unusual tanning by chris sanders. chief complaints weaker and more tired over past 4 months severe...
TRANSCRIPT
Unusual TanningBy Chris Sanders

Chief Complaints
Weaker and more tired over past 4 months
Severe increase in past week
Unable to enjoy outdoor activities
Unusual tan
History of Present Illness/Previous Medical
History
48 year old white woman
Loss of appetite
Progressive fatigue
Mild nausea
Surgically treated appendicitis 10 years ago
Seroconverted to PPD (+) 6 years ago; treated for 12 months with INH
Pernicious anemia x 5 years
Hypercholesterolemia x 1 year; controlled with diet and exercise
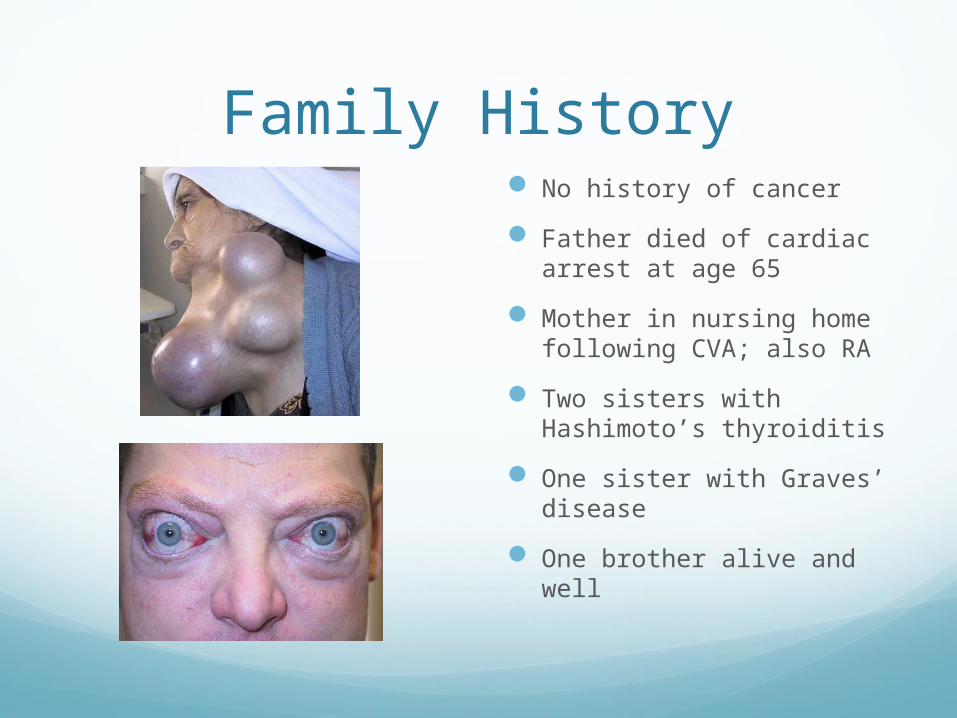
Family History No history of cancer
Father died of cardiac arrest at age 65
Mother in nursing home following CVA; also RA
Two sisters with Hashimoto’s thyroiditis
One sister with Graves’ disease
One brother alive and well
What is the major significance of this
patient’s family history?
The Common Factor
Rheumatoid Arthritis Autoimmune Disease
Hashimoto thyroiditis Autoimmune Disease
Autoimmune Disease Graves’ disease
Meds Cyanocobalamin, 200µg
IM on 15th of each month (physician recently increased dosage)
ASA → swelling of face
TMP-SMX → bright red rash that covered her torso and face, reportedly with fever
Cyanocobalamin
Why is the patient taking this medication?
Vitamin B12 deficiency
Why is oral cyanocobalamin not an option for her condition?
