use of intense pulsed light (ipl) in indian skin...
TRANSCRIPT
Use of Intense Pulsed Light (IPL) in Indian Skin TypesPresented at the 27th American Society for Laser Medicine and Surgery(ASLMS) Annual Conference In Grapevine, Texas April 11-15th 2007
Dr Maya Vedamurthy M.B.B.S; M.D; D.D, Consultant Dermatologist, Chennai, IndiaAB 76 1st Street Anna Nagar, Chennai, 600040, INDIA E-mail: [email protected]
Godfrey TownLaser Protection Adviser, Haywards Heath, UK.
Address for correspondence: [email protected] or [email protected]
CyDen Indian Skin handout 10/4/07 16:22 Page 2

IntroductionUnwanted hair, benign pigmented lesions and acne are major cosmetic problems in Indian skin types. It is usually assumed that many lasers and IPL devices are not suitable for dark skinned patients. These assumptions fail to recognisethat the contrast between skin and hair (or lesion) colour remains largely constant or even increases with darker skin.
Numerous previous studies have reported the effectiveness of both Q-switched and microsecond pulsed lasers in theremoval of epidermal benign pigmented lesions and acne in light skin types (Fitzpatrick I – III) [1-7]. Other studies haveshown intense pulsed light (IPL) to be successful in the treatment of unwanted body and facial hair in both Caucasian andEast Asian skin types [8-14]. Early studies by Sherwood et al [15] and Anderson et al [16] exposed pigskin to differentwavelengths to establish ideal wavelength for the treatment of pigmented lesions. These studies variously found 504 nmand 532 nm to achieve ideal pigment clearance thus demonstrating a need for a compromise between a high absorption inmelanin and optimum penetration depth for specific lesion clearance. Other studies have shown efficacy in the use of Q-switched lasers in Caucasian and Asian skin types including lesions with a significant dermal component [17-20].Subsequently, other investigators have shown efficacy in the removal of pigmented lesions using IPL wavelengthsconcentrated in this range [21-23]. However, relatively few studies have focused on treating darker skin types, particularlythose found typically on the tropical and sub-tropical Indian Sub-Continent. In an unpublished study in 1999 of 170 patientsof skin types III-V, R. Shah MD (Baroda, India) reported a total of 360 ruby laser treatments with a normal incidence oftreatment-related skin reactions with few real side effects, particularly when efficient air-cooling of the skin was used.
This study describes the early results of the incidence of side effects and treatment-related problems in dark Indian skintypes (Fitzpatrick 4 & 5) using a novel constant spectrum IPL source (iPulse, CyDen Ltd., Swansea, UK) and its efficacy inhair removal and the treatment of benign pigmented lesions and acne.
2
CyDen Indian Skin handout 10/4/07 16:22 Page 3
MethodsThe cases reviewed in this study were selected amongst ordinary patients attending the private dermatology clinic of Dr Maya Vedmurthy in Chennai. If subjects presented with any of the conditions suitable for IPL, they were offered thetreatment. Whilst the manufacturer’s recommended treatment parameters and application techniques for dark skin typeswere used, fixed intervals between treatments were not maintained easily because of poor patient compliance arising out of lack of familiarity with routine attendance for cosmetic medical treatment.
No Ethics Committee approval was required as the study was conducted in a private dermatology clinic in Chennai. Allsubjects had the purpose of the trial explained to them, and each subject gave written informed consent both to participatein the trial and for the subsequent use of their clinical photography.
Treatment sites & numbersStandardized patient data collection forms were used to record gender, age, ethenicity, skin type, treatment parameters,side effects, pain, treatment outcomes and other observations.
