wegener’s granulomatosis presenting with bilateral facial nerve palsy
TRANSCRIPT

Abstract Primary manifestation of Wegener’s granulo-matosis in the mucosa of the middle ear is rather rare, andhas been reported as presenting with serous otitis media,chronic otitis media, sensorineural hearing loss, and, in rareinstances, unilateral facial palsy. Bilateral facial palsy hasnever been reported. This last fact constitutes the interest inour report of a 23-year-old female patient who presentedwith symptoms of recurrent bilateral otitis media, eventu-ally developing sensorineural hearing loss and bilateral fa-cial palsy. Soon thereafter neurological symptoms ap-peared and lung extension was noted. Histological exami-nation of repeated biopsies taken from the nasal and middleear mucosa was not conclusive for the suspected disease,and c-ANCA titers were also initially repeatedly negative.Eventually, positive lung biopsy and elevated c-ANCAtiters when the patient had developed pulmonary granulo-mas confirmed the diagnosis of Wegener’s granulomatosis.Mastoid surgery with facial nerve decompression of themost severely afflicted side did not result in the recovery offacial nerve function. Medical therapy with corticosteroidsand cyclophosphamide improved the clinical picture butwere ineffective in improving the bilateral sensorineuralhearing loss and the facial paralysis on the operated side.We would contribute to the literature a unique case of bi-lateral facial nerve palsy due to Wegener’s granulomatosis.
Keywords Wegener’s granulomatosis · Otologic manifestations · Bilateral facial palsy
Introduction
Wegener’s granulomatosis is a well-known disease andseveral medical specialties deal with its diagnosis andtreatment. Although Wegener’s granulomatosis is a sys-temic vascular condition, initial presentation may involveonly head and neck symptoms. It becomes obvious thatawareness of all possible variations of the clinical headand neck symptoms at presentation is fundamental inpromptly establishing a correct diagnosis. Peak incidenceof the disease is between 20 and 40 years of age [6].
Several head and neck organs or regions may be af-fected by the disease, producing a conjunction of clinicalmanifestations as follows [6]:
– Nose: nasal congestion, epistaxis, discharge, crusting,saddle-nose deformity, septal perforation
– Larynx: dyspnea, stridor, hoarseness, or other alter-ations of the voice
– Ear and mastoid: symptoms of otitis media, mastoiditis[20], hearing deficit, facial nerve paralysis, vertigo [24]
– Oral cavity: ulcerations, gingivitis– Orbit: swelling, proptosis, redness, pain, visual disor-
ders
Angelos C. Nikolaou · Konstantinos C. Vlachtsis ·Michalis A. Daniilidis · Dimitrios G. Petridis ·Ioannis C. Daniilidis
Wegener’s granulomatosis presenting with bilateral facial nerve palsy
Eur Arch Otorhinolaryngol (2001) 258 :198–202 © Springer-Verlag 2001
Received: 13 December 2000 / Accepted: 5 February 2001
MISCELLANEOUS
A. C. Nikolaou (�) · K. C. Vlachtsis · D. G. Petridis ·I. C. DaniilidisUniversity Department of Otorhinolaryngology, A.H.E.P.A. General Hospital, Medical School of Aristotle University, Thessaloniki, 540 06, Greecee-mail: [email protected].: +30-31-993455, Fax: +30-31-207550
M. A. DaniilidisUniversity Department of Internal Medicine, A.H.E.P.A. General Hospital, Medical School of Aristotle University, Thessaloniki, Greece
Table 1 Number of patients reported with facial paralysis due tootologic Wegener’s granulomatosis
Author, year Number of cases
Calonius and Christensen (1980) 2McCaffrey et al. (1980) 1Illum and Thorling (1981) 2Kornblut et al. (1982) 4Macias et al. (1993) 1Nishino et al. (1993) 8Hern et al. (1996) 1Dagum and Roberson (1998) 1Hofmann et al. (1998) 1Moussa and Abou-Elhmd (1998) 1
Total 22
It has been established that otologic symptoms are fairlyfrequent during the course of Wegener’s granulomatosis[2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 18, 20, 21, 24],
however otologic manifestations as sole presenting symp-toms are uncommon. Only 22 cases have been reportedwith unilateral facial palsy as a result of Wegener’s gran-ulomatosis (Table 1), and none with bilateral facial nerveinvolvement. We would contribute such a unique case, re-viewing the existing literature on the subject.
