using transcranial magnetic stimulation to improve our ... transcranial magnetic stimulation to...
TRANSCRIPT
Using Transcranial magnetic stimulation to improve our understanding of
Transverse Myelitis
Kathy Zackowski, PhD, OTR Kennedy Krieger Institute
Johns Hopkins University School of Medicine

§ TMS (transcranial magnetic stimulation) § Definition § Applications
> Diagnostic tool > Therapeutic intervention
§ Studying brain and spinal cord function in Transverse Myelitis

• In the last 3 decades our view of the CNS has changed.
• Formerly believed to be a rigid structure, not
plausible of changing, now believed to be plastic and dynamic, constantly changing.
• The change in dogma resulted from
technological advancement in all levels • Human studies => PET, fMRI, TMS, MEG
Courtesy of Pablo Celnik

TMS Transcranial magnetic stimulation is a tool used to study: • connectivity of neuronal pathways • cortical plasticity and its mechanisms • behavioral consequences of noninvasive
transient inactivation of specific cortical sites.
v Electrophysiological results could indicate the underlying systems or pathways effected and, provide useful insight into the mechanism of action.

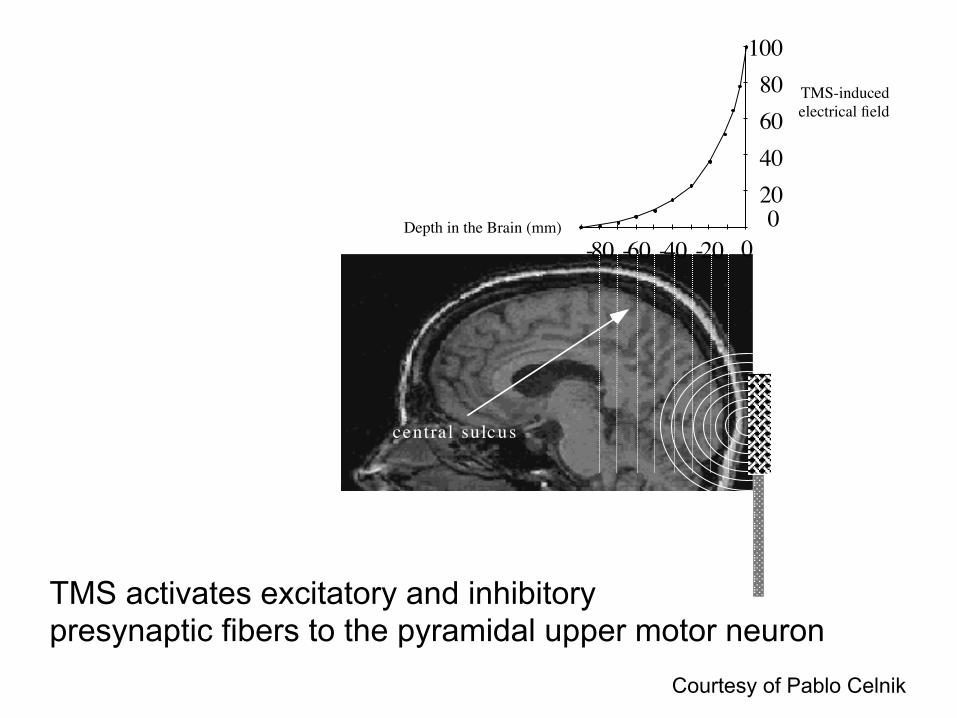
An electric pulse induces a rapidly changing magnetic field with lines of flux that runs�perpendicular to the coil.
Courtesy of Pablo Celnik
2 0 4 0 6 0 8 0
1 0 0
0
- 6 0 - 4 0 - 2 0 0 - 8 0
c e n t r a l s u l c u s
TMS-induced electrical field
Depth in the Brain (mm)
TMS activates excitatory and inhibitory presynaptic fibers to the pyramidal upper motor neuron
Courtesy of Pablo Celnik

Motor Evoked Potential MEP
(Measurement of cor/cal excitability)
Courtesy of Pablo Celnik

Similar to peripheral nerve studies, conduction time is measured from different stimulation sites (i.e. Motor cortex, brainstem, cervical roots)

1. Diagnostic tool a) Central conduction time b) Measuring cortical excitability
• Motor Threshold • Recruitment Curves • Intracortical Inhibition (ICI) • Intracortical Facilitation (ICF) • Interhemispheric inhibition (IHI)
c) Probing cortical function
2. Therapeutic intervention a) To induce plasticity b) To modulate behavior

