vn pocketguide us
DESCRIPTION
Vn Pocketguide UsTRANSCRIPT

System

Interventional Procedure
Patients with inadequate response to their antiplatelet medications may be at significantly greater risk of myocardial
infarction, stent thrombosis and death.1-4
Up to 1/3 of patients on antiplatelet medications may not receive the expected platelet inhibiting effect.5
Numerous factors may cause inadequate response,6 including:
• Drug Interactions
(e.g. Proton Pump Inhibitors)
• Genetic differences
1 2 3 4 5
Residual Clopidogrel Responsiveness Within 3 days, > 50% of patients no longer have antiplatelet effectWithin 3 days, > 50% of patients no longer have antiplatelet effect
20%
40%
60%
80%
% O
F P
AT
IEN
TS
% O
F P
AT
IEN
TS
DAY OF RECOVERYDAY OF RECOVERY
No antiplatelet response
Moderate antiplatelet response
High antiplatelet response
• Pre-existing health
conditions (e.g. diabetes)
• Non-compliance
2

What is Reported?
The lab report may look similar to the following:
PRU reference range is 194-418. Values less than the low end of the reference range are specific evidence of a P2Y12 inhibitor effect.
P2Y12 Reaction Units (PRU) indicate the amount of ADP-mediated aggregation specific to the platelet P2Y12 receptor.
*******************************************************
*******************************************************
Patient Example PRUTest Results Patient A Units Reference Range
P2Y12 Reaction Units 132 PRU (Baseline platelet reactivity to ADP)
25 50 75100
125150
175200
225250
275300
325350
375400
425450
475
Values less than the lower limit (194) are highly specific for a P2Y12 inhibitor e�ectValues less than the lower limit (194) are highly specific for a P2Y12 inhibitor e�ect
Normal ADP Reactivity(No Evidence of P2Y12 Inhibitor E�ect)Normal ADP Reactivity(No Evidence of P2Y12 Inhibitor E�ect)
Supressed ADP Reactivity(Evidence of P2Y12 Inhibitor E�ect)
Supressed ADP Reactivity(Evidence of P2Y12 Inhibitor E�ect)
0
5
10
15
20
25
30
FRE
QU
EN
CY
FRE
QU
EN
CY
PRUPRU

