ultrasound diagnosis in vasoproliferative tumours of the ocular fundus
TRANSCRIPT
a r c h s o c e s p o f t a l m o l . 2 0 1 1;8 6(8):247–253
ARCHIVOS DE LA SOCIEDADESPAÑOLA DE OFTALMOLOGÍA
O
Uo
A
Ud
a
A
R
A
A
K
M
I
V
O
P
M
T
T
E
O
2
www .e lsev ier .es /o f ta lmologia
riginal article
ltrasound diagnosis in vasoproliferative tumours of thecular fundus�
. Pineiro-Ces ∗, M.J. Blanco-Teijeiro, M.P. Mera-Yánez, C. Capeans-Tome
nidad de Retina Quirúrgica y Oncología Ocular, Servicio de Oftalmología, Complejo Hospitalario Universitario de Santiago, Santiagoe Compostela, Spain
r t i c l e i n f o
rticle history:
eceived 1 November 2010
ccepted 4 April 2011
vailable online 21 December 2011
eywords:
elanoma
ntraocular tumor
asoproliferative tumor
cular ultrasound
a b s t r a c t
Objective: The aim of this work is to describe the ultrasound features in vasoproliferative
tumors of the ocular fundus (VPTOF).
Methods: The medical records corresponding to eight patients were retrospectively studied.
Clinical data from the complete ophthalmologic examination and ultrasonographic findings
were analyzed.
Results: Nodular masses affecting either the retina or both the retina and the choroid were
found. The surface contour of the tumor was regular in 5, and irregular in 3 cases. In terms
of dimensions (mm/SD), the average major base was 7.14/2.56; the minor base was 6.74/2.48
and the height was 2.38/1.26. Internal structure was always solid and irregular, and reflec-
tivity was mostly medium–high in 6 eyes. Angle kappa was not present in any case. No
vascularity signs were detected.
Conclusion: According to the results it is suggested that when a differential diagnosis of
VPTOF is carried out, not only should ophthalmoscopic signs be studied, but an ultrasound
examination should also be done.© 2010 Sociedad Española de Oftalmología. Published by Elsevier España, S.L. All rights
reserved.
Diagnóstico ecográfico de los tumores vasoproliferativos del fondo de ojo
alabras clave:
elanoma
umor intraocular
r e s u m e n
Objetivo: Describir las características ecográficas en los tumores vasoproliferativos del fondo
de ojo (TVPFO).
Métodos: Se estudiaron retrospectivamente las historias clínicas correspondientes a
umor vasoprolifrativocografía ocular8 pacientes afectados de TVPFO. Se analizaron los datos correspondientes a la exploración
oftalmológica completa y a la exploración ecográfica.
Resultados: Se encontraron masas nodulares afectando a la retina o bien a la retina y la
coroides. La superficie tumoral era regular en 5 casos e irregular en los 3 restantes. La
media de las dimensiones fue (mm/DE): base mayor, 7,14/2,56; base menor, 6,74/2,48 y altura
� Please cite this article as: Pineiro-Ces A, et al. Diagnóstico ecográfico de los tumores vasoproliferativos del fondo de ojo. Arch Soc Espftalmol. 2011;86:247–53.∗ Corresponding author.
E-mail address: [email protected] (A. Pineiro-Ces).
173-5794/$ – see front matter © 2010 Sociedad Española de Oftalmología. Published by Elsevier España, S.L. All rights reserved.

248 a r c h s o c e s p o f t a l m o l . 2 0 1 1;8 6(8):247–253
2,38/1,26. La estructura interna fue siempre sólida e irregular y la reflectividad era media-alta
en 6 casos. No se detectó ni ángulo kappa ni vascularidad interna en ningún caso.
Conclusión: De acuerdo con los resultados obtenidos se propone que tanto el diagnóstico
como el diagnóstico diferencial de los TVPFO deben ser llevados a cabo no solo con la
oftalmoscopia sino también con la exploración ecográfica.
