca
leforDep
ressionH
Rh
eart
rateIESImpa
ctof
Event
Sca
leM
ISSM
ississippi
RatingSca
leforPTSDP
CLP
TSD
ChecklistPTSDp
osttra
umatic
stress
disorderP
TSSP
osttra
umatic
StressSyn
dromeSca
leS
Cskinconductan
ceS
TAIState-Tra
itAnx
iety
Inventory
TTCtrials
tohab
ituationcriterionVASvisu
alan
alog
scale
294 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
survived 1 or more of the following physical injuries(n=2979) life-threatening medical conditions(n=841) combat-related trauma (n=431) sexualtrauma (n=277) disaster exposure (n=203) andother traumas (n=47) The majority of the partic-ipants (approximately 67) survived a physicalinjury The mean age was approximately 44 yearsand approximately 38 were women
Qualitative Synthesis
Table 3 compares study designs outcomes andlevels of evidence
The studies supporting BZD efficacy for PTSDdemonstrate short-term improvement in sleep9 andanxiety10
The studies demonstrating BZD inefficacy forPTSD demonstrate no significant improvementcompared with controls for overall severity of PTSDsymptoms8ndash10121416ndash24 startle reflex81325 psycho-therapy outcomes81723 depression1012 overallwell-being10 sleep911 nightmares11 anxiety1216
aggression15ndash16 substance use16 and social functio-ning16
The studies showing BZDs being associated withworsened PTSD outcomes demonstrate worsenedoverall severity of PTSD symptoms8ndash9121416ndash23 psy-chotherapy outcomes81723 depression12 aggression15ndash16
substance use16 and anxiety16
Meta-analysis
Twelve studies (4 RCTs 2 nonrandomized 6observational) obtained data sufficient for estimat-ing ESs for PTSD-associated symptoms Individualoutcome measures and their associated ESs and95 CIs are shown in Table 4 Figure 2 summarizesthe ESs and CIs in forest plots by study forhypotheses H1 H2 and H3 Results are presented sothat a positive ES corresponds to BZDs improvingPTSD-associated outcomes and a negative ES cor-responds to BZDs worsening PTSD-associated out-comes The row labeled ldquoPOOLEDrdquo contains theestimated ES and 95 CI for the meta-analysisThe row labeled ldquoRCTs onlyrdquo illustrates the resultswhen restricted to only the 4 RCTs (denoted byldquoRCTrdquo to the right of the corresponding CI)
The estimated ES of BZDs on the development ofPTSD in trauma patients was minus03974 with a 95
CI of (minus06057 minus01891) Thus we reject H1 andconclude that BZDs increase the likelihood ofdeveloping PTSD when taken by trauma patients
The estimated ES of BZDs on PTSD-associatedsymptoms in PTSD patients was minus00839 with a95 CI of (minus03544 01866) Thus we have insuffi-cient evidence to reject H2 That is we have insuf-ficient evidence to conclude that BZDs alleviatePTSD-associated symptoms when taken by patientswho already have PTSD
The estimated ES of BZDs on PTSD-associatedsymptoms in trauma patients with and withoutPTSD (here ldquosymptomsrdquo includes all PTSD-relatedoutcomes including PTSD diagnosis for traumapatients who were not previously diagnosed withPTSD) was minus02798 with a 95 CI of (minus03981minus01616) Thus we reject H3 and conclude thatBZDs have an overall adverse impact in the pre-vention and treatment of PTSD When the analysiswas restricted only to the 4 RCTs the estimated ESof BZDs on PTSD-associated symptoms in traumapatients with and without PTSD was minus00422 witha 95 CI of (minus04505 03661) Thus the RCTs alonedo not provide sufficient evidence to reject H3 Onthe basis of the RCTs alone we conclude that thereis no evidence that BZDs alleviate PTSD-associatedsymptoms in PTSD patients or prevent the devel-opment of PTSD in trauma patients
DISCUSSION
Inefficacy (Level of Evidence A)
Before our study the ceiling for the level of evidencefor inefficacy was at B due to the lack of a con-firmatory meta-analysis However this meta-anal-ysis and at least 1 measure in every study that wasreviewed including all 4 RCTs of BZDs inPTSD8ndash11 suggest a lack of efficacy of BZDs forPTSD All PTSD-specific measures that wereused such as the Clinician-administered PTSDScale (CAPS) and the PTSD Checklist demon-strated that BZDs are at best not significantlydifferent from placebo or no BZD for PTSD BZDinefficacy is also endorsed by every availablePTSD practice guideline These findings are likelyexplained in part by the tolerance and cognitiveeffects associated with BZDs and also indicate thatBZDs appear to inadequately target PTSD patho-physiology
Journal of Psychiatric Practice Vol 21 No 4 July 2015 295
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

A major disadvantage of BZDs is that tolerancedevelops to hypnotic and myorelexant effects withindays to weeks and to anticonvulsant and anxiolyticeffects within weeks to months26ndash28 ThereforeBZDs are unlikely to be effective long-term hyp-notics or anxiolytics which is confirmed by severalgeneral studies of BZDs for sleep and anxiety2728
