what every attorney should know about probability ... · section ix what every attorney should know...
TRANSCRIPT
Section IX
What Every Attorney Should Know About Probability, Coincidence and Causation in
Litigation
Michael D. Freeman, PhD, Forensic Research & Analysis, Portland, Oregon
C
AoFMS
CvgnroclirItpcbtt
I
Tdnpfstncsanrcdrbtdepcr
P1
P
linical Review: Focused
Systematic Approach to Clinical Determinationsf Causation in Symptomatic Spinal Disk Injuryollowing Motor Vehicle Crash Traumaichael D. Freeman, PhD, MPH, DC, Christopher J. Centeno, MD,
ean S. Kohles, PhD
MvUASfD
CsD
SElD
DC
linical determinations of causation in cases of intervertebral disk (IVD) injury after a motorehicle crash (MVC) are often disputed in medicolegal settings. No published systematicuidelines exist for making such determinations, which has resulted in infringement byonclinical personnel into injury causation evaluations, a traditionally clinical activity. Theesult is causal determinations that are potentially disconnected from clinical observationsf injury. The purpose of this review was to evaluate the current literature on causation,ausal determinations after trauma and IVD injury after MVC, and to develop a practicable,ogical, and literature-based approach to causation determinations of symptomatic IVDnjury after MVC. The results of the review indicate IVD injury can result from any MVCegardless of magnitude, thus meeting the first criteria of causation, biologic plausibility.ndividual determinations of causation depend entirely on the temporal association be-ween the collision and the symptom onset (the second criterion) and a lack of a morerobable explanation for the symptoms (the third). When these causal elements are met,linicians can assert causation on a “more probable than not” or “reasonable probability”asis. Because of a lack of an established or reliable relationship between collision force andhe probability of IVD injury the investigation of collision parameters is not a useful adjuncto causal determinations.
NTRODUCTION
he origin of injury to the intervertebral disks (IVD) of the spine is a common source ofispute in medicolegal circumstances. Whereas treating clinicians typically make determi-ations of causal relationships between a trauma and an injury primarily based on theatient-related history of the traumatic event and the onset of symptoms, opposing expertsrequently rely on population-based assumptions as a basis for disputing causal relation-hips. This scenario is observed most often when disk injuries and symptoms are attributedo motor vehicle crashes (MVC), because many crash-related injuries result from theegligence of another driver; thus, the nature and extent of an occupant’s injuries may beontested. There is typically a strong third-party (insurer) interest in minimizing compen-atory payments on behalf of the individuals who are at fault for the crash. As a result, andversarial system has developed in the United States and many other industrializedations, with the injured patient and his or her treating physicians on one side and the partyesponsible for the crash, his or her insurer, and the insurer’s medical and scientificonsultants on the other side [1,2]. Although some clinicians prefer to avoid causaleterminations altogether, it can be argued that such determinations are part and parcel ofegular medical care. To avoid such a determination solely because it may be later disputedy a party with interests opposing those of the patient is to avoid a duty to the patient; a dutyhat can have a significant impact on the patient’s well-being. This is not to say thatissemblance and fraud do not exist in the patient population; however, when there is novidence of dishonesty, there is no reason to assume the presence of fraud simply because aatient is claiming injury after a MVC that was caused by another’s negligence (the mostommon setting for a legal claim for monetary damages). Such events are, for the most part,
andomly distributed in the population that uses motor vehicles and not selective for peopleSa
M&R © 2009 by the American Academy of Physical Me934-1482/09/$36.00
rinted in U.S.A. D
.D.F. Department of Public Health and Pre-entive Medicine, Oregon Health & Scienceniversity School of Medicine, Portland, OR.ddress correspondence to: M.D.F., 205 Libertyt., NE, Suite B, Salem, OR 97301; e-mail:[email protected]: 5B, expert witness
.J.C. Spinal Injury Foundation, Westmin-ter, COisclosure: 5B, expert witness
.S.K. Department of Mechanical & Materialsngineering, Portland State University, Port-
and, ORisclosure: nothing to disclose
isclosure Key can be found on the Table ofontents and at www.pmrjournal.org
ubmitted for publication April 21, 2009;ccepted July 22.
dicine and RehabilitationVol. 1, 951-956, October 2009
OI: 10.1016/j.pmrj.2009.07.009951

igttst[
ninhccdmscaotEapc
tsdtataanm
cbsap
P
Dpdssesgvcds
ioccocwctlc
bHrcsbFpoMriatqodw
1
2
952 Freeman et al SYSTEMATIC APPROACH TO DISK INJURY CAUSATION
n whom fraudulent behavior is more common. When alle-ations of fraud are made in a medicolegal context, despitehe absence of evidence of fraud, it is reasonable to questionhe motivation behind the assertion, because forensic con-ultants who provide partisan opinions are no more immuneo secondary gain pressures than are litigants claiming injury3].
There are some authors who maintain that for a determi-ation of cause and effect to be made between a diagnosed
njury and an MVC, a biomechanical analysis of the forces isecessary to determine whether or not a particular collisionad the potential to cause the injuries [4] or that a detailedrash reconstruction is necessary before a causal associationan be determined [5]. In contrast, most authors who haveocumented IVD injuries associated with an MVC make noention of a biomechanical force analysis or a crash recon-
truction [6,7]. The latter approach is most typical of thelinically pragmatic approach to causation. If it is known thatn injury can be caused by a trauma, then there is no practicalr logical purpose served in quantifying the degree of therauma in order to assess the risk of injury after the event.ven injuries that are deemed highly unlikely or improbablere by definition still slightly likely or possible, and thus injuryresence is typically evaluated after the fact clinically, and notalled into question by a post-hoc suggestion of infrequency.
For the purposes of the present inquiry, a Medline search forhe years 1980 through 2009 (as of July 2009) using the medicalubject headings (MeSH) terms intervertebral disk, intervertebralisk displacement, and disk, herniated as well as the non-MeSHerms cervical disk, in conjunction with “injury” and/or “trauma,”long with “cause,” “causal,” and “causation” in various combina-ions did not elicit any publications that addressed an organizedpproach to determinations of causation between disk injurynd MVC exposure. It appears that, at the present time, there iso widely accepted scientific or clinical standard for such deter-inations.The purpose of this article is to assess the evidence for the
ausal relationship between disk injury and MVC traumaased on the published literature on causal standards and thecience of both disk injury and MVC trauma. Further, theuthors propose a systematic and scientifically based ap-roach to individual determinations of causation.
RIOR PUBLICATIONS ON CAUSATION
eterminations of causal association between a noxious ex-osure (microorganism, chemical, trauma, or other) and aisease or injury outcome in populations is an area of con-iderable interest to epidemiologists and others who studyuch issues. Individual clinical observations of cause andffect can serve as a reasonable basis for a case study anduggestion of a relationship. It is, however, difficult to draweneralizable conclusions from such reports. Case series pro-ide stronger evidence of causation; however, without aontrol group of unexposed subjects, there is no way toetermine which effects can be isolated to a particular expo-
ure. Even when case-control studies, in which diseased ornjured subjects are compared with healthy subjects for levelf exposure to a suspected noxious agent, show positiveorrelations between exposure and disease or injury out-ome, the results cannot be interpreted as validated evidencef a causal relationship, as confounding factors may exist thatan obscure true relationships. An example of confoundingould be the relationship between coffee drinking and lung
ancer. Coffee drinkers may have a higher rate of lung cancerhan non-coffee drinkers, but only because smokers are moreikely to drink coffee than nonsmokers, not because coffee isausally linked to lung cancer.
In an attempt to more clearly identify causal relationshipsetween noxious exposures and outcomes in populations,ill outlined a set of 9 criteria that needed to be considered to
easonably conclude that a particular noxious exposureould result in a particular disease [8]. Hill’s criteria haveerved as a kind of seminal gold standard, in that they haveeen adopted and modified by many others, including theood and Drug Administration, academic investigators, andharmaceutical companies, as a means of approaching issuesf causation systematically [9]. Based in part on Hill’s work,iller et al proposed a 4-stage process for identifying envi-
onmentally caused rheumatic disorders, an application thats more applicable to the goals of this article, because itllowed for assessments of causation in individuals ratherhan as a population-based construct [10]. McLean subse-uently adapted Miller et al’s work for causation in instancesf fibromyalgia after MVC [11]. All causal criteria can beistilled to a minimum of 3 common and essential elements,hich are as follows [12,13].
. There must be a biologically plausible or possible linkbetween the exposure and the outcome. For example,trauma and fracture are plausibly linked, but trauma andleukemia are not. Plausibility is a low threshold that isexceeded with relatively weak evidence, such as fromsmall observational studies (case studies or case serieswith small numbers of subjects) or from the results ofwell-designed experiments with many subjects. Biologicplausibility only pertains to whether an outcome canpossibly result from an exposure, and is unrelated to therate or frequency of the outcome. Thus, evidence of lowincidence is not evidence of biologic implausibility.
. There must be a temporal relationship between the expo-sure and the outcome. The outcome cannot preexist theexposure; however, the outcome of interest may havepreexisted the exposure in a less severe form that wasworsened by the exposure. Such a determination requiresan accurate documentation of the signs and symptoms ofthe condition of interest both before and after the expo-sure of interest. Additionally, the outcome cannot post-date the exposure by a period that is considered, from aclinical perspective, to be too long or too short to relatethe two. This determination is highly dependent on thespecifics of any case. For example, an injury to a nerveroot may cause immediate pain, but electromyogram
changes may lag behind by weeks or months. The deter-
3
AM
Icimiacodi
1
2
1
2
l
1
2
C
Bdr
953PM&R Vol. 1, Iss. 10, 2009
mination of reasonable temporal association is typicallymade as a matter of clinical judgment, rather than fromclearly delineated guidelines or principles.
. There must not be a more likely or probable alternativeexplanation for the symptoms. The term “likely” is ofgreatest importance, as, for example, it is not sufficient tosimply point out that a patient with back pain after traumais obese, that obesity is related to back pain, and thus it ismore likely that the obesity rather than the trauma causedthe back pain. For an alternative etiologic explanation tobe considered more likely than an alleged exposure it mustbe both biologically plausible and have a stronger tempo-ral relationship to the onset of symptoms than the allegedexposure. If plausibility is present and temporality isrelatively comparable, then 2 exposures can be comparedby examining the dose-response (intensity) of each expo-sure. Such a comparison may involve an analysis of theforces of the exposure as well as an epidemiologic assess-ment of injury frequency associated with the forces, and isbeyond the scope of a clinical assessment of causation.
Causation Algorithm for Disk Injury afterVC
n this section, the authors present a practical guideline forlinical determinations of causation in symptomatic disknjuries after an MVC, based on the application of the afore-
entioned 3 causal elements to the facts and findings in anndividual case. The following definitions and assumptionsre made. An IVD injury is defined by all of the followingharacteristics [14,15] (for this definition, “injury” is usednly to define a disk that has become symptomatic after aiscrete loading event of any magnitude, and the cause of the
njury is not addressed).
. It is symptomatic. This may include classic symptoms ofsegmentally appropriate radiculopathy, regional axialpain, or diskogenic referral of pain in a nondermatomaldistribution.
. There is clinical imaging evidence (magnetic resonanceimaging [MRI], computed tomography, or diskography)that the symptomatic disk fits the generally accepteddefinition of a degenerative/traumatic disk [14]. This in-cludes anular tears, herniations, and degeneration. Al-though there are findings specific to disk trauma, such asvertebral endplate fracture and edema presence in themarrow adjacent to the endplate, many traumaticallyinitiated disk injuries are indistinguishable from degener-ative changes in the disk [16]. Because of mediocre sen-sitivity and specificity (ie, true- and false-positive rates),imaging findings alone are insufficient evidence for eithera causal or noncausal determination in a case of suspectedor disputed traumatic disk injury [17,18].
MVC trauma is defined as follows.
. The patient was an occupant of a motor vehicle at the time
of a collision or event. s. The collision or event transmitted a force through thepatient’s spine over a very short time, typically 70-120 ms[19]. Note that the magnitude of the force is not addressedin the definition, because any degree of forceful loadingcould potentially produce a symptomatic disk injury in asufficiently susceptible individual.
There are 2 most likely scenarios in which a forcefullyoaded IVD may become symptomatic.
. A healthy disk with little or no changes associated withdegeneration is subjected to a significant load resulting indisruption of the annulus and possibly instantaneousmigration of nuclear material posteriorly toward the diskperiphery and into the epidural space or the lateral re-cesses. This is the scenario most likely to produce injuryto tissue surrounding the disk, including vertebral end-plate fracture and ligamentous disruption, and is mostlikely to be associated with higher energy crashes withsignificant vehicle damage [20].