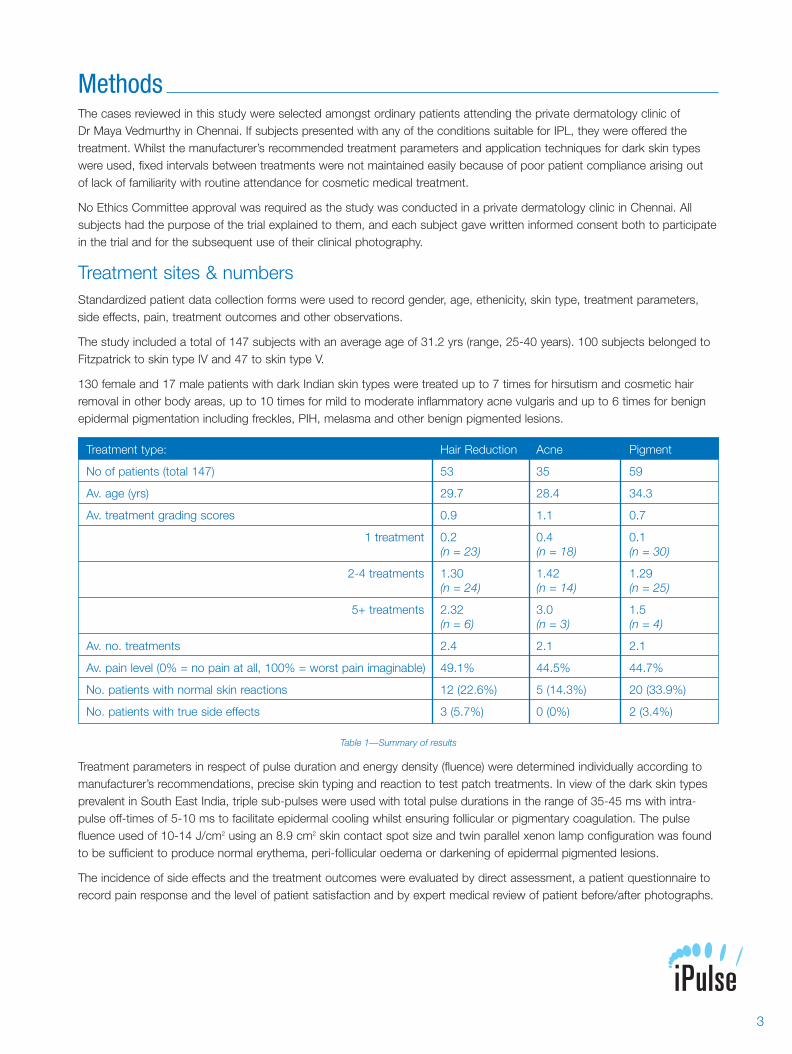
The study included a total of 147 subjects with an average age of 31.2 yrs (range, 25-40 years). 100 subjects belonged toFitzpatrick to skin type IV and 47 to skin type V.
130 female and 17 male patients with dark Indian skin types were treated up to 7 times for hirsutism and cosmetic hairremoval in other body areas, up to 10 times for mild to moderate inflammatory acne vulgaris and up to 6 times for benignepidermal pigmentation including freckles, PIH, melasma and other benign pigmented lesions.
Table 1—Summary of results
Treatment parameters in respect of pulse duration and energy density (fluence) were determined individually according tomanufacturer’s recommendations, precise skin typing and reaction to test patch treatments. In view of the dark skin typesprevalent in South East India, triple sub-pulses were used with total pulse durations in the range of 35-45 ms with intra-pulse off-times of 5-10 ms to facilitate epidermal cooling whilst ensuring follicular or pigmentary coagulation. The pulsefluence used of 10-14 J/cm2 using an 8.9 cm2 skin contact spot size and twin parallel xenon lamp configuration was foundto be sufficient to produce normal erythema, peri-follicular oedema or darkening of epidermal pigmented lesions.
The incidence of side effects and the treatment outcomes were evaluated by direct assessment, a patient questionnaire torecord pain response and the level of patient satisfaction and by expert medical review of patient before/after photographs.
Treatment type: Hair Reduction Acne Pigment
No of patients (total 147) 53 35 59
Av. age (yrs) 29.7 28.4 34.3
Av. treatment grading scores 0.9 1.1 0.7
1 treatment 0.2 0.4 0.1(n = 23) (n = 18) (n = 30)
2-4 treatments 1.30 1.42 1.29(n = 24) (n = 14) (n = 25)
5+ treatments 2.32 3.0 1.5(n = 6) (n = 3) (n = 4)
Av. no. treatments 2.4 2.1 2.1
Av. pain level (0% = no pain at all, 100% = worst pain imaginable) 49.1% 44.5% 44.7%
No. patients with normal skin reactions 12 (22.6%) 5 (14.3%) 20 (33.9%)
No. patients with true side effects 3 (5.7%) 0 (0%) 2 (3.4%)
3
CyDen Indian Skin handout 10/4/07 16:22 Page 4
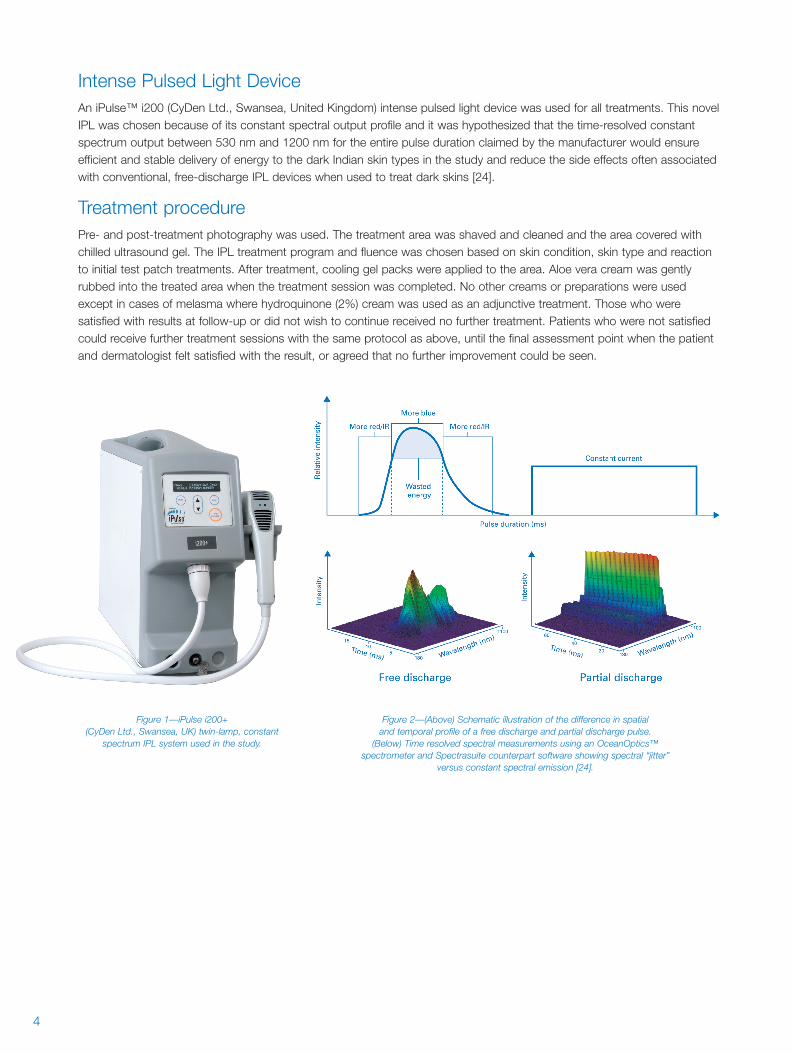
Intense Pulsed Light DeviceAn iPulse™ i200 (CyDen Ltd., Swansea, United Kingdom) intense pulsed light device was used for all treatments. This novelIPL was chosen because of its constant spectral output profile and it was hypothesized that the time-resolved constantspectrum output between 530 nm and 1200 nm for the entire pulse duration claimed by the manufacturer would ensureefficient and stable delivery of energy to the dark Indian skin types in the study and reduce the side effects often associatedwith conventional, free-discharge IPL devices when used to treat dark skins [24].
