what is raynaud's, what is scleroderma?
TRANSCRIPT
What is Raynaud’sWhat is
Scleroderma?Neil McHugh, University of Bath and
Royal National Hospital for Rheumatic DiseasesManchester June 2015
Raynaud’s disease
• De l'asphyxie locale et de la gangrène symétrique des extrémités.
• Discrete episodes of change in colour, of the vasospastic type, induced by cold exposure or emotional stress
• Bilateral• Normal pulsations in palpable
stressDoctoral thesis, published
February 25, 1862.Maurice Raynaud 1834-1881
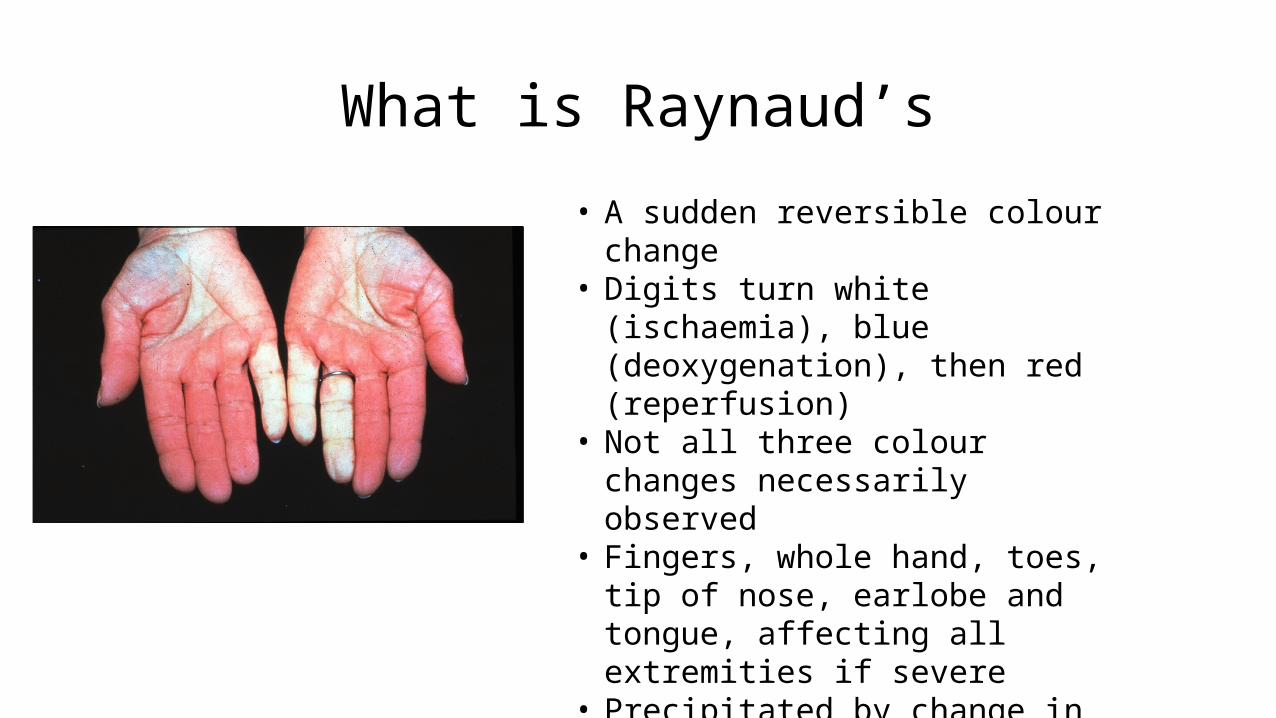
What is Raynaud’s
• A sudden reversible colour change• Digits turn white (ischaemia), blue
(deoxygenation), then red (reperfusion)• Not all three colour changes necessarily
observed• Fingers, whole hand, toes, tip of nose,
earlobe and tongue, affecting all extremities if severe
• Precipitated by change in temperature or emotional stress
• Associated with numbness, pain and paraesthesia

Raynaud’s phenomenon (disease, syndrome)
• Primary Raynaud’s phenomenon• A functional problem affecting small
blood vessels• No evidence of an underlying disease
process• Common affecting 15% female
population• 10 million in UK have Raynaud’s• ‘Benign’ – does not mean insignificant!