VerifyNow PRUTest Results
VerifyNow PRUTest:Platelet response to P2Y12 inhibitors (e.g clopidogrel, prasugrel , ticlopidine, and ticagrelor).
PRU (P2Y12 Reaction Units)• ADP induced aggregation - extent of platelet aggregation in
the presence of P2Y12 inhibitors
• Residual Platelet Reactivity (RPR) of ADP P2Y12 receptor
Pre-Surgical Application• Studies show that there is patient variability in response to P2Y12
inhibitors7.
• Patients that have been administered P2Y12 inhibitors such as clopidogrel and prasugrel are at risk of perioperative bleeding.
• It has been recommended to discontinue P2Y12 inhibitors for 5 – 7 days prior to surgery8 for platelet function to be restored9, however, 2012 STS Guidelines10 recommend using platelet function testing to aid in timing of surgery, instead of arbitrarily waiting a pre-specified period of time.
To Order this Test:
In patients with high on-treatment reactivity (OTR) after PCI, there was substantial variability over time in the pharmacodynamic responses to study drug.Patients with low levels of OTR after PCI appeared to have few (if any) CV events.
Price MJ, AHA 2010
ADAPT-DES: Relationship Between VerifyNow P2Y12 PRU and Stent Thrombosis within 30 Days Definite or probable stent thrombosis
DE
FIN
ITE
/PR
OB
AB
LE S
T (
%)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
0 5 10 15 20 25 30
0.81%
0.21%
P2Y12 PRU > 208 (n=3607)
P2Y12 PRU ≤ 208 (n=4834)
P <0.001
HR [95% CI]=
3.89 [1.90, 7.98]
DAYS
3607 3540 3534 34824834 4754 4752 4686
Number at risk>208 PRU≤208 PRU
500
400
300
200
100
0
PRU VALUE
Post -PCI 30 d 6 mo Post -PCI 30 d 6 mo
N=1013 N=940N=1105 N=1012 N=944N=1109
P = 0.98P < 0.001
PERSISTENTLY HIGH REACTIVITY @ 30 DAYS: 62% VS40%, P<0.001
500
400
300
200
100
0
PRU 12 -24 HRS POST-PCI
High ResidualReactivity
Not HighResidual Reactivity
N=1105 N= 586
Red dots: patients with CV death, MI, or ST
230 PRU
Brar, S et al J Am Coll Cardiol. 2011 Nov 1;58(19):1945-54.*There are currently no definitive criteria that establish a standard PRU/% inhibition cutoff for ischemic risk
N = 3049
DE
AT
H, M
I, O
R S
T
TIME (DAYS)
N=30490.20
0.15
0.10
0.05
0.000 100 200 300 400 500 600 700
Q4 15.8% <0.001
Q3 10.9% 0.02
Q2 6.9% 0.97Q1 5.8% -
EventRateQuartile P-value*
CV Events and Post-PCI PRU In Patients With High and Not High Reactivity Treated With Clopidogrel 75-mg Daily
PharmacodynamicsEffect of SD vs HD Clopidogrel
Standard-Dose High-Dose
VerifyNow Meta AnalysisSurvival Analysis of PRU Quartiles*
Stone GW, et al presented at TCT 2011
Chart Tertiary Title or Labels
NON-THERAPEUTIC RANGE
THERAPEUTIC RANGE
POST ASPIRIN INGESTION
AR
U: A
SPIR
IN R
EA
CT
ION
UN
ITS
700
650
600
550
500
450
400
350
NON-THERAPEUTIC RANGE
THERAPEUTIC RANGE
POST ASPIRIN INGESTION
AR
U: A
SPIR
IN R
EA
CT
ION
UN
ITS
700
650
600
550
500
450
400
350
350
300
250
200
150
100
50
PR
U: P
2Y
12 R
EA
CT
ION
UN
ITS
Example PRU’s
Conditions that May Affect Test Results
• Patient’s exposure to GP IIb/IIIa inhibitors within:
– 48 hours of eptifibatide – 14 days of abciximab
• Improper sample collection (platelet activation)
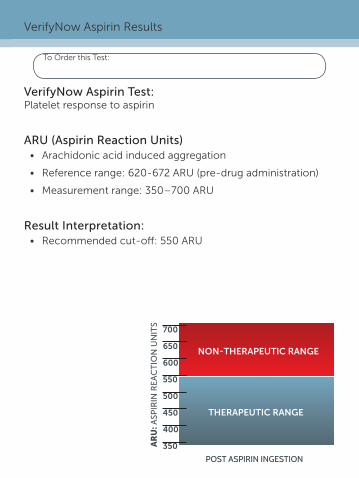
VerifyNow Aspirin Test:Platelet response to aspirin
ARU (Aspirin Reaction Units)• Arachidonic acid induced aggregation
• Reference range: 620-672 ARU (pre-drug administration)
• Measurement range: 350–700 ARU
Result Interpretation:• Recommended cut-off: 550 ARU
VerifyNow Aspirin Results
To Order this Test:
In patients with high on-treatment reactivity (OTR) after PCI, there was substantial variability over time in the pharmacodynamic responses to study drug.Patients with low levels of OTR after PCI appeared to have few (if any) CV events.
Price MJ, AHA 2010
ADAPT-DES: Relationship Between VerifyNow P2Y12 PRU and Stent Thrombosis within 30 Days Definite or probable stent thrombosis
DE
FIN
ITE
/PR
OB
AB
LE S
T (
%)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
0 5 10 15 20 25 30
0.81%
0.21%
P2Y12 PRU > 208 (n=3607)
P2Y12 PRU ≤ 208 (n=4834)
P <0.001
HR [95% CI]=
3.89 [1.90, 7.98]
DAYS
3607 3540 3534 34824834 4754 4752 4686
Number at risk>208 PRU≤208 PRU
500
400
300
200
100
0
PRU VALUE
Post -PCI 30 d 6 mo Post -PCI 30 d 6 mo
N=1013 N=940N=1105 N=1012 N=944N=1109
P = 0.98P < 0.001
PERSISTENTLY HIGH REACTIVITY @ 30 DAYS: 62% VS40%, P<0.001
500
400
300
200
100
0
PRU 12 -24 HRS POST-PCI
High ResidualReactivity
Not HighResidual Reactivity
N=1105 N= 586
Red dots: patients with CV death, MI, or ST
230 PRU
Brar, S et al J Am Coll Cardiol. 2011 Nov 1;58(19):1945-54.*There are currently no definitive criteria that establish a standard PRU/% inhibition cutoff for ischemic risk
N = 3049
DE
AT
H, M
I, O
R S
T
TIME (DAYS)
N=30490.20
0.15
0.10
0.05
0.000 100 200 300 400 500 600 700
Q4 15.8% <0.001
Q3 10.9% 0.02
Q2 6.9% 0.97Q1 5.8% -
EventRateQuartile P-value*
CV Events and Post-PCI PRU In Patients With High and Not High Reactivity Treated With Clopidogrel 75-mg Daily
PharmacodynamicsEffect of SD vs HD Clopidogrel
Standard-Dose High-Dose
VerifyNow Meta AnalysisSurvival Analysis of PRU Quartiles*
Stone GW, et al presented at TCT 2011
Chart Tertiary Title or Labels
NON-THERAPEUTIC RANGE
THERAPEUTIC RANGE
POST ASPIRIN INGESTION
AR
U: A
SPIR
IN R
EA
CT
ION
UN
ITS
700
650
600
550
500
450
400
350
NON-THERAPEUTIC RANGE
THERAPEUTIC RANGE
POST ASPIRIN INGESTION
AR
U: A
SPIR
IN R
EA
CT
ION
UN
ITS
700
650
600
550
500
450
400
350
350
300
250
200
150
100
50
PR
U: P
2Y
12 R
EA
CT
ION
UN
ITS
Example PRU’s

