university of groningen hidradenitis suppurativa janse ...university of groningen, university...
TRANSCRIPT
University of Groningen
Hidradenitis suppurativaJanse, Ineke Christina
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2016
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Janse, I. C. (2016). Hidradenitis suppurativa: Pathogenesis, burden of disease and surgical strategies.[Groningen]: Rijksuniversiteit Groningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 20-02-2020
9SURGICAL PROCEDURES IN HIDRADENITIS SUPPURATIVA
I.C. Janse1, A. Bieniek2, B. Horváth1, Ł. Matusiak2
Department of Dermatology1,
University of Groningen,
University Medical Centre Groningen,
Groningen, the Netherlands,
Department of Dermatology2,
Wroclaw Medical University,
University of Wrocław,
Wrocław, Poland
Published in Dernatologic Clinics,
2016; 34(1): 97-109
105
106
9
KEY POINTS • At least in higher stages of HS, surgery should be introduced early after setting the diag-
nosis. • Preoperatively, immunosuppressive and/or antibacterial medical treatment to calm active
inflammation must be considered. Imaging (ultrasonography, MRI) may be helpful. • Depending on the extent and severity of the disease local, tumescent, spinal and/or
general anesthesia are used. • Acute phase surgical treatment and treatment of the chronic continue intermediary phase
should be distinguished. Incision and drainage can offer pain relief in a setting of a tense fluctuating acute abscess.
• After wide excision, different wound closure techniques can be chosen. Secondary in-tention healing ensures usually good functional and cosmetic results in defects up to 140 cm2.
INTRODUCTIONHidradenitis suppurativa (HS) is difficult to treat owing to its complex pathomechanism; be-side the extensive inflammation with abscesses and inflammatory nodules, there is also sinus tract formation and in severe cases extensive scarring.1 Surgery should be introduced early in the management of HS. Unfortunately, surgical treat-ment is often performed many years after the initial symptoms of the disease, after numerous ineffective cycles of pharmacotherapy.2 Such delays are often caused by misdiagnosis, a doc-tor’s lack of knowledge about the disease, unjustified confidence in the efficacy of non-inva-sive therapies, anxiety about surgical treatment and the embarrassing location.3 The tolerance to and satisfaction with, sometimes debilitating, surgical procedures is surpris-ingly high and may result from the large psychosocial impact of HS. Because the magnitude of life impairment in HS is far greater than in other dermatoses, patients are highly willing to change the condition.4,5
TREATMENT GOALS AND PLANNED OUTCOMESThe comparison of different operative methods of HS is difficult because of the many types of surgery, interindividual differences between patients and between operators, the shortage of randomized trials and the lack of consensus about the endpoints used. To be able to compare different surgical interventions, clear definitions of outcomes should be defined. We therefore suggest outcomes for future studies.
Relapse ratesRelapse (owing to non-radical surgery) is defined as inflammatory activity occurring within 0.5 cm of the surgical scar. The natural progression of HS can be defined as inflammation that develops outside this area but in the same anatomic region.6
107
9
Time to wound closureThe time to wound closure is defined as the duration of the wound healing (complete healing) measured in days. For sutured lesions, complete healing may be considered achieved when the stitches have been removed.
ComplicationsEarly complications include haemorrhage, infection, hypergranulation, necrosis of grafts or flaps, injury of brachial plexus or big axillary vessels and thrombosis of brachial veins.2 Late complications include wound dehiscence, retention of serum (seroma), cicatricial contracture, hypertrophic scars and keloids.2,3,7
Patient reported outcomesPatient satisfaction can be cosmetic or functional. The rate of either is measured on a numer-ical rating scale of 1 to 10 where 1 corresponds with very dissatisfied and 10 with excellent. If the satisfaction rate is measured for both functional and cosmetic results, the mean rate is shown. The recommendation of the treatment to other people and willingness to undergo further surgery are also important patient-reported outcomes.
PRE-OPERATIVE PLANNING AND PREPARATIONMedication to calm the inflammationIn moderate and severe HS, it is broadly recommended and accepted that surgery is combined with immunomodulating treatment. However, it remains unclear whether relapse rates after surgery with perioperative immunomodulation therapy are lower than surgical treatments without perioperative medication.8
ImagingImaging is not routinely used in surgery of HS although it may be beneficial to management.9 Some studies with ultrasonography showed that the inflammation can be extended hori-zontally and vertically far over the visible borders of the inflammation on the skin surface.10 Moreover, differentiating between enterocutaneous fistula formation in Crohn’s disease re-mains challenging especially in the perianal region. Perianal lesions of Crohn’s disease usually present as wide fistulas, entering deeply through the perianal area to the colon and/or vagina, affecting the skin and subcutaneous tissue only to a small extent. Lesions of HS present as pu-rulent, inflammatory infiltrates, frequently reaching the buttocks and perineum with numerous narrow, less visible shallow fistulas reaching the anus. Moreover, mixed clinical presentations can occur because of coexistence of HS and Crohn’s disease.11 In ambiguous cases imaging with ultrasonography, MRI, CT and fistulography are helpful to assess the location and depth of fistulas and sinuses. Shallow lesions expressing the features of HS can be treated surgically by a (dermato)surgeon, independent from the established di-agnosis of Crohn’s disease. If the diagnosis of Crohn’s disease with deep fistulas is confirmed, the surgical treatment should be carried out in cooperation with proctologic specialists. The diagnostic imaging, primarily fistulography, may be decisive.
108
9
PATIENT POSITIONINGSurgery involving the axillae and mons pubis is performed in supine position. Leg rests are used for operating inguinal and perineal lesions. The patient is placed in prone position during operations on perianal and gluteal HS.
PROCEDURAL APPROACHAnaesthesiaLocal anaesthesia
Local anaesthesia is performed in two steps. First, field block anaesthesia is performed with lidocaine 1% (10 mg/mL) plus adrenaline (5 µg/mL). Second, nodules and/or sinus tracts are injected with the same local anaesthetic. If patients have fear of needles or if they experience a lot of pain during local anaesthesia, lidocaine and prilocaine cream (EMLA) can be applied one hour before the injections.6
Tumescent local anaesthesia
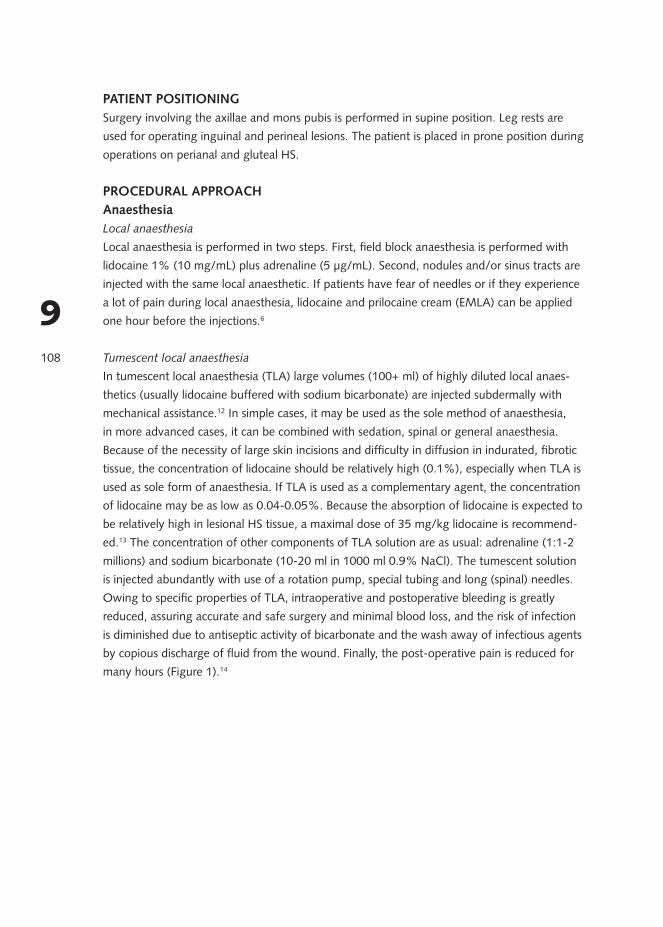
In tumescent local anaesthesia (TLA) large volumes (100+ ml) of highly diluted local anaes-thetics (usually lidocaine buffered with sodium bicarbonate) are injected subdermally with mechanical assistance.12 In simple cases, it may be used as the sole method of anaesthesia, in more advanced cases, it can be combined with sedation, spinal or general anaesthesia. Because of the necessity of large skin incisions and difficulty in diffusion in indurated, fibrotic tissue, the concentration of lidocaine should be relatively high (0.1%), especially when TLA is used as sole form of anaesthesia. If TLA is used as a complementary agent, the concentration of lidocaine may be as low as 0.04-0.05%. Because the absorption of lidocaine is expected to be relatively high in lesional HS tissue, a maximal dose of 35 mg/kg lidocaine is recommend-ed.13 The concentration of other components of TLA solution are as usual: adrenaline (1:1-2 millions) and sodium bicarbonate (10-20 ml in 1000 ml 0.9% NaCl). The tumescent solution is injected abundantly with use of a rotation pump, special tubing and long (spinal) needles. Owing to specific properties of TLA, intraoperative and postoperative bleeding is greatly reduced, assuring accurate and safe surgery and minimal blood loss, and the risk of infection is diminished due to antiseptic activity of bicarbonate and the wash away of infectious agents by copious discharge of fluid from the wound. Finally, the post-operative pain is reduced for many hours (Figure 1).14
109
9Figure 1: Infiltration of the axilla with tumescent local anesthesia (left).Tumescent local anesthesia reduces bleeding and
enhances visualization (right).