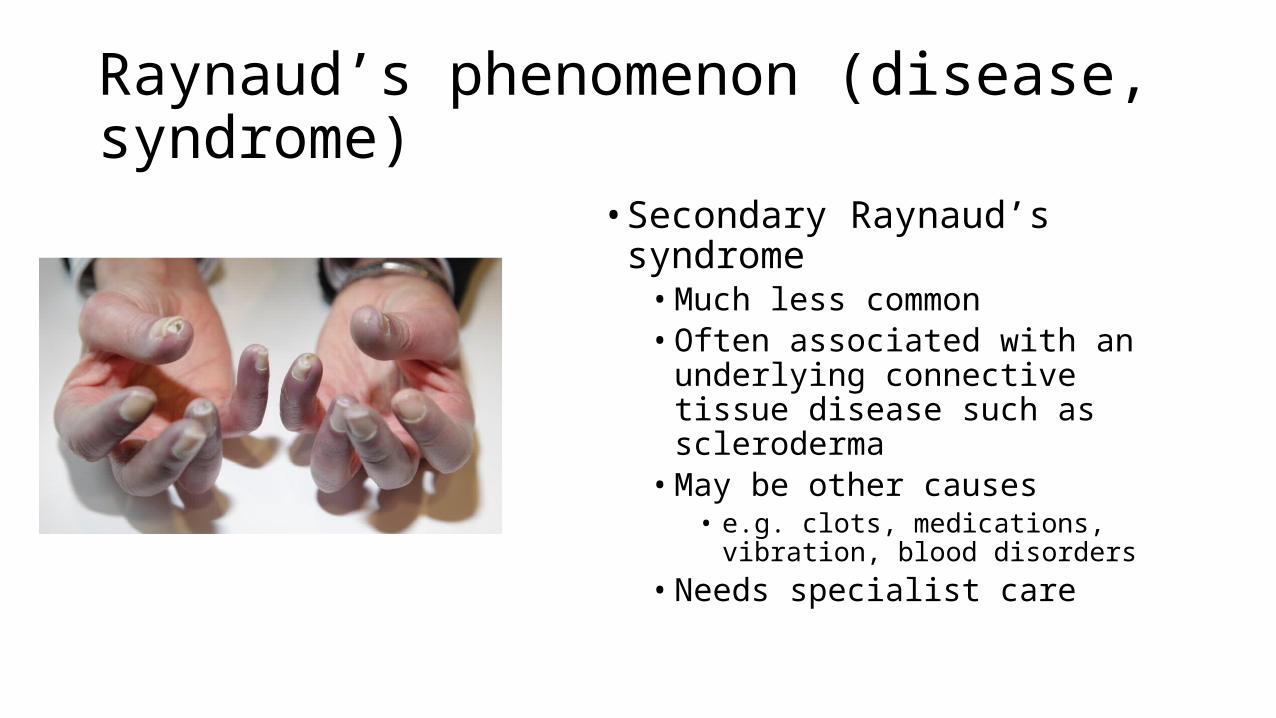
Raynaud’s phenomenon (disease, syndrome)
• Secondary Raynaud’s syndrome• Much less common• Often associated with an underlying
connective tissue disease such as scleroderma
• May be other causes• e.g. clots, medications, vibration, blood
disorders• Needs specialist care

Helpful diagnostic tests
Infrared thermography Nailfold capillaroscopy
Blood tests
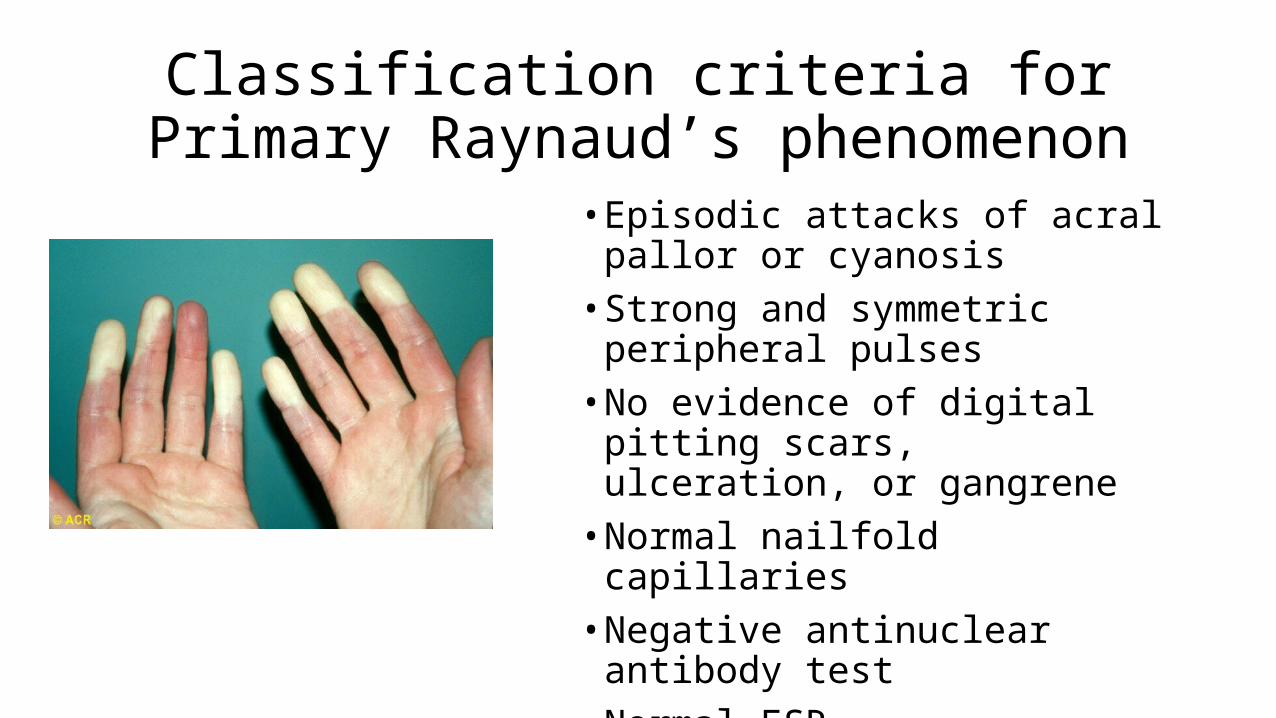
Classification criteria for Primary Raynaud’s phenomenon
• Episodic attacks of acral pallor or cyanosis
• Strong and symmetric peripheral pulses
• No evidence of digital pitting scars, ulceration, or gangrene
• Normal nailfold capillaries• Negative antinuclear antibody test• Normal ESR

