using eeg and symptoms to guide neurofeedback … ansa 20… · using eeg and symptoms to guide...
TRANSCRIPT

Using EEG and Symptoms to
Guide Neurofeedback
Jon Hegg, MA & Moshe Perl, PhD
ANSA Annual Conference
Melbourne
1 September 2012

We will discussThe Symptom based and EEG/QEEG based
approaches
Give a brief history of each
Describe each approach
Give Case examples
Compare and contrast EEG and QEEG analysis
Present the Johnstone, Gunkelman, Lunt EEG Phenotypes
Review Outcome research
Give references for training in this area
Symptom Based Neurofeedback
Two Goals: Stability and Flexibility of the EEG
Prof Barry Sterman trained for stability – trained seizure disorders and discovered that enhancing the SMR rhythm (across the sensory motor strip) stabilised the brains of cats and humans against seizures (Sterman, 2000)
He trained C3-C4 12-15hz reward.
Little did he know that he was actually training the sleep spindle, which stabilises the brain against state changes.
Time line late 1960s, 1970s.
Symptom Based Neurofeedback
Prof Joel Lubar worked with Sterman and noticed a reduction in hyperactivity in epileptics doing neurofeedback.
He successfully applied neurofeedback to hyperactive children without epilepsy
He trained Cz 12-15hz reward.
The EEGs of hyperactives were generally not unstable, but “stuck” - inflexible. It appeared their brains' accelerators were stuck on “on”.
Lubar was training flexibility of arousal
Time line mid 1970s, 1980s.

Symptom Based Neurofeedback
Susan and Siegfried Othmer entered the field in 1989, via Margaret Ayres. She successfully treated their son, who suffered from epilepsy.
Based on Ayres work, they developed and refined the arousal model. It reflected their investigations into the treatment of a variety of disorders, all of which showed deviations from normal arousal levels
She correlated underarousal with left hemisphere issues, and trained there, rewarding 15-18hz
She correlated overarousal with right hemisphere issues, and trained there, rewarding 12-15hz
Symptom Based Neurofeedback
Underarousal Symptoms included:
Inattention
Difficulty following instructions
Lower energy
Dreaminess
Slowed depression
Worry
Frequent waking from sleep without high activation or anxiety
Tired after waking from sleep
Symptom Based Neurofeedback
Overarousal Symptoms included:
Impulsivity
Distractibility
Busy mind – always thinking
Lack of speech prosody
Anxiety/Agitation
Difficulty calming once activated
Difficulty falling asleep
Excessive ego strength
Symptom Based Neurofeedback
Her method showed spectacular clinical success
With ADHD, her success rates approached 75%
Her theories were based on clinical successes with quite severe disorders.
Her categories (underaroused, overaroused, etc) had psychological appeal, but lacked neurological rigor.
Slow wave in the right hemisphere could produce symptoms of “overarousal” in her model.
Fast wave in the left hemisphere could produce symptoms of “underarousal” in the model