Oral side effects may include hives, difficulty breathing, swelling of the face, headache, nausea, diarrhea
Review of Systems (-) for fever, chills,
shortness of breath, night sweats, and cough
(+) for weight loss of 6 pounds in the last month
(+) for salt cravings before nausea developed
(+) for several bouts of dizziness, one fainting spell in the last 6 months
(+) for few aches and pains
(-) for recent changes in vision
(-) for changes in menstrual cycle
(+) for prominent tanning of the skin, although she denies significant exposure to the sun
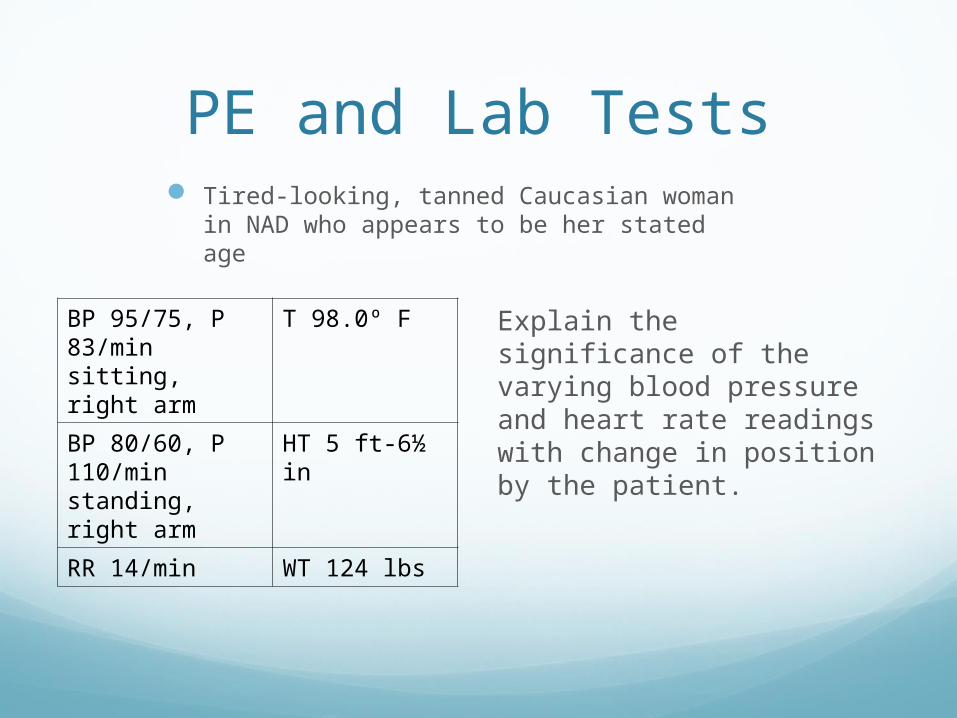
PE and Lab Tests Tired-looking, tanned Caucasian woman in
NAD who appears to be her stated age
