ultrasound quiz
TRANSCRIPT
ULTRASOUND QUIZ
DEPARTMENT OF RADIOLOGYGOVT.MEDICAL COLLEGE
AURANGABAD
DR G J KHADSE PROFF.AND HEAD
DR ANJALI KULKARNI - WASADIKAR
DR VARSHA ROTE – KAGINALKAR
DR VARSHA DESHMUKH
20 year female.
H/o 1 ½ months amenorrhoea.
C/o bleeding p/v-painless.

CLUE
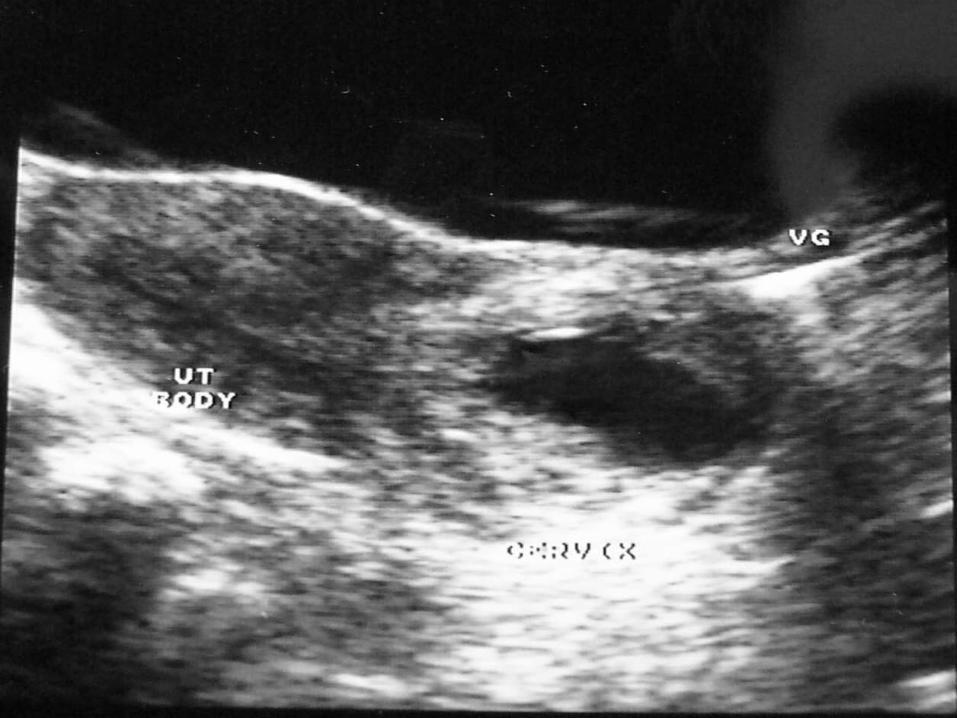
♦Painless bleeding ♦Normal Uterus & endothelial thickness
DIAGNOSIS
♦CERVICAL ECTOPIC PREGNANCY
DIFFERENTIAL DIAGNOSIS
♦Incomplete abortion♦Cervical cyst
DISCUSSION
♦Distension and thinning of cervix♦Decidual reaction ♦Painless bleeding ♦Uterus : Normal with normal
endothelial thickness
HISTORY
♦30 year female ♦C/o pain in right iliac fossa♦Clinical diagnosis: Acute
Appendicitis

CLUE
♦Rapid enlargement ♦Acute presentation ♦No flow on doppler
DIAGNOSIS
♦TORSION OF RIGHT OVARY
DIFFERENTIAL DIAGNOSIS
♦Hemorrhagic ovarian cyst♦PCOD♦PID♦Autoimmune oophoritis
DISCUSSION
♦Acute presentation♦Peripheral small follicular cysts♦Solid appearance ♦Size more than 5 cm ♦Frequently seen on right side.
(3:2)