Treatment procedurePre- and post-treatment photography was used. The treatment area was shaved and cleaned and the area covered withchilled ultrasound gel. The IPL treatment program and fluence was chosen based on skin condition, skin type and reactionto initial test patch treatments. After treatment, cooling gel packs were applied to the area. Aloe vera cream was gentlyrubbed into the treated area when the treatment session was completed. No other creams or preparations were usedexcept in cases of melasma where hydroquinone (2%) cream was used as an adjunctive treatment. Those who weresatisfied with results at follow-up or did not wish to continue received no further treatment. Patients who were not satisfiedcould receive further treatment sessions with the same protocol as above, until the final assessment point when the patientand dermatologist felt satisfied with the result, or agreed that no further improvement could be seen.
Figure 1—iPulse i200+ (CyDen Ltd., Swansea, UK) twin-lamp, constant
spectrum IPL system used in the study.
Figure 2—(Above) Schematic illustration of the difference in spatial and temporal profile of a free discharge and partial discharge pulse.
(Below) Time resolved spectral measurements using an OceanOptics™ spectrometer and Spectrasuite counterpart software showing spectral “jitter”
versus constant spectral emission [24].
4
CyDen Indian Skin handout 10/4/07 16:22 Page 5

Results & DiscussionThe groups comprised hair removal: n=53; acne: n=35 and pigmentation: n=59. The overall average fluence used was11.6, 10.5 and 12.3 J/cm2 respectively.
The study was conducted in Chennai city in Southern India where the normal range of skin types of patients seeking treatmentis Fitzpatrick IV-V and the sunny climate is constantly hot and humid with an average ambient temperature even in air-conditioned rooms above 25ºC. These climatic conditions increase treatment-related problems and increase the incidence ofpost-treatment side effects aggravated by sun exposure to skin areas exposed to intense pulsed light or laser wavelengths.
It is reasonable to assume that certain pigmented lesions may be diagnosed accurately by an expert dermatologist asbenign without the benefit of histological validation (impossible where the treatment with light therapy is entirely non-invasiveand no tissue is removed during the procedure).
The generally poor response after only one or two treatments confirms the importance of completing a course of IPLtreatments at regular intervals. Patients who failed to attend sufficient treatment sessions, showed reduced effectiveness asassessed by the expert clinician. Where more treatment sessions were given, in most cases better results were observed.
In common with other anecdotally reported experience with laser and IPL devices in India, a conservative approach isnormally taken to choosing treatment parameters and it is generally found that numbers of treatments needed to achievesatisfactory results are greater than in countries with lighter skin types and even where treatment energy levels are similar,more treatments appear to be necessary.
