trauma 2015 / 1
DESCRIPTION
ÂTRANSCRIPT
www.tjtes.orgVolume 21 | Number 1 | January 2015
ISSN 1306 - 696X
TURKISH JOURNAL of TRAUMA& EMERGENCY SURGERYUlusal Travma ve Acil Cerrahi Dergisi


TURKISH JOURNAL of TRAUMA& EMERGENCY SURGERYUlusal Travma ve Acil Cerrahi Dergisi
Editor-in-Chief Recep Güloğlu
Editors Kaya Sarıbeyoğlu (Managing Editor) Hakan Yanar M. Mahir Özmen
Former Editors Ömer Türel, Cemalettin Ertekin, Korhan Taviloğlu
Section Editors Anaesthesiology & ICU Güniz Meyancı Köksal, Mert Şentürk Cardiac Surgery Münacettin Ceviz, Murat Güvener Neurosurgery Ahmet Deniz Belen, Mehmet Yaşar Kaynar Ophtalmology Cem Mocan, Halil Ateş Ortopedics and Traumatology Mahmut Nedim Doral, Mehmet Can Ünlü Plastic and Reconstructive Surgery Ufuk Emekli, Figen Özgür Pediatric Surgery Aydın Yagmurlu, Ebru Yeşildağ Thoracic Surgery Alper Toker, Akif Turna Urology Ali Atan, Öner Şanlı Vascular Surgery Cüneyt Köksoy, Mehmet Kurtoğlu
www.tjtes.org

THE TURKISH ASSOCIATION OF TRAUMA AND EMERGENCY SURGERYULUSAL TRAVMA VE ACİL CERRAHİ DERNEĞİ
President (Başkan) Recep Güloğlu Vice President (Başkan Yardımcısı) Kaya Sarıbeyoğlu Secretary General (Genel Sekreter) M. Mahir Özmen Treasurer (Sayman) Ali Fuat Kaan Gök Members (Yönetim Kurulu Üyeleri) Hakan Teoman Yanar Gürhan Çelik Osman Şimşek
CORRESPONDENCEİLETİŞİM
ISSUED BY THE TURKISH ASSOCIATION OF TRAUMA AND EMERGENCY SURGERYULUSAL TRAVMA VE ACİL CERRAHİ DERNEĞİ YAYIN ORGANI
UlusalTravmaveAcilCerrahiDerneği Tel: +90 212 - 588 62 46 - 588 62 46ŞehreminiMah.,KöprülüMehmetPaşaSok. Fax (Faks): +90 212 - 586 18 04DadaşoğluApt.,No:25/1, e-mail (e-posta):[email protected]Şehremini,İstanbul,Turkey Web:www.travma.org.tr
Owner (Ulusal Travma ve Acil Cerrahi Derneği adına Sahibi) RecepGüloğluEditorialDirector (Yazı İşleri Müdürü) RecepGüloğluManagingEditor (Yayın Koordinatörü) M.MahirÖzmenAmblem MetinErtemCorrespondenceaddress (Yazışma adresi) UlusalTravmaveAcilCerrahiDergisiSekreterliği ŞehreminiMah.,KöprülüMehmetPaşaSok., DadaşoğluApt.,No:25/1,34104Şehremini,İstanbul Tel +90 212 - 531 12 46 - 588 62 46 Fax (Faks) +90 212 - 586 18 04
p-ISSN 1306-696x • e-ISSN 1307-7945 • Included in Index Medicus, Medline; EMBASE, Excerpta Medica; Science Citation Index-Expanded (SCI-E), Index Copernicus, DOAJ, and Turkish Medical Index (Index Medicus, Medline; EMBASE, Excerpta Medica; Science Citation Index-Expanded (SCI-E), Index Copernicus, DOAJ ve TÜBİTAK ULAKBİM Türk Tıp Dizini’nde yer almaktadır.)
Publisher (Yayımcı): KARE Yayıncılık (KARE Publishing) • www.kareyayincilik.com • Design (Tasarım): Ali Cangül • Graphics (Grafikler): Edibe Çomaktekin • Linguistic Editor (İngilizce Editörü): Merve Şenol • Redaction (Redaksiyon): Erman Aytaç • Online Manuscript & Web Management (Online Dergi & Web): LookUs • Press (Baskı): Yıldırım Matbaacılık • Press date (Basım tarihi): January (Ocak) 2015 • This publication is printed on paper that meets the international standard ISO 9706: 1994 (Bu dergide kullanılan kağıt ISO 9706: 1994 standardına uygundur.)
www.tjtes.org
KARE

The Turkish Journal of Trauma and Emergency Surgery (TJTES) is an official publication of the Turkish Association of Trauma and Emer-gency Surgery. It is a peer-reviewed periodical that considers for pub-lication clinical and experimental studies, case reports, technical con-tributions, and letters to the editor. Six issues are published annually.As from 2001, the journal is indexed in Index Medicus and Medline, as from 2005 in Excerpta Medica and EMBASE, as from 2007 in Science Citation Index Expanded (SCI-E) and Journal Citation Reports / Sci-ence Edition, and as from 2008 in Index Copernicus. For the five-year term of 2001-2006, our impact factor in SCI-E indexed journals is 0.5. It is cited as ‘Ulus Travma Acil Cerrahi Derg’ in PUBMED. Submission of a manuscript by electronic means implies: that the work has not been published before (except in the form of an abstract or as part of a published lecture, review, or thesis); that it is not under consideration for publication elsewhere; and that its publication in the Turkish Journal of Trauma and Emergency Surgery is approved by all co-authors. The author(s) transfer(s) the copyright to the Turkish Asso-ciation of Trauma and Emergency Surgery to be effective if and when the manuscript is accepted for publication. The author(s) guarantee(s) that the manuscript will not be published elsewhere in any other lan-guage without the consent of the Association. If the manuscript has been presented at a meeting, this should be stated together with the name of the meeting, date, and the place.Manuscripts may be submitted in Turkish or in English. All submissions are initially reviewed by the editor, and then are sent to reviewers. All manuscripts are subject to editing and, if necessary, will be returned to the authors for answered responses to outstanding questions or for ad-dition of any missing information to be added. For accuracy and clarity, a detailed manuscript editing is undertaken for all manuscripts accepted for publication. Final galley proofs are sent to the authors for approval.Unless specifically indicated otherwise at the time of submission, re-jected manuscripts will not be returned to the authors, including ac-companying materials.TJTES is indexed in Science Citation Index-Expanded (SCI-E), Index Medicus, Medline, EMBASE, Excerpta Medica, and the Turkish Medi-cal Index of TUBITAK-ULAKBIM. Priority of publications is given to original studies; therefore, selection criteria are more refined for re-views and case reports.Open Access Policy: Full text access is free. There is no charge for publication or downloading the full text of printed material.Manuscript submission: TJTES accepts only on-line submission via the official web site (please click, www.travma.org.tr/en) and refuses printed manuscript submissions by mail. All submissions are made by the on-line submission system called Journal Agent, by clicking the icon “Online manuscript submission” at the above mentioned web site homepage. The system includes directions at each step but for fur-ther information you may visit the web site (http://www.travma.org/en/journal/).Manuscript preparation: Manuscripts should have double-line spac-ing, leaving sufficient margin on both sides. The font size (12 points) and style (Times New Roman) of the main text should be uniformly taken into account. All pages of the main text should be numbered consecutively. Cover letter, manuscript title, author names and institu-tions and correspondence address, abstract in Turkish (for Turkish au-thors only), and title and abstract in English are uploaded to the Journal Agent system in the relevant steps. The main text includes Introduc-tion, Materials and Methods, Results, Discussion, Acknowledgments, References, Tables and Figure Legends.The cover letter must contain a brief statement that the manuscript has been read and approved by all authors, that it has not been submit-ted to, or is not under consideration for publication in, another journal. It should contain the names and signatures of all authors. The cover letter is uploaded at the 10th step of the “Submit New Manuscript” sec-
tion, called “Upload Your Files”.Abstract: The abstract should be structured and serve as an informa-tive guide for the methods and results sections of the study. It must be prepared with the following subtitles: Background, Methods, Results and Conclusions. Abstracts should not exceed 200 words.Figures, illustrations and tables: All figures and tables should be numbered in the order of appearance in the text. The desired position of figures and tables should be indicated in the text. Legends should be included in the relevant part of the main text and those for photo-micrographs and slide preparations should indicate the magnification and the stain used. Color pictures and figures will be published if they are definitely required and with the understanding that the authors are prepared to bear the costs. Line drawings should be professionally pre-pared. For recognizable photographs, signed releases of the patient or of his/her legal representatives should be enclosed; otherwise, patient names or eyes must be blocked out to prevent identification.References: All references should be numbered in the order of men-tion in the text. All reference figures in the text should be given in brack-ets without changing the font size. References should only include articles that have been published or accepted for publication. Refer-ence format should conform to the “Uniform requirements for manu-scripts submitted to biomedical journals” (http://www.icmje.org) and its updated versions (February 2006). Journal titles should be abbrevi-ated according to Index Medicus. Journal references should provide inclusive page numbers. All authors, if six or fewer, should be listed; otherwise the first six should be listed, followed by “et al.” should be written. The style and punctuation of the references should follow the formats below:Journal article: Velmahos GC, Kamel E, Chan LS, Hanpeter D, Asensio JA, Murray JA, et al. Complex repair for the management of duodenal injuries. Am Surg 1999;65:972-5.Chapter in book: Jurkovich GJ. Duodenum and pancreas. In: Mattox KL, Feliciano DV, Moore EE, editors. Trauma. 4th ed. New York: Mc-Graw-Hill; 2000. p. 735-62.Our journal has succeeded in being included in several indexes, in this context, we have included a search engine in our web site (www.travma.org.tr) so that you can access full-text articles of the previous issues and cite the published articles in your studies.Review articles: Only reviews written by distinguished authors based on the editor’s invitation will be considered and evaluated. Review ar-ticles must include the title, summary, text, and references sections. Any accompanying tables, graphics, and figures should be prepared as mentioned above.Case reports: A limited number of case reports are published in each is-sue of the journal. The presented case(s) should be educative and of in-terest to the readers, and should reflect an exclusive rarity. Case reports should contain the title, summary, and the case, discussion, and refer-ences sections. These reports may consist of maximum five authors.Letters to the Editor: “Letters to the Editor” are only published elec-tronically and they do not appear in the printed version of TJTES and PUBMED. The editors do not issue an acceptance document as an original article for the ‘’letters to the editor. The letters should not ex-ceed 500 words. The letter must clearly list the title, authors, publica-tion date, issue number, and inclusive page numbers of the publication for which opinions are released.Informed consent - Ethics: Manuscripts reporting the results of ex-perimental studies on human subjects must include a statement that informed consent was obtained after the nature of the procedure(s) had been fully explained. Manuscripts describing investigations in animals must clearly indicate the steps taken to eliminate pain and suffering. Authors are advised to comply with internationally accepted guidelines, stating such compliance in their manuscripts and to include the approval by the local institutional human research committee.
INFORMATION FOR THE AUTHORS

Ulusal Travma ve Acil Cerrahi Dergisi, Ulusal Travma ve Acil Cerrahi Derneği’nin yayın organıdır. Travma ve acil cerrahi hastalıklar konuların-da bilimsel birikime katkısı olan klinik ve deneysel çalışmaları, editöryel yazıları, klinik olgu sunumlarını ve bu konulardaki teknik katkılar ile son gelişmeleri yayınlar. Dergi iki ayda bir yayınlanır.Ulusal Travma ve Acil Cerrahi Dergisi, 2001 yılından itibaren Index Me-dicus ve Medline’da, 2005 yılından itibaren Excerpta Medica / EMBASE indekslerinde, 2007 yılından itibaren Science Citation Index-Expanded (SCI-E) ile Journal Citation Reports / Science Edition uluslararası in-dekslerinde ve 2008 yılından itibaren Index Copernicus indeksinde yer almaktadır. 2001-2006 yılları arasındaki 5 yıllık dönemde SCI-E kapsa-mındaki dergilerdeki İmpakt faktörümüz 0,5 olmuştur. Dergide araştırma yazılarına öncelik verilmekte, bu nedenle derleme veya olgu sunumu türündeki yazılarda seçim ölçütleri daha dar tutulmaktadır. PUBMED’de dergi “Ulus Travma Acil Cerrahi Derg” kısaltması ile yer almaktadır. Dergiye yazı teslimi, çalışmanın daha önce yayınlanmadığı (özet ya da bir sunu, inceleme, ya da tezin bir parçası şeklinde yayınlanması dışın-da), başka bir yerde yayınlanmasının düşünülmediği ve Ulusal Travma ve Acil Cerrahi Dergisi’nde yayınlanmasının tüm yazarlar tarafından uygun bulunduğu anlamına gelmektedir. Yazar(lar), çalışmanın yayın-lanmasının kabulünden başlayarak, yazıya ait her hakkı Ulusal Travma ve Acil Cerrahi Derneği’ne devretmektedir(ler). Yazar(lar), izin almaksı-zın çalışmayı başka bir dilde ya da yerde yayınlamayacaklarını kabul eder(ler). Gönderilen yazı daha önce herhangi bir toplantıda sunulmuş ise, toplantı adı, tarihi ve düzenlendiği şehir belirtilmelidir.Dergide Türkçe ve İngilizce yazılmış makaleler yayınlanabilir. Tüm yazı-lar önce editör tarafından ön değerlendirmeye alınır; daha sonra incelen-mesi için danışma kurulu üyelerine gönderilir.Tüm yazılarda editöryel değerlendirme ve düzeltmeye başvurulur; ge-rektiğinde, yazarlardan bazı soruları yanıtlanması ve eksikleri tamam-lanması istenebilir. Dergide yayınlanmasına karar verilen yazılar “ma-nuscript editing” sürecine alınır; bu aşamada tüm bilgilerin doğruluğu için ayrıntılı kontrol ve denetimden geçirilir; yayın öncesi şekline getirilerek yazarların kontrolüne ve onayına sunulur. Editörün, kabul edilmeyen yazıların bütününü ya da bir bölümünü (tablo, resim, vs.) iade etme zo-runluluğu yoktur.Açık Erişim İlkesi: Tam metinlere erişim ücretsizdir. Yayınlanan basılı materyali tam metni indirmek için herhangi bir ücret alınmaz.Yazıların hazırlanması: Tüm yazılı metinler 12 punto büyüklükte “Times New Roman” yazı karakterinde iki satır aralıklı olarak yazılmalıdır. Say-fada her iki tarafta uygun miktarda boşluk bırakılmalı ve ana metindeki sayfalar numaralandırılmalıdır. Journal Agent sisteminde, başvuru mek-tubu, başlık, yazarlar ve kurumları, iletişim adresi, Türkçe özet ve yazının İngilizce başlığı ve özeti ilgili aşamalarda yüklenecektir. İngilizce yazı-lan çalışmalara da Türkçe özet eklenmesi gerekmektedir. Yazının ana metnindeyse şu sıra kullanılacaktır: Giriş, Gereç ve Yöntem, Bulgular, Tartışma, Teşekkür, Kaynaklar, Tablolar ve Şekiller.Başvuru mektubu: Bu mektupta yazının tüm yazarlar tarafından okun-duğu, onaylandığı ve orijinal bir çalışma ürünü olduğu ifade edilmeli ve yazar isimlerinin yanında imzaları bulunmalıdır. Başvuru mektubu ayrı bir dosya olarak, Journal Agent sisteminin “Yeni Makale Gönder” bölü-münde, 10. aşamada yer alan dosya yükleme aşamasında yollanmalıdır.Başlık sayfası: Yazının başlığı, yazarların adı, soyadı ve ünvanları, ça-lışmanın yapıldığı kurumun adı ve şehri, eğer varsa çalışmayı destekle-yen fon ve kuruluşların açık adları bu sayfada yer almalıdır. Bu sayfaya ayrıca “yazışmadan sorumlu” yazarın isim, açık adres, telefon, faks, mo-bil telefon ve e-posta bilgileri eklenmelidir. Özet: Çalışmanın gereç ve yöntemini ve bulgularını tanıtıcı olmalıdır. Türkçe özet, Amaç, Gereç ve Yöntem, Bulgular, Sonuç ve Anahtar Söz-cükler başlıklarını; İngilizce özet Background, Methods, Results, Conc-lusion ve Key words başlıklarını içermelidir. İngilizce olarak hazırlanan çalışmalarda da Türkçe özet yer almalıdır. Özetler başlıklar hariç 190-210 sözcük olmalıdır. Tablo, şekil, grafik ve resimler: Şekillere ait numara ve açıklayıcı bil-giler ana metinde ilgili bölüme yazılmalıdır. Mikroskobik şekillerde resmi açıklayıcı bilgilere ek olarak, büyütme oranı ve kullanılan boyama tekniği de belirtilmelidir. Yazarlara ait olmayan, başka kaynaklarca daha önce yayınlanmış tüm resim, şekil ve tablolar için yayın hakkına sahip kişiler-
den izin alınmalı ve izin belgesi dergi editörlüğüne ayrıca açıklamasıyla birlikte gönderilmelidir. Hastaların görüntülendiği fotoğraflara, hastanın ve/veya velisinin imzaladığı bir izin belgesi eşlik etmeli veya fotoğrafta hastanın yüzü tanınmayacak şekilde kapatılmış olmalıdır. Renkli resim ve şekillerin basımı için karar hakemler ve editöre aittir. Yazarlar renkli baskının hazırlık aşamasındaki tutarını ödemeyi kabul etmelidirler. Kaynaklar: Metin içindeki kullanım sırasına göre düzenlenmelidir. Ma-kale içinde geçen kaynak numaraları köşeli parantezle ve küçültülmeden belirtilmelidir. Kaynak listesinde yalnızca yayınlanmış ya da yayınlan-ması kabul edilmiş çalışmalar yer almalıdır. Kaynak bildirme “Uniform Requirements for Manuscripts Submitted to Biomedical Journals” (http://www.icmje.org) adlı kılavuzun en son güncellenmiş şekline (Şubat 2006) uymalıdır. Dergi adları Index Medicus’a uygun şekilde kısaltılmalıdır. Altı ya da daha az sayıda olduğunda tüm yazar adları verilmeli, daha çok yazar durumunda altıncı yazarın arkasından “et al.” ya da “ve ark.” ek-lenmelidir. Kaynakların dizilme şekli ve noktalamalar aşağıdaki örneklere uygun olmalıdır:Dergi metni için örnek: Velmahos GC, Kamel E, Chan LS, Hanpeter D, Asensio JA, Murray JA, et al. Complex repair for the management of duodenal injuries. Am Surg 1999;65:972-5.Kitaptan bölüm için örnek: Jurkovich GJ. Duodenum and pancreas. In: Mattox KL, Feliciano DV, Moore EE, editors. Trauma. 4th ed. New York: McGraw-Hill; 2000. p. 735-62.Sizlerin çalışmalarınızda kaynak olarak yararlanabilmeniz için www.trav-ma.org.tr adresli web sayfamızda eski yayınlara tam metin olarak ulaşa-bileceğiniz bir arama motoru vardır.Derleme yazıları: Bu tür makaleler editörler kurulu tarafından gerek ol-duğunda, konu hakkında birikimi olan ve bu birikimi literatüre de yan-sımış kişilerden talep edilecek ve dergi yazım kurallarına uygunluğu saptandıktan sonra değerlendirmeye alınacaktır. Derleme makaleleri; başlık, Türkçe özet, İngilizce başlık ve özet, alt başlıklarla bölümlendiril-miş metin ile kaynakları içermelidir. Tablo, şekil, grafik veya resim varsa yukarıda belirtildiği şekilde gönderilmelidir.Olgu sunumları: Derginin her sayısında sınırlı sayıda olgu sunumu-na yer verilmektedir. Olgu bildirilerinin kabulünde, az görülürlük, eğitici olma, ilginç olma önemli ölçüt değerlerdir. Ayrıca bu tür yazıların olabil-diğince kısa hazırlanması gerekir. Olgu sunumları başlık, Türkçe özet, İngilizce başlık ve özet, olgu sunumu, tartışma ve kaynaklar bölümlerin-den oluşmalıdır. Bu tür çalışmalarda en fazla 5 yazara yer verilmesine özen gösterilmelidir.Editöre mektuplar: Editöre mektuplar basılı dergide ve PUBMED’de yer almamakta, ancak derginin web sitesinde yayınlanmaktadır. Bu mektup-lar için dergi yönetimi tarafından yayın belgesi verilmemektedir.Daha önce basılmış yazılarla ilgili görüş, katkı, eleştiriler ya da farklı bir konu üzerindeki deneyim ve düşünceler için editöre mektup yazılabilir. Bu tür yazılar 500 sözcüğü geçmemeli ve tıbbi etik kurallara uygun ola-rak kaleme alınmış olmalıdır. Mektup basılmış bir yazı hakkında ise, söz konusu yayına ait yıl, sayı, sayfa numaraları, yazı başlığı ve yazarların adları belirtilmelidir. Mektup bir konuda deneyim, düşünce hakkında ise verilen bilgiler doğrultusunda dergi kurallarına uyumlu olarak kaynaklar da belirtilmelidir. Bilgilendirerek onay alma - Etik: Deneysel çalışmaların sonuçlarını bil-diren yazılarda, çalışmanın yapıldığı gönüllü ya da hastalara uygulanacak prosedür(lerin) özelliği tümüyle anlatıldıktan sonra, onaylarının alındığını gösterir bir cümle bulunmalıdır. Yazarlar, bu tür bir çalışma söz konusu olduğunda, uluslararası alanda kabul edilen kılavuzlara ve T.C. Sağlık Bakanlığı tarafından getirilen yönetmelik ve yazılarda belirtilen hüküm-lere uyulduğunu belirtmeli ve kurumdan aldıkları Etik Komitesi onayını göndermelidir. Hayvanlar üzerinde yapılan çalışmalarda ağrı, acı ve ra-hatsızlık verilmemesi için neler yapıldığı açık bir şekilde belirtilmelidir.Yazı gönderme - Yazıların gönderilmesi: Ulusal Travma ve Acil Cer-rahi Dergisi yalnızca www.travma.org.tr adresindeki internet sitesinden on-line olarak gönderilen yazıları kabul etmekte, posta yoluyla yollanan yazıları değerlendirmeye almamaktadır. Tüm yazılar ilgili adresteki “Onli-ne Makale Gönderme” ikonuna tıklandığında ulaşılan Journal Agent sis-teminden yollanmaktadır. Sistem her aşamada kullanıcıyı bilgilendiren özelliktedir.
YAZARLARA BİLGİ
ULUSAL TRAVMA VE ACİL CERRAHİ DERGİSİVol. - Cilt 21 Number - Sayı 1 January - Ocak 2015
Deneysel Çalışma - Experimental Study
1-8 Therapeutic evaluation of interleukin 1-beta antagonist Anakinra against traumatic brain injury in rats İnterlökin 1-beta inhibitörü Anakinra’nın sıçanlarda travmatik beyin hasarına karşı terapötik etkinliğinin değerlendirmesi Hasturk AE, Yilmaz ER, Turkoglu E, Kertmen H, Horasanli B, Hayirli N, Erguder IB, Evirgen O
9-14 Effects of alpha lipoic acid on intra-abdominal adhesion: an experimental study in a rat model Alfa lipoik asitin intraabdominal adezyon üzerine etkileri: Sıçan modelinde deneysel bir çalışma Allahverdi TD, Allahverdi E, Yayla S, Deprem T, Merhan O, Vural S, Sülü B, Günerhan Y, Köksal N
15-21 Spontaneous regeneration capacity of controlled small bowel perforations: an experimental study in rats Kontrollü ince bağırsak perforasyonlarının spontan rejenerasyon potansiyeli: Sıçanlarda deneysel bir çalışma Pekel Ö, Hatipoglu S, Turhan AN, Hatipoglu F, Abdullayev R, Göksel S
Klinik Çalışma - Original Articles
22-26 Comparison of morphine–midazolam versus morphine injection for pain relief in patients with limb fractures - a clinical trial Ekstremite kırıkları olan hastalarda ağrı giderimi için morfin-midazolama karşın morfin enjeksiyonunun karşılaştırılması - klinik çalışma Majidi A, Dinpanah H, Ashoori S, Motamed H, Tabatabaey A
27-33 Outpatient burn management and unnecessary referrals Yanık hastalarının ayaktan takibi ve gereksiz hasta nakilleri Sözen İ, Guldogan CE, Kismet K, Sabuncuoğlu MZ, Yasti AC
34-38 Mortality risk factors in burn care units considering the clinical significance of acinetobacter infections Acinetobacter enfeksiyonlarının klinik önemi ışığında yanık ünitesinde mortalite için risk faktörleri Atilla A, Tomak L, Katrancı AO, Ceylan A, Kılıç SS
39-43 Evaluation of serum L-FABP levels in patients with acute pancreatitis Akut pankreatitli hastalarda serum L-FABP düzeylerinin değerlendirilmesi Koçak E, Akbal E, Köklü S, Adam G
44-50 Factors affecting postoperative mortality in patients older than 65 years undergoing surgery for hip fracture Kalça kırığı nedeni ile ameliyat edilen 65 yaş üstü hastalarda mortaliteye etki eden faktörler Karaman Ö, Özkazanlı G, Orak MM, Mutlu S, Mutlu H, Çalışkan G, Karakuş Ö, Saygı B
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 vii
Contents - İçindekiler
TURKISH JOURNAL OF TRAUMA & EMERGENCY SURGERY
Original Articles - Klinik Çalışma
Experimental Study - Deneysel Çalışma
ix-x Editorial - Editörden
51-56 Evaluation of power Doppler sonography in acute cholecystitis to predict intraoperative findings: a prospective clinical study Akut kolesistitte intraoperatif bulguları öngörmede power Doppler ultrasonun değerlendirilmesi: İleriye yönelik klinik çalışma Çetinkünar S, Erdem H, Aktimur R, Soker G, Bozkurt H, Reyhan E, Sozen S, İrkorucu O
57-62 Ciddi yanık travması olan hastalarda hastane kaynaklı idrar yolu enfeksiyonu sıklığı ve risk faktörlerinin araştırılması Investigation of prevalance and risk factors for hospital-acquired urinary tract infections in patients with severe burn injury Ün S, Yılmaz Y, Yıldırım M, Akdeniz F, Türk H, Koca O
Olgu Sunumu - Case Reports
63-67 Closed reduction of traumatic bilateral anterior hip dislocations with sedation: a case report and review of the literature Travmatik çift taraflı anterior kalça çıkıklarında sedasyon ile kapalı redüksiyon: Bir olgu sunumu ve literatürün gözden geçirilmesi Chiu CK, Ng TS, Wazir NN, Bhurhanudeen KA
68-70 Carotid blowout syndrome Karotis patlama sendromu Lin YS, Wang CT, Chen YT, Chen KT
71-74 The care of a patient with Fournier’s gangrene Fournier gangrenli hastanın bakımı Özşaker E, Yavuz M, Altınbaş Y, Köze BŞ, Nurülke B
75-78 Late onset brachial artery thrombosis and total temporary peripheral neuropathy in a child with humerus supracondylar fracture: a case report Pediatrik humerus suprakondiler kırıklı bir hastada geç gelişen brakiyal arter trombozu ve total geçici sinir paralizisi: Olgu sunumu Ege T, Türkkan S, Günay C, Külahçı Y, Kürklü M
Ulus Travma Acil Cerrahi Derg, Ocak 2015, Cilt. 21, No. 1viii
Contents - İçindekiler
Case Reports - Olgu Sunumu
ULUSAL TRAVMA VE ACİL CERRAHİ DERGİSİVol. - Cilt 21 Number - Sayı 1 January - Ocak 2015
TURKISH JOURNAL OF TRAUMA & EMERGENCY SURGERY
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 ix
EDITORIAL
Dear readers of the Turkish Journal of Trauma and Emergency Surgery,
Our journal which maintains its role as being an important and a leading scientific source in the field of trauma and emergency surgery in Turkey is now celebrating its 20th year. Turkish Journal of Trauma and Emergency Surgery has gained the honor of being internationally recognized thanks to your valuable contributions. We will keep on publishing substantial articles along with the first issue of 2015.
As of 2014, our journal pursues its publication life with the standards of American and European biomedical journals, and the papers sent to our journal are evaluated considering the standards of “Committee on Publication Ethics (COPE)”. All papers sent to our journal are assessed by plagiarism detection software, and we provide feedback regarding problem papers.
We would like to announce two novelties that will be brought as of 2015. Our journal has attained an increasing interest from either domestic or foreign authors, and the majority of the papers reaching us are in English. Since published articles require to be cited more in order to increase the influence of our journal, it is obvious that the papers written in English have an enriching and accelerating effect. On the other hand, it would be an advantage to our authors if the number of works cited increased. Therefore, we have taken the decision only to publish papers written in English as of 2015. This decision is not going to affect the evaluation and publishing processes of Turkish papers previously sent. Consequently, we kindly ask you to write your new papers in English.
Another novelty brought by our journal is to put the section editor system into action so as to shorten the evaluation process of the papers and make it more productive. Increased numbers of papers, and difficulties and delays faced during the evaluation process have necessitated managing this process more actively. We hope that this practice will shorten the long evaluation process resulting in your complaints.
Finally, on behalf of our Editorial Board, we wish you a successful and happy new year, and we would like to express our deepest desire for your increasing support and interest in our journal. Hope to see you in the 10th Turkish Trauma and Emergency Surgery Congress between 28 October and 1 November in Antalya.
Best Regards,
Recep Güloğlu, Kaya Sarıbeyoğlu, M. Mahir Özmen, Hakan Yanar
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1x
EDİTÖRDEN
Ulusal Travma ve Acil Cerrahi Dergisi’nin değerli okurları,
Türkiye’de travma ve acil cerrahi alanında öncü ve önemli bilimsel kaynak olmayı sür-düren dergimiz 20. yılını tamamlamakta. Uluslararası dergi kimliğini de kazanmış olan Ulusal Travma ve Acil Cerrahi Dergisi sizlerin değerli katkılarıyla bu onura ulaşmış du-rumda. 2015’in bu ilk sayısıyla birlikte yine birçok değerli makaleyle karşınızdayız.
2014 yılından itibaren Avrupa ve Amerika biyomedikal dergi standartlarında yayın ha-yatına devam eden dergimize gelen yazılar “Committee on Publication Ethics (COPE)” ölçütlerinde değerlendirilmektedir. Dergimize ulaşan tüm eserler intihal (plagiarism) arama programıyla değerlendirilmekte, sorunlu yazılarla ilgili olarak geri bildirimde bu-lunmaktayız.
2015 itibariyle başlatacağımız iki yeniliği daha duyurmak istiyoruz. Dergimiz gerek ulu-sal gerekse de uluslararası çalışmacıların her geçen yıl artan ilgisiyle karşılaşmakta ve tarafımıza ulaşan yazıların çoğunluğunu İngilizce yazılar oluşturmaktadır. Dergimizin etki faktörünün yükselmesi için yayımlanmış yazıların daha çok atıf alması gerektiğinden bu amaca dönük yazıların İngilizce dilinde yayımlanmasının değer katıcı ve hızlandırıcı etkisi olduğu ortadadır. Öte yandan alınacak atıf sayısının yüksekliği çalışmacıların da lehine bir durum ortaya koyacaktır. Bu nedenle 2015 itibariyle gönderilen yazılar içinde sadece İngilizce olanları yayımlama kararı aldık. Bu karar daha önce gönderilmiş olan Türkçe yazıların değerlendirme veya basım süreçlerini etkilemeyecektir. Bu nedenle sizlerden yeni çalışmalarınızı İngilizce dilinde kaleme almanızı rica ediyoruz.
Dergimizin başlatacağı diğer bir yenilik de yazıların değerlendirilme sürecini kısaltmak ve daha nitelikli bir hale getirmek için bölüm editörlüğü sisteminin hayata geçmesini sağlamak olacak. Her yıl artan yazı sayıları ve değerlendirme süreçlerinde yaşanan zor-luklar, gecikmeler bu düzenlemenin daha aktif bir biçimde işletilmesini zorunlu kılmıştır. Bu uygulamamızın şikayetlerinize de yol açan uzun değerlendirme sürecini kısaltacağını umuyoruz.
Son olarak, 28 Ekim - 1 Kasım 2015 tarihinde 10. Ulusal Travma ve Acil Cerrahi Kongresi’nde Antalya’da görüşmek ümidiyle Editörler kurulumuz adına sizlere başarılı ve mutlu bir yeni yıl diler, dergimize olan ilgi ve desteğinizin artarak devam etmesini beklediğimizi ifade ederiz.
Saygılarımızla,
Recep Güloğlu, Kaya Sarıbeyoğlu, M. Mahir Özmen, Hakan Yanar
Therapeutic evaluation of interleukin 1-beta antagonist Anakinra against traumatic brain injury in ratsAskin Esen Hasturk, M.D.,1 Erdal Resit Yilmaz, M.D.,2 Erhan Turkoglu, M.D.,2 Hayri Kertmen, M.D.,2 Bahriye Horasanli, M.D.,3 Nazli Hayirli, MSc.,4 Imge Berrin Erguder, M.D.,5 Oya Evirgen, M.D.4
1DepartmentofNeurosurgery,OncologyTrainingandResearchHospital,Ankara;2DepartmentofNeurosurgery,DiskapiYildirimBeyazitTrainingandResearchHospital,Ankara;3DepartmentofNeurology,BaskentUniversityFacultyofMedicine,Ankara;4DepartmentofHistologyandEmbryology,AnkaraUniversityFacultyofMedicine,Ankara;5DepartmentofBiochemistry,AnkaraUniversityFacultyofMedicine,Ankara
ABSTRACT
BACKGROUND: The aim of this study was to evaluate the therapeutic efficiency of Anakinra, an IL-1β antagonist with anti-inflam-matory effects, in an experimental model of traumatic brain injury (TBI).
METHODS: Fifty-four rats underwent TBI after a weighted object was dropped onto a metal disc secured to their skulls. Animals were randomized into 3 main groups: control (n=18), TBI + saline (n=18; six animals per time-point) with samples obtained at the first, sixth and twenty-fourth h postoperatively, and TBI + Anakinra (n=18; six animals per time-point) with brain samples obtained at the first, sixth and twenty-fourth h postoperatively. Brain tissue and blood serum were extracted for the analysis of IL-1β, malondial-dehyde, glutathione peroxidase, superoxide dismutase, and catalase levels. Tissue sections were evaluated histopathologically under a light microscope.
RESULTS: After trauma, tissue and serum IL-1β levels were significantly elevated and after Anakinra administration, these levels substantially decreased. Glutathione peroxidase, superoxide dismutase, and catalase activity decreased following TBI and Anakinra ad-ministration proved effective in increasing the activity of these antioxidant enzymes. Histopathological analysis confirmed that Anakinra might protect the brain tissue and nerve cells from injury.
CONCLUSION: Results demonstrate that Anakinra reduces the development of inflammation and tissue injury events associated with TBI.
Key words: Antioxidant; anakinra; interleukin-1; neuroprotection; traumatic brain injury.
potentially avoidable event. This secondary neuronal death is determined by a large number of cellular, molecular, and bio-chemical cascades. One such cascade thought to contribute to the evolution of this secondary damage is the local inflam-matory response in the injured brain tissue.[2] Microglial cells have been suggested to be the source of cytotoxic cytokines, such as tumor necrosis factor alpha (TNF-α) and interleukin 1β (IL-1β), killing oligodendrocytes. In fact, increased synthe-sis and/or secretion of IL-1β is detectable at the injury site within one h after spinal cord injury (SCI). IL-1β is a member of the interleukin 1 cytokine family. The gene encoding IL-1β, along with eight other IL-1 family genes, form a cytokine clus-ter on chromosome 2.[3] IL-1β is produced by activated mac-rophages as a pro-protein, which is proteolytically processed to its active form by caspase 1 (CASP1/ICE). This cytokine is an important mediator of the inflammatory response and involves in a variety of cellular activities, including cell prolif-eration, differentiation, and apoptosis.[3]
EXPERIMENTAL STUDY
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 1
Address for correspondence: Askin Esen Hasturk, M.D.
Onkoloji Eğitim ve Araştırma Hastanesi, Beyin ve Sinir Cerrahisi
Bölümü, 06200 Ankara, Turkey
Tel: +90 312 - 336 09 09 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):1-8doi: 10.5505/tjtes.2015.57894
Copyright 2015TJTES
INTRODUCTION
Traumatic brain injury (TBI) immediately causes direct me-chanical damage to the brain, referred to as the primary damage,[1] resulting in the immediate death of a number of neurons that cannot be recovered or regenerated. However, neurons continue to die for hours after TBI, representing a
Hasturk et al. Therapeutic evaluation of interleukin 1-beta antagonist Anakinra against traumatic brain injury in rats
IL-1 is produced in response to inflammatory stimuli and mediates various physiologic responses, including inflamma-tory and immunologic reactions. Anakinra, an antagonist ex-pressed in many tissues and organs, has been shown to com-petitively inhibit the binding of IL-1 to the IL-1 type receptor.[4] In patients with rheumatoid arthritis, this natural IL-1 receptor antagonist is not found in effective concentrations to counteract elevated IL-1 concentrations. Thus, Kineret is not considered a disease-modifying anti-rheumatic drug, but rather a biological response modifier due to its ability to se-lectively target the pathologic element of the disease.[5]
In the current study, the following endpoints of the inflam-matory response were determined: histological damage; cytokine expression (IL-1β); measurement of lipid peroxida-tion and oxidative stress (glutathione peroxidase, malondi-aldehyde, and superoxide dismutase) and these various fac-tors were used to evaluate whether Anakinra administration could protect brain tissue following traumatic brain injury.
MATERIALS AND METHODS
Fifty-four adult male Wistar albino rats weighing 300-350 g were used in this study. Animal care and all experiments were in accordance with the European Communities Council Di-rective of November 24, 1986 (86/609/EEC) on the protec-tion of animals for experimental use. All experimental pro-cedures used in this research were approved by the ethical committee of the Ministry of Health, Ankara Education and Research Hospital.
Surgical Procedure and Sample PreparationAll rats were kept under environmentally controlled condi-tions at 22-25°C with appropriate humidity, a 12-h light cycle, and free access to food and water. The surgical procedure was performed under general anesthesia induced by intra-peritoneal (IP) xylazine (10 mg/kg; Bayer, Istanbul, Turkey) and Ketamine hydrochloride (50 mg/kg; Parke-Davis, Istanbul, Turkey). A rectal probe was inserted and the animals were positioned on a heating pad in order to ensure that their body temperature was maintained at 37°C. A moderate brain-in-jury model, described by Marmarou et al. and modified by Ucar et al., was applied for head trauma.[6,7] Briefly, rats were placed in prone position and a midline incision was made on the head to expose the coronal and lambdoid sutures. A me-tallic disc in 10 mm diameter and 3 mm thickness was fixed to the cranium using bone wax, and a lead object weighing 450 g was allowed a free fall from a height of 70 cm through a copper tube onto the metal disc. The head of the animals was supported on a 10-cm foam bed providing confirmation of impact. After surgery, 1.0 cc of saline was subcutaneously administered to replace the blood volume lost during surgery and the wound was closed in layers with silk sutures. All ani-mals were anesthetized with the above-mentioned agents at 24 h after trauma and their brains were extracted without any
damage. Neural tissue samples were obtained by excising the left frontoparietal lobes from the boundary of the interhemi-spheric fissure and were subjected to biochemical analyses. The remaining parts of the brains were maintained in formal-dehyde solution for histopathological analysis.
Experimental GroupsRats were randomly allocated into the following 3 main groups and subgroups: Control: (n=18, 6 rats per time window); rats un-derwent skin incisions only and non-traumatic brain samples were obtained at the first, sixth and twenty-fourth h after surgery.
TBI + Saline: (n=18, 6 rats per time window); rats were sub-jected to TBI and received a single IP dose of 1 mL/kg saline. Traumatic brain tissue samples were obtained at the first, sixth and twenty-fourth h after surgery.
TBI + Anakinra: (n=18, 6 rats per time window); rats were subjected to TBI and received a single IP dose of Kineret (Anakinra, Swedish Orphan Biovitrum AB, Stockholm, Swe-den) immediately following TBI. Traumatic brain tissue sam-ples were then obtained at the first, sixth and twenty-fourth h after surgery.
Cytokine AssaySerum and tissue IL-1β concentrations were determined us-ing the double-antibody sandwich enzyme-linked immunosor-bent assay (R & D systems, Minneapolis, MN, USA) according to the manufacturer’s instructions.
Measurement of Lipid Peroxidation andOxidative StressGlutathione Peroxidase AnalysisGlutathione peroxidase (GSH-Px) activity was measured fol-lowing changes in NADPH absorbance at 340 nm.[8] In the activity calculations (IU, international unit), extinction coef-ficients of NADPH were used for GSH-Px. Results were ex-pressed as IU/mg protein.
Malondialdehyde AnalysisMalondialdehyde (MDA) is formed from the breakdown of polyunsaturated fatty acids and serves as an important and reliable index for determining the extent of peroxidation re-actions.[9] Tissue MDA levels were determined by a method based on a reaction with thiobarbituric acid (TBA). Briefly, samples were mixed with two volumes of cold saline solu-tion containing 0.001% butylated hydroxytoluene (BHT) (200 μl of 0.01% BHT solution in methanol) and 0.07% sodium dodecyl sulfate (SDS) (20 μl of 7% SDS). One ml of sample was then added to 500 μl of 0.01 NH2SO4 and 500 μl of the TBA reagent (0.67% TBA in 50% acetic acid) to precipitate protein. Samples were heated in boiling water for 60 min, and after cooling, an equal volume (2 ml) of n-butanol was added
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 12
Hasturk et al. Therapeutic evaluation of interleukin 1-beta antagonist Anakinra against traumatic brain injury in rats
to each test tube and mixed. The mixture was centrifuged at 4,000 rpm for 10 min at room temperature. The absor-bance of the organic layer in a 1-ml cell was read at 535 nm (Molecular Devices Corporation, Sunnyvale, CA, USA). MDA concentrations were expressed as nanomoles per milligram wet tissue weight.
Superoxide Dismutase Analysis Total superoxide dismutase (SOD) (Cu–Zn and Mn, EC 1.15.1.1) activity was determined according to the method of Sun et al.[10] The principle of the method is based on the inhibition of nitroblue tetrazolium (NBT) reduction by the xanthine–xanthine oxidase system as a superoxide generator. Activity was assessed in the ethanol phase of the supernatant after 1.0 ml ethanol/chloroform mixture (5/3, v/v) was added to the same volume of sample and centrifuged. One unit of SOD was defined as the enzyme amount causing 50% inhibi-tion in the NBT reduction rate. SOD activity was expressed as U/mg protein.
Catalase AnalysisCatalase (CAT) activity was determined by the method de-scribed by Aebi.[11] The principle of CAT activity is based on the determination of the rate constant (k, sec-1) or of the hydrogen peroxide decomposition rate at 240 nm. Results were expressed as kU/g of protein.
Histopathological ProceduresFor histological examination, brain tissue samples were fixed at 10% neutral buffered formalin, dehydrated through a graded series of ethanol and embedded in paraffin. 5μm thick sections stained with hematoxylin-eosin were analyzed and photographed with light microscopy (Olympus CX21, Olympus America Inc., Melville, NY, USA). In all groups, a semi quantitative scoring system, ranging between 0 and 3, was used for grading both histopathological changes (vascular congestion, PMNL infiltration, gliosis/satellitosis and spongio-sis) and neuronal degeneration signs (cytoplasmic eosinophil-ia and nuclear pyknosis) in the brain tissues of each animal. Histopathological changes were evaluated by two observers
blinded to the groups and scored as follows: 0: absent; 1: mild; 2: moderate; 3: common. Histopathological scores for each group was calculated averaging the scores of each animal in groups.[12]
Statistical AnalysisData were analyzed using the Statistical Package for Social Sciences (SPSS) software version 19.0 for Windows (SPSS Inc., Chicago, IL). Non-parametric tests were applied and the Mann-Whitney U test was used to compare two independent groups while the Kruskal-Wallis test was used to compare more than two groups. The Wilcoxon Signed Ranks Test was used to compare two dependent groups while the Friedman Test was used to compare more than two groups. Bonferroni correction for multiple tests was used for post-hoc compari-sons. All differences associated with a chance probability of 0.05 or less were considered statistically significant. Continu-ous variables were presented as mean±SD.
RESULTS
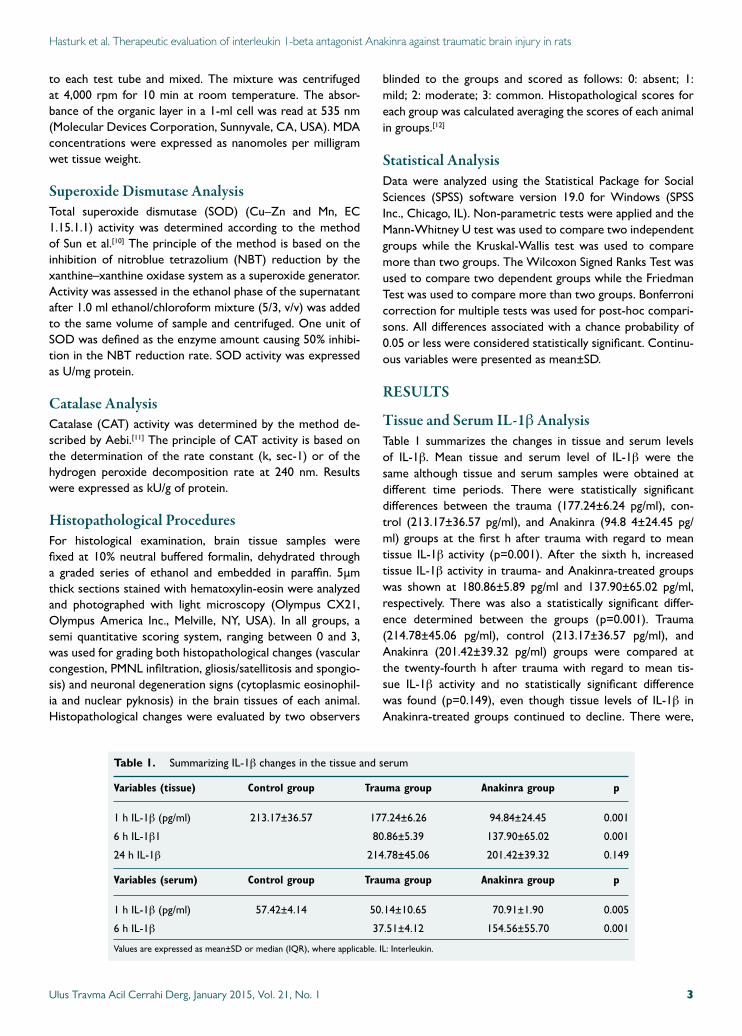
Tissue and Serum IL-1β AnalysisTable 1 summarizes the changes in tissue and serum levels of IL-1β. Mean tissue and serum level of IL-1β were the same although tissue and serum samples were obtained at different time periods. There were statistically significant differences between the trauma (177.24±6.24 pg/ml), con-trol (213.17±36.57 pg/ml), and Anakinra (94.8 4±24.45 pg/ml) groups at the first h after trauma with regard to mean tissue IL-1β activity (p=0.001). After the sixth h, increased tissue IL-1β activity in trauma- and Anakinra-treated groups was shown at 180.86±5.89 pg/ml and 137.90±65.02 pg/ml, respectively. There was also a statistically significant differ-ence determined between the groups (p=0.001). Trauma (214.78±45.06 pg/ml), control (213.17±36.57 pg/ml), and Anakinra (201.42±39.32 pg/ml) groups were compared at the twenty-fourth h after trauma with regard to mean tis-sue IL-1β activity and no statistically significant difference was found (p=0.149), even though tissue levels of IL-1β in Anakinra-treated groups continued to decline. There were,
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 3
Table 1. Summarizing IL-1β changes in the tissue and serum
Variables (tissue) Control group Trauma group Anakinra group p
1 h IL-1β (pg/ml) 213.17±36.57 177.24±6.26 94.84±24.45 0.001
6 h IL-1β1 80.86±5.39 137.90±65.02 0.001
24 h IL-1β 214.78±45.06 201.42±39.32 0.149
Variables (serum) Control group Trauma group Anakinra group p
1 h IL-1β (pg/ml) 57.42±4.14 50.14±10.65 70.91±1.90 0.005
6 h IL-1β 37.51±4.12 154.56±55.70 0.001
Values are expressed as mean±SD or median (IQR), where applicable. IL: Interleukin.
however, statistically significant differences between trauma (50.15±4.88 pg/ml), control (60.05±2.19 pg/ml) and Anakinra-treated (52.25±2.01 pg/ml) groups one h after trauma with regard to mean serum IL-1β activity (p=0.003). Additionally, six h after trauma, a statistically significant increase (p=0.001) in serum IL-1β activity was observed in the Anakinra-treated group (154.56±55.70 pg/ml).
Tissue and Serum MDA AnalysisMean tissue MDA levels in the trauma group were 7.16±1.02 nmol/mg, 11.66±2.94 nmol/mg, and 15.95±02.98 nmol/mg at the first, sixth and twenty-fourth h, respectively. Mean tis-sue levels in the Anakinra group were 7.20±4.39 nmol/mg, 11.46±4.00 nmol/mg, and 9.37±4.44 nmol/mg at the first, sixth and twenty-fourth h after trauma, respectively. A statistically significant difference was observed when mean serum MDA levels in trauma and Anakinra groups were compared with the control group (10.25±2.12 nmol/mg) at all time points (p=0.008). Mean serum MDA levels in the trauma groups were 0.10±0.04 nmol/mg and 0.07±0.04 nmol/mg at the first and sixth h, respectively. Mean tissue levels in the Anakinra group were 0.04±0.01 nmol/mg and 0.05±0.01 nmol/mg at
the fist and sixth h after trauma, respectively. A statistically significant difference was seen when mean serum MDA levels in trauma and Anakinra groups were compared with the con-trol group (0.04±0.01 nmol/mg) at all time-points (p=0.005) (Table 2).
Tissue and Serum GPx AnalysisMean tissue GPx levels at the first h following trauma for trauma (0.28±0.12 IU/mg), control (0.27±0.11 IU/mg), and Anakinra groups (0.21±0.25 IU/mg) were not significantly dif-ferent (p=0.899). Six hours following TBI, mean tissue GPx levels were 0.25±0.12 IU/mg in the trauma groups, 0.41±0.33 IU/mg in the Anakinra groups, and 0.27±0.11 IU/mg in the control group; there were no statistically significant differenc-es between groups at this time-point (p=0.05). After twenty-four h, mean tissue GPx continued to decline in the Anakinra-treated group (0.31±0.19 IU/mg), but this reduction was not determined to be statistically significant (p=0.189). Mean se-rum GPx levels in trauma groups were 0.0041±0.0007 IU/mg and 0.0033±0.002 IU/mg at the first and sixth h, respectively. The mean serum GPx levels in the Anakinra group were 0.0029±0.0011 IU/mg and 0.001±0.00 IU/mg at the first and
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 14
Hasturk et al. Therapeutic evaluation of interleukin 1-beta antagonist Anakinra against traumatic brain injury in rats
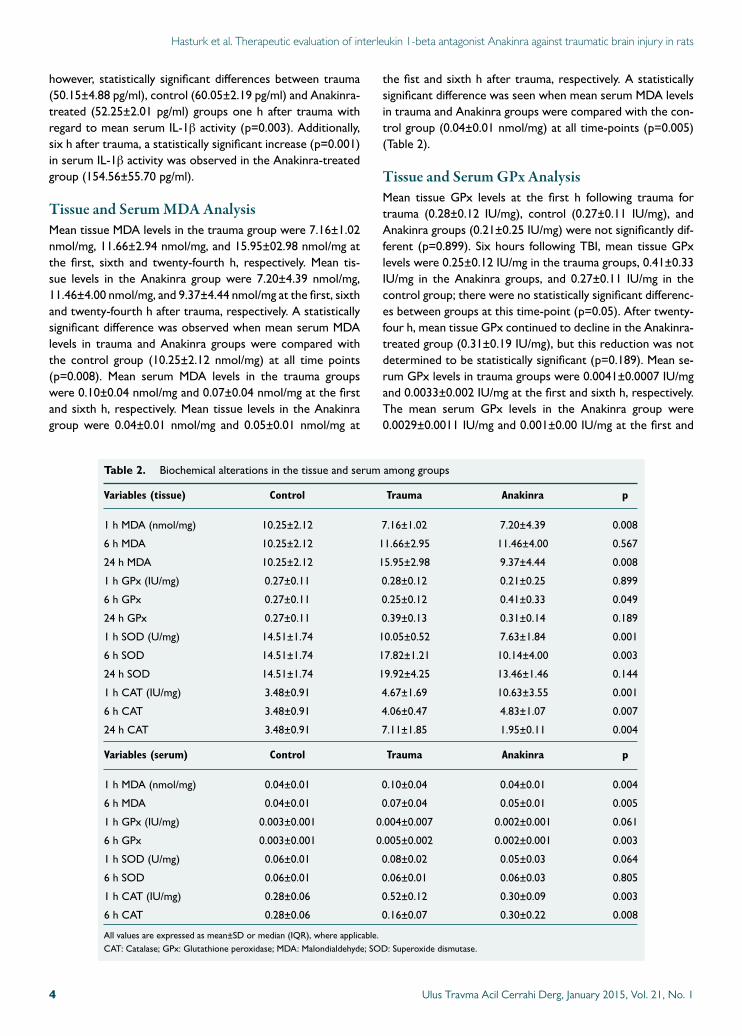
Table 2. Biochemical alterations in the tissue and serum among groups
Variables (tissue) Control Trauma Anakinra p
1 h MDA (nmol/mg) 10.25±2.12 7.16±1.02 7.20±4.39 0.008
6 h MDA 10.25±2.12 11.66±2.95 11.46±4.00 0.567
24 h MDA 10.25±2.12 15.95±2.98 9.37±4.44 0.008
1 h GPx (IU/mg) 0.27±0.11 0.28±0.12 0.21±0.25 0.899
6 h GPx 0.27±0.11 0.25±0.12 0.41±0.33 0.049
24 h GPx 0.27±0.11 0.39±0.13 0.31±0.14 0.189
1 h SOD (U/mg) 14.51±1.74 10.05±0.52 7.63±1.84 0.001
6 h SOD 14.51±1.74 17.82±1.21 10.14±4.00 0.003
24 h SOD 14.51±1.74 19.92±4.25 13.46±1.46 0.144
1 h CAT (IU/mg) 3.48±0.91 4.67±1.69 10.63±3.55 0.001
6 h CAT 3.48±0.91 4.06±0.47 4.83±1.07 0.007
24 h CAT 3.48±0.91 7.11±1.85 1.95±0.11 0.004
Variables (serum) Control Trauma Anakinra p
1 h MDA (nmol/mg) 0.04±0.01 0.10±0.04 0.04±0.01 0.004
6 h MDA 0.04±0.01 0.07±0.04 0.05±0.01 0.005
1 h GPx (IU/mg) 0.003±0.001 0.004±0.007 0.002±0.001 0.061
6 h GPx 0.003±0.001 0.005±0.002 0.002±0.001 0.003
1 h SOD (U/mg) 0.06±0.01 0.08±0.02 0.05±0.03 0.064
6 h SOD 0.06±0.01 0.06±0.01 0.06±0.03 0.805
1 h CAT (IU/mg) 0.28±0.06 0.52±0.12 0.30±0.09 0.003
6 h CAT 0.28±0.06 0.16±0.07 0.30±0.22 0.008
All values are expressed as mean±SD or median (IQR), where applicable.CAT: Catalase; GPx: Glutathione peroxidase; MDA: Malondialdehyde; SOD: Superoxide dismutase.
sixth h following TBI, respectively. A statistically significant difference was observed in mean serum GPx levels when the trauma and Anakinra groups were compared to the control group (0.0032±0.0013 IU/mg) at all time-points (p=0.003). However, there was no statistically significant difference in serum GPx levels between the three time-points of the Anakinra-treated groups (p=0.513) (Table 2).
Tissue and Serum Superoxide Dismutase AnalysisMean tissue SOD levels in the trauma groups were 10.05±0.52 U/mg, 17.82±7.11 U/mg, and 19.92 ± 4.25 nmol/mg at the first, sixth, and twenty-fourth h, respectively. The mean tis-sue SOD levels in the Anakinra group were 7.63±1.84 U/mg, 10.14±4.00 U/mg, and 13.46±1.46 U/mg at the first, sixth, and twenty-fourth h after trauma, respectively. Mean tissue SOD levels of the trauma and Anakinra groups were then compared with those of the control group (14.51±2.74 U/mg) and a statistically significant difference was found at all time-points (p=0.003). Mean serum SOD levels in the con-trol group were 0.08±0.02 U/mg and 0.08±0.01 U/mg at the first and sixth h after sham surgery, respectively. Mean serum SOD levels in the Anakinra group were 0.05±0.03 U/mg and
0.06±0.03 U/mg at the first and sixth h after trauma, respec-tively. When mean tissue SOD levels in trauma and Anakinra groups were compared with the control group (0.06±0.01 U/mg), no statistically significant differences were found be-tween groups at any of the time-points (p=0.805) (Table 2).
Tissue and Serum Catalase AnalysisMean tissue CAT levels in the trauma group were 4.67±1.69 IU/mg, 4.06±0.47 IU/mg, and 7.11±1.85 IU/mg at the first, sixth, and twenty-fourth h, respectively. Mean tissue CAT lev-els in the Anakinra group were 10.63±3.55 IU/mg, 4.83±1.07 IU/mg, and 1.95±0.11 IU/mg 1, 6, and 24 h after trauma, re-spectively. When mean tissue CAT levels in the trauma and Anakinra groups were compared with the control group (3.48±0.91 IU/mg), a statistically significant difference was found between groups at all time-points (p=0.004). Mean serum CAT levels in the trauma group were 0.52±0.12 IU/mg and 0.16±0.07 IU/mg at the first and sixth h, respectively. Mean serum CAT levels in the Anakinra group were 0.30±0.09 IU/mg and 0.30±0.26 IU/mg at the first and sixth h after trau-ma, respectively. No statistically significant difference was observed when CAT levels in the Anakinra group were com-
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 5
Hasturk et al. Therapeutic evaluation of interleukin 1-beta antagonist Anakinra against traumatic brain injury in rats
(a)
(c)
(b)
(d)
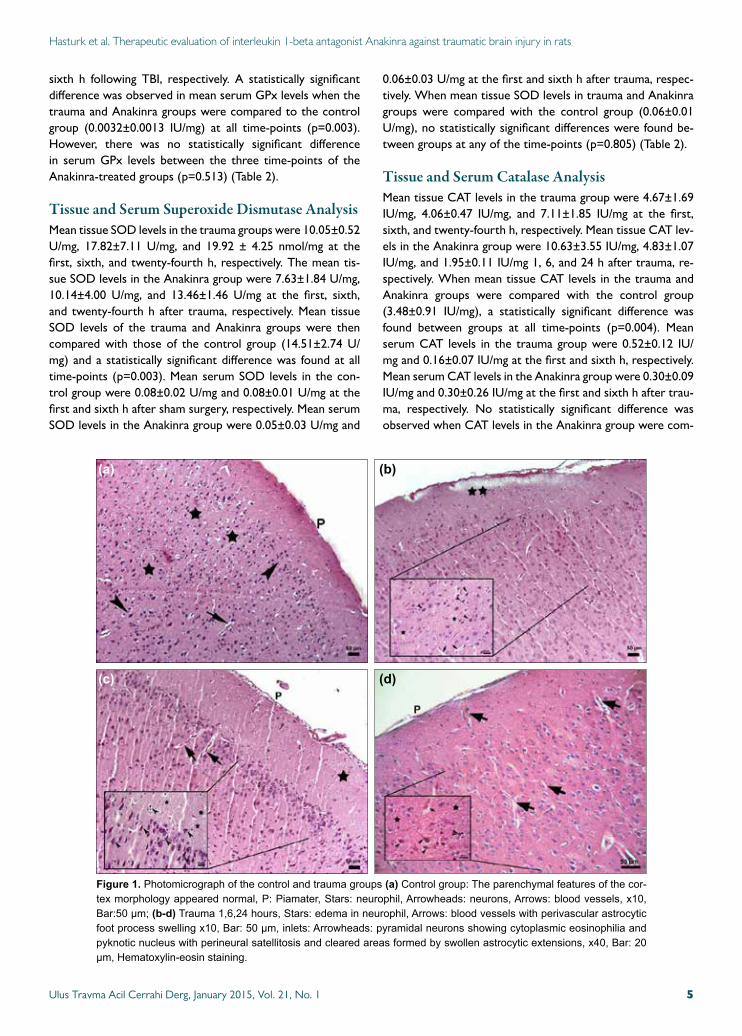
Figure 1. Photomicrographofthecontrolandtraumagroups(a)Controlgroup:Theparenchymalfeaturesofthecor-texmorphologyappearednormal,P:Piamater,Stars:neurophil,Arrowheads:neurons,Arrows:bloodvessels,x10,Bar:50µm;(b-d)Trauma1,6,24hours,Stars:edemainneurophil,Arrows:bloodvesselswithperivascularastrocyticfootprocessswellingx10,Bar:50µm,inlets:Arrowheads:pyramidalneuronsshowingcytoplasmiceosinophiliaandpyknoticnucleuswithperineuralsatellitosisandclearedareasformedbyswollenastrocyticextensions,x40,Bar:20µm,Hematoxylin-eosinstaining.
pared to serum levels in the control group (0.28±0.06 IU/mg) at any of the time-points (p=0.56) (Table 2).
Histopathological AssessmentAll rats of the control group showed no nerve tissue damage in the brain cortex. Neurons and neuroglia cells had normal morphologic features (Fig. 1a). In the first, sixth and twenty-fourth h trauma groups, cortical neurons showed cytoplas-mic eosinophilia so called eosinophilic neuron and pyknotic nucleus with no discernible nucleolus. Perineural satellitosis accumulating of more than one glia cell around eosinophilic neurons were also observed. The perineural and perivascular
spaces were prominent due to the swelling of astrocytic foot processes. In addition, blood vessels showed congestion and stasis. The fibrillary matrix of the cerebral cortex (neurophil) showed spongiosis due to the edema of cellular extensions of the neurons and glia cells (Fig. 1b-d). In the Anakinra ap-plied groups, first, sixth and twenty-fourth h after trauma also showed same signs of damage of nerve tissue including neu-rons and neurophil of the brain cortex (Figs. 2a-f ). Neuronal degeneration (eosinophilic neurons with pyknotic nucleus) and satellitosis scores of the Anakinra groups were found to be better than trauma groups at the sixth and twenty-fourth h. Moreover, vascular congestion scores were determined to
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 16
Hasturk et al. Therapeutic evaluation of interleukin 1-beta antagonist Anakinra against traumatic brain injury in rats
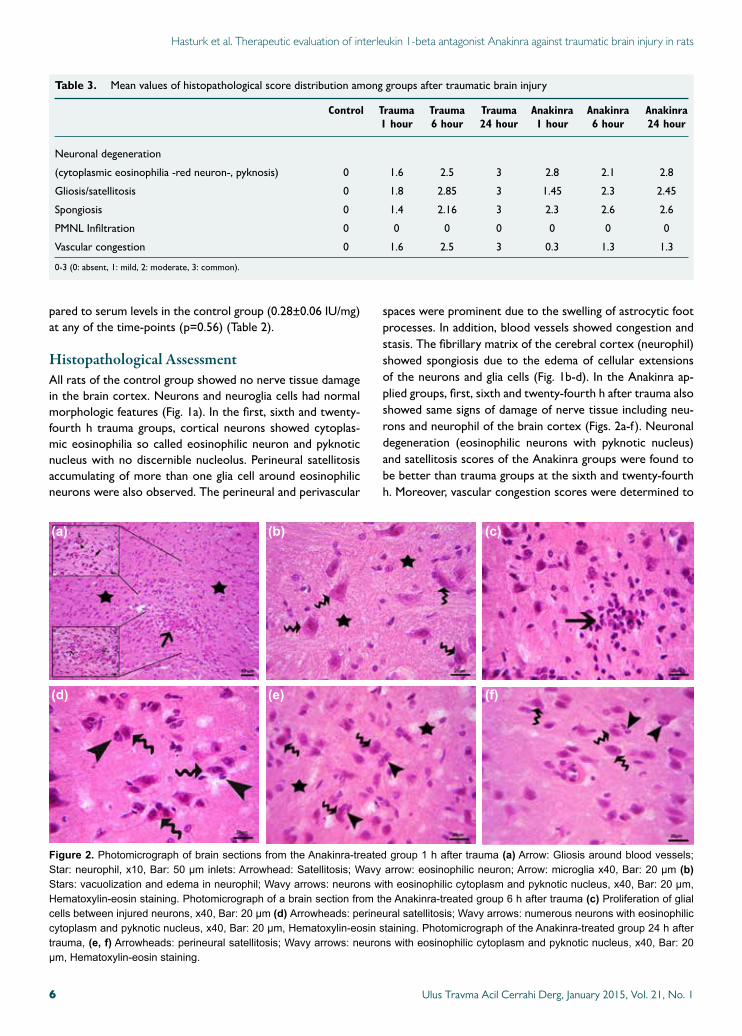
Table 3. Mean values of histopathological score distribution among groups after traumatic brain injury
Control Trauma Trauma Trauma Anakinra Anakinra Anakinra 1 hour 6 hour 24 hour 1 hour 6 hour 24 hour
Neuronal degeneration
(cytoplasmic eosinophilia -red neuron-, pyknosis) 0 1.6 2.5 3 2.8 2.1 2.8
Gliosis/satellitosis 0 1.8 2.85 3 1.45 2.3 2.45
Spongiosis 0 1.4 2.16 3 2.3 2.6 2.6
PMNL Infiltration 0 0 0 0 0 0 0
Vascular congestion 0 1.6 2.5 3 0.3 1.3 1.3
0-3 (0: absent, 1: mild, 2: moderate, 3: common).
Figure 2. PhotomicrographofbrainsectionsfromtheAnakinra-treatedgroup1haftertrauma(a)Arrow:Gliosisaroundbloodvessels;Star:neurophil,x10,Bar:50µminlets:Arrowhead:Satellitosis;Wavyarrow:eosinophilicneuron;Arrow:microgliax40,Bar:20µm(b) Stars:vacuolizationandedemainneurophil;Wavyarrows:neuronswitheosinophiliccytoplasmandpyknoticnucleus,x40,Bar:20µm,Hematoxylin-eosinstaining.PhotomicrographofabrainsectionfromtheAnakinra-treatedgroup6haftertrauma(c)Proliferationofglialcellsbetweeninjuredneurons,x40,Bar:20µm(d) Arrowheads:perineuralsatellitosis;Wavyarrows:numerousneuronswitheosinophiliccytoplasmandpyknoticnucleus,x40,Bar:20µm,Hematoxylin-eosinstaining.PhotomicrographoftheAnakinra-treatedgroup24haftertrauma,(e, f)Arrowheads:perineuralsatellitosis;Wavyarrows:neuronswitheosinophiliccytoplasmandpyknoticnucleus,x40,Bar:20µm,Hematoxylin-eosinstaining.
(a)
(d)
(b)
(e)
(c)
(f)