Tolerance to BZDs is a distinct problem in PTSDbecause most patients have symptoms that persistfor longer than 3 months29
BZDs may be ineffective for PTSD because ofamnestic effects that unintentionally target learninghow to cope with PTSD symptoms rather than trau-matic memories Although therapeutic effectsdecrease with tolerance cognitive effects (ie BZD-induced neurocognitive disorder) usually persist forattention memory and learning28 Cognitiveimpairments are more common with long-term useand high doses but they can also occur with short-term use and low doses2829 Unfortunately PTSD isa risk factor for BZD-induced neurocognitive dis-order as are conditions that are often comorbid withPTSD such as SUD neurocognitive disorders(including TBI) and psychotic bipolar and depres-sive disorders29
BZDs may be ineffective for PTSD because thepathophysiology of PTSD differs from that of theanxiety disorders for which BZDs have some effi-cacy Studies of flumazenil which have demon-strated that GABA-receptor antagonism inducespanic in patients with panic disorder but not inhealthy controls or patients with PTSD3031 suggestthat the pathophysiology underlying anxiety inPTSD is different from that in panic disorderdespite experiential similarities Researchers in 2 ofthe studies that were reviewed1325 concluded thatwhile locus ceruleus dysregulation is implicated inboth panic disorder and PTSD the amygdala andhippocampus are also implicated in PTSD anxietyShalev et al13 speculated that these structures maybe less responsive to BZDs than the locus ceruleusIn addition rather than targeting specific impli-cated structures BZDs indiscriminately depressglobal brain function (including structures such asthe prefrontal cortex that are already hypoactive inPTSD and which when functioning adequatelyallow for various cognitive processes and modu-lation of the amygdala) Therefore anxiety in PTSDmay be different than anxiety in other disordersand may require different treatments
Worsened Outcomes (Level of Evidence B)
Thirteen of the studies that were reviewed(including 2 RCTs) several practice guidelines andsome case reports suggest that BZDs have the riskof worsening the severity and prognosis of PTSDAll but 21024 of the 13 studies that used PTSD-specific measures (eg CAPS PTSD Checklist)demonstrated that BZDs are associated with worseoverall severity of symptoms when compared withplacebo or no BZD Potential biopsychosocialexplanations for BZDs worsening PTSD outcomesinclude discontinuation symptoms disruption ofnormal stress responses avoidance of cognitive andemotional processing of trauma and worsening ofunderlying PTSD pathophysiology (eg effects onthe hypothalamic-pituitary-adrenal [HPA] axis andon gamma-aminobutyric acid [GABA] glutamateand serotonin systems)
Discontinuation symptoms provide a model for howBZDs may worsen PTSD Chronic BZD use leadsto GABA-receptor desensitization and glutamatereceptor sensitization2632 When BZDs are suddenlydiscontinued in tolerant patients the patients expe-rience decreased inhibition from GABA and hyper-active excitation from glutamate causing withdrawalsymptoms that can mimic and worsen PTSD symp-toms (eg anxiety insomnia agitation autonomichyperactivity perceptual disturbances) Althoughless severe than withdrawal rebound symptomswhich are the inverse of the therapeutic effects ofBZDs and include worsened anxiety insomnia andirritability can occur shortly after discontinuationincluding between doses (especially with BZDs thathave a short half-life) Discontinuation symptoms arecommonly misinterpreted as a worsening of under-lying conditions while the iatrogenic contribution ofBZDs is overlooked272833 Although anxiety insom-nia and irritability may be temporarily exacerbatedduring withdrawal general studies of BZDs havedemonstrated that these symptoms are usually lesssevere after discontinuation than while takingBZDs2728 Both PTSD and BZD use have beenassociated with decreased GABA-receptor sensitivityand hyperactive glutamatergic activity34 BecauseBZDs can synergistically worsen underlying PTSDpathophysiology BZDs may actually exacerbatePTSD symptoms rather than improve them
One of the most consistent findings in this reviewwhich was supported by an RCT9 a nonrandomized-
296 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