Explain the significance of the varying blood pressure and heart rate readings with change in position by the patient.
BP 95/75, P 83/min sitting, right arm
T 98.0º F
BP 80/60, P 110/min standing, right arm
HT 5 ft-6½ in
RR 14/min WT 124 lbs
PE and Lab Tests cont.
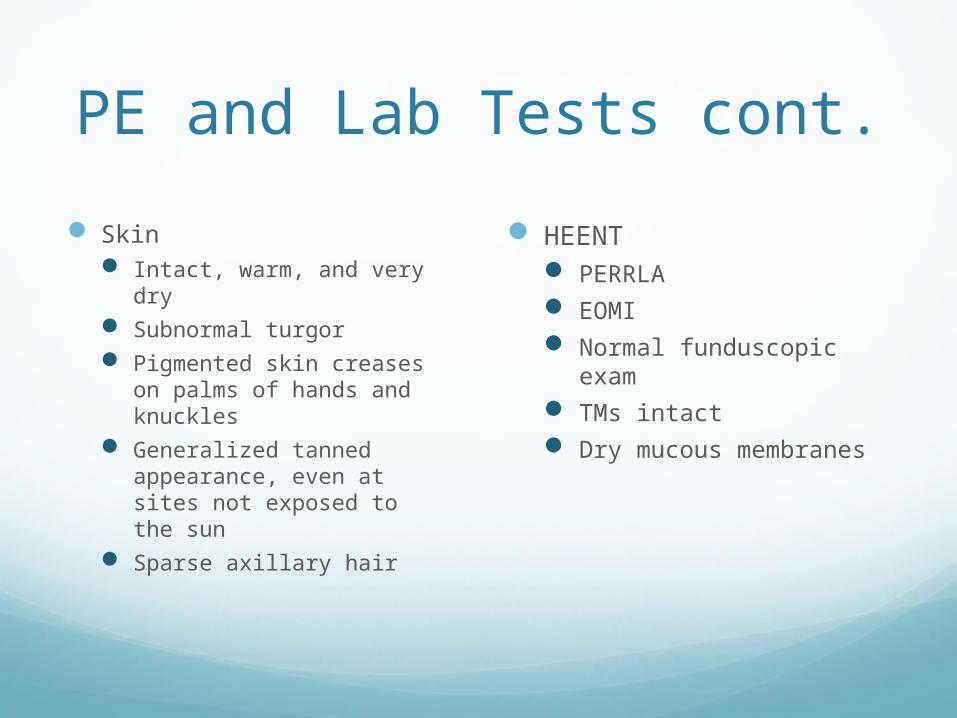
HEENT PERRLA EOMI Normal funduscopic
exam TMs intact Dry mucous membranes
Skin Intact, warm, and very
dry Subnormal turgor Pigmented skin creases
on palms of hands and knuckles
Generalized tanned appearance, even at sites not exposed to the sun
Sparse axillary hair
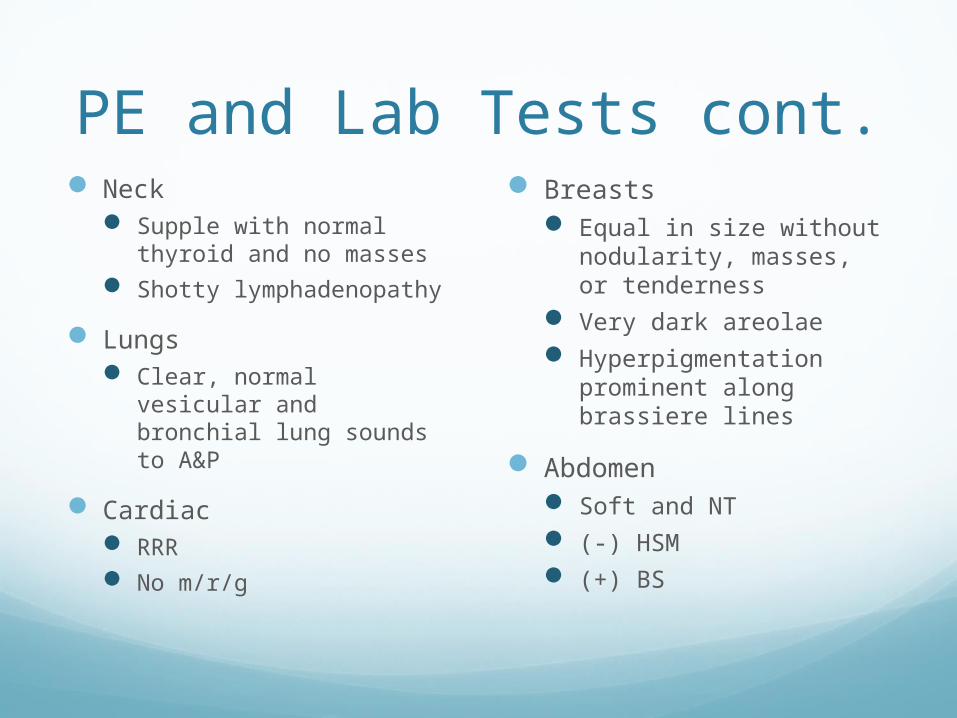
PE and Lab Tests cont. Neck
Supple with normal thyroid and no masses
Shotty lymphadenopathy
Lungs Clear, normal vesicular
and bronchial lung sounds to A&P
Cardiac RRR No m/r/g