Treatment of Raynaud’s phenomenon
• Vasodilators• Calcium channel blockers• Nitrate patches• Serotonin inhibitors• Serotonin re-uptake inhibitors• PDE5 inhibitors• a2-adrenergic blockers
• Vasodilatation and remodelling• ACE inhibitors• Angiotensin receptor blockers• Prostocyclin analogues• Endothelin receptor blockers
• Anti-oxidants• Vitamin E, Vitamin C• Probucol
Stop smokingKeep warmAsk
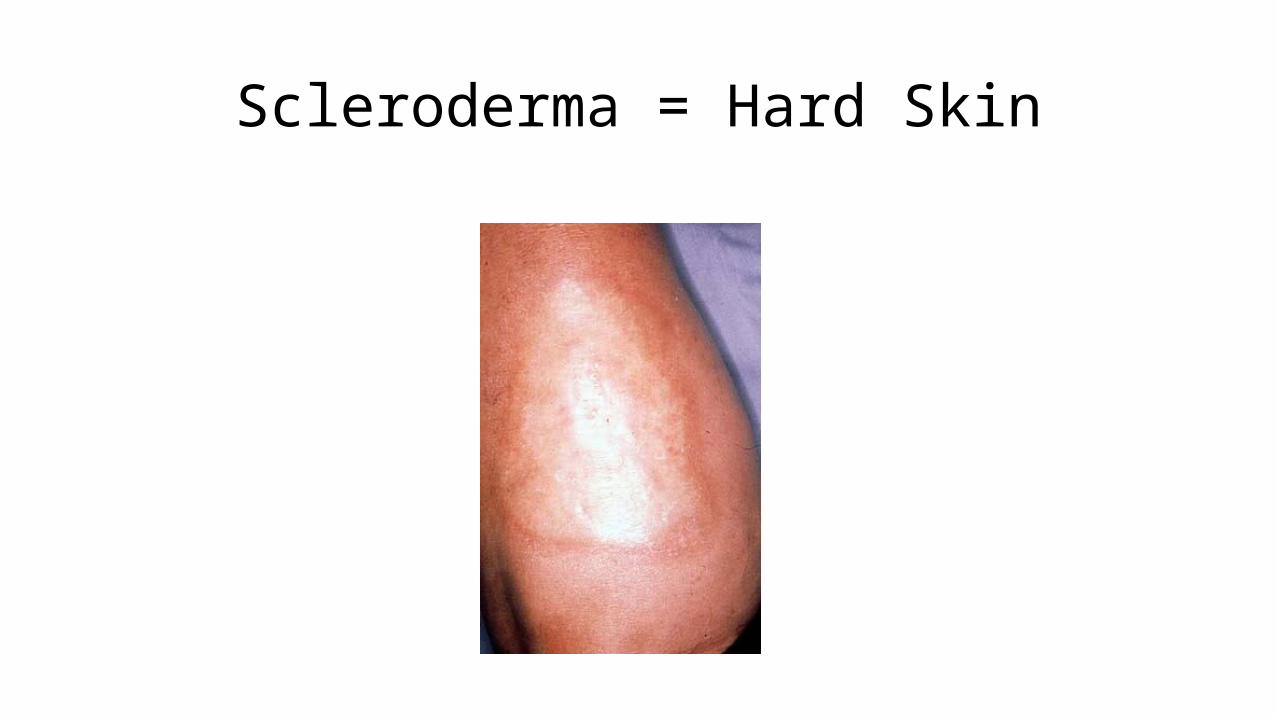
Scleroderma = Hard Skin

Scleroderma spectrum disorders
• Raynaud’s phenomenon• Primary Raynaud’s phenomenon• Autoimmune Raynaud’s phenomenon
• Systemic sclerosis (scleroderma)• Limited cutaneous systemic sclerosis• Diffuse cutaneous systemic sclerosis• Systemic sclerosis sine scleroderma• Scleroderma overlap syndromes