. A degenerated disk (defined as a disk in which one ormore of the following are present to some degree: desic-cation, fibrosis, narrowing of the disk space, diffuse bulg-ing of the anulus beyond the disk space, anular tears,endplate sclerosis, and osteophytes at the vertebralapophyses [14]) is loaded in a manner that initiates asymptomatic response. A significant proportion of theasymptomatic population has some degree of disk degen-eration as seen on MRI; Matsumoto et al have performedthe largest study to date on the topic, with MRI scans ofthe cervical spines of 497 asymptomatic subjects [21].These authors describe a progressive direct relationshipbetween the presence and severity of degenerativechanges and age, with the disk degeneration noted in arange of 17% men and 12% of women in their 20s to 86%and 89% of men and women older than 60 years. Otherauthors have described similar findings with broad rangesof values depending on the age of the subjects; fromvirtually no disk degeneration in subjects �30 years ofage, to 14% in those 30-40, and 62% in subjects �40years of age [22,23]. Similar observations have been pub-lished with regard to lumbar spine degeneration amongasymptomatic patients. Jensen et al described a cohort of98 subjects who underwent lumbar MRI, noting that only36% of subjects had no abnormal disks. Fifty-two percentof the scans were interpreted as having a bulge at aminimum of one level, 38% had abnormality at more thanone level, 27% had a protrusion, and 1% had an extrusion[24]. These findings are consistent with those reported byother authors [25].
ausal Elements
iologic Plausibility. Can an MVC of any severity cause aisk injury? Crash testing of intact cadavers at accelerationsecorded for no-damage rear-impact collisions has demon-
trated IVD injury that cannot be detected by conventional
icsl[dptigvtiam
amtseccs(
TidcTdcsMcwipsovsopaadanidm
cai
hspidititdodcocsc
rgdtfwoat
scaamwMtcccb[psrmcmc
tpoabi
954 Freeman et al SYSTEMATIC APPROACH TO DISK INJURY CAUSATION
maging such as CT and MRI [26]. Although the biomechani-al literature on experimental loading of disks in cadavericled testing has demonstrated disk injuries even in relativelyow accelerations (3.3 and 4.5 times the force of gravity or “g”26]), such ex vivo testing of healthy disks does little toemonstrate minimal thresholds for injury in live humanopulations exposed to real-world crashes. No cadavericesting can duplicate the significant variation in the mannern which loads are transmitted to the human spine in a MVC,iven the variation in occupant position, restraint systems,ehicle interiors, and muscle loads. Additionally, the poten-ial for variation in the condition of an individual IVD,ncluding the ability of the disk to resist forceful loading fromn external source, is too large to ever define in an experi-ental setting.A relevant literature search revealed a complete absence of
ny publications suggesting that symptomatic IVD derange-ent cannot result from MVC exposure of any magnitude. To
he contrary, injury to the disks of the cervical and lumbarpine has been documented in the relatively low level accel-rations associated with little to no-damage collisions, rolleroaster rides, and even sneezing [27-30]. It is reasonable toonclude, as a general precept, that the forceful loading of thepine that can occur in any MVC is a biologically plausiblepossible) cause of symptomatic disk injury.
emporal Association. Temporality is the strongest ev-dence of causation in evaluating the patient with post-MVCisk injury. It must be first established that the MVC pre-eded the onset of symptoms attributed to the disk injury.he exception to this rule is when a previously symptomaticisk is exacerbated by an MVC to the point that the course ofare is significantly altered (ie, a previously diagnosed non-urgical disk condition becomes surgical directly after anVC). In such cases, the determination must be made clini-
ally as to whether the disk symptoms were likely to haveorsened to the point that the surgical intervention was
nevitable absent the MVC. The mere fact that the disk wasreviously symptomatic is not sufficient to draw the conclu-ion that it would have required surgery, given the goodutcomes for patients with diskogenic symptoms who use aariety of surgical and nonsurgical treatments [31-33]. Theymptom onset must be in reasonable proximity to the timef the MVC; however, disk injury symptoms may initiallyresent as identical to symptoms of spinal strain or sprain,nd it may be weeks or months before an MRI is performednd the disk injury diagnosis is first seen [34]. Additionally,isk injury symptoms may be progressive, as an injury to thennulus may progressively allow nuclear migration towardeurologic structures over a period of time while the patient
s in weight bearing and active. Determinations as to whetherelayed symptoms fulfill the temporal association criteriaust be made by clinicians on a case-by-case basis.An obvious weakness of the temporality criterion is that it
an only be established from the history given by the patient,nd patient histories can be erroneous or falsified. The former
s unlikely in the case of injury, however, because one of the callmarks of injury is that there is a close temporal relation-hip between cause and effect (this lack of clear temporalroximity in repetitive traumatic exposures is the reason that
njuries such as carpal tunnel syndrome are classified asiseases) [35]. This close temporal relationship means that it
s unlikely that a patient will misattribute symptoms to araumatic cause. As a practical matter, the most reliablendicator of when a patient began to have symptoms after arauma is the patient. This is not to say that patients do not getetails concerning an injury event wrong; patient perceptionr recollection of vehicle speeds, crash sequence, and otheretails of a collision may be inconsistent with the facts of aase for reasons other than untruthfulness. For example, anccupant who is injured in a minimal damage rear endollision may believe that the impact must have been at highpeed despite a lack of physical evidence that this was thease.
With regard to the truthfulness of the patient, it is not theole of the clinician to investigate the veracity of the historyiven by the patient. Absent some ancillary indication ofeception, clinicians are generally safe to believe their pa-ients. The rate of fraud of any kind in auto insurance claimsor treatment benefits (personal injury protection coverage)as estimated to be 6% for 2007 [36]. Even if every instancef fraud in auto insurance cases consisted of a patient givingfalse history, clinicians would still be justified in believing
heir patients 94% of the time.Intuitively, it makes sense that the closer the onset of
ymptoms is to the time of the collision the stronger theausal relationship between the MVC and the disk injury,nd the strength of this relationship can be quantified usingn indirect approach. For example, in a case of a 40-year-oldale with neck pain and cervical radiculopathy that aroseithin 12 hours of a rear impact collision (later attributed toRI findings of disk herniation), assuming no intervening
rauma, it can be postulated, as a tautology, that either therash caused the disk injury or that it was coincidental to theollision, regardless of cause. Thus, the probability that therash caused the disk injuries [P(diskMVC)] plus the proba-ility the disk symptoms are coincidental to the crashP(diskCOINC)] when added together account for all of theossible causes (100% or 1) of the disk injury and associatedymptoms. If [P(diskMVC) � P(diskCOINC) � 1] then rear-anging the terms gives [1 � P(diskCOINC) � P(diskMVC)],eaning that if the probability that a disk injury occurred
oincidentally on the same day of the MVC can be deter-ined then the probability the MVC caused the disk injury
an also be determined indirectly.The probability of 2 unrelated events occurring in close
emporal proximity can be calculated by multiplying therobability or odds of one times the other (odds are the ratiof 2 probabilities). For example, the odds of rolling 2 sixes inrow with a fair die are [(1:6) � (1:6) � 1:36]. This is
ecause there are 36 possible combinations for any 2 rolls,ncluding 1 and 1, 1 and 2, 1 and 3, etc, and only one of the
ombinations is a 6 and 6.
ctmymtmpmtwMi1tt1
L
Aittwfpapnswisfsttwdifiws
D
IMlTdsii
bd
cMmlmgrbaitctwaipard
loastgwcadoiaeagir
harrThfm
C
IM
955PM&R Vol. 1, Iss. 10, 2009
In a similar fashion the odds of a disk injury occurringoincidentally on the day of a collision can be calculated forhe example given earlier. The annualized odds of involve-ent in a MVC for a 40-year-old male are 1:14 (once every 14
ears), and the daily odds of crash involvement are approxi-ately 1:5100 (one crash every 5100 days) [37]. The odds of
he spontaneous development of disk symptoms are a bitore difficult to estimate. For example, it can be said that theatient had a single-day episode of neck and arm pain 12onths before the MCV, with no intervening episodes until
he time of the collision. Thus, the odds that the symptomsould recur on any single day were no greater than 1:365.ultiplied together these 2 odds yield an odds of a disk
njury occurring coincidentally on the day of the collision of:1,861,500. Conversely, the odds in favor of a causal rela-ionship between the collision and the disk injury, givenhe onset of symptoms on the day of the collision, are,861,500:1.
ack of Likely Alternative Explanations
lternative explanations for a disk injury include an interven-ng trauma that followed the MVC and preceded the symp-oms indicative of disk injury. Another alternative explana-ion is the insidious onset of symptoms, possibly associatedith a trivial perturbation such as sneezing. Although minor
orces are possible causes of disk injury, they cannot bereferentially selected over the substantially greater forces ofcollision when the two have occurred in close temporal
roximity. If, for example, a patient sustains what is diag-osed as a lumbar strain in a collision and a week laterneezes and has a sudden onset of radicular pain associatedith a disk extrusion, then it is most likely that the disk was
njured in the MVC and the sneeze only prompted a progres-ion of symptoms. It is not reasonable to point to minororces associated with daily activities as a likely cause of aymptomatic disk in preference to the significantly greaterrauma associated even with minimal and no-damage MVCshat is temporally relevant to the symptoms, particularlyhen the patient performed such minor activities with noifficulty prior to the MVC. A “likely” alternative explanation
s one that is most probably causal and the best explanation tot all of the facts at hand, not one that is only a possible causeith no historical or temporal evidence to link it to the
ymptomatic disk injury.
ISCUSSION
ndividual determinations of causation for IVD injury afterVC by clinicians require only that temporal association and
ack of likely alternative explanation be satisfactorily present.he biologic plausibility or possibility that symptomatic diskerangement can follow any degree of forceful loading of thepine is satisfactorily present and need not be revisited inndividual cases. Thus, the concept of measuring crash forces
n detail as a means of determining disk injury potential can pe abandoned as serving no useful purpose in causationeterminations.
There is no reliable index of the degree of force required toause a particular degree of disk derangement. Walz anduser theorized that unless a crash reconstruction and bio-echanical loading assessment was performed for a particu-
ar crash and occupant that causation could not be deter-ined, or, put another way, it must be determined that a
iven crash was sufficiently forceful to cause diagnosed inju-ies [4]. These authors suggested that parameters such as seatelt use, head restraint and seat properties, age, body size,nd preexisting damage (sic) to the spine, inter alia, be takennto account when making causation determinations, effec-ively taking causal determinations out of the hands of clini-ians. What these authors do not explain is how an evalua-ion of any or all of such factors could help determinehether or not any type or severity of injury is possible aftercrash. Even if it could be determined that the risk of disk
njury was exceedingly low for a particular occupant in aarticular crash, this would not be evidence that contradictsny of the 3 elements of causation. Thus, this biomechanicalisk model of injury presence has no utility for real-worldeterminations of causation.
After a determination of causation has been reached, theegal standard for expressing the opinion is as “more probabler likely than not” or as a “reasonable probability” or “reason-ble medical probability” [38]. In some jurisdictions, thetandard is that the clinician must be “more than 50% cer-ain” that the opinion is correct. The purpose of such lan-uage is to describe the results of an internal process ofeighing evidence, and to arrive at a conclusion that the
linician is more certain than not that his or her opinion isccurate or true. The methodology presented in this article isesigned to provide a framework for clinicians to arrive atpinions of causation that can be expressed in terms of whats more likely than not. Thus, when using these guidelines in
narrative report setting, the clinician can write that thessential causal elements of biologic plausibility, temporality,nd lack of likely alternative explanation have been met for aiven case (if true), and that a particular symptomatic disknjury resulted from a particular motor vehicle crash, as aeasonable medical probability.
It must be noted that the model of causation presentederein suffers from the fact that there is no other alternativegainst which it can be evaluated for accuracy. Clinicianseceive little or no formal education in medical school oresidency regarding a systematic approach to causation.hus, the authors recommend that guidelines presentederein be evaluated, modified if necessary, and consideredor adoption by consensus by appropriate scientific andedical organizations.
ONCLUSIONS
ndividual determinations of causation for disk injury afterVC are most appropriately conducted by clinicians, based
rimarily on an evaluation of the temporal association be-
tmsoa
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
956 Freeman et al SYSTEMATIC APPROACH TO DISK INJURY CAUSATION
ween the MVC and the symptom onset. The lack of a valid oreaningful collision force threshold below which it can be
aid that a disk injury will not occur means that investigationf collision parameters for the purposes of injury causationssessment is a pointless endeavor.
EFERENCES1. Freeman MD, Centeno C. Whiplash and secondary gain. J Whiplash Rel
Dis 2003;2:1-4.2. Centeno CJ, Freeman MD, Welkins WL. A review of the literature
refuting the concept of minor impact soft tissue injury. Pain Res Manage2005;10:71-74.
3. Freeman MD, Centeno CJ. A fatal case of secondary gain; a cautionarytale. Am J Case Reports 2008;9:97-103.
4. Tencer AF, Mirza S. Whiplash mechanics in low speed rear-end auto-mobile collisions. J Musculoskel P 2000;8:69-86.
5. Walz FH, Muser MH. Biomechanical assessment of soft tissue cervicalspine disorders and expert opinion in low speed collisions. AccidentAnal Prevent 2000;32:161-165.
6. Jonsson H Jr, Cesarini K, Sahlstedt B, Rauschning W. Findings andoutcome in whiplash-type neck distortions. Spine 1994;19:2733-2743.
7. Scuderi GJ, Sherman AL, Brusovanik GV, Pahl MA, Vaccaro AR. Symp-tomatic cervical disc herniation following a motor vehicle collision:return to work comparative study of workers’ compensation versuspersonal injury insurance status. Spine J 2005;5:639-644.
8. Hill AB. The environment and disease: association or causation? ProcRoy Soc Med 1965;5:295-300.
9. Stephens MD. The diagnosis of adverse medical events associated withdrug treatment. Adv Drug React Ac Poison Rev 1987;6:1-35.
0. Miller FW, Hess HV, Clauw DJ, et al. Approaches for identifying anddefining environmentally associated rheumatic disorders. Arth Rheum2000;43:243-249.
1. McLean SA, William DA, Clauw DJ. Fibromyalgia after motor vehiclecollision: evidence and implications. Traffic Injury Prev 2005;6:97-104.
2. Evans AS. Causation and disease: a chronological journey. The ThomasParran Lecture. Am J Epidemiol 1978;108:249-258.
3. Freeman MD, Rossignol AC. Forensic epidemiology: a systematic ap-proach to probabilistic determinations in disputed matters. J ForensicLegal Med 2008;15:281-290.
4. Pfirrmann CW, Dora C, Schmid MR, Zanetti M, Hodler J, Boos N. MRimage-based grading of lumbar nerve root compromise due to diskherniation: reliability study with surgical correlation. Radiology 2004;230:583-588.
5. Fardon DF, Milette PC. Nomenclature and classification of lumbar discpathology. Recommendations of the Combined task Forces of theNorth American Spine Society, American Society of Spine Radiology,and American Society of Neuroradiology. Spine 2001;26:E93-E113.
6. Carragee E, Alamin T, Cheng I, Franklin T, van den Haak E, Hurwitz E.Are first-time episodes of serious LBP associated with new MRI find-ings? Spine J 2006;6:624-635.
7. O’Neill C, Kurgansky M, Kaiser J, Lau W. Accuracy of MRI for diagnosisof discogenic pain. Pain Physician 2008;11:311-326.
8. Carragee EJ, Paragioudakis SJ, Khurana S. 2000 Volvo Award winner inclinical studies: lumbar high-intensity zone and discography in sub-
jects without low back problems. Spine 2000;25:2987-2992.9. Siegmund GP, King DJ, Lawrence JM, Wheeler JP, Brault JR, Smith TA.Head/neck kinematic response of human subjects in low-speed rear-end collisions. Society of Automotive Engineers, Proceedings of the41st Stapp Car Crash Conference 973341. 1997:357-385.
0. Knobloch K, Wagner S, Haasper C, et al. Sternal fractures occur mostoften in old cars to seat-belted drivers without any airbag often withconcomitant spinal injuries: clinical findings and technical collisionvariables among 42,055 crash victims. Ann Thorac Surg 2006;82:444-450.
1. Matsumoto M, Fujimura Y, Suzuki N, et al. MRI of cervical interverte-bral discs in asymptomatic subjects. J Bone Joint Surg Br 1998;80-B:19-24.
2. Boden SD, McCowin PR, Davis DO, Dina TS, Mark AS, Wiesel S.Abnormal magnetic-resonance scans of the cervical spine in asymp-tomatic subjects. J Bone Joint Surg 1990;72-A:1178-1184.
