vertical oculomotor apraxia and memory loss
TRANSCRIPT

Vertical Oculomotor Apraxia and Memory Loss
Richard P. Mills, MD, a n d Phillip D. Swanson, MD
A case of vertical oculomotor apraxia w i t h severe memory loss and hypokinet ic inertia is described i n a 34-year-old woman who was t a k i n g oral contraceptives. The eye movement disorder was l imited to paralysis of voluntary vertical saccades; pursui t movements, reflex eye movement, and horizontal saccades were normal. Random involuntary vertical saccades documented b y electronystagmography qualified this as a true apraxia.
Similar cases f rom the l i terature have i n common involvement of both medial thalami, a localization supported in this case by distinctive abnormalities on C A T scan. The clinical course suggested acute infarction, possibly d u e to embolism, i n a terr i tory supplied by the thalamosubthalamic paramedian arteries.
Mills RP, Swanson PD: Vertical oculomotor apraxia and memory loss. Ann Neurol 4:149-153, 1978
Children with congenital oculomotor apraxia d e m o n - s t ra te a global loss of horizontal saccadic e y e move- ments , although pursu i t a n d oculovestibular move- ments are of ten intact [7]. Rare instances of acquired horizontal oculomotor apraxia have b e e n descr ibed due t o bilateral f rontal lobe lesions [ 181, multiple sclerosis [ 3 11, and superior longitudinal sinus throm- bosis [t i] . Global vertical saccadic paralysis with pres- ervat ion of following or reflex movements , or both , has been descr ibed as a t ransient phase of parkin- sonism [ 1 11, in progressive supranuclear palsy [ 2 31, and in Niemann-Pick disease [24]. We recent ly ob- served a pat ient who s h o w e d isolated total paralysis of voluntary vertical saccadic m o v e m e n t but preser- vation of all other ocular m o v e m e n t functions. This vertical o c u l o m o t o r apraxia was associated with se- v e r e m e m o r y loss a n d apathy. After t h e apoplect ic o n s e t of illness, t h e condi t ion has pers is ted un- changed for t h r e e years.
Case Report A 34-year-old woman was found comatose at 2 : O O AM on July 18, 1974, by her husband, who was awakened by sounds of moaning and teeth grinding. She had been in excellent health. She had been taking oral contraceptive medication for six years but took no other drug. She had a master's degree in mathematics and was a nondrinker. She had given no indication of illness to her husband or friends when she went to bed at 1O:OO PM.
She was brought to the emergency room of a local hospi- tal. Blood pressure was 120/80, pulse was 60, respirations were 16, and temperature was 37°C. General physical ex- amination was unremarkable. She was comatose with de-
cerebrate posturing to noxious stimuli. No focal abnor- malities were found. Pupils were 2 mm in diameter and reactive. Horizontal eye movements were full to doll's head maneuver and to ice-water caloric stimulation. Verti- cal eye movements were not tested. The neck was supple, the face symmetrical, and the extremities flaccid. Bilateral Babinski signs and sucking and snout reflexes were present. Despite the absence of sweating, pharmacological pupillary testing with 49% cocaine failed to confirm the presence of Horner syndrome.
Complete analysis of blood and urine was normal, includ- ing screening for toxic substances. The spinal fluid showed an opening pressure of 140 mm H20, protein of 40 mgldl with 9.8% IgG, glucose of 70 mg/dl, and only 1 mononu- clear cell in two specimens obtained during the first hos- pital day. The electroencephalogram was suggestive of a normal drowsy state with bilateral background slowing. Chest roentgenogram, electrocardiogram, and lung scan were normal.
The patient began to show gradual neurological im- provement from the time of admission. Decerebrate re- sponses persisted for 24 hours. She gradually became less comatose but remained drowsy and inattentive. Toward the end of the first week she became more mobile but yawned and ground her teeth frequently. She began to feed herself and appeared to recognize her family. Sucking and grasping were absent and plantar reflexes were downgoing.
At the time of transfer to University Hospital on the eighth day of her illness, she was withdrawn but conscious. She often lay in bed with her eyes closed and yawned fre- quently, but knew she was in a hospital. O n the eleventh day her sister visited and the patient failed to recognize her.
Several EEG records documented slowly improving gen- eralized disturbance of brain function compatible with a deep midline subcortical lesion. Skull roentgenograms,
From the Department of Ophthalmology and the Division of Neu- Address reprint requests to Dr Mills, Department of Ophthal- rology, Department of Medicine, University of Washington mology, RJ-10, University of Washington School of Medicine, School of Medicine, Seattle, WA. Seattle, WA 98195.