• Localised scleroderma• Morphea
• Localised• Generalised
• Linear scleroderma• En coup de sabre
Digital ulceration

Limited cutaneous systemic sclerosis
• Formerly called CREST• Calcinosis• Raynaud’s• oEsophageal disease
• e.g.relux, heartburn• Sclerodactyly• Telangiectasia
• 80 % of scleroderma cases• Frequent Digital Ulceration• Monitor for Pulmonary
Hypertension
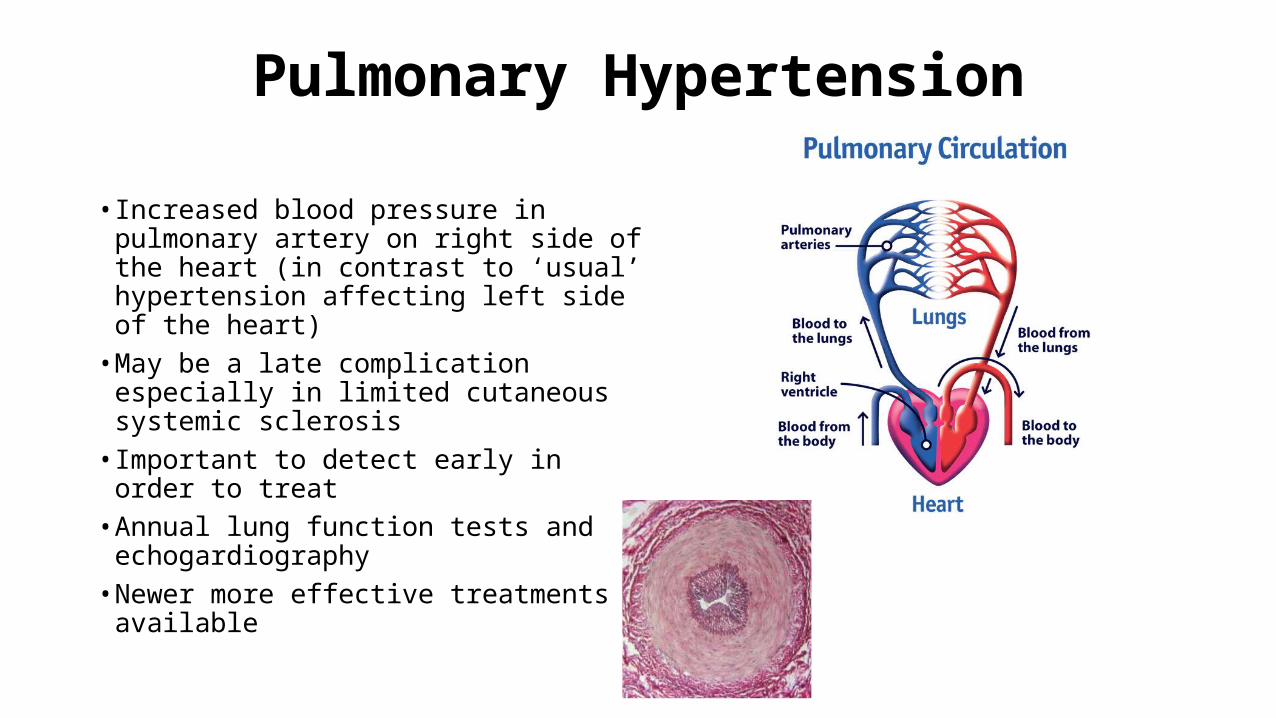
Pulmonary Hypertension
• Increased blood pressure in pulmonary artery on right side of the heart (in contrast to ‘usual’ hypertension affecting left side of the heart)
• May be a late complication especially in limited cutaneous systemic sclerosis