Symptom Based Neurofeedback
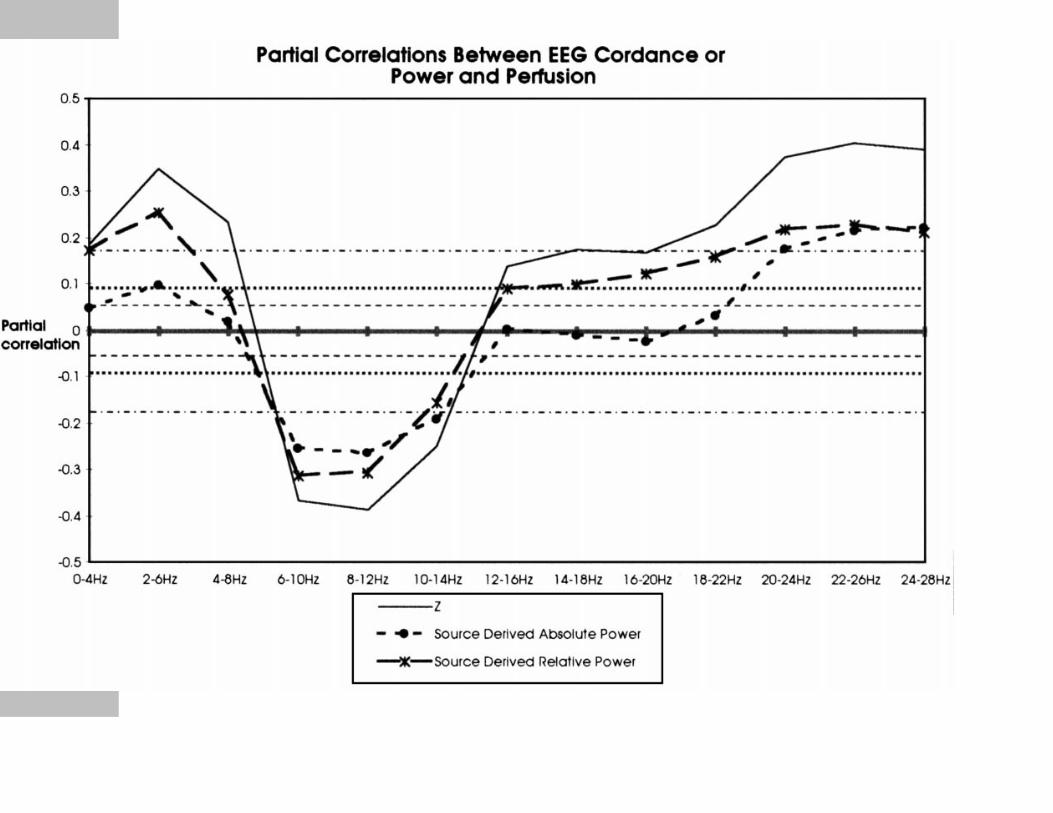
Thus, her categories did not correspond at all with EEG and arousal graphs (Leuchter et al, 1999)
These graphs clearly show theta and alpha to correlate with low sugar uptake and low brain activation.
The graphs also show SMR to have higher activation, and beta above 15hz to have high activation.
The high activation in the delta band may be related to activity of Glia.
Symptom Based Neurofeedback
Symptom Based Neurofeedback
Susan Othmer addressed more complex disturbances by training frontally, parietally and temporally.
These moves, including Cz and C3-C4, involved training unstable arousal and/or instabilities.
In these instances she moved slightly away from the arousal model, especially when she trained interhemispherically (T3-T4, F3-F4, P3-P4)
Her method, still used today, involved adjusting the reward band up or down, depending on the level of activation of the client (either in session, or by report after the session)

Symptom Based Neurofeedback
More recently, Susan Othmer has been training infra low frequencies (below 1hz), mostly interhemispheric training.
This takes us out of the rhythmic EEG training, and into the slow cortical potential field.
Criticisms of her work include a lack of research confirmation for her findings, difficulty describing her work with generally recognised neurological metrics and a failure to adequately address treatment failures or adverse reactions
Nevertheless, her successes have given the field a direction it continues to pursue.

Symptom Based Neurofeedback
Shortcomings:
Terms like overarousal and underarousal must correspond to brain over and underarousal
Focal disturbances in the EEG often occur in clinical cases, and may involve epileptiform, paroxysmal or sharp wave discharges, that need to be addressed specifically and directly.
Nutritional issues may interfere with the orderly production of the chemicals the brain needs to function properly.
Learning disabilities can occur without any disturbance in arousal and attention

Symptom Based Neurofeedback
We come to a place where the arousal model breaks down and more specific information is needed to make good clinical decisions about neurofeedback.
We need additional descriptors, relating to EEG, which itself can show
� overarousal � underarousal � unstable arousal� instability, and� disordered arousal (Dr. Ed Hamlin)

EEG: Definitions
EEG analysis involves looking at raw EEG, and noting the normal or abnormal background rhythms and transient EEG phenomena
QEEG analysis involves transforming the raw data mathematically to produce summary data. These data may include averages of power, amplitude, coherence and other measures.
Normative databases may be used to determine the degree of deviation of the results from the norm.
EEG: DefinitionsA Clinical EEG analysis is an EEG analysis
performed by a Neurologist. The minimum standards for a Clinical EEG are 20 minutes of EEG data, reviewed in at least two montages, to reduce the likelihood of incorrectly interpreting results that were produced by contaminated ear references.
Neurologists are looking for gross disturbances in the EEG (epileptiform activity), with a view to medicating the patient. From this perspective, most findings other than epilepsy, are inconsequential. However, those findings often produce severe psychiatric disturbances.