Motor Threshold (MT) • Lowest stimulus intensity that evoke MEP of 50
mV in 5 of 10 trials in a target muscle during 2% reductions in intensity from above threshold (Rossini 1994)
• Drugs that block voltage-gated sodium channels elevate motor threshold (Ziemann 1996)
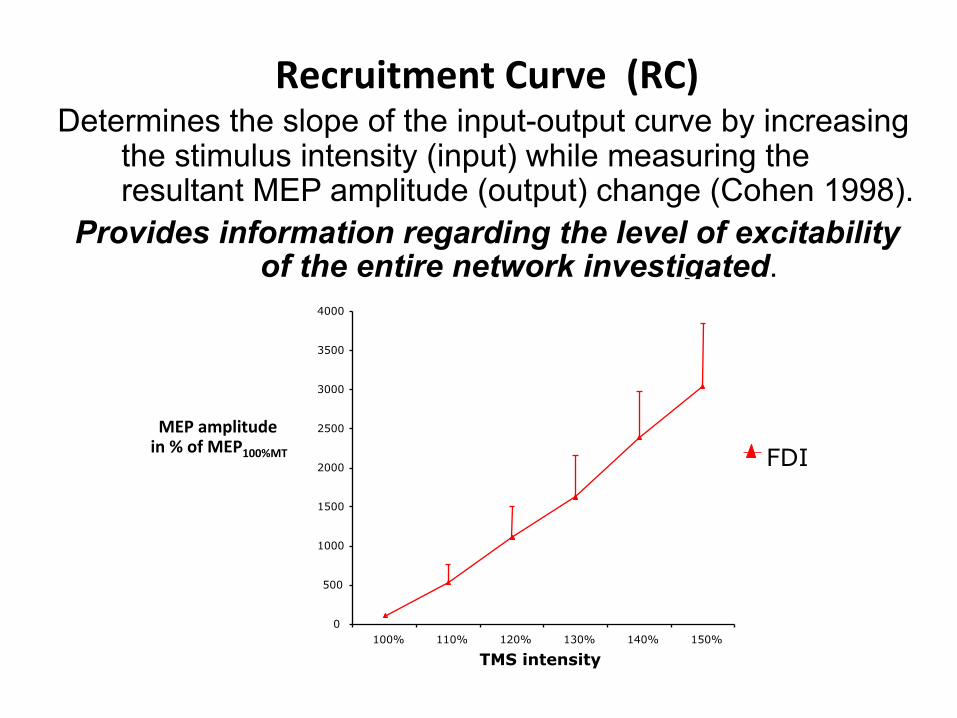
Recruitment Curve (RC) Determines the slope of the input-output curve by increasing
the stimulus intensity (input) while measuring the resultant MEP amplitude (output) change (Cohen 1998).
Provides information regarding the level of excitability of the entire network investigated.
FDI MEP amplitude in % of MEP100%MT
TMS intensity 0
500
1000
1500
2000
2500
3000
3500
4000
100% 110% 120% 130% 140% 150%

Intracortical Excitability • Short Intracor/cal Inhibi/on (sICI) • Short intracor/cal Facilita/on (sICF)"
sICI
GABA
sICF
Glutamate
2 msec 10 msec
-1.5
0
1
Test pulse
mV

Intracortical Excitability • Short Intracor/cal Inhibi/on (sICI) • Short intracor/cal Facilita/on (sICF)"
Interstimulus Interval (ms)

What studies have been done involving transverse myelitis?

Ø an isolated lesion in the posterior white columns of the spinal cord may lead to long-term changes in motor cortex. Can sensory training help?

Motor-Evoked Potentials in a Child Recovering from Transverse Myelitis
Yukio Noguchi, MD, Osami Okubo, MD, Tatsuo Fuchigami, MD,
Yukihiko Fujita, MD, and Kensuke Harada, MD
Ø Motor recovery paralleled MEP improvements