Accepted for publication Feb 22, 1078.
0364-5134/78/0004-0208$01.25 @ 1978 by Richard P. Mills 149

brain scan, echocardiogram, and spinal fluid examinations were normal. Four-vessel cerebral arteriography carried out 15 days after the onset of her illness was normal. T h e right posterior cerebral artery filled from the right internal carotid artery, indicating a large posterior communicating artery on that side. Selective injection of the left vertebral artery filled both posterior cerebral arteries, though the right posterior cerebral artery flash-filled, again indicating filling from the carotid artery on that side. A pneumoen- cephalogram done three weeks after the onset of her illness was normal, but the third ventricle was only partially filled.
Neurological residua that have persisted for three years include sleepiness, mild loss of intellectual capacity, severe memory dysfunction, severe apathy, and abnormality of saccadic vertical eye movement. At recent examinations she remained apathetic. She slept 12 to 20 hours a day depending on her environment. When stimulated she re- sponded normally to commands, and she could ambulate and speak without difficulty. She demonstrated inconsis- tent disorientation to time, place, and person. She volun- teered almost no spontaneous information and initiated lit- tle behavior. If given a specific task with an observer pres- ent, she would work in a slow and conscientious manner until the task either became somewhat complex or involved some transition, at which point she would terminate her work. If left alone to d o a simple task, she would w o n stop and simply sit.
H e r ability to do complex logical activities was very lim- ited and her ability to learn new things and to retain recent information was severely compromised. She had a defec- tive Wechsler memory quotient of 57 to 70. She com- prehended most sentences and paragraphs but could remember from none to only 20% of the content of sen- tences several minutes after a conversation. She was, how- ever, able to recall much information learned prior to her illness in the area of vocabulary, general information, and basic arithmetic. Immediate recall was also at the average level. She achieved a full-scale IQ of 74 five weeks after the onset of the illness. Six months later her IQ was 100. though the memory deficits persisted.
The patient was totally unable to look up or down on command or to refixate in the vertical plane. She was able to follow slowly moving objects to full vertical gaze excur- sion, and Bell's phenomenon was present. She was unable to suppress the doll's eye phenomenon with vertical head movement, and full vertical excursion could be demon- strated with this maneuver. Vertical opticokinetic stimulus resulted in full following movement but n o saccadic refixa- tion. Calorically induced vertical nystagmus was normal, with slow and fast components. Although the patient could not voluntarily initiate a vertical saccade, spontaneous ver- tical saccades were demonstrated with electronystagmog- raphy. In the horizontal plane, saccades, following move- ments, opticokinetic nystagmus, and convergence were normal. Doll's eye movements were absent horizontally, being inhibited by voluntary effort and fixation influences. Pupillary responses to light and near were normal, and the normally positioned eyelids responded appropriately to the direction of attempted gaze. O n the eleventh and twentieth days of her illness, the left pupil was transiently noted to be
larger than the right, but was briskly reactive to light. O n other occasions the pupils were equal.
Because of her inability to suppress fixation-induced ver- tical following movemenrs, she demonstrated a unique problem of mobility. While walking, she would fixate on an object in front of her; her eyes would follow it as she approached and as it passed underfoot. Now looking straight down and unable to fixate upward, she would be unable to see. O n being reminded to close her eyes (her memory defect prevented learning this simple maneuver), Bell's phenomenon recentered the eyes, and she was able to continue walking. O n command, she could also recenter her eyes by the use of vertical head thrusts similar in type but perpendicular in direction to those exhibited by pa- tients with Cogan's horizontal oculomotor apraxia. For example, full downward eye rotation resulted from back- ward head movement. If backward head movement was continued, the eyes followed passively, still in full down- ward gaze, until a higher plane of gaze resulted. Now, with forward head movement, the eyes rotated upward to a more comfortable gaze position in response to ocu- locephalic reflexes.