3. Lehto IJ, Tertti MO, Komu ME, Paajanen HEK, Tuominen J, KormanoMJ. Age-related MRI changes at 0.1 T in cervical discs in asymptomaticsubjects. Neuroradiology 1994;36:49-53
4. Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malka-sian D, Ross JS. Magnetic resonance imaging of the lumbar spine inpeople without back pain. N Engl J Med 1994;331:69-73.
5. Savage RA, Whitehouse GH, Roberts N. The relationship between themagnetic resonance imaging appearance of the lumbar spine and lowback pain, age and occupation in males. Eur Spine J 1997;6:106-114.
6. Yoganandan N, Cusick JF, Pintar FA, Rao RD. Whiplash injury deter-mination with conventional spine imaging and cryomicrotomy. Spine2001;26:2443-2448.
7. Freeman MD, Centeno CJ. Etiologic and demographic characteristicsof traffic crash-related disc injuries. Spine J [in press doi:10.1016/j.spinee.2008.06.373]
8. Giuliano V, Giuliano C, Pinto F, Scaglione M. The use of flexion andextension MR in the evaluation of cervical spine trauma: initial experi-ence in 100 trauma patients compared with 100 normal subjects.Emerg Radiol 2002;9:249-253.
9. Freeman MD, Croft AC, Nicodemus CN, Centeno CJ, Welkins WL.Significant spinal injury resulting from low-level accelerations: a caseseries of roller coaster injuries. Arch Phys Med Rehab 2005;86:2126-2130.
0. Sadanand V, Kelly M, Varughese G, Fourney DR. Sudden quadriplegiaafter acute cervical disc herniation. Can J Neurol Sci 2005;32:356-358.
1. Schechter NA, France MP, Lee CK. Painful internal disc derangementsof the lumbosacral spine: discographic diagnosis and treatment byposterior lumbar interbody fusion. Orthopedics 1991;14:447-451.
2. Dallolio V. Lumbar spinal decompression with a pneumatic orthesis(Orthotrac): preliminary study. Acta Neurochir Suppl 2005;92:133-137.
3. Kruse RA, Imbarlina F, De Bono VF. Treatment of cervical radiculop-athy with flexion distraction. J Manipulative Physiol Ther 2001;24:206-209.
4. Goreham FW. Cervical disc injury; symptoms and conservative treat-ment. Calif Med 1964;101:363-367.
5. Kao SY. 2003. Carpal tunnel syndrome as an occupational disease. J AmBoard Fam Pract 2003:16:533-542.
6. http://www.ircweb.org/News/IRC_Fraud_NR.pdf. Accessed April 16,2009.
7. http://www-nrd.nhtsa.dot.gov/Pubs/98.010.PDF. Accessed April 19,2009.
8. Mossman D. Interpreting clinical evidence of malingering: a Bayesian
perspective. J Am Acad Psychiatry Law 2000;28:293-302.
Wien Med Wochenschr (2011)DOI 10.1007/s10354-011-0909-3! Springer-Verlag 2011Printed in Austria
An evaluation of applied biomechanicsas an adjunct to systematic speci!c causationin forensic medicineMichael D. Freeman1 and Sean S. Kohles2
1Department of Public Health and Preventive Medicine, Oregon Health and Science University,Portland, Oregon, USA, and Institute of Forensic Medicine, Faculty of Health Sciences, AarhusUniversity, Aarhus, Denmark
2Regenerative Bioengineering Laboratory, Department of Mechanical and Materials Engineering,Portland State University, Portland, Oregon, USA
Received September 25, 2010, accepted (after revision) December 14, 2010, published online July 29, 2011
Summary. Biomechanical tests of post hoc probability havebeen proposed by prior authors as reliable tests of causation inforensic settings. Biomechanical assessment of injury kineticsand kinematics is a potentially important tool in forensic medi-cine, but there is also the potential for misapplication. The mostreliable application is when biomechanical analysis is used toexplain injury mechanisms, such as how an injury may haveoccurred. When a biomechanical analysis is used as a means ofdeterminingwhether, rather than how an injury has resulted froma traumatic exposure, then a lack of reliability of themethodologylimits its application in forensic medicine. Herein, we describe asystematic assessment of causation by adapting established gen-eral causation principles to speci!c causation scenarios, and howbiomechanical analysis of injury mechanics is properly used toaugment such an approach in conjunction with the principles offorensic epidemiology. An example calculation of relative riskassociated with cervical spine injury is provided as a representa-tive probabilistic metric for assessing causation. The statisticalbene!ts and limitations of biomechanical analysis are discussedas an adjunct to forensic medicine.
Key words: Forensic medicine, biomechanics, Hill criteria,causation, forensic epidemiology
Introduction
The use of biomechanical analysis of injury me-chanisms as an adjunct to forensic medicine has beenincreasing over the past 20 years. Biomechanics may be
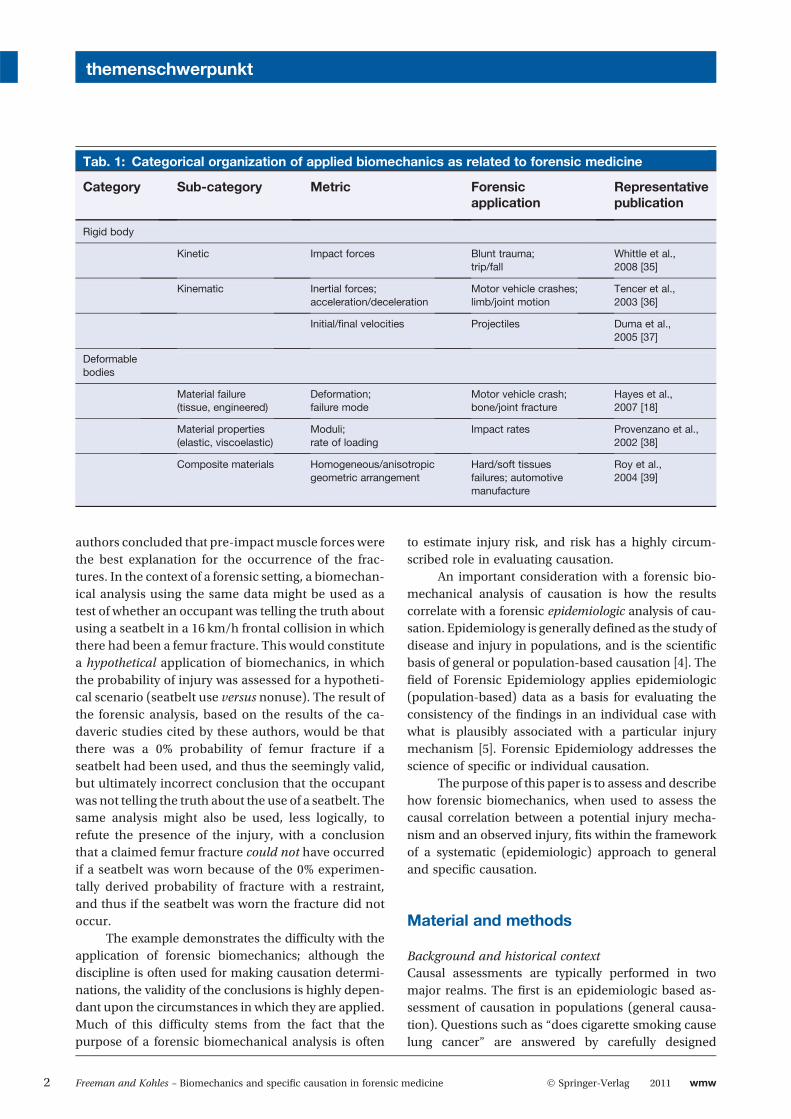
simply de!ned as the study of the effect of mechanicalenergy on biological tissue. However, in the context offorensic medicine the discipline is used most often tode!ne injury thresholds, and to match injury mechan-isms with expected or observed injuries as a means ofcausal determination [1]. As an applied mathematicsdiscipline, various categorical approaches de!ne thefundamental assumptions typically applied in forensicssuch as rigid body kinetics/kinematics or deformablebody deformations (Tab. 1). These initial assumptionsguide the appropriate mathematical treatment of thecase at hand. Biomechanics has been demonstrated asan important but limited role in forensic investigationof death and injury. The discipline can be very helpfuland relevant for analyzing how injuries occur and indifferentiating between competing injury mechanismsfor observed injuries, but it can result in error-proneconclusions for other applications [2].
We have previously described how forensic bio-mechanics is most reliable when used to explain howobserved injuries occur, less reliable when evaluatingcompeting hypothetical explanations for an observedinjury, and least reliable when used to refute thepresence of observed injuries [2]. As an example, agroup of authors have described 20 femur fracturesoccurring in restrained occupants in frontal collisions,some at unexpectedly low speeds (16 km/h) [3]. Ananalysis of the collision forces was compared to priorbiomechanical experimental ex vivo data that pre-dicted a low or non-existent risk of fracture. The
Correspondence: Michael D. Freeman, PhD, MPH, Department ofPublic Health and Preventive Medicine, Oregon Health and ScienceUniversity, 1234 SW 18th Ave, Suite 102, Portland, OR 97205, USA.Fax: !!1-971-255-1046, E-mail: [email protected]
themenschwerpunkt
wmw 2011 ! Springer-Verlag 1
authors concluded that pre-impactmuscle forces werethe best explanation for the occurrence of the frac-tures. In the context of a forensic setting, a biomechan-ical analysis using the same data might be used as atest of whether an occupant was telling the truth aboutusing a seatbelt in a 16 km/h frontal collision in whichthere had been a femur fracture. This would constitutea hypothetical application of biomechanics, in whichthe probability of injury was assessed for a hypotheti-cal scenario (seatbelt use versus nonuse). The result ofthe forensic analysis, based on the results of the ca-daveric studies cited by these authors, would be thatthere was a 0% probability of femur fracture if aseatbelt had been used, and thus the seemingly valid,but ultimately incorrect conclusion that the occupantwas not telling the truth about the use of a seatbelt. Thesame analysis might also be used, less logically, torefute the presence of the injury, with a conclusionthat a claimed femur fracture could not have occurredif a seatbelt was worn because of the 0% experimen-tally derived probability of fracture with a restraint,and thus if the seatbelt was worn the fracture did notoccur.
The example demonstrates the dif!culty with theapplication of forensic biomechanics; although thediscipline is often used for making causation determi-nations, the validity of the conclusions is highly depen-dant upon the circumstances in which they are applied.Much of this dif!culty stems from the fact that thepurpose of a forensic biomechanical analysis is often
to estimate injury risk, and risk has a highly circum-scribed role in evaluating causation.
An important consideration with a forensic bio-mechanical analysis of causation is how the resultscorrelate with a forensic epidemiologic analysis of cau-sation. Epidemiology is generally de!ned as the study ofdisease and injury in populations, and is the scienti!cbasis of general or population-based causation [4]. The!eld of Forensic Epidemiology applies epidemiologic(population-based) data as a basis for evaluating theconsistency of the !ndings in an individual case withwhat is plausibly associated with a particular injurymechanism [5]. Forensic Epidemiology addresses thescience of speci!c or individual causation.
The purpose of this paper is to assess and describehow forensic biomechanics, when used to assess thecausal correlation between a potential injury mecha-nism and an observed injury, !ts within the frameworkof a systematic (epidemiologic) approach to generaland speci!c causation.
Material and methods
Background and historical contextCausal assessments are typically performed in twomajor realms. The !rst is an epidemiologic based as-sessment of causation in populations (general causa-tion). Questions such as !does cigarette smoking causelung cancer" are answered by carefully designed
Tab. 1: Categorical organization of applied biomechanics as related to forensic medicine
Category Sub-category Metric Forensicapplication
Representativepublication
Rigid body
Kinetic Impact forces Blunt trauma;trip/fall
Whittle et al.,2008 [35]
Kinematic Inertial forces;acceleration/deceleration
Motor vehicle crashes;limb/joint motion
Tencer et al.,2003 [36]
Initial/!nal velocities Projectiles Duma et al.,2005 [37]
Deformablebodies
Material failure(tissue, engineered)
Deformation;failure mode
Motor vehicle crash;bone/joint fracture
Hayes et al.,2007 [18]
Material properties(elastic, viscoelastic)
Moduli;rate of loading
Impact rates Provenzano et al.,2002 [38]
Composite materials Homogeneous/anisotropicgeometric arrangement
Hard/soft tissuesfailures; automotivemanufacture
Roy et al.,2004 [39]
themenschwerpunkt
2 Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine ! Springer-Verlag 2011 wmw

epidemiologic studies showing repeated and consistentrelationships between suspected cause and observeddisease or injury effect.
The second type of causal assessment is the eval-uation of cause and effect in individuals (speci!c cau-sation), most often performed by clinicians in a clinicalsetting, but also a frequent issue of contention in foren-sic settings. The two are inextricably interwoven, in-asmuch as speci!c causation depends on principles ofgeneral causation, and general causation is based upona foundation of individual cases of speci!c causation.Clinicians make determinations of causation that arecentered around diagnosis and history, and based uponinteraction with patients. Epidemiologists typically as-sess speci!c causation in a post-clinical setting as ameans of determining whether an individual case !tsthe de!nition for inclusion in a larger group of similarpatients or subjects. Biomechanical analysis is mostoften used in such a setting after a causal determinationhas been made, as a means of explaining injuriesthat have been observed medically and cataloguedepidemiologically.
Forensic Epidemiology has historically served as abasis for quantifying causal determinations in legal andforensic settings. General and speci!c causation ap-proaches employing epidemiologic data and methodshave been applied in legal rulings by U.S. courts in-cluding cases in administrative law, civil law, criminallaw, and public health law [6]. As an example of theadmission of epidemiology as relevant evidence, courtshave accepted as evidence reports of epidemiologicalstudies conducted by the U.S. Centers for DiseaseControl that analyzed the association between tamponuse and the risk of toxic shock syndrome as a means ofspeci!c causation determination [7]. In reaching itsdecision, the Court relied on several prior cases thathad permitted the admission of epidemiological evi-dence for causal determinations. In another case, epi-demiologic testimony was used to establish the timeperiod during which an individual was at increased riskof contracting Guillain Barre syndrome following SwineFlu vaccination, a critical factor in determining bothgeneral and speci!c causation [8]. Epidemiologic evi-dence has also been used to address issues of causationpertaining to communicable disease transmission [9,10]. Epidemiologic causation has been used in manyother legal circumstances, ranging from the criminalcontext [11] to disputes over regulatory issues regardingexposure to toxic substances [12].