© 2010 Sociedad Española de Oftalmología. Publicado por Elsevier España, S.L. Todos los
Introduction
Ocular fundus vasoproliferative tumors (OFVPT) are benignchorioretinal lesions of undetermined etiology. Isolated casesor short series of this entity have been published underdifferent denominations: angioma-like masses,1 presumablyacquired retinal hemangioma,2 hemangioma-like masses,3
massive retinal glyosis,4 all of which probably describe thesame ocular disease. In 1995 Shields et al.5 published a longseries and for the first time applied the term “ocular fundusvasoproliferative tumors”.
In most cases, OFVPT affect healthy individuals between 40and 60, regardless of sex. Generally, OFVPT are nodular tumorsexhibiting uneven surface in ocular fundus exploration anda high degree of vascularization which is easily detectablein ophthalmoscopy and exhibiting reddish-yellowish colorswhich vary from one case to another. OFVPT are generallylocated anterior to the equator and predominantly in thelower temporal quadrant.6,7 In general, OFVPT are associatedto exudative and hemorrhagic changes or epiretinal growthswhich end up affecting the macular area giving rise to its mainsymptom which is diminished visual acuity.
OFVPT has been described as associated with other ocu-lar diseases such as uveitis (pars planitis, toxoplasmosis andhistoplasmosis), cup-shaped cell retinopathy, pigments retini-tis, retinopathy of prematurity and Coats disease.5 However,in most cases (about 75%) no associations with other diseaseshave been found.7
In pathologic anatomy study, the said tumors have beenclassified as benign lesions characterized by reactive glyalproliferations with variable degrees of glyosis and vascularproliferation. In addition, literature reports thin capillary net-works and dilated and hyalinized vessels, some occluded, aswell as exudates, macrophages and foreign body-like giantcells.6,8,9 Accordingly, the histopathology of these tumors doesnot truly indicate a vasoproliferative tumor. For this reason,the term reactive retinal ganglioangiosis has been suggested.9
Even though the natural course of OFVPT is not pre-dictable, various treatments have been proposed. Someauthors suggest radiotherapy10 while other interventions suchas laser photocoagulation, cryotherapy,11 photodynamic ther-apy (PDT),12,13 intraocular injection of antiangiogenic agents14
and surgical resection9 have been also tried with variousdegrees of success.
Although OFVPT are non-malign lesions because nometastatic potential or malign proliferation has been
described, it is very important to carry out an adequate dif-ferential diagnostic. On the one hand, tumor entities involvedin the posterior segment of the eye, such as malign melanomaor choroidal metastasis, must be excluded. On the other hand,derechos reservados.
the possibility of benign entities such as choroidal heman-gioma must also be considered. Accordingly, ophthalmoscopyis a crucial technique when performed by an ocular oncol-ogy expert. Echography has been utilized as a supplementarytechnique in the majority of published cases. However, noin-depth studies have been performed to date to analyze itsactual contribution to diagnosis and differential diagnostic ofthese tumors.
Subjects, material and methods
Eight eyes of 8 patients (4 female and 4 male) with OFVPTwho were referred to the Ocular Oncology Unit of the Santiagode Compostela hospital complex were retrospectively stud-ied. The patients included in this study were consecutivelyselected between January 1999 and February 2009.
In all cases, anamnesis was performed together with acomprehensive ophthalmological exploration including visualacuity, intraocular pressure, anterior segment study andocular fundus ophthalmoscopy with photographic documen-tation and fluorescein angiography in all cases. The ecographicstudy was performed with the I3-ABD system (10 MHz probefor posterior segment echography and 8 MHz probe for stan-dardized echography, Innovative Imaging Inc., CA, USA). Theprobes were utilized directly over the ocular globe after theadministration of 2 drops of topical anesthesia.