HISTORY
♦30 years female♦Menorrhagia

CLUE
♦SPOT DIAGNOSIS
DIAGNOSIS
♦ENDOMETRIAL HYPERPLASIA
DIFFERENTIAL DIAGNOSIS
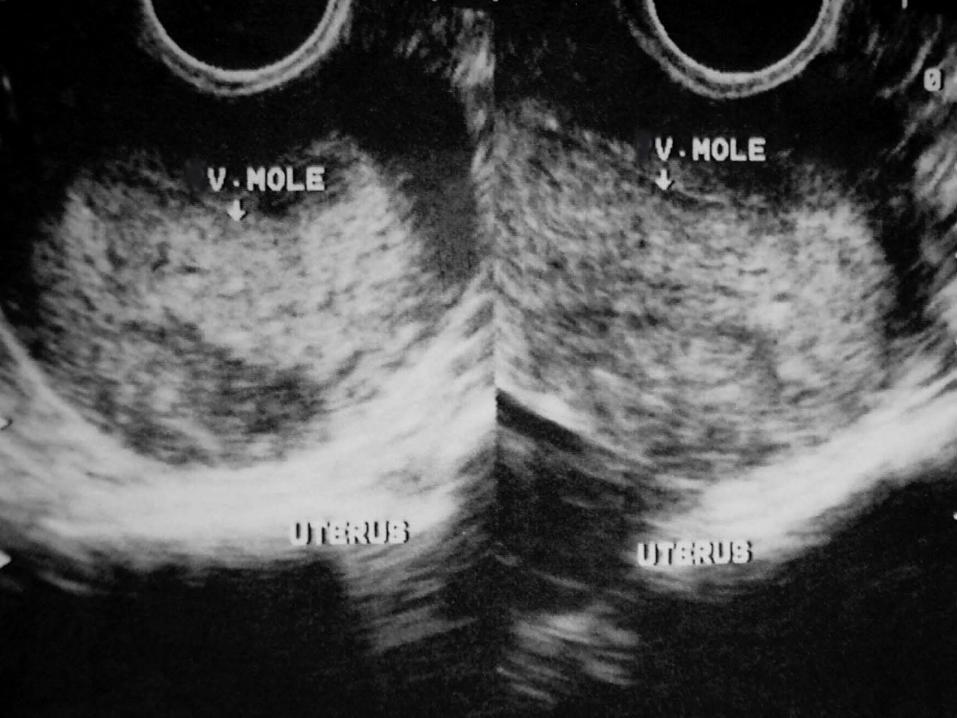
♦Polyp ♦Vesicular mole♦Incomplete abortion♦Carcinoma of endometrium
COMMENTS
♦Normal endometrium measures between 4 to 14 mm.