General and spinal anaesthesia
Under general and spinal anaesthesia, large areas can be operated without the limitation of the maximum allowed amount of local anaesthetics. In addition, some patients favour general anaesthesia above local anaesthesia which can be painful and hard to achieve in areas of active inflammation and fibrosis.
Lesion removal techniquesIncision and drainage The purpose of incision and drainage is pain relief in case of a tense, fluctuating acute abscess. There is only a short term effect as lesions treated by incision and drainage tend to relapse.15 For drainage, 6- to 8-mm punch biopsies can be used. By digital pressure and rinsing with saline solution the remaining pus is removed.
Deroofing
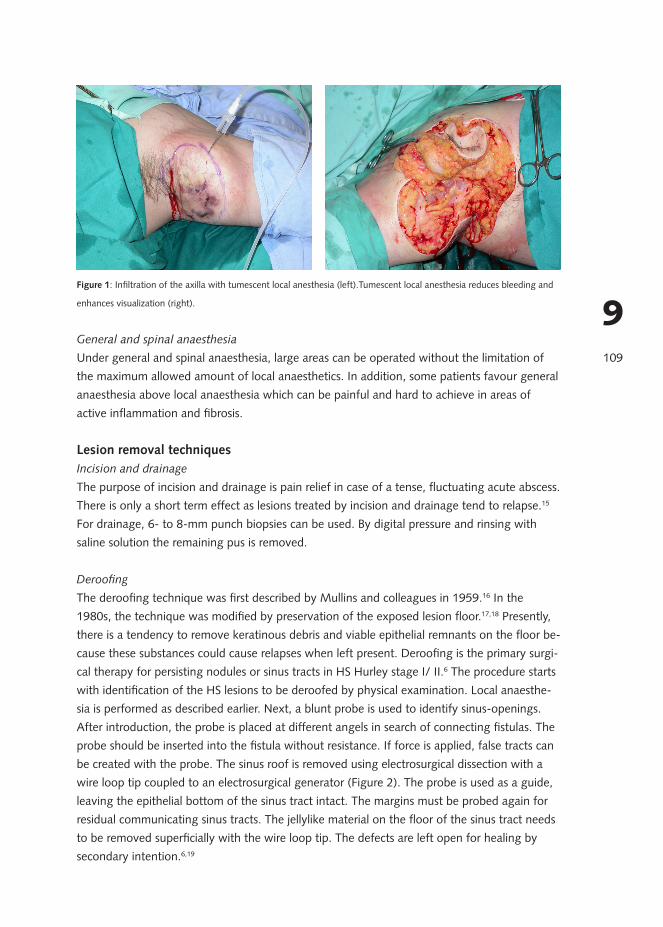
The deroofing technique was first described by Mullins and colleagues in 1959.16 In the 1980s, the technique was modified by preservation of the exposed lesion floor.17,18 Presently, there is a tendency to remove keratinous debris and viable epithelial remnants on the floor be-cause these substances could cause relapses when left present. Deroofing is the primary surgi-cal therapy for persisting nodules or sinus tracts in HS Hurley stage I/ II.6 The procedure starts with identification of the HS lesions to be deroofed by physical examination. Local anaesthe-sia is performed as described earlier. Next, a blunt probe is used to identify sinus-openings. After introduction, the probe is placed at different angels in search of connecting fistulas. The probe should be inserted into the fistula without resistance. If force is applied, false tracts can be created with the probe. The sinus roof is removed using electrosurgical dissection with a wire loop tip coupled to an electrosurgical generator (Figure 2). The probe is used as a guide, leaving the epithelial bottom of the sinus tract intact. The margins must be probed again for residual communicating sinus tracts. The jellylike material on the floor of the sinus tract needs to be removed superficially with the wire loop tip. The defects are left open for healing by secondary intention.6,19
110
9
Figure 2: The sinus roof is removed by electrosurgical dissection in the deroofing procedure.