Case report
A 23-year-old female Caucasian patient was admitted on 26 June1998 at the University Department of Otolaryngology of Thessa-loniki presenting with chronic bilateral aural discharge, otalgia,and hearing loss. These symptoms had already been troubling thepatient for almost a year, and at the time had consulted anotherENT outpatient clinic of the region with bilateral hearing loss andearache. An initial course of nasal decongestants and antibioticshad failed to definitely resolve the problems, achieving only tem-porary remission for a few weeks. In November 1997 aural grom-mets had been inserted bilaterally, improving the clinical pictureduring their 3-month stay in the eardrum. Upon extrusion, how-ever, the symptoms recurred. At the time, biopsies from the oraland nasal mucosa tested for systemic diseases such as tuberculosisand Wegener’s granulomatosis, as well as Mantoux testing, hadbeen negative. In May 1998 the patient had been initiated on acourse of oral corticosteroids and had shown improvement whichonly lasted until mid-June 1998, at which time she was admitted toour department.
On admission the patient was suffering from bilateral purulentaural discharge and severe earache. Otoscopy revealed, on the left,
199
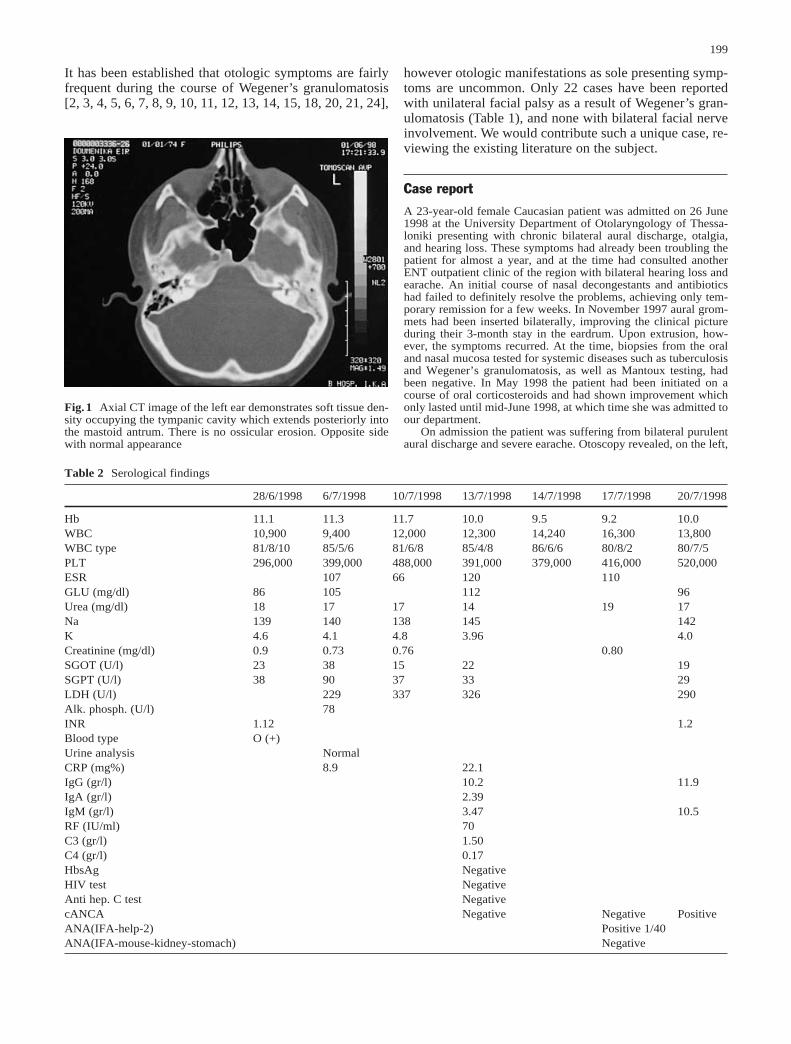
Fig.1 Axial CT image of the left ear demonstrates soft tissue den-sity occupying the tympanic cavity which extends posteriorly intothe mastoid antrum. There is no ossicular erosion. Opposite sidewith normal appearance
Table 2 Serological findings
28/6/1998 6/7/1998 10/7/1998 13/7/1998 14/7/1998 17/7/1998 20/7/1998
Hb 11.1 11.3 11.7 10.0 9.5 9.2 10.0WBC 10,900 9,400 12,000 12,300 14,240 16,300 13,800WBC type 81/8/10 85/5/6 81/6/8 85/4/8 86/6/6 80/8/2 80/7/5PLT 296,000 399,000 488,000 391,000 379,000 416,000 520,000ESR 107 66 120 110GLU (mg/dl) 86 105 112 96Urea (mg/dl) 18 17 17 14 19 17Na 139 140 138 145 142K 4.6 4.1 4.8 3.96 4.0Creatinine (mg/dl) 0.9 0.73 0.76 0.80SGOT (U/l) 23 38 15 22 19SGPT (U/l) 38 90 37 33 29LDH (U/l) 229 337 326 290Alk. phosph. (U/l) 78INR 1.12 1.2Blood type O (+)Urine analysis NormalCRP (mg%) 8.9 22.1IgG (gr/l) 10.2 11.9IgA (gr/l) 2.39IgM (gr/l) 3.47 10.5RF (IU/ml) 70C3 (gr/l) 1.50C4 (gr/l) 0.17HbsAg NegativeHIV test NegativeAnti hep. C test NegativecANCA Negative Negative PositiveANA(IFA-help-2) Positive 1/40ANA(IFA-mouse-kidney-stomach) Negative

a thickened tympanic membrane with polypoid masses arisingfrom the middle ear through a central perforation, while the rightear showed an inflamed tympanic membrane with two central per-forations. Both ears were discharging.