be lower than the trauma groups at all time points and PMNL infiltration was not seen in trauma and Anakinra groups at all time points (Table 3).
DISCUSSIONNeuronal damage is thought to continue for several days af-ter the initial ischemia expansion occurring within the first 24 h of TBI.[13] The expression of proinflammatory cytokines at the site of injury, including IL-1β and TNF-α, regulate precise cellular events that occur within the first few hours of TBI and persist in the neural tissue for several days with cytokines also being detectable on microglia, perivascular macrophages, and astrocytes.[14,15] Most important secondary factors leading to further neuronal death are lipid peroxidation, apoptosis, and development of reactive oxygen species.[16-20] In our study, cellular and biochemical changes were observed in order to assess the actual outcome of TBI in relation to short-term histological damage and cytokine expression. Fassbender et al. have analyzed trauma-induced release of IL-1β in brain tissue perfusates and reported that IL-1β was unexpectedly detected within 60 min of injury. Moreover, extracellularly se-creted IL-1β protein was found to gradually increase, peaking at day two, and decrease thereafter. Therefore, IL-1β release may represent a precondition for the orchestrating role of this mediator in the inflammatory response cascade.[21] In this study, we also demonstrated that serum and tissue levels of IL-1β were elevated at the sixth h after TBI. As shown in our results, Anakinra was found to be more effective in reducing tissue levels of IL-1β in the first h after trauma. This finding is not surprising since the release of IL-1β in brain tissue occurs within less than one h of trauma. Rothwell et al. have shown that neuronal inflammation, inducing pro-cytokine IL-1β, plays a key role in this process involving glial cells as well as in-vading immune cells. Moreover, induced cytokines have been suggested to indicate the extent of central nervous system in-jury.[14,22] In the present study, morphological features relevant with neuronal injury and higher histopathological scores fol-lowing brain trauma in rats were demonstrated. In contrast, administration of Anakinra led to an improvement of nerve tissue and cell morphology after TBI through a reduction in oxidative stress. Furthermore, this amelioration was revealed to be associated with decreased tissue and serum levels of IL-1β. On the contrary, no significant reduction in MDA was observed, indicating a lack of lipid peroxidation inhibition in brain sections and serum levels obtained from Anakinra-treated rats. This observation is in disagreement with a study conducted by Marini et al. demonstrating that inhibition of lipid peroxidation has reduced IL-1β expression and pro-tected neuronal tissue from damage.[20] Finally, the evalua-tion with light microscopy showed that the histopathological damage scores of neuronal degeneration, satellitosis, vascular congestion and spongiosis were reduced in rats treated with Anakinra at the twenty-fourth h after TBI. The findings of the current study suggested that IL-1β played a detrimental role in the development and severity of post-traumatic injury and
that this damaging effect could be attenuated by blocking this cytokine’s signaling pathway.
Treatment with Anakinra inhibits IL-1β and protects the brain tissue and neuronal cells from damage in TBI. However, a few of the possible mechanisms by which Anakinra attenu-ates neurological injury were demonstrated in this study and a better understanding of the mechanisms of Anakinra might lead to future clinical strategies aimed at treating TBI.
Conflict of interest: None declared.
REFERENCES
1. Yakovlev AG, Faden AI. Mechanisms of neural cell death: implications for development of neuroprotective treatment strategies. NeuroRx 2004;1:5-16.
2. Bartholdi D, Schwab ME. Methylprednisolone inhibits early inflamma-tory processes but not ischemic cell death after experimental spinal cord lesion in the rat. Brain Res 1995;672:177-86.
3. Hayashi M, Ueyama T, Nemoto K, Tamaki T, Senba E. Sequential mRNA expression for immediate early genes, cytokines, and neurotroph-ins in spinal cord injury. J Neurotrauma 2000;17:203-18.
4. Courcoul A, Vignot E, Chapurlat R. Successful treatment of Erdheim-Chester disease by interleukin-1 receptor antagonist protein. Joint Bone Spine 2014;81:175-7.
5. Nandi P, Kingsley GH, Scott DL. Disease-modifying antirheumatic drugs other than methotrexate in rheumatoid arthritis and seronegative arthritis. Curr Opin Rheumatol 2008;20:251-6.
6. Marmarou A, Foda MA, van den Brink W, Campbell J, Kita H, Deme-triadou K. A new model of diffuse brain injury in rats. Part I: Pathophysi-ology and biomechanics. J Neurosurg 1994;80:291-300.
7. Ucar T, Tanriover G, Gurer I, Onal MZ, Kazan S. Modified experimen-tal mild traumatic brain injury model. J Trauma 2006;60:558-65.
8. Paglia DE, Valentine WN. Studies on the quantitative and qualitative characterization of erythrocyte glutathione peroxidase. J Lab Clin Med 1967;70:158-69.
9. Tator CH, Fehlings MG. Review of the secondary injury theory of acute spinal cord trauma with emphasis on vascular mechanisms. J Neurosurg 1991;75:15-26.
10. Sun Y, Oberley LW, Li Y. A simple method for clinical assay of superoxide dismutase. Clin Chem 1988;34:497-500.
11. Aebi H, Wyss SR, Scherz B, Skvaril F. Heterogeneity of erythrocyte cata-lase II. Isolation and characterization of normal and variant erythrocyte catalase and their subunits. Eur J Biochem 1974;48:137-45.
12. Mena H, Cadavid D, Rushing EJ. Human cerebral infarct: a proposed histopathologic classification based on 137 cases. Acta Neuropathol 2004;108:524-30.
13. Yilmaz ER, Kertmen H, Gürer B, Kanat MA, Arikok AT, Ergüder BI, et al. The protective effect of 2-mercaptoethane sulfonate (MESNA) against traumatic brain injury in rats. Acta Neurochir (Wien) 2013;155:141-9.
14. Song C, Zhang Y, Dong Y. Acute and subacute IL-1β administrations differentially modulate neuroimmune and neurotrophic systems: possible implications for neuroprotection and neurodegeneration. J Neuroinflam-mation 2013;10:59.
15. Cheong CU, Chang CP, Chao CM, Cheng BC, Yang CZ, Chio CC. Etan-ercept attenuates traumatic brain injury in rats by reducing brain TNF-α contents and by stimulating newly formed neurogenesis. Mediators In-flamm 2013;2013:620837.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 7
Hasturk et al. Therapeutic evaluation of interleukin 1-beta antagonist Anakinra against traumatic brain injury in rats

Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 18
Hasturk et al. Therapeutic evaluation of interleukin 1-beta antagonist Anakinra against traumatic brain injury in rats
OLGU SUNUMU
İnterlökin 1-beta inhibitörü Anakinra’nın sıçanlarda travmatikbeyin hasarına karşı terapötik etkinliğinin değerlendirmesiDr. Aşkın Esen Hastürk,1 Dr. Erdal Reşit Yılmaz,2 Dr. Erhan Türkoğlu,2 Dr. Hayri Kertmen,2
Dr. Bahriye Horasanlı,3 Uzm. Bio. Nazlı Hayırlı,4 Dr. Imge Berrin Ergüder,5 Dr. Oya Evirgen4
1OnkolojiEğitimveAraştırmaHastanesi,BeyinveSinirCerrahisiBölümü,Ankara;2DışkapıYıldırımBeyazıtEğitimveAraştırmaHastanesi,BeyinveSinirCerrahisiBölümü,Ankara;3BaşkentÜniversitesiTıpFakültesi,NörolojiAnabilimDalı,Ankara;4AnkaraÜniversitesiTıpFakültesi,HistolojiveEmbriyolojiAnabilimDalı,Ankara;5AnkaraÜniversitesiTıpFakültesi,BiyokimyaAnabilimDalı,Ankara
AMAÇ: Bu çalışmanın amacı, deneysel travmatik beyin hasarı (TBH) modelinde interlökin 1 beta (IL-1β) inhibitörü Anakinra’nın tedavi edici etkin-liğinin değerlendirilmesidir.GEREÇ VE YÖNTEM: Elli dört Wistar albino sıçana anestezi uygulaması sonrası kafatası üzerine konan bir metal disk üzerine 2 metreden 450 g ağırlık düşürülerek deneysel kapalı kafa travması oluşturuldu. Hayvanlar üç ana gruba ayrıldı: Kontrol (n=18), TBH + salin (n=18; zaman başına altı hayvan) numuneler bir, altı ve 24 saat sonra alındı ve TBH + Anakinra (n=18; zaman başına altı hayvan) numuneler bir, altı ve 24 saat sonra alındı. IL-1β, malondialdehit, glutatyon peroksidaz, süperoksit dismutaz ve katalaz düzeylerinin analizi için beyin dokusu ve kan örnekleri alındı. Doku kesitleri histopatolojik olarak ışık mikroskobunda değerlendirildi.BULGULAR: Travma sonrası, doku ve serum IL-1β düzeyleri önemli ölçüde artmıştı ve bu düzeyler Anakinra verilmesinden sonra azaldı. TBH taki-ben glutatyon peroksidaz, süperoksit dismutaz ve katalaz aktivitesi azalmış ve Anakinra uygulanması bu antioksidan enzimlerin aktivitesini artırmada etkili olmuştur. Histopatolojik analiz Anakinra’nın beyin dokusu ve sinir hücrelerini travmadan koruyabileğini doğrulamıştır.TARTIŞMA: Anakinra’nın TBH ile ortaya çıkan enflamasyon ve doku hasarı gelişimini azalttığını göstermektedir.Anahtar sözcükler: Anakinra; antioksidan; interlökin-1; nöroproteksiyon; travmatik beyin hasarı.
Ulus Travma Acil Cerrahi Derg 2015;21(1):1-8 doi: 10.5505/tjtes.2015.57894
DENEYSEL ÇALIŞMA - ÖZET
16. Ates O, Cayli S, Altinoz E, Gurses I, Yucel N, Sener M, et al. Neuro-protection by resveratrol against traumatic brain injury in rats. Mol Cell Biochem 2007;294:137-44.
17. Awasthi D, Church DF, Torbati D, Carey ME, Pryor WA. Oxidative stress following traumatic brain injury in rats. Surg Neurol 1997;47:575-82.
18. Nishio S, Yunoki M, Noguchi Y, Kawauchi M, Asari S, Ohmoto T. De-tection of lipid peroxidation and hydroxyl radicals in brain contusion of rats. Acta Neurochir Suppl 1997;70:84-6.
19. Pineda JA, Wang KK, Hayes RL. Biomarkers of proteolytic damage fol-
lowing traumatic brain injury. Brain Pathol 2004;14:202-9.20. Marini H, Altavilla D, Bellomo M, Adamo EB, Marini R, Laureanti F, et
al. Modulation of IL-1 beta gene expression by lipid peroxidation inhibi-tion after kainic acid-induced rat brain injury. Exp Neurol 2004;188:178-86.
21. Fassbender K, Schneider S, Bertsch T, Schlueter D, Fatar M, Ragoschke A, et al. Temporal profile of release of interleukin-1beta in neurotrauma. Neurosci Lett 2000;284:135-8.
22. Rothwell N. Interleukin-1 and neuronal injury: mechanisms, modifica-tion, and therapeutic potential. Brain Behav Immun 2003;17:152-7.