CAT scanning in this patient was unsuccessful in 1975 due to motion artifact, but agood-quality scan was obtained in 1977, two and a half years after the onset of her illness (Figure). The lateral ventricles were of normal size, but the third ventricle was wider than normal, particularly cephalad. The maximal width of 9.6 rnm was in excess of the normal range of 1.7 to 8.3 mm for all ages and well above the range of 1.7 to 3.3 mm for normal adult females under 40 years [ 141. O n both sides of this widening there were small, approximately symmetrical zones of low ab- sorption thought by the radiologist to be located in the region of the dorsomedial nuclei of the thalamus. Other measurements of maximum width of the anterior horns, septum caudate distance, and skull width were within nor- mal limits, The entire width of the third ventricle plus the contiguous low-density thalamic regions was 26 mm. The sulci were slightly widened over the frontal and parietal convexities. There was no enlargement of the temporal horns of the lateral ventricles to suggest hippocampal at- rophy.
Discussion Available clinical and experimental ev idence indi- cates that the final common pathways for vertical gaze originate in the upper midbrain: i n the pretectum- pos te r ior commissure region for upward gaze [lS] a n d i n the area medial and dorsal to the red nuclei for downward gaze [17]. Bilateral lesions in these areas reliably produce paralysis of all upward or all down- ward m o v e m e n t s of the eyes, usually associated with abnormalities of convergence, lid position, or pupil- lary reactions, or with retraction nystagmus. Occa- sionally, strictly unilateral lesions at t h e posterior commissure level have produced upward gaze palsy [19, 201.
Contr ibut ions from various e y e m o v e m e n t subsys-
150 Annals of Neurology Vol 4 No 2 August 1978
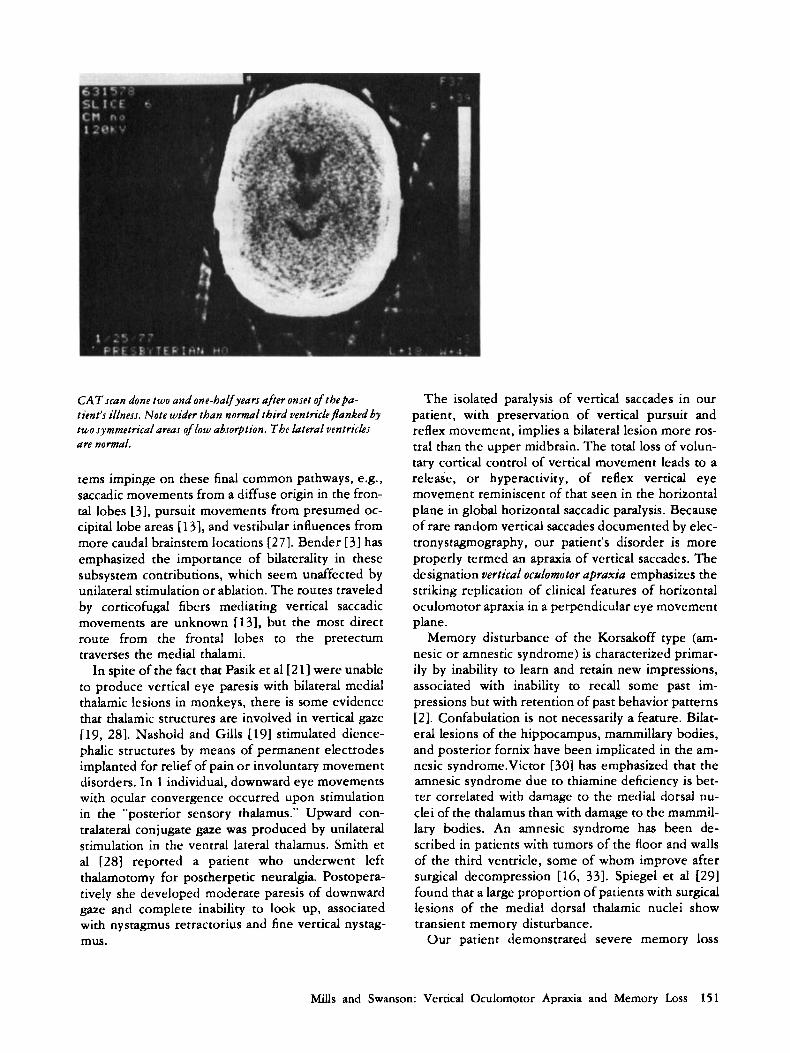
CAT scan done two and one-halfyears afrer onset of thepa- tient’s illness. Note wider than normal third ventricle flanked by two symmetricalareas of low absorption. The lateral ventrich are normal.
tems impinge on these final common pathways, e.g., saccadic movements from a diffuse origin in the fron- tal lobes [3], pursuit movements from presumed oc- cipital lobe areas [ 131, and vestibular influences from more caudal brainstem locations [27]. Bender [3] has emphasized the importance of bilaterality in these subsystem contributions, which seem unaffected by unilateral stimulation or ablation. The routes traveled by corticofugal fibers mediating vertical saccadic movements are unknown [13], but the most direct route from the frontal lobes to the pretectum traverses the medial thalami.