controlled trial12 6 observational studies and a sys-tematic review of PTSD risk factors in patients on anintensive care unit35 is that BZD use after traumaincreases the risk of developing PTSD Only 2 studiesof trauma patients receiving BZDs2024 did not findan increased risk for PTSD although both suggestedinefficacy for PTSD prevention Those studies pro-viding sufficient data91219 suggest that the risk ofdeveloping PTSD is 2 to 5 times higher in groupsreceiving BZDs than in control groups BZDs likelydisrupt normal HPA axis stress responses andmemory-related processes Interfering with normalevolutionarily advantageous physiological responsesseems to increase vulnerability to subsequent stressand worsen outcomes in PTSD36 Three animalstudies43337 have demonstrated that BZDs increaseposttraumatic behaviors upon subsequent exposureto stress suggesting that the fear-sensitizing effectsof BZDs may act synergistically with trauma-relatedfear creating a generalized fear response to sub-sequent stressors (eg trauma-related cues) Despitetheoretical predictions that BZDs might preventthe development of PTSD after trauma (eg byinhibiting memory consolidation and preventingstress-induced changes in the noradrenergic sys-tem)12 no studies support BZDs for PTSD pre-vention and this review suggests that the short-termantistress effects of BZDs may actually increase thelong-term risk of PTSD In hindsight Gelpin et al12
acknowledged
The inhibitory effect of benzodiazepines onmemory acquisition is mostly anterogradeHence benzodiazepines do not alter memoryfor prior episodes and therefore should nothave affected traumatic memories whenadministered several days after the traumaMoreover recovery from trauma should not beequated with forgetting but rather adaptationreappraisal and learning Administered duringthe recovery phase benzodiazepines may infact interfere with such relearning hellip it may beargued that early treatment with benzodiaze-pines negatively affected survivors who mighthave otherwise recovered (p 393)
Three studies examined the effects of BZDs inpatients receiving psychotherapy Van Minnenet al23 found that daily BZD use was associatedwith worse outcomes and Rosen et al17 and
Rothbaum et al8 had mixed results (ie inefficacy orworsening depending on whether measures wererated by observers or patients) Rather than aug-menting psychotherapy BZDs seem to do nothingor to inhibit recovery Evidence-based trauma-focused psychotherapies (eg prolonged exposurecognitive processing therapy) require that patientsexperience and then master anxiety BZDs canimpair that experience by numbing emotionsdecreasing learning efficiency and inhibitingmemory processing of material learned in ther-apy1738 BZD-induced ldquoemotional anesthesiardquo26
directly interferes with the therapeutic effects ofexposure to anxiety-provoking stimuli (in psycho-therapy or the natural environment) by inhibitingfear activation a ldquonecessary condition for effectiveexposure therapyrdquo23 Several animal and humanstudies have demonstrated that BZDs interferewith fear extinction which is critical to exposuretherapy23940 For fear extinction to occur patientsmust emotionally and cognitively process theexperience of anxiety but BZDs allow patients toavoid these processes Some patients with PTSDuse distraction techniques to avoid internalreminders of trauma some rarely leave places ofcomfort to avoid external reminders and othersengage in reckless behaviors to ldquoescaperdquo29 BZDsmay provide another form of avoidance an attemptto self-medicate hyperarousal numb feelings sup-press memories and escape thoughts Overcomingavoidance behaviors is essential for successfultreatment but it is often the patientrsquos largestobstacle for recovery As Herman41 explains
The helpless person escapes from her situationnot by action in the real world but rather byaltering her state of consciousness hellip Trauma-tized people who cannot spontaneously disso-ciate may attempt to produce similar numbingeffects by using alcohol or narcotics hellipAlthough dissociative alterations in conscious-ness or even intoxication may be adaptive atthe moment of total helplessness they becomemaladaptive once the danger is past Becausethese altered states keep the traumatic experi-ence walled off from ordinary consciousnessthey prevent the integration necessary forhealing hellip They narrow and deplete thequality of life and ultimately perpetuate theeffects of the traumatic event (p 44)
Journal of Psychiatric Practice Vol 21 No 4 July 2015 297
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

Because an avoidant coping style is a poor prog-nostic factor for trauma-related disorders29 andBZDs are inherently avoidant (eg they inhibitcognitive processing and induce emotional numb-ing) BZDs may prolong and worsen PTSD