EfficacyTreatment outcomes were only assessed and recorded atthe end of a treatment or course of treatments when thepatient and/or dermatologist were satisfied that no furtherimprovement could be achieved, where the patient did notwish to continue or where the patient simply failed to appearfor further scheduled treatments. The standard descriptionsof efficacy used in this study by the expert clinical assessorwere graded and assessed as follows:
Hair Reduction:
Grade 0 = No reduction (<10%),Grade 1 = Some Reduction (>25%), Grade 2 = Moderate Reduction (>50%), Grade 3 = Good Reduction (>70%).
As expected, where multiple treatments were given thegreatest degree of hair reduction was achieved. In general,there was little reduction in regrowth of hair follicles after asingle treatment, a moderate reduction only after 3-4treatments and in two cases of thick, facial hair, a goodreduction after 7 treatments. Table 2 indicates better results infewer treatments for cosmetic hair removal versus hirsutism.Intervals between treatments needed to be 3-4 weeks and thetrial subjects did not always follow this.
There were fewer cases of cosmetic hair removal on bodyareas than might be seen in comparable studies in lighter skintypes. This is probably explained by cultural preferences andtraditional Indian garment design.
Figure 3—Hirsutism: Female, age 20 yrs, skin type V, 50% reduction withregrowth of finer lighter hair. 6 treatments at irregular intervals over 10 months
using a fluence of 11-13 J/cm2, triple sub-pulses: 14 ms on, 7 ms off.
0
1
1 2 3 4 5 6 7
2
3
No. of treatments
Significantreduction
Hisuitism
Cosmetic
Moderatereduction
Somereduction
No reduction
Sat
isfa
ctio
n
Figure 4—Hair Removal: Graph showing patient satisfaction, with progressively better results with increasing numbers of treatments
in both hirsutism and purely cosmetic hair removal cases
5
CyDen Indian Skin handout 10/4/07 16:22 Page 6
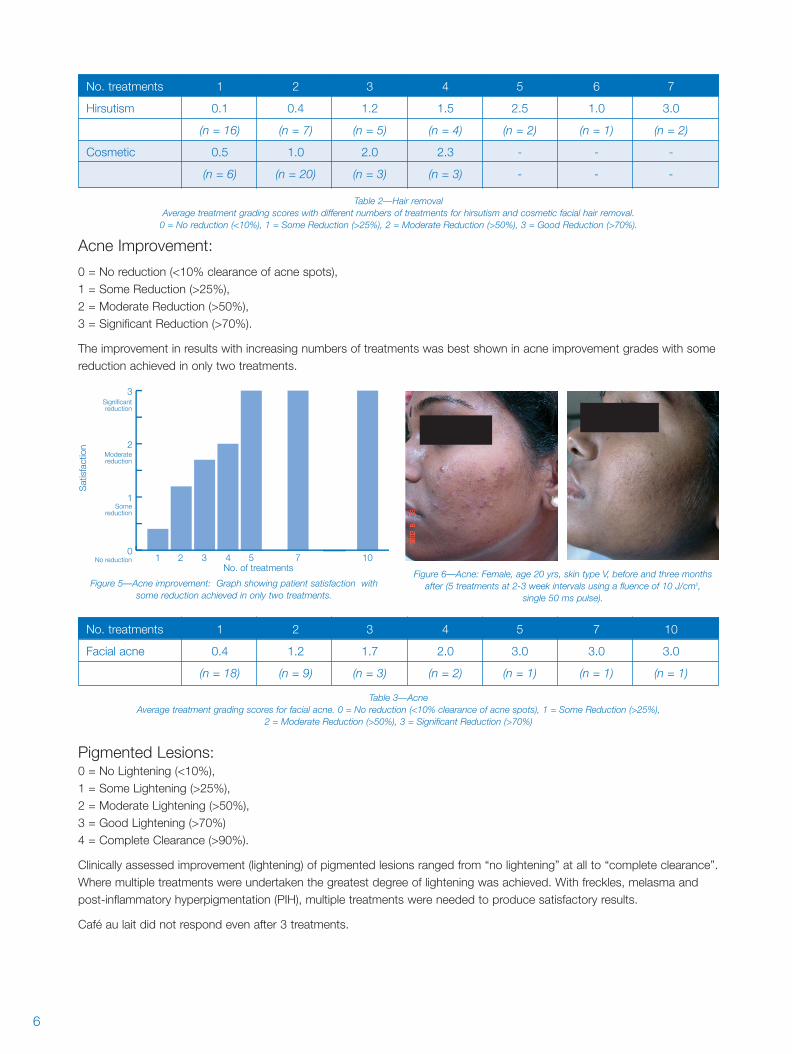
Acne Improvement:
0 = No reduction (<10% clearance of acne spots),1 = Some Reduction (>25%), 2 = Moderate Reduction (>50%), 3 = Significant Reduction (>70%).
The improvement in results with increasing numbers of treatments was best shown in acne improvement grades with somereduction achieved in only two treatments.