EEG Based Neurofeedback
EEG in humans was first described by Hans Berger in 1928.
By the mid 1930's publications on EEG began to appear, and continued to appear, until the early 1960's, from which time the number of publications diminished significantly.
The hope that EEG would lead to diagnostic specificity failed to materialise
The first neuroleptic medication achieved widespread use and success in controlling symptoms of schizophrenia (Largactil or Thorazine)

EEG Based Neurofeedback
By the mid 1980's, Joel Lubar (theta beta ratio), William Hudspeth, Robert Thatcher, Barry Sterman, were looking at EEG average values
The first EEG Databases were published in 1989.
These gave normative comparisons in Amplitude (voltage), Power (voltage squared), Coherence (comodulation, phase synchrony).
Over time, the databases became more sophisticated, and were able to transform the standard measurement montage (linked-ears as the reference for each electrode)

EEG Based Neurofeedback
Other montages include:
Average reference (each electrode compared to the average of all electrodes)
Average weighted reference (each electrode compared to the average of all electrodes, weighted to the electrodes closer to the electrode under consideration. Also known as Hjorth or Laplacian montage).

EEG Based Neurofeedback
These first databases were often derived from particular research interests (NxLink – brain damage), or simply did not consider certain ranges of EEG as valuable (Neuroguide 2-30hz), or did not consider certain sites to be useful (Sterman – SKIL did not have norms for the midline). Over time, these databases were found to be deficient in their numbers of subjects (SKIL no norms for children), the quality of their "normalness", and the lack of certain data when used outside of the purpose for which they were developed.

EEG Based Neurofeedback
More recent databases have improved on many of these shortcomings.
The Brain Resource Company has a huge normative database, with a wide frequency spectrum. The most significant issue is the lack of artifacting in the database, which brings into question the low frequencies (movement, eye blink) and high frequency (EMG).
The WinEEG (Mitsar) software has an excellent normative sample across the age range, and is artifacted.
EEG Based Neurofeedback
As the neurofeedback field began using EEG derived data – Quantitative EEG analysis – it moved away from EEG analysis.
Although the originators of the QEEG databases were all experts in EEG, the users of the databases were not trained in understanding EEG, and the first step of looking at raw EEG was overlooked.
This is a significant weakness in our training – the analysis (visual review) of raw EEG.

EEG Based Neurofeedback
Reviewing raw EEG, vs QEEG only - Advantages:
Some artifacts cannot be removed from QEEG analysis (movement, EMG, pulse, etc)
Alpha, or alphas, and their frequencies – differentiating slowed alpha from theta
Transients often disappear in the averaged data – spindling beta, sharp wave discharges, paroxysms, epileptiform/epileptogenic activity.
State changes within a measurement (eg, falling asleep).
The quality of the EEG – organised, disorganised, rhythmic, non-rhythmic

EEG Based Neurofeedback
Montage change allows us to see the EEG from different viewpoints. There is no correct or incorrect montage.
Linked ears montage – Very good for sites not adjacent to the ears. Sites will tend to have significant overlap (built in coherence).
Average montage – Shows temporal lobe sites more clearly. Minimises temporal lobe contamination of the record (In LE montage, contaminated reference shows up as a similar EEG pattern in all electrodes except T3 and/or T4.)

EEG Based Neurofeedback
Average weighted montage – Shows temporal lobe sites clearly, minimises ear contamination of the record. Very good at showing the separate contribution of each electrode site – localises focal abnormalities
Spurious coherences are minimised in this montage. Strong coherences here are especially meaningful.
There is a tendency for temporal, prefrontal, and occipital sites to be a little higher.
EEG Based Neurofeedback
Using only the linked ears montage runs the risk of missing temporal lobe disturbance.
The NxLink and Hudspeth databases have this problem. - They will not reflect temporal lobe issues accurately when there is a temporal lobe disturbance.