Two studies that were reviewed measuredaggression both of which found that BZDs wereassociated with aggression in some patients withPTSD1516 In general BZDs have been known tocause ldquoparadoxical reactionsrdquo (eg behavioral dis-inhibition impulsivity irritability aggression) inwhich patients may engage in uncharacteristicbehaviors such as assaults theft or sexual indis-cretions without any history of similar behaviorsbefore use or after discontinuation26324243 This istroublesome for patients with PTSD who oftenalready display irritability aggression and recklessbehavior Proposed mechanisms for paradoxicalreactions include rebound irritability inhibition ofserotonin regulation inhibition of emotional reac-tivity to aversive events that deters behavioralactivation and inhibition of cognitive processing inwhich causal associations are formed betweenbehaviors and their consequences3242 Risk factorsfor paradoxical reactions include several conditionscommon in PTSD SUD (especially alcohol use dis-order) neurocognitive disorders (especially TBI)anxiety disorders (comorbid to and includingPTSD) previous impulsivity and previous aggres-sion2151640 Unfortunately factors such as SUDTBI and comorbid anxiety disorders are also cor-related with increased prescription of BZDs forPTSD1239
Two of the studies that were reviewed measureddepression Braun et al10 found that BZDs wereineffective for depression in PTSD and Gelpinet al12 found that BZD use after trauma increasedthe risk of developing major depressive disorder Ingeneral BZDs have been known to cause or worsendysphoria and suicidality (ie BZD-induced depres-sive disorder) even in individuals without a historyof depression5394344 Unfortunately although thetherapeutic effects of BZDs decrease with tolerancedepression and impulsivity with high suicidal riskcommonly persist27 The mechanisms responsiblefor BZD-induced depression are a matter of spec-ulation but they may be similar to those causingparadoxical reactions (eg inhibition of serotoninregulation impulsivity) Regardless of the explan-ation the prospect of BZDs worsening depression is
of concern for patients with PTSD who commonlyhave negative moods and cognitions anhedoniasuicidality and comorbid depressive disorders
One study16 that was reviewed measured sub-stance use and the findings suggested that BZDsare associated with substance use in some patientswith PTSD Although BZDs are some of the morecommonly misused substances following traumadata about BZDs and SUD specific to patients withPTSD are limited In general 58 to 100 of thoseprescribed chronic BZDs become physicallydependent (especially with high doses and short-acting BZDs)2845 Risk factors for developing BZDuse disorder include preexisting or active SUDfamily history early onset of use medical avail-ability chronic medical conditions chronic painchronic anxiety chronic insomnia chronic dyspho-ria previous impulsivity and personalitydisorders227ndash2945 Unfortunately SUD and chronicanxiety are also correlated with increased pre-scriptions for BZDs for PTSD1239 Because BZD usedisorder develops in at least 50 of patients with ahistory of SUD who are prescribed BZDs manyauthors and organizations have declared BZDscontraindicated in all patients with histories ofSUD except during withdrawal2640 Although aprevious SUD may be the predominant risk factorwhen BZDs are continuously available drugreinforcement can lead to misuse by patients with-out any history of substance misuse46 ldquoTheirgreatest asset is also their greatest liability drugsthat work immediately tend to be addictiverdquo26 SUDoccurs in 21 to 43 of patients with PTSD47 andin as many as 50 of veterans with PTSD3 Thishigh comorbidity suggests that PTSD and SUD arefunctionally related a concept supported by severalstudies that indicate a pathway related to cortico-tropin-releasing hormone and norepinephrinewhereby PTSD precedes SUD47 The high risk ofSUD in patients with PTSD is one reason why somany authors and organizations recommendagainst treating PTSD with BZDs
Efficacy (Level of Evidence D)
A few anecdotal reports and parts of 2 RCTs supportshort-term symptomatic treatment but there is noavailable expert consensus endorsing BZDs for PTSDtreatment so the ceiling for the level of evidence is D
298 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

Although both the studies supporting efficacy areRCTs910 they had mixed findings (ie they also dem-onstrated inefficacy or worsening of PTSD) and at bestthey only supported short-term use for some PTSD-associated symptoms For example Mellman et al9
found that temazepam initially improved sleep but thatit was not significantly different from placebo after thefirst night and worsened overall PTSD severity in thelong term Braun et al10 found short-term improve-ment in anxiety (described as a ldquoslight reductionrdquoldquomodestrdquo and ldquodisappointingrdquo) but no significantdifference from placebo in any other measure (overallseverity of PTSD symptoms depression overall well-being) Other studies that were reviewed demon-strated inefficacy for sleep11 and anxiety1216 Only 1other nonanecdotal study supported efficacy Leeet al48 found that lorazepam improved intrusivesymptoms but the RCT was excluded from thisreview because the participants experienced an arti-ficial ldquotraumardquo by video and were assessed only 1 daylater (less than the 1month threshold for PTSD) Thestudy by Lee and colleagues also found no significantimprovement in anxiety depression or arousal Theauthors suggested that lorazepam is ldquoatypicalrdquo anddiffers from other BZDs such as diazepam that cantrigger intrusion Even if BZDs improve PTSD-asso-ciated symptoms on a short-term basis the benefitsare unlikely to last due to tolerance