Effects of alpha lipoic acid on intra-abdominal adhesion: an experimental study in a rat modelTülay Diken Allahverdi, M.D.,1 Ertuğrul Allahverdi, M.D.,2 Sadık Yayla, M.D.,3
Turgay Deprem, M.D.,4 Oguz Merhan, M.D.,5 Sevil Vural, M.D.,6
Barlas Sülü, M.D.,1 Yavuz Günerhan, M.D.,3 Neşet Köksal, M.D.1
1DepartmentofGeneralSurgery,KafkasUniversityFacultyofMedicine,Kars;2DepartmantofOrthopedicandTraumatology,KarsStateHospital,Kars;3DepartmentofSurgery,KafkasUniversityFacultyofVeterinary,Kars;4DepartmentofHistology,KafkasUniversityFacultyofVeterinary,Kars;5DepartmentofBiochemistry,KafkasUniversityFacultyofVeterinary,Kars;6DepartmentofPatology,AnkaraUniversityFacultyofVeterinary,Ankara
ABSTRACT
BACKGROUND: This study was performed to determine the effect of alpha lipoic acid, a powerful antioxidant, on intra-abdominal adhesion formation.
METHODS: Twenty-four female Wistar Albino rats weighing 250-300 g were used in this study conducted on three groups consist-ing of the alpha lipoic acid group (Group I, n=8), control group (Group II, n=8), and sham group (Group III, n=8). After performing laparotomy with a midline incision under general anesthesia, the adhesion model was created on the antimesenteric side of the caecum in Group I and Group II. 50 mg/kg alpha-lipoic acid was administered intraperitoneally (IP) in Group I while the surgical procedure was performed but no drugs administered in Group II. Only laparotomy was performed in Group III. Rats were sacrificed at the end of the tenth day.
RESULTS: Macroscopic scoring was performed, tissue samples were obtained and subjected to biochemical and histopathological evaluation. The degree of adhesion and malondialdehyde level decreased (p<0.01), and glutathione levels had increased (p<0.01) in Group I compared to Group II in macroscopic scoring.
CONCLUSION: Alpha lipoic acid was found to significantly decrease (p<0.01) intra-abdominal adhesion when administered IP com-pared to the control group.
Key words: Alpha lipoic acid; peritoneal adhesion; rat.
Although the use of barrier forming agents, such as fibrino-lytic agents, anticoagulants, anti-inflammatory agents, antibi-otics, surfactants, and seprafilm, are emphasized to prevent intra-abdominal adhesions, there is no totally effective meth-od or substance. The issue, therefore, remains current and studies continue.[6-9]
The alpha-lipoic acid molecule is oxidized and converted to dihydrolipoic acid (DHLA) during the first contact of alpha-lipoic acid (ALA), an antioxidant substance, with free radicals.[10-13] Alpha lipoic acid also has anti-inflammatory effects and increases the levels of glutathione (GSH), tocopherol, and other natural antioxidants as ascorbic acid. It can indirectly af-fect the continuity of the cellular antioxidant defense.[10] Due to its strong antioxidant nature, ALA has been reported to have positive effects in various pathological conditions such as diabetes, arteriosclerosis, neuron degeneration, multiple sclerosis, and joint diseases.[10,13] Özler et al.[1] have reported that oral ALA reduces oxidative stress and has beneficial ef-
EXPERIMENTAL STUDY
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 9
Address for correspondence: Tülay Diken Allahverdi, M.D.
Korupark Sitesi, H Blok, No: 10, 36100 Kars, Turkey
Tel: +90 474 - 225 11 50 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):9-14doi: 10.5505/tjtes.2015.15985
Copyright 2015TJTES
INTRODUCTION
Adhesion formation is frequently encountered after trauma or surgical procedures.[1-3] Postoperative intra-abdominal adhesion rates of 60-95% have been noted.[3] Postoperative adhesions can cause complications such as small bowel ob-struction, chronic pelvic pain, and infertility that may affect an individual’s quality of life.[2-5]
Diken Allahverdi et al. Effects of alpha lipoic acid on intra-abdominal adhesion: an experimental study in a rat model
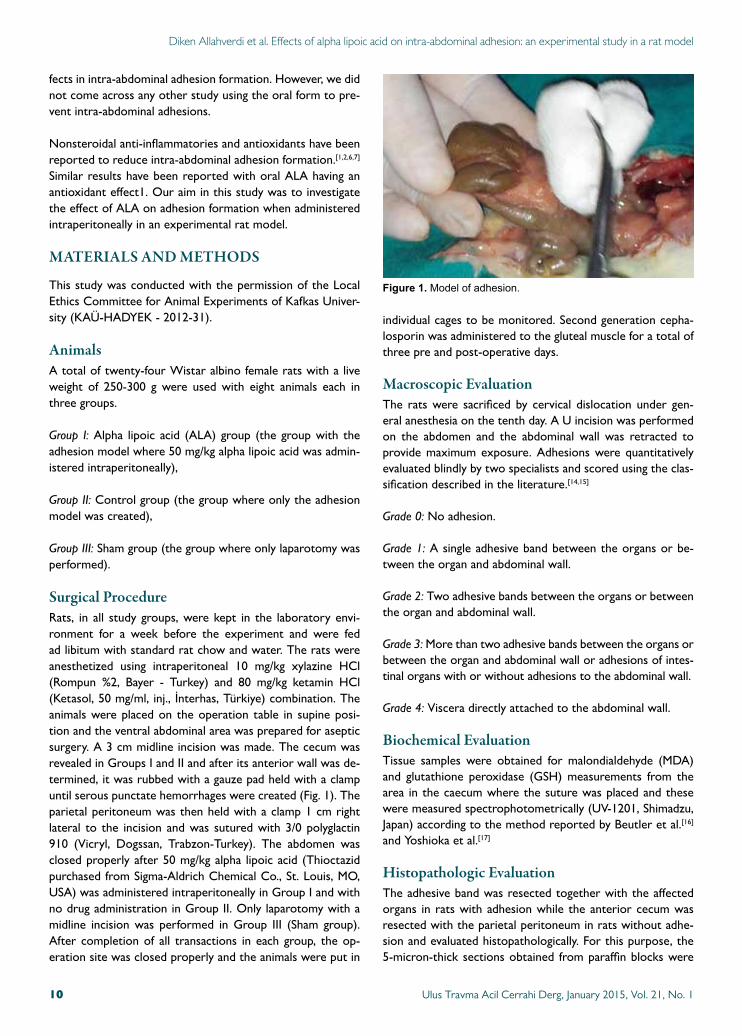
fects in intra-abdominal adhesion formation. However, we did not come across any other study using the oral form to pre-vent intra-abdominal adhesions.
Nonsteroidal anti-inflammatories and antioxidants have been reported to reduce intra-abdominal adhesion formation.[1,2,6,7] Similar results have been reported with oral ALA having an antioxidant effect1. Our aim in this study was to investigate the effect of ALA on adhesion formation when administered intraperitoneally in an experimental rat model.
MATERIALS AND METHODS
This study was conducted with the permission of the Local Ethics Committee for Animal Experiments of Kafkas Univer-sity (KAÜ-HADYEK - 2012-31).
AnimalsA total of twenty-four Wistar albino female rats with a live weight of 250-300 g were used with eight animals each in three groups.
Group I: Alpha lipoic acid (ALA) group (the group with the adhesion model where 50 mg/kg alpha lipoic acid was admin-istered intraperitoneally),
Group II: Control group (the group where only the adhesion model was created),
Group III: Sham group (the group where only laparotomy was performed).
Surgical ProcedureRats, in all study groups, were kept in the laboratory envi-ronment for a week before the experiment and were fed ad libitum with standard rat chow and water. The rats were anesthetized using intraperitoneal 10 mg/kg xylazine HCl (Rompun %2, Bayer - Turkey) and 80 mg/kg ketamin HCl (Ketasol, 50 mg/ml, inj., İnterhas, Türkiye) combination. The animals were placed on the operation table in supine posi-tion and the ventral abdominal area was prepared for aseptic surgery. A 3 cm midline incision was made. The cecum was revealed in Groups I and II and after its anterior wall was de-termined, it was rubbed with a gauze pad held with a clamp until serous punctate hemorrhages were created (Fig. 1). The parietal peritoneum was then held with a clamp 1 cm right lateral to the incision and was sutured with 3/0 polyglactin 910 (Vicryl, Dogssan, Trabzon-Turkey). The abdomen was closed properly after 50 mg/kg alpha lipoic acid (Thioctazid purchased from Sigma-Aldrich Chemical Co., St. Louis, MO, USA) was administered intraperitoneally in Group I and with no drug administration in Group II. Only laparotomy with a midline incision was performed in Group III (Sham group). After completion of all transactions in each group, the op-eration site was closed properly and the animals were put in
individual cages to be monitored. Second generation cepha-losporin was administered to the gluteal muscle for a total of three pre and post-operative days.
Macroscopic EvaluationThe rats were sacrificed by cervical dislocation under gen-eral anesthesia on the tenth day. A U incision was performed on the abdomen and the abdominal wall was retracted to provide maximum exposure. Adhesions were quantitatively evaluated blindly by two specialists and scored using the clas-sification described in the literature.[14,15]
Grade 0: No adhesion.
Grade 1: A single adhesive band between the organs or be-tween the organ and abdominal wall.
Grade 2: Two adhesive bands between the organs or between the organ and abdominal wall.
Grade 3: More than two adhesive bands between the organs or between the organ and abdominal wall or adhesions of intes-tinal organs with or without adhesions to the abdominal wall.
Grade 4: Viscera directly attached to the abdominal wall.
Biochemical EvaluationTissue samples were obtained for malondialdehyde (MDA) and glutathione peroxidase (GSH) measurements from the area in the caecum where the suture was placed and these were measured spectrophotometrically (UV-1201, Shimadzu, Japan) according to the method reported by Beutler et al.[16] and Yoshioka et al.[17]
Histopathologic EvaluationThe adhesive band was resected together with the affected organs in rats with adhesion while the anterior cecum was resected with the parietal peritoneum in rats without adhe-sion and evaluated histopathologically. For this purpose, the 5-micron-thick sections obtained from paraffin blocks were
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 110
Figure 1. Modelofadhesion.
Diken Allahverdi et al. Effects of alpha lipoic acid on intra-abdominal adhesion
stained with hematoxylin-eosin (H&E), evaluated under a light microscope (Leica DM4000B) and recorded (Leica DFC280). The grading of lesions was performed based on inflammatory and necrotic changes according to the scoring system below in ten different fields at the same magnification (H&Ex100).
(-) No lesion was found(+) Mild lesions (<10%)(++) Moderate lesions (10-50%)(+++) Severe lesions (<50%)
StatisticsSPSS18 software package was used for the statistical analysis of all data obtained from the study. Mean and standard de-
viations and the central distribution criteria were calculated for statistical analysis and the differences between nominal values of the groups were evaluated with Fisher’s definite chi-square test for the analysis of nonparametric data. P values <0.05 were considered significant. The significance between the two groups for parameters found to be statistically sig-nificant in the Kruskall-Wallis test was evaluated with the Mann-Whitney U test and P values <0.015 after Bonferroni correction were considered significant.
RESULTS
One animal each in Groups I and III and two animals in Group II died in the postoperative period and were not included into the evaluation.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 11
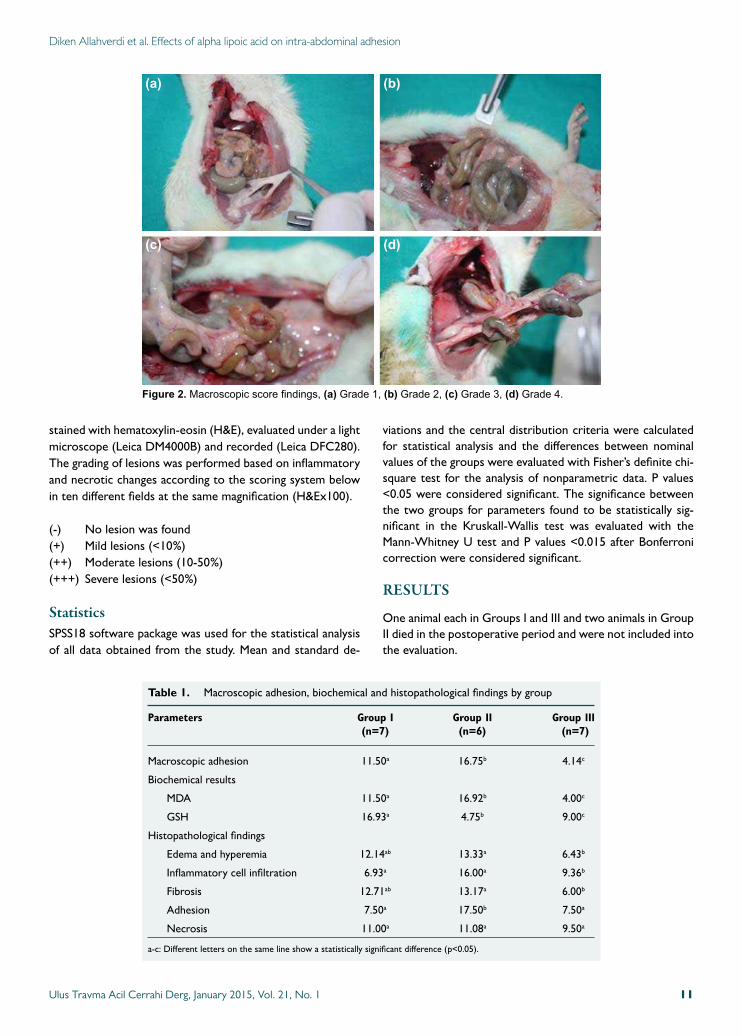
Figure 2. Macroscopicscorefindings,(a) Grade1,(b) Grade2,(c) Grade3,(d) Grade4.
(a)
(c)
(b)
(d)
Table 1. Macroscopic adhesion, biochemical and histopathological findings by group
Parameters Group I Group II Group III (n=7) (n=6) (n=7)
Macroscopic adhesion 11.50a 16.75b 4.14c
Biochemical results
MDA 11.50a 16.92b 4.00c
GSH 16.93a 4.75b 9.00c
Histopathological findings
Edema and hyperemia 12.14ab 13.33a 6.43b
Inflammatory cell infiltration 6.93a 16.00a 9.36b
Fibrosis 12.71ab 13.17a 6.00b
Adhesion 7.50a 17.50b 7.50a
Necrosis 11.00a 11.08a 9.50a
a-c: Different letters on the same line show a statistically significant difference (p<0.05).
Macroscopic EvaluationAll animals underwent relaparotomy to expose the abdominal cavity and evaluation was performed according to the NAIR scoring system (Fig. 2 a-d). A statistically significant lower val-ue was found in Group I than in Group II (p<0.05) (Table 1).
Biochemical ResultsA significant difference was found between the groups in terms of MDA and GSH (p<0.05). A significant decrease was found in Group I compared to Group II in terms of MDA (p<0.05). GSH was higher in Group I compared to both Groups II and III.
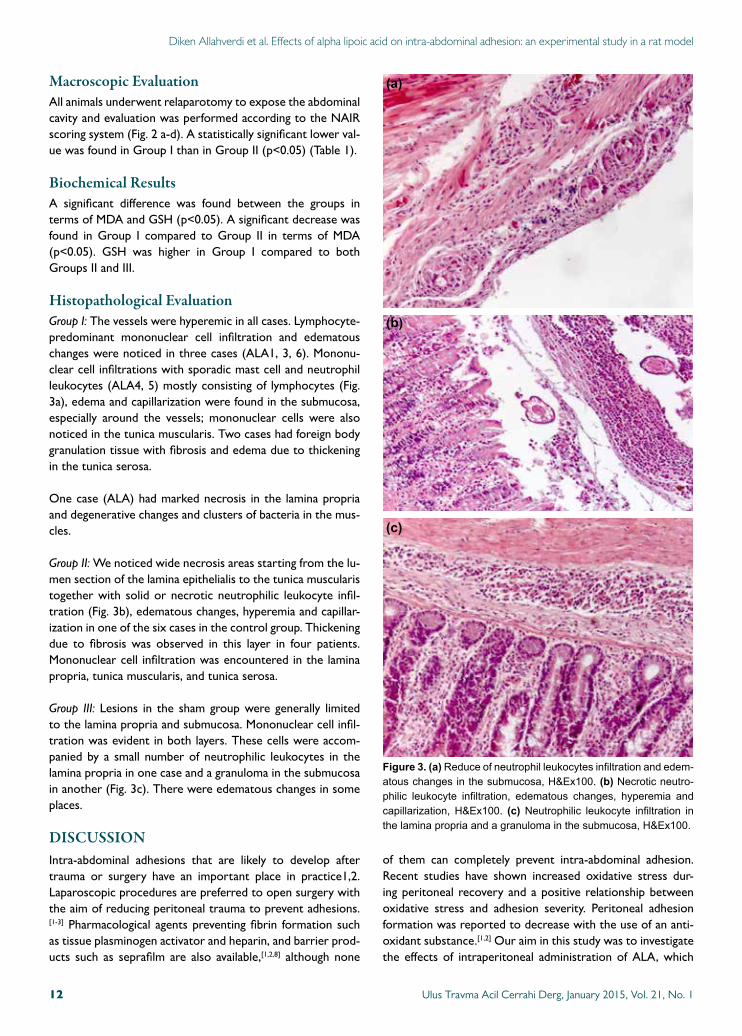
Histopathological EvaluationGroup I: The vessels were hyperemic in all cases. Lymphocyte-predominant mononuclear cell infiltration and edematous changes were noticed in three cases (ALA1, 3, 6). Mononu-clear cell infiltrations with sporadic mast cell and neutrophil leukocytes (ALA4, 5) mostly consisting of lymphocytes (Fig. 3a), edema and capillarization were found in the submucosa, especially around the vessels; mononuclear cells were also noticed in the tunica muscularis. Two cases had foreign body granulation tissue with fibrosis and edema due to thickening in the tunica serosa.
One case (ALA) had marked necrosis in the lamina propria and degenerative changes and clusters of bacteria in the mus-cles.
Group II: We noticed wide necrosis areas starting from the lu-men section of the lamina epithelialis to the tunica muscularis together with solid or necrotic neutrophilic leukocyte infil-tration (Fig. 3b), edematous changes, hyperemia and capillar-ization in one of the six cases in the control group. Thickening due to fibrosis was observed in this layer in four patients. Mononuclear cell infiltration was encountered in the lamina propria, tunica muscularis, and tunica serosa.
Group III: Lesions in the sham group were generally limited to the lamina propria and submucosa. Mononuclear cell infil-tration was evident in both layers. These cells were accom-panied by a small number of neutrophilic leukocytes in the lamina propria in one case and a granuloma in the submucosa in another (Fig. 3c). There were edematous changes in some places.
DISCUSSIONIntra-abdominal adhesions that are likely to develop after trauma or surgery have an important place in practice1,2. Laparoscopic procedures are preferred to open surgery with the aim of reducing peritoneal trauma to prevent adhesions.[1-3] Pharmacological agents preventing fibrin formation such as tissue plasminogen activator and heparin, and barrier prod-ucts such as seprafilm are also available,[1,2,8] although none
of them can completely prevent intra-abdominal adhesion. Recent studies have shown increased oxidative stress dur-ing peritoneal recovery and a positive relationship between oxidative stress and adhesion severity. Peritoneal adhesion formation was reported to decrease with the use of an anti-oxidant substance.[1,2] Our aim in this study was to investigate the effects of intraperitoneal administration of ALA, which
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 112
Diken Allahverdi et al. Effects of alpha lipoic acid on intra-abdominal adhesion: an experimental study in a rat model
Figure 3. (a)Reduceofneutrophilleukocytesinfiltrationandedem-atouschangesinthesubmucosa,H&Ex100.(b) Necroticneutro-philic leukocyte infiltration, edematous changes, hyperemia andcapillarization,H&Ex100. (c) Neutrophilic leukocyte infiltration inthelaminapropriaandagranulomainthesubmucosa,H&Ex100.
(a)
(b)
(c)

has an antioxidant effect, on intra-abdominal adhesion forma-tion.
The powerful biological antioxidant ALA can be used orally or intraperitoneally.[1,10] Özler et al.[1] have reported that ALA decreases adhesion when administered orally at a dose of 100 mg/kg. Ozbal et al.[10] have also stated high dose as a single intraperitoneal dose of 100 mg/kg. Testicular ischemia and reperfusion injury have been reduced by ALA as well in that study. Our aim was to determine whether ALA, given at high doses in the other two studies and shown to have anti-inflam-matory and antioxidant effects, had any effect on adhesion when administered at a lower dose (50 mg/kg). Drugs have side effects in addition to therapeutic effects therefore the lowest therapeutic dose should be administered to decrease the incidence of side effects. ALA reaches its peak concen-tration thirty minutes to two hours after administration and is rapidly metabolized. Since inflammation starts in minutes after surgical trauma, the drug should reach an effective con-centration at the moment of injury.[18,19] ALA was adminis-tered intraoperatively in our study.
Alleva et al. have shown with various parameters that ALA has positive effects on wound healing.[20] Lipoic acid has also been shown to regulate angiogenesis in many studies,[21] de-creasing adhesion formation. Özler et al. have evaluated mac-roscopic adhesion with alpha lipoic acid by administering the drug in oral form and found adhesion to be decreased. Mac-roscopic adhesion evaluation of our study showed that the IP use of ALA significantly decreased adhesion compared to the control group. It is to our belief that ALA continues to exert positive effects when administered through the IP route.
MDA level indicates the presence of lipid peroxidation due to free oxygen radicals produced in tissues after ischemia and has been shown to increase after peritoneal adhesion and de-crease with antioxidant use.[1,2] MDA level was found to show a significant decrease in the group administered with ALA compared to the control group in our study. This decrease had a course close to the sham group.
When ischemic damage occurs, glutathione is consumed through conjugation and the intracellular glutathione level is consequently reduced. The decrease in the amount of glu-tathione is compensated by exogenous GSH intake. When oxidative stress increases, a decrease in glutathione occurs. When oxidative stress decreases, an increase is observed in the glutathione level.[22] ALA has been shown to increase glu-tathione levels and decrease cell death in a study conducted by Rocamonde et al.[21] A significant increase in the GSH level was found in the group where antioxidant was administered compared to the control group. This increase was close to the level of the sham group. The increase of MDA level and decrease of GSH level in the group where ALA was adminis-tered is one more indicator that ALA is a powerful antioxi-dant.
Lin et al.[13] have reported a decrease in edema and hyper-emia, inflammation, fibrosis and alveolar wall thickness in acute lung trauma with the use of ALA. The author links this effect of ALA to the decreased release of the proinflamma-tory cytokines and its anti-inflammatory effect. A significant decrease was seen in edema and hyperemia, inflammation, fibrosis and adhesion in the drug-treated group compared to the control group in the microscopic evaluation of our study. However, no significant difference was seen in the necrosis rate between the groups. As Lin et al.[13] has stated, it is pos-sible to link the significant decrease in all microscopic vales evaluated to a reduction in the secretion of cytokines and anti-inflammatory effect of ALA.
ALA, a naturally occurring thiol antioxidant, is used to pre-vent hepatic fibrosis in clinical practice and can also be used to prevent submucous fibrosis and peritoneal adhesion with oral use.[23] Low doses of intraperitoneal ALA was found to prevent intraabdominal adhesion due to the effects similar to those reported in the literature,[10-13] indicating the lack of a difference between low and high doses in terms of decreasing adhesion. Determining the lowest dose of ALA that is effec-tive in preventing intraabdominal adhesions requires further studies.
Conflict of interest: None declared.
REFERENCES
1. Özler M, Ersöz N, Özerhan İH, Topal T, Öter Ş, Korkmaz A. The ef-fect of alpha-lipoic acid in the prevention of peritoneal adhesions. Turk J Gastroenterol 2011;22:190-4.
2. Celeplı S, Kismet K, Kaptanoğlu B, Erel S, Ozer S, Celeplı P, et al. The ef-fect of oral honey and pollen on postoperative intraabdominal adhesions. Turk J Gastroenterol 2011;22:65-72.
3. Kirdak T, Uysal E, Korun N. Assessment of effectiveness of different dos-es of methylprednisolone on intraabdominal adhesion prevention. Ulus Travma Acil Cerrahi Derg 2008;14:188-91.
4. Müller SA, Treutner KH, Tietze L, Anurov M, Titkova S, Polivoda M, et al. Efficacy of adhesion prevention and impact on wound healing of intraperitoneal phospholipids. J Surg Res 2001;96:68-74.
5. Saed GM, Munkarah AR, Diamond MP. Cyclooxygenase-2 is expressed in human fibroblasts isolated from intraperitoneal adhesions but not from normal peritoneal tissues. Fertil Steril 2003;79:1404-8.
6. Guvenal T, Cetin A, Ozdemir H, Yanar O, Kaya T. Prevention of post-operative adhesion formation in rat uterine horn model by nimesulide: a selective COX-2 inhibitor. Hum Reprod 2001;16:1732-5.
7. Cofer KF, Himebaugh KS, Gauvin JM, Hurd WW. Inhibition of adhesion reformation in the rabbit model by meclofenamate: an in-hibitor of both prostaglandin and leukotriene production. Fertil Steril 1994;62:1262-5.
8. Inoue M, Uchida K, Otake K, Nagano Y, Ide S, Hashimoto K, et al. Ef-ficacy of Seprafilm for preventing adhesive bowel obstruction and cost-benefit analysis in pediatric patients undergoing laparotomy. J Pediatr Surg 2013;48:1528-34.
9. Golan A, Maymon R, Winograd I, Bukovsky I. Prevention of post-sur-gical adhesion formation using aspirin in a rodent model: a preliminary report. Hum Reprod 1995;10:1797-800.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 13
Diken Allahverdi et al. Effects of alpha lipoic acid on intra-abdominal adhesion

