use of a confocal laser scanning ophthalmoscope to detect glaucomatous cupping of the optic disc
TRANSCRIPT
Austrafian and New Zeafand Jourwal of Ophtbalniology (1997) 25, 217-220
Original article
Use of a confocal laser scanning ophthalmoscope to detect glaucomatous cupping of the optic disc Viviene Cucevic, BSc,' Anne MV Brooks, MD, PhD, FRACO, FRACP,2 Nicole T Strang, DipAppSci(Orthoptics), DOBA,2 Anthony G Klein, FAA, BEE, PhDl and Keith A Nugent, PhDl 'School of Physics, The University of Melbourne, Parkville and IThe Royal Victorian Eye and Ear Hospital, East Melbourne, Victoria, Australia
ABSTRACT Purpose: The aim of the present study was t o test the
hypothesis that the three-dimensional (3-D) topography of the optic disc contains sufficient information to diagnose glaucoma with a high degree of reliability.
Methods: The Zeiss 'Confocal Laser Scanning Ophthalmoscope' (CLSO) was used to obtain digitized samples of 3-D images of optic nerve heads from the fol- lowing three groups of patients: (i) 40 normals with normal optic discs, normal Humphrey 24-2 full threshold visual fields and an intraocular pressure (IOP) I 2 I mmHg; (ii) 20 established glaucoma patients with cupping, glaucomatous field loss and an IOP > 21 mmHg; and (iii) 20 early glau- coma patients with early cupping, field loss with a mean defect less than - I0 dB and IOP > 2 I mmHg.The cupping in these patients was paramaterized by spherical harmonics and was classified by multivariate statistical analysis.
Results: Of 40 glaucoma patients, 39 were correctly classi- fied. Of 40 normal patients one was classified as glaucoma.
Conclusions: This study demonstrates that the CLSO, with the use of spherical harmonics, can differentiate glaucoma- tous from normal optic discs in this selected group of patients without the need for a skilled observetThis con- stitutes a promising technique to be tested on a large, un- selected body of patients as a screening tool.
Key words: confocal laser scanning ophthalmoscope, early detection of glaucoma, optic disc cupping, spherical har- monics
In mass screening of populations for glaucoma, the identifi- cation and measurement of the geometric features that char- acterize the shape of the optic disc and that enable
differentiation of glaucomatous from normal discs, such as the size of the cup, volume of the cup and cup:disc ratio, has hitherto required skilled operator intervention.'-6
In the study presented here, three-dimensional (3-D) measurement of the optic nerve head was performed auto- matically by the Zeiss 'Confocal Laser Scanning Ophthalmoscope' (CLSO; Oberkochen, Germany) and the shape of the optic nerve head was expressed in mathemati- cal terms. This was done by obtaining sets of coefficients for primary shape functions, known as spherical harmonics, fitted to the array of numbers with which the CLSO expresses the shape of the optic disc. This has enabled us to separate glaucomatous from non-glaucomatous cupping in a selected group of patients without subjective operator inter- vention to interpret the results.
METHODS We obtained 3-D images of optic nerve heads using the Zeiss CLSO with an associated Compaq computer (Compaq Desk Pro 386s; Houston, TX, USA), from the fol- lowing three groups of patients: ( i ) a normal group of 40 patients with normal optic discs, normal full threshold 24-2 Humphrey computerized visual fields and an intraocular pressure (IOP) I 2 t mmHg, (ii) a group of 20 patients with established glaucoma, glaucomatous cupping of the optic disc, typical glaucomatous visual field loss on full threshold Humphrey 24-2 fields with a mean deviation (MD) of greater than -10dB and an IOP > 21 mmHg; and (ii i) a group of 20 patients with early glaucoma, developing glau- comatous cupping of the optic disc, a visual field defect sug- gestive of glaucoma, with a MD on Humphrey 24-2 full threshold visual fields of less than -10 dB and 1OP > 21 mmHg.