As an adjunct to causation, Forensic Biomechan-ics has a briefer history in the courts. Biomechanics hasbeen applied in forensic settings primarily as an adjunct
analytical approach in motor vehicle crash cases [13].These forensic applications of biomechanical analysishave not been directed at absolute causation (i.e.whether injury occurred), but rather at assessing theprobability of competing theories of injury. In 2000,Walz and Muser introduced the theory that a bio-mechanical analysis was an essential part of causaldeterminations of so-called !whiplash" injury aftertraf!c crashes [14]. These authors suggested that with-out such an analysis a clinical determination of causa-tion was not suf!cient for a court setting. Multiplebioengineering approaches have been proposed forthe forensic setting as a means of introducing a tech-nology-based approach to causal analysis. These ap-proaches include detailed anatomic distinctions intissue-joint properties [15], three-dimensional compu-tational analyses [16, 17], and tissue-joint failurethresholdmetrics [18]. The application of suchmethodsmay carry with them the implication of greater validityin a forensic setting because of the lay misperceptionthat a high-technology approach to causation is insome way superior to the more traditional but low-technology clinical approach.
General causationA working de!nition of causation represents a speci!cevent as an antecedent event, condition, or character-istic that was necessary for the occurrence of the dis-ease, injury, etc. at the moment it occurred, given thatother conditions are !xed [19]. In other words, thecause of a disease or injury event is an event, condition,or characteristic that preceded the disease event andwithout which the disease or injury would not haveoccurred at all or would not have occurred until somelater time. The scienti!c basis for general and speci!cdeterminations of cause and effect was introducedthrough the inductive canons of John Stuart Mill [20]and the rules proposed by the philosopher DavidHume [21].
In the current era, a practical approach to causa-tion was laid out in a systematic fashion by Sir AustinBradford-Hill in 1965 [22]. Hill outlined nine criteria bywhich population-based determinations of causationcould be made when there is substantial epidemiologicevidence linking a disease or injury with an exposure,e.g. smoking and lung cancer [23]. Hill#s criteria haveserved as the seminal basis from which virtually allsubsequent systematic approaches to general and spe-ci!c causation have been derived, including those fora variety of injuries including traumatic brain injury[24], carpal tunnel syndrome [25], needle stick injuries[26] and spinal disk injuries [27], inter alia.
themenschwerpunkt
wmw 2011 ! Springer-Verlag Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine 3

Hill#s original nine criteria, and how they pertainto both general and speci!c causation, are as follows.
Strength of associationHill considered strength of association to be themost important determinant of causation. Most sim-ply stated, a strong association is more likely toindicate a causal relationship than is a modest orweak association. Strength of association can bemeasured in general causation by the percentagedecrease of an illness or injury in society or in aspeci!c population if the injury cause were to beeliminated [19]. This is also known as the etiologicfraction that the particular cause contributes to thetotal societal burden of the disease.
In speci!c causation, strength of association isdetermined by a comparison between the injury ordisease risk of the exposure and the risk of alternativeor competing explanations for the injury or diseasegiven the temporal relationship between exposure andoutcome. An example would be a death occurring1 hour following the administration of an intravenousdrug. The death may be very rarely associated with thedrug (e.g. 1 death per 100,000 doses), and thus thestrength of association, relative to general causation, isvery low (only a very small proportion of total deathswould be avoided if the drug became unavailable).However, if the probability that other causes of deaththat would have been likely to act coincidentally be-tween the time of the drug administration and the death(e.g. infection, sudden cardiac death, etc.) is evenlower, then the relative strength of association of thedrug to the death, in comparison to other causes, is veryhigh.
The strength of association is measured byrelative risk (RR), which is the ratio between therate of injury or disease outcomes in the exposedpopulation versus the rate of injury or disease out-comes in the unexposed population. In speci!c cau-sation, RR is measured by the risk of the conditionresulting from the exposure versus the risk of thecondition arising at the same time as the exposurefrom some cause other than the prime causal sus-pect. In order to meet the !more probable than not"(>50% probable) criterion for presentation in a fo-rensic setting, an exposure must have an RR ofgreater than 2.0, given the speci!c circumstances ofthe case in question (mathematically, a relative riskof 2.0 is the same as a 50% probability). A commonexample of the use of RR in a forensic setting is seenin the evaluation of causation in cases of disease thatare associated with exposure to a toxin, such as
cigarette smoking. For example, passive exposure tocigarette smoking has a relative risk for lung cancerof 3.4 for certain populations [28]. This means thatamong equivalent populations, there will be 3.4cases of lung cancer among the exposed for every1.0 case of lung cancer among the unexposed. Thus,among the exposed, 71% of the cases of disease (2.4of the 3.4 cases) resulted solely from the exposure,and 29% of the cases (1.0 of the 3.4) occurredregardless of the exposure to secondhand smoke.Based on these data it could be concluded, in anindividual case of lung cancer associated with pas-sive exposure to cigarette smoke, that more oftenthan not (>50% of the time) the lung cancer wascaused by the smoking.
ConsistencyIn general causation, the repetitive observation of acausal relationship in different circumstances strength-ens the causal inference. For example, a causal rela-tionship between cigarette smoking and lung cancer isobservable for all brands and varieties of cigarettes.Consistency is present in speci!c causation if otherindividuals have been observed with the same outcomefollowing substantially similar exposures, for examplein observational (epidemiologic) study.
Speci!cityIn general causation, speci!city refers to the degreeto which a factor is associated with a particularoutcome or population. In his original paper, Hillfamously referred to scrotal cancer in chimneysweeps as an example of speci!city, as the conditionrarely occurred outside that particular population.For example, in an intravenous drug death, the drugmay have a low speci!city for death, as a very smallproportion of deaths are caused by overdose of thedrug, and the cause of death is typically multifacto-rial. In contrast, a decedent found with a 3 cm cir-cular depression in his skull and a hammer nearbyhas an injury that is highly speci!c for having beenstruck in the head with the hammer. Thus, speci!cityhas value in speci!c causation when it#s present,but a lack of speci!city does not imply lack ofcausation.
TemporalityTemporality is the sine qua non of injury causation, inthat the exposure must precede the injury. Hill onlyrefers to temporality as the basis for making certain thatthe !horse comes before the cart" in general causation.In speci!c causation, however, an additional parameter
themenschwerpunkt
4 Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine ! Springer-Verlag 2011 wmw

of temporality is considered, and that is the latencybetween the exposure and the !rst evidence of theinjury [29]. Evidence of injury presence must not followthe exposure by a time period that is considered toogreat to link the two. Further, the time between theexposure and the !rst evidence of the injury outcomeserves as a basis from which to assess the incidence ofcompeting coincidental causes, as described underStrength of Association.
Biological gradientIn general causation, this refers to the observation thatthe injury or disease outcome increases monotonicallywith increasing dose of exposure. This criterion isparticularly applicable to toxic exposures and at middlelevels of traumatic exposure, but at the extremes ofexposure it is not particularly helpful for assessingcausation. For example, from a general causation per-spective, a fall from 5mwill result in fracturemore oftenthan a fall from 2 m, however there is unlikely to be anappreciable difference in fracture rate between a 200and 300m fall.
For speci!c causation, the criterion of biologicgradient has more limited practical applicability. Whileit can be concluded, as a general principle, that theincidence of injury will generally increase as exposureintensity increases (to a point), injury incidence onlyserves as the numerator of the relative risk assessmentcritical to an evaluation of Strength of Association, andonly has meaning or relevance when compared withmagnitude of the potential competing causes in thedenominator.
PlausibilityFor both general and speci!c causation, plausibilityrefers to the degree to which the observed associationcan be plausibly explained by known scienti!c princi-ples. Hill did not putmuch weight in plausibility, notingthat a hypothesized disease cause that is thought to beimplausible today may be discovered to be plausible atsome time in the future as a result of new scienti!cinquiry. A more accurate to way to characterize thepractical application of the plausibility criterion is that itis met when there is a lack of established implausibility(impossibility). For example, a brain tumor discoveredthe day following a head trauma is implausibly relatedto the trauma due to the nature of the disease and injurymechanisms, respectively. A common error in causa-tion is to consider a rare outcome to be the same as animplausible outcome. Rarity is not the same as implau-sibility, since a particularly rare outcomemay still resultin a large RR favoring the prime causal suspect if the
denominator of competing causes is substantially smal-ler than the incidence numerator.
If a causal correlation is determined solely basedupon the temporal association between an exposureand outcome, but implausibility is well established,then the post hoc ergo propter hoc fallacy has beencommitted. This fallacy is commonly explained usingthe example of the rooster who crows and sees the suncome up and subsequently infers that his crowing wasthe cause of the sunrise. Because the association isimplausible, the rooster#s inference is fallacious.
Just as important, however is the recognition ofthe false assertion of the post hoc fallacy, in which a rareoutcome (low probability) ismistaken for implausibility(0% probability), or implausibility is incorrectly as-serted, and causation is improperly rejected in thepresence of a close temporal relationship betweenexposure and outcome.
CoherenceFor both general and speci!c causation, a causal con-clusion should not fundamentally contradict presentsubstantive knowledge – it should !make sense" givencurrent knowledge. In some ways this criterion is muchlike plausibility. To use the earlier example, a blow tothe head will not cause a tumor to develop overnight, asthis is so far beyond of what is known about thepathophysiology of tumors that it is not a coherentexplanation of cause and effect.
ExperimentIn some cases there may be evidence from randomizedexperiments on animals or humans, in which an expo-sure is removed and there is a corresponding change inthe frequency of the outcome. Experimental evidencefor causation is treated identically in both general andspeci!c causation; when it is present it is helpful, butthe absence of experimental evidence is not evidenceagainst a causal relationship.
AnalogyIn both general and speci!c causations, an analogousexposure and outcome may be translatable to thecircumstances of a previously unexplored causal inves-tigation. Hill noted, as an example of analogy, that thebirth defects that have been investigated and found tobe causally associated with thalidomide or rubella ex-posure make it easier to accept a cause and effectrelationship between another drug or virus for whichthere was less evidence. Evidence of analogy can serveas evidence in favor of plausibility.
themenschwerpunkt
wmw 2011 ! Springer-Verlag Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine 5

Errors of causationTwo errors that can result from a faulty speci!c causa-tion analysis are the acceptance of causation when it isnot present (a Type I or Alpha error), and the rejectionof causation when it is present (Type II or Beta error). AType I error can result from the miscalculation ofrelative risk, resulting in a failure to account for a moreprobable alternative explanation, or from the lack ofacknowledgement of well established implausibilitybetween exposure and outcome. A Type II error resultsfrom either the lack of consideration, or inaccuracy ofthe incidence of alternative explanations (the denomi-nator of the relative risk ratio described below). Further,an erroneous conclusion of implausibility will alsoresult in a Type II error.
Another potential source of error stems from thefact that both forensic biomechanical and forensicepidemiologic analysis of speci!c causation are, inmost instances, dependent upon the accuracy of themedically determined diagnosis as well as the accuracyof the history of the traumatic exposure and onset ofsigns indicative of the injury outcome. In a forensicsetting, unless there is evidence of substantive inaccu-racy in clinical or historical records it cannot be as-sumed that it is present.
Results and discussion
Applied forensic biomechanics and systematicspeci!c causationAs a practical matter, for determinations of speci!ccausation Hill#s criteria can be simpli!ed and groupedinto 2 major categories: criteria that answer the ques-tion !could the exposure have caused the disease orinjury outcome in this case?" (Biologic Plausibility) andthose that answer the question !did the exposure causethe disease or injury outcome in this case?" (CausalAssociation Strength).
Biologic Plausibility – This collective criterion ismeant to assess whether or not the exposure couldreasonably have caused the disease or injury outcome(regardless of how often), and is a composite of thepreviously described plausibility, coherence, speci!ci-ty, consistency, biologic gradient, analogy, and experi-ment criteria. No single factor must be present toestablish biologic plausibility, but it implausibility can-not be a well-established fact.
In injury causation, a forensic biomechanicalanalysis may be useful in evaluating biologic plausi-bility. A description of the magnitude, direction, ma-terial properties, and rate of application of a load
source can help explain how a particular injury mayhave occurred. Caution must be exercised with suchan analysis, however, as it is primarily unidirectional.Plausibility refers to a probability ofmore than 0%, andimplausibility refers to a probability of no greater than0%. A lack of plausibility is neither, and thus implau-sibility (probability" 0%) and lack of plausibility arenot equivalent. From a probabilistic perspective, how-ever, a relationship for which plausibility is unknownis more likely to be plausible (>0%) than implausible(0%).
Hayes et al. have described a metric that theyhave called !biomechanical plausibility" which is in-tended to replace Hill#s plausibility criterion [18].These authors describe biomechanical plausibility asthe ability to demonstrate, using experimental datathat forces from a possible injury event are suf!cient toexceed the injury tolerance such that the injury can besaid to have been !caused" by the event. Conversely,these authors interpret the inability to demonstratebiomechanical plausibility as an indication that theinjury event could not have caused the injury in ques-tion. In drawing this conclusion these authors committhe !fallacy of the transposed conditional" by conclud-ing that the absence of evidence of biomechanicalplausibility of causation is equivalent to evidence ofimplausibility. This conclusion is incorrect and is indirect contradiction of Hill#s conclusion that he was!convinced that [plausibility] is a feature that we can-not demand [in causation]".
Implausibility is only established when causeand effect is ruled out because of the violation of afundamental biologic principle, such as the univer-sally accepted and incontrovertible maxim that headtrauma cannot cause brain tumors to spontaneouslyappear overnight. A lack of experimental biomechan-ical data supporting a plausible relationship betweena loading event and an injury does not equate toevidence of implausibility, but rather stands as a lackof biomechanical evidence of plausibility. This is notan obstacle to a causal analysis, particularly if plau-sibility is bolstered by the presence of coherence andanalogy.