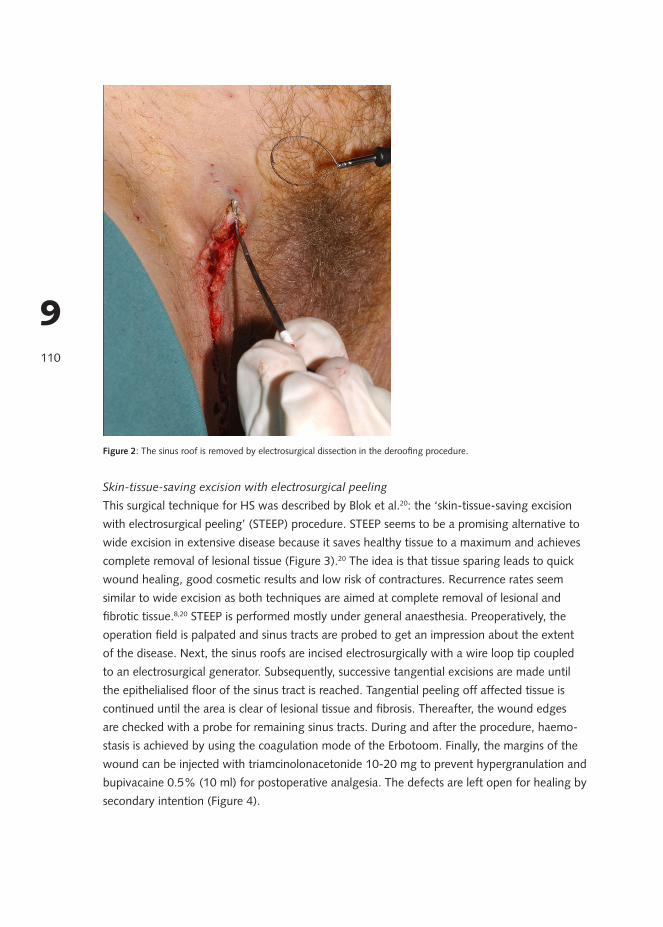
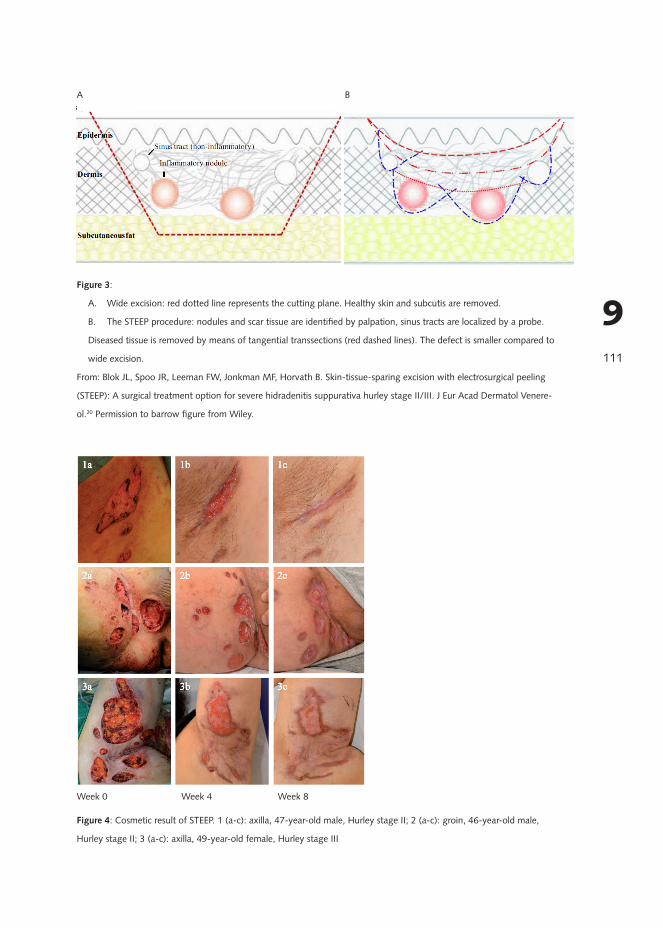
Skin-tissue-saving excision with electrosurgical peeling This surgical technique for HS was described by Blok et al.20: the ‘skin-tissue-saving excision with electrosurgical peeling’ (STEEP) procedure. STEEP seems to be a promising alternative to wide excision in extensive disease because it saves healthy tissue to a maximum and achieves complete removal of lesional tissue (Figure 3).20 The idea is that tissue sparing leads to quick wound healing, good cosmetic results and low risk of contractures. Recurrence rates seem similar to wide excision as both techniques are aimed at complete removal of lesional and fibrotic tissue.8,20 STEEP is performed mostly under general anaesthesia. Preoperatively, the operation field is palpated and sinus tracts are probed to get an impression about the extent of the disease. Next, the sinus roofs are incised electrosurgically with a wire loop tip coupled to an electrosurgical generator. Subsequently, successive tangential excisions are made until the epithelialised floor of the sinus tract is reached. Tangential peeling off affected tissue is continued until the area is clear of lesional tissue and fibrosis. Thereafter, the wound edges are checked with a probe for remaining sinus tracts. During and after the procedure, haemo-stasis is achieved by using the coagulation mode of the Erbotoom. Finally, the margins of the wound can be injected with triamcinolonacetonide 10-20 mg to prevent hypergranulation and bupivacaine 0.5% (10 ml) for postoperative analgesia. The defects are left open for healing by secondary intention (Figure 4).
111
9Figure 3:
A. Wide excision: red dotted line represents the cutting plane. Healthy skin and subcutis are removed.
B. The STEEP procedure: nodules and scar tissue are identified by palpation, sinus tracts are localized by a probe.
Diseased tissue is removed by means of tangential transsections (red dashed lines). The defect is smaller compared to
wide excision.
From: Blok JL, Spoo JR, Leeman FW, Jonkman MF, Horvath B. Skin-tissue-sparing excision with electrosurgical peeling
(STEEP): A surgical treatment option for severe hidradenitis suppurativa hurley stage II/III. J Eur Acad Dermatol Venere-
ol.20 Permission to barrow figure from Wiley.
Figure 4: Cosmetic result of STEEP. 1 (a-c): axilla, 47-year-old male, Hurley stage II; 2 (a-c): groin, 46-year-old male,
Hurley stage II; 3 (a-c): axilla, 49-year-old female, Hurley stage III
Week 0 Week 4 Week 8
A B
112
9
Excision
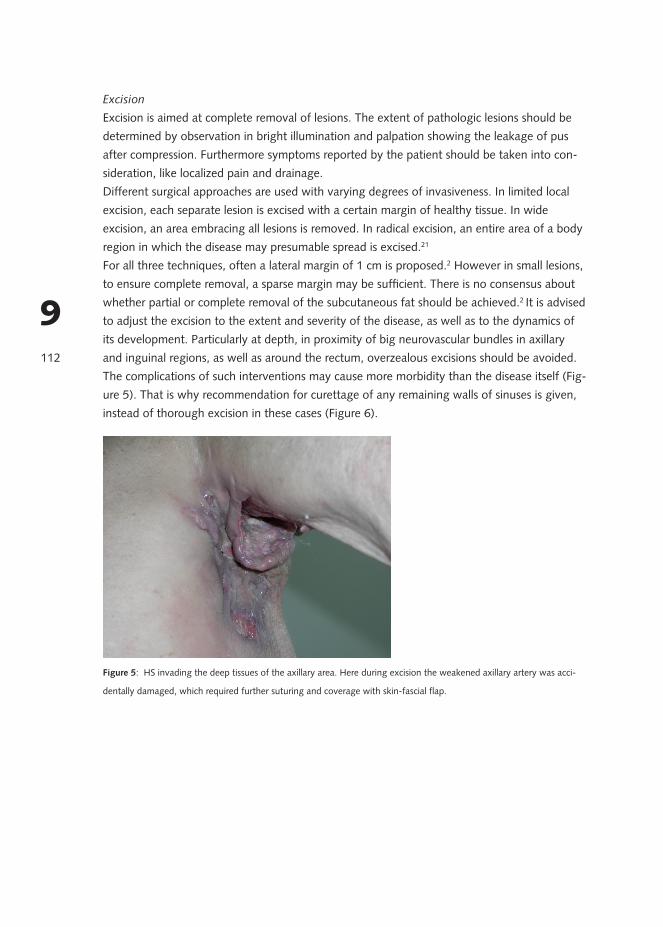
Excision is aimed at complete removal of lesions. The extent of pathologic lesions should be determined by observation in bright illumination and palpation showing the leakage of pus after compression. Furthermore symptoms reported by the patient should be taken into con-sideration, like localized pain and drainage. Different surgical approaches are used with varying degrees of invasiveness. In limited local excision, each separate lesion is excised with a certain margin of healthy tissue. In wide excision, an area embracing all lesions is removed. In radical excision, an entire area of a body region in which the disease may presumable spread is excised.21 For all three techniques, often a lateral margin of 1 cm is proposed.2 However in small lesions, to ensure complete removal, a sparse margin may be sufficient. There is no consensus about whether partial or complete removal of the subcutaneous fat should be achieved.2 It is advised to adjust the excision to the extent and severity of the disease, as well as to the dynamics of its development. Particularly at depth, in proximity of big neurovascular bundles in axillary and inguinal regions, as well as around the rectum, overzealous excisions should be avoided. The complications of such interventions may cause more morbidity than the disease itself (Fig-ure 5). That is why recommendation for curettage of any remaining walls of sinuses is given, instead of thorough excision in these cases (Figure 6).
Figure 5: HS invading the deep tissues of the axillary area. Here during excision the weakened axillary artery was acci-
dentally damaged, which required further suturing and coverage with skin-fascial flap.