• Important to detect early in order to treat
• Annual lung function tests and echogardiography
• Newer more effective treatments available
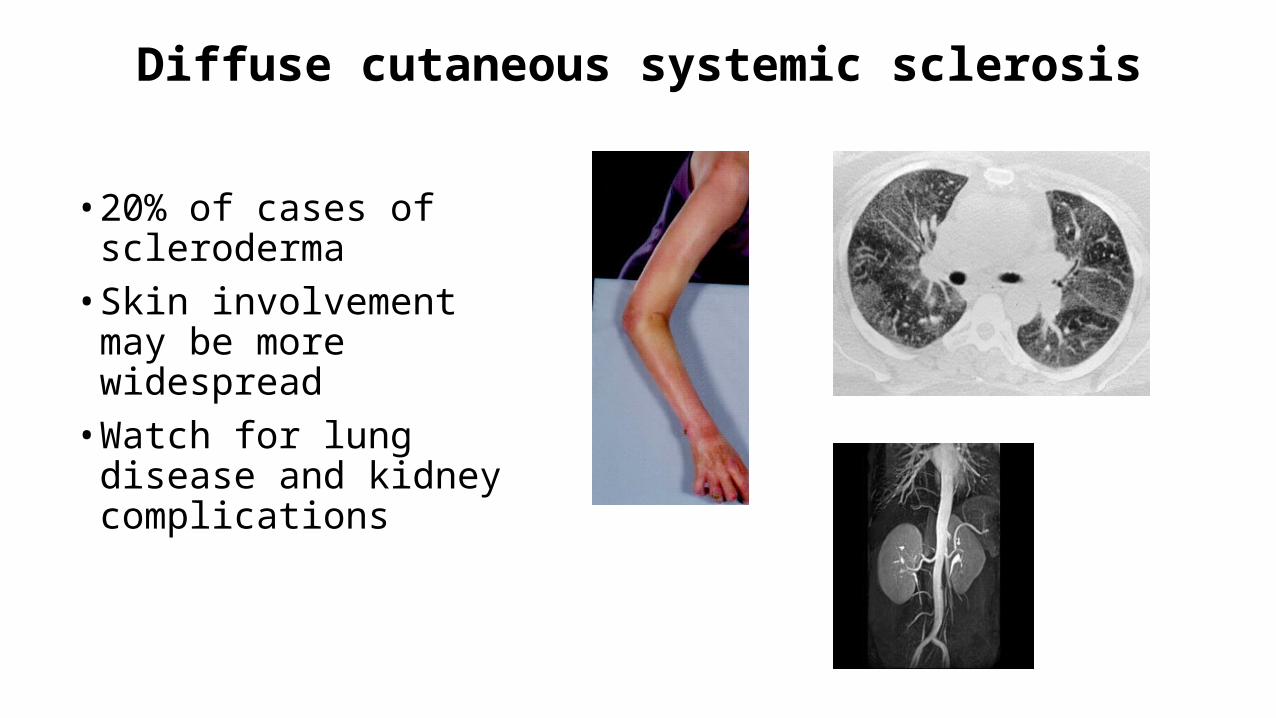
Diffuse cutaneous systemic sclerosis
• 20% of cases of scleroderma• Skin involvement may be
more widespread• Watch for lung disease and
kidney complications
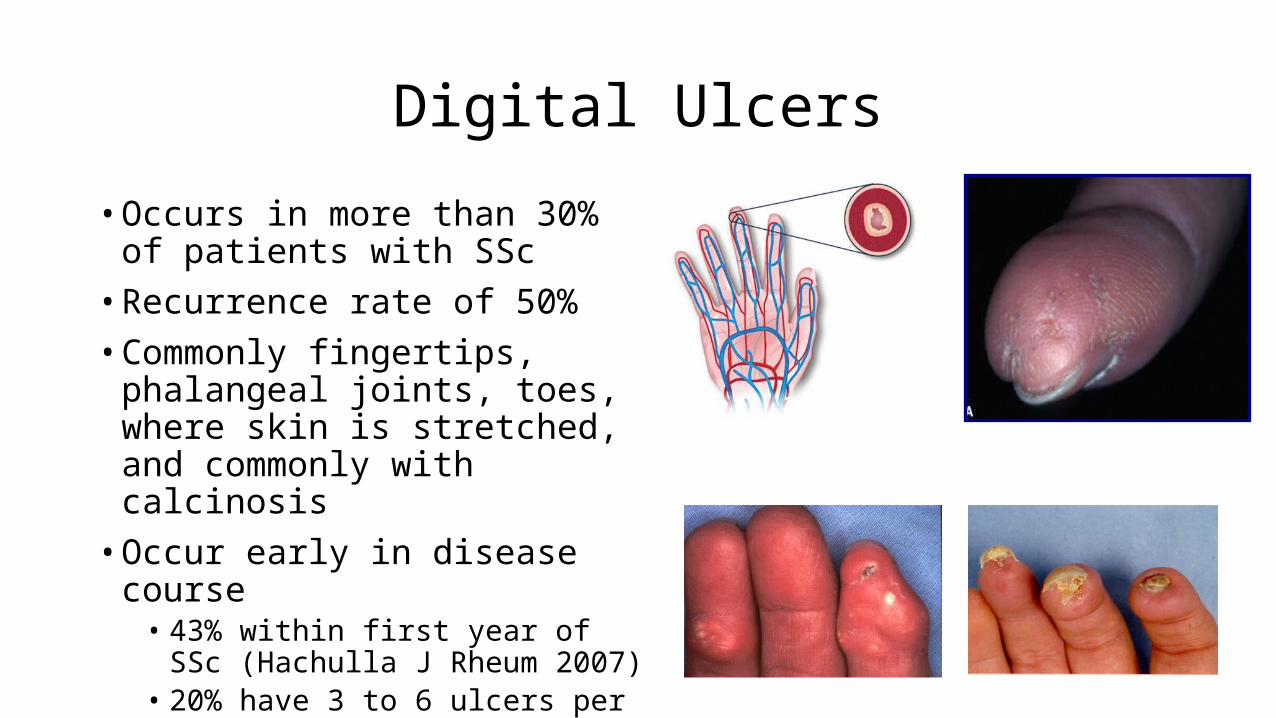
Digital Ulcers
• Occurs in more than 30% of patients with SSc
• Recurrence rate of 50%• Commonly fingertips, phalangeal
joints, toes, where skin is stretched, and commonly with calcinosis
• Occur early in disease course• 43% within first year of SSc (Hachulla J
Rheum 2007)• 20% have 3 to 6 ulcers per episode