Research Based Neurofeedback
Research: In his landmark 2009 paper, Martijn Arns referenced many studies, some of which had randomised subject selection and were double blind. They give strong support to the efficacy of this methodology.
Arns M, deRidder S, Strehl U, Breteler M & Coenen A. Efficacy of Neurofeedback Treatment in ADHD: The effects on Inattention, Impulsivity and Hyperactivity: A Meta Analysis. (2009) Clin EEG & Neuroscience. 40 (3) p. 180-189.
Research Based Neurofeedback
Other recent studies include:
Perreau-Linck, E., Lessard, N., Lévesque, J., Beauregard, M.(2010).Effects of neurofeedback training on inhibitory capacities in ADHD children: A single-blind, randomized, placebo-controlled study. Journal of Neurotherapy 14(3), 229 – 242.
Surmeli, T., & Ertem, A. (2010). Post WISC-R and TOVA improvement with QEEG guided neurofeedback training in mentally retarded: A clinical case series of behavioral problems. Clinical EEG & Neuroscience, 41(1), 32-41.
Research Based Neurofeedback
Neurofeedback for the treatment of children and adolescents with ADHD: a randomized and controlled clinical trial using parental reports. Duric NS, Assmus J, Gundersen D & , Elgen IB. BMC Psychiatry 2012, 12:107
Sterman MB. Basic concepts and clinical findings in the treatment of seizure disorders with EEG operant conditioning. Clin Electroencephalogr 2000; 31:45-55
Research Based Neurofeedback
Cases: David, a 4½ year old autistic and very hyperactive boy. During intake, would not sit still, continually ran and jumped on his mother, would not allow himself to be held. Was not socially appropriate, disregarded others, was unreactive to most approaches to him.
At creche would not comply, would not interact with others, except aggressively.
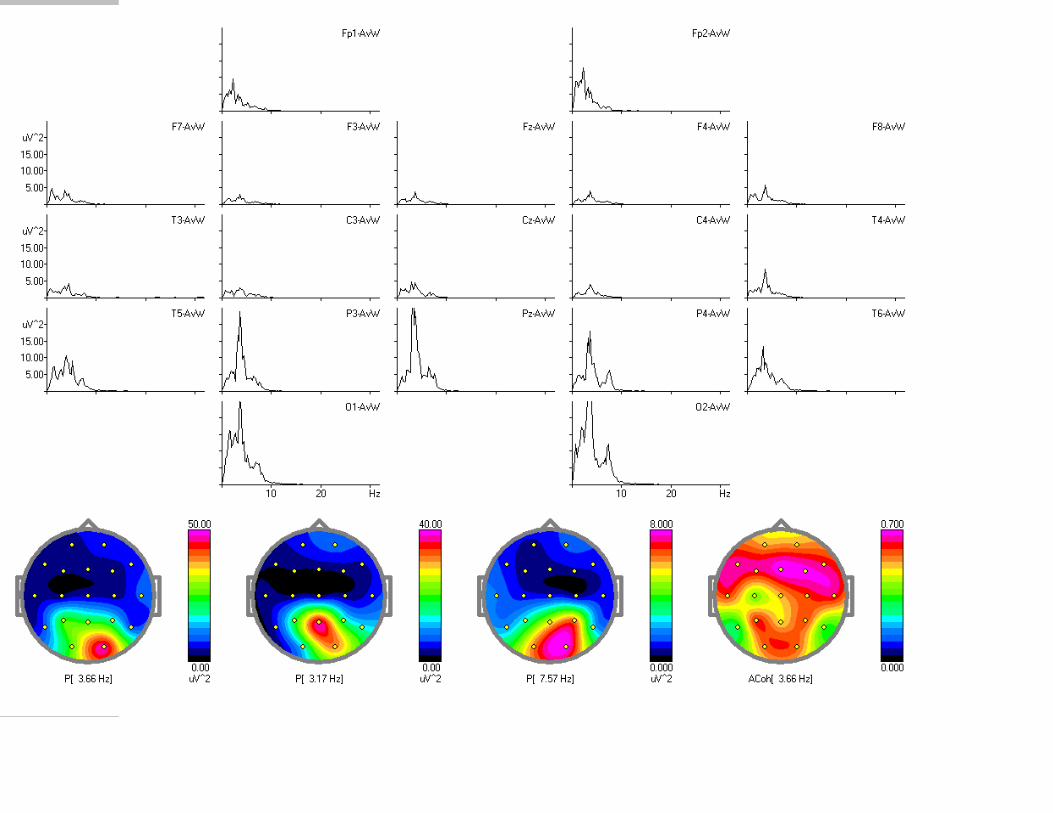
His EEG showed excessive slow wave parietally and centrally.
Research Based Neurofeedback

Research Based Neurofeedback
Neurofeedback focussed exclusively on Cz-A2, rewarding 11-14hz, later including Pz-A2 11-14hz
In order to train more efficently, the reward frequency was varied slightly, to calm for sleep and daily activity, while improving focus.
David reacted to more than six minutes training at Pz, so Cz was used extensively.
After over 100 training sessions, David was calmer, he interacted appropriately with peers, followed his mother's direction, slept better.
His behaviour at creche normalised. For weeks at a time, he showed little autistic behaviour.