Correspondmce Dr AMV Brooks, 394 Albert Street, East Melbourne, Victoria 3002, Australia. Email: <[email protected]>
218 Cucevic et al
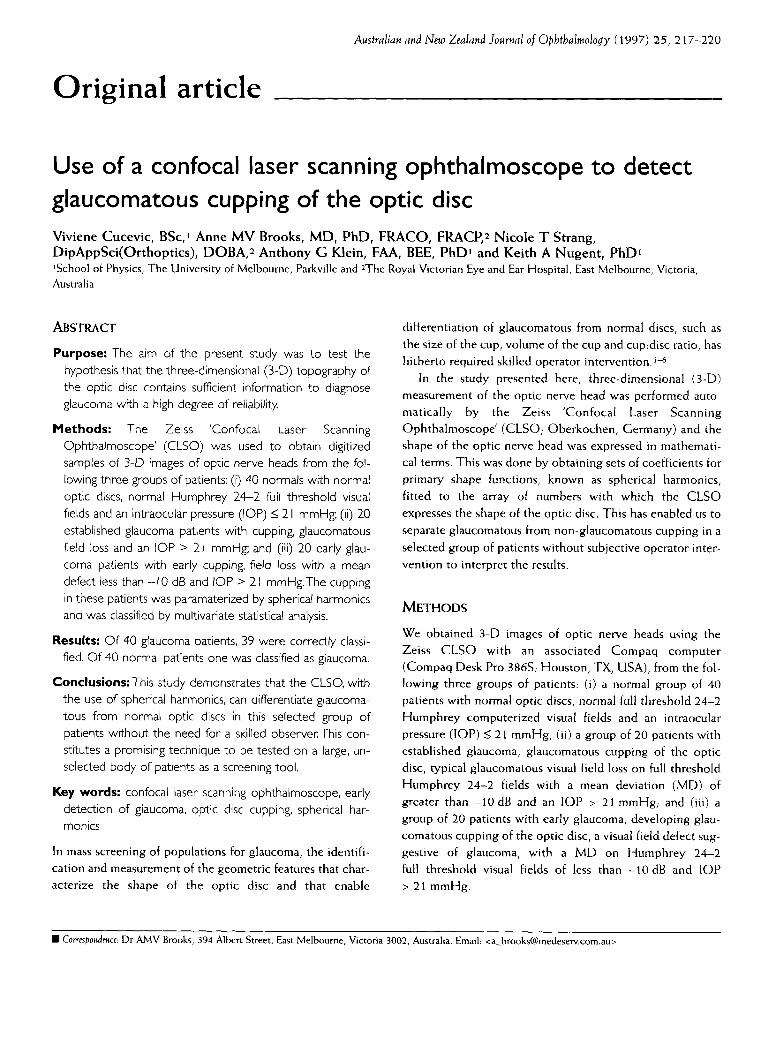
Figure 1. Simplified two-dimensional schematic illustrating how a CLSO image can be approximated to a set of plane curves ( ), which are symbolically represented in rnathe- matics as Y,,m,
Glaucomatous cupping was assessed clinically in accor- dance with the criteria of Kirsch and Anderson,' with par- ticular attention paid to destruction of tissue at the rim of the disc, by two independent observers. The observers were satisfied that the discs showed glaucomatous cupping con- sistent with the field defect or that the disc was normal, con- sistent with a normal field. They were unaware of the CLSO findings or of the proportion of normal and glaucomatous patients examined. The CLSO examination was performed in all cases by the same worker (VC) who was unaware of the findings of the independent observers.
In mathematical terms, the description of shapes may be achieved by fitting weighted sums of various primitive shape functions to the object to be parameterized. In our case, we have used a set of independent, mutually exclusive primitive shape functions, known as spherical harmonics,E which allow the reduction of any shape to a set of coefficients. The lowest- order spherical harmonic is a sphere. The next highest order is a dumb-bell shape which, when added to the sphere, results in an elongated, plum-shaped object and so on, with higher and higher order functions giving more and more precise approximations to the actual shape. A two-dimensional (2-D) analogue of this process is shown in Fig. 1, which attempts to fit curves to a cross-sectional view of a slice representing the optic disc shape.
Our procedure was to fit CLSO optic disc topography measurements with spherical harmonics (up to the 10th order), thus reducing each measurement to a set of 12 1 coef- ficients: Yo,, YIo . . . Y,,,,,. This was performed for the samples of eyes described earlier. The normals were an age- matched random sample.