113
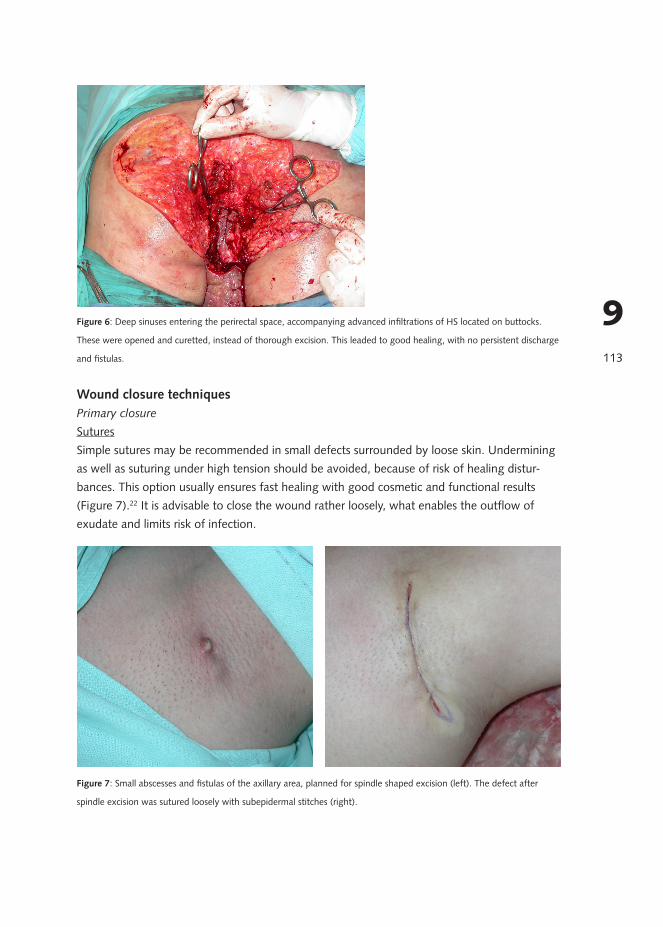
9Figure 6: Deep sinuses entering the perirectal space, accompanying advanced infiltrations of HS located on buttocks.
These were opened and curetted, instead of thorough excision. This leaded to good healing, with no persistent discharge
and fistulas.
Wound closure techniquesPrimary closure
SuturesSimple sutures may be recommended in small defects surrounded by loose skin. Undermining as well as suturing under high tension should be avoided, because of risk of healing distur-bances. This option usually ensures fast healing with good cosmetic and functional results (Figure 7).22 It is advisable to close the wound rather loosely, what enables the outflow of exudate and limits risk of infection.
Figure 7: Small abscesses and fistulas of the axillary area, planned for spindle shaped excision (left). The defect after
spindle excision was sutured loosely with subepidermal stitches (right).
114
9
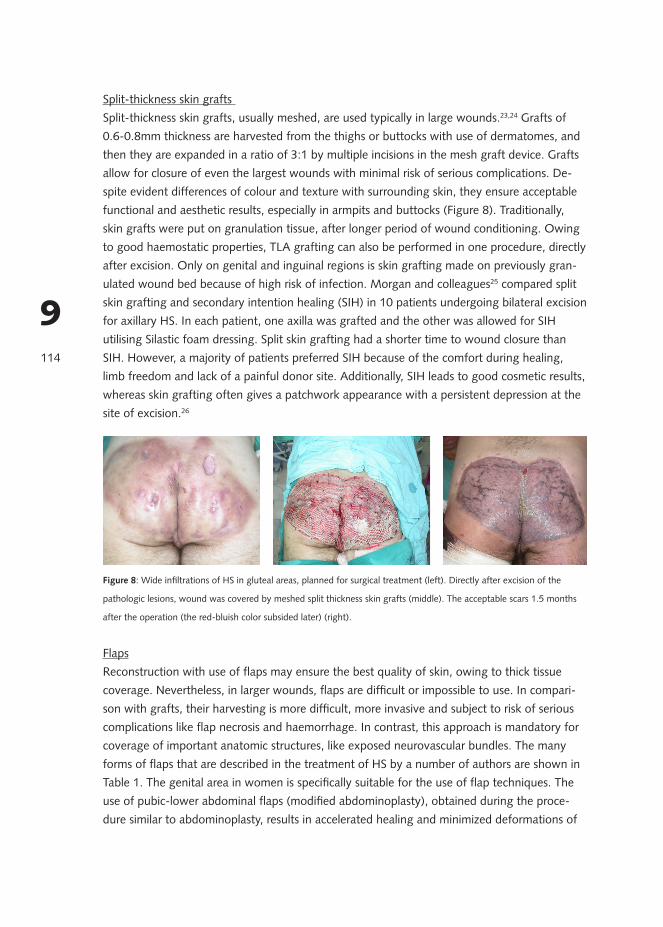
Split-thickness skin grafts Split-thickness skin grafts, usually meshed, are used typically in large wounds.23,24 Grafts of 0.6-0.8mm thickness are harvested from the thighs or buttocks with use of dermatomes, and then they are expanded in a ratio of 3:1 by multiple incisions in the mesh graft device. Grafts allow for closure of even the largest wounds with minimal risk of serious complications. De-spite evident differences of colour and texture with surrounding skin, they ensure acceptable functional and aesthetic results, especially in armpits and buttocks (Figure 8). Traditionally, skin grafts were put on granulation tissue, after longer period of wound conditioning. Owing to good haemostatic properties, TLA grafting can also be performed in one procedure, directly after excision. Only on genital and inguinal regions is skin grafting made on previously gran-ulated wound bed because of high risk of infection. Morgan and colleagues25 compared split skin grafting and secondary intention healing (SIH) in 10 patients undergoing bilateral excision for axillary HS. In each patient, one axilla was grafted and the other was allowed for SIH utilising Silastic foam dressing. Split skin grafting had a shorter time to wound closure than SIH. However, a majority of patients preferred SIH because of the comfort during healing, limb freedom and lack of a painful donor site. Additionally, SIH leads to good cosmetic results, whereas skin grafting often gives a patchwork appearance with a persistent depression at the site of excision.26
Figure 8: Wide infiltrations of HS in gluteal areas, planned for surgical treatment (left). Directly after excision of the
pathologic lesions, wound was covered by meshed split thickness skin grafts (middle). The acceptable scars 1.5 months
after the operation (the red-bluish color subsided later) (right).