There is no evidence besides anecdotal reports thatsupports the use of BZDs for the treatment of PTSDcore symptoms (ie intrusion avoidance hyper-arousal) or for long-term symptomatic treatment ofPTSD Many researchers have criticized the frequentcitation of case reports to justify the use of BZDs totreat patients with PTSD ldquodespite risks and lack ofstudiesrdquo11 These case reports are mostly retro-spective and based on subjective reports Patientsrsquoreports of their experiences while taking BZDs areinherently unreliable as 1 case series49 concedes
It is possible that patientsrsquo memories ofsubjective sensations while intoxicated do notcorrespond to their actual affective state Forinstance many people report euphoria after thefact with alcohol intoxication even though atthe time of intoxication they were tearful andagitated (p 374)
In the case of sleep BZDs are often credited (likealcohol) for improving sleep quality but they actually
promote sleep induction while inhibiting the deepestmost restorative stages of sleep2845 At times sub-jective reports of improvement with BZDs may reflectdistortions due to cognitive impairments or they maybe due to patients mistaking the temporary relief ofdiscontinuation symptoms for improvement of base-line symptoms or mistaking sedation for genuineimprovement of their condition
The findings of Mellman et al50 highlight theimportance of caution when extrapolating the resultsof anecdotal evidence to clinical practice In this pro-spective case series of 4 recent trauma patients withinsomnia the researchers found that short-termtemazepam was associated with improved PTSDsymptoms however this was a pilot study for Mell-man et al9 the RCT that found that short-termtemazepam increases the risk of developing PTSD Inaddition ldquobecause benzodiazepines reduce anxietywithout addressing the underlying PTSD cliniciansmay incorrectly believe the patient has improved thusdelaying definitive PTSD carerdquo40 BZDs ldquoneed to becarefully considered taking into account their poten-tial harm to the spontaneous recovery process and thetrajectory of PTSD and not only judging themaccording to their immediate (comforting) effectsrdquo36
Limitations
There was little consistency in participants diagnosticmethod trauma type recency severity interventionfollow-up or outcome measures among the studiesselected for review For example the studies con-ducted in intensive care units examined only life-threatening medical conditions18ndash2022 whereasMcGhee et al24 examined only combat-related PTSDNine articles studied the use of any BZD whereasothers studied specific agents Follow-up ranged from2 weeks to 4 years Seven studies used multipleassessment instruments and no instrument was usedin more than 4 studies These inconsistenciesresulted in heterogeneity among the studies How-ever random-effects models were used in the meta-analyses to account for this heterogeneity resultingin wider CIs for ESs than would have resulted if afixed-effects approach had been used
Our meta-analytic approach also had some limi-tations In particular publication bias if presentwould result in an underreporting of nonsignificantstudies However in the present context there is
Journal of Psychiatric Practice Vol 21 No 4 July 2015 299
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

less reason for studies with nonsignificant resultsnot to have been published as they would havesupported the view that BZDs are not harmful Anadditional potential limitation is that the meta-analytic method chosen implicitly assumes thatthere is no systematic bias across these studiesfavoring positive associations
Although there is evidence that BZDs can worsenPTSD-associated symptoms the authors cannotexclude the likelihood that those patients who weretreated with BZDs in the observational studies thatwere reviewed were more severely affected and hadworse prognoses For example the results of the
intensive care unit studies were likely confounded byindication (eg patients who are more delirious agi-tated or anxious in the ICU may be more likely toreceive higher BZD doses) Therefore BZD use may bean indicator rather than a cause of poorer prognosisHowever such confounding factors were eliminated ina study by Treggiari et al51 a RCT that found thatlower sedation in critically ill patients is associatedwith fewer PTSD symptoms (this study was excludedfrom this review because it did not distinguish BZDsfrom other sedatives) Likewise similar confoundingfactors were eliminated in the reviewed RCTs thatdemonstrated worsening of PTSD89
