using motivational interviewing with adolescents: can · pdf fileusing motivational...
TRANSCRIPT
Using Motivational Interviewing with Adolescents: Can we talk?
Pam Burke PhD, RN, FNP, PNP, FSAHM, FAAN
AMERSA Workshop
11-8-13 2:15-3:45 pm

I have
NO

Workshop Objectives
1. To examine the use of motivational interviewing in SBIRT with adolescents.
2. To explore the use of selected tools with motivational interviewing.
Overview
• Highlights from MI3
• MI Micro-Skills – OARS
• Tools for use with MI
Role Play
• Evoking and responding to Change Talk
• Recognizing and responding to Sustain Talk & Discord
What’s the Game Plan?
The Wisdom is in the Room
Bill Miller PhD Steve Rollnick PhD
Arkowitz, Westra, Miller, Rollnick (2008) Motivational Interviewing in the Treatment
of Psychological Problems. New York: Guilford Press.
Hohman, M (2011) Motivational Interviewing in Social Work Practice. New York:
Guilford Press.
Matulich. (2013) How To Do Motivational Interviewing: A Guidebook for Beginners
(2nd ed.) e-book ($6.97) http://www.motivationalinterviewingonline.com/ebook.html
Miller & Rollnick (2013) Motivational Interviewing: Helping People Change. (3rd ed.)
New York: Guilford Press.
MINT (MI Network of Trainers) Website http://www.motivationalinterviewing.org
Naar-King & Suarez (2011) Motivational Interviewing with Adolescents and Young
Adults. New York: Guilford Press.
Rosengren, D (2009) Building Motivational Interviewing Skills: A Practitioner
Workbook. New York: Guilford Press.
Wagner, C & Ingersoll, K (2012) Motivational Interviewing in Groups. New York:
Guilford Press.
2012 (3rd ed.)

From the website: Welcome to Group MI for Teens! Here you'll find guidance on facilitating our motivational interviewing-based interventions in group settings with adolescents. Register to view training videos, download intervention materials, get continuing education credits, and explore MI resources – all free of charge.
https://groupmiforteens.org
Rand Corp NIH Funded

Motivational Interviewing (MI)
"Motivational Interviewing is a collaborative, goal-oriented style of communication with particular attention to the language of change. It is designed to strengthen the personal motivation for and commitment to a specific goal by eliciting and exploring the person's own reasons for change within an atmosphere of acceptance and compassion." Miller & Rollnick (2013) Motivational Interviewing: Helping People Change (3rd ed.) New York: Guilford Press (p. 29)

Spirit of MI: Collaboration Acceptance Compassion Evocation
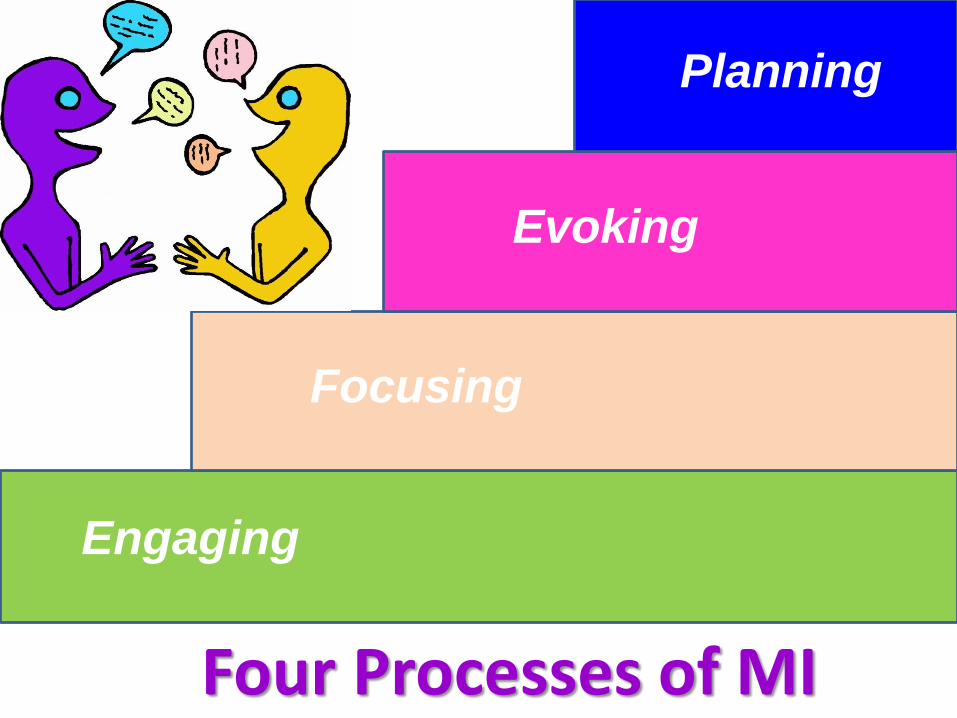
Engaging
Focusing
Evoking
Planning
Four Processes of MI