Ethical approval for the study was provided by the Human Research Ethics Committee of the Royal Victorian Eye and Ear Hospital.
The CLSO used in the present study was the Zeiss CLSO, in which the focused 633 nm HeNe laser beam is scanned across the retina. It is characterized by a spot size of 10 pm, a power of 150 pW at the eye and a scan time of 0.32 s and it outputs data of 672 x 576 pixels in eight planes
separated by 100 pm each. Its operation is based on the con- focal principle6.9 whereby the scattered return light from the focal spot is passed through a pinhole at the conjugate focus of the instrument. This isolates the light that comes from a particular plane and largely rejects the light that originates either in front of or behind the plane being measured at that time.'&l2 Eight different positions of the confocal pinhole give an image slice in each of the eight planes mentioned; the output data is, therefore, a 3-D block of data represent- ing a 3-D image of the area of the optic disc under observa- tion.
In the present study we concentrated on characterizing the topography of the optic disc using software provided with the ophthalmoscope. The details of the programming of the software were not available, but the principle is to identify the brightest point in a scan in depth as corre- sponding to a point on the surface of the optic disc. Thus, a quantitative 2-D image of the topography of the optic disc is returned and these were the data used in the remainder of the study reported here.
For each eye under study we obtained a 672 x 576 pixel image of the topography of the optic disc. Using software written for the purpose, these data were reduced to the coef- ficients of a sum of the spherical harmonic functions. Coefficients were obtained only up to the order 10 for this study, although the images would require a much higher order to be fully characterized and this may be the subject for further work.
The accuracy and reproducibility of CLSO measure- ments have been discussed by Cioffi et al.10 In the case of the study here, where our raw data has been reduced to spheri- cal harmonic coefficients, the key data are these coefficients and repeat images of eight patients produced an average dif- ference in the coefficients of 2.0%; this was deemed to be adequate for the purposes of our study.
Linear multivariate analysis using the Minitab (version 10.51 Xtra (1995); Minitab Inc, State College, PA, USA) was then used to maximally discriminate between normal and glaucomatous optic disc shapes. Multivariate analysisl3,l4 i s
a statistical technique that finds the multi-dimensional dis- tribution of weighted coefficients such that the distributions under study have least overlap. In this work we took two sets of data: one characterized the optic disc topography of a set of normal eyes and the other characterized the set of glau- comatous eyes. Having found the combination of parame- ters that maximally distinguished our two sets of data we were able to feed the data from a given eye back into the program to classify it as either glaucomatous or normal by determining the region of parameter space to which it most closely corresponded. The number of misclassified eyes, therefore, will indicate the degree to which the two distrib- utions overlap. We anticipate that a small number of mis-

CLSO to detect glaucomatous cupping 219
classifications gives confidence that glaucomatous eyes are well identified by the optic disc topography determined and characterized by the methods described here.
RESULTS There were 24 males and 16 females (mean (*SD) age 6 2 i 15 years; range 24-9 1 years) in the normal group and 24 males and 16 females (mean age 68* 1 3 years; range 23-86 years) in the glaucoma group. Of the 40 patients in the glau- coma group, there were 12 males and eight females (mean age 68* 16 years, range 23-86 years) in the early glaucoma group and, in the more advanced glaucoma group, there were 12 males and eight females (mean age 68*9 years; range 46-83 years). One eye from each patient was analysed, giving a total of 80 eyes from 80 patients.
The results are shown in Table 1 , which compares the output of linear multivariate analysis with the clinicians' diagnosis. It may be seen that: ( 1 ) One group of 40 eyes of 40 patients included 39 diag- nosed as clinically normal and one patient diagnosed as clin- ically glaucomatous. This indicates that the analysis differentiated 39 patients correctly as normal giving 97.5% correct negatives. The one normal patient misclassified by the method as 'glaucoma' had a normal visual field and IOP and was considered by the observers to have a normal optic disc. Thus, this case was a false positive. (2) The other group of 40 eyes of 40 patients included 39 patients diagnosed as glaucoma and one patient diagnosed as clinically normal. This indicates that the analysis cor- rectly differentiated 39 patients, giving 97.5% correct posi- tives. ( 3 ) Of the 40 eyes of 40 patients clinically diagnosed as having glaucoma, all 20 with established glaucoma were cor- rectly classified, but one of 20 with early glaucoma was com- puted as being normal using the sets of coefficients obtained, giving 2.5% false negatives for the 40 patients with glaucoma. This misclassified patient had a difference in cup:disc ratio of 0.2 between the two eyes, an IOP over 2 i mmHg and early field loss suggestive of glaucoma. (4) The overall diagnosis was correct in 78 of 80 eyes, one eye with early glaucoma being misdiagnosed as normal and one normal eye incorrectly classified as glaucoma. This gave an overall correct rate of 97.5%, with an overall misclassifi- cation rate of 2.5%.