The ecographic findings considered for this study matchedthe first exploration carried out in each patient before follow-up or application of treatment. The relevant ecographicparameters were studied by means of quantitative and kinetictopographic echography, which was always carried out by thesame physician (Antonio Pineiro-Ces). In order to avoid los-ing kinetic echography information, the findings derived fromthis echography were recorded on video and immediatelyreported by the explorer. The relevant ecographic param-eters were those utilized for the diagnostic and follow-upof other intraocular tumors such as choroidal melanoma.Accordingly, the following parameters were considered: massmorphology, superficial contour, dimensions, location, exis-tence of associated retinal detachment, kappa angle, choroidalcup and vitreous gel condition (posterior hyaloids detach-ment or inflammatory infiltration and/or hemorrhage). Theexact location of the tumor was obtained by means of longi-tudinal, transversal and axial B echographies. On the otherhand, in all cases an exhaustive study of the integrity ofthe tumoral base was carried out as well as an estimation
15
of its size by means of standardized echography A and B.Mode A echography was carried out with probe A and thevector associated to echography in mode B. The internal struc-ture, reflectiveness and presence of Kappa angle were studied
a r c h s o c e s p o f t a l m o l . 2 0 1 1;8 6(8):247–253 249
Table 1 – Clinical findings of ocular fundus vasoproliferative tumors.
Case Sex Age Eye BCVA Ocular diseaseassociated to uveitis
Referencediagnostic
Macularinvolvement
Treatment
1 F 22 R FC AM CME + E 125I2 M 67 R 0.5 Retinopathy of prematurity AM E Observation3 F 52 L 1.0 AM – Observation4 F 56 R 0.05 Coats disease CM CME + E Observation5 F 43 L 0.05 AM E Observation6 M 21 L 0.05 Magnus myopia H E Observation7 M 43 R 1.0 AM – Observation8 M 65 R 0.15 Retina detachment H E Observation
BCVA: best corrected visual acuity; FC: finger counting; R: right; E: exudation; CME: cystoid macular edema; H: hemangioma; L: left; 125I:brachytherapy with I125; F: female; AM: atypical melanoma; CM: choroidal metastasis; M: male.
ielceiu
R
Ttaia
Fn
n a detailed quantitative echography. The reflectiveness ofach mass was included in one of the following categories:ow, medium or high, depending on the height of peaksompared with the initial echogram peak. The quantitativecho technique was performed utilizing the tissue sensitiv-ty setting.15 Finally, internal vascularity signs were analyzedtilizing kinetic echography techniques.
esults
he clinical records of 4 females and 4 males were retrospec-
ively studied. The subject ages were comprised between 21nd 67 (mean: 46.12). Five of these patients exhibited OFVPTn the right eye and 3 in the left eye. The best corrected visualcuity in the affected eye ranged between finger counting andig. 1 – Retinographies corresponding to cases 1–4 (identified in
odular lesions with irregular contour and yellowish-reddish co
1.0. The follow-up of these patients ranged between 6 and85 months.
All cases had been referred to the Ocular Oncology Unitof the Santiago de Compostela hospital complex with the fol-lowing reference diagnostics: atypical choroidal melanoma (5cases), choroidal hemangioma (2 cases), and choroidal metas-tasic carcinoma (one case). The final diagnostic of all thepatients was carried out utilizing a combination of ophthal-moscopy and echography, without any case requiring biopsyfor diagnostic confirmation.
It was decided to treat case 1 with brachytherapy with 125Iin an attempt to improve the macular changes experienced bythe patient (Table 1). The remainder of patients were assessed
regularly. To date, no enucleation was necessary.In addition, 5 of the 8 patients had ocular disease histories:retinopathy of prematurity (one case), uveitis (one case), Coatsdisease (one case) and myopia magnus (one case) (Table 1).
the upper left corner). It can be seen how OFVPT areloring.
250 a r c h s o c e s p o f t a l m o l
Tabl
e
2
–
Ecog
rap
hic
char
acte
rist
ics.