Pigmented Lesions: 0 = No Lightening (<10%),1 = Some Lightening (>25%), 2 = Moderate Lightening (>50%), 3 = Good Lightening (>70%)4 = Complete Clearance (>90%).
Clinically assessed improvement (lightening) of pigmented lesions ranged from “no lightening” at all to “complete clearance”.Where multiple treatments were undertaken the greatest degree of lightening was achieved. With freckles, melasma andpost-inflammatory hyperpigmentation (PIH), multiple treatments were needed to produce satisfactory results.
Café au lait did not respond even after 3 treatments.
No. treatments 1 2 3 4 5 7 10
Facial acne 0.4 1.2 1.7 2.0 3.0 3.0 3.0
(n = 18) (n = 9) (n = 3) (n = 2) (n = 1) (n = 1) (n = 1)
No. treatments 1 2 3 4 5 6 7
Hirsutism 0.1 0.4 1.2 1.5 2.5 1.0 3.0
(n = 16) (n = 7) (n = 5) (n = 4) (n = 2) (n = 1) (n = 2)
Cosmetic 0.5 1.0 2.0 2.3 - - -
(n = 6) (n = 20) (n = 3) (n = 3) - - -
0
1
1 2 3 4 5 7 10
2
3
No. of treatments
Significantreduction
Moderatereduction
Somereduction
No reduction
Sat
isfa
ctio
n
Figure 6—Acne: Female, age 20 yrs, skin type V, before and three monthsafter (5 treatments at 2-3 week intervals using a fluence of 10 J/cm2,
single 50 ms pulse).
Figure 5—Acne improvement: Graph showing patient satisfaction withsome reduction achieved in only two treatments.
Table 2—Hair removalAverage treatment grading scores with different numbers of treatments for hirsutism and cosmetic facial hair removal.
0 = No reduction (<10%), 1 = Some Reduction (>25%), 2 = Moderate Reduction (>50%), 3 = Good Reduction (>70%).
Table 3—AcneAverage treatment grading scores for facial acne. 0 = No reduction (<10% clearance of acne spots), 1 = Some Reduction (>25%),
2 = Moderate Reduction (>50%), 3 = Significant Reduction (>70%)
6
CyDen Indian Skin handout 10/4/07 16:22 Page 7
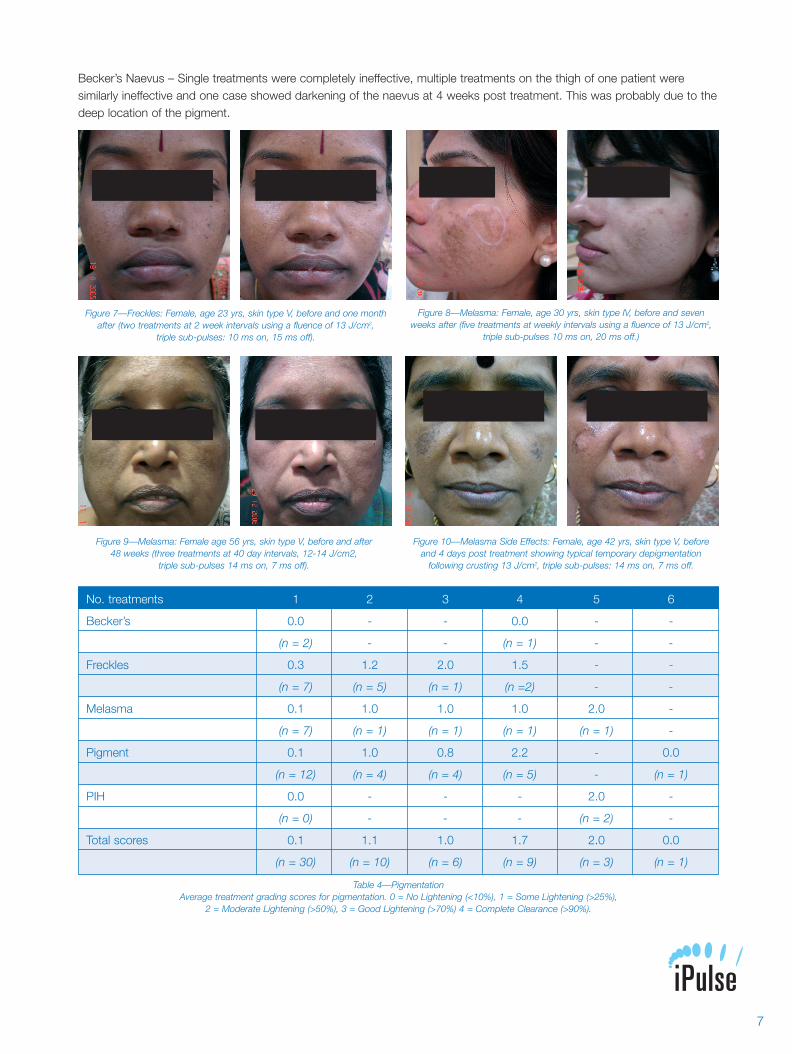
Becker’s Naevus – Single treatments were completely ineffective, multiple treatments on the thigh of one patient weresimilarly ineffective and one case showed darkening of the naevus at 4 weeks post treatment. This was probably due to thedeep location of the pigment.