Bill Miller’s Metaphor:
MI Hill
Contemplation Preparation Action (Pre-)

Flow of Change Talk
Desire
Ability
Reasons
Need
Commitment
Change
MI

Change Talk • Change talk is any client speech that favors movement in the direction of change • Change talk is linked to a particular behavior change goal
DARN CATs
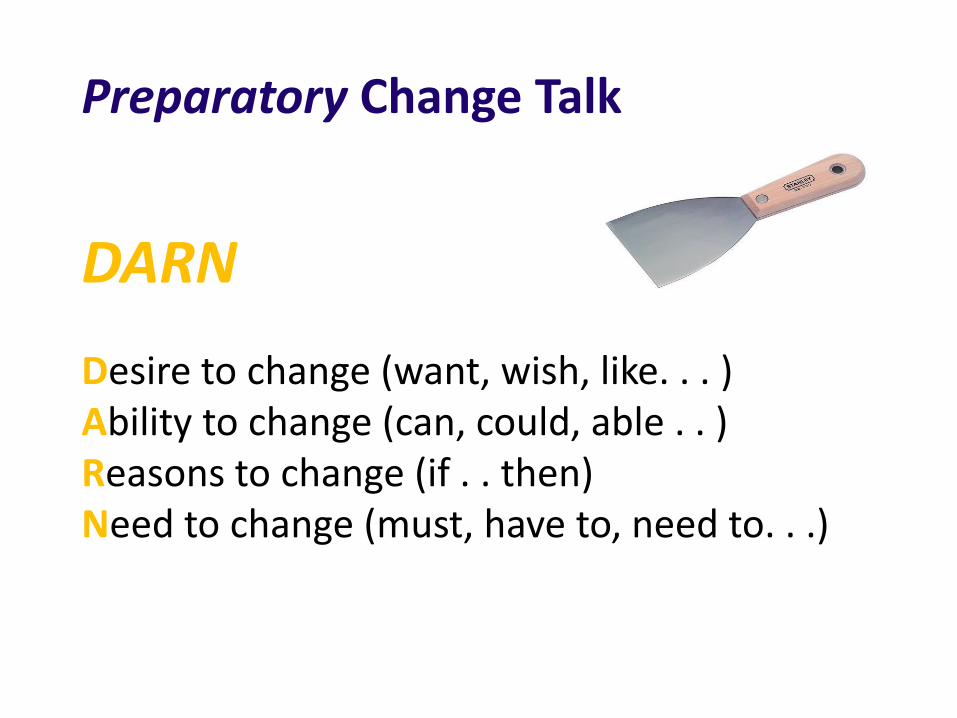
Preparatory Change Talk
DARN
Desire to change (want, wish, like. . . ) Ability to change (can, could, able . . ) Reasons to change (if . . then) Need to change (must, have to, need to. . .)
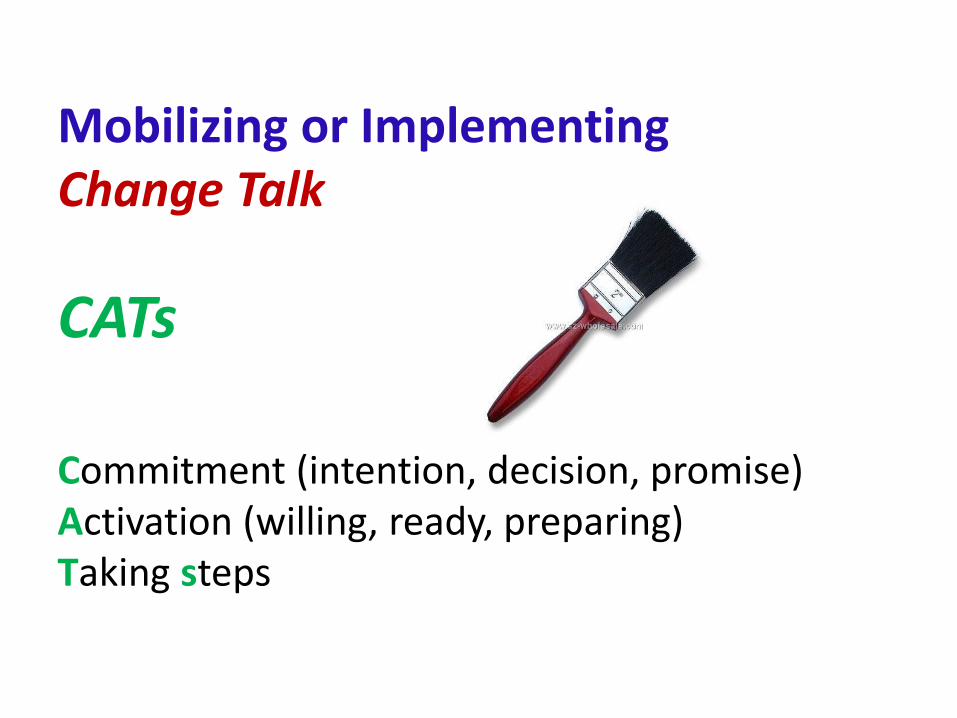
Mobilizing or Implementing Change Talk
CATs
Commitment (intention, decision, promise) Activation (willing, ready, preparing) Taking steps