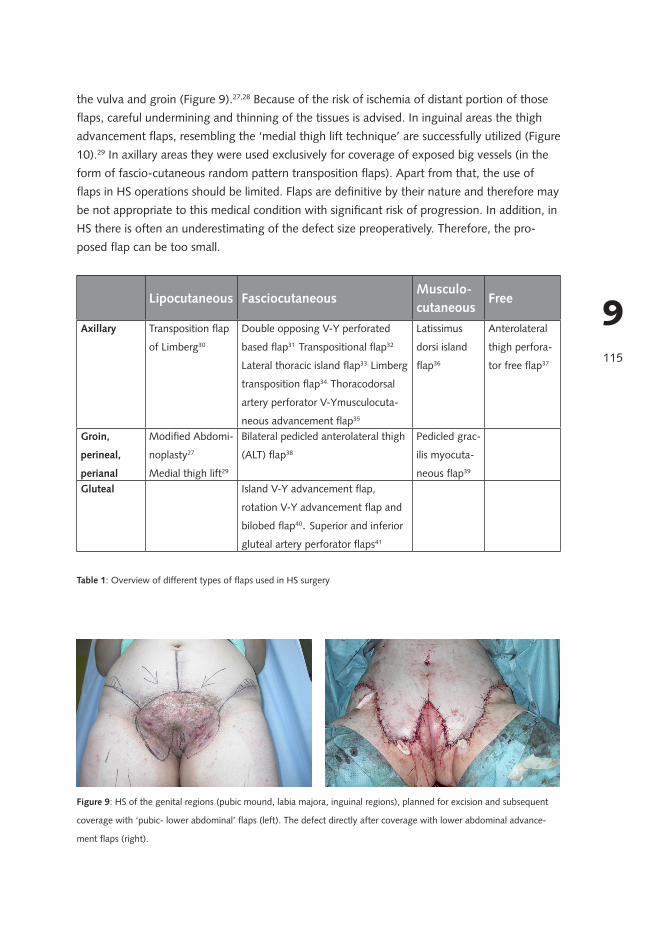
FlapsReconstruction with use of flaps may ensure the best quality of skin, owing to thick tissue coverage. Nevertheless, in larger wounds, flaps are difficult or impossible to use. In compari-son with grafts, their harvesting is more difficult, more invasive and subject to risk of serious complications like flap necrosis and haemorrhage. In contrast, this approach is mandatory for coverage of important anatomic structures, like exposed neurovascular bundles. The many forms of flaps that are described in the treatment of HS by a number of authors are shown in Table 1. The genital area in women is specifically suitable for the use of flap techniques. The use of pubic-lower abdominal flaps (modified abdominoplasty), obtained during the proce-dure similar to abdominoplasty, results in accelerated healing and minimized deformations of
115
9
the vulva and groin (Figure 9).27,28 Because of the risk of ischemia of distant portion of those flaps, careful undermining and thinning of the tissues is advised. In inguinal areas the thigh advancement flaps, resembling the ‘medial thigh lift technique’ are successfully utilized (Figure 10).29 In axillary areas they were used exclusively for coverage of exposed big vessels (in the form of fascio-cutaneous random pattern transposition flaps). Apart from that, the use of flaps in HS operations should be limited. Flaps are definitive by their nature and therefore may be not appropriate to this medical condition with significant risk of progression. In addition, in HS there is often an underestimating of the defect size preoperatively. Therefore, the pro-posed flap can be too small.
Lipocutaneous FasciocutaneousMusculo-cutaneous
Free
Axillary Transposition flap
of Limberg30
Double opposing V-Y perforated
based flap31 Transpositional flap32
Lateral thoracic island flap33. Limberg
transposition flap34. Thoracodorsal
artery perforator V-Ymusculocuta-
neous advancement flap35
Latissimus
dorsi island
flap36
Anterolateral
thigh perfora-
tor free flap37
Groin,
perineal,
perianal
Modified Abdomi-
noplasty27
Medial thigh lift29
Bilateral pedicled anterolateral thigh
(ALT) flap38
Pedicled grac-
ilis myocuta-
neous flap39
Gluteal Island V-Y advancement flap,
rotation V-Y advancement flap and
bilobed flap40. Superior and inferior
gluteal artery perforator flaps41
Table 1: Overview of different types of flaps used in HS surgery
Figure 9: HS of the genital regions (pubic mound, labia majora, inguinal regions), planned for excision and subsequent
coverage with ‘pubic- lower abdominal’ flaps (left). The defect directly after coverage with lower abdominal advance-
ment flaps (right).

116
9 Figure 10: HS of the genital regions (inguinal and labia majora), planned for excision and coverage with ‘medial thigh lift’
flaps (left). The defect was covered with skin-subcutaneous ‘medial thigh advancement flaps’ (right).
Healing by secondary intention
Secondary intention healing (SIH) may be successful in defects up to 140 cm2 (Figure 4, 11).42 SIH occurs along with the natural processes of granulation, wound shrinkage and epithelisa-tion. This approach is typically utilized in the anogenital region, trunk and axillary area.28 SIH ensures usually good functional and cosmetic results (Figure 4, 11). Moreover, the final scar has considerably reduced dimensions in comparison with the initial defect.25 This approach is usually well-tolerated by patients owing to the minimal number of wounds (absence of donor sites) and amazingly unproblematic course of healing (except for the first difficult days).25,28,43 Its major drawbacks are long healing duration (mean 6 - 12 weeks), the risk of unsightly scars in extensive defects, and the development of contractures over flexion areas. Of note, the most important factor responsible for healing period is the size of the wound. The localization was not of relevant.43
Figure 11: HS of axillary area, planned for surgical treatment (left). The scar 3 months after completing secondary inten-
tion healing (SIH). Its size is much smaller than the primary defect (right).
117
9
Combined reconstructions
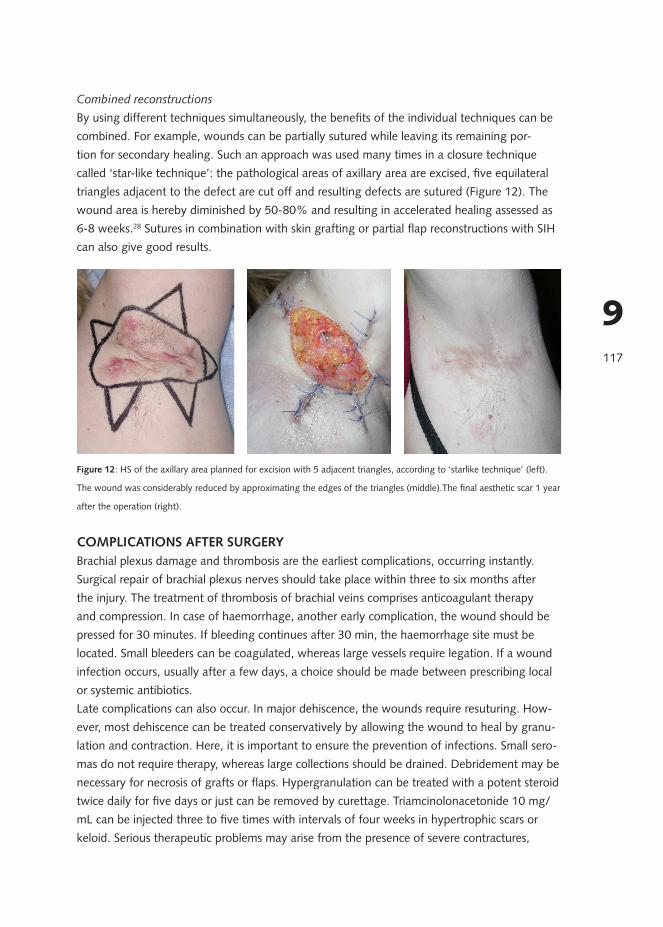
By using different techniques simultaneously, the benefits of the individual techniques can be combined. For example, wounds can be partially sutured while leaving its remaining por-tion for secondary healing. Such an approach was used many times in a closure technique called ‘star-like technique’: the pathological areas of axillary area are excised, five equilateral triangles adjacent to the defect are cut off and resulting defects are sutured (Figure 12). The wound area is hereby diminished by 50-80% and resulting in accelerated healing assessed as 6-8 weeks.28 Sutures in combination with skin grafting or partial flap reconstructions with SIH can also give good results.
Figure 12: HS of the axillary area planned for excision with 5 adjacent triangles, according to ‘starlike technique’ (left).
The wound was considerably reduced by approximating the edges of the triangles (middle).The final aesthetic scar 1 year
after the operation (right).