There are several reasons why the inability todemonstrate biomechanical plausibility does notequate to implausibility. Inherent in a determinationof implausibility is a point estimate of 0% probability.The presence of bias and random error in experimentalbiomechanical data limits, to a certain extent, the ex-trapolability of the study results to circumstances andsubjects like those in the experiment. Experimentalbiomechanical studies of animal, cadaver, and human
themenschwerpunkt
6 Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine ! Springer-Verlag 2011 wmw
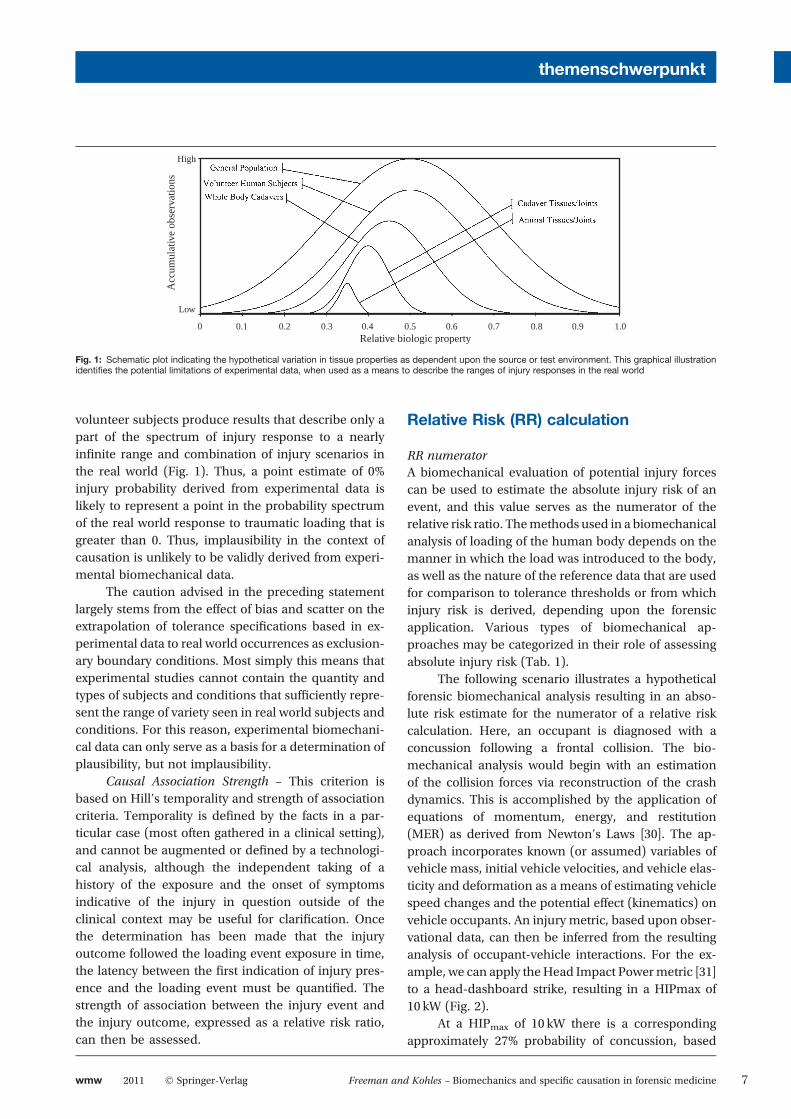
volunteer subjects produce results that describe only apart of the spectrum of injury response to a nearlyin!nite range and combination of injury scenarios inthe real world (Fig. 1). Thus, a point estimate of 0%injury probability derived from experimental data islikely to represent a point in the probability spectrumof the real world response to traumatic loading that isgreater than 0. Thus, implausibility in the context ofcausation is unlikely to be validly derived from experi-mental biomechanical data.
The caution advised in the preceding statementlargely stems from the effect of bias and scatter on theextrapolation of tolerance speci!cations based in ex-perimental data to real world occurrences as exclusion-ary boundary conditions. Most simply this means thatexperimental studies cannot contain the quantity andtypes of subjects and conditions that suf!ciently repre-sent the range of variety seen in real world subjects andconditions. For this reason, experimental biomechani-cal data can only serve as a basis for a determination ofplausibility, but not implausibility.
Causal Association Strength – This criterion isbased on Hill#s temporality and strength of associationcriteria. Temporality is de!ned by the facts in a par-ticular case (most often gathered in a clinical setting),and cannot be augmented or de!ned by a technologi-cal analysis, although the independent taking of ahistory of the exposure and the onset of symptomsindicative of the injury in question outside of theclinical context may be useful for clari!cation. Oncethe determination has been made that the injuryoutcome followed the loading event exposure in time,the latency between the !rst indication of injury pres-ence and the loading event must be quanti!ed. Thestrength of association between the injury event andthe injury outcome, expressed as a relative risk ratio,can then be assessed.
Relative Risk (RR) calculation
RR numeratorA biomechanical evaluation of potential injury forcescan be used to estimate the absolute injury risk of anevent, and this value serves as the numerator of therelative risk ratio. Themethods used in a biomechanicalanalysis of loading of the human body depends on themanner in which the load was introduced to the body,as well as the nature of the reference data that are usedfor comparison to tolerance thresholds or from whichinjury risk is derived, depending upon the forensicapplication. Various types of biomechanical ap-proaches may be categorized in their role of assessingabsolute injury risk (Tab. 1).
The following scenario illustrates a hypotheticalforensic biomechanical analysis resulting in an abso-lute risk estimate for the numerator of a relative riskcalculation. Here, an occupant is diagnosed with aconcussion following a frontal collision. The bio-mechanical analysis would begin with an estimationof the collision forces via reconstruction of the crashdynamics. This is accomplished by the application ofequations of momentum, energy, and restitution(MER) as derived from Newton#s Laws [30]. The ap-proach incorporates known (or assumed) variables ofvehicle mass, initial vehicle velocities, and vehicle elas-ticity and deformation as a means of estimating vehiclespeed changes and the potential effect (kinematics) onvehicle occupants. An injury metric, based upon obser-vational data, can then be inferred from the resultinganalysis of occupant-vehicle interactions. For the ex-ample, we can apply theHead Impact Powermetric [31]to a head-dashboard strike, resulting in a HIPmax of10 kW (Fig. 2).
At a HIPmax of 10 kW there is a correspondingapproximately 27% probability of concussion, based
High
Low
0 0.1 0.2 0.3 0.4 0.5 0.6Relative biologic property
Acc
umul
ativ
e ob
serv
atio
ns
0.7 0.8 0.9 1.0
Fig. 1: Schematic plot indicating the hypothetical variation in tissue properties as dependent upon the source or test environment. This graphical illustrationidenti!es the potential limitations of experimental data, when used as a means to describe the ranges of injury responses in the real world
themenschwerpunkt
wmw 2011 ! Springer-Verlag Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine 7
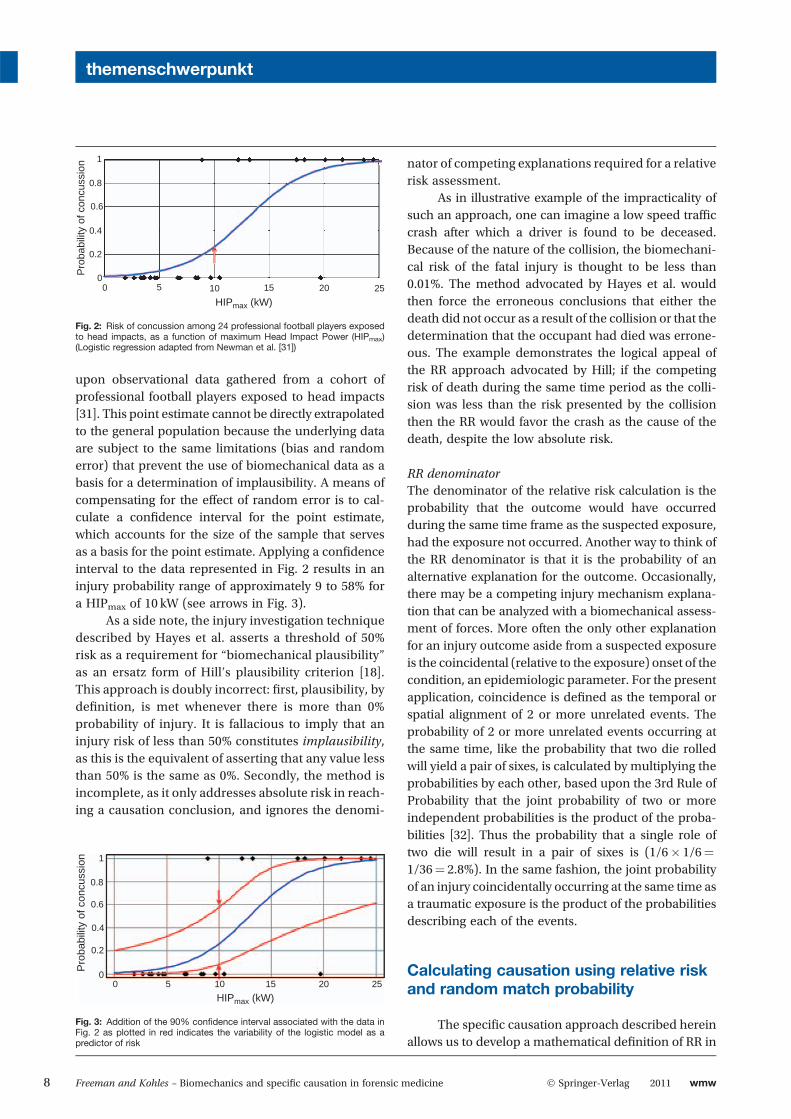
upon observational data gathered from a cohort ofprofessional football players exposed to head impacts[31]. This point estimate cannot be directly extrapolatedto the general population because the underlying dataare subject to the same limitations (bias and randomerror) that prevent the use of biomechanical data as abasis for a determination of implausibility. A means ofcompensating for the effect of random error is to cal-culate a con!dence interval for the point estimate,which accounts for the size of the sample that servesas a basis for the point estimate. Applying a con!denceinterval to the data represented in Fig. 2 results in aninjury probability range of approximately 9 to 58% fora HIPmax of 10 kW (see arrows in Fig. 3).
As a side note, the injury investigation techniquedescribed by Hayes et al. asserts a threshold of 50%risk as a requirement for !biomechanical plausibility"as an ersatz form of Hill#s plausibility criterion [18].This approach is doubly incorrect: !rst, plausibility, byde!nition, is met whenever there is more than 0%probability of injury. It is fallacious to imply that aninjury risk of less than 50% constitutes implausibility,as this is the equivalent of asserting that any value lessthan 50% is the same as 0%. Secondly, the method isincomplete, as it only addresses absolute risk in reach-ing a causation conclusion, and ignores the denomi-
nator of competing explanations required for a relativerisk assessment.
As in illustrative example of the impracticality ofsuch an approach, one can imagine a low speed traf!ccrash after which a driver is found to be deceased.Because of the nature of the collision, the biomechani-cal risk of the fatal injury is thought to be less than0.01%. The method advocated by Hayes et al. wouldthen force the erroneous conclusions that either thedeath did not occur as a result of the collision or that thedetermination that the occupant had died was errone-ous. The example demonstrates the logical appeal ofthe RR approach advocated by Hill; if the competingrisk of death during the same time period as the colli-sion was less than the risk presented by the collisionthen the RR would favor the crash as the cause of thedeath, despite the low absolute risk.
RR denominatorThe denominator of the relative risk calculation is theprobability that the outcome would have occurredduring the same time frame as the suspected exposure,had the exposure not occurred. Another way to think ofthe RR denominator is that it is the probability of analternative explanation for the outcome. Occasionally,there may be a competing injury mechanism explana-tion that can be analyzed with a biomechanical assess-ment of forces. More often the only other explanationfor an injury outcome aside from a suspected exposureis the coincidental (relative to the exposure) onset of thecondition, an epidemiologic parameter. For the presentapplication, coincidence is de!ned as the temporal orspatial alignment of 2 or more unrelated events. Theprobability of 2 or more unrelated events occurring atthe same time, like the probability that two die rolledwill yield a pair of sixes, is calculated by multiplying theprobabilities by each other, based upon the 3rd Rule ofProbability that the joint probability of two or moreindependent probabilities is the product of the proba-bilities [32]. Thus the probability that a single role oftwo die will result in a pair of sixes is (1/6# 1/6"1/36" 2.8%). In the same fashion, the joint probabilityof an injury coincidentally occurring at the same time asa traumatic exposure is the product of the probabilitiesdescribing each of the events.
Calculating causation using relative riskand random match probability
The speci!c causation approach described hereinallows us to develop a mathematical de!nition of RR in
1
0.8
0.6
0.4
0.2
00 5 10 15
HIPmax (kW)
Pro
babi
lity
of c
oncu
ssio
n
20 25
Fig. 3: Addition of the 90% con!dence interval associated with the data inFig. 2 as plotted in red indicates the variability of the logistic model as apredictor of risk
1
0.8
0.6
0.4
0.2
00 5 10 15 20 25
HIPmax (kW)
Pro
babi
lity
of c
oncu
ssio
n
Fig. 2: Risk of concussion among 24 professional football players exposedto head impacts, as a function of maximum Head Impact Power (HIPmax)(Logistic regression adapted from Newman et al. [31])
themenschwerpunkt
8 Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine ! Springer-Verlag 2011 wmw

order to answer the question !did exposure A causecondition B?" by comparing all of the known and po-tential causes of B given the temporal relationshipbetween A and B. Here, the probability that a conditionB resulted from a !prime causal suspect" As out of nknown alternative causes plus the in"uence of coinci-dence can be represented with the following RR calcu-lation for the causal relationship of $BjAs%:
relative risk $B Asj % " P$B Asj %Pn
i"1 P$BjAai% ! P$Bj Act2 %
!
in which P$B Asj % is the probability of the diagnosedcondition B given exposure to prime causal suspect As;Pn
i"1 P$BjAai% is the sum of the risk of all known alter-native plausible causes of B occurring in the same timeframe as As as i goes from 1 to n alternative causes; andP$BjAc=t2% is the probability of the coincidental occur-rence of B per the time span between prime causalsuspect As and the !rst clinical sign of condition B,designated as t. Taking into account the joint probabil-ity of the temporal alignment of (theoretically indepen-dent) events As and B, the t2 factor in the denominatorrepresents the random match probability associatedwith coincidental cause Ac. The resulting algorithmprovides a metric for assessing the relative nature ofcausal in"uences while taking into account the biome-chanically or epidemiologically derived injury risk va-lues in the numerator of the RR calculation as well asthe duration of time between exposure to the primecausal suspect and the injury outcome.
Example: causal analysis of forensicbiomechanics data
An example of a common application of bio-mechanical analysis in a forensic setting is the analysisof a claimed intervertebral disk injury following amotorvehicle crash or other trauma. Various features of suchinjuries can complicate a clinical determination ofcausation, as both disk and simple spinal strain injuriesmay initially result in similar clinical presentations.Thus, there is a reasonable appeal to quantifying thebiomechanical risk of injury in the collision as anadjunct to clinical causation. The dif!culty in such ananalysis arises because of the potential for widevariation in the pre-collision condition of the interver-tebral disk; variation that results from the nearlyuniversal prevalence of age-related degenerativechanges in the disk nucleus and annulus. Additionally,a precise or even rough estimate of the magnitude,
direction, and rate of load sustained at a given disklevel may be virtually impossible to determine given thenumber of unknown variables required to accuratelyreconstruct the intraspinal loads induced by thecollision.