HISTORY
♦35 years female ♦Lower abdominal pain ♦Menorrhagia
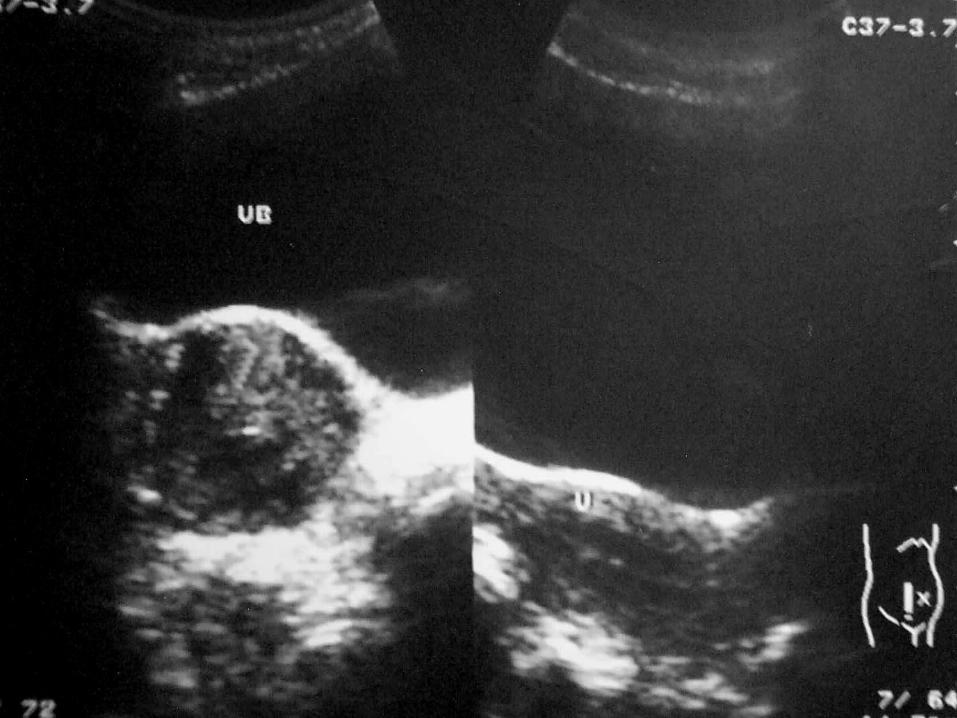
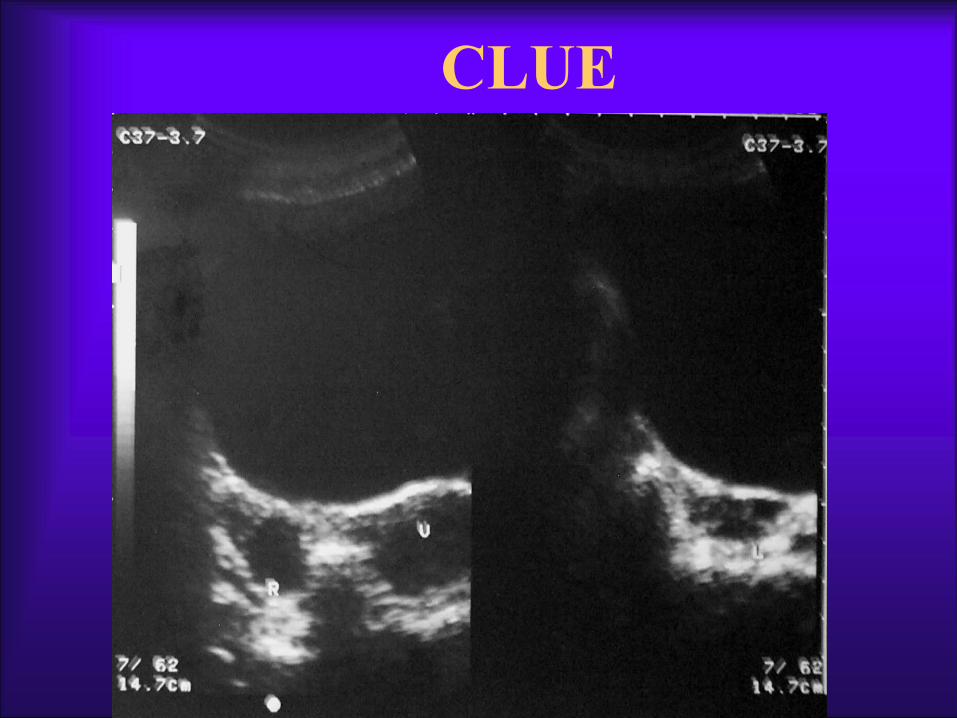
CLUE