COMPLICATIONS AFTER SURGERYBrachial plexus damage and thrombosis are the earliest complications, occurring instantly. Surgical repair of brachial plexus nerves should take place within three to six months after the injury. The treatment of thrombosis of brachial veins comprises anticoagulant therapy and compression. In case of haemorrhage, another early complication, the wound should be pressed for 30 minutes. If bleeding continues after 30 min, the haemorrhage site must be located. Small bleeders can be coagulated, whereas large vessels require legation. If a wound infection occurs, usually after a few days, a choice should be made between prescribing local or systemic antibiotics. Late complications can also occur. In major dehiscence, the wounds require resuturing. How-ever, most dehiscence can be treated conservatively by allowing the wound to heal by granu-lation and contraction. Here, it is important to ensure the prevention of infections. Small sero-mas do not require therapy, whereas large collections should be drained. Debridement may be necessary for necrosis of grafts or flaps. Hypergranulation can be treated with a potent steroid twice daily for five days or just can be removed by curettage. Triamcinolonacetonide 10 mg/mL can be injected three to five times with intervals of four weeks in hypertrophic scars or keloid. Serious therapeutic problems may arise from the presence of severe contractures,
118
9
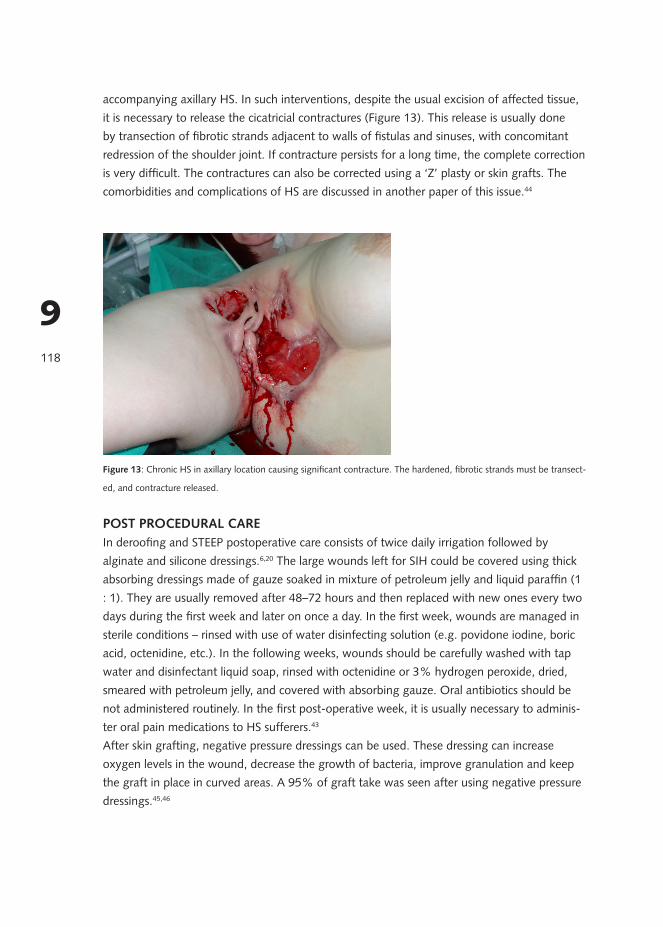
accompanying axillary HS. In such interventions, despite the usual excision of affected tissue, it is necessary to release the cicatricial contractures (Figure 13). This release is usually done by transection of fibrotic strands adjacent to walls of fistulas and sinuses, with concomitant redression of the shoulder joint. If contracture persists for a long time, the complete correction is very difficult. The contractures can also be corrected using a ‘Z’ plasty or skin grafts. The comorbidities and complications of HS are discussed in another paper of this issue.44
Figure 13: Chronic HS in axillary location causing significant contracture. The hardened, fibrotic strands must be transect-
ed, and contracture released.
POST PROCEDURAL CAREIn deroofing and STEEP postoperative care consists of twice daily irrigation followed by alginate and silicone dressings.6,20 The large wounds left for SIH could be covered using thick absorbing dressings made of gauze soaked in mixture of petroleum jelly and liquid paraffin (1 : 1). They are usually removed after 48–72 hours and then replaced with new ones every two days during the first week and later on once a day. In the first week, wounds are managed in sterile conditions – rinsed with use of water disinfecting solution (e.g. povidone iodine, boric acid, octenidine, etc.). In the following weeks, wounds should be carefully washed with tap water and disinfectant liquid soap, rinsed with octenidine or 3% hydrogen peroxide, dried, smeared with petroleum jelly, and covered with absorbing gauze. Oral antibiotics should be not administered routinely. In the first post-operative week, it is usually necessary to adminis-ter oral pain medications to HS sufferers.43
After skin grafting, negative pressure dressings can be used. These dressing can increase oxygen levels in the wound, decrease the growth of bacteria, improve granulation and keep the graft in place in curved areas. A 95% of graft take was seen after using negative pressure dressings.45,46
119
9
REHABILITATION AND RECOVERYIn many cases multistaged, prolonged surgical treatment is needed. That is why optimal thera-py requires the participation of family physician and public health nurses, as well as assistance and acceptance from the family. Lifestyle measures include losing weight in case of obesity and discontinuing smoking. To prevent cicatricial contractures, it is advisable to introduce physical therapy and physiotherapy subsequent to surgery. Depending on the size of the oper-ation, the time until full recovery to pre-operative activity ranges between 4 and 10 weeks.42,47
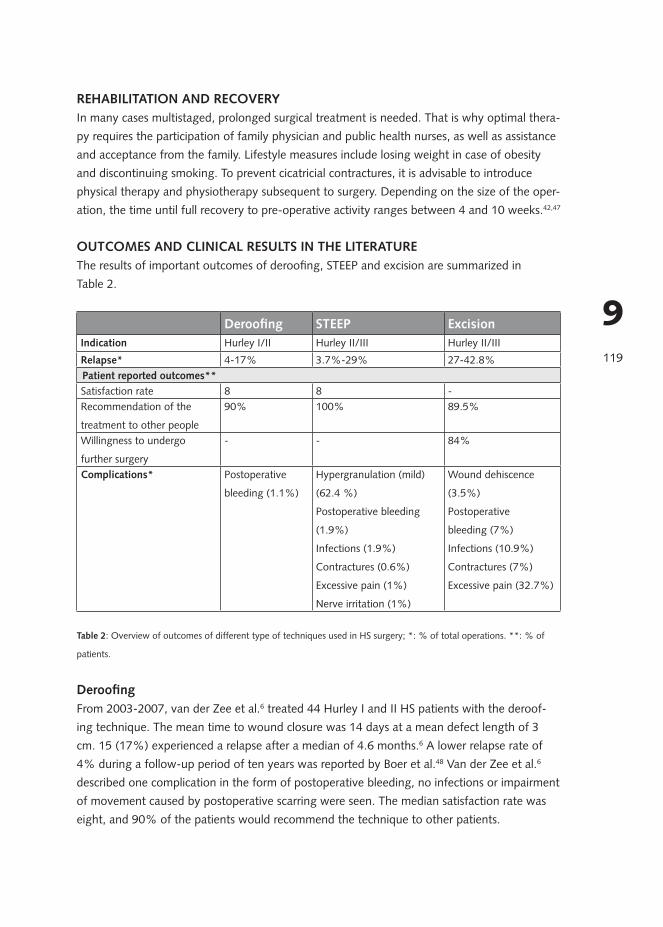
OUTCOMES AND CLINICAL RESULTS IN THE LITERATUREThe results of important outcomes of deroofing, STEEP and excision are summarized in Table 2.
Deroofing STEEP ExcisionIndication Hurley I/II Hurley II/III Hurley II/III
Relapse* 4-17% 3.7%-29% 27-42.8%Patient reported outcomes**Satisfaction rate 8 8 -Recommendation of the
treatment to other people
90% 100% 89.5%
Willingness to undergo
further surgery
- - 84%
Complications* Postoperative
bleeding (1.1%)
Hypergranulation (mild)
(62.4 %)
Postoperative bleeding
(1.9%)
Infections (1.9%)
Contractures (0.6%)
Excessive pain (1%)
Nerve irritation (1%)
Wound dehiscence
(3.5%)
Postoperative
bleeding (7%)
Infections (10.9%)
Contractures (7%)
Excessive pain (32.7%)
Table 2: Overview of outcomes of different type of techniques used in HS surgery; *: % of total operations. **: % of
patients.