10. Ozbal S, Ergur BU, Erbil G, Tekmen I, Bagrıyanık A, Cavdar Z. The effects of α-lipoic acid against testicular ischemia-reperfusion injury in Rats. ScientificWorldJournal 2012;2012:489248.
11. Moini H, Packer L, Saris NE. Antioxidant and prooxidant activities of alpha-lipoic acid and dihydrolipoic acid. Toxicol Appl Pharmacol 2002;182:84-90.
12. Kiemer AK, Müller C, Vollmar AM. Inhibition of LPS-induced nitric oxide and TNF-alpha production by alpha-lipoic acid in rat Kupffer cells and in RAW 264.7 murine macrophages. Immunol Cell Biol 2002;80:550-7.
13. Lin YC, Lai YS, Chou TC. The protective effect of alpha-lipoic Acid in lipopolysaccharide-induced acute lung injury is mediated by heme oxy-genase-1. Evid Based Complement Alternat Med 2013;2013:590363.
14. Galili Y, Ben-Abraham R, Rabau M, Klausner J, Kluger Y. Reduction of surgery-induced peritoneal adhesions by methylene blue. Am J Surg 1998;175:30-2.
15. Hemadeh O, Chilukuri S, Bonet V, Hussein S, Chaudry IH. Prevention of peritoneal adhesions by administration of sodium carboxymethyl cel-lulose and oral vitamin E. Surgery 1993;114:907-10.
16. Beutler E, Duron O, Kelly BM. Improved method for the determination of blood glutathione. J Lab Clin Med 1963;61:882-8.
17. Yoshioka T, Kawada K, Shimada T, Mori M. Lipid peroxidation in ma-
ternal and cord blood and protective mechanism against activated-oxygen toxicity in the blood. Am J Obstet Gynecol 1979;135:372-6.
18. Liebman SM, Langer JC, Marshall JS, Collins SM. Role of mast cells in peritoneal adhesion formation. Am J Surg 1993;165:127-30.
19. Siegler AM, Kontopoulos V, Wang CF. Prevention of postoperative adhe-sions in rabbits with ibuprofen, a nonsteroidal anti-inflammatory agent. Fertil Steril 1980;34:46-9.
20. Alleva R, Tomasetti M, Sartini D, Emanuelli M, Nasole E, Di Donato F, et al. alpha-Lipoic acid modulates extracellular matrix and angiogenesis gene expression in non-healing wounds treated with hyperbaric oxygen therapy. Mol Med 2008;14:175-83.
21. Rocamonde B, Paradells S, Barcia JM, Barcia C, García Verdugo JM, Mi-randa M, et al. Neuroprotection of lipoic acid treatment promotes angio-genesis and reduces the glial scar formation after brain injury. Neurosci-ence 2012;224:102-15.
22. Jaeschke H. Molecular mechanisms of hepatic ischemia-reperfusion injury and preconditioning. Am J Physiol Gastrointest Liver Physiol 2003;284:G15-26.
23. Kaya M, Yildirim CH, Kosemehmetoglu K, Huseyinoglu U, Erdogan H, Akbasak A, et al. Alpha-lipoic acid reduces peridural fibrosis after laminectomy of lumbar vertebrae in rabbits. Acta Neurochir (Wien) 2012;154:1241-5.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 114
Diken Allahverdi et al. Effects of alpha lipoic acid on intra-abdominal adhesion: an experimental study in a rat model
OLGU SUNUMU
Alfa lipoik asitin intraabdominal adezyon üzerine etkileri:Sıçan modelinde deneysel bir çalışmaDr. Tülay Diken Allahverdi,1 Dr. Ertuğrul Allahverdi,2 Dr. Sadık Yayla,3 Dr. Turgay Deprem,4
Dr. Oguz Merhan,5 Dr. Sevil Vural,6 Dr. Barlas Sülü,1 Dr. Yavuz Günerhan,3 Dr. Neşet Köksal1
1KafkasÜniversitesiTıpFakültesi,GenelCerrahiAnabilimDalı,Kars;2KarsDevletHastanesi,OrtopediveTravmatolojiKliniği,Kars;3KafkasÜniversitesiVeterinerFakültesi,CerrahiAnabilimDalı,Kars;4KafkasÜniversitesiVeterinerFakültesi,HistolojiAnabilimDalı,Kars;5KafkasÜniversitesiVeterinerFakültesi,BiyokimyaAnabilimDalı,Kars;6AnkaraÜniversitesiVeterinerFakültesi,PatolojiAnabilimDalı,Ankara
AMAÇ: Çalışma, güçlü bir antioksidan olan alfa lipoik asidin intraabdominal adezyon oluşumu üzerine olan etkisini saptamak amacıyla yapıldı.GEREÇ VE YÖNTEM: Alfa lipoik asit grubu (Grup I), kontrol grubu (Grup II, n=8) ve Sham grubu (Grup III, n=8) olmak üzere üç grup üzerinde yürütülen bu çalışmada 250-300 g canlı ağırlığında olan Wistar Albino cinsi 24 adet dişi sıçan kullanıldı. Genel anestezisi eşliğinde orta hat insizyonuyla laparotomi yapıldıktan sonra Grup I ve Grup II’de çekumun antimezenterik tarafında adezyon modeli oluşturuldu. Grup I’e 50 mg/kg alfa lipoik asid intraperitoneal (IP) olarak verilirken Grup II’de cerrahi işlem yapıldı fakat herhangi bir ilaç uygulanmadı. Grup III’te ise sadece laparatomi yapıldı. Sıçanlar 10. gün sonunda sakrifiye edilip makroskopik skorlama yapıldı ve doku örnekleri alınarak biyokimyasal ve histopatolojik değerlendirmeye tabi tutuldu.BULGULAR: Makroskopik skorlamada ve histopatolojik incelemede Grup I’de, Grup II’ye göre adezyon derecesinin ve malondialdehid düzeyinin azaldığı (p<0.01), glutation düzeyinin ise arttığı (p<0.01) tespit edildi.TARTIŞMA: Çalışma bulguları, alfa lipoik asidin IP olarak uygulandığında intraabdominal adezyonu kontrol grubuna göre belirgin derecede azalttığı (p<0.01) tespit edildi.Anahtar sözcükler: Alfa lipoik asid; peritoneal adezyon; sıçan.
Ulus Travma Acil Cerrahi Derg 2015;21(1):9-14 doi: 10.5505/tjtes.2015.15985
DENEYSEL ÇALIŞMA - ÖZET
Spontaneous regeneration capacity of controlled small bowel perforations: an experimental study in ratsÖzgür Pekel, M.D.,1 Sinan Hatipoglu, M.D.,2 Ahmet Nuray Turhan, M.D.,3
Filiz Hatipoglu, M.D.,4 Ruslan Abdullayev, M.D.,5 Süha Göksel, M.D.6
1DepartmentofGeneralSurgeryUnit,SevketYilmazTrainingandResearchHospital,Bursa;2DepartmentofGeneralSurgeryUnit,AdiyamanUniversityFacultyofMedicine,Adiyaman;3DepartmentofGeneralSurgeryUnit,IstanbulCerrahiHospital,Istanbul;4DepartmentofObstetricsandGynecologyUnit,AdiyamanUniversityFacultyofMedicine,Adiyaman;5DepartmentofAnesthesiologyandReanimationUnit,AdiyamanUniversityFacultyofMedicine,Adiyaman;6DepartmentofPathologyUnit,Acibadem(Maslak)Hospital,Istanbul
ABSTRACT
BACKGROUND: Selective observation method has started to replace routine laparotomy application for abdominal penetrating trauma patients after Shaftan’s selective observation method applied in the 1960s. In this respect, there is a possibility of bowel perfo-rations healing without operations. An experimental model was established in this study in order to clarify this possibility.
METHODS: Fifty Wistar-Albino rats were divided into five groups, ten in each. While one group served as the control, distal part of the small bowel of the rats in the other four groups was perforated 1, 2, 3, and 4 mm in diameter with appropriate cutters. After a week of observation, test rats were sacrificed and relaparotomy was applied. The test material consisting of the perforated bowel, covering 1 cm of proximal and distal margins, and some peritoneal tissue was taken for histopathological examination.
RESULTS: Small bowel perforations with a diameter of 2 mm or below healed spontaneously without any operation. Peritonitis intensity increased in direct ratio with perforation diameters. Wall repair capacity of the bowel diminished with increasing perforation diameters.
CONCLUSION: It was observed that small perforations in the small bowel of rats could be limited by the organism itself without a necessity of any surgical intervention.
Key words: Experimental study; penetrating abdominal trauma; small bowel perforation; spontaneous regeneration.
with penetrating abdominal trauma has made the treatment of these patients possible without surgery with the help of developing diagnostic methods. Basic clinical approach to penetrating stab wounds has changed with Shaftan’s selec-tive observation method applied in the 1960s.[1] After the introduction of selective observation method, it has started to replace routine laparotomy application in penetrating ab-dominal trauma patients all over the world. This method has diminished both negative laparotomy rates and morbidity caused by negative laparotomy.[2-7]
Besides the advantages of selective observation, it has also arisen some questions. One of these questions is the pres-ence of a healing chance of a perforated small bowel without surgical intervention. Retrospective analysis of patients with penetrated abdominal trauma has shown that small bowel wound ratio is found to be higher in clinics using routine laparotomy compared to those using selective observation method.[2-5] Therefore, there can be a possibility of spontane-
EXPERIMENTAL STUDY
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 15
Address for correspondence: Sinan Hatipoglu, M.D.
Adıyaman Üniversitesi Tıp Fakültesi, Genel Cerrahi Anabilim Dalı,
02040 Adıyaman, Turkey
Tel: +90 505 - 450 94 02 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):15-21doi: 10.5505/tjtes.2015.31369
Copyright 2015TJTES
INTRODUCTION
Developing technology and knowledge of the diagnosis and treatment of patients with penetrating abdominal stab wounds have led to major changes regarding the clinical ap-proach to these patients. In the past, every case with a com-plaint of penetrating abdominal trauma underwent routine operation. Selective observation method in selected patients
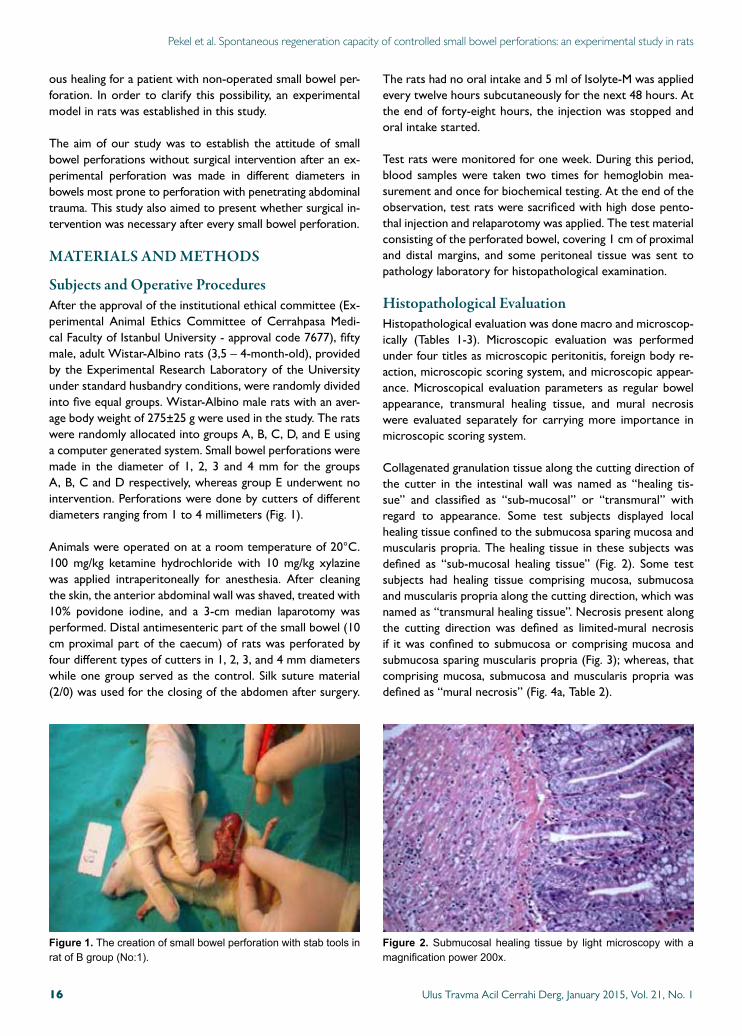
Pekel et al. Spontaneous regeneration capacity of controlled small bowel perforations: an experimental study in rats
ous healing for a patient with non-operated small bowel per-foration. In order to clarify this possibility, an experimental model in rats was established in this study.
The aim of our study was to establish the attitude of small bowel perforations without surgical intervention after an ex-perimental perforation was made in different diameters in bowels most prone to perforation with penetrating abdominal trauma. This study also aimed to present whether surgical in-tervention was necessary after every small bowel perforation.
MATERIALS AND METHODS
Subjects and Operative ProceduresAfter the approval of the institutional ethical committee (Ex-perimental Animal Ethics Committee of Cerrahpasa Medi-cal Faculty of Istanbul University - approval code 7677), fifty male, adult Wistar-Albino rats (3,5 – 4-month-old), provided by the Experimental Research Laboratory of the University under standard husbandry conditions, were randomly divided into five equal groups. Wistar-Albino male rats with an aver-age body weight of 275±25 g were used in the study. The rats were randomly allocated into groups A, B, C, D, and E using a computer generated system. Small bowel perforations were made in the diameter of 1, 2, 3 and 4 mm for the groups A, B, C and D respectively, whereas group E underwent no intervention. Perforations were done by cutters of different diameters ranging from 1 to 4 millimeters (Fig. 1).
Animals were operated on at a room temperature of 20°C. 100 mg/kg ketamine hydrochloride with 10 mg/kg xylazine was applied intraperitoneally for anesthesia. After cleaning the skin, the anterior abdominal wall was shaved, treated with 10% povidone iodine, and a 3-cm median laparotomy was performed. Distal antimesenteric part of the small bowel (10 cm proximal part of the caecum) of rats was perforated by four different types of cutters in 1, 2, 3, and 4 mm diameters while one group served as the control. Silk suture material (2/0) was used for the closing of the abdomen after surgery.
The rats had no oral intake and 5 ml of Isolyte-M was applied every twelve hours subcutaneously for the next 48 hours. At the end of forty-eight hours, the injection was stopped and oral intake started.
Test rats were monitored for one week. During this period, blood samples were taken two times for hemoglobin mea-surement and once for biochemical testing. At the end of the observation, test rats were sacrificed with high dose pento-thal injection and relaparotomy was applied. The test material consisting of the perforated bowel, covering 1 cm of proximal and distal margins, and some peritoneal tissue was sent to pathology laboratory for histopathological examination.
Histopathological EvaluationHistopathological evaluation was done macro and microscop-ically (Tables 1-3). Microscopic evaluation was performed under four titles as microscopic peritonitis, foreign body re-action, microscopic scoring system, and microscopic appear-ance. Microscopical evaluation parameters as regular bowel appearance, transmural healing tissue, and mural necrosis were evaluated separately for carrying more importance in microscopic scoring system.
Collagenated granulation tissue along the cutting direction of the cutter in the intestinal wall was named as “healing tis-sue” and classified as “sub-mucosal” or “transmural” with regard to appearance. Some test subjects displayed local healing tissue confined to the submucosa sparing mucosa and muscularis propria. The healing tissue in these subjects was defined as “sub-mucosal healing tissue” (Fig. 2). Some test subjects had healing tissue comprising mucosa, submucosa and muscularis propria along the cutting direction, which was named as “transmural healing tissue”. Necrosis present along the cutting direction was defined as limited-mural necrosis if it was confined to submucosa or comprising mucosa and submucosa sparing muscularis propria (Fig. 3); whereas, that comprising mucosa, submucosa and muscularis propria was defined as “mural necrosis” (Fig. 4a, Table 2).
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 116
Figure 1. ThecreationofsmallbowelperforationwithstabtoolsinratofBgroup(No:1).
Figure 2. Submucosal healing tissueby lightmicroscopywithamagnificationpower200x.
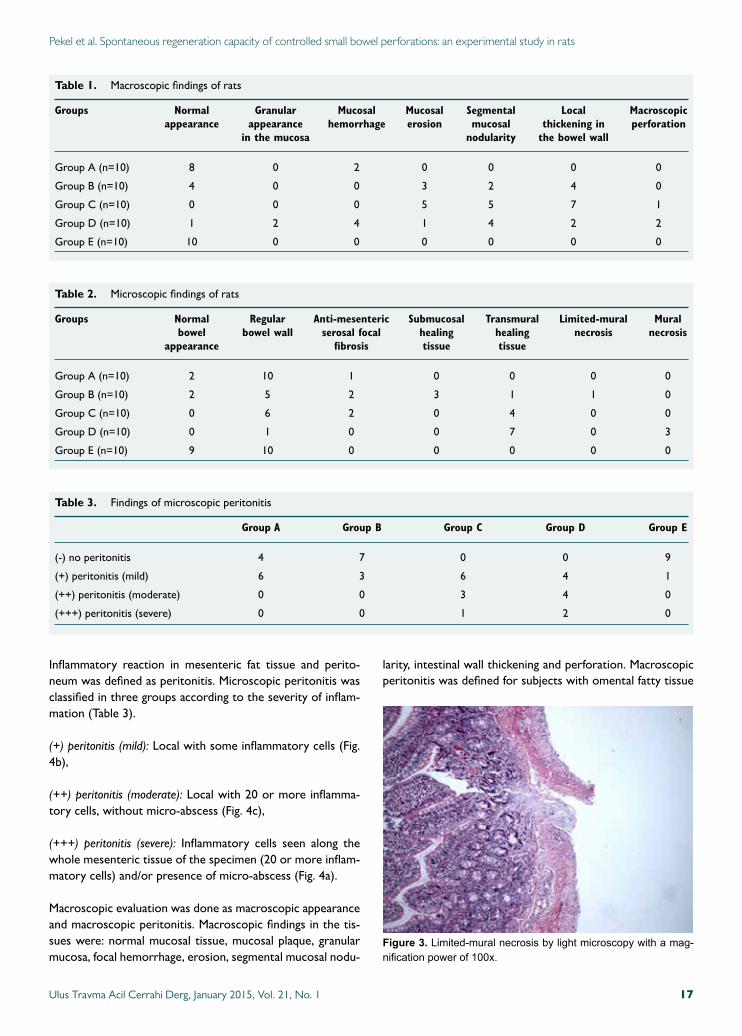
Pekel et al. Spontaneous regeneration capacity of controlled small bowel perforations: an experimental study in rats
Inflammatory reaction in mesenteric fat tissue and perito-neum was defined as peritonitis. Microscopic peritonitis was classified in three groups according to the severity of inflam-mation (Table 3).
(+) peritonitis (mild): Local with some inflammatory cells (Fig. 4b),
(++) peritonitis (moderate): Local with 20 or more inflamma-tory cells, without micro-abscess (Fig. 4c),
(+++) peritonitis (severe): Inflammatory cells seen along the whole mesenteric tissue of the specimen (20 or more inflam-matory cells) and/or presence of micro-abscess (Fig. 4a).
Macroscopic evaluation was done as macroscopic appearance and macroscopic peritonitis. Macroscopic findings in the tis-sues were: normal mucosal tissue, mucosal plaque, granular mucosa, focal hemorrhage, erosion, segmental mucosal nodu-
larity, intestinal wall thickening and perforation. Macroscopic peritonitis was defined for subjects with omental fatty tissue
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 17
Table 1. Macroscopic findings of rats
Groups Normal Granular Mucosal Mucosal Segmental Local Macroscopic appearance appearance hemorrhage erosion mucosal thickening in perforation in the mucosa nodularity the bowel wall
Group A (n=10) 8 0 2 0 0 0 0
Group B (n=10) 4 0 0 3 2 4 0
Group C (n=10) 0 0 0 5 5 7 1
Group D (n=10) 1 2 4 1 4 2 2
Group E (n=10) 10 0 0 0 0 0 0
Table 2. Microscopic findings of rats
Groups Normal Regular Anti-mesenteric Submucosal Transmural Limited-mural Mural bowel bowel wall serosal focal healing healing necrosis necrosis appearance fibrosis tissue tissue
Group A (n=10) 2 10 1 0 0 0 0
Group B (n=10) 2 5 2 3 1 1 0
Group C (n=10) 0 6 2 0 4 0 0
Group D (n=10) 0 1 0 0 7 0 3
Group E (n=10) 9 10 0 0 0 0 0
Table 3. Findings of microscopic peritonitis
Group A Group B Group C Group D Group E
(-) no peritonitis 4 7 0 0 9
(+) peritonitis (mild) 6 3 6 4 1
(++) peritonitis (moderate) 0 0 3 4 0
(+++) peritonitis (severe) 0 0 1 2 0
Figure 3. Limited-muralnecrosisbylightmicroscopywithamag-nificationpowerof100x.
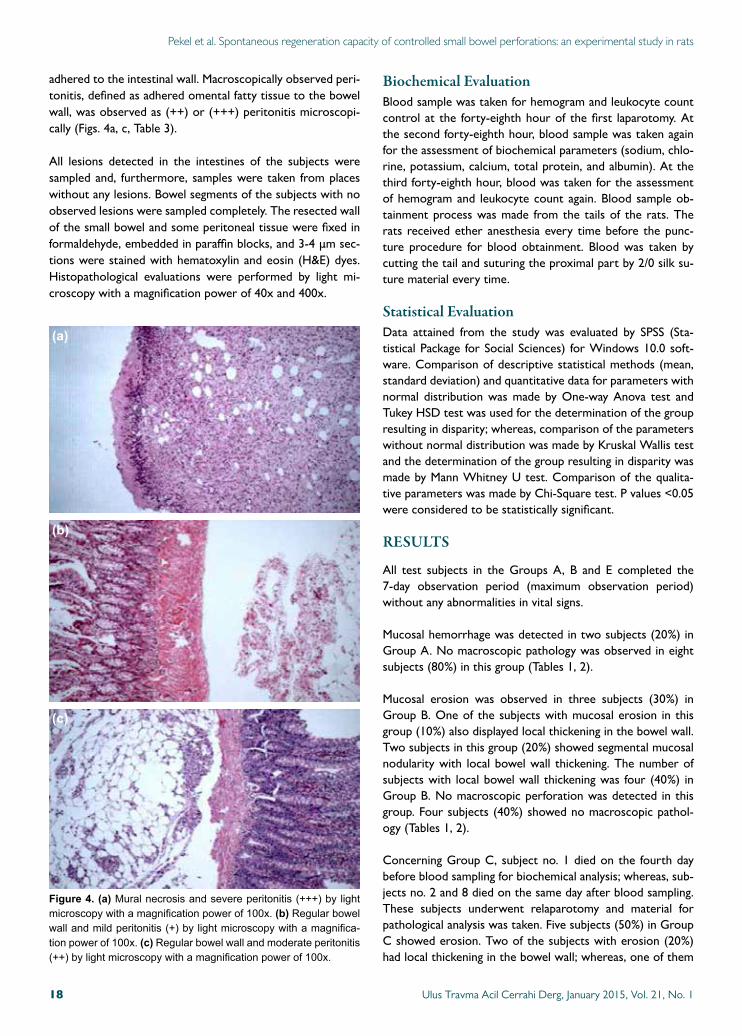
adhered to the intestinal wall. Macroscopically observed peri-tonitis, defined as adhered omental fatty tissue to the bowel wall, was observed as (++) or (+++) peritonitis microscopi-cally (Figs. 4a, c, Table 3).
All lesions detected in the intestines of the subjects were sampled and, furthermore, samples were taken from places without any lesions. Bowel segments of the subjects with no observed lesions were sampled completely. The resected wall of the small bowel and some peritoneal tissue were fixed in formaldehyde, embedded in paraffin blocks, and 3-4 μm sec-tions were stained with hematoxylin and eosin (H&E) dyes. Histopathological evaluations were performed by light mi-croscopy with a magnification power of 40x and 400x.
Biochemical EvaluationBlood sample was taken for hemogram and leukocyte count control at the forty-eighth hour of the first laparotomy. At the second forty-eighth hour, blood sample was taken again for the assessment of biochemical parameters (sodium, chlo-rine, potassium, calcium, total protein, and albumin). At the third forty-eighth hour, blood was taken for the assessment of hemogram and leukocyte count again. Blood sample ob-tainment process was made from the tails of the rats. The rats received ether anesthesia every time before the punc-ture procedure for blood obtainment. Blood was taken by cutting the tail and suturing the proximal part by 2/0 silk su-ture material every time.
Statistical EvaluationData attained from the study was evaluated by SPSS (Sta-tistical Package for Social Sciences) for Windows 10.0 soft-ware. Comparison of descriptive statistical methods (mean, standard deviation) and quantitative data for parameters with normal distribution was made by One-way Anova test and Tukey HSD test was used for the determination of the group resulting in disparity; whereas, comparison of the parameters without normal distribution was made by Kruskal Wallis test and the determination of the group resulting in disparity was made by Mann Whitney U test. Comparison of the qualita-tive parameters was made by Chi-Square test. P values <0.05 were considered to be statistically significant.
RESULTS
All test subjects in the Groups A, B and E completed the 7-day observation period (maximum observation period) without any abnormalities in vital signs.
Mucosal hemorrhage was detected in two subjects (20%) in Group A. No macroscopic pathology was observed in eight subjects (80%) in this group (Tables 1, 2).
Mucosal erosion was observed in three subjects (30%) in Group B. One of the subjects with mucosal erosion in this group (10%) also displayed local thickening in the bowel wall. Two subjects in this group (20%) showed segmental mucosal nodularity with local bowel wall thickening. The number of subjects with local bowel wall thickening was four (40%) in Group B. No macroscopic perforation was detected in this group. Four subjects (40%) showed no macroscopic pathol-ogy (Tables 1, 2).
Concerning Group C, subject no. 1 died on the fourth day before blood sampling for biochemical analysis; whereas, sub-jects no. 2 and 8 died on the same day after blood sampling. These subjects underwent relaparotomy and material for pathological analysis was taken. Five subjects (50%) in Group C showed erosion. Two of the subjects with erosion (20%) had local thickening in the bowel wall; whereas, one of them
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 118
Pekel et al. Spontaneous regeneration capacity of controlled small bowel perforations: an experimental study in rats
Figure 4. (a)Muralnecrosisandsevereperitonitis(+++)bylightmicroscopywithamagnificationpowerof100x.(b)Regularbowelwallandmildperitonitis(+)bylightmicroscopywithamagnifica-tionpowerof100x.(c)Regularbowelwallandmoderateperitonitis(++)bylightmicroscopywithamagnificationpowerof100x.
(a)
(b)
(c)
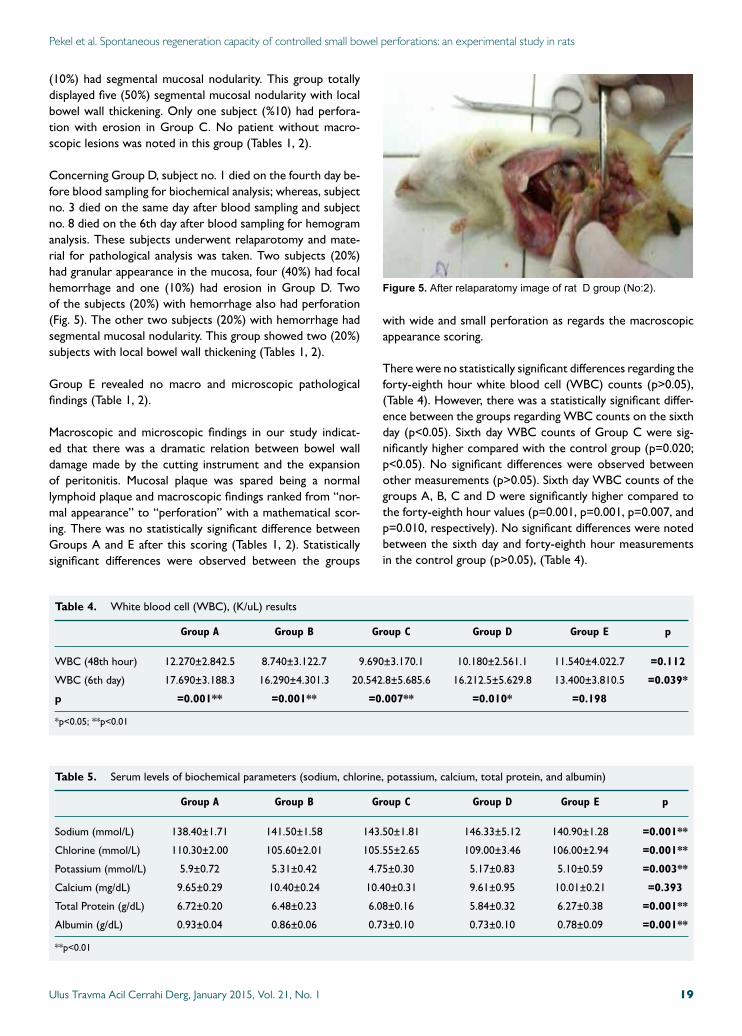
(10%) had segmental mucosal nodularity. This group totally displayed five (50%) segmental mucosal nodularity with local bowel wall thickening. Only one subject (%10) had perfora-tion with erosion in Group C. No patient without macro-scopic lesions was noted in this group (Tables 1, 2).
Concerning Group D, subject no. 1 died on the fourth day be-fore blood sampling for biochemical analysis; whereas, subject no. 3 died on the same day after blood sampling and subject no. 8 died on the 6th day after blood sampling for hemogram analysis. These subjects underwent relaparotomy and mate-rial for pathological analysis was taken. Two subjects (20%) had granular appearance in the mucosa, four (40%) had focal hemorrhage and one (10%) had erosion in Group D. Two of the subjects (20%) with hemorrhage also had perforation (Fig. 5). The other two subjects (20%) with hemorrhage had segmental mucosal nodularity. This group showed two (20%) subjects with local bowel wall thickening (Tables 1, 2).
Group E revealed no macro and microscopic pathological findings (Table 1, 2).
Macroscopic and microscopic findings in our study indicat-ed that there was a dramatic relation between bowel wall damage made by the cutting instrument and the expansion of peritonitis. Mucosal plaque was spared being a normal lymphoid plaque and macroscopic findings ranked from “nor-mal appearance” to “perforation” with a mathematical scor-ing. There was no statistically significant difference between Groups A and E after this scoring (Tables 1, 2). Statistically significant differences were observed between the groups
with wide and small perforation as regards the macroscopic appearance scoring.
There were no statistically significant differences regarding the forty-eighth hour white blood cell (WBC) counts (p>0.05), (Table 4). However, there was a statistically significant differ-ence between the groups regarding WBC counts on the sixth day (p<0.05). Sixth day WBC counts of Group C were sig-nificantly higher compared with the control group (p=0.020; p<0.05). No significant differences were observed between other measurements (p>0.05). Sixth day WBC counts of the groups A, B, C and D were significantly higher compared to the forty-eighth hour values (p=0.001, p=0.001, p=0.007, and p=0.010, respectively). No significant differences were noted between the sixth day and forty-eighth hour measurements in the control group (p>0.05), (Table 4).
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 19
Pekel et al. Spontaneous regeneration capacity of controlled small bowel perforations: an experimental study in rats
Table 4. White blood cell (WBC), (K/uL) results
Group A Group B Group C Group D Group E p
WBC (48th hour) 12.270±2.842.5 8.740±3.122.7 9.690±3.170.1 10.180±2.561.1 11.540±4.022.7 =0.112
WBC (6th day) 17.690±3.188.3 16.290±4.301.3 20.542.8±5.685.6 16.212.5±5.629.8 13.400±3.810.5 =0.039*
p =0.001** =0.001** =0.007** =0.010* =0.198
*p<0.05; **p<0.01
Table 5. Serum levels of biochemical parameters (sodium, chlorine, potassium, calcium, total protein, and albumin)
Group A Group B Group C Group D Group E p
Sodium (mmol/L) 138.40±1.71 141.50±1.58 143.50±1.81 146.33±5.12 140.90±1.28 =0.001**
Chlorine (mmol/L) 110.30±2.00 105.60±2.01 105.55±2.65 109.00±3.46 106.00±2.94 =0.001**
Potassium (mmol/L) 5.9±0.72 5.31±0.42 4.75±0.30 5.17±0.83 5.10±0.59 =0.003**
Calcium (mg/dL) 9.65±0.29 10.40±0.24 10.40±0.31 9.61±0.95 10.01±0.21 =0.393
Total Protein (g/dL) 6.72±0.20 6.48±0.23 6.08±0.16 5.84±0.32 6.27±0.38 =0.001**
Albumin (g/dL) 0.93±0.04 0.86±0.06 0.73±0.10 0.73±0.10 0.78±0.09 =0.001**
**p<0.01
Figure 5. AfterrelaparatomyimageofratDgroup(No:2).

Serum levels of the biochemical parameters (sodium, chlo-rine, potassium, calcium, total protein and albumin) of the rats were controlled on the fourth day. There were some statistically significant differences among the groups regarding these values; however, no reasonable data was obtained to make any comments (Table 5).
DISCUSSIONPenetrating abdominal trauma is increasing due to the world-wide growth of violence and there are a large number of patients with penetrating abdominal traumas in emergency surgery services. Main approach for penetrating abdominal trauma should be identifying injuries requiring surgical repair and avoiding unnecessary laparotomy with its associated mor-bidity.[8-11] The decision as to when an emergency laparotomy on a patient with a penetrating abdominal stab wound should be done is a continuing challenge. Routine laparotomy is not indicated in hemodynamically stable patients with penetrating abdominal stab wounds without signs of peritonitis or diffuse abdominal tenderness.[8,12-14]
Two approach models including emergency laparotomy and selective observation model have been described for pen-etrating abdominal trauma.[15-18] The only treatment choice for patients with penetrating abdominal trauma was routine laparotomy before the 1960s.[4] However, wide patient series demonstrate that nearly half of the patients have undergone perfect laparotomy.[4,5,15] Treatment approach to these patients has started to change, especially with the recommendation of selective observation method by Shaftan.[5] Studies regarding this issue have been confined to clinical trials so far. Selec-tive non-operative model of penetrating abdominal trauma is safe and has been shown to decrease the rate of unnecessary laparotomy, length of hospital stay, and management costs.[19]
Both solid and hollow organs possess the risk of damage after penetrating abdominal trauma. Studies have shown that most commonly affected hollow and solid organs after penetrating abdominal trauma are small intestines (30%) and liver (19%), respectively.[20-22] Colon (18%), stomach (13%), pancreas, and duodenum follow.[21,22] Bowel rupture following penetrating ab-dominal trauma lead to the gas and other intestinal ingredients leak into the peritoneum resulting in peritonitis.[23] Small bowel injury is rarely diagnosed preoperatively, especially when there are no specific signs of haemoperitoneum or peritonitis.[24]
In this study, biochemical and pathological changes in rats were studied after the formation of an experimental gut per-foration model. Perforation models in rats up to the pres-ent have generally been carried out to form peritonitis and caecum ligation method has been commonly used to force peritonitis formation.[24] However, it was aimed to form a perforation model most similar to the perforation with pierc-ing-cutting tool in humans in this study. Thus, perforations in different diameters were made in terminal ileum without any intervention to the intraperitoneal space.
Different sized perforations were made in the present study to eliminate the risk of coincidental or subject type risks. The reason why analgesics were not used in this study was not to hinder peritoneal inflammation after perforation. Blood samples were taken for cell count on the second and sixth days; and for biochemical analysis on the fourth day of the experiment for evaluation of the local morphological changes of the occurred peritonitis, as well as the systemic inflamma-tory response.
Following indications were noted after evaluation of the rela-tionship between macro- and microscopic findings. The lesion formed in the cutting device puncture point, also defined as se-rosal fibrous cap, was not recognized macroscopically. Segmen-tal mucosal nodularity was formed as a result of sub-mucosal or transmural healing tissue along the cutting device direction. Thickening in the bowel wall was also formed with the healing tissue along the direction. The pathological tests of this ex-perimental study showed that peritonitis intensity increased in direct ratio with the perforation diameter. As the perforation diameter increased, wall repair of the bowel diminished.
There were no significant differences regarding WBC counts in the first forty-eight hours including the control group, which was an indication of the inflammatory response formed in the first hours due to surgical trauma rather than perfora-tion. However, evaluating WBC counts on the sixth day, it could be said that the inflammatory response to perforation evolved later.
The reason for routine biochemical analyses in the clinical observation of patients is to determine changes in electro-lyte concentrations or protein values that can be important in tissue repair and to intervene if needed. Levels of some biochemical parameters on the fourth day were controlled in our study. However, the levels of the parameters included into the study revealed no significant results to comment on.
It was observed on rats that small bowel perforations in 2 mm diameter and below were repaired by the organism itself spontaneously without any operation needed. Perforations in 3 mm diameter were repaired totally although small bowel wall repair tissue was observed. However, probability of seri-ous peritonitis was found to be higher in this case. In perfora-tions of 4 mm in diameter, they were still present even after 7 days of observation.
The findings of this study showed that small perforations in the small bowel of rats could be limited by the organism itself without a necessity of any surgical intervention. Great de-velopments were noted in the selective observation method with the growth of resuscitation, surgical techniques, anti-biotic treatments and observation equipment. Secure treat-ment of patients without operation is proper both scientifi-cally and ethically.
Conflict of interest: None declared.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 120
Pekel et al. Spontaneous regeneration capacity of controlled small bowel perforations: an experimental study in rats

REFERENCES
1. Alzamel HA, Cohn SM. When is it safe to discharge asymptomatic pa-tients with abdominal stab wounds? J Trauma 2005;58:523-5.
2. Demetriades D, Rabinowitz B. Indications for operation in abdomi-nal stab wounds. A prospective study of 651 patients. Ann Surg 1987;205:129-32.
3. Arikan S, Kocakusak A, Yucel AF, Adas G. A prospective comparison of the selective observation and routine exploration methods for penetrating abdominal stab wounds with organ or omentum evisceration. J Trauma 2005;58:526-32.
4. Shaftan GW. Indications for operation in abdominal trauma. Am J Surg 1960;99:657-64.
5. Shaftan GW. Selective conservatism in penetrating abdominal trauma. J Trauma 1969;9:1026-8.
6. Velmahos GC, Demetriades D, Toutouzas KG, Sarkisyan G, Chan LS, Ishak R, et al. Selective nonoperative management in 1,856 patients with abdominal gunshot wounds: should routine laparotomy still be the stan-dard of care? Ann Surg 2001;234:395-403.
7. Biffl WL, Moore EE. Management guidelines for penetrating abdominal trauma. Curr Opin Crit Care 2010;16:609-17.
8. Sanei B, Mahmoudieh M, Talebzadeh H, Shahabi Shahmiri S, Aghaei Z. Do patients with penetrating abdominal stab wounds require lapa-rotomy? Arch Trauma Res 2013;2:21-5.
9. Morrison JJ, Dickson EJ, Jansen JO, Midwinter MJ. Utility of admission physiology in the surgical triage of isolated ballistic battlefield torso trau-ma. J Emerg Trauma Shock 2012;5:233-7.
10. Wiewióra M, Sosada K, Piecuch J, Zurawiński W. The role of laparos-copy in abdominal trauma - review of the literature. Wideochir Inne Tech Malo Inwazyjne 2011;6:121-6.
11. Shan CX, Ni C, Qiu M, Jiang DZ. Is laparoscopy equal to laparotomy in detecting and treating small bowel injuries in a porcine model? World J Gastroenterol 2012;18:6850-5.
12. Sugrue M, Balogh Z, Lynch J, Bardsley J, Sisson G, Weigelt J. Guide-lines for the management of haemodynamically stable patients with stab
wounds to the anterior abdomen. ANZ J Surg 2007;77:614-20.13. Inaba K, Demetriades D. The nonoperative management of penetrating
abdominal trauma. Adv Surg 2007;41:51-62.14. Demetriades D, Rabinowitz B. Indications for operation in abdomi-
nal stab wounds. A prospective study of 651 patients. Ann Surg 1987;205:129-32.
15. Kessel B, Peleg K, Hershekovitz Y, Khashan T, Givon A, Ashkenazi I, et al. Abdominal stab wounds in Israel, 1997-2004: significant increase in overall incidence and prevalence of severe injury. Isr Med Assoc J 2008;10:135-7.
16. Butt MU, Zacharias N, Velmahos GC. Penetrating abdominal inju-ries: management controversies. Scand J Trauma Resusc Emerg Med 2009;17:19.
17. Clarke DL, Allorto NL, Thomson SR. An audit of failed non-operative management of abdominal stab wounds. Injury 2010;41:488-91.
18. Demetriades D, Hadjizacharia P, Constantinou C, Brown C, Inaba K, Rhee P, et al. Selective nonoperative management of penetrating abdomi-nal solid organ injuries. Ann Surg 2006;244:620-8.
19. Renz BM, Feliciano DV. The length of hospital stay after an unnecessary laparotomy for trauma: a prospective study. J Trauma 1996;40:187-90.
20. Nicholas JM, Rix EP, Easley KA, Feliciano DV, Cava RA, Ingram WL, et al. Changing patterns in the management of penetrating abdominal trauma: the more things change, the more they stay the same. J Trauma 2003;55:1095-110.
21. Taviloglu K, Günay K, Ertekin C, Calis A, Türel O. Abdominal stab wounds: the role of selective management. Eur J Surg 1998;164:17-21.
22. Aysan E, Ertekin C, Guloglu R, Aren A. Approach to blunt abdominal trauma (general results of monthly inter-hospital meetings of the Turk-ish association for trauma and emergency surgery 2). Ulus Travma Derg 2002;8:129-31.
23. Tsikitis V, Biffl WL, Majercik S, Harrington DT, Cioffi WG. Selective clinical management of anterior abdominal stab wounds. Am J Surg 2004;188:807-12.
24. Bostanoğlu S, Bostanoğlu A, Erverdi N, Hamamcı O, Gülan Ö, Dursun A, et al. The role of oxygen free radicals in an experimental sepsis model. The Turkish Journal of Gastroenterology 1999;10:427-31.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 21
Pekel et al. Spontaneous regeneration capacity of controlled small bowel perforations: an experimental study in rats
OLGU SUNUMU
Kontrollü ince bağırsak perforasyonlarının spontan rejenerasyon potansiyeli:Sıçanlarda deneysel bir çalışmaDr. Özgür Pekel,1 Dr. Sinan Hatipoglu,2 Dr. Ahmet Nuray Turhan,3 Dr. Filiz Hatipoglu,4
Dr. Ruslan Abdullayev,5 Dr. Süha Göksel6
1ŞevketYılmazEğitimveAraştırmaHastanesi,GenelCerrahiKliniği,Bursa;2AdıyamanÜniversitesiTıpFakültesi,GenelCerrahiAnabilimDalı,Adıyaman;3İstanbulCerrahiHastanesi,GenelCerrahiKliniği,İstanbul;4AdıyamanÜniversitesiEğitimveAraştırmaHastanesi,KadınHastalıklarıveDoğumKliniği,Adıyaman;5AdıyamanÜniversitesiEğitimveAraştırmaHastanesi,AnesteziveReanimasyonKliniği,Adıyaman;6Acıbadem(Maslak)Hastanesi,PatolojiBölümü,İstanbul
AMAÇ: Penetran karın travmalarında temel cerrahi yaklaşım, 1960’lı yıllarda Shaftan’nın ortaya attığı seçici gözlem yöntemiyle temelden değişmiş ve tüm dünyada penetran karın travmalı hastalarda rutin laparotomi uygulama yöntemi yerine seçici gözlem yöntemi kullanılması ağırlık kazanmıştır. Bu durumda ameliyat edilmeden iyileşebilmiş bağırsak perforasyonlu hastalar olabileceği ihtimali doğmaktadır. Bu konuyu araştırmak amacıyla deneysel bir model oluşturduk.GEREÇ VE YÖNTEM: Elli adet wistar albino cinsi sıçan 10 adetlik beş gruba ayrıldıktan sonra ince bağırsaklarının distal kısmı hazırlanan uygun ebattaki kesiciler ile 1 mm, 2 mm, 3 mm ve 4 mm olmak üzere farklı büyüklükte perfore edildi ve bir grup kontrol grubu olarak ayrıldı. Gruplardaki sıçanlar bir hafta süreyle takip edildikten sonra sakrifiye edilerek, perfore edilen bağırsak lokalizasyonunun 1 cm proksimali ile distalini içerecek şekilde ileum segmenti ve periton dokusu histopatolojik inceleme için patoloji laboratuvarına gönderildi.BULGULAR: Çalışma gruplarımızdaki sıçanlarda, 2 mm ve altındaki ince bağırsak perforasyonlarının herhangi bir cerrahi girişime gerek olmadan spontan olarak iyileşebilir olduğunu gözlemledik. Yedi günlük takibe karşın 4 mm’lik bağırsak yaralanmalarında halen devam eden perforasyonlar görüldü. Patolojik inceleme sonunda perforasyon çapları ile orantılı olarak peritonitin şiddetlendiği ve bağırsak duvarı onarımının azaldığı saptandı.TARTIŞMA: Sonuç olarak, sıçanlarda küçük çaplı ince bağırsak perforasyonlarının herhangi bir cerrahi müdahale gerekmeden organizma tarafından sınırlanabileceği gözlemlendi.Anahtar sözcükler: Deneysel çalışma; ince bağırsak perforasyonu; penetran karın travmaları; spontan rejenerasyon.
Ulus Travma Acil Cerrahi Derg 2015;21(1):15-21 doi: 10.5505/tjtes.2015.31369
DENEYSEL ÇALIŞMA - ÖZET

Comparison of morphine–midazolam versusmorphine injection for pain relief in patientswith limb fractures - a clinical trialAlireza Majidi, M.D.,1 Hossein Dinpanah, M.D.,1 Sahar Ashoori, M.D.,1
Hassan Motamed, M.D.,2# Ali Tabatabaey, M.D.1*
1DepartmentofEmergencyMedicine,ShahidBeheshtiMedicalUniversity,Tehran,Iran;2DepartmentofEmergencyMedicine,JundishapoorUniversityofMedicalSciences,Ahvaz,Iran
ABSTRACT
BACKGROUND: Pain relief, using opiates as a primary choice, is an important part of treating limb fractures. Yet, in order to reduce opiate consumption, other combinations have been introduced. This study aimed to compare pain reduction by a combination of morphine–midazolam with morphine injection in patients with limb fractures.
METHODS: A randomized double-blind study of patients with upper or lower extremity fractures was conducted. Patients’ response to treatment with either morphine-midazolam solution or morphine at 15, 30, 45, 60, 120, and 180 minutes were assessed. The Kaplan-Meier curves and generalized estimating equations were examined to evaluate the success of treatment.
RESULTS: A total of seventy-two patients aged 18-60 (80.6% male; mean age: 35±17.9 years) were included. At 15, 30, 45, and 60 minutes, successful pain control was seen in 8.83 22.2%, 33.3% and 63.9% of the patients in the morphine group, and 11.1%, 27.7%, 44.4% and 63.8% in the midazolam-morphine group. By the third hour, pain-control was achieved in all patients receiving morphine while pain persisted in one patient receiving morphine-midazolam. Log-rank test showed no significant difference between the two groups (p=0.55).
CONCLUSION: Our findings revealed that adding midazolam to morphine did not improve its pain-relief profile.
Key words: Bone fracture; midazolam; morphine; pain.
and severe pain.[5,6] Such guidelines recommend the use of MS for patients with a pain score of 6 or higher on the visual analogue scale (VAS) until the pain is controlled (severity of pain reduced to 3 or lower).
Yet, using MS is limited by a variety of factors including fear of side effects, impairment of physical examination, and fear of addiction.[7] Furthermore, dose adjustment is required on a personal bases to achieve balance between pain control and these concerns. Recent evidence has pointed to the fact that MS is not as effective as once thought in ED patients. It has been suggested that within 15 minutes of administration, only 50% of the patients experience pain control.[4,8,9] Therefore, despite noticeable strides, pain control in the ED is still an unresolved issue.[3,1-12] Consequently, researchers have pro-posed other drug regimens to reduce MS consumption in the ED. Combination drug therapy is one such regimen aiming to improve pain control whilst reducing MS use.[13-15]
Midazolam is an imidazobenzodiazepine with unique charac-teristics. It acts faster than other drugs in this category and is a stronger sedative, hypnotic, and anxiolytic. These proper-
O R I G I N A L A R T I C L E
Current affiliation: #Department of Emergency Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran;*Department of Emergency Medicine, Qom University of Medical Sciences, Qom, Iran
Address for correspondence: Ali Tabatabaey, M.D.
Department of Emergency Medicine, Qom University of Medical
Sciences, Qom, Iran
Tel: +98 2536122000 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):22-26doi: 10.5505/tjtes.2015.64494
Copyright 2015TJTES
INTRODUCTION
Pain reduction of limb fracture patients in the emergency department (ED) is a treatment priority for the emergency physician.[1-3] Pain control is closely related to patient satis-faction.[2,4] For years, opiates, namely Morphine sulfate (MS), have been the primary pain relief medication. Many current guidelines support intravenous administration of MS for acute
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 122
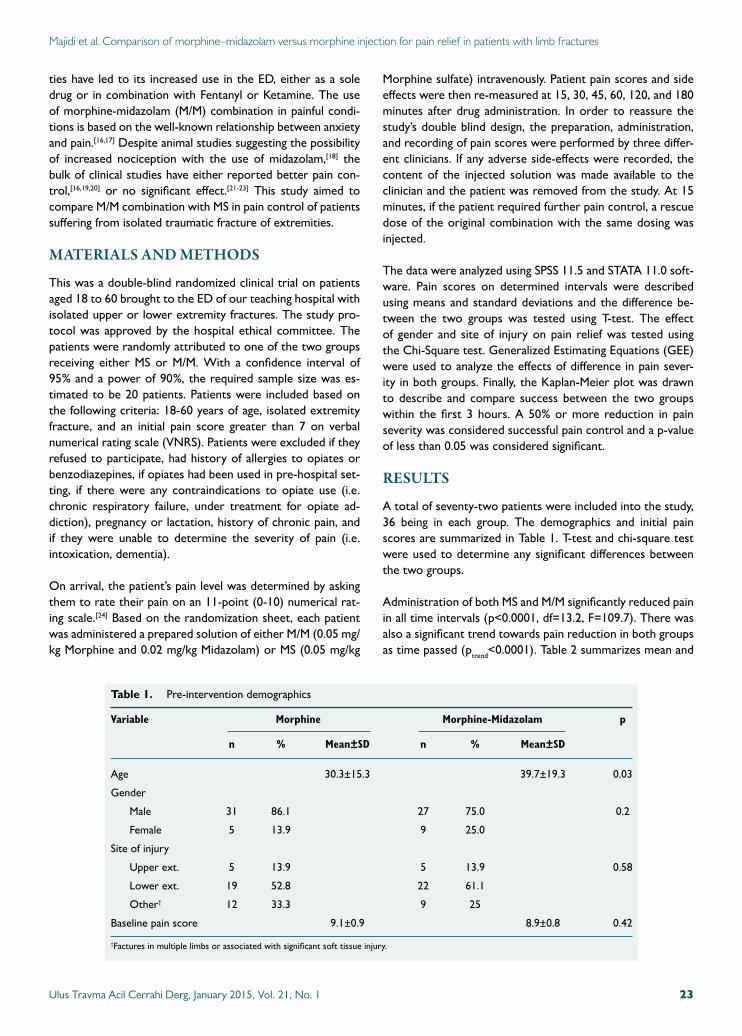
Majidi et al. Comparison of morphine–midazolam versus morphine injection for pain relief in patients with limb fractures
ties have led to its increased use in the ED, either as a sole drug or in combination with Fentanyl or Ketamine. The use of morphine-midazolam (M/M) combination in painful condi-tions is based on the well-known relationship between anxiety and pain.[16,17] Despite animal studies suggesting the possibility of increased nociception with the use of midazolam,[18] the bulk of clinical studies have either reported better pain con-trol,[16,19,20] or no significant effect.[21-23] This study aimed to compare M/M combination with MS in pain control of patients suffering from isolated traumatic fracture of extremities.
MATERIALS AND METHODS
This was a double-blind randomized clinical trial on patients aged 18 to 60 brought to the ED of our teaching hospital with isolated upper or lower extremity fractures. The study pro-tocol was approved by the hospital ethical committee. The patients were randomly attributed to one of the two groups receiving either MS or M/M. With a confidence interval of 95% and a power of 90%, the required sample size was es-timated to be 20 patients. Patients were included based on the following criteria: 18-60 years of age, isolated extremity fracture, and an initial pain score greater than 7 on verbal numerical rating scale (VNRS). Patients were excluded if they refused to participate, had history of allergies to opiates or benzodiazepines, if opiates had been used in pre-hospital set-ting, if there were any contraindications to opiate use (i.e. chronic respiratory failure, under treatment for opiate ad-diction), pregnancy or lactation, history of chronic pain, and if they were unable to determine the severity of pain (i.e. intoxication, dementia). On arrival, the patient’s pain level was determined by asking them to rate their pain on an 11-point (0-10) numerical rat-ing scale.[24] Based on the randomization sheet, each patient was administered a prepared solution of either M/M (0.05 mg/kg Morphine and 0.02 mg/kg Midazolam) or MS (0.05 mg/kg
Morphine sulfate) intravenously. Patient pain scores and side effects were then re-measured at 15, 30, 45, 60, 120, and 180 minutes after drug administration. In order to reassure the study’s double blind design, the preparation, administration, and recording of pain scores were performed by three differ-ent clinicians. If any adverse side-effects were recorded, the content of the injected solution was made available to the clinician and the patient was removed from the study. At 15 minutes, if the patient required further pain control, a rescue dose of the original combination with the same dosing was injected.
The data were analyzed using SPSS 11.5 and STATA 11.0 soft-ware. Pain scores on determined intervals were described using means and standard deviations and the difference be-tween the two groups was tested using T-test. The effect of gender and site of injury on pain relief was tested using the Chi-Square test. Generalized Estimating Equations (GEE) were used to analyze the effects of difference in pain sever-ity in both groups. Finally, the Kaplan-Meier plot was drawn to describe and compare success between the two groups within the first 3 hours. A 50% or more reduction in pain severity was considered successful pain control and a p-value of less than 0.05 was considered significant.
RESULTS
A total of seventy-two patients were included into the study, 36 being in each group. The demographics and initial pain scores are summarized in Table 1. T-test and chi-square test were used to determine any significant differences between the two groups.
Administration of both MS and M/M significantly reduced pain in all time intervals (p<0.0001, df=13.2, F=109.7). There was also a significant trend towards pain reduction in both groups as time passed (ptrend<0.0001). Table 2 summarizes mean and
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 23
Table 1. Pre-intervention demographics
Variable Morphine Morphine-Midazolam p
n % Mean±SD n % Mean±SD
Age 30.3±15.3 39.7±19.3 0.03
Gender
Male 31 86.1 27 75.0 0.2
Female 5 13.9 9 25.0
Site of injury
Upper ext. 5 13.9 5 13.9 0.58
Lower ext. 19 52.8 22 61.1
Other† 12 33.3 9 25
Baseline pain score 9.1±0.9 8.9±0.8 0.42
†Factures in multiple limbs or associated with significant soft tissue injury.
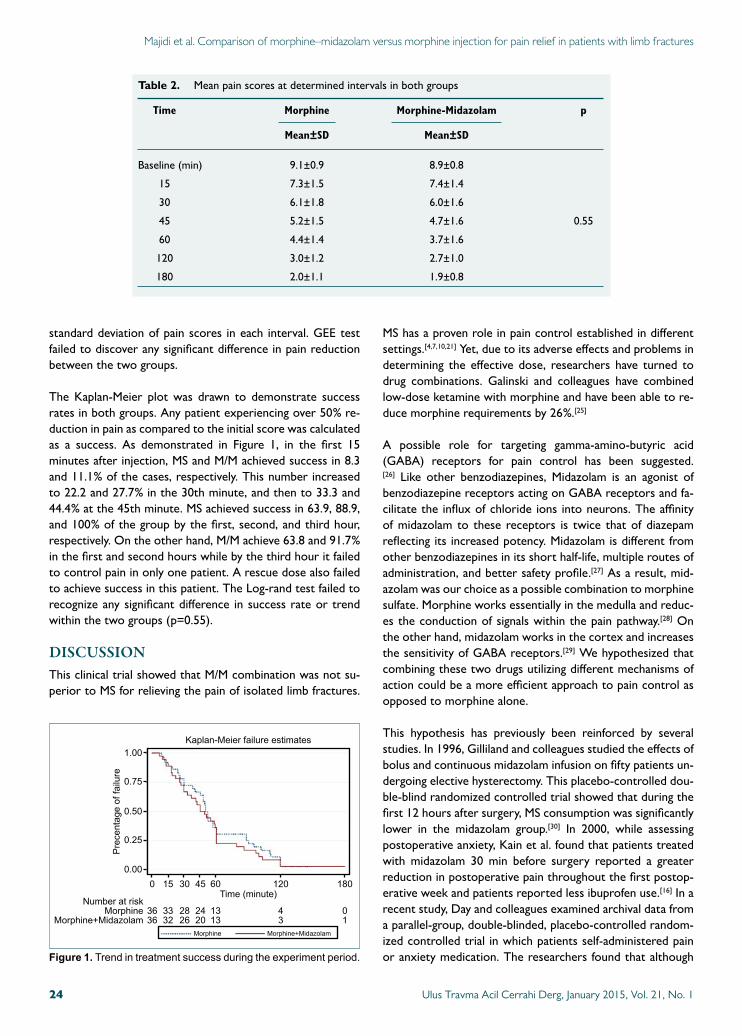
Majidi et al. Comparison of morphine–midazolam versus morphine injection for pain relief in patients with limb fractures
standard deviation of pain scores in each interval. GEE test failed to discover any significant difference in pain reduction between the two groups.
The Kaplan-Meier plot was drawn to demonstrate success rates in both groups. Any patient experiencing over 50% re-duction in pain as compared to the initial score was calculated as a success. As demonstrated in Figure 1, in the first 15 minutes after injection, MS and M/M achieved success in 8.3 and 11.1% of the cases, respectively. This number increased to 22.2 and 27.7% in the 30th minute, and then to 33.3 and 44.4% at the 45th minute. MS achieved success in 63.9, 88.9, and 100% of the group by the first, second, and third hour, respectively. On the other hand, M/M achieve 63.8 and 91.7% in the first and second hours while by the third hour it failed to control pain in only one patient. A rescue dose also failed to achieve success in this patient. The Log-rand test failed to recognize any significant difference in success rate or trend within the two groups (p=0.55).
DISCUSSIONThis clinical trial showed that M/M combination was not su-perior to MS for relieving the pain of isolated limb fractures.
MS has a proven role in pain control established in different settings.[4,7,10,21] Yet, due to its adverse effects and problems in determining the effective dose, researchers have turned to drug combinations. Galinski and colleagues have combined low-dose ketamine with morphine and have been able to re-duce morphine requirements by 26%.[25]
A possible role for targeting gamma-amino-butyric acid (GABA) receptors for pain control has been suggested.[26] Like other benzodiazepines, Midazolam is an agonist of benzodiazepine receptors acting on GABA receptors and fa-cilitate the influx of chloride ions into neurons. The affinity of midazolam to these receptors is twice that of diazepam reflecting its increased potency. Midazolam is different from other benzodiazepines in its short half-life, multiple routes of administration, and better safety profile.[27] As a result, mid-azolam was our choice as a possible combination to morphine sulfate. Morphine works essentially in the medulla and reduc-es the conduction of signals within the pain pathway.[28] On the other hand, midazolam works in the cortex and increases the sensitivity of GABA receptors.[29] We hypothesized that combining these two drugs utilizing different mechanisms of action could be a more efficient approach to pain control as opposed to morphine alone.
This hypothesis has previously been reinforced by several studies. In 1996, Gilliland and colleagues studied the effects of bolus and continuous midazolam infusion on fifty patients un-dergoing elective hysterectomy. This placebo-controlled dou-ble-blind randomized controlled trial showed that during the first 12 hours after surgery, MS consumption was significantly lower in the midazolam group.[30] In 2000, while assessing postoperative anxiety, Kain et al. found that patients treated with midazolam 30 min before surgery reported a greater reduction in postoperative pain throughout the first postop-erative week and patients reported less ibuprofen use.[16] In a recent study, Day and colleagues examined archival data from a parallel-group, double-blinded, placebo-controlled random-ized controlled trial in which patients self-administered pain or anxiety medication. The researchers found that although
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 124
Table 2. Mean pain scores at determined intervals in both groups
Time Morphine Morphine-Midazolam p
Mean±SD Mean±SD
Baseline (min) 9.1±0.9 8.9±0.8
15 7.3±1.5 7.4±1.4
30 6.1±1.8 6.0±1.6
45 5.2±1.5 4.7±1.6 0.55
60 4.4±1.4 3.7±1.6
120 3.0±1.2 2.7±1.0
180 2.0±1.1 1.9±0.8
Figure 1. Trendintreatmentsuccessduringtheexperimentperiod.
1.00
0.75
0.50
0.25
0.000
36MorphineNumberatrisk
Time(minute)
Kaplan-Meierfailureestimates
Precentageoffailure
Morphine+Midazolam 36
15
3332
30
2826
45
2420
60
13
Morphine Morphine+Midazolam
13
120
43
180
01