FIGURE 2 AndashC Summary of effect sizes (boxes) and confidence intervals (horizontal lines) ofreviewed studies of benzodiazepines (BZDs) in posttraumatic stress disorder (PTSD)
A H1 BZDs are not associated with the development of PTSD in trauma patients B H2 BZDs are not associated with PTSD-associated symptoms in patients with PTSD C H3 BZDs are not associated with PTSD-associated symptoms in trauma patientswith and without PTSD
300 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

The greatest limitation of this review was thelimited number of RCTs available Of the 4 placebo-controlled trials only 2 were double-blind810
whereas 111 was single-blind and another was open-label9 Nevertheless the authors believed it wasworthwhile to compile the data from all of theavailable studies given the widespread use of BZDsfor PTSD and disagreements and misconceptionsamong clinicians about this practice When themeta-analysis was limited only to the RCTs theresults were inconclusive due to the small samplesizes of those RCTs and the great amount of het-erogeneity among the studies with 2 showing non-significant negative effects and 2 showing non-significant positive effects Although one mightargue that only RCTs should be considered forinclusion in a rigorous review in light of the limitednumber of studies of BZDs in PTSD we elected touse more expansive inclusion criteria to create acomprehensive review of the available literatureand to stimulate clinical thought and furtherresearch Further studies are recommended espe-cially randomized placebo-controlled trials withextended follow-up
CONCLUSIONS
Although BZDs have been in use since 1960 andtrauma survivors have always existed hardknowledge is scanty Nevertheless based on ourmeta-analysis and qualitative synthesis we canconclude that BZDs are more likely to be ineffectivethan effective for the treatment or prevention ofPTSD and that risks tend to outweigh potentialshort-term benefits Consistent evidence supports alack of efficacy especially for PTSD core symptomspsychotherapy augmentation and depressionThere is also suggestive evidence that BZDs mayworsen outcomes with BZDs being correlated withworse overall severity of PTSD symptomsincreased risk of trauma patients developing PTSDand worse psychotherapy outcomes However moredouble-blind placebo-controlled trials are neededbefore it can be concluded that BZDs consistentlyworsen PTSD There is little evidence for anythingexcept the most transient efficacy which is limitedto a few symptoms and this is outweighed by betterevidence for inefficacy and potential risks For thesereasons and others BZDs should be consideredrelatively contraindicated in trauma patients
Most studies specific to BZDs in PTSD are small andfew are RCTs However taken together and in com-bination with general BZD studies they raise enoughquestions about potential harms that providers shoulduse considerable caution when continuing BZD pre-scriptions and would be safer to avoid starting themaltogether in PTSD patients Some of these potentialproblems are general concerns about the medicationclass (eg cognitive effects dependence misuse) andothers are specific to the diagnosis (eg adverse effectssynergistically worsening PTSD symptoms inhibitingpsychotherapy promoting avoidance) Although BZDsmight be effective if they were to selectively inhibit thestress and anxiety centers of the brain that are oftenhyperactive in PTSD (eg amygdala HPA axis) theyindiscriminately target the entire brain includingthose areas that are already hypoactive in PTSDincluding the cognitive and memory centers (eg pre-frontal cortex hippocampus) and serotonergic circuits(implicated in PTSD anxiety depression suicidalityimpulsivity aggression) Although it may be temptingto treat PTSD-associated symptoms with BZDs theyare best avoided due to evidence of long-term risksoutweighing evidence of any short-term benefits andthe difficulty of discontinuing BZDs once startedWhen patients with PTSD are already taking BZDsproviders should evaluate whether the treatment isactually improving the patientsrsquo functioning or if thereare anymdashoften subtlemdashiatrogenic effects on the courseof their condition After weighing risks and benefitssome providers will choose to continue BZDs somewill unilaterally discontinue or change medicationsand some will work through the stages of change tohelp patients transition toward evidence-based treat-ments Regardless recovery from PTSD should denoteimproved functioning (eg healthy relationshipsemployment) not simply sedation