Please cite this article in press as: P.H. Ellaway, et al., Development of quantitative and sensitive assessments of physiological and functionaloutcome during recovery from spinal cord injury: A Clinical Initiative, Brain Res. Bull. (2010), doi:10.1016/j.brainresbull.2010.08.007
ARTICLE IN PRESSG Model
BRB-8182; No. of Pages 15
8 P.H. Ellaway et al. / Brain Research Bulletin xxx (2010) xxx–xxx
Fig. 4. Mean changes over the 6-week exercise period in maximal motor evoked potentials (MEPs) elicited by transcranial magnetic stimulation (TMS). TMS stimulus pulseswere applied over the vertex of the cranium (schematic on right). MEPs were recorded with the subjects at rest, at four motor points corresponding to C5, C6, C7 and C8/T1spinal segmental levels. Motor points and treatment groups are represented by different coloured lines and symbols as listed in the middle. Note the increasing trend after6 weeks in biceps and wrist extensor MEPs in the ReJoyce treatment group. This suggests increasing cortico-motoneuronal excitability through C5 and C6 segments.
icance was not reached. MEPs in the other two muscle groupsremained unchanged.
The contrast between the clear improvements in the functionaltests and the ambiguity of the TMS results raises two questions.First, were the functional improvements due to neuronal plas-ticity leading to improved connectivity between the brain andspinal motoneurons, or were they due to a combination of musclestrengthening and improved control of the available musculature?Second, is TMS a useful outcome measure for SCI treatments? Withregard to neuronal plasticity, our TMS data were consistent withan improvement in connectivity at C5 and C6 levels, but statisticalsignificance was not reached, so this question remains open. It isworth pointing out that TMS may not excite all of the pathwaysfrom supraspinal to spinal centres that could be involved in func-tional gains. Regarding the utility of TMS as an outcome measure, itis clearly not a reliable surrogate for the functional tests related toADLs. However it remains one of the few methods available for elu-cidating neural plasticity that may underlie the functional gains, soif neuronal mechanisms are the focus, TMS remains an importanttool.
The lack of statistically significant changes in EPTs indicatedeither that there was no change in the segmental distribution ofsensory inputs, or that the EPT method did not have sufficient res-olution to detect any changes that may have occurred. The samplesizes in the sub-group analyses comparing incomplete and com-plete participants were too small to allow conclusions to be drawnregarding the small differences in the time courses of improvement.
4. Comprehensive evaluation of the physiological andfunctional adaptations induced by Lokomat training inincomplete spinal cord injured subjects (B.A. Conway, S.Galen, C.J. Catton, D.B. Allan)
WAT training is a recognized rehabilitation paradigm that canaid in improving gait in patients with incomplete paraplegia [23].This approach to gait rehabilitation can be accomplished by pro-viding patients with intensive gait training in which a body weightsupport system is used in conjunction with a moving treadmill. Thetraining is provided either via manual assistance or robotic devicesthat assist the patient to move their legs with kinematics remi-niscent of normal stepping [22]. In this component of the ClinicalInitiative a robotic driven gait orthoses (Lokomat) was used to pro-vide gait training for incomplete spinal cord injury patients. Forthe purpose of this study the Lokomat provided an intervention onwhich an evaluation on the effectiveness of a battery of assessmenttests able to identify changing functional outcome or physiologywere investigated. A number of Quantitative Sensory Tests devel-oped from phase 1 of the ISRT Clinical Initiative [26] were includedtogether with standard clinical assessments, gait outcome mea-sures and additional sensory and motor assessments as listed inTable 2. The work presented here will focus on results on func-tional outcome and sensory tests including Electrical PerceptualThreshold (EPT) and Somatosensory Evoked Potentials (SSEP). Amore detailed description of the results of these and other testswill be presented elsewhere.
Fig. 5. Mean electrical perceptual thresholds (EPTs) in response to stimulation at five ASIA sensory testing points corresponding to sensory inputs to C5, C6, C7 and C8 spinalsegmental levels. (A) Conventional treatment group, (B) ReJoyce treatment group.
Please cite this article in press as: P.H. Ellaway, et al., Development of quantitative and sensitive assessments of physiological and functionaloutcome during recovery from spinal cord injury: A Clinical Initiative, Brain Res. Bull. (2010), doi:10.1016/j.brainresbull.2010.08.007
ARTICLE IN PRESSG Model
BRB-8182; No. of Pages 15
Brain Research Bulletin xxx (2010) xxx–xxx
Contents lists available at ScienceDirect
Brain Research Bulletin
journa l homepage: www.e lsev ier .com/ locate /bra inresbul l
Review
Development of quantitative and sensitive assessments of physiological andfunctional outcome during recovery from spinal cord injury: A Clinical Initiative
P.H. Ellawaya,!, A. Kuppuswamya, A.V. Balasubramaniama, R. Maksimovica, A. Gallb, M.D. Craggsb,c,C.J. Mathiasa, M. Bacond, A. Prochazkae, J. Kowalczewskie, B.A. Conwayf,g, S. Galenf,g, C.J. Cattonf,D.B. Allang, A. Curth, B. Wirthh,i, H.J.A. van Hedelh
a Department of Clinical Neuroscience, Imperial College, London W6 8RP, UKb The London Spinal Cord Injuries Centre, Royal National Orthopaedic Hospital NHS Trust, HA7 4LP, UKc Institute of Orthopaedics and Musculoskeletal Science, Division of Surgery and Interventional Science, University College London WC1E 6BT, UKd International Spinal Research Trust, Bramley, GU5 0AZ, UKe Centre for Neuroscience, University of Alberta, Edmonton, AB, Canada T6G 2S2f Bioengineering Unit, University of Strathclyde, Glasgow G4 0NW, UKg Queen Elizabeth National Spinal Injuries Unit, Southern General Hospital, Glasgow, UKh Spinal Cord Injury Center, University of Zurich and Balgrist University Hospital, CH-8008 Zurich, Switzerlandi Institute of Human Movement Sciences and Sport, ETH Zurich, CH-8092 Zurich, Switzerland
a r t i c l e i n f o
Article history:Received 16 February 2010Received in revised form 11 August 2010Accepted 12 August 2010Available online xxx
Keywords:Spinal cord injuryOutcome measuresSensorimotor functionRehabilitation
a b s t r a c t
The ability to detect physiological changes associated with treatments to effect axonal regeneration, ornovel rehabilitation strategies, for spinal cord injury will be challenging using the widely employed Amer-ican Spinal Injuries Association (ASIA) impairment scales (AIS) for sensory and motor function. Despitemany revisions to the AIS standard neurological assessment, there remains a perceived need for more sen-sitive, quantitative and objective outcome measures. The purpose of Stage 1 of the Clinical Initiative wasto develop these tools and then, in Stage 2 to test them for reliability against natural recovery and treat-ments expected to produce functional improvements in those with complete or incomplete spinal cordinjury (SCI). Here we review aspects of the progress made by four teams involved in Stage 2. The strategiesemployed by the individual teams were (1) application of repetitive transcranial magnetic stimulation(rTMS) to the motor cortex in stable (chronic) SCI with intent to induce functional improvement of upperlimb function, (2) a tele-rehabilitation approach using functional electrical stimulation to provide handopening and grip allowing incomplete SCI subjects to deploy an instrumented manipulandum for handand arm exercises and to play computer games, (3) weight-assisted treadmill walking therapy (WAT)comparing outcomes in acute and chronic groups of incomplete SCI patients receiving robotic assistedtreadmill therapy, and (4) longitudinal monitoring of the natural progress of recovery in incomplete SCIsubjects using motor tests for the lower extremity to investigate strength and coordination.
© 2010 Elsevier Inc. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 001.1. Proof of principle and underlying mechanisms of treatments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 001.2. Confounding issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 001.3. The Clinical Initiative . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
2. The Clinical Initiative—a quest for reliable and sensitive assessments of outcome after treatments for spinal cord injury(P.H. Ellaway, A. Kuppuswamy, A.V. Balasubramaniam, Maksimovic R, A. Gall, M.D. Craggs, C.J. Mathias) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 002.1. Sensitivity of EPT test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 002.2. Reliability of EPT measures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 002.3. EPT as a measure of the dorsal (posterior) column pathway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
! Corresponding author at: Department of Clinical Neuroscience, Imperial College, Charing Cross Campus, St Dunstan’s Road, London W6 8RP, UK. Tel.: +44 2033117593;fax: +44 2033117577.
E-mail address: [email protected] (P.H. Ellaway).
0361-9230/$ – see front matter © 2010 Elsevier Inc. All rights reserved.doi:10.1016/j.brainresbull.2010.08.007
Ø Motor recovery paralleled MEP changes. Sample size small!