Breasts Equal in size without
nodularity, masses, or tenderness
Very dark areolae Hyperpigmentation
prominent along brassiere lines
Abdomen Soft and NT (-) HSM (+) BS
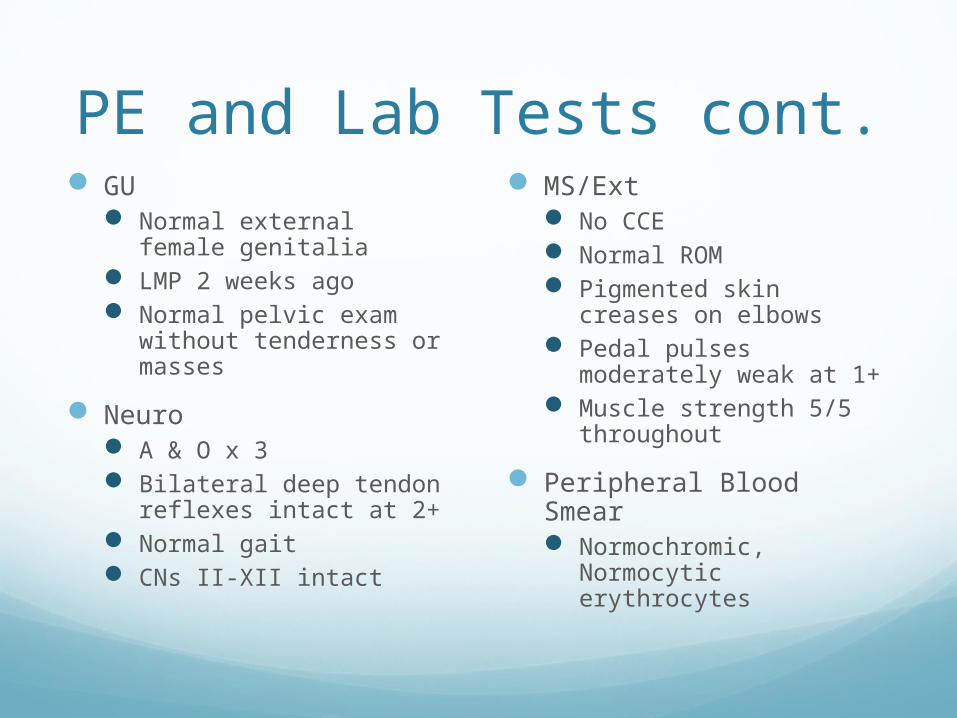
PE and Lab Tests cont. GU
Normal external female genitalia
LMP 2 weeks ago Normal pelvic exam
without tenderness or masses
Neuro A & O x 3 Bilateral deep tendon
reflexes intact at 2+ Normal gait CNs II-XII intact
MS/Ext No CCE Normal ROM Pigmented skin creases
on elbows Pedal pulses moderately
weak at 1+ Muscle strength 5/5
throughout
Peripheral Blood Smear Normochromic,
Normocytic erythrocytes
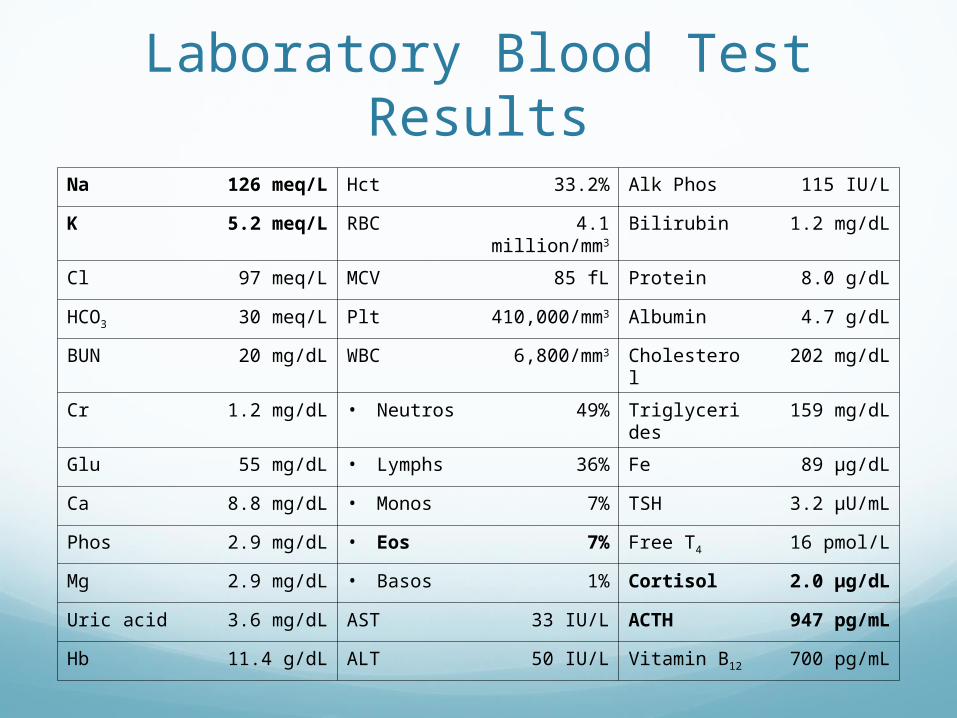
Laboratory Blood Test ResultsNa 126 meq/L Hct 33.2% Alk Phos 115 IU/L
K 5.2 meq/L RBC 4.1 million/mm3