Cas
eTo
pog
rap
hic
ech
ogra
ph
yQ
uan
tita
tive
ech
ogra
ph
yK
inet
ic
ech
ogra
ph
y
Mor
ph
olog
yLo
cali
zati
onSu
rfac
eco
nto
ur
Dim
ensi
ons
(Lb
×sb
×H
) mm
Ret
ina
det
ach
men
tD
VP
Stru
ctu
reR
eflec
tive
nes
sK
app
aan
gle
Vas
cula
rity
sign
s
1N
ITI
3.1
×3
×3
Yes
No
IM
H–
–2
NIT
R6.
87
×5.
99
×3.
2N
oY
esI
L–
–3
NIT
R5.
03
×5.
87
×1.
47N
oN
oI
MH
––
4N
ITI
11.6
5
×10
.19
×1.
7N
oY
esI
MH
––
5N
ITI
6.48
×6.
60
×2.
7Y
esY
esI
L–
–6
NIT
R7.
08
×7.
44
×5.
24Y
esY
esI
ML
––
7N
INR
5.94
×6.
25
×1.
66N
oY
esI
ML
––
8N
ITR
10.3
0
×9.
65
×3.
68N
oN
oI
ML
––
H: h
eigh
t;
L:
low
; VD
: vit
reou
s
det
ach
men
t;
I:
irre
gula
r;
IN: i
nfe
ron
asal
; IT:
infe
rote
mp
oral
; MH
: med
ium
–hig
h; s
b:
smal
ler
base
; Lb:
larg
er
base
; N: n
odu
lar;
R: r
egu
lar.
. 2 0 1 1;8 6(8):247–253
The ocular fundus and fluorescein angiography findingswere highly vascularized yellowish-pinkish masses in thelower quadrants, visible at the tumor surface (Fig. 1).
Changes in the adjacent retina and macula (lipidic exu-dation, edema and hemorrhage) were also detected (Fig. 1and Table 1). Fluorescein angiography did not exhibit suffi-cient quality in any of the cases and therefore the visibilityof angiographic signs largely depended on the inflammatoryinfiltration and/or hemorrhage in the vitreous gel. In general,we found a loss of contrast derived from the tumoral vesselsduring the arterial-venous phase and in later phases of thetest (images not shown).
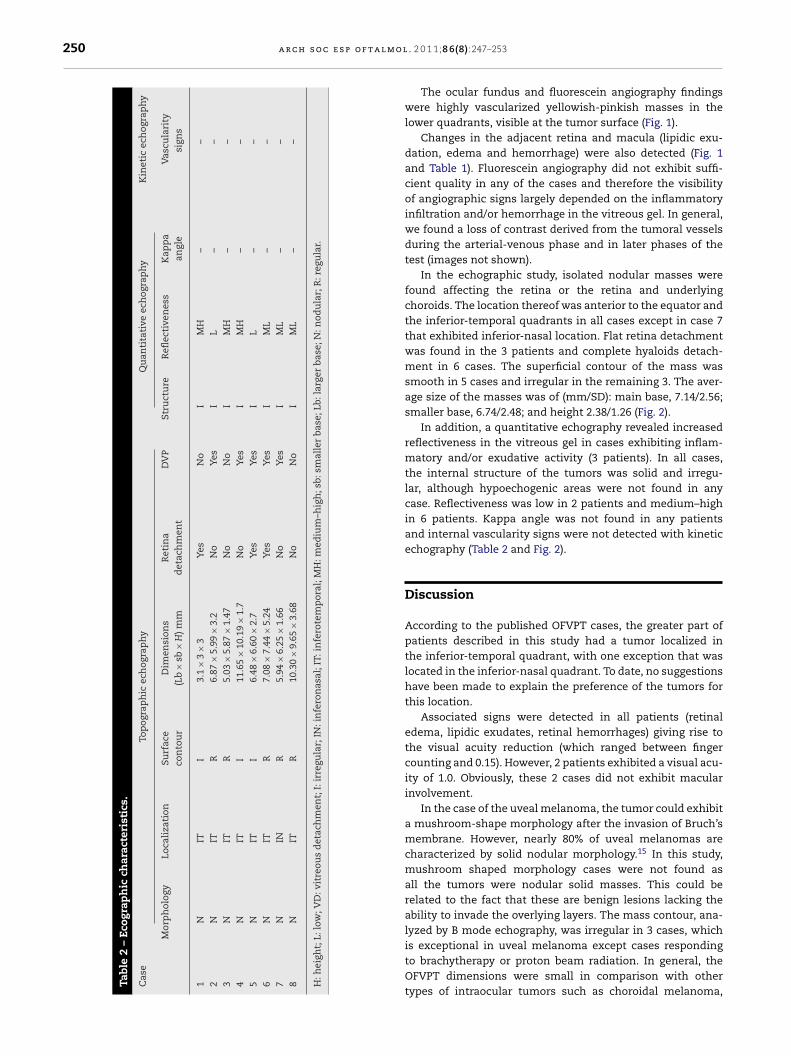
In the echographic study, isolated nodular masses werefound affecting the retina or the retina and underlyingchoroids. The location thereof was anterior to the equator andthe inferior-temporal quadrants in all cases except in case 7that exhibited inferior-nasal location. Flat retina detachmentwas found in the 3 patients and complete hyaloids detach-ment in 6 cases. The superficial contour of the mass wassmooth in 5 cases and irregular in the remaining 3. The aver-age size of the masses was of (mm/SD): main base, 7.14/2.56;smaller base, 6.74/2.48; and height 2.38/1.26 (Fig. 2).