Digital ulcer – burden to patient• Interfere with activities of daily living
• Restrict an individual's capabilities• Impair hand function• Impact on work opportunities and family commitments
• Increased disability, more pain and reduced QoL compared with those without digital ulcers (Merkel 2002)
• Can be exquisitely painful with prolonged healing time
Epidemiology of scleroderma
• Prevalance 10-300 per million• About 8000 cases in UK
• Female predominance (especially anti-centromere positive)• Ethnic differences in subgroups• Enviromental factors
• e.g. silica, bleomycin,vinyl chloride, organic solvents, epoxy resins
• Genetic factors• e.g. MHC
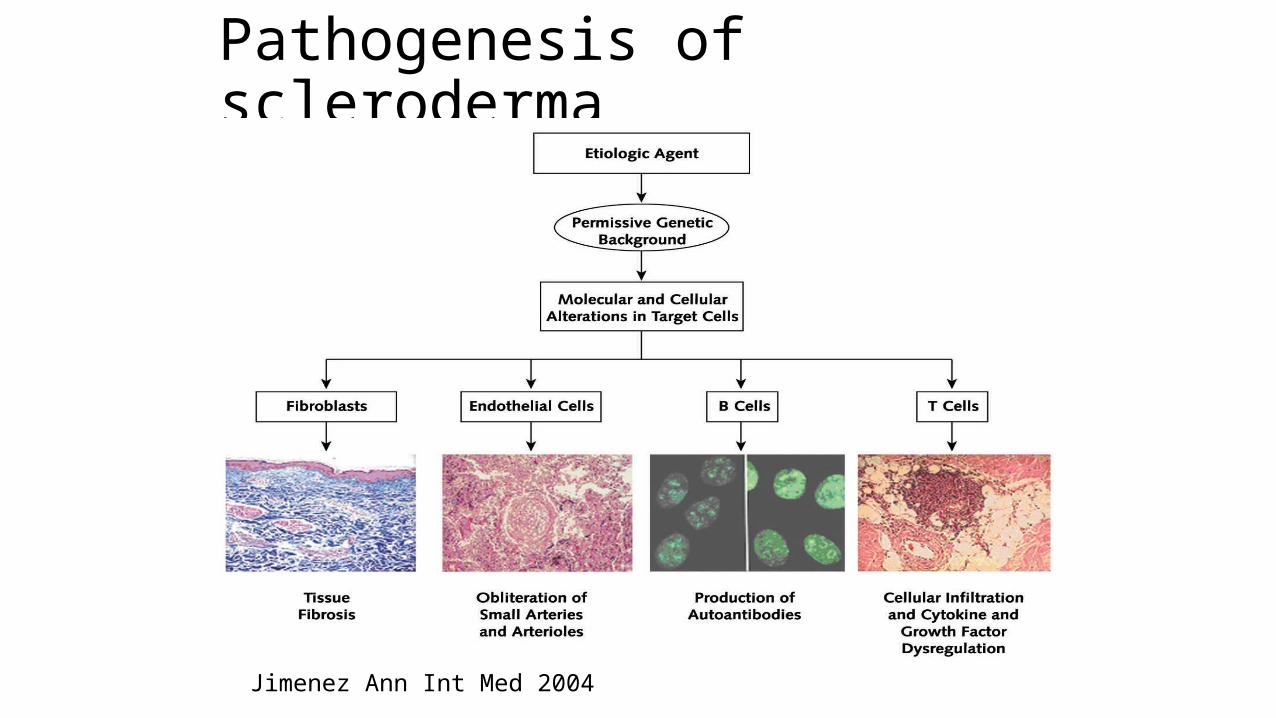
Pathogenesis of scleroderma
Jimenez Ann Int Med 2004