Bilirubin 1.2 mg/dL
Cl 97 meq/L MCV 85 fL Protein 8.0 g/dL
HCO3 30 meq/L Plt 410,000/mm3
Albumin 4.7 g/dL
BUN 20 mg/dL WBC 6,800/mm3 Cholesterol 202 mg/dL
Cr 1.2 mg/dL • Neutros 49% Triglycerides 159 mg/dL
Glu 55 mg/dL • Lymphs 36% Fe 89 µg/dL
Ca 8.8 mg/dL • Monos 7% TSH 3.2 µU/mL
Phos 2.9 mg/dL • Eos 7% Free T4 16 pmol/L
Mg 2.9 mg/dL • Basos 1% Cortisol 2.0 µg/dL
Uric acid 3.6 mg/dL AST 33 IU/L ACTH 947 pg/mL
Hb 11.4 g/dL ALT 50 IU/L Vitamin B12 700 pg/mL
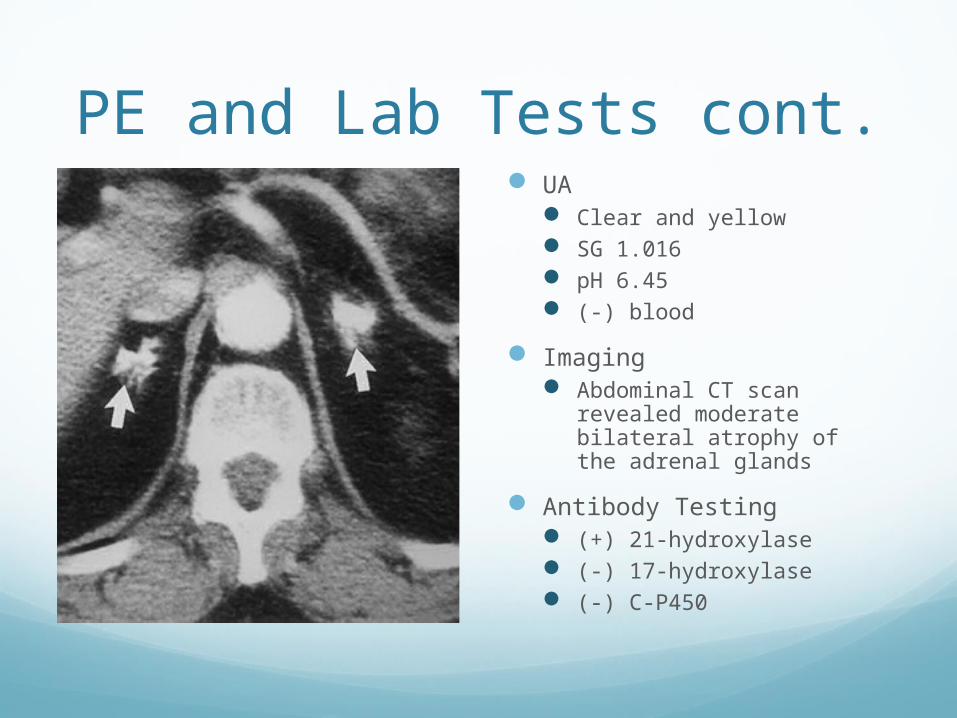
PE and Lab Tests cont. UA
Clear and yellow SG 1.016 pH 6.45 (-) blood
Imaging Abdominal CT scan
revealed moderate bilateral atrophy of the adrenal glands
Antibody Testing (+) 21-hydroxylase (-) 17-hydroxylase (-) C-P450
What is your diagnosis?