Pure-tone audiometry revealed bilateral mixed hearing loss at50 dB for the right ear and 75 dB for the left. A Schuller plain viewof the mastoids and a CT scan showed reduced pneumatizationmainly on the left (Fig.1). Plain films of the paranasal sinuses andthe chest had no pathological findings. On 28 June 1998, 2 days af-ter admission, the patient presented with a complete low motorneuron left facial nerve paralysis, prompting a left radical mas-toidectomy with facial nerve decompression on the following day.The surgical findings during mastoid exploration showed thicken-ing of the middle ear and mastoid mucosa, as well as thickening ofthe tympanic membrane with two perforations of the pars tensaand severe ossicular chain damage. Biopsies of the middle ear mu-cosa were taken at the time and showed inflammatory granulo-matosis suggesting the possibility of tuberculosis.
On admission serum leucocytosis was at 10,900, ESR = 107 mm,and CRP = 8.9. The rest of the routine hematological and bio-
chemical tests were within normal limits (Table 2). HIV and HbSscreening were negative, and Mantoux skin testing was twice neg-ative (28 June 1998 and 6 July 1998). Blood cultures and PCR formycobacterium were also negative. A CT scan of the area (3 July1998) showed inflammatory material occupying the mastoid aircells and the middle ear (Fig.2).
In view of the histological results, further chest Roentgeno-grams and CT scans were deemed appropriate, which revealed dis-seminated bronchopulmonary infiltrations of the upper and lowerlobes bilaterally (Fig.3). On 3 July 1998 the patient developed aright-sided facial nerve paralysis. A new audiogram showed stablehearing on the right and total deafness on the left ear. On 10 July1998 she presented pyrexia (38°C). A new cerebrospinal fluid testwas also done and was negative. An immunology series on the pa-tient showed the following results: ANA (IFA Hep 2) marginallypositive with serum titer at 1/40, ANCA (IFA) negative, IgG 11.9GPL-U/ml (negative), and IgM 10.5 GPL-U/ml (negative).
During hospitalization, the patient underwent a course of broadspectrum IV antibiotics and IV corticosteroids. On the 12 July1998, the patient developed a left Horner’s syndrome and signs ofinvolvement of the glossopharyngeal and hypoglossal nerves onthe left side. At this point, and in view of the above findings, pul-monary and neurology specialists were consulted, and the patientwas transferred to the Pulmonary Ward of the University Clinic atPapanikolaou Hospital. An MRI scan was performed revealing adegree of meningeal enhancement, with significant sinus disease(Figs. 4, 5). No parenchymal brain lesions were noted. A new c-ANCA serology came back positive this time, with a titer of 3.2.New biochemical and urine tests confirmed the lack of renal in-volvement. The diagnosis of Wegener’s granulomatosis was estab-lished at this time, confirmed with biopsies of the pulmonary le-sions.