In spite of the fact that Pasik et a1 [21] were unable to produce vertical eye paresis with bilateral medial thalamic lesions in monkeys, there is some evidence that thalamic structures are involved in vertical gaze [19, 281. Nashold and Gills [19] stimulated dience- phalic structures by means of permanent electrodes implanted for relief of pain or involuntary movement disorders. In 1 individual, downward eye movements with ocular convergence occurred upon stimulation in the “posterior sensory thalamus.” Upward con- tralateral conjugate gaze was produced by unilateral stimulation in the ventral lateral thalamus. Smith et a1 [28] reported a patient who underwent left thalamotomy for postherpetic neuralgia. Postopera- tively she developed moderate paresis of downward gaze and complete inability to look up, associated with nystagmus retractorius and fine vertical nystag- m u .
The isolated paralysis of vertical saccades in our patient, with preservation of vertical pursuit and reflex movement, implies a bilateral lesion more ros- tral than the upper midbrain. The total loss of volun- tary cortical control of vertical movement leads to a release, or hyperactivity, of reflex vertical eye movement reminiscent of that seen in the horizontal plane in global horizontal saccadic paralysis. Because of rare random vertical saccades documented by elec- tronystagmography, our patient’s disorder is more properly termed an apraxia of vertical saccades. The designation vertical oculomotor apraxia emphasizes the striking replication of clinical features of horizontal oculomotor apraxia in a perpendicular eye movement plane.
Memory disturbance of the Korsakoff type (am- nesic or amnestic syndrome) is characterized primar- ily by inability to learn and retain new impressions, associated with inability to recall some past im- pressions but with retention of past behavior patterns [ 2 ] . Confabulation is not necessarily a feature. Bilat- eral lesions of the hippocampus, mammillary bodies, and posterior fornix have been implicated in the am- nesic syndrome.Victor [30] has emphasized that the amnesic syndrome due to thiamine deficiency is bet- ter correlated with damage to the medial dorsal nu- clei of the thalamus than with damage to the mammil- lary bodies. An amnesic syndrome has been de- scribed in patients with tumors of the floor and walls of the third ventricle, some of whom improve after surgical decompression [16, 331. Spiegel et al [291 found that a large proportion of patients with surgical lesions of the medial dorsal thalamic nuclei show transient memory disturbance.
Our patient demonstrated severe memory loss
Mills and Swanson: Vertical Oculomotor Apraxia and Memory Loss 151
with only mild residual loss of intellectual capacity following recovery from an apoplectic event with no antecedent illness. The absence of fever, cerebro- spinal fluid abnormalities, or hippocampal lesions on CAT scan [ 3 2 ] made a postencephalitic origin un- likely. There was no clinical or historical evidence to implicate a deficiency or toxic state. The rapidity of onset and the course of improvement, beginning within 2 4 hours, suggested a vascular cause with isch- emia and infarction secondary to embolus or arterial thrombosis. Since she had been taking birth control pills at the time her illness began, her risk of cerebral infarction was considerably greater than that of other women her age [91. Bickerstaff [41 emphasized the increased incidence of occlusion in the territory of the vertebrobasilar system that has occurred since the introduction of oral contraceptives. Enzell and Lin- dernalm [ 121 have stressed the likelihood of cerebral emboli occurring in women taking oral contracep- tives. In 4 of their 1 4 patients, arteriographic changes characteristic of embolus were present, but they em- phasize that after 2 4 hours the embolus might not be demonstrable. They suggest that the pulmonary ve- nous bed might be a source for emboli.
The hypokinetic, somnolent tendency of our pa- tient resembles that seen in the syndrome of akinetic mutism described with infarctions in the territory of the posterior thalamosubthalamic paramedian artery arising from the head of the basilar artery [26]. This territory is bilateral and includes the posteroinferior portion of the medial dorsal nuclei and the an- teromedial portion of the centrum medianum. Sev- eral incomplete cases of akinetic mutism, variously described as lethargic stupor or decreased spontane- ous activity with somnolence, have shown involve- ment more anteriorly in the thalamus [5, 61. These patients, who sleep unless stimulated but who are capable of speech and movement and who are some- what demented, resemble our patient closely.
