traumatic aortic injury mi zucker, md. a dr z lecture on aortic injuries
TRANSCRIPT
TRAUMATIC AORTIC INJURY
MI Zucker, MD
A dr Z Lecture on Aortic Injuries

Aortic Injuries: Defined
• They are TEARS not dissections, so best terminology would be:
Traumatic Aortic Injury or TAI
Epidemiology
• Major deceleration force as in high speed MVA, auto vs pedestrian, fall from a height
• 80-85% die at scene, aortic root area tear
• 15-20% survive to ED, aortic isthmus tear

PATHOLOGY
• The lesion is an aortic wall TEAR, not a dissection.
• The tear is through the intima and media, with the thin but tough adventitia containing the blood volume as a pseudoaneurysm for a time.
• When the adventitia fails, the patient usually immediately expires.
Location of TAI
(On a Conventional Angiogram)


TAI
In TAI, the mediastinum is of abnormal size or contour.
• Abnormal mediastinum MAY be due to hemorrhage into the mediastinum.
• The hemorrhage is due to small vessel bleeding, rarely from the torn aorta itself.

But…
• If there has been enough deceleration force to rupture small vessels, then there has been enough force to tear the aorta.
However…
• Other things may and often do alter the mediastinum size and contour:
• Supine position
• Portable film
• Poor inspiration
• Tortuous aorta
• Fat, non-trauma diseases

And so…
• The chest film is very sensitive, but not specific for TAI.
• If fact, 90-95% of patients with trauma and abnormal mediastinum DO NOT have TAI.
• But, only 1 % with normal mediastinum DO have TAI.
CHEST FILM FINDINGS of TAI
• Abnormal shape or size of aortic arch• Indistinct aortic arch or aortopulmonary window• Abnormally wide right paratracheal stripe• Deviation of trachea or esophagus (NGT) to right• Left apical cap• Abnormal paraspinal line• Wide mediastinum (over 8 cm)

And: “I don’t know why, but the mediastinum just don’t look
right.”
(You need a little experience to use this one.)

Of these,
• NONE is any better or worse than any other.
• ONE abnormality makes the mediastinum abnormal.

First, the NORMAL Mediastinum
Young
Middle aged
Elderly



An “abnormal” mediastinumin a normal patient
Caused by portable technique, supine position, and poor inspiration


Abnormal mediastinum
• Caused by Traumatic Aortic Injury.
• The subtle and the unsubtle.
• We are going to look for the mediastinum abnormalities we just talked about on each film.






So, Chest Film is Abnormal: What’s Next?
• CT
• TEE
• Angiography
• MRI
• With contrast bolus CTA. Multidetector unit
• Unstable patient. Operator dependent
• Invasive. Labor intensive
• Slow. Harder to manage patient. Availability
ANGIOGRAPHY
Invasive
Labor intensive
The “gold standard”


CTA
Universally available
Quick
Accurate
The new “gold standard”



TREATMENT of TAI
Operate emergently
Graft placement

Prognosis
• Without surgery, classical data show 99% death rate
• With surgery, 70% survival. Most of post-operative deaths due to associated injuries, especially head trauma, not to TAI.
• But…

A Case to Think About:
• Code Trauma
• Young man, MVA, stable, but multiple injuries, including chest.

The Chest Film
Multiple injuries, abnormal mediastinum


The CTA
Called “suggestive” of TAI, but technically limited examination

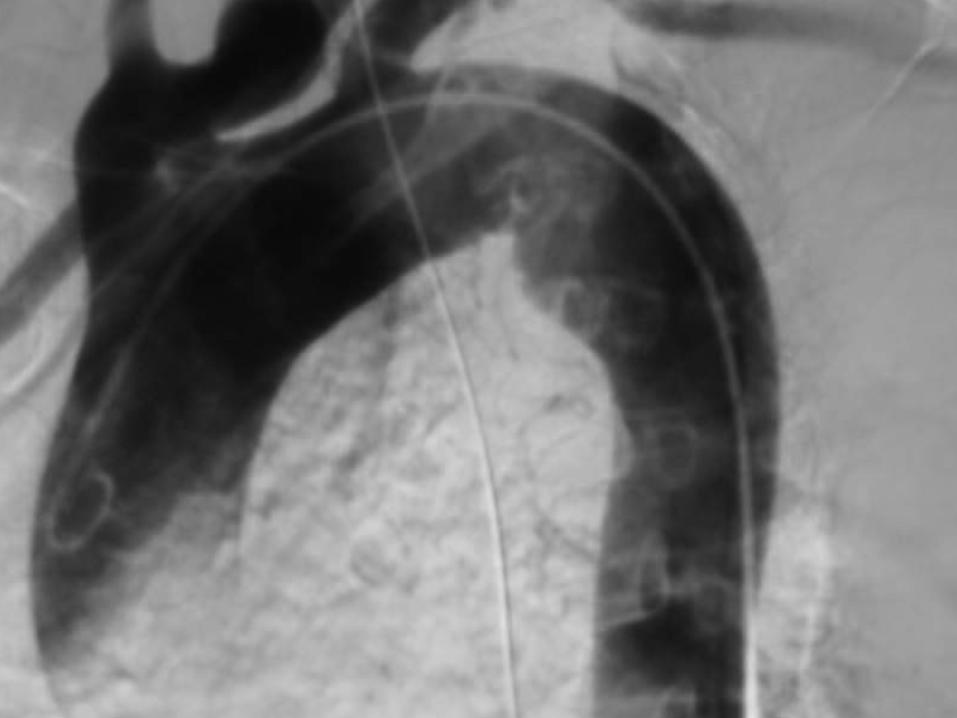
The Angiogram
Done because of uncertain CT.
Called “normal”


So:
• Chest film: Abnormal
• CT: Abnormal, but uncertain for TAI
• Angiogram: Normal

The Outcome:
• No surgery on aorta
• Patient recovered from other injuries
• Discharged
• Still alive, as far as we know

But:
Was the Aorta Injured?

????
• Were the chest film and the CT results correct and the angiogram, the so-called “Gold Standard,” wrong?
• Is MDCT the new “Gold Standard”?
“MINIMAL AORTIC INJURY”
• There are patients with aortic injury who have survived without surgery.
• There may be a subtype of Minimal Intimal Injury with a more benign outcome, where the injured intima heals without intervention.
• So, the 99% death rate without surgery may be an overestimate.

Goodbye
• Copyright 2004
MI Zucker