Helpful diagnostic tests for scleroderma
Infrared thermography Nailfold capillaroscopy
Blood tests
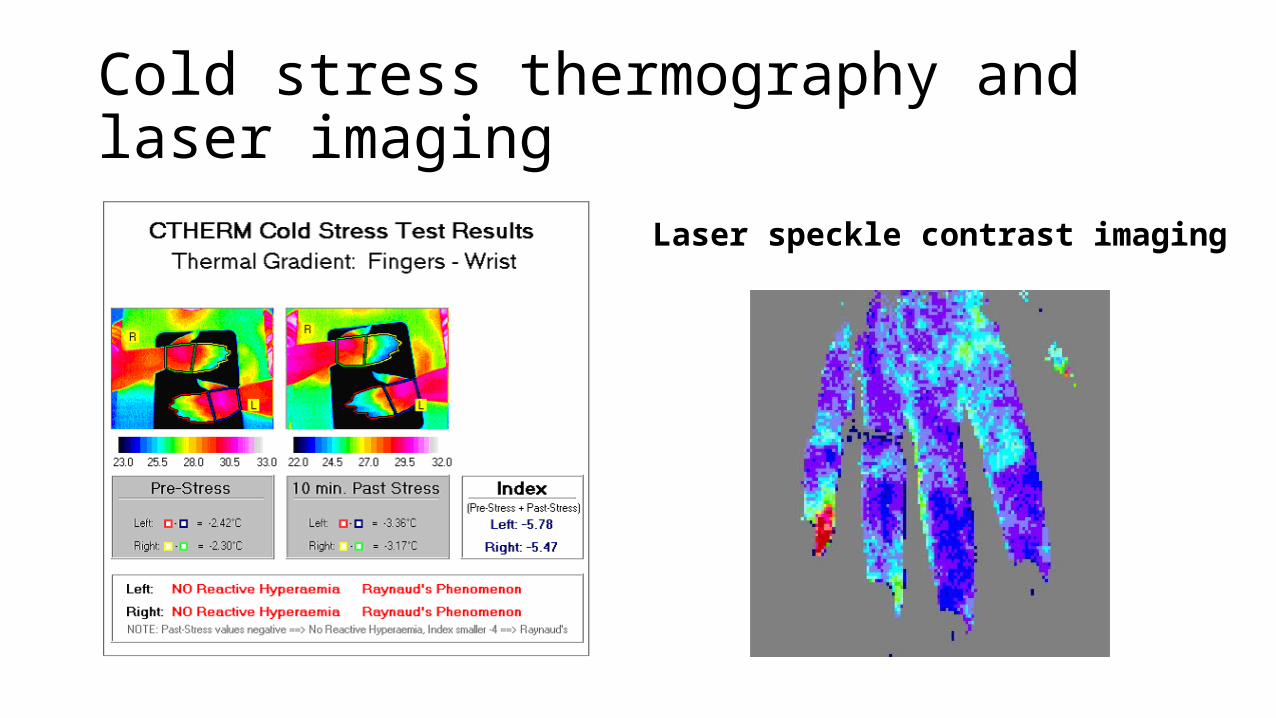
Cold stress thermography and laser imaging
Laser speckle contrast imaging

Nailfold capillaroscopy
Earlypattern
Activepattern
Latepattern
Blood tests
‘It’s all in the blood’
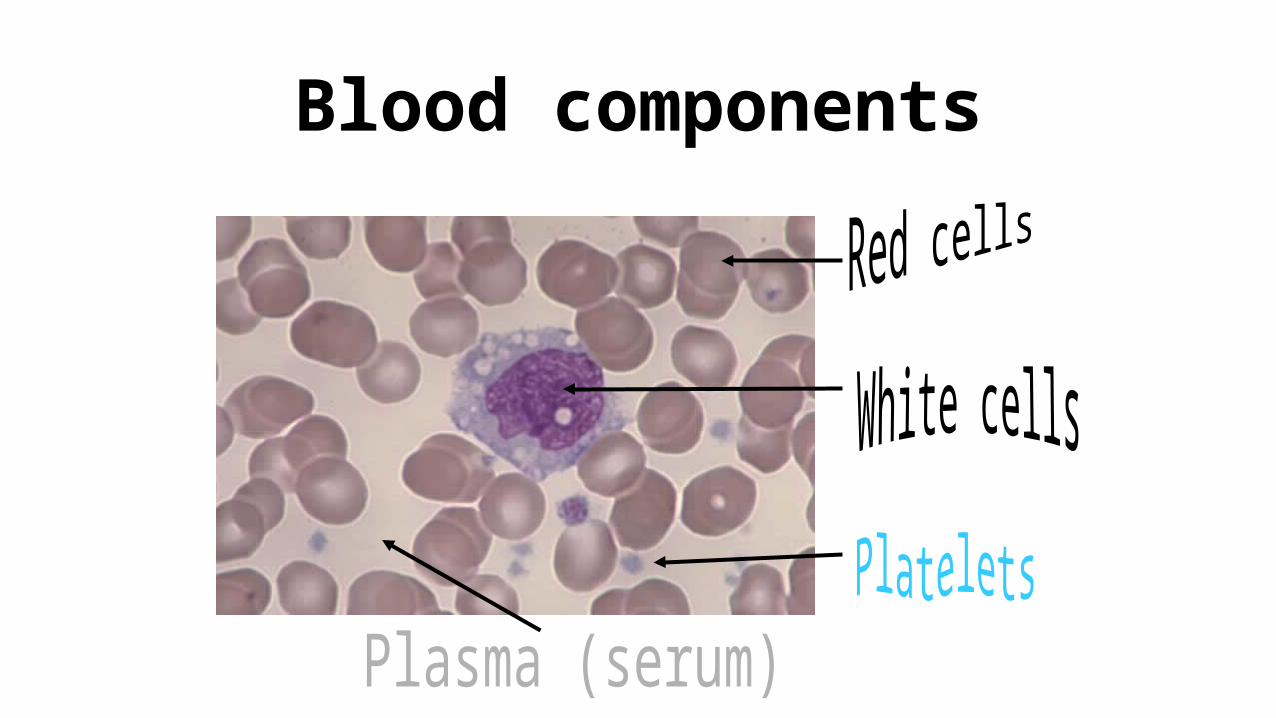
Blood components
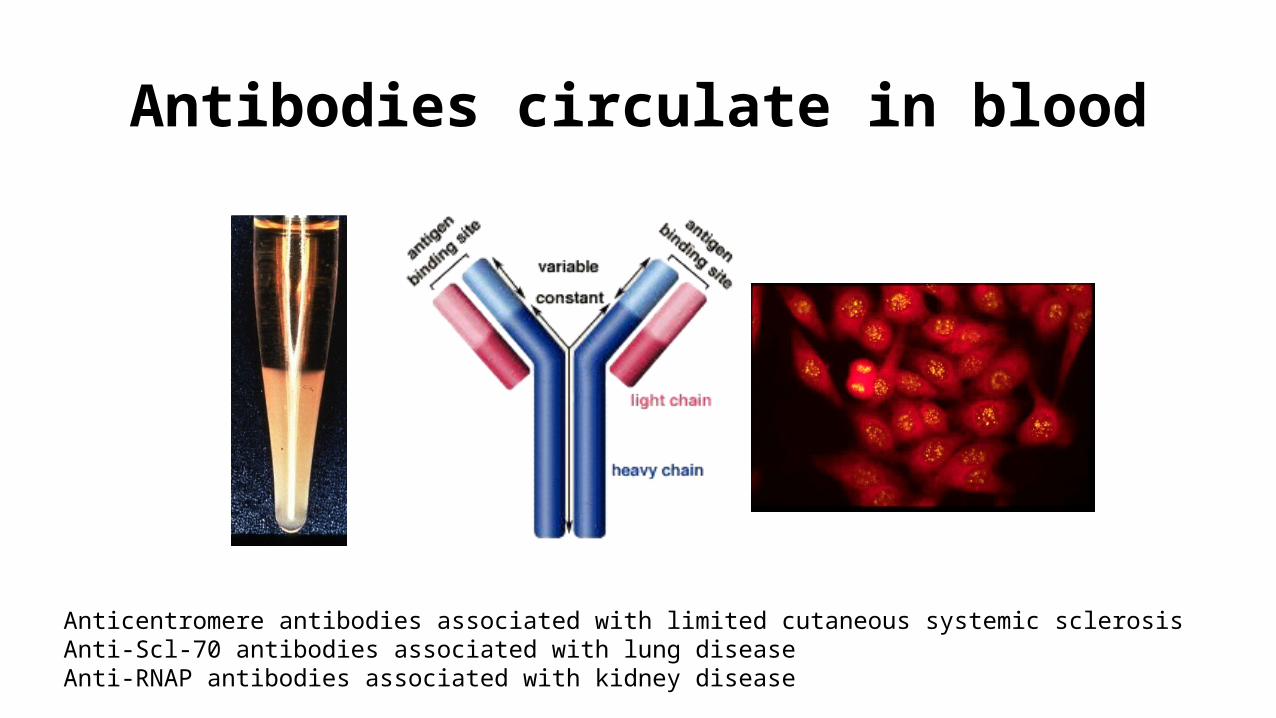
Antibodies circulate in blood
Anticentromere antibodies associated with limited cutaneous systemic sclerosisAnti-Scl-70 antibodies associated with lung diseaseAnti-RNAP antibodies associated with kidney disease
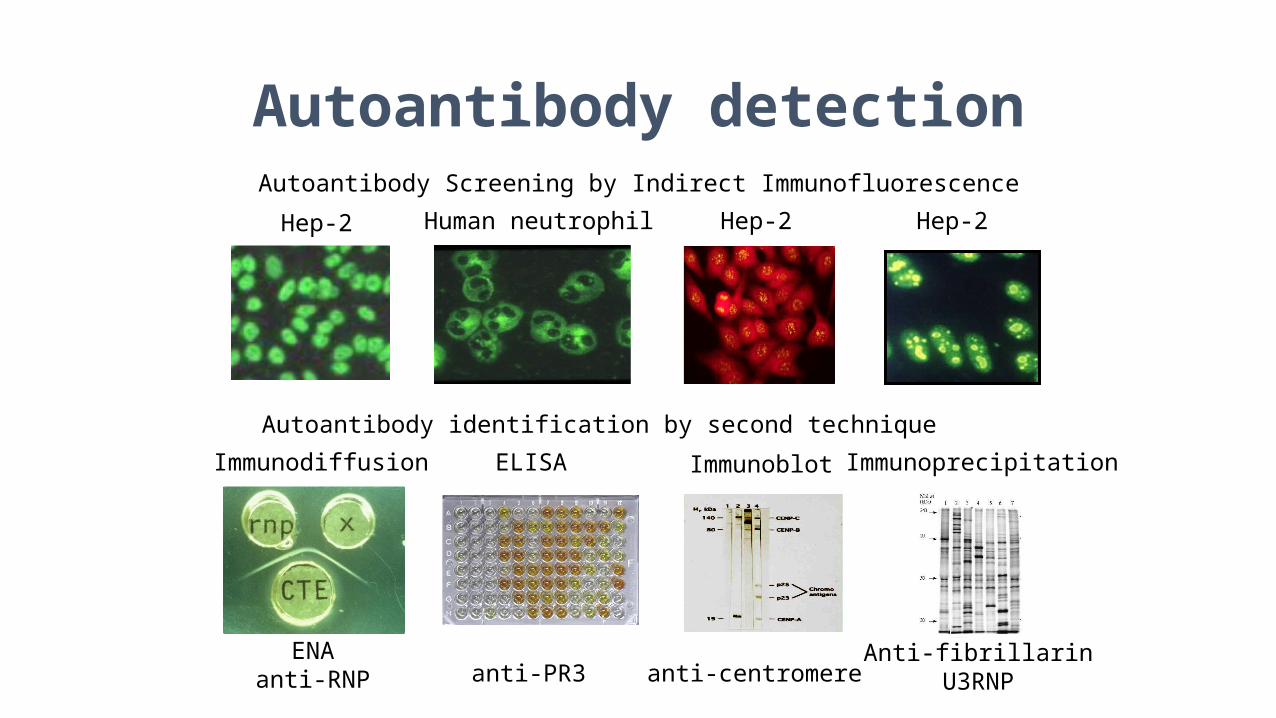
Autoantibody detectionAutoantibody Screening by Indirect Immunofluorescence