Most interesting are previous reports of patients showing combinations of vertical gaze paresis, mem- ory loss, and disorders of alertness. Eleven cases of Parinaud syndrome associated with memory loss due to decompensation of hydrocephalus were reported by Cophignon et al [lo]. Vertical gaze palsy and akinetic mutism coexisted in Case 2 of Segarra [ 2 6 ] , in whom pathological examination showed butterfly- shaped infarctions involving the periventricular gray matter of the ventrocaudal walls of the third ventricle and extending laterally to the posterior thalami and the upper midbrain periaqueductal gray matter, pre- tectal areas, and posterior commissure. Castaigne et al [5] described 2 patients with decreased spontane- ous activity, memory loss, and vertical gaze paresis resulting from bilateral infarctions in the anterior and middle thalami. These patients were found to
have infarctions in the territory of the anterior thalamosubthalamic paramedian artery. In the case described by Angelergues et a1 [l], vertical eye movement paralysis with preservation of Bell's phe- nomenon was found in a confused patient with Kor- sakoff syndrome. Infarcts involved primarily the periventricular gray matter around the third ventricle and the periaqueductal gray matter. Akinesia was ab- sent, perhaps because of the lack of lateral thalamic reticular system involvement. Case 11 of Schuster [ 2 5 ] was a 49-year-old woman who suddenly became comatose. In addition to downgaze paresis with pres- ervation of downward movement to the ocu- locephalic maneuver, she showed marked apathy and decreased spontaneous activity. The lesions in- volved the periventricular gray matter around the third ventricle as well as the medial nuclei and me- dial parts of the lateral nuclei of the thalamus.
The unusual clinical combinations of memory loss, vertical gaze abnormalities, and mild akinetic mutism have all been related to bilateral involvement of the medial thalami and periaqueductal regions. Those cases examined pathologically have shown infarctions in the distribution of anterior or posterior thal- amosubthalamic paramedian arteries. Percheron [ 2 2 ] has shown that these paramedian arteries typi- cally arise from one branch of the basilar bifurcation but supply both sides of the thalamus. Thus, occlu- sion of one paramedian artery can produce bilateral involvement.
No pathological proof of the site of involvement exists in our patient. However, indirect evidence for a major thalamic area of involvement is provided by the CAT scan obtained two and a half years after the onset of her illness. Focal widening of the cephalad extremity of the third ventricle was found together with small, symmetrical zones of low absorption in both thalami corresponding to the dorsomedial nu- clei. Although this seems to provide good evidence for bilateral thalamic infarction as a cause of our pa- tient's symptoms, caution must be exercised in draw- ing that conclusion. Many small lesions could be pres- ent at other sites and escape detection on CAT scan. Our speculation that bilateral thalamic damage is re- sponsible for the observed symptom complex of ver- tical oculomotor apraxia, amnesic syndrome, and hypokinesia is based on circumstantial evidence: similarity to previously reported cases with patholog- ical proof and a CAT scan suggesting atrophy of thalamic substance.
References 1 . Angelergues R, deAjuriaguerra J, Hecaen H: Paralysie de la
verticalit6 du regard d'origine vasculaire. Rev Neurol (Paris) 96:301, 1957
2. Barbizet J: Human Memory and Its Pathology. San Francisco, Freeman, 1970
152 Annals of Neurology Vol 4 No 2 August 1978
3. Bender MG: Comments on the physiology and pathology of eye movements in the vertical plane. J Nerv Ment Dis 130: 156, 1960
4. Bickersraff E R Neurological Complications of Oral Con- traceptives. Oxford, Engl, Clarendon, 1976
5. Castaigne P, Buge A, Cambier J, et al: DPmence thalamique d'origine vasculaire par ramollissement bilateral, limite au ter- ritoire du pedicule retro-mamillaire. Rev Neurol (Paris) 114239, 1966