there was no significant difference in pain scores, the treat-ment group used significantly less morphine than the control group and felt better.[19]
On the other hand, several studies have questioned analgesic enhancement by midazolam. Wille-Ledon and colleagues have demonstrated a similar pain relief profile for Morphine and Morphine-Midazolam combination in the pediatric population with limb fractures.[21] More recently, Auffret et al. have stud-ied the role of adding midazolam to MS in pre-hospital trauma patients. The study was a prospective randomized double-blind placebo-controlled trial. Pain was assessed using a NRS and a difference of 3 points between the groups was consid-ered significant effect. The study failed to find any benefit of midazolam adjunctive therapy to morphine in pain control.[23]
To our knowledge, ours is the first study comparing M/M and MS in the setting of adult trauma patients in the emergency department. Like that of Wille-Ledon and Auffret, our results failed to prove an added analgesic effect when midazolam was added to morphine. In our study, patients in both groups showed a similar amount and trend in pain reduction and the success rate in both groups was comparable. Furthermore, our results showed that despite even using a rescue dose, more than half of the patients still suffered from significant pain 30 minutes after either MS or M/M injection, reflecting, to some extent, the unreliability of morphine in its initial dose and justifying the search for a more effective and reliable an-algesic in limb fractures.
Limitations and ConclusionThis study was the first double-blind randomized control trial to compare the effects of M/M to MS for pain reduc-tion in acute isolated limb fractures. Since the study was set in the emergency department, only short term results were sought and possible long-term outcomes derived from the combination therapy were not evaluated. A placebo group was not used for ethical concerns. Another limitation was homogeneity of the two groups. As seen in Table 1, both groups were found to be significantly different regarding age (p=0.03). Taking into account the mean age of both groups, it is to our belief that this should not affect the interpretation of our findings. Results of the current study showed that add-ing midazolam to morphine did not improve its pain relieving characteristics in limb fractures.
Acknowledgement and Conflict of InterestThe study was funded by the authors’ academic grants and the authors have no conflict of interest to report.
REFERENCES
1. Jennings PA, Cameron P, Bernard S. Epidemiology of prehospital pain: an opportunity for improvement. Emerg Med J 2011;28:530-1.
2. Le May S, Gouin S, Fortin C, Messier A, Robert MA, Julien M. Efficacy
of an ibuprofen/codeine combination for pain management in children presenting to the emergency department with a limb injury: a pilot study. J Emerg Med 2013;44:536-42.
3. Brown JC, Klein EJ, Lewis CW, Johnston BD, Cummings P. Emergency department analgesia for fracture pain. Ann Emerg Med 2003;42:197-205.
4. Bounes V, Charpentier S, Houze-Cerfon CH, Bellard C, Ducassé JL. Is there an ideal morphine dose for prehospital treatment of severe acute pain? A randomized, double-blind comparison of 2 doses. Am J Emerg Med 2008;26:148-54.
5. Ward KR, Yealy DM. Systemic analgesia and sedation in managing or-thopedic emergencies. Emerg Med Clin North Am 2000;18:141-66.
6. Smally AJ, Nowicki TA, Simelton BH. Procedural sedation and analgesia in the emergency department. Curr Opin Crit Care 2011;17:317-22.
7. Gallagher EJ, Esses D, Lee C, Lahn M, Bijur PE. Randomized clinical tri-al of morphine in acute abdominal pain. Ann Emerg Med 2006;48:150-60 .e1-4.
8. Galinski M, Dolveck F, Borron SW, Tual L, Van Laer V, Lardeur JY, et al. A randomized, double-blind study comparing morphine with fentanyl in prehospital analgesia. Am J Emerg Med 2005;23:114-9.
9. Rickard C, O’Meara P, McGrail M, Garner D, McLean A, Le Lievre P. A randomized controlled trial of intranasal fentanyl vs intravenous morphine for analgesia in the prehospital setting. Am J Emerg Med 2007;25:911-7.
10. Bijur PE, Kenny MK, Gallagher EJ. Intravenous morphine at 0.1 mg/kg is not effective for controlling severe acute pain in the majority of patients. Ann Emerg Med 2005;46:362-7.
11. Todd KH. Emergency medicine and pain: a topography of influence. Ann Emerg Med 2004;43:504-6.
12. Rupp T, Delaney KA. Inadequate analgesia in emergency medicine. Ann Emerg Med 2004;43:494-503.
13. Chang AK, Bijur PE, Lupow JB, John Gallagher E. Randomized clinical trial of efficacy and safety of a single 2-mg intravenous dose of hydromor-phone versus usual care in the management of acute pain. Acad Emerg Med 2013;20:185-92.
14. Chaplin S, Campbell W. Properties and use of compound analgesics in pain management. Prescriber 2013;24:38-40.
15. Leung S, Bulloch B, Young C, Yonker M, Hostetler M. Effectiveness of standardized combination therapy for migraine treatment in the pediatric emergency department. Headache 2013;53:491-197.
16. Kain ZN, Sevarino F, Pincus S, Alexander GM, Wang SM, Ayoub C, et al. Attenuation of the preoperative stress response with midazolam: effects on postoperative outcomes. Anesthesiology 2000;93:141-7.
17. Ploghaus A, Narain C, Beckmann CF, Clare S, Bantick S, Wise R, et al. Exacerbation of pain by anxiety is associated with activity in a hippocam-pal network. J Neurosci 2001;21:9896-903.
18. Ito K, Yoshikawa M, Maeda M, Jin XL, Takahashi S, Matsuda M, et al. Midazolam attenuates the antinociception induced by d-serine or mor-phine at the supraspinal level in rats. Eur J Pharmacol 2008;586:139-44.
19. Day MA, Rich MA, Thorn BE, Berbaum ML, Mangieri EA. A placebo-controlled trial of midazolam as an adjunct to morphine patient-con-trolled analgesia after spinal surgery. J Clin Anesth 2014;26:300-8.
20. Aydogan MS, Parlakpinar H, Ali Erdogan M, Yucel A, Ucar M, Sağır M, et al. Effects of dexmedetomidine and midazolam on motor coordi-nation and analgesia: a comparative analysis. Curr Ther Res Clin Exp 2013;75:22-6.
21. Wille-Ledon C, Chappuy H, Giraud C, Tréluyer JM, Chéron G. Com-parison of a morphine and midazolam combination with morphine alone for paediatric displaced fractures: a randomized study. Acta Paediatr
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 25
Majidi et al. Comparison of morphine–midazolam versus morphine injection for pain relief in patients with limb fractures

2011;100:e203-7.
22. Bauer KP, Dom PM, Ramirez AM, O’Flaherty JE. Preoperative intrave-nous midazolam: benefits beyond anxiolysis. J Clin Anesth 2004;16:177-83.
23. Auffret Y, Gouillou M, Jacob GR, Robin M, Jenvrin J, Soufflet F, et al. Does midazolam enhance pain control in prehospital management of traumatic severe pain? Am J Emerg Med 2014;32:655-9.
24. Todd KH, Funk KG, Funk JP, Bonacci R. Clinical significance of report-ed changes in pain severity. Ann Emerg Med. 1996;27:485-9.
25. Galinski M, Dolveck F, Combes X, Limoges V, Smaïl N, Pommier V, et al. Management of severe acute pain in emergency settings: ketamine re-duces morphine consumption. Am J Emerg Med 2007;25:385-90.
26. Jasmin L, Wu MV, Ohara PT. GABA puts a stop to pain. Curr Drug
Targets CNS Neurol Disord 2004;3:487-505.
27. Hardmeier M, Zimmermann R, Rüegg S, Pflüger M, Deuster S, Suter K, et al. Intranasal midazolam: pharmacokinetics and pharmacodynamics assessed by quantitative EEG in healthy volunteers. Clin Pharmacol Ther 2012;91:856-62.
28. Yaksh TL. Pharmacology and mechanisms of opioid analgesic activity. Acta Anaesthesiol Scand 1997;41(1 Pt 2):94-111.
29. Rogers WK, McDowell TS. Remimazolam, a short-acting GABA(A) receptor agonist for intravenous sedation and/or anesthesia in day-case surgical and non-surgical procedures. IDrugs 2010;13:929-37.
30. Gilliland HE, Prasad BK, Mirakhur RK, Fee JP. An investigation of the potential morphine sparing effect of midazolam. Anaesthesia 1996;51:808-11.
OLGU SUNUMU
Ekstremite kırıkları olan hastalarda ağrı giderimi için morfin-midazolama karşınmorfin enjeksiyonunun karşılaştırılması - klinik çalışma Dr. Alireza Majidi,1 Dr. Hossein Dinpanah,1 Dr. Sahar Ashoori,1 Dr. Hassan Motamed,2 Dr. Ali Tabatabaey1
1ShahidBeheshtiTıpÜniversitesi,AcilTıpAnabilimDalı,Tehran,Iran;2JundishapoorTıpBilimleriÜniversitesi,AcilTıpAnabilimDalı,Ahvaz,Iran
AMAÇ: Ağrı giderimi için ilk olarak opiyatların kullanılması ekstremite kırıkları tedavisinin önemli bir bölümünü oluşturur. Ancak opiyat tüketiminin azaltılması için başka kombinasyonlar da ortaya atılmıştır. Bu çalışma, bu hastalarda ağrıyı hafifletmede morfin-midazolam kombinasyonuyla morfin enjeksiyonunu karşılaştırmayı amaçlamaktadır.GEREÇ VE YÖNTEM: Alt ve üst ekstremite kırıkları olan hastalarda bir randomize çift-kör çalışma yürütüldü. Hastaların morfin-midazolam çözeltisi veya morfin tedavisine yanıtları 15., 30., 45., 60., 120. ve 180. dakikalarda değerlendirildi. Tedavinin başarısını değerlendirmek için Kaplan-Meier eğrileri ve genelleştirilmiş tahmin denklemleri incelendi. Anlamlılık düzeyi olarak p<0.05 kabul edildi.BULGULAR: Çalışmaya 18-60 yaş arası toplam 72 hasta (%80.6 erkek; yaş ortalaması: 35±17.9 yıl) alındı. On beşinci, 30., 45. ve 60. dakikalarda morfin grubunda hastaların sırasıyla %8.83; %22.2; %33.3 ve %63.9’unda, midazolam-morfin grunda ise %11.1; %27.7; %44.4 ve %63.8’inde ağrının kontrolü başarıldı. Üçüncü saate gelindiğinde morfin alanların hepsinde ağrı kontrolü gerçekleşmişken morfin-midazolam grubunda yalnızca bir hastada ağrı sebat etmiştir. Log-sıra testi iki gruplar arasında herhangi bir anlamlı farklılık göstermedi (p=0.55).TARTIŞMA: Bulgularımız midazolamın morfine ilavesinin ağrı giderimi profilini iyileştirmediğini göstermektedir.Anahtar sözcükler: Ağrı; kemik kırığı, midazolam; morfin.
Ulus Travma Acil Cerrahi Derg 2015;21(1):22-26 doi: 10.5505/tjtes.2015.64494
KLİNİK ÇALIŞMA - ÖZET
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 126
Majidi et al. Comparison of morphine–midazolam versus morphine injection for pain relief in patients with limb fractures

Outpatient burn management and unnecessary referralsİsa Sözen, M.D.,1 Cem Emir Guldogan, M.D.,1 Kemal Kismet, M.D.,2
Mehmet Zafer Sabuncuoğlu, M.D.,3 Ahmet Çınar Yasti, M.D.1,4
1DepartmentofGeneralSurgery,BurnsTreatmentCenter,AnkaraNumuneTrainingandResearchHospital,Ankara;2DepartmentofGeneralSurgery,BurnsUnit,AnkaraTrainingandResearchHospital,Ankara;3DepartmentofGeneralSurgery,SuleymanDemirelUniversityFacultyofMedicine,Isparta;4DepartmentofGeneralSurgery,HititUniversityFacultyofMedicine,Corum
ABSTRACT
BACKGROUND: This study aimed to determine the profile of burn patients presented in our polyclinic and evaluate the current status in comparison to the treatment methods of past series.
METHODS: Burn patients presented in the polyclinic in a one-year period were included into this prospective study. The records of all patients were examined in respect of gender, age, burn percentage, burn location, cause of burn, degree of burn, dressing material, number of dressings, type of treatment, place of trauma, and month of trauma.
RESULTS: From a total of one thousand seven hundred and ninety-five patients presented, management was completed in the poly-clinic for one thousand five hundred and eleven cases with a mean age of 27.9 years, with a female: male ratio of 0.88. While most patients were in the 18-64 age group, hot liquid burn was the leading cause in all age groups (p<0.05, p<0.001). Of the total patients, 89.6% were injured at home (p<0.001). The extremities were determined as the body area most often burned (p<0.001). While a single dressing was applied to 446 patients (29.5%), in 64.9% of cases polyclinic follow-up was terminated after the first 3 dressings. The mean number of dressings was greater in patients with deep dermal burns (mean 14.5, median 14, p<0.001).
CONCLUSION: A higher incidence of burns was found due to increasing urban populations compared to previous years. Currently, the majority of patients are referred to a healthcare facilty near their residences for follow-up after a few dressings. Unneccessary pre-sentation at specialist centres increases the workload of these centres and creates a burden of wasted time and transport expense for the patients. The application of current burn treatment principles in primary and secondary health facilities will reduce the workload of reference centres.
Key words: Burn; management; outpatient; referral.
muscle, and bones can be observed. Burns are not localised events affecting only the skin, but a very comprehensive trau-ma affecting the whole organism and the systemic physio-pathological effects define the clinical course and prognosis.
Burn is an injury which may be often encountered by an in-dividual and seen in the general population. Diagnosis and treatment principles of burns are quite different from those of other injuries. Treatment choices may vary from dressings of superficial skin lesions with conventional approaches to surgical intervention. In addition, it is an injury with different effects in the acute and chronic stages which can affect the whole life of the patient and their family. Burns may have a physical and psychological effect on healthcare personnel hav-ing a role in the treatment just as much on the patient and their family. Therefore, the teams working in this area need special training and experience.[1]
In burn injuiries, the majority of which occur as a result of ac-
O R I G I N A L A R T I C L E
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 27
Address for correspondence: Ahmet Çınar Yasti, M.D.
Doga AvSpor, Vakif Is Hani, Cankiri Cad., No: 67/2,
Dışkapı, 06030 Ankara, Turkey
Tel: +90 312 - 508 55 62 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):27-33doi: 10.5505/tjtes.2015.89217
Copyright 2015TJTES
INTRODUCTION
Burn injury is a significant health problem caused by the effect of heat, electricity and chemical substances, resulting in dam-ages of different depths and extent. By surrounding almost all body, these damages may spread to the epidermis and dermis layers, the most important protection against physical exter-nal effects, and in some cases damage to subcutaneous layers,

Sözen et al. Outpatient burn management and unnecessary referrals
cidents or neglect, the most important factors affecting mor-tality are the patient’s age, the surface area, and depth of the burn.[2] In inhalation burns, the severity is increased more. De-termination of the degree of the burn depth is generally made clinically and with physical examination. In the acute phase, a burn, as a dynamic injury, may continue to deepen in the first seventy-two hours.[3] In the determination of total body sur-face area burnt, rule of nines is widely used. For burn patients, treatment should be planned specifically for burns after any emergency trauma intervention has been made. The success of shock treatment, early eschar excision and early grafting, appropriate and timely use of antibiotics to combat infection, new dressing materials and some new closure methods are positive developments providing good results in burn treat-ment.[4] In addition to all these characteristics, vast majority of burns are suitable for treatment and follow-up in polyclinic conditions.[5] As has been reported in various series, the ma-jority of burns constitute less than 5% of total body surface area. The superficial nature of these burns makes it possible for the patients to be treated as outpatients.[5]
Until recently, burn facilities and healthcare personnel dealing with burns experienced difficulties since low number of units in operation were uncoordinated and lacked current treat-ment modalities. One of these problems was the unnecessary transfer of patients. In order to highlight this subject, the cor-rect application of the criteria for the referral of polyclinic pa-tients was clarified in a study published in 2002.[6] In addition to burn units and rooms established in intervening years,[7] the Directive on Action and Establishment of Burn Treat-ment Units in Healthcare Facilities with Beds was published in 2010[8] and in the following years, burn treatment algorithm was published in 2012.[9] This prospective study was planned with the aim of evaluating polyclinic demographics and refer-rals of an experienced burn unit centre and summarising the treatments made.
MATERIALS AND METHODS
This prospective study comprised all patients presented at the Burn Treatment Centre polyclinic of our hospital be-tween 1 January 2013 and 31 December 2013. These patients were followed up with prepared forms additional to the hos-pital records. Patients admitted to the Emergency Depart-ment and transferred directly to the clinic from other units by ambulance were excluded from the study.
The centre has a total of twelve beds consisting six intensive care, one isolation, two adult isolation, and three paediat-ric beds in the hospital located in the city centre. There is an operating theatre and a dressings room in the burn clinic and a polyclinic where outpatients are followed up. The burn clinic is approved by the Ministry of Health of Turkey as a reference hospital and has the role of a training centre giv-ing burn training and providing many specialist doctors and nurses with current information and treatment modalities.
In the current study, a record was made from the patients presented in the polyclinic including age, burn agents, number of dressings applied, choice of treatment applied (convention-al/sophisticated wound care products), rate of admittance or outpatient follow-up, hypertrophic scarring, keloid formation, and contracture development. The admittance criteria pub-lished by the Turkish Ministry of Health Burn Scientific Com-mittee were taken as the basis for differentiating outpatient or admittance indications of the patients (Table 1).[9]
The Chi-square test was used in data analysis and the Stu-dent’s t-test and Anova in the comparison of group mean values. A value of p<0.05 was accepted statistically significant.
RESULTS
In the period of the study, one thousand seven hundred and ninety-five patients presented in the polyclinic. The patients constituted eight hundred and fifty-four (47.6%) females and nine hundred and forty-one (52.4%) males, with a mean age of 28.63±20.03 years (range, 1 month-90 years) and median 28.0 years. The mean total burnt surface area (TBSA) was found to be 3.24%±4.26% with a median value of 2%.
Of the patients, two hundred and eighty-four (15.8%) were hospitalized for treatment. The hospitalized patients included 51.4% (146) females and 48.6% (138) males with a mean age of 32.55±21.96 years (range, 3 months-90 years), median age 31 years and a mean TBSA of 5.48%±5.56% (range, 1%-69%). The reason of admittance for treatment was that 47.5% (135/284) had second degree depth, of which 66% were deep dermal burns. As 32.4% (92/284) of the patients had super-ficial second degree burns, ninety-five patients were admit-ted due to superficial dermal burns. In the study period, 53% (284/535) of the patients admitted to the clinic comprised
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 128
Table 1. Patients requiring hospitalization for treatment
At all ages, TBSA <20% 2nd and 3rd degree burns
At all ages, TBSA ≥%5-10, 3rd degree burns
Ages <10 and >50, TBSA ≥%10, 2nd and 3rd degree burns
Face, ear, hand and foot burns
Major joint burns
Genital and perineal burns
Chemical burns
Electric burns
Lightening
Inhalation injuries
Concomitant multitrauma
Presence of co-morbidities
Pregnancy
Child abuse or suspicion
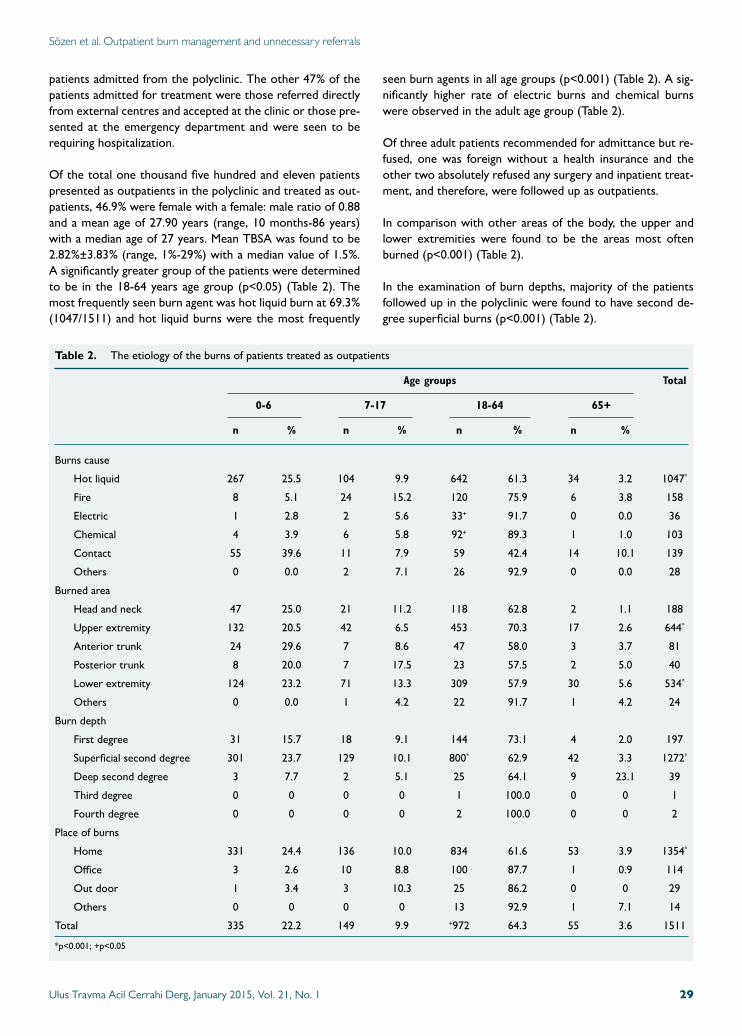
Sözen et al. Outpatient burn management and unnecessary referrals
patients admitted from the polyclinic. The other 47% of the patients admitted for treatment were those referred directly from external centres and accepted at the clinic or those pre-sented at the emergency department and were seen to be requiring hospitalization.
Of the total one thousand five hundred and eleven patients presented as outpatients in the polyclinic and treated as out-patients, 46.9% were female with a female: male ratio of 0.88 and a mean age of 27.90 years (range, 10 months-86 years) with a median age of 27 years. Mean TBSA was found to be 2.82%±3.83% (range, 1%-29%) with a median value of 1.5%. A significantly greater group of the patients were determined to be in the 18-64 years age group (p<0.05) (Table 2). The most frequently seen burn agent was hot liquid burn at 69.3% (1047/1511) and hot liquid burns were the most frequently
seen burn agents in all age groups (p<0.001) (Table 2). A sig-nificantly higher rate of electric burns and chemical burns were observed in the adult age group (Table 2).
Of three adult patients recommended for admittance but re-fused, one was foreign without a health insurance and the other two absolutely refused any surgery and inpatient treat-ment, and therefore, were followed up as outpatients.
In comparison with other areas of the body, the upper and lower extremities were found to be the areas most often burned (p<0.001) (Table 2).
In the examination of burn depths, majority of the patients followed up in the polyclinic were found to have second de-gree superficial burns (p<0.001) (Table 2).
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 29
Table 2. The etiology of the burns of patients treated as outpatients
Age groups Total
0-6 7-17 18-64 65+
n % n % n % n %
Burns cause
Hot liquid 267 25.5 104 9.9 642 61.3 34 3.2 1047*
Fire 8 5.1 24 15.2 120 75.9 6 3.8 158
Electric 1 2.8 2 5.6 33+ 91.7 0 0.0 36
Chemical 4 3.9 6 5.8 92+ 89.3 1 1.0 103
Contact 55 39.6 11 7.9 59 42.4 14 10.1 139
Others 0 0.0 2 7.1 26 92.9 0 0.0 28
Burned area
Head and neck 47 25.0 21 11.2 118 62.8 2 1.1 188
Upper extremity 132 20.5 42 6.5 453 70.3 17 2.6 644*
Anterior trunk 24 29.6 7 8.6 47 58.0 3 3.7 81
Posterior trunk 8 20.0 7 17.5 23 57.5 2 5.0 40
Lower extremity 124 23.2 71 13.3 309 57.9 30 5.6 534*
Others 0 0.0 1 4.2 22 91.7 1 4.2 24
Burn depth
First degree 31 15.7 18 9.1 144 73.1 4 2.0 197
Superficial second degree 301 23.7 129 10.1 800* 62.9 42 3.3 1272*
Deep second degree 3 7.7 2 5.1 25 64.1 9 23.1 39
Third degree 0 0 0 0 1 100.0 0 0 1
Fourth degree 0 0 0 0 2 100.0 0 0 2
Place of burns
Home 331 24.4 136 10.0 834 61.6 53 3.9 1354*
Office 3 2.6 10 8.8 100 87.7 1 0.9 114
Out door 1 3.4 3 10.3 25 86.2 0 0 29
Others 0 0 0 0 13 92.9 1 7.1 14
Total 335 22.2 149 9.9 +972 64.3 55 3.6 1511
*p<0.001; +p<0.05
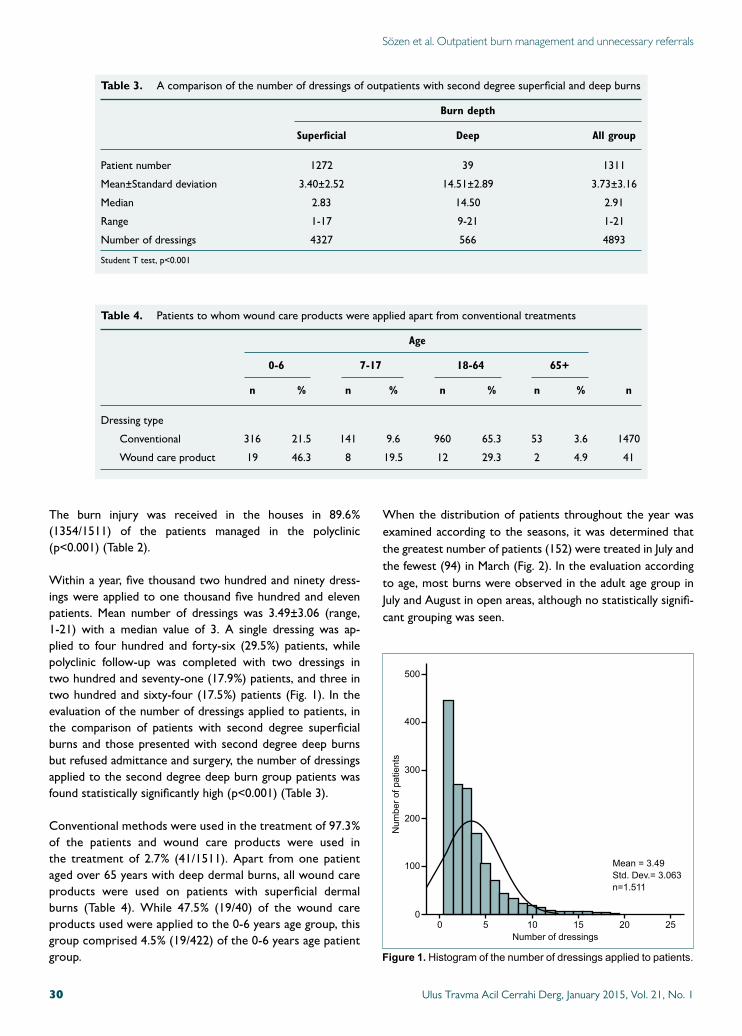
The burn injury was received in the houses in 89.6% (1354/1511) of the patients managed in the polyclinic (p<0.001) (Table 2).
Within a year, five thousand two hundred and ninety dress-ings were applied to one thousand five hundred and eleven patients. Mean number of dressings was 3.49±3.06 (range, 1-21) with a median value of 3. A single dressing was ap-plied to four hundred and forty-six (29.5%) patients, while polyclinic follow-up was completed with two dressings in two hundred and seventy-one (17.9%) patients, and three in two hundred and sixty-four (17.5%) patients (Fig. 1). In the evaluation of the number of dressings applied to patients, in the comparison of patients with second degree superficial burns and those presented with second degree deep burns but refused admittance and surgery, the number of dressings applied to the second degree deep burn group patients was found statistically significantly high (p<0.001) (Table 3).
Conventional methods were used in the treatment of 97.3% of the patients and wound care products were used in the treatment of 2.7% (41/1511). Apart from one patient aged over 65 years with deep dermal burns, all wound care products were used on patients with superficial dermal burns (Table 4). While 47.5% (19/40) of the wound care products used were applied to the 0-6 years age group, this group comprised 4.5% (19/422) of the 0-6 years age patient group.
When the distribution of patients throughout the year was examined according to the seasons, it was determined that the greatest number of patients (152) were treated in July and the fewest (94) in March (Fig. 2). In the evaluation according to age, most burns were observed in the adult age group in July and August in open areas, although no statistically signifi-cant grouping was seen.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 130
Sözen et al. Outpatient burn management and unnecessary referrals
Table 3. A comparison of the number of dressings of outpatients with second degree superficial and deep burns
Burn depth
Superficial Deep All group
Patient number 1272 39 1311
Mean±Standard deviation 3.40±2.52 14.51±2.89 3.73±3.16
Median 2.83 14.50 2.91
Range 1-17 9-21 1-21
Number of dressings 4327 566 4893
Student T test, p<0.001
Table 4. Patients to whom wound care products were applied apart from conventional treatments
Age
0-6 7-17 18-64 65+
n % n % n % n % n
Dressing type
Conventional 316 21.5 141 9.6 960 65.3 53 3.6 1470
Wound care product 19 46.3 8 19.5 12 29.3 2 4.9 41
Figure 1. Histogramofthenumberofdressingsappliedtopatients.
500
400
300
200
100
Num
berofpatients
Numberofdressings
Mean=3.49Std.Dev.=3.063n=1.511
00 5 10 15 20 25
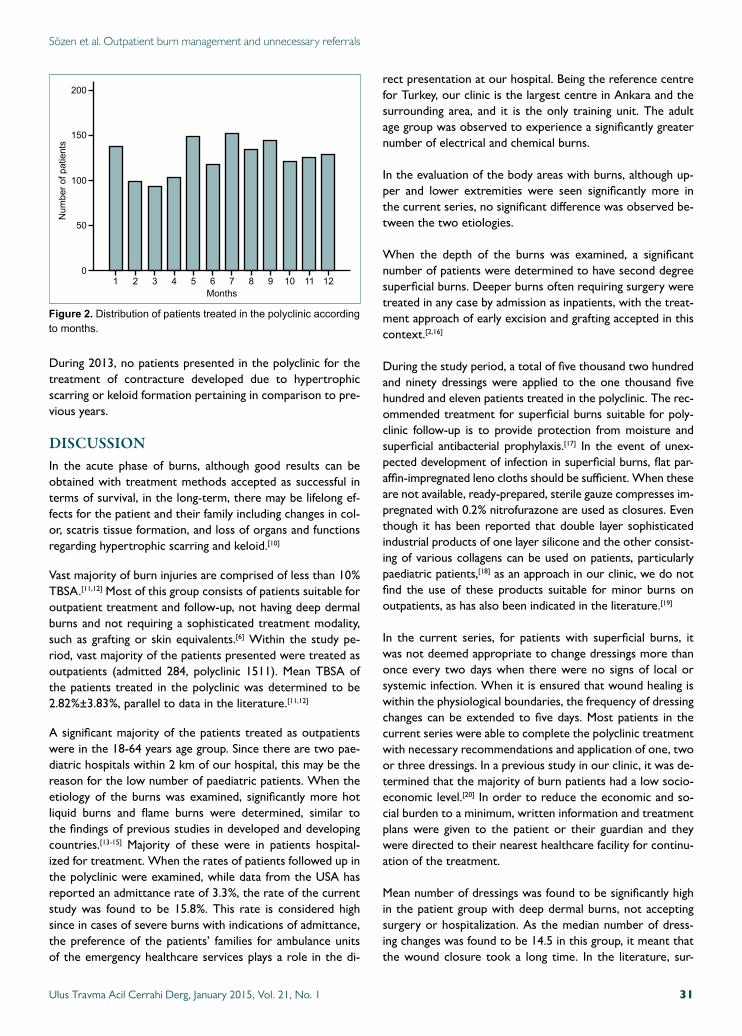
During 2013, no patients presented in the polyclinic for the treatment of contracture developed due to hypertrophic scarring or keloid formation pertaining in comparison to pre-vious years.
DISCUSSIONIn the acute phase of burns, although good results can be obtained with treatment methods accepted as successful in terms of survival, in the long-term, there may be lifelong ef-fects for the patient and their family including changes in col-or, scatris tissue formation, and loss of organs and functions regarding hypertrophic scarring and keloid.[10]
Vast majority of burn injuries are comprised of less than 10% TBSA.[11,12] Most of this group consists of patients suitable for outpatient treatment and follow-up, not having deep dermal burns and not requiring a sophisticated treatment modality, such as grafting or skin equivalents.[6] Within the study pe-riod, vast majority of the patients presented were treated as outpatients (admitted 284, polyclinic 1511). Mean TBSA of the patients treated in the polyclinic was determined to be 2.82%±3.83%, parallel to data in the literature.[11,12]
A significant majority of the patients treated as outpatients were in the 18-64 years age group. Since there are two pae-diatric hospitals within 2 km of our hospital, this may be the reason for the low number of paediatric patients. When the etiology of the burns was examined, significantly more hot liquid burns and flame burns were determined, similar to the findings of previous studies in developed and developing countries.[13-15] Majority of these were in patients hospital-ized for treatment. When the rates of patients followed up in the polyclinic were examined, while data from the USA has reported an admittance rate of 3.3%, the rate of the current study was found to be 15.8%. This rate is considered high since in cases of severe burns with indications of admittance, the preference of the patients’ families for ambulance units of the emergency healthcare services plays a role in the di-
rect presentation at our hospital. Being the reference centre for Turkey, our clinic is the largest centre in Ankara and the surrounding area, and it is the only training unit. The adult age group was observed to experience a significantly greater number of electrical and chemical burns.
In the evaluation of the body areas with burns, although up-per and lower extremities were seen significantly more in the current series, no significant difference was observed be-tween the two etiologies.
When the depth of the burns was examined, a significant number of patients were determined to have second degree superficial burns. Deeper burns often requiring surgery were treated in any case by admission as inpatients, with the treat-ment approach of early excision and grafting accepted in this context.[2,16]
During the study period, a total of five thousand two hundred and ninety dressings were applied to the one thousand five hundred and eleven patients treated in the polyclinic. The rec-ommended treatment for superficial burns suitable for poly-clinic follow-up is to provide protection from moisture and superficial antibacterial prophylaxis.[17] In the event of unex-pected development of infection in superficial burns, flat par-affin-impregnated leno cloths should be sufficient. When these are not available, ready-prepared, sterile gauze compresses im-pregnated with 0.2% nitrofurazone are used as closures. Even though it has been reported that double layer sophisticated industrial products of one layer silicone and the other consist-ing of various collagens can be used on patients, particularly paediatric patients,[18] as an approach in our clinic, we do not find the use of these products suitable for minor burns on outpatients, as has also been indicated in the literature.[19]
In the current series, for patients with superficial burns, it was not deemed appropriate to change dressings more than once every two days when there were no signs of local or systemic infection. When it is ensured that wound healing is within the physiological boundaries, the frequency of dressing changes can be extended to five days. Most patients in the current series were able to complete the polyclinic treatment with necessary recommendations and application of one, two or three dressings. In a previous study in our clinic, it was de-termined that the majority of burn patients had a low socio-economic level.[20] In order to reduce the economic and so-cial burden to a minimum, written information and treatment plans were given to the patient or their guardian and they were directed to their nearest healthcare facility for continu-ation of the treatment.
Mean number of dressings was found to be significantly high in the patient group with deep dermal burns, not accepting surgery or hospitalization. As the median number of dress-ing changes was found to be 14.5 in this group, it meant that the wound closure took a long time. In the literature, sur-
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 31
Sözen et al. Outpatient burn management and unnecessary referrals
Figure 2. Distributionofpatientstreatedinthepolyclinicaccordingtomonths.
200
150
50
100
Num
berofpatients
Months
01 2 3 4 5 6 7 8 9 10 11 12