Responding to Change Talk
Be all EARS
E: Elaborating: Asking for elaboration, more
detail, in what ways, an example, etc.
A: Affirming: Commenting positively on the
person’s statement
R: Reflecting: Continuing the paragraph, etc.
S: Summarizing: Collecting bouquets of change talk

Acronym for MI Skills: OARS
O = Open-ended Questions
A = Affirmations
R = Reflective Listening
S = Summaries

Open-Ended Questions
Please describe your early experiences
with marijuana use.
How have your friends reacted to your
marijuana use?
Where are you at as far as cutting down
on your marijuana use?
Open-ended questions elicit more of the person’s
thoughts and feelings about a behavior, which is
likely to help evoke change talk.
Closed-Ended Questions
How old were you when you first used
marijuana?
Do your family or friends think you
should quit smoking marijuana?
Are you ready to cut down on your
marijuana use?

• Emphasize a strength, but focus on specific behaviors instead of attitudes, decisions, and goals.
• Attend to non-problem areas rather than problem areas.
• Nurture a competent instead of a deficit worldview of patients.
• Think of affirmations as attributing interesting qualities to patients.
• Focus on descriptions and not evaluations. Compliments typically have an evaluative judgment implicit within them.
• Express positive regard and caring.
• Be genuine.

Examples Compliments vs. Affirmations
Obese male who lost 50 lbs in a year. C I think you look fit and trim.
A You put a lot of effort into exercising and made healthy changes to your diet.
New mother with a history of drug abuse. C I applaud you for getting off drugs when you discovered you were
pregnant.
A You decided to stop drugs for the sake of your health and your baby’s health. That took a great deal of determination and hard work.
Female quit smoking after young cousin had fatal MI. C I think it’s great that you quit smoking.
A You thought through the risks of smoking and made the decision to quit to avoid developing heart disease.
Reflective Listening
Reflective Listening
• Reflections are statements, not questions.
• Provider makes a guess about what the person means or feels. There’s no penalty for missing. Reflections don’t have to perfect!
• Reflections provide more information and better understanding than questions. They encourage person to elaborate, amplify, confirm or correct.
• Feeling truly understood and accepted by a provider, can make a patient more open to considering behavior change.
• In general, a reflection should not be longer than the patient’s statement.