Although there is little evidence of benefits asso-ciated with BZDs in PTSD substantial evidencesupports the benefits associated with other treat-ments A myriad of evidence-based treatments forPTSD exist (eg psychotherapy serotonergic anti-depressants adrenergic inhibitors)33840 all ofwhich should be exhausted before BZDs are con-sidered For years sedatives were the only thing wehad in our armamentarium for PTSD Now wehave many more tools and our patientsmdashwhethersurvivors of assault combat or any other traumamdashdeserve those treatments that have been proven tobe safer and more effective than BZDs
Journal of Psychiatric Practice Vol 21 No 4 July 2015 301
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
REFERENCES
1 Harpaz-Rotem I Rosenheck RA Mohamed S et alPharmacologic treatment of posttraumatic stress disor-der among privately insured Americans Psychiatr Serv2008581184ndash1190
2 Lund BC Bernardy NC Vaughan-Sarrazin M et alPatient and facility characteristics associated withbenzodiazepine prescribing for veterans with PTSDPsychiatr Serv 201364149ndash155
3 Veterans Affairs and Department of Defense VADoDclinical practice guideline for management of post-trau-matic stress 2010 Available at httpwwwhealthqualityvagovguidelinesMHptsdcpg_PTSD-FULL-201011612pdf Accessed April 8 2013
4 Matar MA Zohar J Kaplan Z et al Alprazolam treat-ment immediately after stress exposure interferes withthe normal HPA-stress response and increases vulner-ability to subsequent stress in an animal model of PTSDEur Neuropsychopharmacol 200919283ndash295
5 Foa EB Keane TM Friedman MJ et al EffectiveTreatments for PTSD Practice Guidelines From theInternational Society for Traumatic Stress Studies 2nded New York NY Guilford 2009566
6 US Department of Health and Human Services ClinicalPractice Guideline No 5 Depression in Primary Care Vol2 Treatment of Major Depression Rockville MDAHCPR Publications 199371ndash123
7 Moher D Liberati A Tetzlaff J et al Preferred reportingitems for systematic reviews and meta-analyses thePRISMA statement PLoS Med 20096e1000097
8 Rothbaum OR Price M Jovanovic T et al A randomizeddouble-blind evaluation of D-cycloserine or alprazolamcombined with virtual reality exposure therapy forposttraumatic stress disorder in Iraq and Afghanistanwar veterans Am J Psychiatry 2014171640ndash648
9 Mellman TA Bustamante V David D et al Hypnoticmedication in the aftermath of trauma J Clin Psychiatry2002631183ndash1184
10 Braun P Greenberg D Dasberg H et al Core symptomsof posttraumatic stress disorder unimproved by alprazo-lam treatment J Clin Psychiatry 199051236ndash238
11 Cates ME Bishop MH Davis LL et al Clonazepam fortreatment of sleep disturbances associated with combat-related posttraumatic stress disorder Ann Pharmac-other 2004381395ndash1399
12 Gelpin E Bonne O Peri T et al Treatment of recenttrauma survivors with benzodiazepines a prospectivestudy J Clin Psychiatry 199657390ndash394
13 Shalev AY Bloch M Peri T et al Alprazolam reducesresponse to loud tones in panic disorder but not inposttraumatic stress disorder Biol Psychiatry 19984464ndash68
14 Zatzick DF Rivara FP Nathens AB et al A nationwide USstudy of post-traumatic stress after hospitalization forphysical injury Psychol Med 2007371469ndash1480
15 Shin HJ Rosen CS Greenbaum MA et al Longitudinalcorrelates of aggressive behavior in help-seeking USveterans with PTSD J Trauma Stress 201225649ndash656
16 Kosten TR Fontana A Sernyak MJ et al Benzodiaze-pine use in posttraumatic stress disorder among veteranswith substance abuse J Nerv Ment Dis 2000188454ndash459
17 Rosen CS Greenbaum MA Schnurr PP et al Dobenzodiazepines reduce the effectiveness of exposure
therapy for posttraumatic stress disorder J Clin Psy-chiatry 2013741241ndash1248
18 Jones C Backman C Capuzzo M et al Precipitants ofpost-traumatic stress disorder following intensive care ahypothesis generating study of diversity in care Inten-sive Care Med 200733978ndash985
19 Samuelson KAM Lundberg D Fridlund B Stressfulmemories and psychological distress in adult mechan-ically ventilated intensive care patientsmdasha 2 monthfollow-up study Acta Anaesthesiol Scand 200751671ndash678
20 Bienvenu OJ Gellar J Althouse BM et al Post-traumatic stress disorders symptoms after acute lunginjury a 2-year prospective longitudinal study PsycholMed 2013432657ndash2671
21 Baranyi A Krauseneck T Rothenhausler HB Posttrau-matic stress symptoms after solid-organ transplantationpreoperative risk factors and the impact on health-related quality of life and life satisfaction Health QualLife Outcomes 201311111
22 Girard TD Shintani AK Jackson JC et al Risk factorsfor post-traumatic stress disorder symptoms followingcritical illness requiring mechanical ventilation a pro-spective cohort study Crit Care 200711R28