If an injury risk can be reliably estimated from abiomechanical analysis, then this probabilistic valuecould be used in the numerator of the RR calculationonce implausibility of the prime causal suspect is re-jected; thus (P$B Asj % „ 0). If there are no known com-peting discrete traumatic causes of disk injury withinthe relevant timeframe, then
Pni"1 P$BjAai% " 0. Thus,
the only comparative risk to be included in the denom-inator is that of the insidious onset of a symptomaticdisk derangement that simply coincided with the colli-sion (P$BjAc=t2% „ 0).
To further develop this example, we hypothesize arear impact collision with the following facts: the dam-age to the vehicle was con!ned to the rear bumper, andthe reconstructed speed of the collision was <16 km/h.The driver was a 40-year-old male with a prior historyof neck pain and a presumed (non-imaged) cervical(C5–C6) disk injury three years prior to the collision, butno treatment for the three years prior to the collision.The man develops neck and right arm pain within onehour of the collision, and within one week is diagnosedwith a C5–C6 disk herniation based on a magneticresonance imaging scan. What is the causal RR forthe disk injury (B) and the prime causal suspect, thecollision (As)?
A review of similar collisions and injuries in theNational Automotive Sampling System (NASS) of theU.S. National Highway Traf!c Safety Administrationreveals a very low incidence of cervical disk injury inrear impact collisions of <16 km/h; slightly morethan 1 in 2000 collisions or 0.05% [33]. This is nota population-based rate as the NASS database onlyincludes collisions in which at least one vehicle wastowed away, and only includes diagnoses that areevident in the !rst few days following the collision.The actual population-based risk of cervical diskinjury under similar crash circumstances is likely4–10 times greater than what is seen in the NASSdatabase. However, the use of such a low incidencefor P$B Asj % in the numerator helps avoid a Type Istatistical error, in which causation is erroneouslyfound when it is not present. It is important to notethat the biomechanical analysis of the crash forceson the occupant is limited to quanti!cation ofthe collision severity, as there are too many un-known variables to allow for a reliable quanti!cationof the forces at the C5–C6 disk.
themenschwerpunkt
wmw 2011 ! Springer-Verlag Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine 9

For the denominator, the evidence given for theexample assumes there are no known competing injurycauses outside of the coincidental onset of symptomswithin the single hour following the collision, and soPn
i"1 P$BjAai% " 0. Thus, the probability that the driverwould have developed neck pain indicative of a diskinjury in the hour following the collision had the colli-sion not occurred is arrived at using the randommatchcalculation described earlier. As an estimate in the roleof coincidence, we !rst must have some idea of the riskof the condition occurring over some period of time (t)during which it is assumed that the man#s risk wasstable and constant (rather, there is no evidence thatit was not stable and constant). It is reasonable toassume that a 40-year-old man#s risk of developing asymptomatic disk injury would be relatively stablewithin the period of the year prior to the collision basedon his daily driving patterns. Thus the annual preva-lence of disk injury inmale drivers in this age group canbe used for the denominator. Unfortunately, there areno reliable values for the annual prevalence of diskinjury; however, the annual prevalence of any episodeof neck pain is estimated at an average of 37.2% acrossa number of studies and populations [34]. Using theprevalence of the far more common condition of neckpain rather than cervical disk injury further reduces theprobability of a Type I error. Finally, because the one-hour post collision timeframe is a contribution to thecausation assessment, we need to consider any one ofthe t" 8,760 hours in a year as a possible coincidentaloccurrence of the injury. Thus the RR calculation forthis biomechanical example is:
relative risk$disk injuryj16 km=h crash%
" 0:05%
0! 37:2%8760 h$ %2
! "
0
@
1
A " 103;142
The resulting odds of 103,142 to 1 are the relativerisk in favor of the subject collision having caused thedisk injury, taking into account the competing explana-tion of coincidence. For presentation in a forensicsetting this is the equivalent of >99.99% probability ofcausation. From this example it is evident that thetemporal proximity between the injury exposure andthe relevant symptom onset (here 1 hour) plays acritical role in the assessment of causation because ofthe randommatch calculation. For the sake of compar-ison, if the symptom onset in the example had beendelayed by 2 days, the RR odds in favor of causationwould have dropped to 45 to 1 or 97.8% as the mostprobable cause.
The preceding example helps to indicate the lim-itations in the approach advocated by Walz and Muserand others, when they suggest that knowledge of occu-pant position, restraint use, etc., provides the primarybasis for assessing the probability that a claimed!whiplash" injury actually resulted from a particularcollision [14]. Without accounting for the risk of thesymptoms indicative of injury absent the collision aswell as the temporal proximity between the collisionand the onset of symptoms, the biomechanics-onlyderived injury risk plays a relatively minor role in thedetermination of cause and effect.
Conclusion
Forensic biomechanical analysis is a useful ad-junctive tool in forensic medicine, however limitationsin its usemust be acknowledged and heeded, otherwisethe potential for erroneous application arises. Whenapplied to questions of causation, biomechanical as-sessment of injury risk has a place within a frameworkof forensic epidemiologic analysis of causation, basedupon a systematic approach to causation !rst laid outby Hill in 1965. These two forensic disciplines (biome-chanics and epidemiology) are complimentary and canserve as a reliable means of quantifying the probabilityof cause and effect in disputed matters.
Con"ict of interest
Both authors provide forensic consultation inmatters that include the application of epidemiologicand biomechanical concepts and analysis to disputedissues.
References[1] Nahum AM, Melvin JW. Accidental injury: biomechanics and pre-
vention, 2nd edn. Springer, New York, 2002.[2] Freeman MD, Kohles SS. Applications and limitations of Forensic
Biomechanics: a Bayesian perspective. J Forensic LegMed, 17: 67–77,2010.
[3] Tencer AF, Kaufman R, Ryan K, et al. Femur fractures in relatively lowspeed frontal crashes: the possible role of muscle forces. Accid AnalPrev, 34: 1–11, 2002.
[4] Szklo M, Nieto FJ. Epidemiology: beyond the basics, 2nd edn. Jonesand Bartlett Publishers, Boston, 2007.
[5] Freeman MD, Rossignol AC, Hand ML. Forensic epidemiology: asystematic approach to probabilistic determinations in disputedmatters. J Forensic Leg Med, 15: 281–290, 2008.
[6] Loue S. Forensic epidemiology: integrating public health and lawenforcement. Jones and Bartlett Publishers, Boston, 2010.
[7] Kehm v. Proctor and Gamble Manufacturing Company, 724 F.2d 613(8th Cir.), 1983 [supreme.justia.com].
[8] United States v. Migliorini, 521 F. Supp. 1210, 1218 (M.D. FL), 1981[supreme.justia.com].
[9] United States v. Bygrave, 46 M.J. 491 (Ct. App. Armed Forces), 1997[supreme.justia.com].
themenschwerpunkt
10 Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine ! Springer-Verlag 2011 wmw

[10] United States v. Moore, 846 F.2d 1163 (8th Cir.), 1988[supreme.justia.com].
[11] State v. McKnight, 576 S.E.2d 168 (S.C.), 2003 [supreme.justia.com].[12] Ohio Administrative Code xx 3701-52-01, -02, -09, 2008
[supreme.justia.com].[13] Robbins DH, Melvin JW, Huelke DF, et al. Biomechanical accident
investigation methodology using analytic techniques. SAE 831609.Society of Automotive Engineers, Warrendale, PA, 1983.
[14] Walz FH, Muser MH. Biomechanical assessment of soft tissuecervical spine disorders and expert opinion in low speed collisions.Accident Anal Prevent, 32: 161–165, 2000.
[15] Nahum AM, Gomez MA. Injury reconstruction: the biomechanicalanalysis of accidental injury. SAE 940568. International Congress &Exposition, Warrendale, PA, Society of Automotive Engineers,1994.
[16] King AI. Fundamentals of impact biomechanics: Part I – Biomechan-ics of the head, neck, and thorax. Annu Rev Biomed Eng, 2: 55–81,2000.
[17] King AI. Fundamentals of impact biomechanics: Part 2 – Biomechan-ics of the abdomen, pelvis, and lower extremities. Annu Rev BiomedEng, 3: 27–55, 2001.
[18] Hayes WC, Erickson MS, Power ED. Forensic injury biomechanics.Annu Rev Biomed Eng, 9: 55–86, 2007.
[19] Rothman KJ, Greenland S. Causation and causal inference in epide-miology. Am J Public Health, 95(Suppl. 1): S144–S150, 2005.
[20] Mill JS. A system of logic, ratiocinative and inductive, 5th edn.London, England, Parker, Son and Bowin, 1862. Cited in Clark DW,MacMahon B. Preventive and community medicine, 2nd edn.Boston, Little, Brown, 1981.
[21] Hume D. A treatise of human nature. (Originally published in 1739)Oxford University Press edition, with an Analytical Index by L. A.Selby-Bigge, published 1888. Second edition with text revised andnotes by P. H. Nidditch, 1978.
[22] Hill AB. The environment and disease: association or causation?Proc Roy Soc Med, 5: 295–300, 1965.
[23] Morabia A. On the origin of Hill#s causal criteria. Epidemiology, 2:367–369, 1991.
[24] van Reekum R, Streiner DL, Conn DK. Applying Bradford Hill#scriteria for causation to neuropsychiatry: challenges and opportu-nities. J Neuropsychiatry Clin Neurosci, 13: 318–325, 2001.
[25] Lozano-Calderón S, Anthony S, Ring D. The quality and strength ofevidence for etiology: example of carpal tunnel syndrome. J HandSurg Am, 33: 525–538, 2008.
[26] Batty L, Holland-Elliott K, Rosenfeld D. Investigation of eye splashand needlestick incidents from anHIV-positive donor on an intensivecare unit using root cause analysis. Occup Med (Lond), 53: 147–150,2003.
[27] Freeman MD, Centeno CJ, Kohles SS. A systematic approach toclinical determinations of causation in symptomatic spinal diskinjury following motor vehicle crash trauma. PM R, 1: 951–956, 2009.
[28] Trichopoulos D, Kalandidi A, Sparros L, et al. Lung cancer andpassive smoking. Int J Cancer, 27: 1–4, 1981.
[29] Kohles SS, Freeman MD. Mathematical models characterizing theprobability of trigger event, ambient-risk, and coincidental in"u-ences on inductive and abductive conclusions of speci!c causa-tion. Ann Epidemiol, 20(9): 713–714, 2010.
[30] Costanzo F, Plesha ME, Gray GL. Engineering mechanics: staticsand dynamics. McGraw-Hill Higher Education, Boston, 2010.
[31] Newman JA, Shewchenko N, Welbourne E. A proposed new bio-mechanical head injury assessment function – the maximum powerindex. Stapp Car Crash J, 44: 215–247, 2000.
[32] Taroni F, Aitken C, Garbolino P, et al. Bayesian networks andprobabilistic inference in forensic science. Statistics in practice. JohnWiley, Chichester, 2006.
[33] FreemanMD, Centeno CJ. Etiologic and demographic characteristicsof traf!c crash-related disc injuries. Spine J, doi: 10.1016/j.spinee.2008.06.373.
[34] Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in theworld population: a systematic critical review of the literature. EurSpine J, 15: 834–848, 2006.
[35] Whittle K, Kieser J, Ichim I, et al. The biomechanical modelling ofnon-ballistic skin wounding: blunt-force injury. Forensic Sci MedPathol, 4: 33–39, 2008.
[36] Tencer AF, Huber P, Mirza SK. A comparison of biomechanicalmechanisms of whiplash injury from rear impacts. Annu Proc AssocAdv Automot Med, 47: 383–98, 2003.
[37] Duma SM, Ng TP, Kennedy EA, et al. Determination of signi!cantparameters for eye injury risk from projectiles. J Trauma, 59: 960–964,2005.
[38] Provenzano PP, Lakes RS, Corr DT, et al. Application of nonlinearviscoelastic models to describe ligament behavior. Biomech ModelMechanobiol, 1: 45–57, 2002.
[39] Roy R, Kohles SS, Zaporojan V, et al. Bending behavior of nativeand engineered, auricular and costal cartilage. J Biomed Matls Res,68A: 597–602, 2004.
themenschwerpunkt
wmw 2011 ! Springer-Verlag Freeman and Kohles – Biomechanics and speci!c causation in forensic medicine 11
C
AoFMS
CvgnroclirItpcbtt
I
Tdnpfstncsanrcdrbtdepcr
P1
P
linical Review: Focused
Systematic Approach to Clinical Determinationsf Causation in Symptomatic Spinal Disk Injuryollowing Motor Vehicle Crash Traumaichael D. Freeman, PhD, MPH, DC, Christopher J. Centeno, MD,
ean S. Kohles, PhD
MvUASfD
CsD
SElD
DC
linical determinations of causation in cases of intervertebral disk (IVD) injury after a motorehicle crash (MVC) are often disputed in medicolegal settings. No published systematicuidelines exist for making such determinations, which has resulted in infringement byonclinical personnel into injury causation evaluations, a traditionally clinical activity. Theesult is causal determinations that are potentially disconnected from clinical observationsf injury. The purpose of this review was to evaluate the current literature on causation,ausal determinations after trauma and IVD injury after MVC, and to develop a practicable,ogical, and literature-based approach to causation determinations of symptomatic IVDnjury after MVC. The results of the review indicate IVD injury can result from any MVCegardless of magnitude, thus meeting the first criteria of causation, biologic plausibility.ndividual determinations of causation depend entirely on the temporal association be-ween the collision and the symptom onset (the second criterion) and a lack of a morerobable explanation for the symptoms (the third). When these causal elements are met,linicians can assert causation on a “more probable than not” or “reasonable probability”asis. Because of a lack of an established or reliable relationship between collision force andhe probability of IVD injury the investigation of collision parameters is not a useful adjuncto causal determinations.