DIAGNOSIS
♦BROAD LIGAMENT FIBROID
DIFFERENTIAL DIAGNOSIS
♦Solid ovarian mass♦Tubo-ovarian mass
DISCUSSION
♦Solid mass ♦Cystic degeneration♦E/o increased through transmission
HISTORY
♦25 years female with BOH
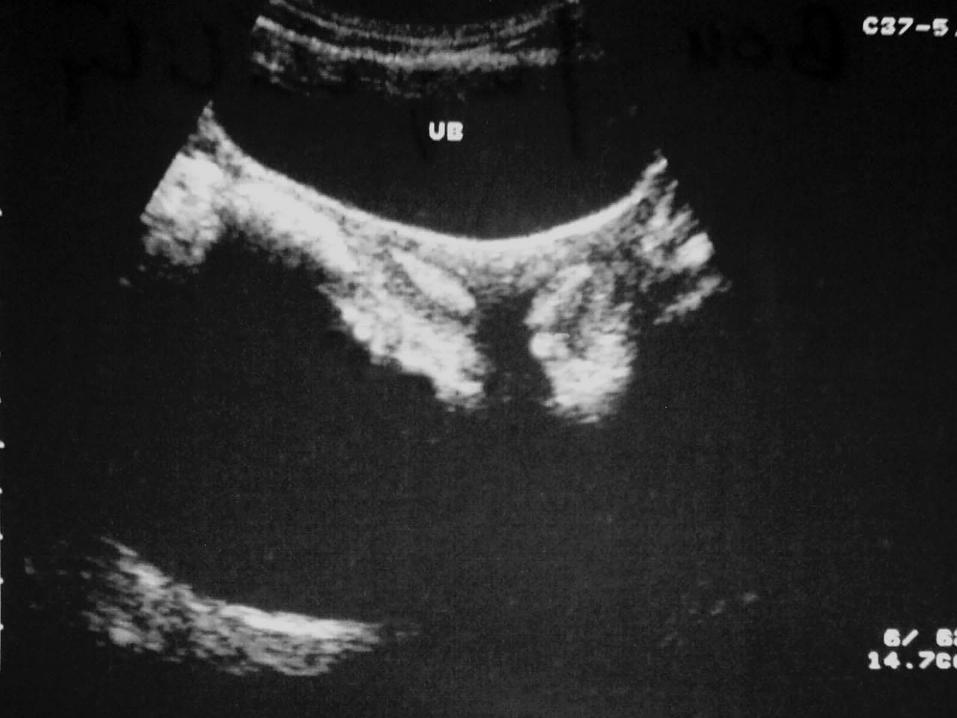
CLUE
♦Congenital anomaly
DIAGNOSIS
♦BICORNUATE UTERUS
DIFFERENTIAL DIAGNOSIS
♦Uterus didelphys-rare ♦Septate uterus
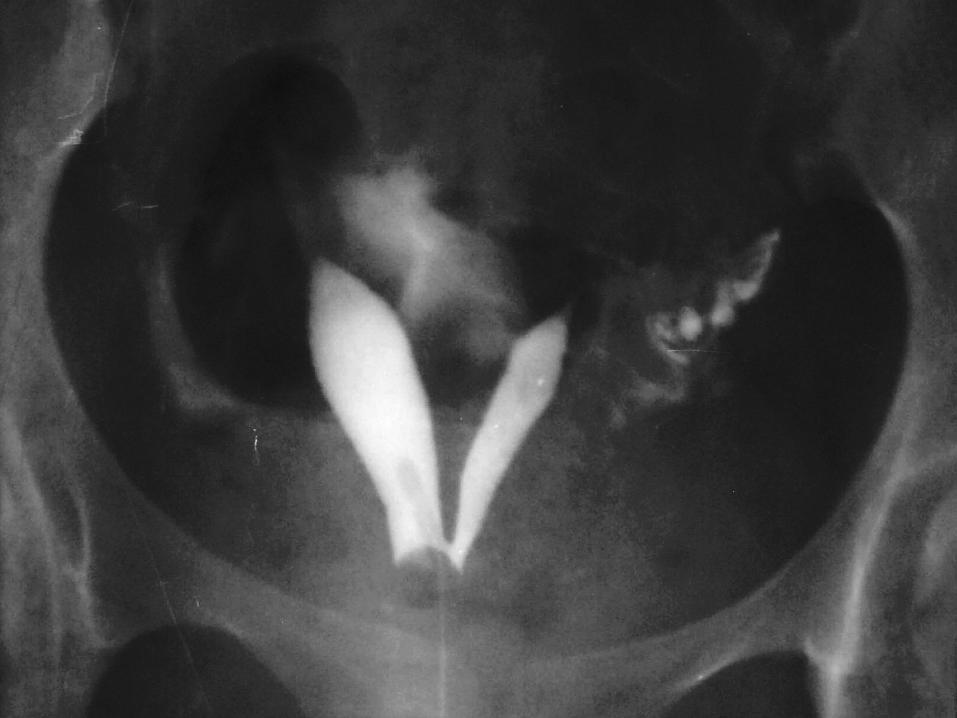