gical treatment has been recommended for patients whose wound healing is thought to take a 21-day period.[21] Of the total one thousand three hundred and eleven patients in the current study with second degree burns, thirty-nine patients had deep burns. In this patient group, the maximum healing period was determined as 21 days with daily dressing changes. No data of formation of hypertrophic scarring was found in this patient group. In addition, no patient presented at the plastic surgery clinic of our hospital or clinic owing to con-tracture during the study period. This can be considered to be explained by the provision of appropriate physical exer-cises and proper application of treatment. In this respect, it would not have been ethical to have planned a randomized prospective study.
When the outpatient numbers of our polyclinic for 2013 were compared with those of 2002, an increase of 169.2% was seen (1511/893).[6] For the same period, a 20% increase was observed in the population of the province of Ankara (4.007.860, 2002; 4.965.384, 2013; data from the Turkish Board of Statistics [TÜİK]).
For 29.6% of the patients in the current study, a single dress-ing was sufficient. In a study from the same centre in 2002, this rate was 38%.[6] Although seen as a decrease in percent-age, the number of patients was three hudrend and forty-two compared to the current study number of four hundred and forty-six. This rate, explaining an increase of 30.4% in the patient group with a single dressing applied, is significant for the period in which the population of Ankara increased 20%. Furthermore, within that period, two burn units and a burn centre and polyclinic for paediatric patients came into ser-vice. From 2008, the Burn Scientific Committee established by the Ministry of Health came into operation, prepared a di-rective, and published the Burn Treatment Algorithm, which has value in the sense of being the first original treatment algorithm in Turkey.[7-9] However, from 2013 onwards, be-sides the acquisition of current information and treatment approaches by healthcare personnel, the necessity for treat-ments of simple burn injuries outside third stage healthcare institutions came to the fore. In a study by Lloyd et al.[22] of the American example, majority of burn patients has been observed to be treated by family doctors through postgradu-ate training and training programmes of discussions at con-gresses. By this way, a tangible improvement was obtained for both the patient and social security institutions. The close location of a healthcare provider for treatment will obviously be more useful for patients physically, economically, socially, and psychologically.
As our clinic is accepted as a developed, reference unit burn centre, the number of polyclinic patients is much greater. By increasing the number of staff trained in the field of burns, instead of burns of a degree requiring a single dressing, the intensity of our centre will be reduced. Thus, we will have room for patients who truly need treatment in an advanced
burn centre. Otherwise, there will be economic loss in addi-tion to the physical and psychological trauma to the patient and their family even when the burn injury is minor.
Of the patients admitted to our clinic, 53% were from the polyclinic and 47% were referred for hospitalization. These patients were not only from nearly every region of Turkey but also from neighbouring countries such as Azerbaijan, Iraq, Syria, Afghanistan, Russia, Albania, Libya, Somalia, and Sudan and also from distant countries. The obtained results are positive feedbacks for a reference centre and repeated patient referencing is accepted as a measurement for our clinic accepted as a reference centre. Moreover, our clinic has been accredited as a Burn Training Centre by the Ministry of Health of Turkey.
While 97.3% of the patients were treated by the above-men-tioned conventional methods, wound care products were used on a very small number, showing that the effort and labour input of healthcare personnel are very important in the treatment of burns. That the number of physicians and nurses providing service was the same in 2013 as in 2002 clearly shows the additional workload. The use of wound care products for polyclinic patients would decrease the frequency of dressing changes and increase patient comfort. The real reason for the low use of these products in the polyclinic is that reimbursement is not made by the social security system for this outpatient group of patients.
ConclusionThe increase in the number of patients determined in the study period reveals that burns are still a serious problem in our country. In comparison with the past, a high number of patients treated with one or two dressings indicates that the treatment of minor burns is not made in primary and sec-ondary healthcare facilities. The treatment of patients with minor burns in close or convenient other healthcare institu-tions would reduce the workload of centres as well as ad-ditional economic and psychological burden on patients and their families and would, thus, save time for all.
Conflict of interest: None declared.
REFERENCES
1. Pavoni V, Gianesello L, Paparella L, Buoninsegni LT, Barboni E. Out-come predictors and quality of life of severe burn patients admitted to intensive care unit. Scand J Trauma Resusc Emerg Med 2010;18:24.
2. Wolf SE, Debroy M, Herndon DN. The cornerstones and directions of pediatric burn care. Pediatr Surg Int 1997;12:312-20.
3. Youn YK, LaLonde C, Demling R. The role of mediators in the response to thermal injury. World J Surg 1992;16:30-6.
4. Supple KG. Physiologic response to burn injury. Crit Care Nurs Clin North Am 2004;16:119-26.
5. National Burn Repository 2005 report. American Burn Association; 2006:35.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 132
Sözen et al. Outpatient burn management and unnecessary referrals

6. Yastı AÇ, Kama AN. Yanık olgularında gereksiz hasta nakilleri ve sonuçları. Ankara Cerrahi Dergisi 2005;7:75-8.
7. Yasti AC, Koc O, Sencan I. Organizing burn patient hospitalisation and transfer at a developing country. World J Surg 2011;35:430.
8. http://www.istanbulsaglik.gov.tr/w/sb/tedk/pdf/yonergeson.pdf.
9. http://www.tkhk.gov.tr/Eklenti/307,23022012-tc-sb-yanik-algoritma-si.pdf?
10. Rossi LA, Braga EC, Barruffini RC, Carvalho EC. Childhood burn inju-ries: circumstances of occurrences and their prevention in Ribeirão Preto, Brazil. Burns 1998;24:416-9.
11. American Burn Association. Burn incidence and treatment in the United States: fact sheet 2011. http://www. ameriburn.org/resources_factsheet.php [cited 25.10.13].
12. Brusselaers N, Monstrey S, Vogelaers D, Hoste E, Blot S. Severe burn injury in Europe: a systematic review of the incidence, etiology, morbidity, and mortality. Crit Care 2010;14:R188.
13. Herndon D. Epidemiological, demographic, and outcome characteristics of burn injury. Total burn care (4th ed.). Edinburgh: Saunders; p. 23. ISBN 978-1-4377-2786-9.
14. Asuquo ME, Ekpo R, Ngim O, Agbor C. A prospective study of burn trauma in adults at the university of calabar teaching hospital, calabar (South eastern Nigeria). Eplasty 2008;8:36.
15. Han TH, Kim JH, Yang MS, Han KW, Han SH, Jung JA, et al. A retro-spective analysis of 19,157 burns patients: 18-year experience from Hal-lym Burn Center in Seoul, Korea. Burns 2005;31:465-70.
16. Senel E, Yasti AC, Reis E, Doganay M, Karacan CD, Kama NA. Effects on mortality of changing trends in the management of burned children in Turkey: eight years’ experience. Burns 2009;35:372-7.
17. Durtschi MB, Orgain C, Counts GW, Heimbach DM. A prospective study of prophylactic penicillin in acutely burned hospitalized patients. J Trauma 1982;22:11-4.
18. Barret JP, Dziewulski P, Ramzy PI, Wolf SE, Desai MH, Herndon DN. Biobrane versus 1% silver sulfadiazine in second-degree pediatric burns. Plast Reconstr Surg 2000;105:62-5.
19. Hartford CE. Care of outpatient burns. In: Herndon DN, editor. Total burn care. 4th ed., 2012. p. 81-92.
20. Yasti AC, Tumer AR, Atli M, Tutuncu T, Derinoz A, Kama NA. A clini-cal forensic scientist in the burns unit: necessity or not? A prospective clinical study. Burns 2006;32:77-82.
21. Engrav LH, Heimbach DM, Reus JL, Harnar TJ, Marvin JA. Early exci-sion and grafting vs. nonoperative treatment of burns of indeterminant depth: a randomized prospective study. J Trauma 1983;23:1001-4.
22. Lloyd EC, Rodgers BC, Michener M, Williams MS. Outpatient burns: prevention and care. Am Fam Physician 2012;85:25-32.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 33
Sözen et al. Outpatient burn management and unnecessary referrals
OLGU SUNUMU
Yanık hastalarının ayaktan takibi ve gereksiz hasta nakilleriDr. İsa Sözen,1 Dr. Cem Emir Guldogan,1 Dr. Kemal Kismet,2 Dr. Mehmet Zafer Sabuncuoğlu,3 Dr. Ahmet Çınar Yasti1,4
1AnkaraNumuneEğitimveAraştırmaHastanesi,GenelCerrahiKliniği,YanıkTedaviMerkezi,Ankara;2AnkaraEğitimveAraştırmaHastanesi,GenelCerrahiKliniği,YanıkÜnitesi,Ankara;3SüleymanDemirelÜniversitesiTıpFakültesi,GenelCerrahiAnabilimDalı,Isparta;4HititÜniversitesiTıpFakültesi,GenelCerrahiAnabilimDalı,Çorum
AMAÇ: Polikliniğimize başvuran yanık hasta profilini ortaya koymak ve tedavi yönetimini geçmiş seriler ile karşılaştırarak güncel durumu değerlen-dirmektir.GEREÇ VE YÖNTEM: Bir yıl süreyle polikliniğimize başvuran hastalar ileriye yönelik çalışmaya alındı. Tüm hastaların kayıt altına alınan cinsiyet, yaş, yanık yüzdesi, yanık yeri, yanık nedeni, yanık derecesi, pansuman malzemesi, pansuman sayısı, tedavi şekli, olay yeri ve olayın olduğu aya göre dağılımı incelendi.BULGULAR: Toplam 1795 hastanın yönetimleri poliklinikte tamamlanan 1511’inin ortalama yaşı 27.9, kadın/erkek oranı 0.88 olmuştur. Çoğunluğu 18-64 yaş hastalar oluştururken tüm gruplarda sıcak sıvı yanığı ilk sıradaydı (p<0.05, p<0.001). Hastaların %89.6’sı evde yaralanmıştı (p<0.001). Ekstremiteler diğer bölgelere göre daha sık yanan vücut bölgesiydi (p<0.001). Hastaların 446’sına (%29.5) tek pansuman uygulanırken %64.9’u ilk üç pansuman sonrasında hastanemiz poliklinik takipleri sonlandırılmıştır. Derin dermal yanıklı hastalarda ortalama pansuman sayısı daha fazla olmuştur (ortalama 14.5, ortanca 14, p<0.001).TARTIŞMA: Geçmiş yıllar ile yapılan karşılaştırmada il nüfusu artışından daha yüksek yanık insidansı bulunmuştur. Halen hastaların çoğunluğu az sayıda pansuman sonrası takipleri için evlerine yakın sağlık birimlerine yönlendirilmektedir. Mevcut durumda hastaların deneyimli merkezlere ge-reksiz başvuruları ile bu merkezlerin iş yükünün artırılması yanında hastalara ilave ulaşım yükü ve zaman israfı yaşatılmaktadır. Güncel yanık tedavi prensiplerinin birinci ve ikinci basamakta edinilmesi ile referans merkezin iş yükü azaltılabilecektir.Anahtar sözcükler: Ayaktan; nakil; yanık; yönetim.
Ulus Travma Acil Cerrahi Derg 2015;21(1):27-33 doi: 10.5505/tjtes.2015.89217
KLİNİK ÇALIŞMA - ÖZET
Mortality risk factors in burn care units consideringthe clinical significance of acinetobacter infectionsAynur Atilla, M.D.,1 Leman Tomak, M.D.,2 Ali Osman Katrancı, M.D.,3 Alper Ceylan, M.D.,4 S. Sırrı Kılıç, M.D.1
1DepartmentofInfectiousDiseasesandClinicalMicrobiology,SamsunTrainingandResearchHospital,Samsun;2DepartmentofBiostatistics,OndokuzmayisUniversityFacultyofMedicine,Samsun;3DepartmentofPediatricSurgery,SamsunTrainingandResearchHospital,Samsun;4DepartmentofGeneralSurgery,SamsunTrainingandResearchHospital,Samsun
ABSTRACT
BACKGROUND: This study aimed to evaluate risk factors and the role of Acinetobacter isolates in mortality due to burns since morbidity and mortality rates are considerably high.
METHODS: A total of four hundred and sixty-five patients hospitalized in our Burn Care Unit between January 2009 and May 2011 were reviewed retrospectively. Logistic regression analysis was used in order to predict the risk.
RESULTS: Mortality rates were as follows: 7.5% in general, 3.9% for under 17 years of age, 12% for between 18-64 years of age, and 24% for over 65 years of age (p<0.001).
CONCLUSION: As the burnt body surface area increased, higher mortality rates were detected. Despite higher mortality rates, Acinetobacter infections were not found risk factors for mortality.
Key words: Acinetobacter; burn; infection; mortality.
burns.[2] Although recent studies indicate increased role of Acinetobacter infection in mortality in burn patients, some controversy still remains about its exact impact.[3] Due to the increased rate of worldwide resistance and infections, Acinetobacter isolates represent a challenge in the treatment of burns.[4]
The data of a total of four hundred and sixty five patients in our burn care unit were reviewed and patients’ characteris-tics and outcome including burn data, infections encountered, pathogens and antibiotic susceptibility tests, infections caused by resistant organisms, risk factors for mortality, and the role of Acinetobacter isolates in mortality were evaluated.
MATERIALS AND METHODS
This study was conducted at Samsun Education and Train-ing Hospital, a 620-bed hospital with 13 beds reserved for the burn unit. Our burn unit is a tertiary care center serving Northern Turkey, the Black Sea region, with an approximate area population of 5.000.000. The burn unit consists an inten-sive care unit with 4 beds and 9 single rooms. The electronic medical records database of the burn unit and the file records of Infection Control Committee were searched to identify all patients hospitalized from January 2009 to May 2011.
O R I G I N A L A R T I C L E
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 134
Address for correspondence: Aynur Atilla, M.D.
Samsun Eğitim ve Araştırma Hastanesi, Kadıköy Mahallesi,
Barış Bulvarı, No: 199, Samsun, Turkey
Tel: +90 362 - 311 15 00 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):34-38doi: 10.5505/tjtes.2015.76814
Copyright 2015TJTES
INTRODUCTION
Burns are one of the most common and devastating forms of trauma. Improved outcomes for severely burnt patients have been attributed to medical advances in fluid resuscitation, nutritional support, pulmonary care, burn wound care, and infection control practices. Seventy-five percent of all deaths are currently related to sepsis from burn wound infections or other infection complications in patients with severe burns over more than 40% of Total Body Surface Area (TBSA).[1] Seriously burnt patients have an increased risk for noso-comial infections (NIs) due to the nature of the burn injury itself and NI is the most common cause of death following
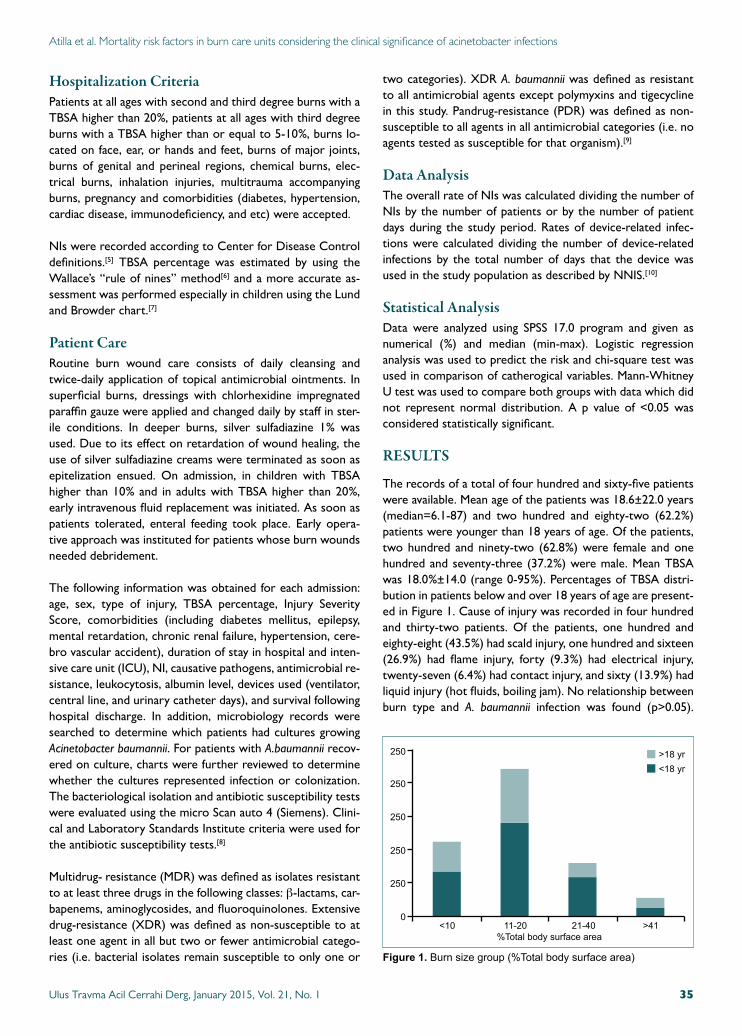
Hospitalization CriteriaPatients at all ages with second and third degree burns with a TBSA higher than 20%, patients at all ages with third degree burns with a TBSA higher than or equal to 5-10%, burns lo-cated on face, ear, or hands and feet, burns of major joints, burns of genital and perineal regions, chemical burns, elec-trical burns, inhalation injuries, multitrauma accompanying burns, pregnancy and comorbidities (diabetes, hypertension, cardiac disease, immunodeficiency, and etc) were accepted.
NIs were recorded according to Center for Disease Control definitions.[5] TBSA percentage was estimated by using the Wallace’s “rule of nines” method[6] and a more accurate as-sessment was performed especially in children using the Lund and Browder chart.[7]
Patient CareRoutine burn wound care consists of daily cleansing and twice-daily application of topical antimicrobial ointments. In superficial burns, dressings with chlorhexidine impregnated paraffin gauze were applied and changed daily by staff in ster-ile conditions. In deeper burns, silver sulfadiazine 1% was used. Due to its effect on retardation of wound healing, the use of silver sulfadiazine creams were terminated as soon as epitelization ensued. On admission, in children with TBSA higher than 10% and in adults with TBSA higher than 20%, early intravenous fluid replacement was initiated. As soon as patients tolerated, enteral feeding took place. Early opera-tive approach was instituted for patients whose burn wounds needed debridement.
The following information was obtained for each admission: age, sex, type of injury, TBSA percentage, Injury Severity Score, comorbidities (including diabetes mellitus, epilepsy, mental retardation, chronic renal failure, hypertension, cere-bro vascular accident), duration of stay in hospital and inten-sive care unit (ICU), NI, causative pathogens, antimicrobial re-sistance, leukocytosis, albumin level, devices used (ventilator, central line, and urinary catheter days), and survival following hospital discharge. In addition, microbiology records were searched to determine which patients had cultures growing Acinetobacter baumannii. For patients with A.baumannii recov-ered on culture, charts were further reviewed to determine whether the cultures represented infection or colonization. The bacteriological isolation and antibiotic susceptibility tests were evaluated using the micro Scan auto 4 (Siemens). Clini-cal and Laboratory Standards Institute criteria were used for the antibiotic susceptibility tests.[8]
Multidrug- resistance (MDR) was defined as isolates resistant to at least three drugs in the following classes: β-lactams, car-bapenems, aminoglycosides, and fluoroquinolones. Extensive drug-resistance (XDR) was defined as non-susceptible to at least one agent in all but two or fewer antimicrobial catego-ries (i.e. bacterial isolates remain susceptible to only one or
two categories). XDR A. baumannii was defined as resistant to all antimicrobial agents except polymyxins and tigecycline in this study. Pandrug-resistance (PDR) was defined as non-susceptible to all agents in all antimicrobial categories (i.e. no agents tested as susceptible for that organism).[9]
Data AnalysisThe overall rate of NIs was calculated dividing the number of NIs by the number of patients or by the number of patient days during the study period. Rates of device-related infec-tions were calculated dividing the number of device-related infections by the total number of days that the device was used in the study population as described by NNIS.[10]
Statistical AnalysisData were analyzed using SPSS 17.0 program and given as numerical (%) and median (min-max). Logistic regression analysis was used to predict the risk and chi-square test was used in comparison of catherogical variables. Mann-Whitney U test was used to compare both groups with data which did not represent normal distribution. A p value of <0.05 was considered statistically significant.
RESULTS
The records of a total of four hundred and sixty-five patients were available. Mean age of the patients was 18.6±22.0 years (median=6.1-87) and two hundred and eighty-two (62.2%) patients were younger than 18 years of age. Of the patients, two hundred and ninety-two (62.8%) were female and one hundred and seventy-three (37.2%) were male. Mean TBSA was 18.0%±14.0 (range 0-95%). Percentages of TBSA distri-bution in patients below and over 18 years of age are present-ed in Figure 1. Cause of injury was recorded in four hundred and thirty-two patients. Of the patients, one hundred and eighty-eight (43.5%) had scald injury, one hundred and sixteen (26.9%) had flame injury, forty (9.3%) had electrical injury, twenty-seven (6.4%) had contact injury, and sixty (13.9%) had liquid injury (hot fluids, boiling jam). No relationship between burn type and A. baumannii infection was found (p>0.05).
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 35
Figure 1. Burnsizegroup(%Totalbodysurfacearea)
250
250
250
250
250
<10 11-20 21-40 >41%Totalbodysurfacearea
>18yr<18yr
0
Atilla et al. Mortality risk factors in burn care units considering the clinical significance of acinetobacter infections
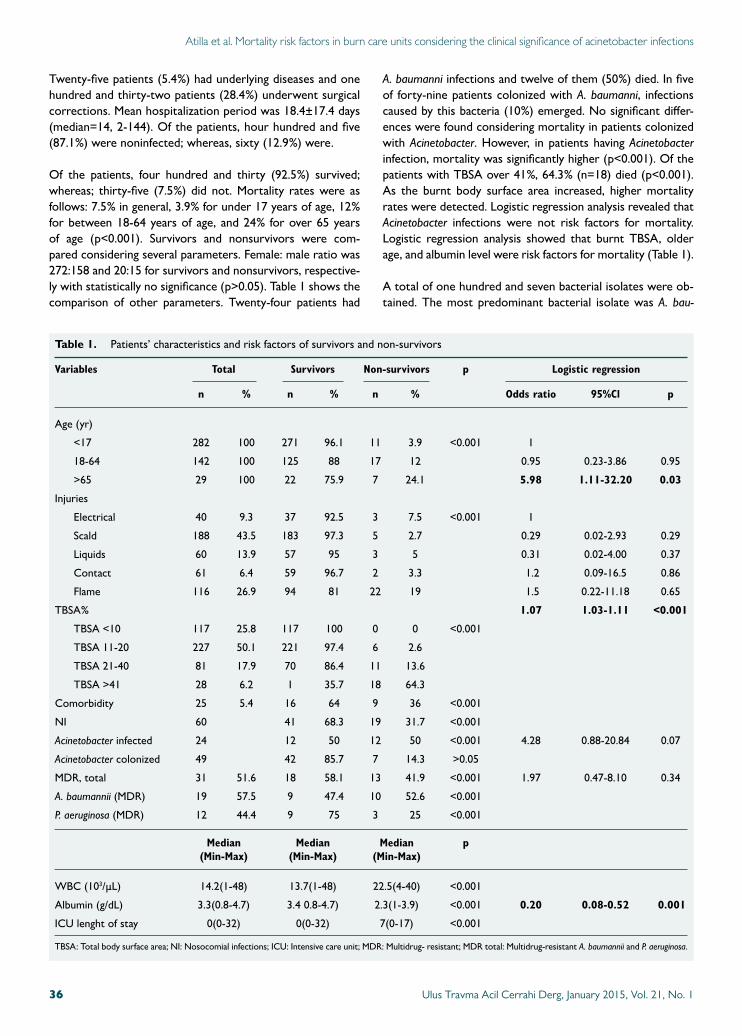
Twenty-five patients (5.4%) had underlying diseases and one hundred and thirty-two patients (28.4%) underwent surgical corrections. Mean hospitalization period was 18.4±17.4 days (median=14, 2-144). Of the patients, hour hundred and five (87.1%) were noninfected; whereas, sixty (12.9%) were.
Of the patients, four hundred and thirty (92.5%) survived; whereas; thirty-five (7.5%) did not. Mortality rates were as follows: 7.5% in general, 3.9% for under 17 years of age, 12% for between 18-64 years of age, and 24% for over 65 years of age (p<0.001). Survivors and nonsurvivors were com-pared considering several parameters. Female: male ratio was 272:158 and 20:15 for survivors and nonsurvivors, respective-ly with statistically no significance (p>0.05). Table 1 shows the comparison of other parameters. Twenty-four patients had
A. baumanni infections and twelve of them (50%) died. In five of forty-nine patients colonized with A. baumanni, infections caused by this bacteria (10%) emerged. No significant differ-ences were found considering mortality in patients colonized with Acinetobacter. However, in patients having Acinetobacter infection, mortality was significantly higher (p<0.001). Of the patients with TBSA over 41%, 64.3% (n=18) died (p<0.001). As the burnt body surface area increased, higher mortality rates were detected. Logistic regression analysis revealed that Acinetobacter infections were not risk factors for mortality. Logistic regression analysis showed that burnt TBSA, older age, and albumin level were risk factors for mortality (Table 1).
A total of one hundred and seven bacterial isolates were ob-tained. The most predominant bacterial isolate was A. bau-
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 136
Table 1. Patients’ characteristics and risk factors of survivors and non-survivors
Variables Total Survivors Non-survivors p Logistic regression
n % n % n % Odds ratio 95%Cl p
Age (yr)
<17 282 100 271 96.1 11 3.9 <0.001 1
18-64 142 100 125 88 17 12 0.95 0.23-3.86 0.95
>65 29 100 22 75.9 7 24.1 5.98 1.11-32.20 0.03
Injuries
Electrical 40 9.3 37 92.5 3 7.5 <0.001 1
Scald 188 43.5 183 97.3 5 2.7 0.29 0.02-2.93 0.29
Liquids 60 13.9 57 95 3 5 0.31 0.02-4.00 0.37
Contact 61 6.4 59 96.7 2 3.3 1.2 0.09-16.5 0.86
Flame 116 26.9 94 81 22 19 1.5 0.22-11.18 0.65
TBSA% 1.07 1.03-1.11 <0.001
TBSA <10 117 25.8 117 100 0 0 <0.001
TBSA 11-20 227 50.1 221 97.4 6 2.6
TBSA 21-40 81 17.9 70 86.4 11 13.6
TBSA >41 28 6.2 1 35.7 18 64.3
Comorbidity 25 5.4 16 64 9 36 <0.001
NI 60 41 68.3 19 31.7 <0.001
Acinetobacter infected 24 12 50 12 50 <0.001 4.28 0.88-20.84 0.07
Acinetobacter colonized 49 42 85.7 7 14.3 >0.05
MDR, total 31 51.6 18 58.1 13 41.9 <0.001 1.97 0.47-8.10 0.34
A. baumannii (MDR) 19 57.5 9 47.4 10 52.6 <0.001
P. aeruginosa (MDR) 12 44.4 9 75 3 25 <0.001
Median Median Median p (Min-Max) (Min-Max) (Min-Max)
WBC (103/µL) 14.2(1-48) 13.7(1-48) 22.5(4-40) <0.001
Albumin (g/dL) 3.3(0.8-4.7) 3.4 0.8-4.7) 2.3(1-3.9) <0.001 0.20 0.08-0.52 0.001
ICU lenght of stay 0(0-32) 0(0-32) 7(0-17) <0.001
TBSA: Total body surface area; NI: Nosocomial infections; ICU: Intensive care unit; MDR: Multidrug- resistant; MDR total: Multidrug-resistant A. baumannii and P. aeruginosa.
Atilla et al. Mortality risk factors in burn care units considering the clinical significance of acinetobacter infections

manni 36 (33.6%), followed by Pseudomonas aeruginosa 27 (25.2%). Nineteen of the twenty-seven P. aeruginosa isolates (70.3%) and twenty-nine of the thirty-three A. baumannii iso-lates (87.8%) were multidrug resistant. Of the Acinetobacter isolates, fifteen had XDR and in Pseudomonas isolates nine-teen had XDR; whereas, none had PDR.
Incidence of InfectionSixty (60/465=12.9%) patients had sixty-eight NIs with an incidence density of 9.9 infections/ 1000 patient days. Burn wound infection (n=38, 55%) was the most frequent NI. The rates of central vascular catheter, urinary catheter and ven-tilator usage per 1000 hospitalization days were 0.14, 0.15, 0.02, respectively. NI rates related to central vascular cath-eter, urinary catheter and ventilator usage were 5.1, 1.8 and 0 per 1000 invasive device usage days, respectively.
DISCUSSIONIn burn patients, existence of infection, especially sepsis, still remains the most prominent predictive factor affecting mor-tality and morbidity. Burn injury, reduced immunity, invasive therapeutic and diagnostic procedures, and longer duration of hospitalization are all responsible for serious complications in burn patients. However, NIs are solely the most common cause of death in burns. Evaluating risk factors by assessing microbiological analysis of pathogens and preventive mea-sures, infection control and reducing the incidence of resis-tance are very important to lead treatment strategies.[2]
Considering emerging infection rates as success criteria, our incidence of NI was 12.9% and incidence density was 9.9/1000 patient days. It has been apparently known that burnt skin serves as an environment for colonization and in-fection and subsequently sepsis and possible death.[2] Despite the fact that NI was not the most important risk factor for mortality in our study, Alp et al. reported infected patients had approximately three times higher mortality rates than uninfected patients. Moreover, advanced age, underlying dis-eases, and higher TBSA percentage were the most significant risk factors for mortality in the study.[11] Zarei et al. have found that non-work-related burns, burnt TBSA, and body surface area affected by second- or third- degree burns are independent predictors of mortality.[12]
Although variables like age, type of injuries, TBSA percentage, co-morbidity, leukocyte, and serum albumin parameters may have affected mortality, only age over 65, TBSA percentage and serum albumin levels were found to be independent risk factors for mortality. Wang et al. have reported 30% mortal-ity in patients with TBSA higher than 70%. In addition, burn size, severe inhalation injury, serum creatinine, inotropic sup-port, thrombocytopenia, sepsis, and ventilator dependency have been reported as associated factors for mortality.[13] Al et al. have found that in addition to some other parameters, hypoalbuminemia and sepsis are important factors for mor-
tality.[14] Brusselaers et al. reported in a systematic review of the severe burn injuries in Europe from 1985 to 2009 that burn size and age were the main factors associated with mor-tality.[15] Church et al. have reported in an excellent review of burn wound infections that burns in the elderly population are more severe and result in a higher number of fatalities.[2] They have also indicated in a recent study assessing factors affecting burn mortality in the elderly population where two hundred and one patients were over 75 years of age that the mortality rate was 47.3%. In our study, mortality rates were found to gradually increase with age, 24% for over 65 years.
Due to emerging multidrug-resistant organisms mainly as Pseudomonas and Acinetobacter species, infections are asso-ciated with significant morbidity and mortality in burn pa-tients. Of special concern, Acinetobacter isolates have been increasingly reported in recent years and have emerged as a significant nosocomial pathogen.[4] The most common mi-croorganism isolated was A. baumannii in our study. As a high prevalance, 33.6% was in concordance with some reports. Chong et al. have reported A. baumannii in fifty-five of ninety-four patients[16] and Bayram et al. have found fifty-nine of two hundred and fifty isolates to be positive for A. baumannii.[17]
Acinetobacter was first considered in the 1970s as an impor-tant nosocomial pathogen. Majority of the clinical isolates were susceptiple to most antimicrobials in earlier periods; however, multi-drug resistant isolates have emerged due to extensive use of broad spectrum agents worldwide.[4] Our results revealed that MDR rates were also associated with increased mortality, not emerging as an underlying risk factor. Of the thirty-three patients with Acinetobacter, twenty-nine of them and of the twenty-seven patients with P. aeruginosa, nineteen of them represented MDR. Keen et al. reported their experience over a 5-year period that more than half of A. baumannii isolates were multi-drug resistant.[18]
Increased mortality rates were detected in Acinetobacter in-fections (p<0.001); however, this was not regarded a risk fac-tor for mortality (logistic regression analysis). Albrecht et al. have revealed that Acinetobacter infection is associated with burn related mortality and morbidity in a univariate analysis but was not independently associated with death.[3] Recent studies have had mixed results to indicate mortality attrib-utable of Acinetobacter. Some authors reported increased mortality rates secondary to Acinetobacter[19] while others in-cluding ours found not.[20] A. baumannii isolates common with relatively higher MDR rates may be due to habits of frequent prescribing or using wide spectrum antimicrobials in our country. Besides, some clinical characteristics of A. bauman-nii isolates, such as its presence in normal skin flora, easier transmissibility and viability in hospital environment due to being multi-drug resistant, may lead to increased incidences of NIs.
Older age, higher TBSA percentage, and albumin level were
Atilla et al. Mortality risk factors in burn care units considering the clinical significance of acinetobacter infections
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 37

found significant risk factors for mortality. Besides, A. bau-mannii was not found a risk factor for mortality in our study. However, due to higher rates of mortality occurring in in-fections by causative microorganisms capable of developing multidrug resistance like A. baumannii and P. aeruginosa, these microorganisms play an essential role when considering mor-tality in general.
Conflict of interest: None declared.
REFERENCES
1. Rafla K, Tredget EE. Infection control in the burn unit. Burns 2011;37:5-15.
2. Church D, Elsayed S, Reid O, Winston B, Lindsay R. Burn wound infec-tions. Clin Microbiol Rev 2006;19:403-34.
3. Albrecht MC, Griffith ME, Murray CK, Chung KK, Horvath EE, Ward JA, et al. Impact of Acinetobacter infection on the mortality of burn pa-tients. J Am Coll Surg 2006;203:546-50.
4. Towner KJ. Acinetobacter: an old friend, but a new enemy. J Hosp Infect 2009;73:355-63.
5. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance defini-tion of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 2008;36:309-32.
6. American College of Surgeons. Advanced trauma life support.6th ed. Chicago: American College of Surgeons; 1997.
7. Lund CC, Browder NC. The estimation of areas of burns. Surg Gynecol Obstet 1944;79:352-8.
8. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial disc susceptibility tests. CLSI Document M100-S12, 2002. CLSI, Wayne, PA.
9. Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, et al. Multidrug-resistant, extensively drug-resistant and pandrug-
resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 2012;18:268-81.
10. National Nosocomial Infections Surveillance System. National Nosoco-mial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Con-trol 2004;32:470-85.
11. Alp E, Coruh A, Gunay GK, Yontar Y, Doganay M. Risk factors for noso-comial infection and mortality in burn patients: 10 years of experience at a university hospital. J Burn Care Res 2012;33:379-85.
12. Zarei MR, Dianat S, Eslami V, Harirchi I, Boddouhi N, Zandieh A, et al. Factors associated with mortality in adult hospitalized burn patients in Tehran. Ulus Travma Acil Cerrahi Derg 2011;17:61-5.
13. Wang Y, Tang HT, Xia ZF, Zhu SH, Ma B, Wei W, et al. Factors affecting survival in adult patients with massive burns. Burns 2010;36:57-64.
14. Al B, Yildirim C, Coban S, Aldemir M, Güloğlu C. Mortality factors in flame and scalds burns: our experience in 816 patients. Ulus Travma Acil Cerrahi Derg 2009;15:599-606.
15. Brusselaers N, Monstrey S, Vogelaers D, Hoste E, Blot S. Severe burn injury in Europe: a systematic review of the incidence, etiology, morbidity, and mortality. Crit Care 2010;14:R188.
16. Chong SJ, Ahmed S, Tay JM, Song C, Tan TT. 5 year analysis of bacteri-ology culture in a tropical burns ICU. Burns 2011;37:1349-53.
17. Bayram Y, Parlak M, Aypak C, Bayram I. Three-year review of bacterio-logical profile and antibiogram of burn wound isolates in Van, Turkey. Int J Med Sci 2013;10:19-23.
18. Keen EF 3rd, Robinson BJ, Hospenthal DR, Aldous WK, Wolf SE, Chung KK, et al. Incidence and bacteriology of burn infections at a mili-tary burn center. Burns 2010;36:461-8.
19. Lortholary O, Fagon JY, Hoi AB, Slama MA, Pierre J, Giral P, et al. Noso-comial acquisition of multiresistant Acinetobacter baumannii: risk fac-tors and prognosis. Clin Infect Dis 1995;20:790-6.
20. Blot S, Vandewoude K, Colardyn F. Nosocomial bacteremia involving Acinetobacter baumannii in critically ill patients: a matched cohort study. Intensive Care Med 2003;29:471-5.
Atilla et al. Mortality risk factors in burn care units considering the clinical significance of acinetobacter infections
OLGU SUNUMU
Acinetobacter enfeksiyonlarının klinik önemi ışığındayanık ünitesinde mortalite için risk faktörleriDr. Aynur Atilla,1 Dr. Leman Tomak,2 Dr. Ali Osman Katrancı,3 Dr. Alper Ceylan,4 Dr. S. Sırrı Kılıç1
1SamsunEğitimveAraştırmaHastanesi,EnfeksiyonHastalıklarıveKlinikMikrobiyoloji,Samsun;2OndokuzMayısÜniversitesiTıpFakültesi,BiyoistatistikAnabilimDalı,Samsun;3SamsunEğitimveAraştırmaHastanesi,PediatrikCerrahiKliniği,Samsun;4SamsunEğitimveAraştırmaHastanesi,GenelCerrahiKliniği,Samsun
AMAÇ: Morbidite ve mortalite oranlarının yüksek olması nedeniyle yanıklardaki mortalitede risk faktörleri ve Acinetobacter izolatlarının buradaki rolünü değerlendirmeyi amaçladık.GEREÇ VE YÖNTEM: Ocak 2009’dan Mayıs 2011’e kadar yanık ünitemizde yatırılarak tedavi edilen toplam 465 hasta geriye dönük olarak gözden geçirildi. Risk belirlenmesinde lojistik regresyon analizi kullanıldı.BULGULAR: Mortalite oranları genelde %7.5, 17 yaş altı %3.9, 18-64 yaş arası %12 ve 65 yaş üzeri %24 idi (p<0.001). Total Vücut Yüzey Alanı (TBSA) %41’in üzerinde olan hastaların %64.3’ü (18 hasta) kaybedildi (p<0.001). TBSA%, ileri yaş ve albümin seviyeleri mortalitede risk faktörü olarak bulundu. En sık rastlanan bakteriyel izolat Acinetobacter baumanni idi.TARTIŞMA: Yanık oranları arttıkça mortalite oranlarının da arttığı görüldü. Yüksek mortalite oranlarına rağmen Acinetobacter enfeksiyonları morta-litede risk faktörü olarak bulunmadı.Anahtar sözcükler: Acinetobacter; enfeksiyon; mortalite; yanık.
Ulus Travma Acil Cerrahi Derg 2015;21(1):34-38 doi: 10.5505/tjtes.2015.76814
KLİNİK ÇALIŞMA - ÖZET
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 138