The outcome of the present investigation was that the distributions of shape parameters of the two different groups, glaucomatous and normal, were almost completely separate; that is, the weighted set of coefficients that describe a glaucomatous shape are sufficiently different from those that describe a normal shape as to give a correct clas- sification to 39 of 40 cases in each group.
Table 1 . Classification rates for the analysis technique with respect to clinician diagnosis, with the glaucoma group separated into established and early
Clinician diagnosed Normal Glaucoma
Established Early Total ~~ ~
Analysis technique Normal 97.5% (39) 0% (0) 5.0% ( 1 ) 2.5% ( 1 ) Glaucoma 2.5% ( 1 ) 100% (20) 95.0% (19) 97.5% (39)
DISCUSSION The aim of the present study was to test the hypothesis that the morphology of the optic disc (i.e. the 3-D shape) contains sufficient information by itself to diagnose glaucoma without the use of a skilled observer as compared with diagnoses by experienced clinicians using complex clinical methods. The measurement of the 3-D shape of the optic disc is made pos- sible by the CLSO, which has been briefly described.
Ranked segment distribution curves have been used recently to describe and quantify the configuration of the optic nerve head, relying on estimates of rim area and retinal nerve fibre layer cross-section area.15 Another method has used the third moment of optic disc depth values to dis- criminate early glaucomatous from normal discs.16-18 Unlike the method described in the present paper, these methods have required skilled interpretation and have had substantial overlap between the distribution of the parameters measured for normal and glaucomatous eyes.
The method described here identified glaucomatous changes in the optic disc by a mathematical description of its topography, allowing the detection of subtle changes associ- ated with the destruction of the nerve fibre layer. This consti- tutes a promising technique to be tested on a large, unselected body of patients as a screening tool. This would include patients with the range of different types of cup recently described by Nicolela and Drance.19 I f the method proves reliable it would be better than stereophotography or direct ophthalmoscopy, as it would not need a skilled observer.
In a screening programme, attention would also need to be paid to measurement of IOP which, although not always elevated in glaucoma,20J' may sometimes be significantly elevated without causing optic disc changes and must still be considered a serious risk factor. Differences in cup:disc ratio between the two eyes of 0.2 or more may indicate progres- sive cupping which has not yet caused visual field changes or detectable nerve fibre loss. The present method of describing optic disc cupping should obviate the need to use time-consuming visual fields as a screening procedure, par- ticularly given their unreliability o n a single test basis.22-26
A simple, rapid test such as that described here would

220 Cucevic et al
facilitate large scale screening for glaucoma and an early case missed by this method would be likely to be found at a subsequent screening. In the future, the method may be further adapted to quantify the amount of cupping due to glaucoma and, thus, to detect progression of cupping.
ACKNOWLEDGEMENTS This research was performed under Research Projects 87/100/93 and 89/126/94 of the Royal Victorian Eye and Ear Hospital and was funded by the Eye Ear Nose and Throat Research Institute, the Australian Research Council and the Research Committee of the Royal Victorian Eye and Ear Hospital. The software developed for this project is subject to copyright in the name of the University of Melbourne.
REFERENCES 1.
2.
3.
4.
5.
6
7
8
9
Weinreb R. Laser scanning tomography to diagnose and monitor glaucoma (Editorial Review). Cun. Opin. Opbtbalmol. 1993; 4: 3-6. Damms T, Dannheim F. Sensitivity and specificity of optic disc parameters in chronic glaucoma. Invest. Opbtbalmol. Vis. Sci.