DISCUSSION
♦Deep fundal notch ♦Better seen in secretary phase♦Single cervix♦Separate myometrial covering for
each endometrial cavity
HISTORY
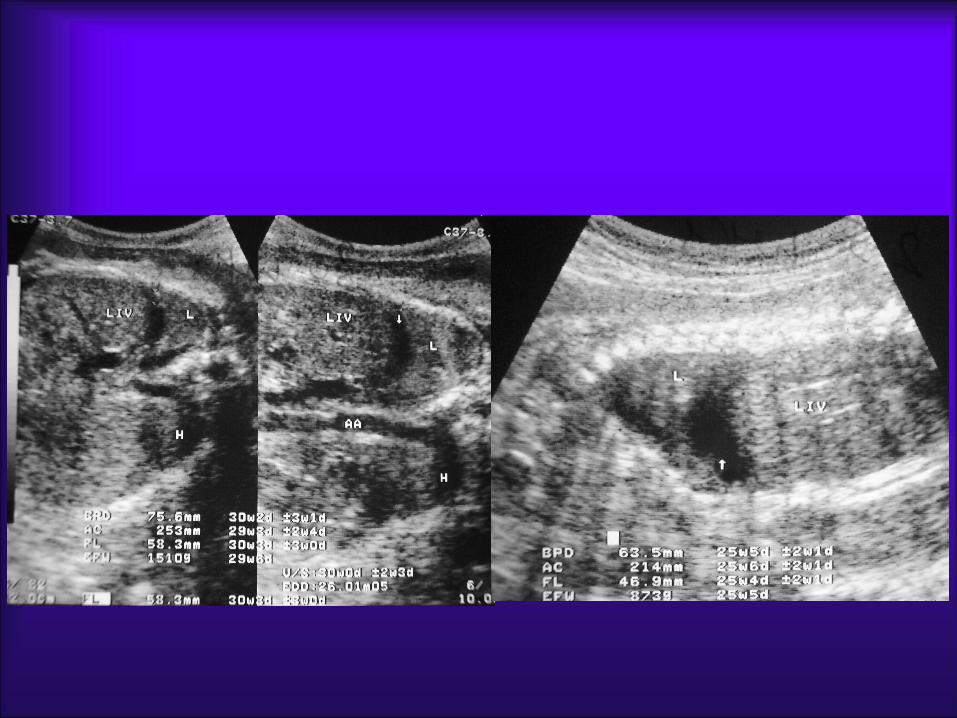
♦Young females of with 25 and 30 weeks gestation
♦Normal scan
EXCEPT
We thank u for active participation in the quiz.
Hope u have enjoyed stay in Aurangbad
CLUE
♦Isolated congenital anomaly
DIAGNOSIS
♦UNILATERAL FETAL PLEURAL EFFUSION
DIFFERENTIAL DIAGNOSIS
♦Pseudo-ascitis
DISCUSSION
♦Prognostic indicators
–Size - small is better
–Mediastinal shift - less is better
–Hydrops – none is best