In addition, a quantitative echography revealed increasedreflectiveness in the vitreous gel in cases exhibiting inflam-matory and/or exudative activity (3 patients). In all cases,the internal structure of the tumors was solid and irregu-lar, although hypoechogenic areas were not found in anycase. Reflectiveness was low in 2 patients and medium–highin 6 patients. Kappa angle was not found in any patientsand internal vascularity signs were not detected with kineticechography (Table 2 and Fig. 2).
Discussion
According to the published OFVPT cases, the greater part ofpatients described in this study had a tumor localized inthe inferior-temporal quadrant, with one exception that waslocated in the inferior-nasal quadrant. To date, no suggestionshave been made to explain the preference of the tumors forthis location.
Associated signs were detected in all patients (retinaledema, lipidic exudates, retinal hemorrhages) giving rise tothe visual acuity reduction (which ranged between fingercounting and 0.15). However, 2 patients exhibited a visual acu-ity of 1.0. Obviously, these 2 cases did not exhibit macularinvolvement.
In the case of the uveal melanoma, the tumor could exhibita mushroom-shape morphology after the invasion of Bruch’smembrane. However, nearly 80% of uveal melanomas arecharacterized by solid nodular morphology.15 In this study,mushroom shaped morphology cases were not found asall the tumors were nodular solid masses. This could berelated to the fact that these are benign lesions lacking theability to invade the overlying layers. The mass contour, ana-lyzed by B mode echography, was irregular in 3 cases, which