Caprioli J , Ortiz-Colberg R, Miller JM, Tressler C. Measurements of peripapillary nerve fibre layer contour in glaucoma. Am. J . Opbtbalmol. 1989; 108: 404-13. Caprioli J, Miller JM. Videographic measurements of optic nerve topography in glaucoma. Invest. Opbtbalmol. VIS. Sci. 1988;
Zinser C, Harbath U, Schroder H. Formation and analysis of three-dimensional data with the laser tomographic scanner (LTS). In: Nasemann J, Burk ROW (eds). Scanning laser opbtbal- moscopy and tomograpby. Munich: Quintessenz, 1990; 243-52. Weinreb R, Dreher AW, Bille JF. Quantitative assessment of the optic nerve head with the laser tomographic scanner. Int. Opbtbalmol. 1989, 13: 25-9. Kirsch RE, Anderson DR. Clinical recognition of glaucoma- tous cupping. Am. J. Opbtbalmol. 1973; 75: 442-54. Mathews J , Walker RL. Matbematical metbods of pbysics, 2nd edn. New York: WA Benjamin Inc., 1970. Woon WH, Fitzke FW, Bird AC, Marshall J. Confocal imaging of the fundus using a scanning laser ophthalmoscope. Br. J. Opbtbalmol. 1992; 76: 470-4.
1993; 34: 2246-50.
29: 1294-8.
10.
1 1
12
13
14
15
16
17
18.
19
20
21
22
23
24
25
Cioffi GA, Robin AL, Eastman RD, Perell HF, Sarfarazi FA, Kelman SE. Confocal laser scanning ophthalmoscope. Reproducibility of optic nerve head topographic measure- ments with the confocal laser scanning ophthalmoscope. Opbtbalmology 1993; 100: 57-62. Offenhauser F. Applications of the laser scan ophthalmoscope in ophthalmology. Jpn. J. Vis. Sci. 1992; 12: 1-7. Wilson T, Sheppard CJR. Tbeory and practices of scanning optical microscopy. London: Academic Press, 1 984. Johnson RA, Wichern DW. Applied multivariate statistical arralysis, 2nd edn. New Jersey: Prentice Hall, 1988. Ryan BF, Joiner BL, Pyan TA. Minitab Handbook, 2nd edn. Boston: Duxbury Press, 1985. Asawaphureekorn S, Zangwill L, Weinreb RN. Ranked segment distribution curve for interpretation of optic nerve topography. J . Glaucoma 1996; 5: 79-90. Uchida H, Brigatti L, Caprioli J . Discrimination between normal and early glaucoma with a confocal scanning laser. Invest. Opbtbalmol. Iris. Sci. 1996; 37 (Suppl.): s1096. Caprioli J, Prum B, Zeyen T. Comparison of methods to eval- uate the optic nerve head and nerve fibre layer for glaucoma- tous change. Am. J. Opbtbalmol. 1996; 121: 659-67. Brigatti L, Caprioli J . Correlation of visual field with scanning confocal laser optic disc measurements in glaucoma. Arcb. Opbtbalmol. 1995; 1 1 3: 1191-4. Nicolela MT, Drance SM. Various glaucomatous optic nerve appearances: Clinical correlations. Opbtbalmology 1996; 103:
Xelsch JM. Screening for glaucoma in the 21st century. Symposium: Diagnostic and therapeutic projections for glau- coma management into the 21st century. J. Glaucoma 1993; 2:
Xelsch JM. Screening for primary open-angle glaucoma: Alternative strategies and future directions. J. Glaucoma 1992; I : 214-18. Lichter PR. Visual field validity and search for glaucoma's holy grail (Editorial). Opbtbalmology 1994; 101: 1479-80. Weinreb RN. How should a clinician evaluate a new visual field test in glaucoma (Editorial)? J . Glaucoma 1994; 3: 2-3. Zulauf M, Caprioli J . Fluctuation of the visual field in glau- coma. Opbtbalmol. Clin. Nortb Am. 1991; 4: 671-97. Schulzer M. Errors in the diagnosis of visual field progression in normal-tension glaucoma. Opbtba lmology 1994; 1 0 1 :
640-9.
128-30.
1589-95. 26. Anderson DR. The future of automated perimetry. J. Glaucoma
1993; 2: 133-5.