Hep-2 Hep-2 Hep-2Human neutrophil
Autoantibody identification by second technique
Immunodiffusion
ENAanti-RNP
ELISA
anti-PR3 anti-centromere
Immunoblot Immunoprecipitation
Anti-fibrillarinU3RNP
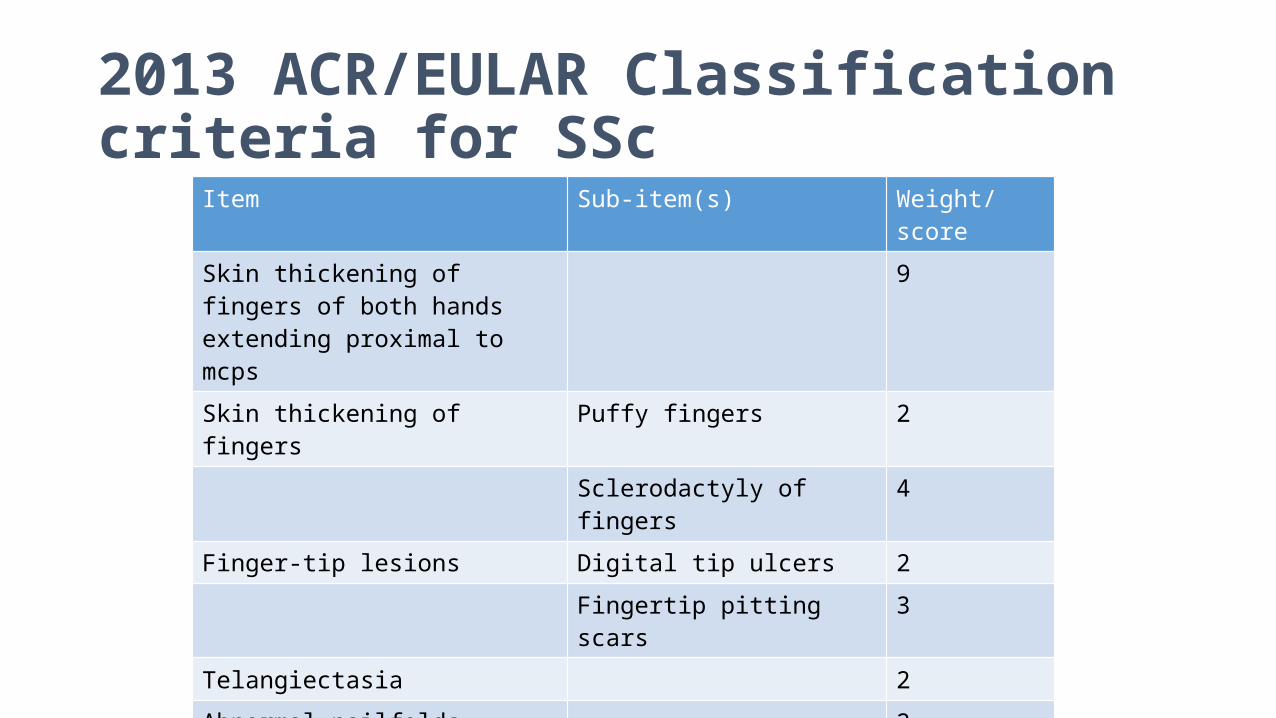
2013 ACR/EULAR Classification criteria for SSc
Item Sub-item(s) Weight/score
Skin thickening of fingers of both hands extending proximal to mcps
9
Skin thickening of fingers Puffy fingers 2
Sclerodactyly of fingers 4
Finger-tip lesions Digital tip ulcers 2
Fingertip pitting scars 3
Telangiectasia 2
Abnormal nailfolds 2
PAH +/- ILD 2
Raynaud’s phenomenon 2
SSc related autoantibodies ACA 3
Anti-topo 1
Anti-RNAP 3

And some of the Bath Team…