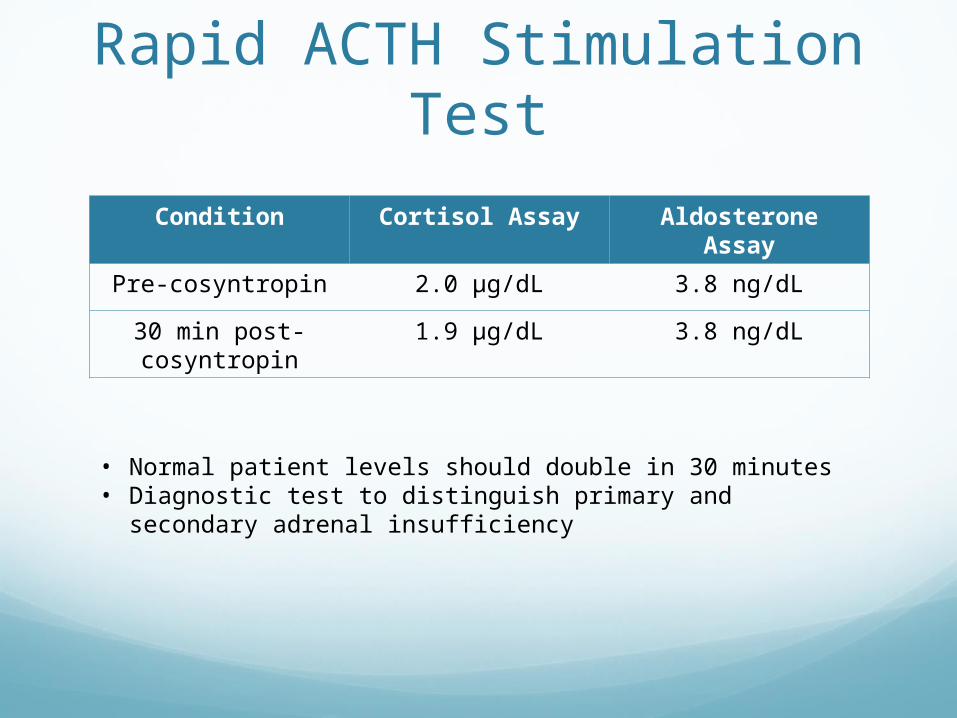
Rapid ACTH Stimulation Test
Condition Cortisol Assay Aldosterone Assay
Pre-cosyntropin 2.0 µg/dL 3.8 ng/dL
30 min post-cosyntropin
1.9 µg/dL 3.8 ng/dL
• Normal patient levels should double in 30 minutes• Diagnostic test to distinguish primary and secondary
adrenal insufficiency
Closing QuestionsWhat is the single greatest risk factor for
Addison disease in this patient?
What is the most likely cause of Addison disease in this patient?
Why can tuberculosis be ruled out as a cause of Addison disease in this patient?
Which two test results are most suggestive of the cause of Addison disease in this patient?
Closing QuestionsWould supplementation with fludrocortisone be
appropriate in this patient?
Does this patient have any signs of hypothyroidism, a disorder that is commonly associated with Addison disease?
There are 19 clinical signs and symptoms in this case study that are consistent with Addison disease. Identify 15 of them.
Which single test result is diagnostic for Addison disease in this patient?
Closing QuestionsWhich test results support the assessment that
the patient’s anemia is not the result of iron deficiency?
Which test results support the assessment that the patient’s anemia is not the result of vitamin B12 deficiency?
Why is shotty lymphadenopathy consistent with a diagnosis of Addison disease in this patient?