Fibrinogen
GP IIb-IIIa
GP IIb-IIIa
Thrombin Receptors
ADP (P2Y1)
ADP (P2Y12)Epinephrine
Plasmin
CollagenShear Forces
Serotonin Platelet Activating Factor
AA
TXA2 Thromboxane A2
Aspirin
GP IIb/IIIa InhibitorsAbciximabEptifibatide
P2Y12 InhibitorsClopidogrelPrasugrelTicagrelor
Blood SampleShowing Inhibition of
Platelet Function
Red Blood Cells
Fibrinogen-Coated Beads
Low LightTransmittance
Platelet-Bead Aggregates
Blood SampleShowing NormalPlatelet Function
Increased LightTransmittance
Platelets
Agonist
How It Works: Activates Specific Drug Receptor Sites

VerifyNow Aspirin or PRUTest Sample Collection Procedure
5 ml
1 CBC
X5
1
2
3
4
5
2
1 2
2 CBC
X5
1
2
3
4
5
6
5 ml
1 CBC
X5
1
2
3
4
5
2
1 2
2 CBC
X5
1
2
3
4
5
6
Direct Venipuncture Sample collection directly into vacuum collection tubes
1. Use 2 mL Greiner Bio-One partial-fill vacuette tubes with 3.2% sodium citrate (blue top). Greiner #454322.
2. Collect 2 tubes of whole blood using a 21 gauge or larger needle. First, collect a discard tube (at least 2 mL) making sure the discard tube does not contain any platelet inhibiting substance (e.g. EDTA). Butterfly (21 gauge) is OK to use.
3. Fill the second tube (sample tube) to the black line (1/2 tube). Do not under fill. Discard the first tube. Keep the second tube for testing.
4. If drawing blood for a CBC at the same time, fill the CBC tube last
5. Gently invert the tube at least 5 times to ensure complete mixing of the contents. Samples with evidence of clotting should not be used.
6. Label the tube with the patient ID, date and time it was drawn. Do not refrigerate.
Indwelling Catheter
1. Discard the first 5 mL from an indwelling catheter to clear the line. Ensure the catheter is free of clots.
2. Immediately transfer blood to a 2 mL Greiner Bio-One partial-fill vacuette tube with 3.2% sodium citrate (blue top). Greiner #454322. Fill to the black line (1/2 tube). Do not under fill.
3. If drawing blood for a CBC at the same time, fill the CBC tube last
4. Gently invert the tube at least 5 times to ensure complete mixing of the contents. Samples with evidence of clotting should not be used.
5. Label the tube with the patient ID, date and time it was drawn. Do not refrigerate.

Verif
yNow
Te
st
Med
icat
ion(
s)
Test
ed
Dos
e G
iven
Sugg
este
d
Test
Tim
ing
Sam
ple
In
cuba
tion
(M
inut
es)
Run
Tim
e (M
inut
es)
PR
UTe
st
Clopidogrel
75 mg 7 days on maintenance1
10 ~3
300 mg 8 hours post bolus2
600 mg 6 hours post bolus3
Ticlopidine250 mg 2 hours post dose4
250 mg (bid) 21 days (steady state)4
Prasugrel
5 mg 5 days on maintenance5
10 mg 5 days on maintenance5
60 mg 45 minutes post bolus9
Ticagrelor 90 mg (bid)
1 day on maintenance7 (within 8 hours of last dose for maximal effect)
180 mg2 hours post bolus8 (within 8 hours for maximal effect)
Aspirin Aspirin 81 - 325 mg 2 hours post dose 30 ~5
For more details, see the VerifyNow Test package insert.1 Plavix (clopidogrel bisulfate) tablets Prescribing Information. Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership. 3/2010 Update. 2 Price, MJ et al. Am J Cardiol 2006;98:681-684. 3 Hochholzer W. et al. Circulation. 2005;111:2560-2564. 4 Ticlid (ticlopidine hydrochloride) tablets Prescribing Information. Roche Laboratories Inc. Revised 12/2005. 5 Effient (prasugrel) tablets Prescribing Information. Daiichi Sankyo, Inc. and Eli Lilly and Company. July 10, 2009. 6 VerifyNow IIb/IIIa Test Package Insert. 14320.K. 2009-06-10. 7 Increased Active Metabolite Formation Explains the Greater Platelet Inhibition With Prasugrel Compared to High-dose Clopidogrel. June 26, 2007 8 Husted S et al. Eur Heart J. 2006;27:1038–1047 9 Brilinta (ticagrelor) tablets prescribing information. AstraZeneca group of companies. July 20, 2011. 10 2012 Update to The Society of Thoracic Surgeons Guideline on Use of Antiplatelet Drugs in Patients having Cardiac and Noncardiac Operations. © 2102 by the Society of Thoracic Surgeons. Published by Elsevier Inc.
3985 Sorrento Valley BoulevardSan Diego, California USA 92121Toll Free: [email protected]
www.accumetrics.com
3985 Sorrento Valley BoulevardSan Diego, California USA 92121Toll Free: [email protected]
www.accumetrics.com
The Accumetrics logo and VerifyNow are registered trademarks of Accumetrics, Inc., ©2012 Accumetrics, Inc.
PN:148039.F 01/2013