is exceptional in uveal melanoma except cases respondingto brachytherapy or proton beam radiation. In general, theOFVPT dimensions were small in comparison with othertypes of intraocular tumors such as choroidal melanoma,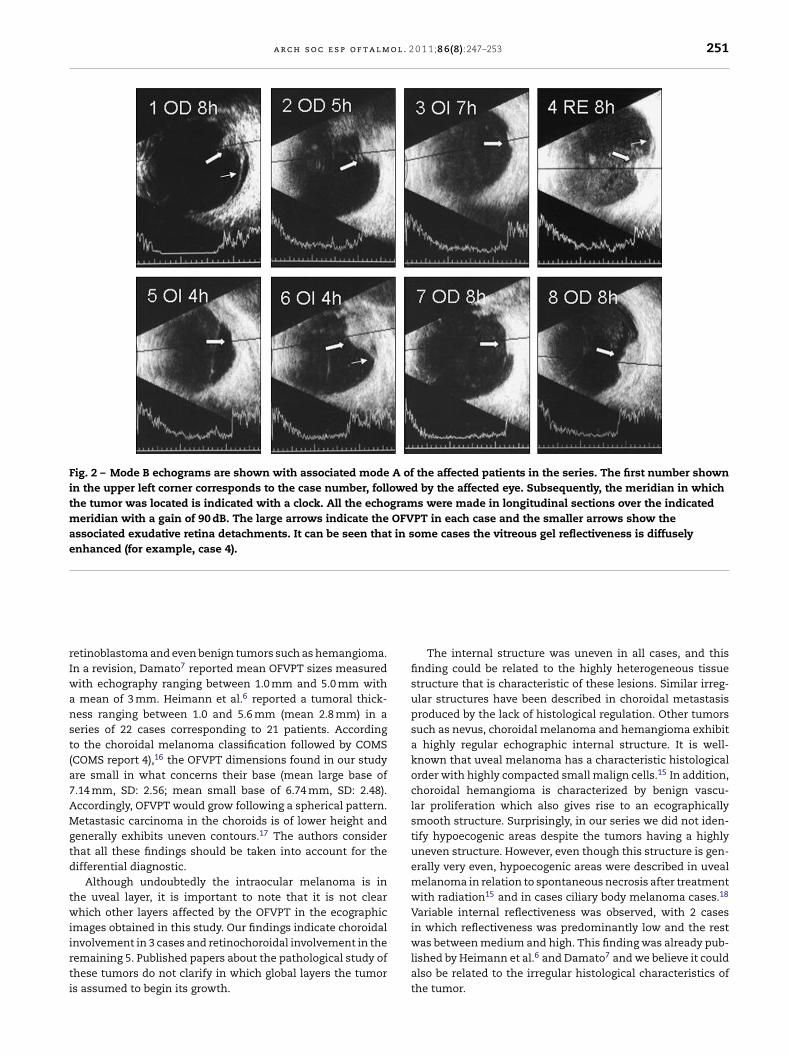
a r c h s o c e s p o f t a l m o l . 2 0 1 1;8 6(8):247–253 251
Fig. 2 – Mode B echograms are shown with associated mode A of the affected patients in the series. The first number shownin the upper left corner corresponds to the case number, followed by the affected eye. Subsequently, the meridian in whichthe tumor was located is indicated with a clock. All the echograms were made in longitudinal sections over the indicatedmeridian with a gain of 90 dB. The large arrows indicate the OFVPT in each case and the smaller arrows show theassociated exudative retina detachments. It can be seen that in some cases the vitreous gel reflectiveness is diffuselyenhanced (for example, case 4).
rIwanst(a7AMgtd
twiirti
etinoblastoma and even benign tumors such as hemangioma.n a revision, Damato7 reported mean OFVPT sizes measuredith echography ranging between 1.0 mm and 5.0 mm with
mean of 3 mm. Heimann et al.6 reported a tumoral thick-ess ranging between 1.0 and 5.6 mm (mean 2.8 mm) in aeries of 22 cases corresponding to 21 patients. Accordingo the choroidal melanoma classification followed by COMSCOMS report 4),16 the OFVPT dimensions found in our studyre small in what concerns their base (mean large base of.14 mm, SD: 2.56; mean small base of 6.74 mm, SD: 2.48).ccordingly, OFVPT would grow following a spherical pattern.etastasic carcinoma in the choroids is of lower height and
enerally exhibits uneven contours.17 The authors considerhat all these findings should be taken into account for theifferential diagnostic.