HISTORY
♦30 years female ♦8 months amenorrhoea ♦Polyhydramnios

CLUE
♦Open neural tube defect
DIAGNOSIS
♦OCCIPITAL ENCEPHALOCELE
DIFFERENTIAL DIAGNOSIS
♦Cystic hygroma ♦Scalp oedema ♦Teratoma – nasal
DISCUSSION
♦Herniation of meninges or/& brain tissue through the defect in bony calvarium
♦Site: occipital region ♦Open neural tube defect
HISTORY
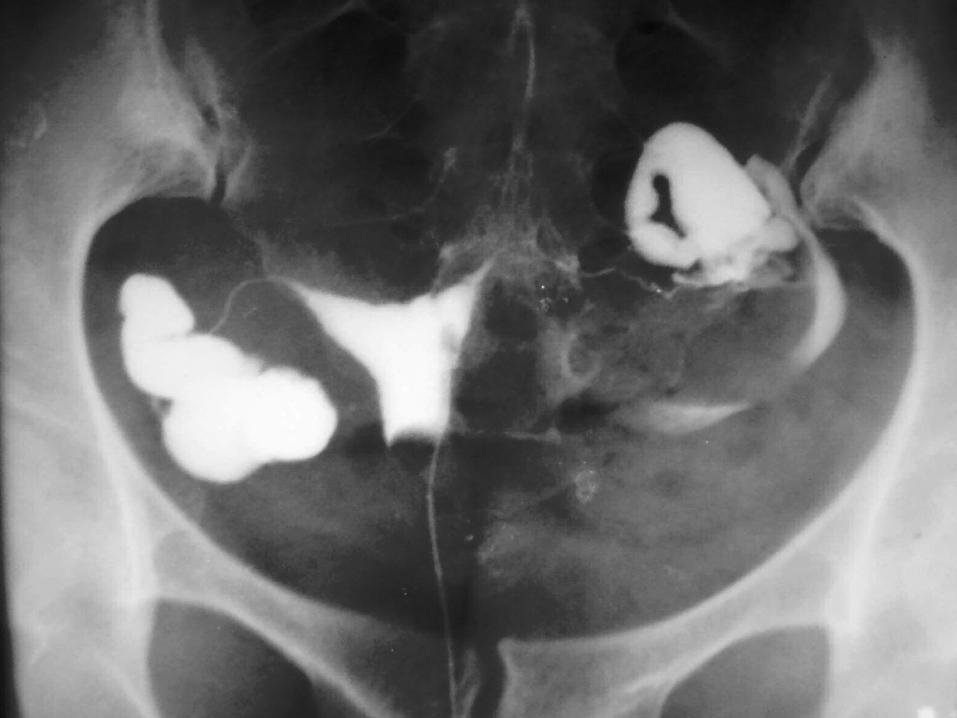
♦32 Years female ♦Married since 15 years ♦H/o IUD 12 years back ♦Infertility since then
CLUE
♦Chronic lower abdominal pain
DIAGNOSIS
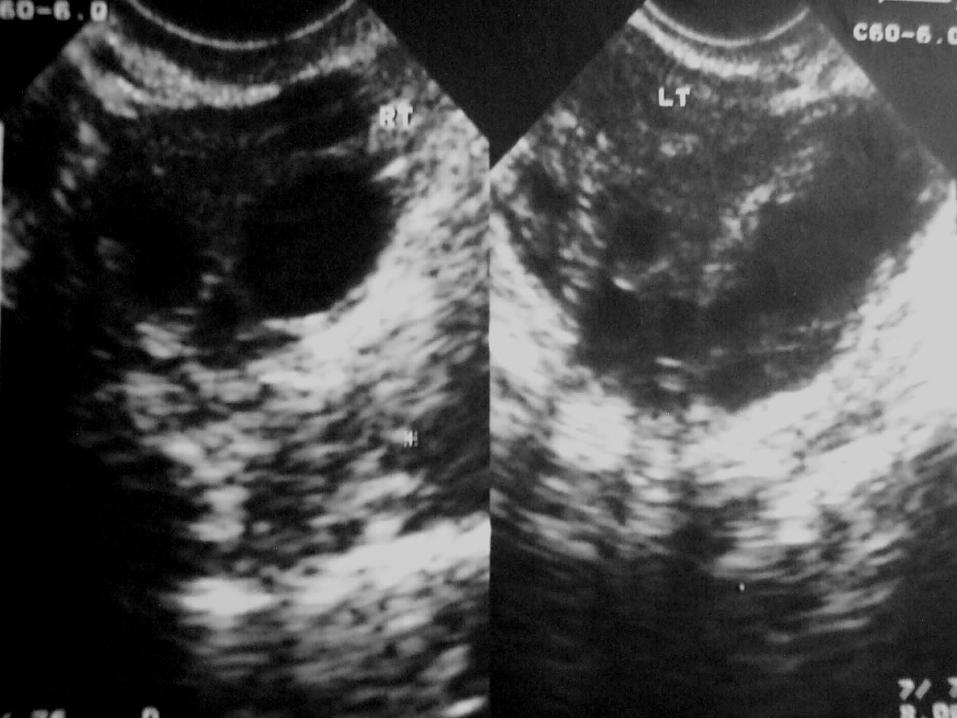
♦BILATERAL HYDROSALPINX