• Simple Reflection: (simple, stabilizing) – Repeating an element of what the patient said.
– Rephrasing what the patient said but in different words.
• Complex Reflection: (deep, forward moving) – Paraphrasing (making a guess about) the meaning or feelings
implied by the patient’s words.
– Similes or Metaphors and Continuing the Paragraph are also complex reflections.
• Double-Sided Reflection: acknowledges both sides of a person’s ambivalence. Use and to connect the two sides rather than but.
• Amplified Reflection: exaggerates the point so that the patient disavows or disagrees. A variation is an understatement, which minimizes the point. Do not overdo it. Patients who feel mocked or patronized, may respond with anger.

Forming Reflections
• Your voice should go down at end so it does not sound like a question (e.g., avoid Valley-girl style speech).
• Some ways to open: So you feel… It sounds like you…
You’re wondering if… It seems to you that…
You’re feeling… You…
• Note that you do not need to preface with: So what I hear you saying is…
Let me see if I understand you correctly….
“My parents are always on my case about
smoking. They search my room for my cigarettes, they listen in on my phone calls, they smell my clothes and breath and they sometimes check my backpack and pockets for cigarettes or matches.
How might a professional respond to the following?

Possible Responses: Using simple reflection (saying what the person has said, but in
different words): “They bug you about smoking and they spy on you about it.” or Using reflection of meaning (restating the meaning that may be implied by the words): “As though they’re always trying to figure out if and when you’re smoking.” or Using reflection of feeling (restating what you perceive to be the feeling conveyed in the statement): “It’s annoying to you, for them to get on your case like that.”
Double-Sided Reflection
“So you really enjoy smoking, and you’re worried that it might be hurting your health.”
or
“You’re not sure that you want to stop smoking , and, at the same time, you don’t want to get into any more trouble with your parents.”
27

Amplified Reflection Patient: But I can't quit smoking. I mean, all of my friends smoke!
Provider: So you really couldn't quit using because then you'd be too different to fit in with your friends.
Patient: Well, that would make me different from them, but they might not really care as long as I didn't try to get them to quit.
28
Collects material that has been offered
or
Links something just said with something discussed earlier
or
Draws together what has happened and transitions to a new task.
Like a bouquet

Collect material that has been offered.
“So far you’ve expressed concern about your parents’ divorce, your brother’s deployment, and feeling pressured to apply to an Ivy league college.”
Link something just said with something discussed earlier.
“That sounds a bit like what you told me earlier about that lonely feeling you get.”
Draw together what has happened and transition to a new task or topic.
“Before I ask you the questions I mentioned earlier, let me summarize what you’ve told me so far, and tell me if I’ve missed anything important. You came in because you have been having trouble concentrating, and . . . “
Like a Bouquet

Change Talk and Sustain Talk (Ambivalence)
Opposite sides of the same coin
Examples of Sustain Talk The other side of ambivalence
• I really enjoy marijuana (D) • I don’t think I can give up pot (A) • I have to smoke to be creative (R) • I don’t think I need to quit (N) • I intend to keep smoking and (C) nobody can stop me • I’m not ready to quit (A) • I bought a new water pipe (T)

Sustain Talk and Discord • Sustain Talk is about the target behavior I really don’t want to stop smoking. I have to have my pills to make it through the day.
• Discord is about the provider-patient relationship You can’t make me quit. You don’t understand how hard it is for me.
• Both are highly responsive to counselor style
What is Discord? • Behavior • Interpersonal (It takes two to have discord) • A signal of dissonance in your relationship • Predictive of non-change
Some Discord Signals Defensiveness Arguing
• Challenging • Discounting • Hostility
Interrupting • Talking over the counselor
Ignoring • Inattention • Changing the subject

STRATEGIES for Dealing with Discord and Sustain Talk

Emphasize Personal Choice - Autonomy
• When people perceive that their freedom of choice is being threatened, they tend to react by asserting their liberty. It is as if they are saying to themselves: I’ll show you; nobody tells me what to do!
• Assure the person that truly, in the end, it is s/he who determines what happens (i.e., autonomy). Early assurance of this kind can diminish resistance. For example:
“Whether or not you decide to cut down on your marijuana use will be your choice. ”