No. treatments 1 2 3 4 5 6
Becker’s 0.0 - - 0.0 - -
(n = 2) - - (n = 1) - -
Freckles 0.3 1.2 2.0 1.5 - -
(n = 7) (n = 5) (n = 1) (n =2) - -
Melasma 0.1 1.0 1.0 1.0 2.0 -
(n = 7) (n = 1) (n = 1) (n = 1) (n = 1) -
Pigment 0.1 1.0 0.8 2.2 - 0.0
(n = 12) (n = 4) (n = 4) (n = 5) - (n = 1)
PIH 0.0 - - - 2.0 -
(n = 0) - - - (n = 2) -
Total scores 0.1 1.1 1.0 1.7 2.0 0.0
(n = 30) (n = 10) (n = 6) (n = 9) (n = 3) (n = 1)
Figure 8—Melasma: Female, age 30 yrs, skin type IV, before and sevenweeks after (five treatments at weekly intervals using a fluence of 13 J/cm2,
triple sub-pulses 10 ms on, 20 ms off.)
Figure 7—Freckles: Female, age 23 yrs, skin type V, before and one monthafter (two treatments at 2 week intervals using a fluence of 13 J/cm2,
triple sub-pulses: 10 ms on, 15 ms off).
Table 4—PigmentationAverage treatment grading scores for pigmentation. 0 = No Lightening (<10%), 1 = Some Lightening (>25%),
2 = Moderate Lightening (>50%), 3 = Good Lightening (>70%) 4 = Complete Clearance (>90%).
Figure 9—Melasma: Female age 56 yrs, skin type V, before and after 48 weeks (three treatments at 40 day intervals, 12-14 J/cm2,
triple sub-pulses 14 ms on, 7 ms off).
Figure 10—Melasma Side Effects: Female, age 42 yrs, skin type V, beforeand 4 days post treatment showing typical temporary depigmentation
following crusting 13 J/cm2, triple sub-pulses: 14 ms on, 7 ms off.
7
CyDen Indian Skin handout 10/4/07 16:22 Page 8
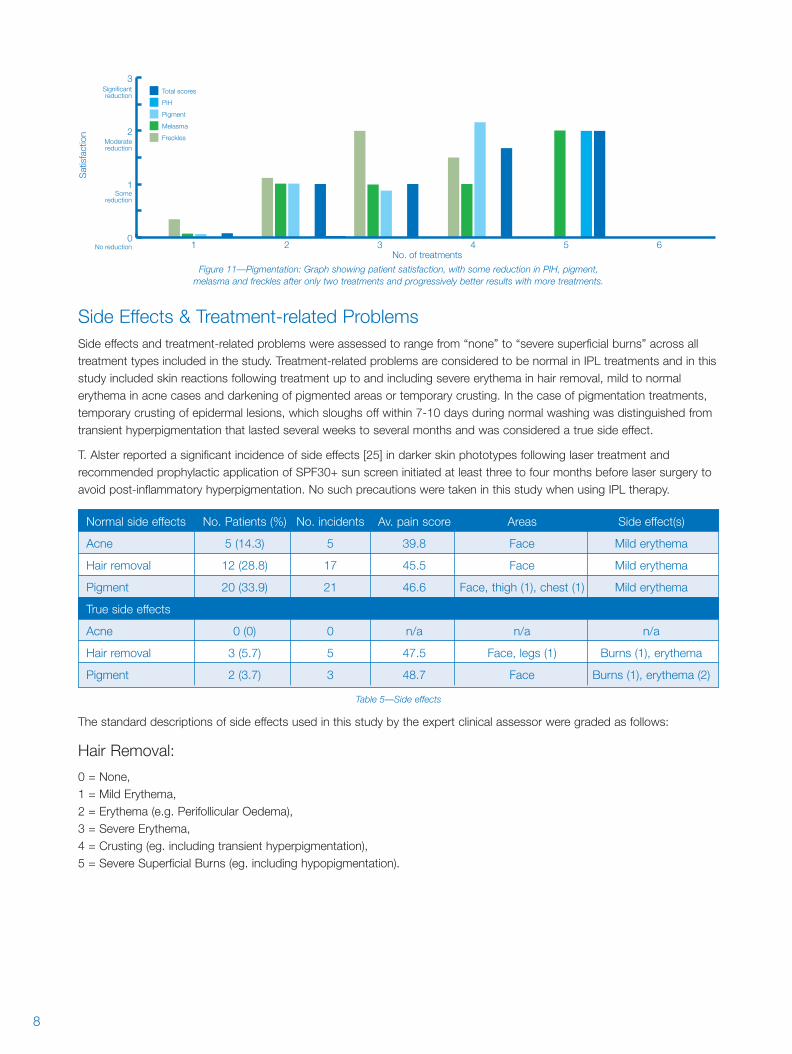
Side Effects & Treatment-related ProblemsSide effects and treatment-related problems were assessed to range from “none” to “severe superficial burns” across alltreatment types included in the study. Treatment-related problems are considered to be normal in IPL treatments and in thisstudy included skin reactions following treatment up to and including severe erythema in hair removal, mild to normalerythema in acne cases and darkening of pigmented areas or temporary crusting. In the case of pigmentation treatments,temporary crusting of epidermal lesions, which sloughs off within 7-10 days during normal washing was distinguished fromtransient hyperpigmentation that lasted several weeks to several months and was considered a true side effect.