Treatment was commenced at this time, with corticosteroidsand cyclophosphamide. Appropriately enough, the clinical pictureand general condition of the patient improved within the week,however the bilateral facial paralysis and the hearing loss remainedunaltered. The c-ANCA tests from this point onward all remainednegative. Six months into treatment the patient was in acceptablygood general condition with the right facial nerve showing signs ofimprovement, while a year later the right facial nerve had com-pletely recovered. Otoscopy was almost normal on the right, whilethe operated left ear was still wet with a mastoid cavity not com-pletely epithelialized. Deafness persisted in the left ear, while the
200
Fig.3 CT of the lungs reveals basal areas of poorly defined con-solidation and multiple pleural nodules. Note also the bilateralpleural effusion
Fig.2 Axial CT image of the right ear demonstrates soft tissuedensity filling the middle ear cavity. Note the presence of fluidlevel within a well-developed mastoid, indicating acute mastoiditis
Fig.4 MRI SE T1W image shows a soft tissue low signal lesionfilling the entire middle ear cavity and the mastoid air cells

right ear presented a sensorineural hearing loss of 50 dB at500–2,000 Hz and 30 dB at the higher frequencies. Repeated X-rays of the lungs appeared normal and the kidneys remained unaf-fected by the disease.
Discussion
Bilateral facial palsy occurs rarely, and may indicate alife-threatening problem. May and Klein [17] reviewing2,856 patients with facial palsy reported that only 2% pre-sented with simultaneous bilateral involvement. The at-tributable causes listed by the authors were Moebius syn-drome, skull fracture, Lyme’s disease, viral meningitis orencephalitis, post-influenza or -poliomyelitis immuniza-tion, infectious mononucleosis, botulism, tetanus, syph-ilis, malaria, herpes zoster cephalicus, otitis media, lep-rosy, acute porphyria, diabetes, acute leukemia, Guillain-Barre syndrome, sarcoidosis, periarteritis nodosa, Bell’spalsy, Melkersson-Rosenthal syndrome, and iatrogenic bi-lateral arterial immobilization.
Wegener’s granulomatosis is an uncommon, systemicdisease that mainly affects the head and neck region, thelungs, and the kidneys. McDonald and DeRemee [19] re-viewing 411 patients affected by the disease found that72.3% presented head and neck involvement, while71.2% had pulmonary symptoms and 57.5% involvementof the kidneys. Other organs may be affected as well, suchas the skin, articulations, the eyes, and the nervous sys-tem. Although it is obvious from the above percentagerates that ear, nose, and throat symptoms coexist in themajority of cases, it is uncommon for the disease to pre-sent initially only with otolaryngological symptoms. Thehead and neck surgeon remains therefore justified in re-membering this uncommon disease when a patient pre-sents with a subglottic stenosis of unknown origin, or with
persistent middle ear disease with a blank otologic history,or with nasal crusting, epistaxis or even ulcerations andnasal deformity.
During the last 5 years, our department diagnosed andtreated eight new cases of Wegener’s granulomatosis pre-senting initially with head and neck symptoms. Three ofthese cases presented with otologic symptoms only, how-ever the case described here was exceptional in its bilat-eral involvement of the facial nerves. The incidence ofotologic manifestations varies widely from 19% to 61%[21], according to recent literature. Documented facialparalysis cases are few. A review of British and Germanliterature revealed 22 reported cases of facial paralysis,none however with bilateral involvement of the VII nerve[3, 8, 9, 10, 15, 16, 18, 20, 22]. According to McCaffreyet al. [18] otologic involvement may be classified intothree distinct patterns: serous otitis media, sensorineuralhearing loss, and chronic otitis media. Dagum and Robert-son [4], in their reviewed classification, added facialparalysis to the above parameters. Eustachian tube dys-function, a condition that leads to the most common oto-logic manifestation, namely serous otitis media, needstherefore careful assessment and specifically definite ex-clusion of nasopharyngeal malignancy or other conditionobstructing the pharyngeal orifice of the Eustachian tube,such as Wegener’s granulomatosis. Insertion of tympa-nostomy tubes is a primary mode of treatment for such pa-tients.