Although undoubtedly the intraocular melanoma is inhe uveal layer, it is important to note that it is not clearhich other layers affected by the OFVPT in the ecographic
mages obtained in this study. Our findings indicate choroidal
nvolvement in 3 cases and retinochoroidal involvement in theemaining 5. Published papers about the pathological study ofhese tumors do not clarify in which global layers the tumors assumed to begin its growth.The internal structure was uneven in all cases, and thisfinding could be related to the highly heterogeneous tissuestructure that is characteristic of these lesions. Similar irreg-ular structures have been described in choroidal metastasisproduced by the lack of histological regulation. Other tumorssuch as nevus, choroidal melanoma and hemangioma exhibita highly regular echographic internal structure. It is well-known that uveal melanoma has a characteristic histologicalorder with highly compacted small malign cells.15 In addition,choroidal hemangioma is characterized by benign vascu-lar proliferation which also gives rise to an ecographicallysmooth structure. Surprisingly, in our series we did not iden-tify hypoecogenic areas despite the tumors having a highlyuneven structure. However, even though this structure is gen-erally very even, hypoecogenic areas were described in uvealmelanoma in relation to spontaneous necrosis after treatmentwith radiation15 and in cases ciliary body melanoma cases.18
Variable internal reflectiveness was observed, with 2 casesin which reflectiveness was predominantly low and the rest
was between medium and high. This finding was already pub-lished by Heimann et al.6 and Damato7 and we believe it couldalso be related to the irregular histological characteristics ofthe tumor.
l m o l
r
1
1
1
1
1
1
1
1
1999;10:164–7.18. Lois N, Shields CL, Shields JA, Eagle R, De Potter P. Cavitary
melanoma of the ciliary body. Ophthalmology.1998;105:1091–8.
252 a r c h s o c e s p o f t a
The kappa angle is a quantitative echography sign whichis present in most choroidal melanomas.19 It is related to theechographic attenuation attributable to the histological regu-lation of melanoma. In our OFVPT series the kappa angle wasnot identified in any of the cases.
Choroidal excavation has been described for uvealmelanoma20 and it is believed it is linked to the homo-geneous infiltration carried out by the tumor in theunderlying healthy choroids. However, it has also beendescribed in other lesions and it is not consideredpathognomonic of uveal melanoma.21 In this study, nochoroidal excavations have been identified in any ofthe cases, although there also are other tumor lesionssuch as choroidal hemangioma which did not exhibit iteither.
Exudative retinal detachment is frequent in the diag-nostic of choroidal melanoma as a consequence of thetumoral activity (growth and/or related to inflammation)and these retina detachments are located close to thetumor or even in lower quadrants without an identifi-able spatial relationship with the tumor. In our series wedetected retina detachment in 3 cases and in these patientsthe detachment was flat and was found below the mass.We believe that this finding was related to the cases inwhich the tumor began growing from within the retinaitself.
The study of the vitreous revealed a full detach-ment of the posterior vitreous in 6 cases. The vit-reous gel reflectiveness was increased in the patientsand, in these cases, these findings were correlated withinflammatory and/or exudative activity of the tumor orthe hemorrhages detected in the ocular fundus explo-ration.
The internal vascular flow (internal vascularity) is anechographic sign that can be observed in almost all uvealmelanomas.22 In order to identify this sign it is necessaryto utilize an ecograph with an analog screen to observe itin real-time. It can be identified in mode A as well as inmode B, and it is characterized by fast movement of dotson the tumoral base. This sign is clearly related to the vas-cular tree of the melanoma and has not been describedfor other vascular tumors such as the choroidal heman-gioma. In relation with this fact, we did not detect thissign in any of the cases studied in our series. We believethat this finding has the same cause proposed for choroidalhemangioma as both are vascularized tumors and prob-ably the spaces are filled in with non-circulating bloodand for this reason the internal vascularity sign fails toappear.
In summary, even though OFVPT share ecographicsigns with other intraocular tumors, the authors pro-pose the following profile to assist in the final diagnostic:nodular and solid morphology, low height, tendencytowards uneven/irregular surface contour, uneven inter-nal structure, variable reflectiveness and absence ofkappa angle, absence of choroidal excavation and lackof internal vascularity signs. Accordingly, an adequateOFVPT diagnostic must be carried out taking intoaccount not only ophthalmoscopic but also ecographicsigns.
. 2 0 1 1;8 6(8):247–253
Conflict of interests
None of the authors have declared any conflict of interests.
e f e r e n c e s
1. Barr CC, Rice TA, Michels RG. Angioma-like mass in a patientwith retrolental fibroplasias. Am J Ophthalmol.1980;89:647–50.