DeroofingFrom 2003-2007, van der Zee et al.6 treated 44 Hurley I and II HS patients with the deroof-ing technique. The mean time to wound closure was 14 days at a mean defect length of 3 cm. 15 (17%) experienced a relapse after a median of 4.6 months.6 A lower relapse rate of 4% during a follow-up period of ten years was reported by Boer et al.48 Van der Zee et al.6 described one complication in the form of postoperative bleeding, no infections or impairment of movement caused by postoperative scarring were seen. The median satisfaction rate was eight, and 90% of the patients would recommend the technique to other patients.
120
9
STEEPIn a prospective case series the mean time to complete wound healing was 53 days with a median defect size of 15 cm2.42 The size of the wound and the Hurley stage were indepen-dent predictors for wound healing. A retrospective analysis on 363 deroofings and STEEPs under general anesthesia showed 34% natural progression and 29% relapses due to irradical surgery.8 The relapse rate was much lower in the prospective case series in which only one of the 27 operations sites relapsed. Hypergranulation is the most common complication. The hy-pergranulation is usually mild with good reaction to topical treatment with superpotent topical steroids. Wound infections, nerve irritation, post operative bleeding and stricture formation are seen very rarely.8 With a functional outcome of 8.7, a cosmetic outcome of 7.2 and 100% of the patients that would recommend STEEP to others, patients are generally satisfied with the STEEP procedure (Figure 4).
ExcisionThe relapse rate depends on the margin of the excision. After limited excision, the relapse rate is 42.8% with a disease free interval of 11 months. Wide excision has a relapse of 27% after 20 months.49 The time to wound closure after excision is 6.6 weeks (range 2–12 weeks) with a mean size of the wounds of 40.6 cm2.43 Bieniek et al.28 performed 229 operations among 182 patients. During the one-year follow-up period complete recovery was observed in 60% of the patients. 31.5% had new but less severe lesions in an adjacent area or at the site of the surgical intervention and 8.5% of the patients showed no improvement. The nature and frequency of complications were similar to those described by others with 7% postoperative bleeding, 10.9% infections, 7% contractures, 32.7% excessive pain and 3.5% wound dehis-cence. Overall, 84-89.5% of patients declared willingness to undergo further surgery in case of disease recurrence, and to recommend it to other patients, whereas about 9% would not choose the surgery again.28
Wound closure techniquesIt is believed that the relapse rate is primarily determined by the radicality of the excision and not by the wound closure technique.3,7 Conversely, the relapse rate after primary closure was found to be much higher (54% ) than the rates of split-thickness skin grafting (13%) or local flaps (19%).50,51 In SIH the relapse rate is low.25,52 SIH is preferred by patients over skin graft-ing because of shorter hospital stay and sick leave, less limitation of mobility after surgery, and better cosmetic results.25,53
Other factors influencing the risk of relapseWomen are at higher risk of relapses than men.8 Also, the location of HS influences the re-lapse rates. Inguinal, genital and submammary HS relapses more frequently than axillary and perianal HS.49,52
121
9
CONCLUSIONSSurgical treatment in HS should be carried out by dermatosurgeons who have thorough knowledge on the pathology of the disease and excellent surgical skills. At least in more se-vere stages of HS, surgery should be introduced early after setting the diagnosis. Because the great impairment of quality of life in HS, patients are often highly motivated to change their condition by means of surgery. Preoperatively, medical treatment to calm active inflammation and imaging must be considered. Depending on the extent and severity of the disease local, tumescent, spinal and/or general anaesthesia are used. Incision and drainage can relief pain in a setting of a tense, acute abscess. Deroofing is the primary surgical therapy for Hurley stage I/II. Until recently, wide excision was regarded as the preferred surgical method for Hurley stage II/III. The STEEP procedure seems to be a promising alternative to wide excision because it saves healthy tissue to a maximum and achieves complete removal of lesional tissue. After wide excision, different wound closure techniques can be chosen. Simple sutures can be used in small defects surrounded by loose skin. Split thickness skin grafts are employed typically in large wounds. Especially in genital and inguinal areas, flaps can be used successfully. However, the use of flap reconstruction, which is definitive by its nature, may not be appropriate to this disease with significant risk of progression. SIH ensures usually good functional and cosmetic results in defects up to 140 cm2. By using different techniques simultaneously, the benefits of the individual techniques can be combined.
122
9
REFERENCES1. Revuz JE, Jemec GB. Diagnosing Hidradenitis Suppurativa. Dermatol Clin 2016 Jan;34(1):1-5.
2. Weyandt G. Operative Therapie der Acne inversa. Hautarzt 2005;56:1033-1039.
3. Rompel R, Petres J. Long-term results of wide surgical excision in 106 patients with hidradenitis suppurativa. Derma-
tol Surg 2000 Jul;26(7):638-643.
4. Wolkenstein P, Loundou A, Barrau K, Auquier P, Revuz J, Quality of Life Group of the French Society of Derma-
tology. Quality of life impairment in hidradenitis suppurativa: a study of 61 cases. J Am Acad Dermatol 2007
Apr;56(4):621-623.
5. Deckers IE, Kimball AB. The Handicap of Hidradenitis Suppurativa. Dermatol Clin 2016 Jan;34(1):17-22.
6. van der Zee HH, Prens EP, Boer J. Deroofing: a tissue-saving surgical technique for the treatment of mild to moder-
ate hidradenitis suppurativa lesions. J Am Acad Dermatol 2010 Sep;63(3):475-480.
7. Kagan RJ, Yakuboff KP, Warner P, Warden GD. Surgical treatment of hidradenitis suppurativa: a 10-year experience.
Surgery 2005 Oct;138(4):734-40; discussion 740-1.
8. Blok JL, Boersma M, Terra JB, Spoo JR, Leeman FW, van den Heuvel ER, et al. Surgery under general anaesthesia in
severe hidradenitis suppurativa: a study of 363 primary operations in 113 patients. J Eur Acad Dermatol Venereol
2015 Jan 15.
9. Wortsman X. Imaging of Hidradenitis Suppurativa. Dermatol Clin 2016 Jan;34(1):59-68.
10. Zarchi K, Yazdanyar N, Yazdanyar S, Wortsman X, Jemec GB. Pain and inflammation in hidradenitis suppurativa
correspond to morphological changes identified by high-frequency ultrasound. J Eur Acad Dermatol Venereol 2015
Mar;29(3):527-532.
11. Church JM, Fazio VW, Lavery IC, Oakley JR, Milsom JW. The differential diagnosis and comorbidity of hidradenitis
suppurativa and perianal Crohn’s disease. Int J Colorectal Dis 1993 Sep;8(3):117-119.
12. Klein JA. Anesthetic formulation of tumescent solutions. Dermatol Clin 1999 Oct;17(4):751-9, v-vi.
13. Glowacka K, Orzechowska-Juzwenko K, Bieniek A, Wiela-Hojenska A, Hurkacz M. Optimization of lidocaine appli-
cation in tumescent local anesthesia. Pharmacol Rep 2009 Jul-Aug;61(4):641-653.
14. Namias A, Kaplan B. Tumescent anesthesia for dermatologic surgery. Cosmetic and noncosmetic procedures. Derma-
tol Surg 1998 Jul;24(7):755-758.
15. Ellis LZ. Hidradenitis suppurativa: surgical and other management techniques. Dermatol Surg 2012 Apr;38(4):517-
536.
16. MULLINS JF, MCCASH WB, BOUDREAU RF. Treatment of chronic hidradenitis suppurativa: surgical modification.
Postgrad Med 1959 Dec;26:805-808.
17. Brown SC, Kazzazi N, Lord PH. Surgical treatment of perineal hidradenitis suppurativa with special reference to
recognition of the perianal form. Br J Surg 1986 Dec;73(12):978-980.
18. Culp CE. Chronic hidradenitis suppurativa of the anal canal. A surgical skin disease. Dis Colon Rectum 1983
Oct;26(10):669-676.
19. van Hattem S, Spoo JR, Horvath B, Jonkman MF, Leeman FW. Surgical treatment of sinuses by deroofing in hidrade-
nitis suppurativa. Dermatol Surg 2012 Mar;38(3):494-497.