DIFFERENTIAL DIAGNOSIS
♦Multiloculated ovarian cyst ♦Fluid filled bowel ♦Pelvic veins
DISCUSSION
♦Normal tube measurement 1-4 mm
♦Dilatation s/o chronic infection
HISTORY
♦21 years female ♦6 months amenorrhoea for routine
USG♦Polyhydramnios ♦Both parents are of normal stature

OBSERVATIONS
♦All limbs are short – length reduction less than 2.5 percentile
♦No corresponding interval growth♦Thoracic circumference less than 2.5
percentile

DIAGNOSIS
♦ MUSCULOSKELETAL DYSPLASIA –LETHAL
♦ THANATOPHORIC DWARFISM

DIFFERENTIAL DIAGNOSIS
♦Severe IUGR♦Homozygous achondroplasia ♦Achondrogenesis ♦Osteogenesis imperfecta
MESSAGE
♦Femur length is the single and most helpful parameter in identification of most of short limb lethal dysplasias
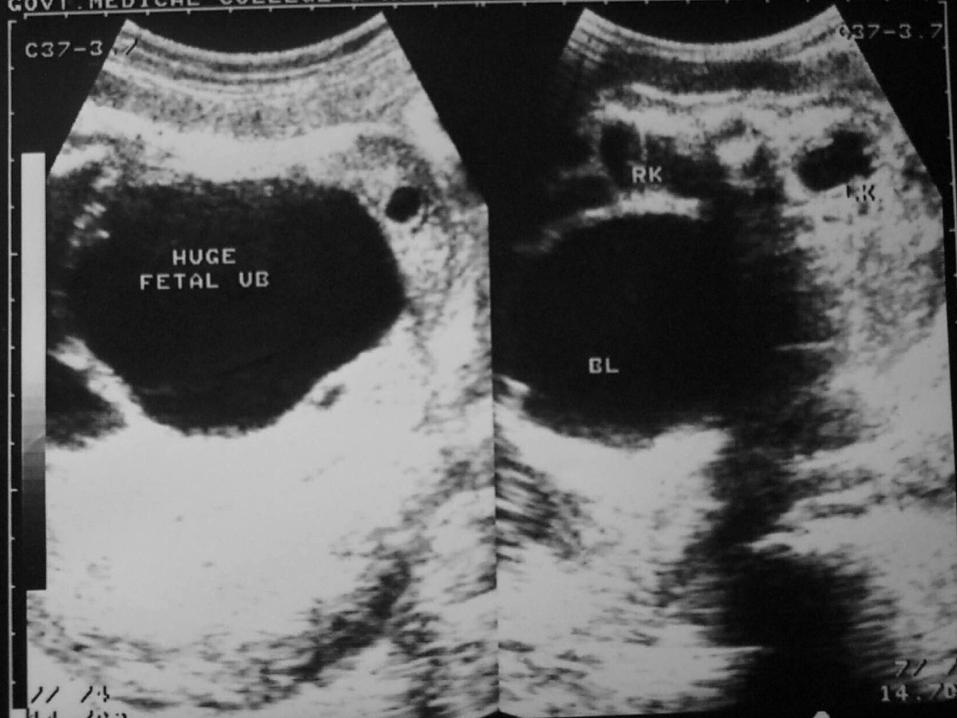
HISTORY
♦26 weeks gestation in a young female♦Oligo to anhydramnios