23 Van Minnen A Arntz A Keijsers GPJ Prolongedexposure in patients with chronic PTSD predictors oftreatment outcome and dropout Behav Res Ther200240439ndash457
24 McGhee LL Maani CV Garza TH et al The relationshipof intravenous midazolam and posttraumatic stressdisorder development in burned soldiers J Trauma200966(suppl)S186ndashS190
25 Shalev AY Rogel-Fuchs Y Auditory startle reflex in post-traumatic stress disorder patients treated with clonaze-pam Isr J Psychiatry Relat Sci 1992291ndash6
26 Longo LP Johnson B Addiction part I Benzodiazepinesmdashside effects abuse risk and alternatives Am FamPhysician 2000612121ndash2128
27 Michelini S Cassano GB Frare F et al Long-term use ofbenzodiazepines tolerance dependence and clinical prob-lems in anxiety and mood disorders Pharmacopsychiatry199629127ndash134
28 Ashton H The diagnosis and management of benzodiaze-pine dependence Curr Opin Psychiatry 200518249ndash255
29 American Psychiatric Association Diagnostic and Statis-tical Manual of Mental Disorders Fifth ed Arlington VAAmerican Psychiatric Association 2013265ndash290 550ndash560
30 Coupland NJ Lillywhite A Bell CE et al A pilotcontrolled study of the effects of flumazenil in posttrau-matic stress disorder Biol Psychiatry 199741988ndash990
31 Randall PK Bremner JD Krystal JH et al Effects of thebenzodiazepine antagonist flumazenil in PTSD BiolPsychiatry 199538319ndash324
32 Tasman A Kay J Lieberman JA Psychiatry 3rd ed Vol 1Chichester UK John Wiley amp Sons 20081186ndash12002603ndash2615
33 Li S Murakami Y Wing M et al The effects of chronicvalproate and diazepam in a mouse model of posttrau-matic stress disorder Pharmacol Biochem Behav200685324ndash331
34 Geuze E van Berckel BNM Lammertsma AA et alReduced GABAA benzodiazepine receptor binding inveterans with post-traumatic stress disorder Mol Psy-chiatry 20081374ndash83
35 Davydow DS Gifford JM Desai SV et al Posttraumaticstress disorder in general intensive care unit survivors
302 July 2015 Journal of Psychiatric Practice Vol 21 No 4
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved
a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved

a systematic review Gen Hosp Psychiatry 200830421ndash434
36 Zohar J Juven-Wetzler A Sonnino R et al New insightsinto secondary prevention in post-traumatic stressdisorder Dialogues Clin Neurosci 201113301ndash309
37 Hebert MA Potegal M Moore T et al Diazepamenhances conditioned defeat in hamsters PharmacolBiochem Behav 199655405ndash413
38 Berger W Mendlowicz MV Marques-Portella C et alPharmacologic alternatives to antidepressants in post-traumatic stress disorder a systematic review ProgNeuropsychopharmacol Biol Psychiatry 200933169ndash180
39 Hawkins EJ Malte CA Imel ZE et al Prevalence andtrends of benzodiazepine use among Veterans Affairspatients with posttraumatic stress disorder 2003ndash2010Drug Alcohol Depend 2012124154ndash161
40 Jeffreys M Capehart B Friedman MJ Pharmacotherapyfor posttraumatic stress disorder review with clinicalapplications J Rehabil Res Dev 201249703ndash715
41 Herman J Trauma and Recovery The Aftermath ofViolencemdashFrom Domestic Abuse to Political Terror NewYork NY Basic Books 199244ndash45
42 Bond AJ Drug-induced behavioural disinhibition inci-dence mechanisms and therapeutic implications CNSDrugs 1998941ndash57
43 PDR Network Physiciansrsquo Desk Reference 2014 Avail-able at httpwwwpdrnet Accessed March 5 2014)
44 Baldwin DS Anderson IM Nutt DJ et al Evidence-based guidelines for the pharmacological treatment ofanxiety disorders recommendations from the BritishAssociation for Psychopharmacology J Psychopharmacol200519567ndash596
45 Pary R Lewis S Prescribing benzodiazepines in clinicalpractice Resid Staff Physician 2008548ndash17
46 Griffiths RR Weerts EM Benzodiazepine self-adminis-tration in humans and laboratory animalsmdashimplicationsfor problems of long-term use and abuse Psychopharma-cology 19971341ndash37
47 Jacobsen LK Southwick SM Kosten TR Substance usedisorders in patients with posttraumatic stress disordera review of the literature Am J Psychiatry 20011581184ndash1190
48 Lee HS Lee HP Lee SK et al Anti-intrusion effect oflorazepam an experimental study Psychiatry Investig201310273ndash280
49 Bremner JD Southwick SM Darnell A et al ChronicPTSD in Vietnam combat veterans course of illness andsubstance abuse Am J Psychiatry 1996153369ndash375
50 Mellman TA Byers PM Augenstein JS Pilot evaluationof hypnotic medication during acute traumatic stressresponse J Trauma Stress 199811563ndash569
51 Treggiari MM Romand JA Yanez ND et al Randomizedtrial of light versus deep sedation on mental health aftercritical illness Crit Care Med 2009372427ndash2534
Journal of Psychiatric Practice Vol 21 No 4 July 2015 303
BENZODIAZEPINES FOR PTSD
Copyright copy 2015 Wolters Kluwer Health Inc All rights reserved