Research Based Neurofeedback
Neurofeedback

David at Intake - NeuroGuide
Neurofeedback

Research Based Neurofeedback
Neurofeedback
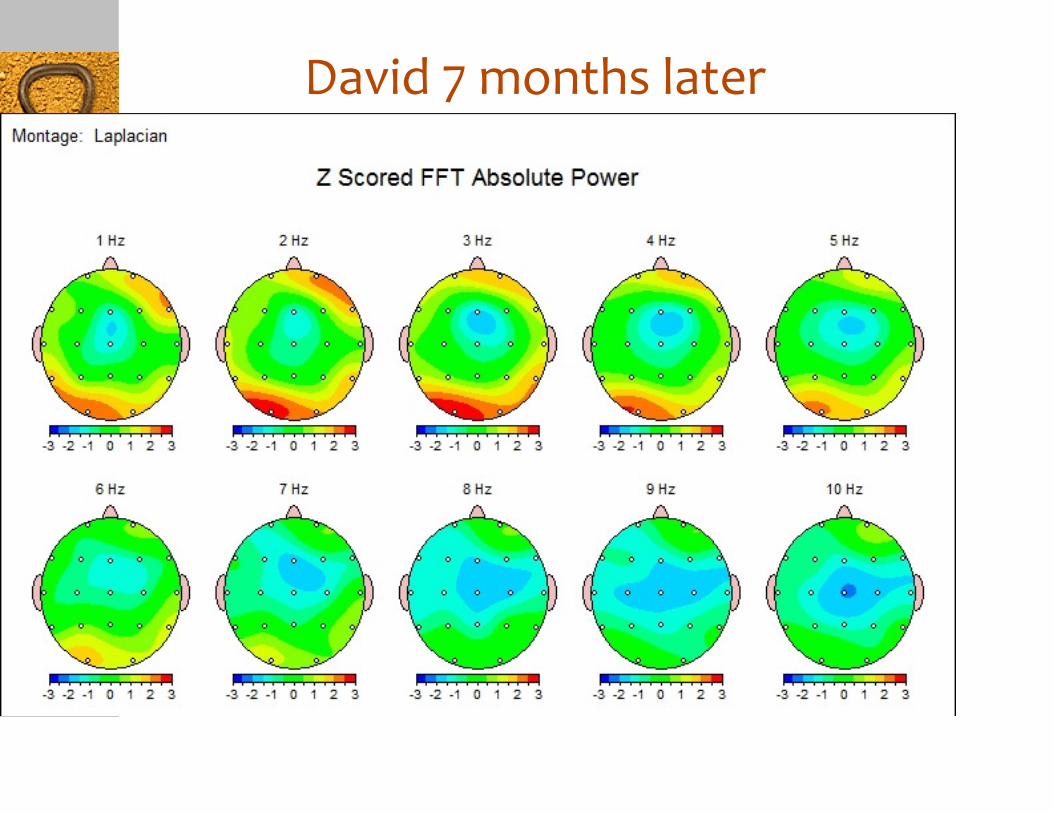
David 7 months later
Neurofeedback

Research Based Neurofeedback
Neurofeedback

Equipment and TrainingAll major manufacturers of neurofeedback
equipment offer training. These include:
EEG Education & Research
Thought Technology
Brain Master
Bio Explorer
Stens biofeedback
These can be found on the web

Equipment & TrainingConsiderations
Quality of the training – will this course teach you what you need
Format of the training (face-to-face; Skype; webinar, DVD)
Quality of the equipment, ease of use
Availability of technical support (telephone, email, Skype)
Availability of professional and peer support
Ongoing professional education
Cost of the equipment and training

Symptom Basedand
EEG/QEEG Based Neurofeedback
Thank you for your attention.
Do you have any questions?