• TMS can be used to understand brain processes (diagnostic tool) or to induce plastic changes (therapeutic tool) like excitability changes or modulation of behavior.
• Understanding the basic physiology mechanisms associated to motor behavior has permitted the development of novel strategies to enhance recovery processes in patients with CNS lesions.

How can we use this technique to provide additional information about TM?
² Evaluate the effectiveness of a known pharmacologic therapy

New Study Efficacy of Sustained Release Oral Dalfampridine in Transverse Myelitis Site Johns Hopkins University, Transverse Myelitis Center Study Investigators
Michael Levy Carlos Pardo Daniel Becker Kathleen Zackowski

h;p://ampyra.com/about-‐ampyra/what-‐is-‐ampyra/
What is Oral Dalfamridine (Ampyra)?
Fampridine (4-aminopyridine) -Amplified conductivity in demyelinated peripheral nerves -Limited therapeutic window due to stimulation of seizure activity

What do we know about dalfamradine’s effects?

(Goodman et al., 2009)
Results:

Dalfampridine, a sustained-release potassium channel blocker that has been shown to be effective in improving gait and other neurologic functions in people with MS. Dalfampridie has the potential to improve gait and neurologic function in patients with TM because it shares a similar pathogenic process with MD. ² We hypothesize that Dalfampridine will improve gait
and neurologic function in patients with TM, and that TMS will improve our understanding of what the characteristics are for “responders”.

0
2 4 8 10 12 16
18
6 14
20
2-‐week Placebo Run-‐in
8-‐week cross over treatment period
Dalfampradine
Placebo
2-‐week Follow-‐up
Dalfampradine
Placebo
Week
Study Protocol for TM:

Inclusion criteria for this study include: • Diagnosis of idiopathic transverse myelitis confirmed by
MRI
• Gait impairment defined by a timed 25-foot walk
• Age 18-70 yrs
We are happy to answer questions about this study.
Email Maureen Mealy at [email protected] if you are interested in participating.

Thank you for your support!