T. Alster reported a significant incidence of side effects [25] in darker skin phototypes following laser treatment andrecommended prophylactic application of SPF30+ sun screen initiated at least three to four months before laser surgery toavoid post-inflammatory hyperpigmentation. No such precautions were taken in this study when using IPL therapy.
The standard descriptions of side effects used in this study by the expert clinical assessor were graded as follows:
Hair Removal:
0 = None, 1 = Mild Erythema, 2 = Erythema (e.g. Perifollicular Oedema), 3 = Severe Erythema, 4 = Crusting (eg. including transient hyperpigmentation), 5 = Severe Superficial Burns (eg. including hypopigmentation).
Normal side effects No. Patients (%) No. incidents Av. pain score Areas Side effect(s)
Acne 5 (14.3) 5 39.8 Face Mild erythema
Hair removal 12 (28.8) 17 45.5 Face Mild erythema
Pigment 20 (33.9) 21 46.6 Face, thigh (1), chest (1) Mild erythema
True side effects
Acne 0 (0) 0 n/a n/a n/a
Hair removal 3 (5.7) 5 47.5 Face, legs (1) Burns (1), erythema
Pigment 2 (3.7) 3 48.7 Face Burns (1), erythema (2)
Table 5—Side effects
0
1
1 2 3 4 5 6
2
3
No. of treatments
Significantreduction
PIH
Pigment
Melasma
Freckles
Total scores
Moderatereduction
Somereduction
No reduction
Sat
isfa
ctio
n
Figure 11—Pigmentation: Graph showing patient satisfaction, with some reduction in PIH, pigment, melasma and freckles after only two treatments and progressively better results with more treatments.
8
CyDen Indian Skin handout 10/4/07 16:22 Page 9

Acne:
0 = None, 1 = Mild to Normal Erythema, 2 = Hyperpigmentation, 3 = Severe Superficial Burns.
All acne patients showed a reduction in the number of inflamed lesions with no side effects. The reduction of acne spotsobserved was similar to results reported in the literature for lighter skin types treated with IPL.
Pigment:
0 = None, 1 = Mild to Normal Erythema / darkening of pigmented lesion / crusting, 2 = Hyperpigmentation,3 = Severe Superficial Burns, 4 = Hypopigmentation.
Normal erythema was only seen in about one third of patients suggesting an over-cautious approach. Side effects wereseen with increased fluence. Two cases of post hair removal treatment burns were reported. The consequentialhyperpigmentation resolved in both of these cases within 3 months (See figures 7-9).
PainPain experienced by the patients during all of the treatments was graded using a blank visual analogue scale (0 = no painat all and 10 = worst pain imaginable). Average pain scores for hair removal, acne and pigmentation were 4.5, 4.7 and 4.2respectively. Most subjects found the level of discomfort easily tolerated and no subjects felt the pain was unbearable as noscores were recorded above 7.0 (See figure 10).
9
CyDen Indian Skin handout 10/4/07 16:22 Page 10
ConclusionsWhen a sufficient number of treatments were performed, the iPulse constant spectrum IPL was found to be effective in thispreliminary study in the treatment of benign pigmented lesions, acne and in the long-term delay of hair regrowth in hirsutism.
Normal treatment related problems including patient assessed pain response and side effects using the iPulse IPL with itsconstant spectral output, large 8.9 cm2 spot size and relatively low fluence characteristics, were found to be comparable in dark Indian skin to those reported in the literature in lighter skin types with conventional IPL devices. Early indications of efficacy in the treatment of hirsutism, pigmentation and acne were broadly similar to lasers and other IPL systems inlighter skin types.
Both the follow-up period and the number of lesions included in the present study may not be sufficient to fully evaluate the potentials of this treatment modality as well as the true incidence of recurrence of the original condition. Therefore, theresults obtained should be confirmed in larger studies.
10
CyDen Indian Skin handout 10/4/07 16:22 Page 11
References1. Alster TS. Complete elimination of large café-au-lait birthmarks by the
510-nm pulsed dye laser. Plast Reconstr Surg 1995; 95: 1660–4.