Shifting Focus If the patient feels pressured or becomes
argumentative, then acknowledge their
frustration and shift the focus. For example:
Patient: How many times do I have to tell you, birth control medicine makes me nauseous and screws up my periods. I’ve tried a hundred times and I just can’t take any of that stuff.
Provider: It’s been frustrating trying to find a birth control medicine that works for you and having us ask you about it every time you come to clinic. Let’s put that aside for now and talk about what brought you here today.
Reframing
• You invite patients to examine their perceptions in a new light or a reorganized form. In this way, new meaning is given to what has been said.
• For example, if a patient reports “I can drink most of my room mates under the table. I mean I can easily have 5 or 6 beers and not even feel drunk."
• You can reframe this as “Your inner warning signal about alcohol doesn’t turn on like your friends. You’ve developed such a high tolerance that you probably
become legally drunk before you feel it."

Agreement with a Twist
This retains a sense of consonance between you and the patient, while allowing you to continue to influence the direction of change. Offer initial agreement, but with a slight twist or change of direction. For example:
Patient: “Smoking cigarettes calms me. If I quit then I’d probably be a basket case. My parents should stop bugging me to quit.”
Provider: “Smoking is the main way you relax. Your parents are so worried about your health that they keep trying to get you to stop smoking.
Siding with the Negative Provider: “Maybe yoga or meditation or other
relaxation techniques won’t help your headaches. You don’t have to try these if you are not ready or interested.”
The Righting Reflex
• Usually expressed in the form of a strong persuasive effort
– Practitioner takes center stage in making the case for the person to change behavior.
• Human beings seem to have a built-in desire to set things right.
• Born of concern and caring.
– There’s a problem, let’s fix it!
• Fails to consider ambivalence in the change process.
– May engender resistance.

it is more like dancing
is not wrestling…
Motivational Interviewing

Tools for use with MI
• Agenda Map
• Decisional Balance (Pros & Cons) - Ambivalence
• Readiness/Importance/Confidence Rulers – Ready, Willing, Able?
• Value Card Sort - Developing Discrepancy
• Change Plan – Why, What, When, How, What if?

Agenda Map

Sleep
Agenda Map example – patient with heavy MJ use
School
Job Search
Alcohol
Tobacco
Relationships

Decisional Balance

Making a change
Not making a change
Pros/Benefits Cons/Costs
Life could be better I like my life the way it is
I wouldn’t have to give
up something I enjoy
What I enjoy now could
eventually harm me

I’ll save money.
My parents will stop
nagging me to quit.
My grades would improve.
Smoking makes me mellow
I can continue to socialize
with friends.
I think more creatively
when I am high.
It will be difficult to be
around my friends who
smoke.
I will feel irritable and more
anxious.
I might drink more.
If I apply for a job that does
drug testing, then I’d fail.
I could increase my
risk of getting cancer.
I might not get into college
Reduce MJ use Make a change
Keep using MJ Not make
a change
Pros/Benefits Cons/Costs

Decisional Balance Scale

RATING RULERS

“How ready are you to …?”
“How important is it to you to …?”
“How confident are you that …?”
Not at all Extremely
0 1 2 3 4 5 6 7 8 9 10
Assessing Readiness,
Importance, and Confidence

“How ready are you to …?”
Not at all
Ready
Extremely
Ready 0 1 2 3 4 5 6 7 8 9 10
Assessing Readiness
“What makes you say 3?”
“Why a 3 and not a 1 or 2?
“What would it take to move up a point?”
“How important is it to you to …?”
Not at all
important
Extremely
important 0 1 2 3 4 5 6 7 8 9 10
Assessing Importance
“What makes you say 4?”
“Why a 4 and not a 1 or 2?
“What would it take to move up a point?”
“What is something difficult that you set your mind to
doing in the past and succeeded at?”
“How confident are you that you will be able to eventually …?”
Not at all
confident
Extremely
confident 0 1 2 3 4 5 6 7 8 9 10
Assessing Confidence
“What makes you say 6 and not a 2 or 3?
“What might help you to get to a 7 or 8?”
Value Card Sort