The presence of sensorineural hearing loss or chronicotitis media in Wegener’s granulomatosis leads one to theassumption that the disease asserts itself directly withinthe ear with the development of granulomas in the middleear cleft or in the internal auditory canal [4, 23]. The usualotoscopic findings are in evidence in Wegener’s inducedchronic otitis, with perforated ear drum, polypoid forma-tions of the middle ear mucosa, and purulent discharge. Inthe case presently described, the existence of two perfora-tions of the pars tensa of the right ear was more suggestiveof tuberculosis rather than any other inflammatory dis-ease.
The diagnosis of Wegener’s granulomatosis can be dif-ficult to obtain in the best of cases, even when laboratoryand histological examinations are employed to this end.Primarily, the clinical picture can be misleading shouldthe disease manifest itself solely with otologic symptoms.In these cases, the unremarkable otologic history shouldlead to the exclusion of an obstructive nasopharyngealmalignancy or a malignancy of the middle ear. The likelyfailure of the ubiquitous antibiotic course should orientthe physician toward a more aggressive investigative pro-cedure. In the main, chest X-ray, Mantoux testing, p andcANCA titers, and biopsy of the middle ear mucosashould be performed [1, 14, 16, 19, 23]. The presence ofpulmonary nodules disseminated in both lungs should besuggestive of Wegener’s granulomatosis or tuberculosis.In cases of extensive tuberculosis, negative Mantoux test-ing is not a rare finding. Histology can also be misleadingin primary otologic Wegener’s granulomatosis, oftenshowing non-specific fibrino-purulence. Finally, although
201
Fig.5 Post-contrast T1W image demonstrates the enhanced thick-ened dura without any temporal lobe involvement

202
elevated cANCA levels are well-documented indicatorsof Wegener’s granulomatosis, attaining rates of 90% pos-itivity in cases of active disease [1], sensitivity is not100% and may be negative in a few cases. In the case de-scribed here the test was performed three times, only be-coming positive when pulmonary and bilateral mastoidand facial nerve involvement was present.
From the above elements, one should conclude that di-agnosis of Wegener’s granulomatosis should combinethorough physical examination, positive histological find-ings, and the presence of positive cANCA titers. Biopsiestaken from pulmonary lesions are more specifically diag-nostic of the disease than those from the middle ear mu-cosa [4, 6], as demonstrated by Dagum and Robertson’sexperience[4] as well as our own in the present case.
Prognosis of Wegener’s granulomatosis-induced neu-ropathies depends mainly on early diagnosis and promptinitiation of treatment, according to most authors [2, 4,15]. Dagum’s review of such cases [4] concludes that de-lay of medical treatment may require mastoidectomy withdecompression of the facial nerve in order to avoid per-manent nerve damage. A dissimilar view is held by othershowever [3, 9, 10, 16]; medical treatment is advocated inall instances by these authors who doubt as to the neces-sity or efficacy of surgical intervention in Wegener’s-in-duced facial paralysis. In the case presented here, facialnerve decompression was performed 1 day following thedevelopment of a left-sided facial paralysis, and medicaltherapy for the disease was commenced 1 month later. Sixmonths later the left facial nerve had not yet recovered de-spite the early surgery, while the right-sided facial nervehad shown partial improvement under medical treatmentonly.
Overall survival rates of Wegener’s granulomatosishave improved over the last decades, reversing the fatalprognosis attached to the disease, since the widespread in-stitution of early treatment with prednisone and cy-clophosphamide. Remission rates of 70% to 85% havebeen achieved, depending on the extension and the sever-ity of lesions on the afflicted organs [4, 6, 10].
In conclusion, a unique case of bilateral facial nervepalsy due to Wegener’s granulomatosis is hereby pre-sented and its significant elements highlighted in the con-text of already reported cases of unilateral facial paralysis,few though they may be. The rarity of primary affectionof the middle ear mucosa due to Wegener’s granulomato-sis is established, and the usual presenting clinical mani-festations such as serous otitis media, chronic otitis me-dia, and sensorineural hearing loss are described.