Evaluation of serum L-FABP levels in patientswith acute pancreatitisErdem Koçak, M.D.,1 Erdem Akbal, M.D.,2 Seyfettin Köklü, M.D.,3 Gürhan Adam, M.D.4
1DepartmentofGastroenterology,ÇanakkaleStateHospital,Çanakkale;2DepartmentofGastroenterology,ÇanakkaleOnsekizmartUniversityFacultyofMedicine,Çanakkale;3DepartmentofGastroenterology,HacettepeUniversityFacultyofMedicine,Ankara;4DepartmentofRadiology,ÇanakkaleOnsekizmartUniversityFacultyofMedicine,Çanakkale
ABSTRACT
BACKGROUND: The aim of this study was to assess the serum L-FABP levels in patients with acute pancreatitis and compare with healthy subjects.
METHODS: Thirty patients with acute pancreatitis and thirty consecutive healthy age- and sex-matched control subjects were in-cluded into the study. The serum levels of L-FABP were measured upon admission and at the remission period.
RESULTS: Upon admission, serum L-FABP concentration was significantly higher in patients with acute pancreatitis compared to control subjects (41009.41±32401.31 pg/ml vs. 17057.00±5015.74 pg/ml, p=0.008). Serum L-FABP levels decreased after the remission period; however, the differences were not statistically significant. In addition, serum L-FABP levels showed significant correlation with AST and LDH levels.
CONCLUSION: Increased serum L-FABP levels may be related to the mechanism of pancreatic microcirculatory disturbance in patients with acute pancreatitis, suggesting that serum L-FABP could be used for a potential biomarker of acute pancreatitis.
Key words: Acute pancreatitis; diagnosis; serum L-FABP.
lecular weight (14-15 k dal) proteins involved in the intra-cellular transport of long chain bioactive fatty acids.[4] Being abundantly low molecular cytoplasmic proteins with tissue specific expression profiles, FABPs serve as markers of tissue injury. Various FABPs have been tested to detect the early damage of tissues with a clinical utility in view. If damage pro-cess continues, FABP is detectable in serum.[5-7]
In the course of acute pancreatitis development, oxygen-free radicals and their derivatives play an important role as the molecular trigger in constituting lesions in the pancreas. Damaged acinar cells as well as activated neutrophils and macrophages produce large amounts of oxygen radicals in acute pancreatitis. Hydrogen peroxide, superoxide, hydroxyl radical, and singlet oxygen are key elements capable of cel-lular injury in acute pancreatitis. These highly reactive species cause various reactions, such as destruction of lipid mem-branes by peroxidation of fatty acids and destruction of lyso-somal membranes.[8] Liver fatty acid-binding protein (L-FABP) binds selectively to intracellular free unsaturated fatty acids and lipid peroxidation products during hypoxic tissue injury. Therefore, L-FABP may modulate inflammatory responses in acute pancreatitis. However, the involvement of L-FABP in acute pancreatitis is not known yet.
O R I G I N A L A R T I C L E
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 39
Address for correspondence: Erdem Koçak, M.D.
Çanakkale Devlet Hastanesi, Endoskopi Ünitesi, Çanakkale, Turkey
Tel: +90 286 - 217 33 13 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):39-43doi: 10.5505/tjtes.2015.49879
Copyright 2015TJTES
INTRODUCTION
Acute pancreatitis is an inflammatory disease associated with auto digestion of the pancreas due to intra-pancreatic acti-vation and the release of digestive enzymes. Most patients suffer from mild disease but in about 20% of the cases, the patient develops a severe form of the disease with a mortality of 7-15%. A number of biochemical markers have been used in the diagnosis of acute pancreatitis.[1-3] Several of these mark-ers have been documented to be present at increased con-centrations in the plasma of patients with acute pancreatitis.
Fatty acid binding proteins (FABPs) are a group of low mo-
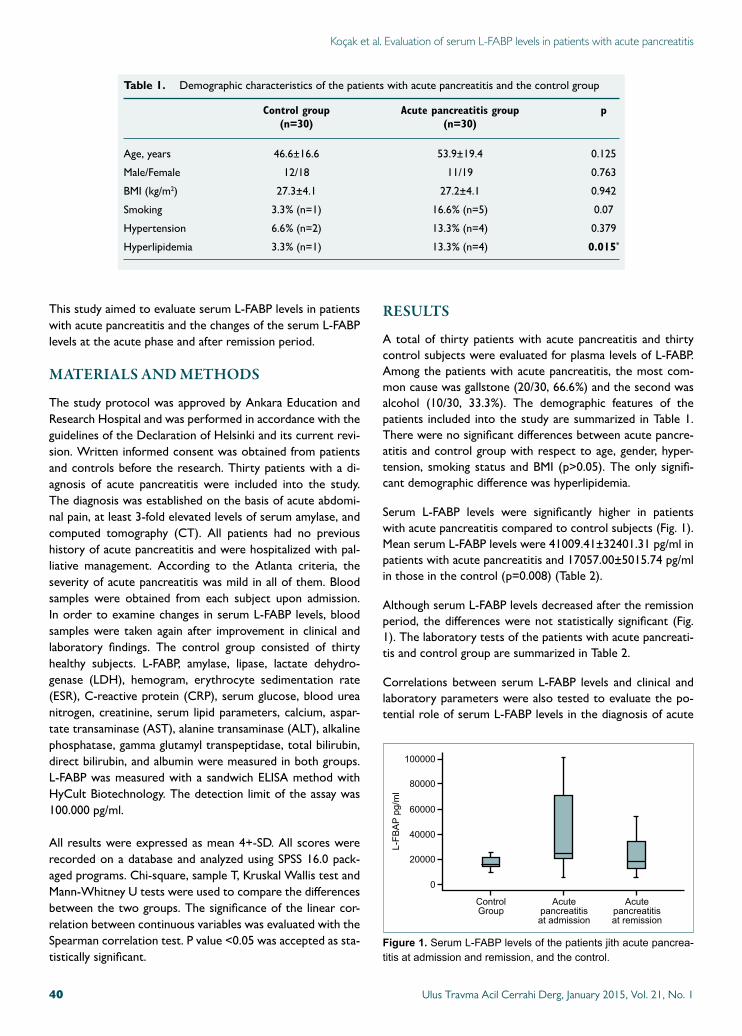
Koçak et al. Evaluation of serum L-FABP levels in patients with acute pancreatitis
This study aimed to evaluate serum L-FABP levels in patients with acute pancreatitis and the changes of the serum L-FABP levels at the acute phase and after remission period.
MATERIALS AND METHODS
The study protocol was approved by Ankara Education and Research Hospital and was performed in accordance with the guidelines of the Declaration of Helsinki and its current revi-sion. Written informed consent was obtained from patients and controls before the research. Thirty patients with a di-agnosis of acute pancreatitis were included into the study. The diagnosis was established on the basis of acute abdomi-nal pain, at least 3-fold elevated levels of serum amylase, and computed tomography (CT). All patients had no previous history of acute pancreatitis and were hospitalized with pal-liative management. According to the Atlanta criteria, the severity of acute pancreatitis was mild in all of them. Blood samples were obtained from each subject upon admission. In order to examine changes in serum L-FABP levels, blood samples were taken again after improvement in clinical and laboratory findings. The control group consisted of thirty healthy subjects. L-FABP, amylase, lipase, lactate dehydro-genase (LDH), hemogram, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), serum glucose, blood urea nitrogen, creatinine, serum lipid parameters, calcium, aspar-tate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase, gamma glutamyl transpeptidase, total bilirubin, direct bilirubin, and albumin were measured in both groups. L-FABP was measured with a sandwich ELISA method with HyCult Biotechnology. The detection limit of the assay was 100.000 pg/ml.
All results were expressed as mean 4+-SD. All scores were recorded on a database and analyzed using SPSS 16.0 pack-aged programs. Chi-square, sample T, Kruskal Wallis test and Mann-Whitney U tests were used to compare the differences between the two groups. The significance of the linear cor-relation between continuous variables was evaluated with the Spearman correlation test. P value <0.05 was accepted as sta-tistically significant.
RESULTS
A total of thirty patients with acute pancreatitis and thirty control subjects were evaluated for plasma levels of L-FABP. Among the patients with acute pancreatitis, the most com-mon cause was gallstone (20/30, 66.6%) and the second was alcohol (10/30, 33.3%). The demographic features of the patients included into the study are summarized in Table 1. There were no significant differences between acute pancre-atitis and control group with respect to age, gender, hyper-tension, smoking status and BMI (p>0.05). The only signifi-cant demographic difference was hyperlipidemia.
Serum L-FABP levels were significantly higher in patients with acute pancreatitis compared to control subjects (Fig. 1). Mean serum L-FABP levels were 41009.41±32401.31 pg/ml in patients with acute pancreatitis and 17057.00±5015.74 pg/ml in those in the control (p=0.008) (Table 2).
Although serum L-FABP levels decreased after the remission period, the differences were not statistically significant (Fig. 1). The laboratory tests of the patients with acute pancreati-tis and control group are summarized in Table 2.
Correlations between serum L-FABP levels and clinical and laboratory parameters were also tested to evaluate the po-tential role of serum L-FABP levels in the diagnosis of acute
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 140
Table 1. Demographic characteristics of the patients with acute pancreatitis and the control group
Control group Acute pancreatitis group p (n=30) (n=30)
Age, years 46.6±16.6 53.9±19.4 0.125
Male/Female 12/18 11/19 0.763
BMI (kg/m2) 27.3±4.1 27.2±4.1 0.942
Smoking 3.3% (n=1) 16.6% (n=5) 0.07
Hypertension 6.6% (n=2) 13.3% (n=4) 0.379
Hyperlipidemia 3.3% (n=1) 13.3% (n=4) 0.015*
Figure 1. SerumL-FABPlevelsofthepatientsjithacutepancrea-titisatadmissionandremission,andthecontrol.
100000
80000
60000
40000
20000
ControlGroup
Acutepancreatitisatadmission
Acutepancreatitisatremission
L-FB
APpg/ml
0
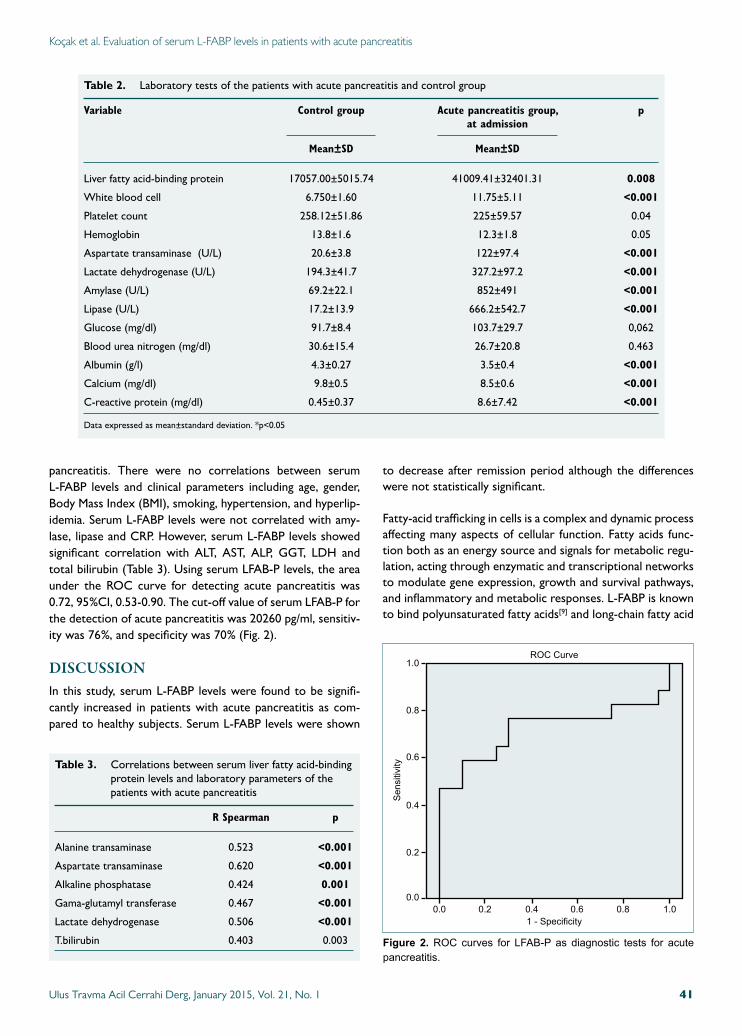
Koçak et al. Evaluation of serum L-FABP levels in patients with acute pancreatitis
pancreatitis. There were no correlations between serum L-FABP levels and clinical parameters including age, gender, Body Mass Index (BMI), smoking, hypertension, and hyperlip-idemia. Serum L-FABP levels were not correlated with amy-lase, lipase and CRP. However, serum L-FABP levels showed significant correlation with ALT, AST, ALP, GGT, LDH and total bilirubin (Table 3). Using serum LFAB-P levels, the area under the ROC curve for detecting acute pancreatitis was 0.72, 95%CI, 0.53-0.90. The cut-off value of serum LFAB-P for the detection of acute pancreatitis was 20260 pg/ml, sensitiv-ity was 76%, and specificity was 70% (Fig. 2).
DISCUSSIONIn this study, serum L-FABP levels were found to be signifi-cantly increased in patients with acute pancreatitis as com-pared to healthy subjects. Serum L-FABP levels were shown
to decrease after remission period although the differences were not statistically significant.
Fatty-acid trafficking in cells is a complex and dynamic process affecting many aspects of cellular function. Fatty acids func-tion both as an energy source and signals for metabolic regu-lation, acting through enzymatic and transcriptional networks to modulate gene expression, growth and survival pathways, and inflammatory and metabolic responses. L-FABP is known to bind polyunsaturated fatty acids[9] and long-chain fatty acid
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 41
Table 2. Laboratory tests of the patients with acute pancreatitis and control group
Variable Control group Acute pancreatitis group, p at admission
Mean±SD Mean±SD
Liver fatty acid-binding protein 17057.00±5015.74 41009.41±32401.31 0.008
White blood cell 6.750±1.60 11.75±5.11 <0.001
Platelet count 258.12±51.86 225±59.57 0.04
Hemoglobin 13.8±1.6 12.3±1.8 0.05
Aspartate transaminase (U/L) 20.6±3.8 122±97.4 <0.001
Lactate dehydrogenase (U/L) 194.3±41.7 327.2±97.2 <0.001
Amylase (U/L) 69.2±22.1 852±491 <0.001
Lipase (U/L) 17.2±13.9 666.2±542.7 <0.001
Glucose (mg/dl) 91.7±8.4 103.7±29.7 0,062
Blood urea nitrogen (mg/dl) 30.6±15.4 26.7±20.8 0.463
Albumin (g/l) 4.3±0.27 3.5±0.4 <0.001
Calcium (mg/dl) 9.8±0.5 8.5±0.6 <0.001
C-reactive protein (mg/dl) 0.45±0.37 8.6±7.42 <0.001
Data expressed as mean±standard deviation. *p<0.05
Table 3. Correlations between serum liver fatty acid-binding protein levels and laboratory parameters of the patients with acute pancreatitis
R Spearman p
Alanine transaminase 0.523 <0.001
Aspartate transaminase 0.620 <0.001
Alkaline phosphatase 0.424 0.001
Gama-glutamyl transferase 0.467 <0.001
Lactate dehydrogenase 0.506 <0.001
T.bilirubin 0.403 0.003 Figure 2. ROC curves for LFAB-P as diagnostic tests for acutepancreatitis.
1.0
0.8
0.6
0.4
0.2
0.0 0.2 0.4 0.6 0.8 1.00.0
Sensitivity
1-Specificity
ROC Curve

peroxidation products.[10] Sztefko et al. have suggested that high serum free fatty acid concentration may be involved in the development of complications in acute pancreatitis.[11] By binding polyunsaturated fatty acids, L-FABP modulates the availability of these fatty acids to intracellular oxidative path-ways. In addition to these well-known functions, recent stud-ies have shown that L-FABP plays a protective role in kidney injury.[12,13] From a theoretical point, it was suggested that high levels of L-FABP could protect against oxidative stress and inflammation in the pancreatic tissue.
CRP is one of the acute phase reactants made by the liver in response to the release of interleukin-1 and interleukin-6. Most authors have put forward that CRP is a valuable marker in the early assessment of the severity of acute pancreatitis.[14] Other mutiple serum markers have been studied so as to predict the severity of pancreatitis including urinary tryp-sinogen activation peptide, procalcitonin, polymorphonuclear elastase, pancreatic-associated protein, amylase and lipase, serum glucose, serum creatinine and calcium, procarboxy-peptidase-B, carboxypeptidase B activation peptide, serum trypsinogen-2, phospholipase A-2, serum amyloid protein-A, substance P, antithrombin III, platelet activating factor, inter-leukins 1, 6, and 8, tumor necrosis factor-alpha or soluble tumor necrosis factor receptor, and various genetic polymor-phisms.[15,16] L-FABP is predominantly found in the liver and thought to be involved in the regulation of lipid transport and metabolism. Research has shown L-FABP levels to rise significantly after cell damage.[17] Similarly, in this study, sig-nificantly high serum L-FABP levels were found in patients with acute pancreatitis compared with the controls. Further-more, serum L-FABP levels were shown to decrease after the remission period. However, the differences between L-FABP levels in acute attack and after remission did not reach statistical significance. In our study, the serum L-FABP levels were evaluated in the early period of remission and this re-sult can be explained by this methodological limitation. On the other hand, serum L-FABP level was not correlated with amylase, lipase and CRP levels, while it was significantly cor-related with liver damage enzymes including ALT, AST, ALP, GGT, LDH and total bilirubin. Regarding these results, serum L-FABP was suggested a useful marker especially in patients with acute biliary and alcoholic pancreatitis independent of serum biomarkers of acute pancreatitis.
L-FABP may be a useful serum marker for the diagnosis of acute pancreatitis. This is the first study showing that patients with acute pancreatitis have higher serum L-FABP levels than healthy subjects. However, further clinical and experimental studies are needed to evaluate diagnostic and prognostic val-ue of serum L-FABP levels in acute pancreatitis.
Conflict of interest: None declared.
REFERENCES
1. Puolakkainen P, Valtonen V, Paananen A, Schröder T. C-reactive protein (CRP) and serum phospholipase A2 in the assessment of the severity of acute pancreatitis. Gut 1987;28:764-71.
2. Domínguez-Muñoz JE, Carballo F, García MJ, de Diego JM, Rábago L, Simón MA, et al. Clinical usefulness of polymorphonuclear elastase in predicting the severity of acute pancreatitis: results of a multicentre study. Br J Surg 1991;78:1230-4.
3. Gudgeon AM, Heath DI, Hurley P, Jehanli A, Patel G, Wilson C, et al. Trypsinogen activation peptides assay in the early prediction of severity of acute pancreatitis. Lancet 1990;335:4-8.
4. Glatz JF, van der Vusse GJ. Cellular fatty acid-binding proteins: their function and physiological significance. Prog Lipid Res 1996;35:243-82.
5. Akbal E, Özbek M, Güneş F, Akyürek Ö, Üreten K, Delibaşı T. Serum heart type fatty acid binding protein levels in metabolic syndrome. Endo-crine 2009;36:433-7.
6. Oktay B, Akbal E, Firat H, Ardic S, Akdemir R, Kizilgun M. Evaluation of the relationship between heart type fatty acid binding protein levels and the risk of cardiac damage in patients with obstructive sleep apnea syndrome. Sleep Breath 2008;12:223-8.
7. Negishi K, Noiri E, Doi K, Maeda-Mamiya R, Sugaya T, Portilla D, et al. Monitoring of urinary L-type fatty acid-binding protein predicts histo-logical severity of acute kidney injury. Am J Pathol 2009;174:1154-9.
8. Yavuz N, Unal E, Memisoglu K, Krand O, Kiziler AR, Aydemir B, et al. Plasma leptin levels in rats with pancreatitis. Tohoku J Exp Med 2004;204:243-8.
9. Ek BA, Cistola DP, Hamilton JA, Kaduce TL, Spector AA. Fatty acid binding proteins reduce 15-lipoxygenase-induced oxygenation of linoleic acid and arachidonic acid. Biochim Biophys Acta 1997;1346:75-85.
10. Raza H, Pongubala JR, Sorof S. Specific high affinity binding of lipoxy-genase metabolites of arachidonic acid by liver fatty acid binding protein. Biochem Biophys Res Commun 1989;161:448-55.
11. Sztefko K, Panek J. Serum free fatty acid concentration in patients with acute pancreatitis. Pancreatology 2001;1:230-6.
12. Kanaguchi Y, Suzuki Y, Osaki K, Sugaya T, Horikoshi S, Tomino Y. Pro-tective effects of L-type fatty acid-binding protein (L-FABP) in proximal tubular cells against glomerular injury in anti-GBM antibody-mediated glomerulonephritis. Nephrol Dial Transplant 2011;26:3465-73.
13. Matsui K, Kamijo-Ikemorif A, Sugaya T, Yasuda T, Kimura K. Renal liver-type fatty acid binding protein (L-FABP) attenuates acute kidney injury in aristolochic acid nephrotoxicity. Am J Pathol 2011;178:1021-32.
14. Pongprasobchai S, Jianjaroonwong V, Charatcharoenwitthaya P, Komol-tri C, Tanwandee T, Leelakusolvong S, et al. Erythrocyte sedimentation rate and C-reactive protein for the prediction of severity of acute pancre-atitis. Pancreas 2010;39:1226-30.
15. Papachristou GI, Whitcomb DC. Predictors of severity and necrosis in acute pancreatitis. Gastroenterol Clin North Am 2004;33:871-90.
16. Blum T, Maisonneuve P, Lowenfels AB, Lankisch PG. Fatal outcome in acute pancreatitis: its occurrence and early prediction. Pancreatology 2001;1:237-41.
17. Pelsers MM, Hermens WT, Glatz JF. Fatty acid-binding proteins as plasma markers of tissue injury. Clin Chim Acta 2005;352:15-35.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 142
Koçak et al. Evaluation of serum L-FABP levels in patients with acute pancreatitis

Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 43
Koçak et al. Evaluation of serum L-FABP levels in patients with acute pancreatitis
OLGU SUNUMU
Akut pankreatitli hastalarda serum L-FABP düzeylerinin değerlendirilmesiDr. Erdem Koçak,1 Dr. Erdem Akbal,2 Dr. Seyfettin Köklü,3 Dr. Gürhan Adam4
1ÇanakkaleDevletHastanesi,GastroenterolojiKliniği,Çanakkale;2ÇanakkaleOnsekizMartÜniversitesiTıpFakültesi,GastroenterolojiKliniği,Çanakkale;3HacettepeÜniversitesiTıpFakültesi,GastroenterolojiKliniği,Ankara;4ÇanakkaleOnsekizMartÜniversitesiTıpFakültesi,RadyolojiKliniği,Çanakkale
AMAÇ: Bu çalışmanın amacı akut pankreatitli hastalarda serum L-FABP düzeylerini değerlendirmek ve sağlıklı olgular ile karşılaştırmak.GEREÇ VE YÖNTEM: Çalışmaya akut pankreatit tanısı konulan 30 hasta ve yaş ve cinsiyeti benzer 30 sağlıklı olgu alındı. Serum L-FABP düzeyleri başvuru anında ve iyileşme döneminde değerlendirildi.BULGULAR: Akut pankreatitli hastaların başvuru anında serum L-FABP düzeyleri kontrol grubundan belirgin olarak yüksekti (41009.41±32401.31 pg/ml ve 17057.00±5015.74 pg/ml, p=0.008). Serum L-FABP düzeyleri iyileşme periyodunda başvuru düzeylerine göre düşmekle birlikte aradaki fark istatistiksel olarak anlamlı değildi. Bununla birlikte akut pankreatitli hastalarda serum L-FABP düzeyleri AST ve LDH düzeyleri ile korele idi.TARTIŞMA: Akut pankreatitli hastalarda yüksek L-FABP düzeyleri pankreatik mikrosirkulatuar bozukluk ile ilişkili olabilir. Bu sonuçlar serum LFABP düzeylerinin akut pankreatitte kullanılabilecek bir biyomarker olduğunu destekler niteliktedir.Anahtar sözcükler: Akut pankreatit; serum L-FABP; tanı.
Ulus Travma Acil Cerrahi Derg 2015;21(1):39-43 doi: 10.5505/tjtes.2015.49879
KLİNİK ÇALIŞMA - ÖZET

Factors affecting postoperative mortality in patients older than 65 years undergoing surgery for hip fractureÖzgür Karaman, M.D.,1 Gökhan Özkazanlı, M.D.,1 Mehmet Müfit Orak, M.D.,1 Serhat Mutlu, M.D.,2
Harun Mutlu, M.D.,3 Gürkan Çalışkan, M.D.,2 Özgün Karakuş, M.D.,1 Baransel Saygı, M.D.1
1DepartmentofOrthopedicsTraumatology,FatihSultanMehmetTrainingandResearchHospital,İ̇stanbul;2DepartmentofOrthopedicsTraumatology,KanuniSultanSüleymanTrainingandResearchHospital,İstanbul;3DepartmentofOrthopedicsTraumatology,GaziosmanpaşaTaksimTrainingandResearchHospital,İstanbul
ABSTRACT
BACKGROUND: The aim of this study was to determine the factors affecting postoperative mortality in patients older than 65 years of age undergoing surgery for hip fracture.
METHODS: A total of 308 patients (219 males and 89 females) were included into the study. Spinal-epidural anaesthesia was ad-ministered in 203 patients and general anaesthesia in 105 patients. In the evaluation of the patients regarding ASA, two groups were determined ASA 1-2 and ASA 3-4. Systemic diseases present in the patients were determined preoperatively.
RESULTS: Seventy-seven (25%) of the total 308 patients died. In addition, patients with preoperative cardiac disease, patients on whom general anaesthesia was administered, patients in the ASA 3-4 group, and age were found to be significantly higher in mortality. When logistic regression analysis was performed for these four efficient factors, age, general anaesthesia, presence of cardiac disease were effective in mortality. However, ASA score changed depending on the age and cardiac disease.
CONCLUSION: In case of presence of multiple risk factors, it is necessary to determine which factor is, in fact, more effective. Age, ASA score, type of anaesthesia, and presence of cardiac disease are effective in mortality. However, ASA score affects mortality depending on the cardiac disease and age.
Key words: Hip fracture; mortality; risk factors.
It was shown that the highest risk of mortality for hip frac-tures was in the first sixth month. 23.8% of the patients with hip fracture die within the first year.[7]
Method of choice for almost all patients with hip fractures is surgery. In regard to the literature, returning to optimal level of function after surgery has been associated with preopera-tive comorbidity rather than the type of surgery.[8]
The American Society of Anesthesiologists (ASA) classifica-tion system[9] is a useful risk assessment system for patients with hip fractures. Independently from ASA medical and sur-gical assessments used worldwide, general health status of the patient is assessed by an anesthesiologist.[9] ASA clas-sification system consists of five types including ASA type 1, normal healthy patient; ASA type 2, patient with mild systemic disease; ASA type 3, patient with severe systemic disease which is not incapacitating; ASA type 4, patient with incapacitating systemic disease which is a constant threat to life; and ASA type 5, moribund patient not expected to live twenty-four h. Hip fractures are classified according to ana-tomic location.
O R I G I N A L A R T I C L E
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 144
Address for correspondence: Özgür Karaman, M.D.
Barbaros Mahallesi, Kentplus Sitesi, B: 8 Blok, D: 26,
Ataşehir, İstanbul, Turkey
Tel: +90 216 - 578 30 00 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):44-50doi: 10.5505/tjtes.2015.02582
Copyright 2015TJTES
INTRODUCTION
Life expectancy has recently increased in the elderly popula-tion. Hip fractures seen in the geriatric population together with the decrease in bone mass have become a great health concern.[1]
Hip fractures in the elderly population are the second leading cause of hospitalization.[2,3] After hip fractures, mortality risk indicates an increase in the subsequent two-three years and especially in the first year.[4-6]