2. Trelles MA, Verkruysse W, Pickering JW, et al. Monoline argon laser
(512 nm) treatment of benign pigmented lesions with long pulse length.
J Photochem Photobiol 1992; 16:357–65.
3. Alster TS, Williams CM. Cafe-au-lait macule in type V skin: successful
treatment with a 510 nm pulsed dye laser. J Am Acad Dermatol 1995;
33: 1042–3.
4. Somyos K, Boonchu K, Somsak K, et al. Copper vapour laser treatment
of cafe-au-lait macules. Br J Dermatol 1996; 135:964–8.
5. Fitzpatrick RE, Goldman MP, Ruiz-Esparza J. Laser treatment of benign
pigmented epidermal lesions using a 300 nsecond pulse and 510 nm
wavelength. J Dermatol Surg Oncol 1993; 19:341–7.
6. Chu A, Cunliffe WJ. Pulsed-dye laser treatment for inflammatory acne
vulgaris: randomised controlled trial. Lancet. 2003; 362:1347-1352.
7. Butterwick KJ, Butterwick LS, Han A. Laser and light therapies for acne
rosacea. J Drugs Dermatol. 2006; 5(1):35-9.
8. Gold MH, Bell MW, Foster TD, Street S. One-year follow-up using an
intense pulsed light source for long-term hair removal. J Cutan Laser
Ther. 1999 1(3):167-71.
9. Omi T, Clement M. The use of a constant spectrum, uniform temporal
profile intense pulsed light long-term hair removal in Asian skin. J
Cosmetic Laser Ther. 2006; 8:138-145.
10. Bedewi AF. Hair removal with intense pulsed light. Lasers Med Sci.
2004; 19(1):48-51.
11. Bjerring P, Cramers M, Egekvist H, Christiansen K, Troilius A. Hair
reduction using a new intense pulsed light irradiator and a normal mode
ruby laser. J Cosmetic Laser Ther. 2006. 2(2):63-71.
12. Huang YL, Liao YL, Lee SH, Hong HS. Intense pulsed light for the
treatment of facial freckles in Asian skin. Dermatol Surg. 2002;
28(11):1007-12.
13. Negishi K, Kushikata N, Tezuka Y, Takeuchi K, Miyamoto E, Wakamatsu S.
Study of the incidence and nature of "very subtle epidermal melasma" in
relation to intense pulsed light treatment. Dermatol Surg. 2004; 30(6):881-6.
14. Wang CC, Hui CY, Sue YM, Wong WR, Hong HS. Intense pulsed light
for the treatment of refractory melasma in Asian persons. Dermatol Surg.
2004; 30(9):1196-200.
15. Sherwood KA, Murray S, Kurban, AK et al. Effect of wavelength
on cutaneous pigment using pulsed irradiation. J Invest Dermatol
1989; 92:717-20.
References16. Anderson RR, Margolis RJ, Watanabe S, et al. Selective
photothermolysis of cutaneous pigmentation by Q-switched Nd:YAG
laser pulses at 1064 nm, 532 and 355 nm. J Invest Dermatol
1989; 93:28-32.
17. Kono T, Manstein D, Chan HH, Nozaki M, Anderson RR. Q-Switched
Ruby Versus Long-Pulsed Dye Laser Delivered With Compression for
Treatment of Facial Lentigines in Asians. Lasers Surg Med 2006; 38:94-
97.
18. Grevlink JM, van Leeuwen RI, Anderson RR, et al. Clinical and
histological responses of congenital melanocytic nevi after a single
treatment with Q-switched lasers. Arch Dermatol 1997; 133:349-53.
19. Goldberg DJ. Laser treatment of pigmented lesions. Dermatol Clin
1997; 15:397-407.
20. Kopera D, Hohenleutner U, Landthaler M. Quality-switched ruby laser
treatment of solar lentigenes and Becker’s nevus: a histopathological
and immunohistochemical study. Dermatology 1997; 194:338-43.
21. Gold MH, Foster TD, Bell MW. Nevus spillus successfully treated with
an intense pulsed light source. Dermatol Surg. 1999; 25:254-5.
22. Adatto MA. Photorejuvenation of the forearms by treating
hyperpigmented lesions with intense pulsed light source: a case report.
J Cosmetic Laser Ther. 2003. 5(2):117-9.
23. Kligman DE, Zhen Y. Intense pulsed light treatment of photoaged facial
skin. Dermatol Surg. 2004; 30(8):1085-90.
24. Clement M, Daniel G, Trelles M. Optimising the design of a broad-band
light source for the treatment of skin. J Cosmetic Laser Ther. 2005;
7:177-189.
25. Alster TS. Laser Treatment of Darker Skin Phototypes: Recent Progress.
Cosmetic dermatol. 1999; Dec:13-16.
11
CyDen Indian Skin handout 10/4/07 16:22 Page 12

CyDen Indian Skin handout 10/4/07 16:22 Page 1