References
1.Batsakis JG, El-Naggar AK (1993) Wegener’s granulomatosisand antineutrophil cytoplasmic autoantibodies. Ann Otol Rhi-nol Laryngol 102:906–908
2. Bradley PJ (1983) Wegener’s granulomatosis of the ear. J Laryn-gol Otol 97:623–626
3. Calonius IJ, Christensen CK (1980) Hearing impairment and fa-cial palsy as initial signs of Wegener’s granulomatosis. J Laryn-gol Otol 94:649–657
4.Dagum P, Roberson JB Jr (1998) Otologic Wegener’s granulo-matosis with facial nerve palsy. Ann Otol Rhinol Laryngol107: 555–559
5.Dekker PJ (1993) Wegener’s granulomatosis: otological as-pects. J Otolaryngol 22:364–367
6.Devaney KO, Ferlito A, Hunter BC, Devaney SL, Rinaldo A(1998) Wegener’s granulomatosis of the head and neck. AnnOtol Rhinol Laryngol 107:439–445
7.Frank W, Munzel M (1985) Otologic manifestation of We-gener’s granulomatosis. Laryngol Rhinol Otol (Stuttg) 64:527–531
8.Hern JD, Hollis LJ, Moshloulis G, Montgomery PQ, Tolley NS(1996) Early diagnosis of Wegener’s granulomatosis present-ing with facial nerve palsy. J Laryngol Otol 110:459–461
9.Hofmann T, Kainz J, Koc C, Smolle KH, Brunner G (1998)Isolierte einseitige Otitis mit Fazialisparese als Erstsymptombei Wegener-Granulomatose. Ein ungewoehnlicher klinischerVerlauf. Laryngorhinootologie 77:352–354
10. Illum P, Thorling K (1982) Otological manifestations of We-gener’s granulomatosis. Laryngoscope 92:801–804
11. Ito Y, Shinogi J, Yuta A, Okada E, Taki M, Matsukage H(1991) Clinical records: a case report of Wegener’s granulo-matosis limited to the ear. Auris Nasus Larynx 18:281–289
12.Karmody CS (1978) Wegener’s granulomatosis: presentationas an otologic problem. Otolaryngology 86:573–576
13.Kempf HG (1989) Ear involvement in Wegener’s granulo-matosis. Clin Otolaryngol 14:451–456
14.Kempf HG, Bootz F, Berg PA (1992) Wegener’s granulomato-sis: otologic and clinico-immunologic aspects. Laryngorhi-nootologie 71:26–30
15.Kornblut AD, Wolff SM, Fauci AS (1982) Ear disease in pa-tients with Wegener’s granulomatosis. Laryngoscope 92:713–717
16.Macias JD, Wackym PA, McCabe BF (1993) Early diagnosisof otologic Wegener’s granulomatosis using the serologicmarker c-ANCA. Ann Otol Rhinol Laryngol 102:337–341
17.May M, Klein SR (1991) Differential diagnosis of facial nervepalsy. In: Mattox DE (ed) Management of facial nerve disor-ders. Otolaryngol Clin North Am 24:613–645
18.McCaffrey TV, McDonald TJ, Facer GW, DeRemee RA(1980) Otologic manifestations of Wegener’s granulomatosis.Otolaryngol Head Neck Surg 88:586–593
19.McDonald TJ, DeRemee RA (1993) Head and neck involve-ment in Wegener’s granulomatosis. In: Gross WL (ed) ANCA-associated vasculitides; immunological and clinical aspects.Plenum Press, New York, pp 309–313
20.Moussa AE, Abou-Elhmd KA (1998)Wegener’s granulomato-sis presenting as mastoiditis. Ann Otol Rhinol Laryngol107:560–563
21.Murty GE (1990) Wegener’s granulomatosis otorhinolaryngo-logical manifestations (review). Clin Otolaryngol 15:385–393
22.Nishino H, Rubino FA, DeRemee RA, Swansin JW, Parisi JE(1993) Neurologic involvement in Wegener’s granulomatosis:an analysis of 324 consecutive patients at the Mayo Clinic. AnnNeurol 33:4–9
23.Okamura H, Ohtani I, Anzai T (1992) The hearing loss in We-gener’s granulomatosis: relationship between hearing loss andserum ANCA. Auris Nasus Larynx 19:1–6
24.Pagano M, Africano R, Lo Pinto G (1996) Wegener granulo-matosis: a clinical case with parossistic positional vertigo dueto involvement of the lateral semicircular canal. Acta Otorhi-nolaryngol Ital 16:438–440