2. Shields JA, Decker WL, Sanborn GE, Augsburger JJ, GoldbergRE. Presumed acquired retinal hemangiomas.Ophthalmology. 1983;90:1292–300.
3. Campochiaro PA, Conway BP. Hemangioma-like masses of theretina. Arch Ophthalmol. 1988;106:1409–13.
4. Sahel JA, Frederick Jr AR, Pesavento R, Albert DM. Idiopathicretinal gliosis mimicking a choroidal melanoma. Retina.1988;8:282–7.
5. Shields CL, Shields JA, Barret J, Potter P. Vasoproliferativetumors of the ocular fundus. Classification and clinicalmanifestations in 103 patients. Arch Ophthalmol.1995;113:615–23.
6. Heimann H, Bornfeld N, Vij O, Coupland SE, Bechrakis NE,Kellner U, et al. Vasoproliferative tumours of the retina. Br JOphthalmol. 2000;84:1162–9.
7. Damato B. Vasoproliferative tumour. Br J Ophthalmol.2006;90:399–400.
8. Smeets MH, Mooy CM, Baarsma GS, Mertens DE, Van MeursJC. Histopathology of a vasoproliferative tumor of the ocularfundus. Retina. 1998;18:470–2.
9. Irvine F, O’Donell N, Kemp E, Lee WR. Retinalvasoproliferative tumors: surgical management andhistological findings. Arch Ophthalmol. 2000;118:563–9.
0. Anastassiou G, Bornfeld N, Schueler AO, Schilling H, Weber S,Fluehs D, et al. Ruthenium-106 plaque brachytherapy forsymptomatic vasoproliferative tumours of the retina. Br JOphthalmol. 2006;90:447–50.
1. Lafaut BA, Meire FM, Leys AM, Dralands G, De Laey JJ.Vasoproliferative retinal tumors associated with peripheralchorioretinal scars in presumed congenital toxoplasmosis.Graefes Arch Clin Exp Ophthalmol. 1999;237:1033–8.
2. Barbezetto IA, Smith RT. Vasoproliferative tumor of the retinatreated with PDT. Retina. 2003;23:565–7.
3. Blasi MA, Scupola A, Tiberti AC, Sasso P, Balestrazzi E.Photodynamic therapy for vasoproliferative retinal tumors.Retina. 2006;26:404–9.
4. Kenawy N, Groenwald C, Damato B. Treatment of avasoproliferative tumour with intravitreal bevacizumab(Avastin). Eye. 2007;21:893–4.
5. Byrne SF, Green RL. Intraocular tumors. In: Ultrasound of theeye and orbit. 2nd ed. St. Louis, MO: Mosby; 2002.p. 115–90.
6. No authors listed. Mortality in patients with small choroidalmelanoma. COMS report no. 4. The Collaborative OcularMelanoma Study Group. Arch Ophthalmol. 1997;115:886–93.
7. Sobottka B, Kreissig I. Ultrasonography of metastases andmelanomas of the choroid. Curr Opin Ophthalmol.

o l . 2
1
2
2
a r c h s o c e s p o f t a l m
9. Minning Jr CA, Davidorf FH. Ossoinig’s angle of ultrasonicabsorption and its role in the diagnosis of malignant
melanoma. Ann Ophthalmol. 1982;14:564–8.0. Coleman DJ. Reliability of ocular tumor diagnosis withultrasound. Trans Am Acad Ophthalmol Otolaryngol.1973;77:677–86.
2
0 1 1;8 6(8):247–253 253
1. Fuller DG, Snyder WB, Hutton WL, Vaiser A. Ultrasonographicfeatures of choroidal malignant melanomas. Arch
Ophthalmol. 1979;97:1465–72.2. Atta HR. Special examination techniques: globe. In:Ophthalmic ultrasound. A practical guide. New York, NY:Churchill Livingstone; 1996. p. 39–63.