Change Plan Worksheet • The most important reasons why I want to make this change are:
• My main goals in making this change are:
• I plan to do these things to accomplish my goals:
Specific Action? When?
• Other people could help me with change:
Person? Possible ways they can help?
• There are some possible obstacles to change:
Possible obstacles? How I could handle?
• I will know that my plan is working when I see these results:
• Seek to understand the patient's frame of reference • Express acceptance and affirmation • Elicit and selectively reinforce the patient's:
– self motivational statements, problem recognition, concerns – desire, ability, reasons and need to change
• Elicit/increase the strength of the patient’s commitment to change and specific implementation intentions.
• Elicit-Provide-Elicit – Elicit patient’s ideas, needs
– Provide relevant advice, information * – Elicit patient’s reactions and commitment to change
To Summarize:
Behavioral Characteristics of
Motivational Interviewing
* Ask for permission unless patient asked for your advice.

Role Play Time

Role Play in Triads Goal: REFLECTIVE LISTENING SKILLS
Providers: You will use reflective listening skills. Try to use all of the various forms of reflective listening during your role play. If you feel stuck, then you can call freeze to confer with the observer.
Patients: If you feel frustrated or misunderstood, then call freeze to confer with your provider. NOTE: To save time and avoid your having to make up a patient scenario, a brief vignette is provided (next slide). You can then tap into your creative acting skills.
Observers: After the role play, you will offer feedback on what you saw as strengths in the interaction and give a short summary of the patient’s motivations for change. If you observe an important teachable moment during the role play then you may judiciously call freeze and point that out.
TJ is a 16 yo male who smokes marijuana
I only smoke on weekends if I’m at a party with my friends and someone offers us a joint. It’s not like I’m addicted or anything. I could quit any time I want. My grades are good and I’ve never been arrested. Lots of teens smoke weed. I think it should be legal, and anyhow they are saying it is going to be legal everywhere soon. Besides, they use it with cancer patients.

Comments
Observations
Reflections

KF is a 18 yo model whose CRAFFT Score is 5/6 (alcohol use).
My career is taking off, yeah! I am going to Paris for a few months for a big photo shoot. The other girls are older than me so when we finish work and go to the bar to unwind, what am I supposed to order, milk? I am always camera ready the next day. I got into an argument with my boyfriend so I left his apartment in the middle of the night and cracked up my car, but luckily I didn’t get hurt. Hey, I’m young and am having fun. This is what teenagers do. My friends in college drink all the time and they are living off their parents. At least I am paying my own way. There will be plenty of time later for me to go to college if I want, but right now that’s not for me.

CRAFFT Questions C Have you ever ridden in a CAR driven by someone
(including yourself) who was “high” or had been using alcohol / drugs?”
R Do you ever use alcohol or drugs to RELAX, feel better about yourself, or fit in?
T Have you ever gotten into TROUBLE while you were using alcohol or drugs?
F Do your FAMILY or FRIENDS ever tell you that you should cut down on your drinking or drug use?
F Do you ever FORGET things you did while using alcohol or drugs?
A Do you ever use alcohol/drugs while you are by yourself, ALONE?
Knight JR. The CRAFFT questions: A brief screening test for adolescent substance abuse. Boston, MA: Copyright Children's Hospital Boston; 1999.
A total score of > 2 is a positive screen, indicating a need for additional assessment.

Comments
Observations
Reflections
CY is an 19 yo female starting to use marijuana to cope with stress
You know how stressed I’ve been because of my parents not wanting me to be with my boyfriend plus needing money for college and an apartment. It gave me a headache and I was feeling so angry. My girlfriend gave me some marijuana to try and it was like magic! My headache went away and I didn’t feel mad anymore. I was wondering if you could give me a note that states I need this for medical reasons, not a lot, just for when I get a headache and feel really stressed. I don’t want to meet with a counselor. I don’t like telling my business to strangers.

Comments
Observations
Reflections