CLUE
♦Congenital anomaly only seen in male
DIAGNOSIS
♦BLADDER OUTLET OBSTRUCTION-POSTERIOR URETHRAL VALVES
DIFFERENTIAL DIAGNOSIS
♦Urethral atresia
DISUSSION
♦Associated renal dysplasia
HISTORY
♦26 years primigravida ♦Oligo to anhydramnios♦20 weeks of gestation

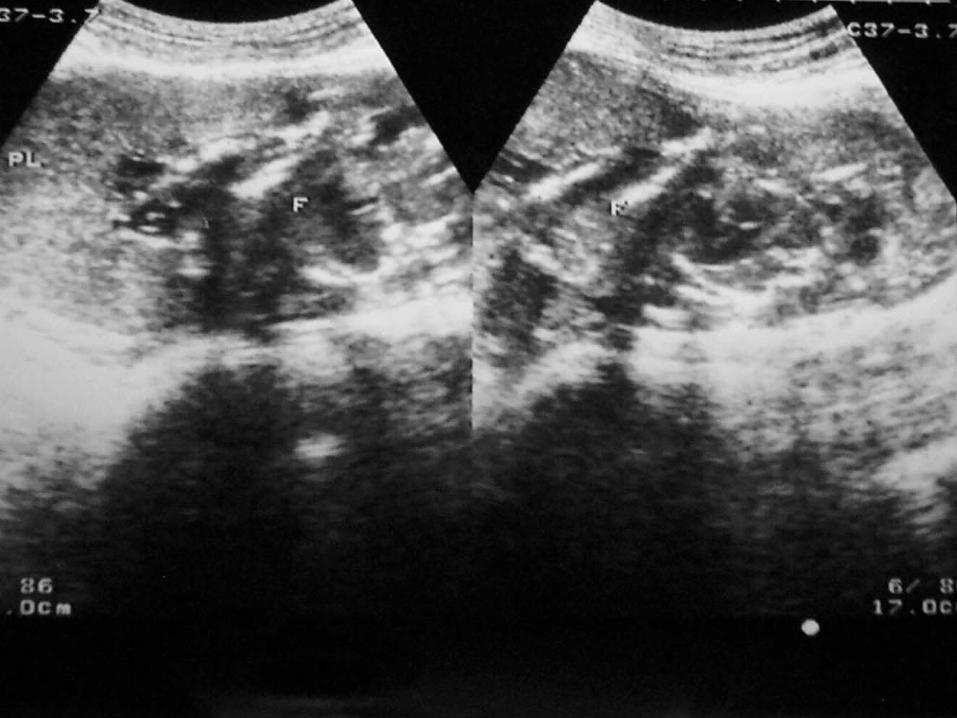

CLUE
♦E/O amniotic fluid in first trimester
♦Anhydramnios at present
DIAGNOSIS
♦B R A(BILATERAL RENAL ATRESIA)
DIFFERENTIAL DIAGNOSIS
♦Severe IUGR♦Bilateral renal dysplasia
COMMENTS
♦ Classical triad – Severe oligohydramnios – Persistent nonvisualization of urinary bladder – Renal nonvisualization
♦ Associations – Potters facies – Pulmonary hypoplasia – Limb deformities – Familial recurrence in 3 to 5%