6. Castaignc P, Buge A, Escourolle R, et al: Ramollissemcnt p6donculaire median, tegmento-thalamique avec ophtalmo- plCgie et hypersomnie. Rev Neurol (Paris) 106:357, 1962
7. Cogan DG: Congenital ocular motor apraxia. Can J Ophthal- mol 1:253. I966
8. Cogan DG, Adams RD: A type of paralysis of conjugate gaze (ocular motor apraxia). Arch Ophthalmol 50:434. 1953
9. Collaborative Group for the Study of Stroke in Young Women: Oral contraception and increased risk of cerebral ischemia or thrombosis. N Engl J Mcd 288:871, 1973
10. Cophignon J, George 8 , Visot A, et al: Syndrome de Pari- naud et troubles mnesiques au cours des poussees de dCcom- pensation de I'hydrociphalie non tumorale de I'adulte. Neurochirurgie 22:124, 1976
11. Corin MS. Mones RJ, Elizan TS, et al: Paresis of vertical gaze in basal ganglia disease. Mt Sinai J Med NY 39:330, 1972
12. Enzell K, Lindernalm G: Cryptogenic cerebral embolism in women taking oral contraceptives. Br Med J 4:507. 1973
13. Gay AJ, Newman NM, Keltner JL, et al: Eye Movement Disorders. St Louis, Mosby, 1974, p 20
14. Gyldensted C, Kosteljanetz M: Measurements of the normal ventricular system with computer tomography of the brain: a preliminary study on 44 adults. Neuroradiology 10:205, 1976
15. Hoyt WF, Daroff RB: Supranuclear disorders of ocular con- trol systems in man-clinical, anatomical, and physiological correlations-1969, in Bach-y-Rita P, Collins CC (eds): The Control of Eye Movements. New York, Academic, 1971, p 175
16. Ignelzi RJ, Squire LR: Recovery from anterograde and retro- grade amnesia after percutanenus drainage of a cystic craniopharynpjoma. J Neurol Neurosurg Psychiatry 39: 123 1, 1976
17. Jacobs L, Anderson PJ, Bender MB: The lesions producing paralysis of downward but not upward gaze. Arch Neurol 28:319, 1973
18. Ling W, Gay AJ: Optokinetic nystagmus: a proposed path- way and clinical application, in Smith JL (ed): Neuro- ophthalmology. St Louis, Mosby, 1968, vol 5, p 117
19. Nashold BS, Gills JP: Ocular signs from brain stimulation and lesions. Arch Ophrhalmol 77:609, 1967
20. Nashold BS, Seaber JH: Defects of txular motility after stereotactic midbrain lesions in man. Arch Ophthalmol H8:245, 1972
21. Pasik P. Pasik T, Bender MB: The pretectal syndrome in monkeys: I. Disrurbances of gaze and body posture. Brain 92:521, 1969
22. Percheron GMJ: Etude anatomique du thalamus de I'homme d u l t e et de sa vascularisation arterielle. Thesis, Paris, 1966 (cited by Segarra [261)
23. Pfaffenbach DD, Layton DD, Kearns T P Ocular manifesta- tions in progressive supranuclear palsy. Am J Ophthalmol 74:1179, 1972
24. Sanders MD, Wybar KC: Vertical supranuclear ophthal- moplegia with compensatory head movcmcnts: report of a case with lipidosis, in Strabismus '69. St Louis, Mosby, 1970,
25. Schuster P: Beitfage zur Pathologie des Thalamus Opticus. Arch Psychiatr Nervenkr 105:358. 550, 1936
26. Segarra JM: Cerebral vascular disease and behavior: I . The syndrome of the mesencephalic artery (basilar artery bifurca- tion). Arch Neurol 22:408, 1970
27. Shanzer S, Bender MB: Oculomotor responses on vestibular stimulation of monkeys with lesions of the brainstem. Brain 82:669, 1959
28. Smith JL, Nashold BS, Kreshon MJ: Ocular signs after stereotactic lesions in the pallidum and thalamus. Arch Ophthalmol 65:532, 1961
29. Spiegel EA, Wycis HT, Orchinik C, et al: Thalamic chronotaraxis. Am J Psychiatry 1 1 3:97. 1956
30. Victor M: The amnesic syndrome and its anatomical basis. Can Med As= J 100: 11 15, 1969
31. Walsh FB, Hoyt W F Clinical Neuro-ophthalmology. Balti- more, Williams & Wilkins, 1969, p 2 14
32. Wechsler AF. Guisado R. Bentson J R Pneumoencephalo- graphic demonstration of the anatomic basis of a postenceph- ahtic Korsakoff syndrome. Mt Sinai J Med NY 41:230, 1974
33. Williams M, Pennybacker J: Memory disturbances in third ventricle tumors. J Neurol Ncurosurg Psychiatry 17:115. 1954
P 63
Mills and Swanson: Vertical Oculomotor Apraxia and Memory Loss 153