20. Blok JL, Spoo JR, Leeman FW, Jonkman MF, Horvath B. Skin-Tissue-sparing Excision with Electrosurgical Peeling
(STEEP): a surgical treatment option for severe hidradenitis suppurativa Hurley stage II/III. J Eur Acad Dermatol
Venereol 2015 Feb;29(2):379-382.
123
9
21. GREELEY PW. Plastic surgical treatment of chronic suppurative hidradenitis. Plast Reconstr Surg (1946) 1951
Feb;7(2):143-146.
22. Stein A, Sebastian G. Acne inversa. Hautarzt 2003 Feb;54(2):173-85; quiz 186-7.
23. Pollock WJ, Virnelli FR, Ryan RF. Axillary hidradenitis suppurativa. A simple and effective surgical technique. Plast
Reconstr Surg 1972 Jan;49(1):22-27.
24. Ramasastry SS, Conklin WT, Granick MS, Futrell JW. Surgical management of massive perianal hidradenitis suppura-
tiva. Ann Plast Surg 1985 Sep;15(3):218-223.
25. Morgan WP, Harding KG, Hughes LE. A comparison of skin grafting and healing by granulation, following axillary
excision for hidradenitis suppurativa. Ann R Coll Surg Engl 1983 Jul;65(4):235-236.
26. Morgan WP, Harding KG, Richardson G, Hughes LE. The use of silastic foam dressing in the treatment of advanced
hidradenitis suppurativa. Br J Surg 1980 Apr;67(4):277-280.
27. Greenbaum AR. Modified abdominoplasty as a functional reconstruction for recurrent hydradenitis suppurativa of
the lower abdomen and groin. Plast Reconstr Surg 2007 Feb;119(2):764-766.
28. Bieniek A, Matusiak L, Okulewicz-Gojlik D, Szepietowski JC. Surgical treatment of hidradenitis suppurativa: experi-
ences and recommendations. Dermatol Surg 2010 Dec;36(12):1998-2004.
29. Rieger UM, Erba P, Pierer G, Kalbermatten DF. Hidradenitis suppurativa of the groin treated by radical excision and
defect closure by medial thigh lift: aesthetic surgery meets reconstructive surgery. J Plast Reconstr Aesthet Surg 2009
Oct;62(10):1355-1360.
30. Hudson D, Krige S. Axillary hidradenitis suppurativa – wide excision and flap coverage is best. Eur J Plast Surg
1993(16):94-97.
31. Geh JL, Niranjan NS. Perforator-based fasciocutaneous island flaps for the reconstruction of axillary defects follow-
ing excision of hidradenitis suppurativa. Br J Plast Surg 2002 Mar;55(2):124-128.
32. Chuang CJ, Lee CH, Chen TM, Wang HJ, Chen SG. Use of a versatile transpositional flap in the surgical treatment of
axillary hidradenitis suppurativa. J Formos Med Assoc 2004 Aug;103(8):644-647.
33. Schwabegger AH, Herczeg E, Piza H. The lateral thoracic fasciocutaneous island flap for treatment of recurrent
hidradenitis axillaris suppurativa and other axillary skin defects. Br J Plast Surg 2000 Dec;53(8):676-678.
34. Varkarakis G, Daniels J, Coker K, Oswald T, Akdemir O, Lineaweaver WC. Treatment of axillary hidradenitis with
transposition flaps: a 6-year experience. Ann Plast Surg 2010 May;64(5):592-594.
35. Rehman N, Kannan RY, Hassan S, Hart NB. Thoracodorsal artery perforator (TAP) type I V-Y advancement flap in
axillary hidradenitis suppurativa. Br J Plast Surg 2005 Jun;58(4):441-444.
36. Blanc D, Tropet Y, Balmat P. Surgical treatment of suppurative axillary hidradenitis: value of a musculocutaneous
island flap of the latissimus dorsi. Apropos of 3 cases. Ann Dermatol Venereol 1990;117(4):277-281.
37. Alharbi Z, Kauczok J, Pallua N. A review of wide surgical excision of hidradenitis suppurativa. BMC Dermatol 2012
Jun 26;12:9-5945-12-9.
38. Rees L, Moses M, Clibbon J. The anterolateral thigh (ALT) flap in reconstruction following radical excision of groin
and vulval hidradenitis suppurativa. J Plast Reconstr Aesthet Surg 2007;60(12):1363-1365.
39. Solanki NS, Roshan A, Malata CM. Pedicled gracilis myocutaneous flap for treatment of recalcitrant hidradenitis
suppurativa of the groin and perineum. J Wound Care 2009 Mar;18(3):111-112.
40. Kishi K, Nakajima H, Imanishi N. Reconstruction of skin defects after resection of severe gluteal hidradenitis suppu-
rativa with fasciocutaneous flaps. J Plast Reconstr Aesthet Surg 2009 Jun;62(6):800-805.
124
9
41. Unal C, Yirmibesoglu OA, Ozdemir J, Hasdemir M. Superior and inferior gluteal artery perforator flaps in reconstruc-
tion of gluteal and perianal/perineal hidradenitis suppurativa lesions. Microsurgery 2011 Oct;31(7):539-544.
42. Janse IC, Hellinga J, Blok JL, van den Heuvel ER, Spoo JR, Jonkman MF, et al. Skin-Tissue-sparing Excision with
Electrosurgical Peeling: A Case Series in Hidradenitis Suppurativa. Acta Derm Venereol 2015 Oct 14.
43. Bieniek A, Matusiak L, Chlebicka I, Szepietowski JC. Secondary intention healing in skin surgery: our own experience
and expanded indications in hidradenitis suppurativa, rhinophyma and non-melanoma skin cancers. J Eur Acad
Dermatol Venereol 2013 Aug;27(8):1015-1021.
44. Miller IM, McAndrew RJ, Hamzavi I. Prevalence, Risk Factors, and Comorbidities of Hidradenitis Suppurativa. Der-
matol Clin 2016 Jan;34(1):7-16.
45. Blackburn JH,2nd, Boemi L, Hall WW, Jeffords K, Hauck RM, Banducci DR, et al. Negative-pressure dressings as a
bolster for skin grafts. Ann Plast Surg 1998 May;40(5):453-457.
46. Elwood ET, Bolitho DG. Negative-pressure dressings in the treatment of hidradenitis suppurativa. Ann Plast Surg
2001 Jan;46(1):49-51.
47. Wormald JC, Balzano A, Clibbon JJ, Figus A. Surgical treatment of severe hidradenitis suppurativa of the axilla: tho-
racodorsal artery perforator (TDAP) flap versus split skin graft. J Plast Reconstr Aesthet Surg 2014 Aug;67(8):1118-
1124.
48. Boer J, Bos W, van der Meer B. Hidradenitis suppurativa (acne inversa): behandeling met deroofing en resorcine.
Ned Tijdschr DermatolVenereol 1994;4:101-103.
49. Ritz JP, Runkel N, Haier J, Buhr HJ. Extent of surgery and recurrence rate of hidradenitis suppurativa. Int J Colorectal
Dis 1998;13(4):164-168.
50. Watson JD. Hidradenitis suppurativa--a clinical review. Br J Plast Surg 1985 Oct;38(4):567-569.
51. Mandal A, Watson J. Experience with different treatment modules in hidradenitis suppuritiva: a study of 106 cases.
Surgeon 2005 Feb;3(1):23-26.
52. Harrison BJ, Mudge M, Hughes LE. Recurrence after surgical treatment of hidradenitis suppurativa. Br Med J (Clin
Res Ed) 1987 Feb 21;294(6570):487-489.
53. Meixner D, Schneider S, Krause M, Sterry W. Acne inversa. J Dtsch Dermatol Ges 2008 Mar;6(3):189-196.
125
9
126
9