NTRODUCTION
he origin of injury to the intervertebral disks (IVD) of the spine is a common source ofispute in medicolegal circumstances. Whereas treating clinicians typically make determi-ations of causal relationships between a trauma and an injury primarily based on theatient-related history of the traumatic event and the onset of symptoms, opposing expertsrequently rely on population-based assumptions as a basis for disputing causal relation-hips. This scenario is observed most often when disk injuries and symptoms are attributedo motor vehicle crashes (MVC), because many crash-related injuries result from theegligence of another driver; thus, the nature and extent of an occupant’s injuries may beontested. There is typically a strong third-party (insurer) interest in minimizing compen-atory payments on behalf of the individuals who are at fault for the crash. As a result, andversarial system has developed in the United States and many other industrializedations, with the injured patient and his or her treating physicians on one side and the partyesponsible for the crash, his or her insurer, and the insurer’s medical and scientificonsultants on the other side [1,2]. Although some clinicians prefer to avoid causaleterminations altogether, it can be argued that such determinations are part and parcel ofegular medical care. To avoid such a determination solely because it may be later disputedy a party with interests opposing those of the patient is to avoid a duty to the patient; a dutyhat can have a significant impact on the patient’s well-being. This is not to say thatissemblance and fraud do not exist in the patient population; however, when there is novidence of dishonesty, there is no reason to assume the presence of fraud simply because aatient is claiming injury after a MVC that was caused by another’s negligence (the mostommon setting for a legal claim for monetary damages). Such events are, for the most part,
andomly distributed in the population that uses motor vehicles and not selective for peopleSa
M&R © 2009 by the American Academy of Physical Me934-1482/09/$36.00
rinted in U.S.A. D
.D.F. Department of Public Health and Pre-entive Medicine, Oregon Health & Scienceniversity School of Medicine, Portland, OR.ddress correspondence to: M.D.F., 205 Libertyt., NE, Suite B, Salem, OR 97301; e-mail:[email protected]: 5B, expert witness
.J.C. Spinal Injury Foundation, Westmin-ter, COisclosure: 5B, expert witness
.S.K. Department of Mechanical & Materialsngineering, Portland State University, Port-
and, ORisclosure: nothing to disclose
isclosure Key can be found on the Table ofontents and at www.pmrjournal.org
ubmitted for publication April 21, 2009;ccepted July 22.
dicine and RehabilitationVol. 1, 951-956, October 2009
OI: 10.1016/j.pmrj.2009.07.009951

igttst[
ninhccdmscaotEapc
tsdtataanm
cbsap
P
Dpdssesgvcds
ioccocwctlc
bHrcsbFpoMriatqodw
1
2
952 Freeman et al SYSTEMATIC APPROACH TO DISK INJURY CAUSATION
n whom fraudulent behavior is more common. When alle-ations of fraud are made in a medicolegal context, despitehe absence of evidence of fraud, it is reasonable to questionhe motivation behind the assertion, because forensic con-ultants who provide partisan opinions are no more immuneo secondary gain pressures than are litigants claiming injury3].
There are some authors who maintain that for a determi-ation of cause and effect to be made between a diagnosed
njury and an MVC, a biomechanical analysis of the forces isecessary to determine whether or not a particular collisionad the potential to cause the injuries [4] or that a detailedrash reconstruction is necessary before a causal associationan be determined [5]. In contrast, most authors who haveocumented IVD injuries associated with an MVC make noention of a biomechanical force analysis or a crash recon-
truction [6,7]. The latter approach is most typical of thelinically pragmatic approach to causation. If it is known thatn injury can be caused by a trauma, then there is no practicalr logical purpose served in quantifying the degree of therauma in order to assess the risk of injury after the event.ven injuries that are deemed highly unlikely or improbablere by definition still slightly likely or possible, and thus injuryresence is typically evaluated after the fact clinically, and notalled into question by a post-hoc suggestion of infrequency.
For the purposes of the present inquiry, a Medline search forhe years 1980 through 2009 (as of July 2009) using the medicalubject headings (MeSH) terms intervertebral disk, intervertebralisk displacement, and disk, herniated as well as the non-MeSHerms cervical disk, in conjunction with “injury” and/or “trauma,”long with “cause,” “causal,” and “causation” in various combina-ions did not elicit any publications that addressed an organizedpproach to determinations of causation between disk injurynd MVC exposure. It appears that, at the present time, there iso widely accepted scientific or clinical standard for such deter-inations.The purpose of this article is to assess the evidence for the
ausal relationship between disk injury and MVC traumaased on the published literature on causal standards and thecience of both disk injury and MVC trauma. Further, theuthors propose a systematic and scientifically based ap-roach to individual determinations of causation.
RIOR PUBLICATIONS ON CAUSATION
eterminations of causal association between a noxious ex-osure (microorganism, chemical, trauma, or other) and aisease or injury outcome in populations is an area of con-iderable interest to epidemiologists and others who studyuch issues. Individual clinical observations of cause andffect can serve as a reasonable basis for a case study anduggestion of a relationship. It is, however, difficult to draweneralizable conclusions from such reports. Case series pro-ide stronger evidence of causation; however, without aontrol group of unexposed subjects, there is no way toetermine which effects can be isolated to a particular expo-
ure. Even when case-control studies, in which diseased ornjured subjects are compared with healthy subjects for levelf exposure to a suspected noxious agent, show positiveorrelations between exposure and disease or injury out-ome, the results cannot be interpreted as validated evidencef a causal relationship, as confounding factors may exist thatan obscure true relationships. An example of confoundingould be the relationship between coffee drinking and lung
ancer. Coffee drinkers may have a higher rate of lung cancerhan non-coffee drinkers, but only because smokers are moreikely to drink coffee than nonsmokers, not because coffee isausally linked to lung cancer.
In an attempt to more clearly identify causal relationshipsetween noxious exposures and outcomes in populations,ill outlined a set of 9 criteria that needed to be considered to
easonably conclude that a particular noxious exposureould result in a particular disease [8]. Hill’s criteria haveerved as a kind of seminal gold standard, in that they haveeen adopted and modified by many others, including theood and Drug Administration, academic investigators, andharmaceutical companies, as a means of approaching issuesf causation systematically [9]. Based in part on Hill’s work,iller et al proposed a 4-stage process for identifying envi-
onmentally caused rheumatic disorders, an application thats more applicable to the goals of this article, because itllowed for assessments of causation in individuals ratherhan as a population-based construct [10]. McLean subse-uently adapted Miller et al’s work for causation in instancesf fibromyalgia after MVC [11]. All causal criteria can beistilled to a minimum of 3 common and essential elements,hich are as follows [12,13].
. There must be a biologically plausible or possible linkbetween the exposure and the outcome. For example,trauma and fracture are plausibly linked, but trauma andleukemia are not. Plausibility is a low threshold that isexceeded with relatively weak evidence, such as fromsmall observational studies (case studies or case serieswith small numbers of subjects) or from the results ofwell-designed experiments with many subjects. Biologicplausibility only pertains to whether an outcome canpossibly result from an exposure, and is unrelated to therate or frequency of the outcome. Thus, evidence of lowincidence is not evidence of biologic implausibility.
. There must be a temporal relationship between the expo-sure and the outcome. The outcome cannot preexist theexposure; however, the outcome of interest may havepreexisted the exposure in a less severe form that wasworsened by the exposure. Such a determination requiresan accurate documentation of the signs and symptoms ofthe condition of interest both before and after the expo-sure of interest. Additionally, the outcome cannot post-date the exposure by a period that is considered, from aclinical perspective, to be too long or too short to relatethe two. This determination is highly dependent on thespecifics of any case. For example, an injury to a nerveroot may cause immediate pain, but electromyogram
changes may lag behind by weeks or months. The deter-
3
AM
Icimiacodi
1
2
1
2
l
1
2
C
Bdr
953PM&R Vol. 1, Iss. 10, 2009
mination of reasonable temporal association is typicallymade as a matter of clinical judgment, rather than fromclearly delineated guidelines or principles.
. There must not be a more likely or probable alternativeexplanation for the symptoms. The term “likely” is ofgreatest importance, as, for example, it is not sufficient tosimply point out that a patient with back pain after traumais obese, that obesity is related to back pain, and thus it ismore likely that the obesity rather than the trauma causedthe back pain. For an alternative etiologic explanation tobe considered more likely than an alleged exposure it mustbe both biologically plausible and have a stronger tempo-ral relationship to the onset of symptoms than the allegedexposure. If plausibility is present and temporality isrelatively comparable, then 2 exposures can be comparedby examining the dose-response (intensity) of each expo-sure. Such a comparison may involve an analysis of theforces of the exposure as well as an epidemiologic assess-ment of injury frequency associated with the forces, and isbeyond the scope of a clinical assessment of causation.
Causation Algorithm for Disk Injury afterVC
n this section, the authors present a practical guideline forlinical determinations of causation in symptomatic disknjuries after an MVC, based on the application of the afore-
entioned 3 causal elements to the facts and findings in anndividual case. The following definitions and assumptionsre made. An IVD injury is defined by all of the followingharacteristics [14,15] (for this definition, “injury” is usednly to define a disk that has become symptomatic after aiscrete loading event of any magnitude, and the cause of the
njury is not addressed).
. It is symptomatic. This may include classic symptoms ofsegmentally appropriate radiculopathy, regional axialpain, or diskogenic referral of pain in a nondermatomaldistribution.
. There is clinical imaging evidence (magnetic resonanceimaging [MRI], computed tomography, or diskography)that the symptomatic disk fits the generally accepteddefinition of a degenerative/traumatic disk [14]. This in-cludes anular tears, herniations, and degeneration. Al-though there are findings specific to disk trauma, such asvertebral endplate fracture and edema presence in themarrow adjacent to the endplate, many traumaticallyinitiated disk injuries are indistinguishable from degener-ative changes in the disk [16]. Because of mediocre sen-sitivity and specificity (ie, true- and false-positive rates),imaging findings alone are insufficient evidence for eithera causal or noncausal determination in a case of suspectedor disputed traumatic disk injury [17,18].
MVC trauma is defined as follows.
. The patient was an occupant of a motor vehicle at the time
of a collision or event. s. The collision or event transmitted a force through thepatient’s spine over a very short time, typically 70-120 ms[19]. Note that the magnitude of the force is not addressedin the definition, because any degree of forceful loadingcould potentially produce a symptomatic disk injury in asufficiently susceptible individual.
There are 2 most likely scenarios in which a forcefullyoaded IVD may become symptomatic.
. A healthy disk with little or no changes associated withdegeneration is subjected to a significant load resulting indisruption of the annulus and possibly instantaneousmigration of nuclear material posteriorly toward the diskperiphery and into the epidural space or the lateral re-cesses. This is the scenario most likely to produce injuryto tissue surrounding the disk, including vertebral end-plate fracture and ligamentous disruption, and is mostlikely to be associated with higher energy crashes withsignificant vehicle damage [20].
. A degenerated disk (defined as a disk in which one ormore of the following are present to some degree: desic-cation, fibrosis, narrowing of the disk space, diffuse bulg-ing of the anulus beyond the disk space, anular tears,endplate sclerosis, and osteophytes at the vertebralapophyses [14]) is loaded in a manner that initiates asymptomatic response. A significant proportion of theasymptomatic population has some degree of disk degen-eration as seen on MRI; Matsumoto et al have performedthe largest study to date on the topic, with MRI scans ofthe cervical spines of 497 asymptomatic subjects [21].These authors describe a progressive direct relationshipbetween the presence and severity of degenerativechanges and age, with the disk degeneration noted in arange of 17% men and 12% of women in their 20s to 86%and 89% of men and women older than 60 years. Otherauthors have described similar findings with broad rangesof values depending on the age of the subjects; fromvirtually no disk degeneration in subjects �30 years ofage, to 14% in those 30-40, and 62% in subjects �40years of age [22,23]. Similar observations have been pub-lished with regard to lumbar spine degeneration amongasymptomatic patients. Jensen et al described a cohort of98 subjects who underwent lumbar MRI, noting that only36% of subjects had no abnormal disks. Fifty-two percentof the scans were interpreted as having a bulge at aminimum of one level, 38% had abnormality at more thanone level, 27% had a protrusion, and 1% had an extrusion[24]. These findings are consistent with those reported byother authors [25].
ausal Elements
iologic Plausibility. Can an MVC of any severity cause aisk injury? Crash testing of intact cadavers at accelerationsecorded for no-damage rear-impact collisions has demon-
trated IVD injury that cannot be detected by conventional
icsl[dptigvtiam
amtseccs(
TidcTdcsMcwipsovsopaadanidm
cai
hspidititdodcocsc
rgdtfwoat
scaamwMtcccb[psrmcmc
tpoabi
954 Freeman et al SYSTEMATIC APPROACH TO DISK INJURY CAUSATION
maging such as CT and MRI [26]. Although the biomechani-al literature on experimental loading of disks in cadavericled testing has demonstrated disk injuries even in relativelyow accelerations (3.3 and 4.5 times the force of gravity or “g”26]), such ex vivo testing of healthy disks does little toemonstrate minimal thresholds for injury in live humanopulations exposed to real-world crashes. No cadavericesting can duplicate the significant variation in the mannern which loads are transmitted to the human spine in a MVC,iven the variation in occupant position, restraint systems,ehicle interiors, and muscle loads. Additionally, the poten-ial for variation in the condition of an individual IVD,ncluding the ability of the disk to resist forceful loading fromn external source, is too large to ever define in an experi-ental setting.A relevant literature search revealed a complete absence of
ny publications suggesting that symptomatic IVD derange-ent cannot result from MVC exposure of any magnitude. To
he contrary, injury to the disks of the cervical and lumbarpine has been documented in the relatively low level accel-rations associated with little to no-damage collisions, rolleroaster rides, and even sneezing [27-30]. It is reasonable toonclude, as a general precept, that the forceful loading of thepine that can occur in any MVC is a biologically plausiblepossible) cause of symptomatic disk injury.
emporal Association. Temporality is the strongest ev-dence of causation in evaluating the patient with post-MVCisk injury. It must be first established that the MVC pre-eded the onset of symptoms attributed to the disk injury.he exception to this rule is when a previously symptomaticisk is exacerbated by an MVC to the point that the course ofare is significantly altered (ie, a previously diagnosed non-urgical disk condition becomes surgical directly after anVC). In such cases, the determination must be made clini-
ally as to whether the disk symptoms were likely to haveorsened to the point that the surgical intervention was
nevitable absent the MVC. The mere fact that the disk wasreviously symptomatic is not sufficient to draw the conclu-ion that it would have required surgery, given the goodutcomes for patients with diskogenic symptoms who use aariety of surgical and nonsurgical treatments [31-33]. Theymptom onset must be in reasonable proximity to the timef the MVC; however, disk injury symptoms may initiallyresent as identical to symptoms of spinal strain or sprain,nd it may be weeks or months before an MRI is performednd the disk injury diagnosis is first seen [34]. Additionally,isk injury symptoms may be progressive, as an injury to thennulus may progressively allow nuclear migration towardeurologic structures over a period of time while the patient
s in weight bearing and active. Determinations as to whetherelayed symptoms fulfill the temporal association criteriaust be made by clinicians on a case-by-case basis.An obvious weakness of the temporality criterion is that it
an only be established from the history given by the patient,nd patient histories can be erroneous or falsified. The former
s unlikely in the case of injury, however, because one of the callmarks of injury is that there is a close temporal relation-hip between cause and effect (this lack of clear temporalroximity in repetitive traumatic exposures is the reason that
njuries such as carpal tunnel syndrome are classified asiseases) [35]. This close temporal relationship means that it
s unlikely that a patient will misattribute symptoms to araumatic cause. As a practical matter, the most reliablendicator of when a patient began to have symptoms after arauma is the patient. This is not to say that patients do not getetails concerning an injury event wrong; patient perceptionr recollection of vehicle speeds, crash sequence, and otheretails of a collision may be inconsistent with the facts of aase for reasons other than untruthfulness. For example, anccupant who is injured in a minimal damage rear endollision may believe that the impact must have been at highpeed despite a lack of physical evidence that this was thease.
With regard to the truthfulness of the patient, it is not theole of the clinician to investigate the veracity of the historyiven by the patient. Absent some ancillary indication ofeception, clinicians are generally safe to believe their pa-ients. The rate of fraud of any kind in auto insurance claimsor treatment benefits (personal injury protection coverage)as estimated to be 6% for 2007 [36]. Even if every instancef fraud in auto insurance cases consisted of a patient givingfalse history, clinicians would still be justified in believing
heir patients 94% of the time.Intuitively, it makes sense that the closer the onset of
ymptoms is to the time of the collision the stronger theausal relationship between the MVC and the disk injury,nd the strength of this relationship can be quantified usingn indirect approach. For example, in a case of a 40-year-oldale with neck pain and cervical radiculopathy that aroseithin 12 hours of a rear impact collision (later attributed toRI findings of disk herniation), assuming no intervening
rauma, it can be postulated, as a tautology, that either therash caused the disk injury or that it was coincidental to theollision, regardless of cause. Thus, the probability that therash caused the disk injuries [P(diskMVC)] plus the proba-ility the disk symptoms are coincidental to the crashP(diskCOINC)] when added together account for all of theossible causes (100% or 1) of the disk injury and associatedymptoms. If [P(diskMVC) � P(diskCOINC) � 1] then rear-anging the terms gives [1 � P(diskCOINC) � P(diskMVC)],eaning that if the probability that a disk injury occurred
oincidentally on the same day of the MVC can be deter-ined then the probability the MVC caused the disk injury
an also be determined indirectly.The probability of 2 unrelated events occurring in close
emporal proximity can be calculated by multiplying therobability or odds of one times the other (odds are the ratiof 2 probabilities). For example, the odds of rolling 2 sixes inrow with a fair die are [(1:6) � (1:6) � 1:36]. This is
ecause there are 36 possible combinations for any 2 rolls,ncluding 1 and 1, 1 and 2, 1 and 3, etc, and only one of the
ombinations is a 6 and 6.
ctmymtmpmtwMi1tt1
L
Aittwfpapnswisfsttwdifiws
D
IMlTdsii
bd
cMmlmgrbaitctwaipard
loastgwcadoiaeagir
harrThfm
C
IM
955PM&R Vol. 1, Iss. 10, 2009
In a similar fashion the odds of a disk injury occurringoincidentally on the day of a collision can be calculated forhe example given earlier. The annualized odds of involve-ent in a MVC for a 40-year-old male are 1:14 (once every 14
ears), and the daily odds of crash involvement are approxi-ately 1:5100 (one crash every 5100 days) [37]. The odds of
he spontaneous development of disk symptoms are a bitore difficult to estimate. For example, it can be said that theatient had a single-day episode of neck and arm pain 12onths before the MCV, with no intervening episodes until
he time of the collision. Thus, the odds that the symptomsould recur on any single day were no greater than 1:365.ultiplied together these 2 odds yield an odds of a disk
njury occurring coincidentally on the day of the collision of:1,861,500. Conversely, the odds in favor of a causal rela-ionship between the collision and the disk injury, givenhe onset of symptoms on the day of the collision, are,861,500:1.
ack of Likely Alternative Explanations
lternative explanations for a disk injury include an interven-ng trauma that followed the MVC and preceded the symp-oms indicative of disk injury. Another alternative explana-ion is the insidious onset of symptoms, possibly associatedith a trivial perturbation such as sneezing. Although minor
orces are possible causes of disk injury, they cannot bereferentially selected over the substantially greater forces ofcollision when the two have occurred in close temporal
roximity. If, for example, a patient sustains what is diag-osed as a lumbar strain in a collision and a week laterneezes and has a sudden onset of radicular pain associatedith a disk extrusion, then it is most likely that the disk was
njured in the MVC and the sneeze only prompted a progres-ion of symptoms. It is not reasonable to point to minororces associated with daily activities as a likely cause of aymptomatic disk in preference to the significantly greaterrauma associated even with minimal and no-damage MVCshat is temporally relevant to the symptoms, particularlyhen the patient performed such minor activities with noifficulty prior to the MVC. A “likely” alternative explanation
s one that is most probably causal and the best explanation tot all of the facts at hand, not one that is only a possible causeith no historical or temporal evidence to link it to the
ymptomatic disk injury.
ISCUSSION
ndividual determinations of causation for IVD injury afterVC by clinicians require only that temporal association and
ack of likely alternative explanation be satisfactorily present.he biologic plausibility or possibility that symptomatic diskerangement can follow any degree of forceful loading of thepine is satisfactorily present and need not be revisited inndividual cases. Thus, the concept of measuring crash forces
n detail as a means of determining disk injury potential can pe abandoned as serving no useful purpose in causationeterminations.
There is no reliable index of the degree of force required toause a particular degree of disk derangement. Walz anduser theorized that unless a crash reconstruction and bio-echanical loading assessment was performed for a particu-
ar crash and occupant that causation could not be deter-ined, or, put another way, it must be determined that a
iven crash was sufficiently forceful to cause diagnosed inju-ies [4]. These authors suggested that parameters such as seatelt use, head restraint and seat properties, age, body size,nd preexisting damage (sic) to the spine, inter alia, be takennto account when making causation determinations, effec-ively taking causal determinations out of the hands of clini-ians. What these authors do not explain is how an evalua-ion of any or all of such factors could help determinehether or not any type or severity of injury is possible aftercrash. Even if it could be determined that the risk of disk
njury was exceedingly low for a particular occupant in aarticular crash, this would not be evidence that contradictsny of the 3 elements of causation. Thus, this biomechanicalisk model of injury presence has no utility for real-worldeterminations of causation.
After a determination of causation has been reached, theegal standard for expressing the opinion is as “more probabler likely than not” or as a “reasonable probability” or “reason-ble medical probability” [38]. In some jurisdictions, thetandard is that the clinician must be “more than 50% cer-ain” that the opinion is correct. The purpose of such lan-uage is to describe the results of an internal process ofeighing evidence, and to arrive at a conclusion that the
linician is more certain than not that his or her opinion isccurate or true. The methodology presented in this article isesigned to provide a framework for clinicians to arrive atpinions of causation that can be expressed in terms of whats more likely than not. Thus, when using these guidelines in
narrative report setting, the clinician can write that thessential causal elements of biologic plausibility, temporality,nd lack of likely alternative explanation have been met for aiven case (if true), and that a particular symptomatic disknjury resulted from a particular motor vehicle crash, as aeasonable medical probability.
It must be noted that the model of causation presentederein suffers from the fact that there is no other alternativegainst which it can be evaluated for accuracy. Clinicianseceive little or no formal education in medical school oresidency regarding a systematic approach to causation.hus, the authors recommend that guidelines presentederein be evaluated, modified if necessary, and consideredor adoption by consensus by appropriate scientific andedical organizations.
ONCLUSIONS
ndividual determinations of causation for disk injury afterVC are most appropriately conducted by clinicians, based
rimarily on an evaluation of the temporal association be-
tmsoa
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
956 Freeman et al SYSTEMATIC APPROACH TO DISK INJURY CAUSATION
ween the MVC and the symptom onset. The lack of a valid oreaningful collision force threshold below which it can be
aid that a disk injury will not occur means that investigationf collision parameters for the purposes of injury causationssessment is a pointless endeavor.
EFERENCES1. Freeman MD, Centeno C. Whiplash and secondary gain. J Whiplash Rel
Dis 2003;2:1-4.2. Centeno CJ, Freeman MD, Welkins WL. A review of the literature
refuting the concept of minor impact soft tissue injury. Pain Res Manage2005;10:71-74.
3. Freeman MD, Centeno CJ. A fatal case of secondary gain; a cautionarytale. Am J Case Reports 2008;9:97-103.
4. Tencer AF, Mirza S. Whiplash mechanics in low speed rear-end auto-mobile collisions. J Musculoskel P 2000;8:69-86.
5. Walz FH, Muser MH. Biomechanical assessment of soft tissue cervicalspine disorders and expert opinion in low speed collisions. AccidentAnal Prevent 2000;32:161-165.
6. Jonsson H Jr, Cesarini K, Sahlstedt B, Rauschning W. Findings andoutcome in whiplash-type neck distortions. Spine 1994;19:2733-2743.
7. Scuderi GJ, Sherman AL, Brusovanik GV, Pahl MA, Vaccaro AR. Symp-tomatic cervical disc herniation following a motor vehicle collision:return to work comparative study of workers’ compensation versuspersonal injury insurance status. Spine J 2005;5:639-644.
8. Hill AB. The environment and disease: association or causation? ProcRoy Soc Med 1965;5:295-300.
9. Stephens MD. The diagnosis of adverse medical events associated withdrug treatment. Adv Drug React Ac Poison Rev 1987;6:1-35.
0. Miller FW, Hess HV, Clauw DJ, et al. Approaches for identifying anddefining environmentally associated rheumatic disorders. Arth Rheum2000;43:243-249.
1. McLean SA, William DA, Clauw DJ. Fibromyalgia after motor vehiclecollision: evidence and implications. Traffic Injury Prev 2005;6:97-104.
2. Evans AS. Causation and disease: a chronological journey. The ThomasParran Lecture. Am J Epidemiol 1978;108:249-258.
3. Freeman MD, Rossignol AC. Forensic epidemiology: a systematic ap-proach to probabilistic determinations in disputed matters. J ForensicLegal Med 2008;15:281-290.
4. Pfirrmann CW, Dora C, Schmid MR, Zanetti M, Hodler J, Boos N. MRimage-based grading of lumbar nerve root compromise due to diskherniation: reliability study with surgical correlation. Radiology 2004;230:583-588.
5. Fardon DF, Milette PC. Nomenclature and classification of lumbar discpathology. Recommendations of the Combined task Forces of theNorth American Spine Society, American Society of Spine Radiology,and American Society of Neuroradiology. Spine 2001;26:E93-E113.
6. Carragee E, Alamin T, Cheng I, Franklin T, van den Haak E, Hurwitz E.Are first-time episodes of serious LBP associated with new MRI find-ings? Spine J 2006;6:624-635.
7. O’Neill C, Kurgansky M, Kaiser J, Lau W. Accuracy of MRI for diagnosisof discogenic pain. Pain Physician 2008;11:311-326.
8. Carragee EJ, Paragioudakis SJ, Khurana S. 2000 Volvo Award winner inclinical studies: lumbar high-intensity zone and discography in sub-
jects without low back problems. Spine 2000;25:2987-2992.9. Siegmund GP, King DJ, Lawrence JM, Wheeler JP, Brault JR, Smith TA.Head/neck kinematic response of human subjects in low-speed rear-end collisions. Society of Automotive Engineers, Proceedings of the41st Stapp Car Crash Conference 973341. 1997:357-385.
0. Knobloch K, Wagner S, Haasper C, et al. Sternal fractures occur mostoften in old cars to seat-belted drivers without any airbag often withconcomitant spinal injuries: clinical findings and technical collisionvariables among 42,055 crash victims. Ann Thorac Surg 2006;82:444-450.
1. Matsumoto M, Fujimura Y, Suzuki N, et al. MRI of cervical interverte-bral discs in asymptomatic subjects. J Bone Joint Surg Br 1998;80-B:19-24.
2. Boden SD, McCowin PR, Davis DO, Dina TS, Mark AS, Wiesel S.Abnormal magnetic-resonance scans of the cervical spine in asymp-tomatic subjects. J Bone Joint Surg 1990;72-A:1178-1184.
3. Lehto IJ, Tertti MO, Komu ME, Paajanen HEK, Tuominen J, KormanoMJ. Age-related MRI changes at 0.1 T in cervical discs in asymptomaticsubjects. Neuroradiology 1994;36:49-53
4. Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malka-sian D, Ross JS. Magnetic resonance imaging of the lumbar spine inpeople without back pain. N Engl J Med 1994;331:69-73.
5. Savage RA, Whitehouse GH, Roberts N. The relationship between themagnetic resonance imaging appearance of the lumbar spine and lowback pain, age and occupation in males. Eur Spine J 1997;6:106-114.
6. Yoganandan N, Cusick JF, Pintar FA, Rao RD. Whiplash injury deter-mination with conventional spine imaging and cryomicrotomy. Spine2001;26:2443-2448.
7. Freeman MD, Centeno CJ. Etiologic and demographic characteristicsof traffic crash-related disc injuries. Spine J [in press doi:10.1016/j.spinee.2008.06.373]
8. Giuliano V, Giuliano C, Pinto F, Scaglione M. The use of flexion andextension MR in the evaluation of cervical spine trauma: initial experi-ence in 100 trauma patients compared with 100 normal subjects.Emerg Radiol 2002;9:249-253.
9. Freeman MD, Croft AC, Nicodemus CN, Centeno CJ, Welkins WL.Significant spinal injury resulting from low-level accelerations: a caseseries of roller coaster injuries. Arch Phys Med Rehab 2005;86:2126-2130.
0. Sadanand V, Kelly M, Varughese G, Fourney DR. Sudden quadriplegiaafter acute cervical disc herniation. Can J Neurol Sci 2005;32:356-358.
1. Schechter NA, France MP, Lee CK. Painful internal disc derangementsof the lumbosacral spine: discographic diagnosis and treatment byposterior lumbar interbody fusion. Orthopedics 1991;14:447-451.
2. Dallolio V. Lumbar spinal decompression with a pneumatic orthesis(Orthotrac): preliminary study. Acta Neurochir Suppl 2005;92:133-137.
3. Kruse RA, Imbarlina F, De Bono VF. Treatment of cervical radiculop-athy with flexion distraction. J Manipulative Physiol Ther 2001;24:206-209.
4. Goreham FW. Cervical disc injury; symptoms and conservative treat-ment. Calif Med 1964;101:363-367.
5. Kao SY. 2003. Carpal tunnel syndrome as an occupational disease. J AmBoard Fam Pract 2003:16:533-542.
6. http://www.ircweb.org/News/IRC_Fraud_NR.pdf. Accessed April 16,2009.
7. http://www-nrd.nhtsa.dot.gov/Pubs/98.010.PDF. Accessed April 19,2009.
8. Mossman D. Interpreting clinical evidence of malingering: a Bayesian
perspective. J Am Acad Psychiatry Law 2000;28:293-302.