Although patients with intertrochanteric fractures are gener-ally found to have more risk for mortality according to col-lum fracture, there are also studies indicating that there is no significant difference between them.[10-12]
Considering anaesthesia methods independently from the type of surgery performed, it has been shown that epidural and spinal anesthesia reduce mortality compared to general anesthesia.[13]
The aim of this study was to determine the factors affecting mortality in patients with collum femoris fractures and inter-trochanteric fractures.
MATERIALS AND METHODS
This study was approved by the ethics committee with the protocol number of 2013-10. Patients with collum femoris fractures and intertrochanteric fractures treated surgically between January 2007 and January 2012 were included into the study. The preoperative criteria of this study were gen-der, type of fracture, age, comorbid factors, hospitalization duration, type of anesthesia and ASA assessments. Mortal-ity rates and type of treatment were evaluated postopera-tively.
Patients older than 65 years of age experiencing hip fracture following low-energy trauma and undergoing hemiarthroplas-ty or internal fixation were included into the study. Our ex-clusion criteria were multiple traumatic injuries, high-energy traumas and malignancies. Patient screening was performed retrospectively from hospital electronic medical record sys-tem. Types of fractures and surgeries performed were deter-mined investigating preoperative and postoperative X-rays of all patients. Internal fixation and hemiarthroplasty were per-formed for intertrochanteric fractures and hemiarthroplasty was performed for collum femoris fractures. Mean ages of the patients as 65-100 (Mean±SD 80.04±8.40), admission dates of all patients, time to surgery and types of treatments were recorded by the surgeon. Types of anesthesia (spinal/epidural), comorbidities and ASA scores of the patients were recorded.
Statistical EvaluationNCSS (Number Cruncher Statistical System) 2007&PASS (Power Analysis and Sample Size) 2008 Statistical Software (Utah, USA) program was used for statistical analysis. During the assessment of the study data, Student t test was used for the comparison of quantitative data in addition to descriptive statistical methods (Mean, Standard Deviation, Frequency, Rate). Yates Continuity Correction test (Yates Corrected Chi-Square) was used for the comparison of qualitative data. Kaplan-Meier Survival analysis and Log-Rank test was used for evaluations of survival. Significance was evaluated at the levels of p<0.01 and p<0.05.
RESULTS
A total of three hundred and eight patients meeting our study criteria comprised our study population. 28.9% of the pa-tients (n=89) were males and 71.1% (n=219) of them were fe-males. Demographic characteristics of the patients are shown in Table 1.
38.6% of the patients (n=119) were diagnosed with inter-trochanteric femur fracture and 61.4% of them (n=189) were diagnosed with collum femur fracture. 32.1% of the patients (n=99) underwent internal fixation and 67.92% (n=209) underwent hemiarthroplasty. While hemiarthro-plasty was performed in 16.8% (n=20) of the one hundred and nineteen patients with intertrochanteric femur fracture diagnosis, internal fixation was performed in 83.2% of them (n=99). Hemiarthroplasty was performed in all (100%) one hundred and eighty-nine patients with collum femur fracture diagnosis.
Time to surgery, total hospitalization duration, diagnosis, treatment, gender, type of anesthesia, ASA score, systemic diseases, and mortality rates of the patients are shown in Table 2. It was determined that advanced age increased the mortality rate significantly (p<0.01). Mortality rate was high-er in patients receiving general anesthesia (p<0.01). Mortality rates of the patients with ASA score 3-4 were significantly higher than the mortality rates of the patients with ASA score 1-2 (p<0.01). Mortality rates of the patients with car-diac disease were found to be higher than the mortality rates of the patients without cardiac disease (p<0.01).
Survival AnalysisWhen the patients were assessed according to diagnosis, it was determined that eighty-five (71.4%) of one hundred and nineteen patients with intertrochanteric fracture diagnosis survived and thirty-four of them died; one hundred and forty-six (77.2%) of one hundred and eighty-nine patients with col-lum fracture diagnosis survived and forty-three of them died. When the patients were assessed according to treatment, it was determined that one hundred and fifty-two (72.7%) of two hundred and nine patients who underwent hemiar-throplasty survived and fifty-seven of them died; seventy-nine (79.8%) of ninety-nine patients who underwent internal fixa-tion survived and twenty of them died.
When the patients were assessed according to ASA scor-ing (Fig. 1), it was determined that seventy-nine (85.9%) of ninety-two patients with ASA score 1-2 survived and thirteen of them died. It was determined that one hundred and fifty-two (70.4%) of two hundred and sixteen patients with ASA score 3-4 survived and sixty-four of them died. Mortalities of the patients with ASA score 3-4 were significantly higher than the mortalities of the patients with ASA score 1-2 (p=0.001). ODDS rate was determined 2.559 (95% CI: 1.33-4.93).
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 45
Karaman et al. Factors affecting postoperative mortality in patients older than 65 years undergoing surgery for hip fracture
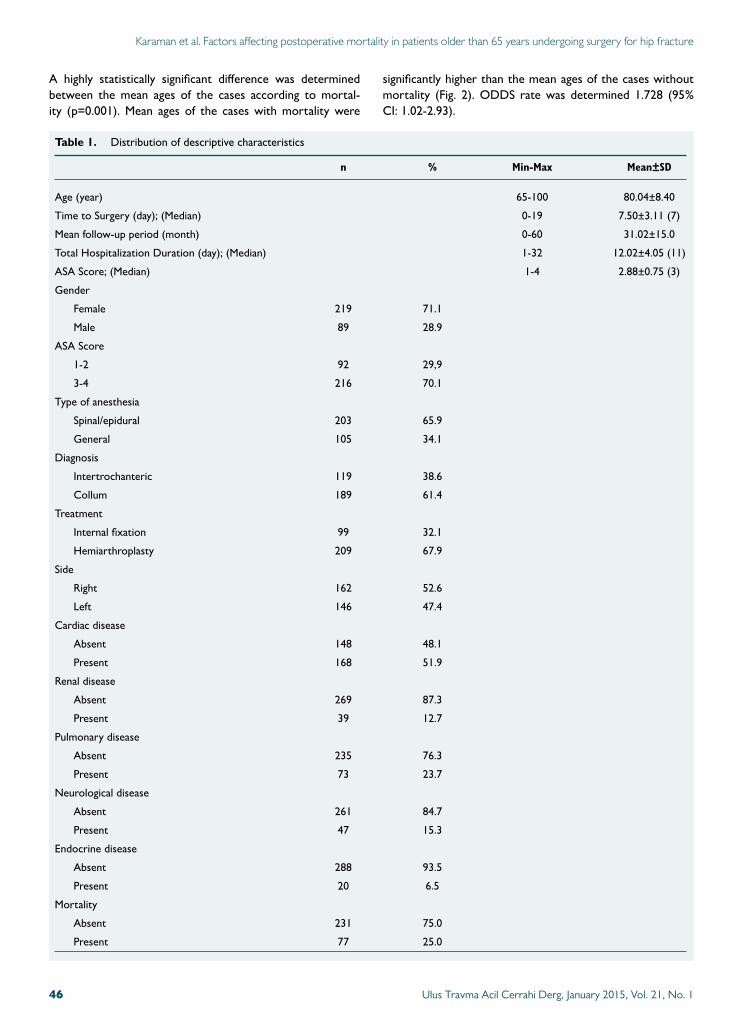
A highly statistically significant difference was determined between the mean ages of the cases according to mortal-ity (p=0.001). Mean ages of the cases with mortality were
significantly higher than the mean ages of the cases without mortality (Fig. 2). ODDS rate was determined 1.728 (95% CI: 1.02-2.93).
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 146
Table 1. Distribution of descriptive characteristics
n % Min-Max Mean±SD
Age (year) 65-100 80.04±8.40
Time to Surgery (day); (Median) 0-19 7.50±3.11 (7)
Mean follow-up period (month) 0-60 31.02±15.0
Total Hospitalization Duration (day); (Median) 1-32 12.02±4.05 (11)
ASA Score; (Median) 1-4 2.88±0.75 (3)
Gender
Female 219 71.1
Male 89 28.9
ASA Score
1-2 92 29,9
3-4 216 70.1
Type of anesthesia
Spinal/epidural 203 65.9
General 105 34.1
Diagnosis
Intertrochanteric 119 38.6
Collum 189 61.4
Treatment
Internal fixation 99 32.1
Hemiarthroplasty 209 67.9
Side
Right 162 52.6
Left 146 47.4
Cardiac disease
Absent 148 48.1
Present 168 51.9
Renal disease
Absent 269 87.3
Present 39 12.7
Pulmonary disease
Absent 235 76.3
Present 73 23.7
Neurological disease
Absent 261 84.7
Present 47 15.3
Endocrine disease
Absent 288 93.5
Present 20 6.5
Mortality
Absent 231 75.0
Present 77 25.0
Karaman et al. Factors affecting postoperative mortality in patients older than 65 years undergoing surgery for hip fracture
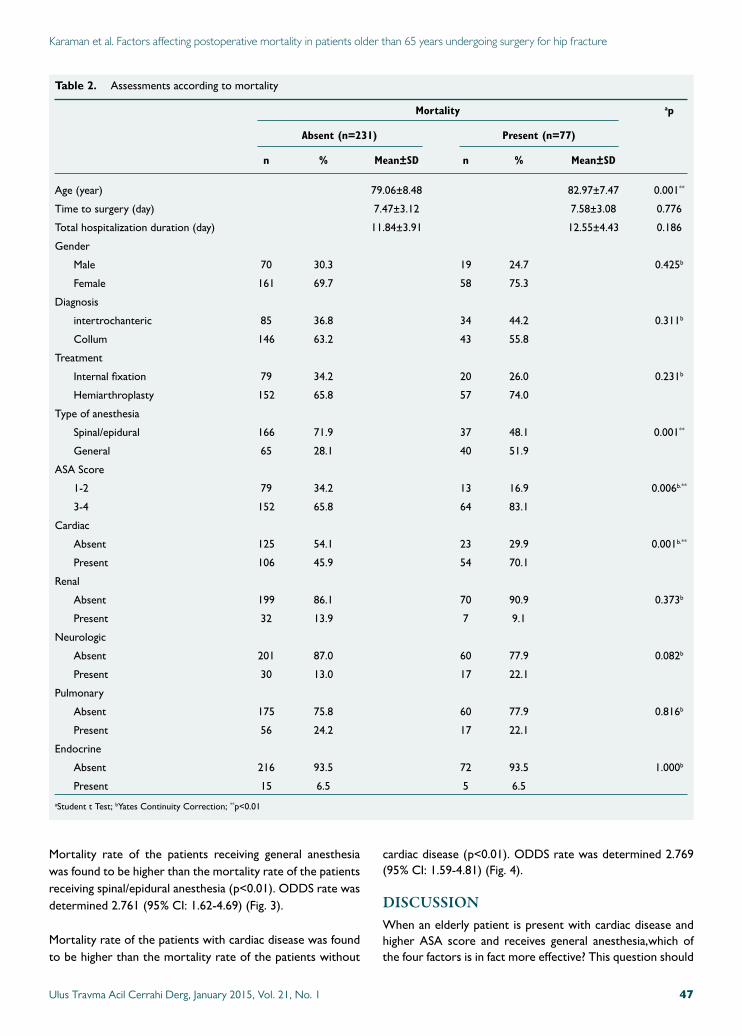
Mortality rate of the patients receiving general anesthesia was found to be higher than the mortality rate of the patients receiving spinal/epidural anesthesia (p<0.01). ODDS rate was determined 2.761 (95% CI: 1.62-4.69) (Fig. 3).
Mortality rate of the patients with cardiac disease was found to be higher than the mortality rate of the patients without
cardiac disease (p<0.01). ODDS rate was determined 2.769 (95% CI: 1.59-4.81) (Fig. 4).
DISCUSSIONWhen an elderly patient is present with cardiac disease and higher ASA score and receives general anesthesia,which of the four factors is in fact more effective? This question should
Table 2. Assessments according to mortality
Mortality ap
Absent (n=231) Present (n=77)
n % Mean±SD n % Mean±SD
Age (year) 79.06±8.48 82.97±7.47 0.001**
Time to surgery (day) 7.47±3.12 7.58±3.08 0.776
Total hospitalization duration (day) 11.84±3.91 12.55±4.43 0.186
Gender
Male 70 30.3 19 24.7 0.425b
Female 161 69.7 58 75.3
Diagnosis
intertrochanteric 85 36.8 34 44.2 0.311b
Collum 146 63.2 43 55.8
Treatment
Internal fixation 79 34.2 20 26.0 0.231b
Hemiarthroplasty 152 65.8 57 74.0
Type of anesthesia
Spinal/epidural 166 71.9 37 48.1 0.001**
General 65 28.1 40 51.9
ASA Score
1-2 79 34.2 13 16.9 0.006b.**
3-4 152 65.8 64 83.1
Cardiac
Absent 125 54.1 23 29.9 0.001b.**
Present 106 45.9 54 70.1
Renal
Absent 199 86.1 70 90.9 0.373b
Present 32 13.9 7 9.1
Neurologic
Absent 201 87.0 60 77.9 0.082b
Present 30 13.0 17 22.1
Pulmonary
Absent 175 75.8 60 77.9 0.816b
Present 56 24.2 17 22.1
Endocrine
Absent 216 93.5 72 93.5 1.000b
Present 15 6.5 5 6.5
aStudent t Test; bYates Continuity Correction; **p<0.01
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 47
Karaman et al. Factors affecting postoperative mortality in patients older than 65 years undergoing surgery for hip fracture
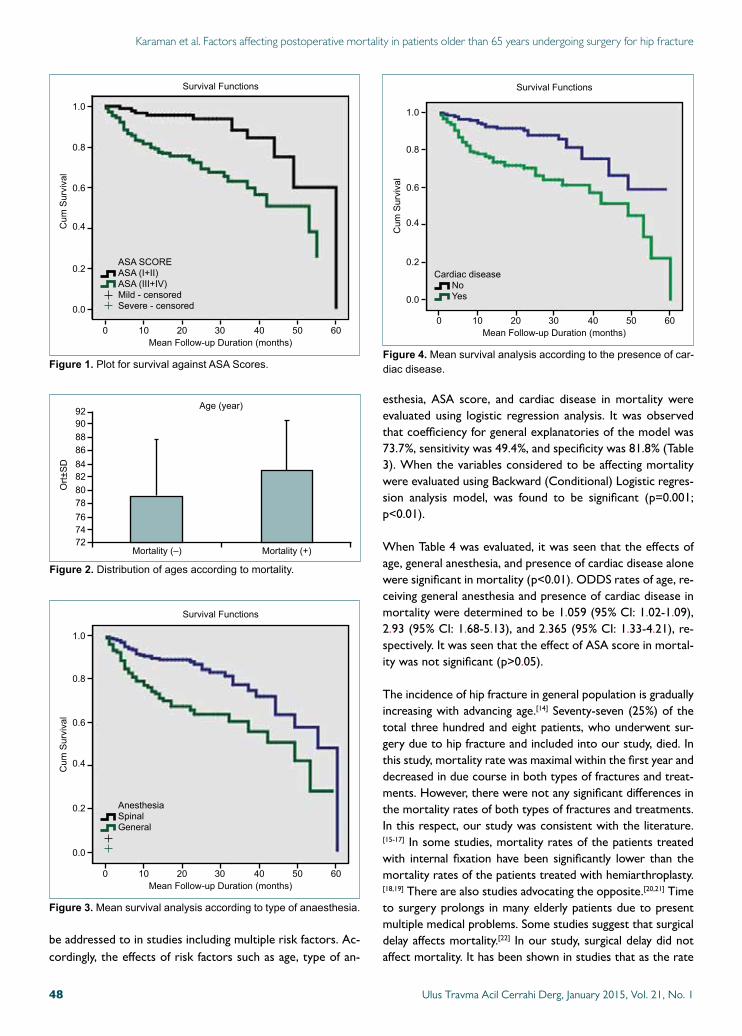
be addressed to in studies including multiple risk factors. Ac-cordingly, the effects of risk factors such as age, type of an-
esthesia, ASA score, and cardiac disease in mortality were evaluated using logistic regression analysis. It was observed that coefficiency for general explanatories of the model was 73.7%, sensitivity was 49.4%, and specificity was 81.8% (Table 3). When the variables considered to be affecting mortality were evaluated using Backward (Conditional) Logistic regres-sion analysis model, was found to be significant (p=0.001; p<0.01).
When Table 4 was evaluated, it was seen that the effects of age, general anesthesia, and presence of cardiac disease alone were significant in mortality (p<0.01). ODDS rates of age, re-ceiving general anesthesia and presence of cardiac disease in mortality were determined to be 1.059 (95% CI: 1.02-1.09), 2.93 (95% CI: 1.68-5.13), and 2.365 (95% CI: 1.33-4.21), re-spectively. It was seen that the effect of ASA score in mortal-ity was not significant (p>0.05).
The incidence of hip fracture in general population is gradually increasing with advancing age.[14] Seventy-seven (25%) of the total three hundred and eight patients, who underwent sur-gery due to hip fracture and included into our study, died. In this study, mortality rate was maximal within the first year and decreased in due course in both types of fractures and treat-ments. However, there were not any significant differences in the mortality rates of both types of fractures and treatments. In this respect, our study was consistent with the literature.[15-17] In some studies, mortality rates of the patients treated with internal fixation have been significantly lower than the mortality rates of the patients treated with hemiarthroplasty.[18,19] There are also studies advocating the opposite.[20,21] Time to surgery prolongs in many elderly patients due to present multiple medical problems. Some studies suggest that surgical delay affects mortality.[22] In our study, surgical delay did not affect mortality. It has been shown in studies that as the rate
Figure 1. PlotforsurvivalagainstASAScores.
1.0
0.8
0.6
0.4
0.2
0 10 20 30 40 50 60
0.0
Cum
Survival
MeanFollow-upDuration(months)
SurvivalFunctions
ASASCOREASA(I+II)ASA(III+IV)Mild-censoredSevere-censored
Figure 3. Meansurvivalanalysisaccordingtotypeofanaesthesia.
1.0
0.8
0.6
0.4
0.2
0 10 20 30 40 50 60
0.0
Cum
Survival
MeanFollow-upDuration(months)
SurvivalFunctions
AnesthesiaSpinalGeneral
Figure 4. Meansurvivalanalysisaccordingtothepresenceofcar-diacdisease.
1.0
0.8
0.6
0.4
0.2
0 10 20 30 40 50 60
0.0
Cum
Survival
MeanFollow-upDuration(months)
SurvivalFunctions
Cardiac diseaseNoYes
Figure 2. Distributionofagesaccordingtomortality.
888684828078767472
9092
Ort±SD
Mortality(–) Mortality(+)
Age(year)
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 148
Karaman et al. Factors affecting postoperative mortality in patients older than 65 years undergoing surgery for hip fracture
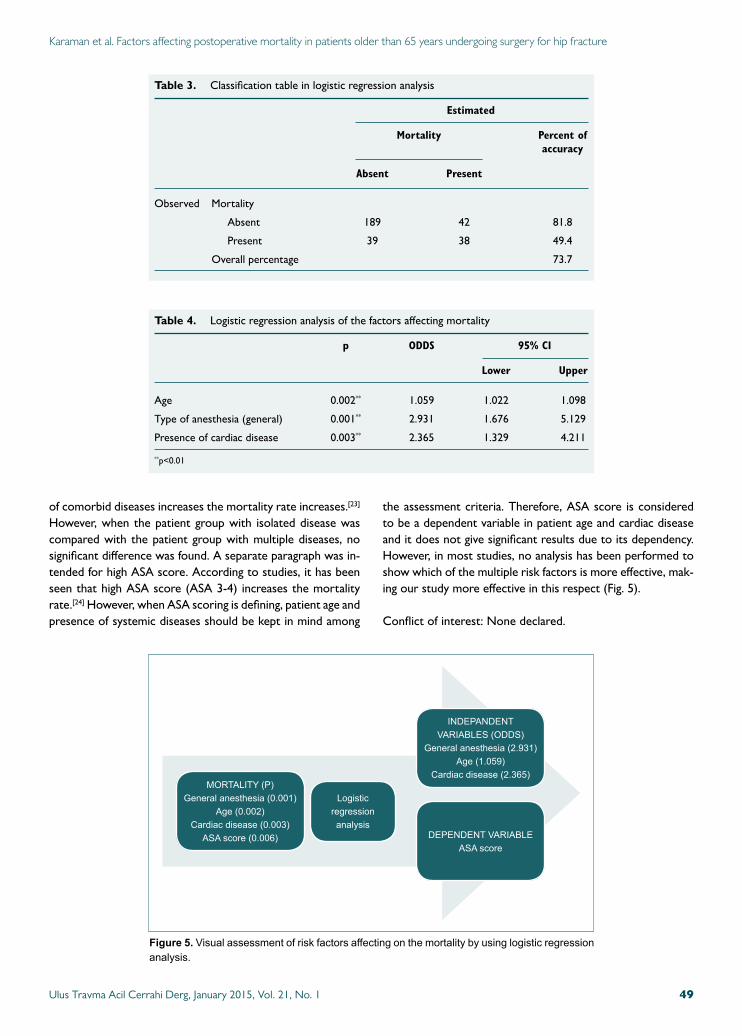
of comorbid diseases increases the mortality rate increases.[23] However, when the patient group with isolated disease was compared with the patient group with multiple diseases, no significant difference was found. A separate paragraph was in-tended for high ASA score. According to studies, it has been seen that high ASA score (ASA 3-4) increases the mortality rate.[24] However, when ASA scoring is defining, patient age and presence of systemic diseases should be kept in mind among
the assessment criteria. Therefore, ASA score is considered to be a dependent variable in patient age and cardiac disease and it does not give significant results due to its dependency. However, in most studies, no analysis has been performed to show which of the multiple risk factors is more effective, mak-ing our study more effective in this respect (Fig. 5).
Conflict of interest: None declared.
Karaman et al. Factors affecting postoperative mortality in patients older than 65 years undergoing surgery for hip fracture
MORTALITY(P)Generalanesthesia(0.001)
Age(0.002)Cardiacdisease(0.003)
ASAscore(0.006)
Logisticregressionanalysis
INDEPANDENTVARIABLES(ODDS)
Generalanesthesia(2.931)Age(1.059)
Cardiacdisease(2.365)
DEPENDENTVARIABLEASAscore
Figure 5. Visualassessmentofriskfactorsaffectingonthemortalitybyusinglogisticregressionanalysis.
Table 4. Logistic regression analysis of the factors affecting mortality
p ODDS 95% CI
Lower Upper
Age 0.002** 1.059 1.022 1.098
Type of anesthesia (general) 0.001** 2.931 1.676 5.129
Presence of cardiac disease 0.003** 2.365 1.329 4.211
**p<0.01
Table 3. Classification table in logistic regression analysis
Estimated
Mortality Percent of accuracy
Absent Present
Observed Mortality
Absent 189 42 81.8
Present 39 38 49.4
Overall percentage 73.7
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 49

REFERENCES
1. Cooper C, Campion G, Melton LJ 3rd. Hip fractures in the elderly: a world-wide projection. Osteoporos Int 1992;2:285-9.
2. Beaupre LA, Jones CA, Saunders LD, Johnston DW, Buckingham J, Ma-jumdar SR. Best practices for elderly hip fracture patients. A systematic overview of the evidence. J Gen Intern Med 2005;20:1019-25.
3. Wilkins K. Health care consequences of falls for seniors. Health Rep 1999;10:47-55.
4. Magaziner J, Lydick E, Hawkes W, Fox KM, Zimmerman SI, Epstein RS, et al. Excess mortality attributable to hip fracture in white women aged 70 years and older. Am J Public Health 1997;87:1630-6.
5. Schrøder HM, Erlandsen M. Age and sex as determinants of mortality after hip fracture: 3,895 patients followed for 2.5-18.5 years. J Orthop Trauma 1993;7:525-31.
6. Vestergaard P, Rejnmark L, Mosekilde L. Has mortality after a hip frac-ture increased? J Am Geriatr Soc 2007;55:1720-6.
7. Richmond J, Aharonoff GB, Zuckerman JD, Koval KJ. Mortality risk af-ter hip fracture. 2003. J Orthop Trauma 2003;17(8 Suppl):S2-5.
8. Donegan DJ, Gay AN, Baldwin K, Morales EE, Esterhai JL Jr, Mehta S. Use of medical comorbidities to predict complications after hip fracture surgery in the elderly. J Bone Joint Surg Am 2010;92:807-13.
9. Saklad M. Grading of patients for surgical procedures. Anesthesiology 1941;2:281-4.
10. Aharonoff GB, Koval KJ, Skovron ML, Zuckerman JD. Hip frac-tures in the elderly: predictors of one year mortality. J Orthop Trauma 1997;11:162-5.
11. Cipitria JA, Sosa MM, Pezzotto SM, Puche RC, Bocanera R. Outcome of hip fractures among elderly subjects. Medicina (B Aires) 1997;57:530-4.
12. Kenzora JE, McCarthy RE, Lowell JD, Sledge CB. Hip fracture mortal-ity. Relation to age, treatment, preoperative illness, time of surgery, and complications. Clin Orthop Relat Res 1984;186:45-56.
13. Rodgers A, Walker N, Schug S, McKee A, Kehlet H, van Zundert A, et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ 2000;321:1493.
14. Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J 1965;14:61-5.
15. Ozkaya U, Parmaksizoğlu AS, Gül M, Kabukçuoğlu Y, Ozkazanli G, Basilgan S. Management of osteoporotic pertrochanteric fractures with external fixation in elderly patients. Acta Orthop Traumatol Turc 2008;42:246-51.
16. Farahmand BY, Michaëlsson K, Ahlbom A, Ljunghall S, Baron JA; Swed-ish Hip Fracture Study Group. Survival after hip fracture. Osteoporos Int 2005;16:1583-90.
17. Vestergaard P, Rejnmark L, Mosekilde L. Has mortality after a hip frac-ture increased? J Am Geriatr Soc 2007;55:1720-6.
18. White BL, Fisher WD, Laurin CA. Rate of mortality for elderly pa-tients after fracture of the hip in the 1980’s. J Bone Joint Surg Am 1987;69:1335-40.
19. Parker MJ, Pryor GA. Internal fixation or arthroplasty for displaced cer-vical hip fractures in the elderly: a randomised controlled trial of 208 pa-tients. Acta Orthop Scand 2000;71:440-6.
20. Bhandari M, Devereaux PJ, Swiontkowski MF, Tornetta P 3rd, Obrem-skey W, Koval KJ, et al. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck. A meta-analysis. J Bone Joint Surg Am 2003;85-A:1673-81.
21. Keene GS, Parker MJ, Pryor GA. Mortality and morbidity after hip frac-tures. BMJ 1993;307:1248-50.
22. Kesmezacar H, Ayhan E, Unlu MC, Seker A, Karaca S. Predictors of mortality in elderly patients with an intertrochanteric or a femoral neck fracture. J Trauma 2010;68:153-8.
23. Zuckerman JD. Hip fracture. N Engl J Med 1996;334:1519-25.
24. Fleisher LA. Risk of anesthesia. In: Miller RD, editor. Miller’s anesthesia. Vol 1, 6th ed. USA: Elsevier; 2005. p. 893-925.
Karaman et al. Factors affecting postoperative mortality in patients older than 65 years undergoing surgery for hip fracture
OLGU SUNUMU
Kalça kırığı nedeni ile ameliyat edilen 65 yaş üstü hastalarda mortaliteye etki eden faktörlerDr. Özgür Karaman,1 Dr. Gökhan Özkazanlı,1 Dr. Mehmet Müfit Orak,1 Dr. Serhat Mutlu,2
Dr. Harun Mutlu,3 Dr. Gürkan Çalışkan,2 Dr. Özgün Karakuş,1 Dr. Baransel Saygı1
1FatihSultanMehmetEğitimveAraştırmaHastanesi,OrtopediveTravmatoljiKliniği,İstanbul;2KanuniSultanSüleymanEğitimveAraştırmaHastanesi,OrtopediveTravmatoljiKliniği,İ̇stanbul;3GaziosmanpaşaTaksimEğitimveAraştırmaHastanesi,OrtopediveTravmatoljiKliniği,İ̇stanbul
AMAÇ: Çalışmamızdaki amaç 65 yaş üstü kalça kırığı nedeni ile ameliyat olan kalça kırığına etki eden mortalite faktörlerinin belirlenmesi.GEREÇ VE YÖNTEM: Altmış beş yaş üstü 219 erkek, 89 kadın toplam 308 hasta dahil edildi. Anestezi tipi olarak 203 hastaya spinal/epidural ve 105 hastaya genel anestezi verildi. Hastaların ASA değerlendirilmesinde ASA 1-2 ve ASA 3-4 olarak iki grup belirlendi. Ameliyat öncesinde hastaların mevcut olan sistemik hastalıkları belirlendi.BULGULAR: Toplam 308 hastanın 77’si (%25) öldü. Ayrıca ameliyat öncesinde olarak kardiyak hastalığı olan hastalar, genel anestezi yapılan hastalar, ASA3-4 grubu olan hastalar ve yaş mortalite için anlamlı yüksek bulundu. Bu dört etkili faktöre lojistik regresyon analizi yapıldığında ise yaş, genel anestezi, kardiyak hastalığın varlığı mortalite üzerinde etkilidir. Ancak ASA skoru yaşa ve kardiyak hastalığa bağımlı olarak değişmektedir.TARTIŞMA: Çoklu risk faktörlerinin bulunduğu durumlarda hangi faktörün gerçekte daha etkili olduğunu hesaplamak gerekli. Yaş, ASA skoru, anastezi şekli ve kardiyak hastalık varlığı mortaliteyi etkilemektedir. Ancak ASA skoru kardiyak hastalık ve yaş faktörüne bağımlı olarak mortaliteyi etkilemektedir.Anahtar sözcükler: Kalça kırığı; mortalite; risk faktörü.
Ulus Travma Acil Cerrahi Derg 2015;21(1):44-50 doi: 10.5505/tjtes.2015.02582
KLİNİK ÇALIŞMA - ÖZET
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 150
Evaluation of power Doppler sonography in acutecholecystitis to predict intraoperative findings:a prospective clinical study
phy’s sign has 95.2% sensitivity for the diagnosis of acute cho-lecystitis.[3] In acute cholecystitis, GB wall thickness is caused by increased vascularity of the GB wall but in chronic chole-cystitis it is caused by fibrosis.[4] On the other hand, a number of conditions can cause GB wall thickness, such as pancreati-tis, hepatitis, cirrhosis, and congestive heart failure. In order to increase the specificity of the diagnosis, determining the vascularity of the GB wall with Doppler sonography showed valuable diagnostic benefits in previous reports and diagnos-tic superiority was obtained especially with power Doppler sonography.[4,5] Despite higher diagnostic capability of power Doppler sonography for the discrimination of acute cholecys-titis from the chronic form, the real challenge is to determine the association between sonographic findings and predicting the difficulty of dissection and to help physician to make a clear decision for performing or not performing an emergent operation. So as to evaluate the diagnostic and prognostic value of gray-scale and power Doppler sonography for acute cholecystitis, it was our aim to show a correlation between
O R I G I N A L A R T I C L E
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 51
Süleyman Çetinkünar, M.D.,1 Hasan Erdem, M.D.,1 Recep Aktimur, M.D.,3 Gokhan Soker, M.D.,2
Hilmi Bozkurt, M.D.,1 Enver Reyhan, M.D.,1 Selim Sozen, M.D.,1 Oktay İrkorucu, M.D.,1
1DepartmentofGeneralSurgery,AdanaNumuneTrainingandResearchHospital,Adana;2DepartmentofRadiology,AdanaNumuneTrainingandResearchHospital,Adana;3DepartmentofGeneralSurgery,SamsunTrainingandResearchHospital,Adana
ABSTRACT
BACKGROUND: This study aimed to evaluate the diagnostic value of gray-scale and power Doppler sonography for acute cholecys-titis and show a correlation between sonographic and intraoperative findings, quantitively.
METHODS: Forty chronic and forty acute cholecystitis patients were examined. Early laparoscopic cholecystectomy was performed for acute cholecystitis. Demographic characteristics, sonographic findings, and adhesion scores were analyzed. Data were collected prospectively (clinicaltrials.gov: NCT02156947).
RESULTS: Wall thickness (≥3 mm) and vascularity increased in acute cholecystitis (p<0.01 and <0.01). Vascularity was found to be moderately correlated with adhesion (p<0.01, r=0.59) but it did not affect the difficulty of the operation by means of perforation, conversion rate, and operation time. In addition, wall thickness did not correlate with adhesion formation (p=0.36). Sensitivity and specifity of wall thickness and vascularity were found to be 96.9%, 72.7%, and 68%, 87.2%, respectively. When both diagnostic mea-surements were taken into account, sensitivity was calculated 69.7% and specificity reached up to 97.6%.
CONCLUSION: Vascularity correlated with adhesion but failed to predict operation difficulty. Specificity of gray-scale sonography could be improved with power Doppler examination; however, desired diagnostic accuracy could not be obtained with only quantitive measurements of sonography.
Key words: Acute; cholecystitis; chronic; power Doppler; vascularity.
Address for correspondence: Recep Aktimur, M.D.
Samsun Eğitim ve Araştırma Hastanesi, Genel Cerrahi Kliniği,
55200 Samsun, Turkey
Tel: +90 362 - 311 15 00 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):51-56doi: 10.5505/tjtes.2015.64505
Copyright 2015TJTES
INTRODUCTION
For a long time, gray-scale sonography has generally been considered first-line diagnostic tool for patients with suspect-ed gallbladder (GB) diseases.[1] Moreover, it has been proven to be a valuable imaging technique in differential diagnosis for acute or chronic cholecystitis.[2] In the presence of gallstones, sonographic findings such as GB wall thickening and the Mur-

Çetinkünar et al. Evaluation of power Doppler sonography in acute cholecystitis to predict intraoperative findings: a prospective clinical study
quantitive sonographic findings and intraoperative adhesion scale and compare it with the chronic cholecystitis as a con-trol group.
MATERIALS AND METHODS
A total of eighty cholecystitis patients (40 symptomatic chronic, 40 acute) treated in our tertiary care center between January 2012 and July 2013 constituted the study groups. An informed consent was taken from all patients before they were included into the study. The protocol of this prospec-tive clinical study was approved by the local Institutional Review Board (4/16.01.2012). Data were collected prospec-tively (clinicaltrials.gov registration ID: NCT02156947). The occurrence of clinical signs in the first 72-96 hours after the onset of symptoms was termed as acute cholecystitis. The diagnosis of acute cholecystitis was made on clinical, sono-graphic and laboratory findings. Acute right upper quadrant abdominal pain with positive Murphy’s sign, fever, leukocy-tosis were considered clinically; distended GB, presence of gallstones or sludge, GB wall thickness of 3-mm or more, and sonographic Murphy’s sign were considered sonographically significant. If a patient was diagnosed with acute cholecystitis, he or she was informed about early laparoscopic cholecystec-tomy (LC) and if LC was accepted, the patient was included into the study and operated in the first 24 hours following the diagnosis. Detected choledocholithiasis and patients <18 years of age were excluded. No age limit was specified. Age and sex were recorded.
All patients were examined by a single radiologist with Min-dray DC-7 ultrasonography device and a 3.5 MHz abdomi-nal transducer, following a fasting period of a minimum of 6 hours. Gray-scale abdominal US examination was followed by power Doppler examinations in which quantitative measure-ments were made according to previous report of Uggowit-zer et al.[5] Vascularity was 0 if there was no vessel within the GB wall; vascularity was + when no more than two signals per centimeter were detected within the wall; vascularity was ++ when there were multiple scattered signals; and continuously depicted vessels for a length of at least 25 mm were assigned a vascularity +++. In addition, sonographic GB wall thickness and free fluid on the GB fossa were recorded.
All operations were performed by the senior staff of our clinic. The technique used for LC was the conventional four-trocar approach. Inability to provide critical view of safety was considered an indication for conversion to open cho-lecystectomy. GB adhesion score developed by Akoğlu et al. and intraoperative findings of patients were assessed and recorded by one surgeon (S. C.).[6] Adhesion scoring scale is based on the degree of inflammatory changes in the GB as a guide for predicting the course of operation. During explo-ration, the extent and thickness of the adhesions in the GB region were graded as follows: grade I, no adhesions; grade II, flimsy adhesions that permit easy dissection; grade III, chronic
pericholecystitis and pericholecystic fibrosis making dissec-tion difficult but permitting visualization of the anatomy; and grade IV, thickened GB wall and anatomical distortion due to dense adhesions around the GB, which do not permit safe dissection. Adhesion score, GB perforation during dissection, conversion to open cholecystectomy, operation time, drain usage and intraoperative complications were recorded. Op-eration time was calculated from the initiation of skin incision to the last skin suture.
Postoperative pain measured by visual analog scale (VAS) was recorded.
Data were presented as mean±standard deviation (SD) or median (min-max) according to the distribution pattern. Stu-dent’s t test and Mann-Whitney U test were used for the comparison of continuous variables. Chi-Square test and Fisher’s Exact test were used for the comparison of categori-cal variables. Kendall’s Tau-b Correlation test was used for correlation analysis of categorical variables. A p value less than 0.05 was considered statistically significant. Statistical analyses were performed with SPSS Version 16.00 (Chicago, IL, USA).
RESULTS
All patients were operated successfully without any intraop-erative complications. Seven (17.5) of the forty patients in the acute cholecystitis group were crossed over to chronic cholecystitis group after the pathological assessment of the specimens. All statistical analyses were conducted according to pathologically proven chronic (n=47) and acute cholecys-titis (n=33).
Age and sex were similar between the groups. Demographic and descriptive characteristics of the groups are presented in Table 1.
For easy interpretation of the association, sub-classification for vascularity and intraoperative adhesion scale were per-formed. After the pilot statistical analysis with different com-binations, mild / severe (0, +/++, +++; and Grade I, II/Grade III, IV) sub-classification for vascularity and intraoperative ad-hesion scale was used.
Wall thickness (≥3 mm) and vascularity were found to be increased in acute cholecystitis (p<0.01 and <0.01).
Vascularity was found to be moderately correlated with adhe-sion in acute cholecystitis (p<0.01, r=0.59) but wall thickness did not reveal any correlation (p=0.36).
In acute cholecystitis patients, according to vascularity and adhesion grade, GB perforation, conversion and operation time were not different (p=0.07, 0.99; 0.99, 0.99; and 0.35, 0.18, respectively). Drain usage was found to be statistically
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 152
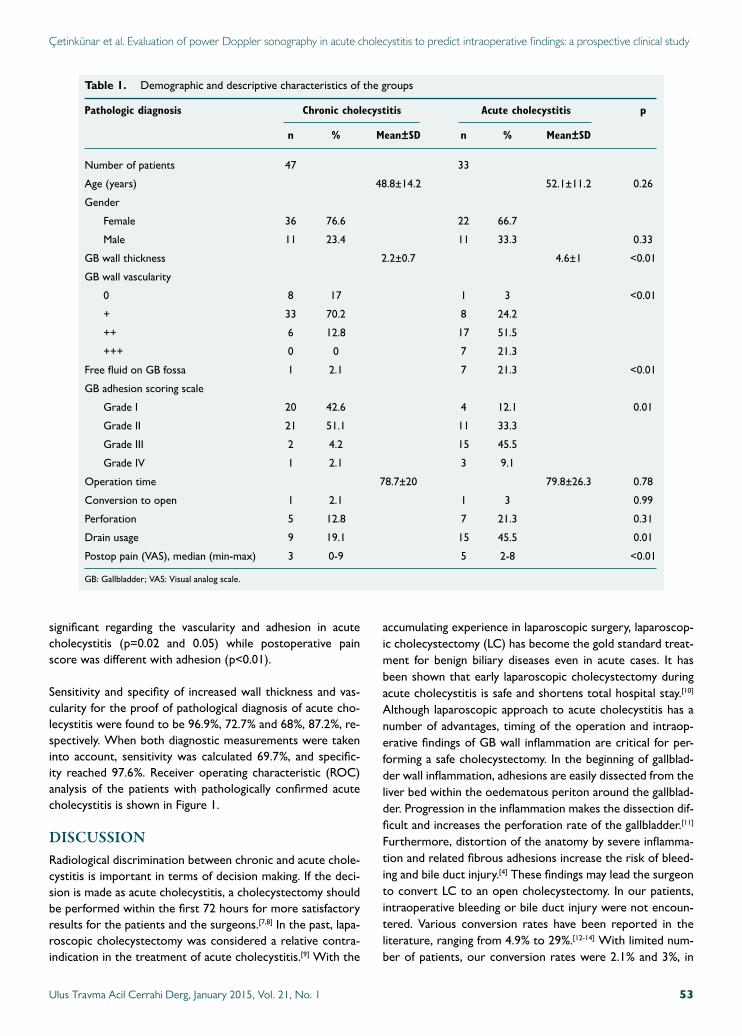
Çetinkünar et al. Evaluation of power Doppler sonography in acute cholecystitis to predict intraoperative findings: a prospective clinical study
significant regarding the vascularity and adhesion in acute cholecystitis (p=0.02 and 0.05) while postoperative pain score was different with adhesion (p<0.01).
Sensitivity and specifity of increased wall thickness and vas-cularity for the proof of pathological diagnosis of acute cho-lecystitis were found to be 96.9%, 72.7% and 68%, 87.2%, re-spectively. When both diagnostic measurements were taken into account, sensitivity was calculated 69.7%, and specific-ity reached 97.6%. Receiver operating characteristic (ROC) analysis of the patients with pathologically confirmed acute cholecystitis is shown in Figure 1.
DISCUSSIONRadiological discrimination between chronic and acute chole-cystitis is important in terms of decision making. If the deci-sion is made as acute cholecystitis, a cholecystectomy should be performed within the first 72 hours for more satisfactory results for the patients and the surgeons.[7,8] In the past, lapa-roscopic cholecystectomy was considered a relative contra-indication in the treatment of acute cholecystitis.[9] With the
accumulating experience in laparoscopic surgery, laparoscop-ic cholecystectomy (LC) has become the gold standard treat-ment for benign biliary diseases even in acute cases. It has been shown that early laparoscopic cholecystectomy during acute cholecystitis is safe and shortens total hospital stay.[10] Although laparoscopic approach to acute cholecystitis has a number of advantages, timing of the operation and intraop-erative findings of GB wall inflammation are critical for per-forming a safe cholecystectomy. In the beginning of gallblad-der wall inflammation, adhesions are easily dissected from the liver bed within the oedematous periton around the gallblad-der. Progression in the inflammation makes the dissection dif-ficult and increases the perforation rate of the gallbladder.[11] Furthermore, distortion of the anatomy by severe inflamma-tion and related fibrous adhesions increase the risk of bleed-ing and bile duct injury.[4] These findings may lead the surgeon to convert LC to an open cholecystectomy. In our patients, intraoperative bleeding or bile duct injury were not encoun-tered. Various conversion rates have been reported in the literature, ranging from 4.9% to 29%.[12-14] With limited num-ber of patients, our conversion rates were 2.1% and 3%, in
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 53
Table 1. Demographic and descriptive characteristics of the groups
Pathologic diagnosis Chronic cholecystitis Acute cholecystitis p
n % Mean±SD n % Mean±SD
Number of patients 47 33
Age (years) 48.8±14.2 52.1±11.2 0.26
Gender
Female 36 76.6 22 66.7
Male 11 23.4 11 33.3 0.33
GB wall thickness 2.2±0.7 4.6±1 <0.01
GB wall vascularity
0 8 17 1 3 <0.01
+ 33 70.2 8 24.2
++ 6 12.8 17 51.5
+++ 0 0 7 21.3
Free fluid on GB fossa 1 2.1 7 21.3 <0.01
GB adhesion scoring scale
Grade I 20 42.6 4 12.1 0.01
Grade II 21 51.1 11 33.3
Grade III 2 4.2 15 45.5
Grade IV 1 2.1 3 9.1
Operation time 78.7±20 79.8±26.3 0.78
Conversion to open 1 2.1 1 3 0.99
Perforation 5 12.8 7 21.3 0.31
Drain usage 9 19.1 15 45.5 0.01
Postop pain (VAS), median (min-max) 3 0-9 5 2-8 <0.01
GB: Gallbladder; VAS: Visual analog scale.
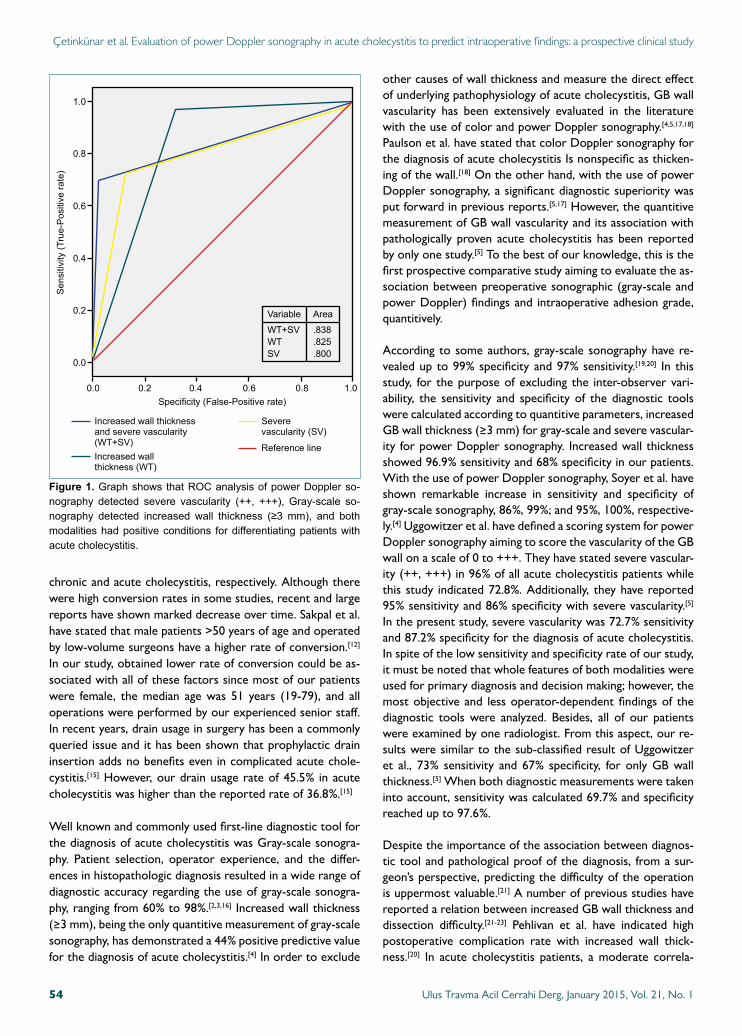
chronic and acute cholecystitis, respectively. Although there were high conversion rates in some studies, recent and large reports have shown marked decrease over time. Sakpal et al. have stated that male patients >50 years of age and operated by low-volume surgeons have a higher rate of conversion.[12] In our study, obtained lower rate of conversion could be as-sociated with all of these factors since most of our patients were female, the median age was 51 years (19-79), and all operations were performed by our experienced senior staff. In recent years, drain usage in surgery has been a commonly queried issue and it has been shown that prophylactic drain insertion adds no benefits even in complicated acute chole-cystitis.[15] However, our drain usage rate of 45.5% in acute cholecystitis was higher than the reported rate of 36.8%.[15]
Well known and commonly used first-line diagnostic tool for the diagnosis of acute cholecystitis was Gray-scale sonogra-phy. Patient selection, operator experience, and the differ-ences in histopathologic diagnosis resulted in a wide range of diagnostic accuracy regarding the use of gray-scale sonogra-phy, ranging from 60% to 98%.[2,3,16] Increased wall thickness (≥3 mm), being the only quantitive measurement of gray-scale sonography, has demonstrated a 44% positive predictive value for the diagnosis of acute cholecystitis.[4] In order to exclude
other causes of wall thickness and measure the direct effect of underlying pathophysiology of acute cholecystitis, GB wall vascularity has been extensively evaluated in the literature with the use of color and power Doppler sonography.[4,5,17,18] Paulson et al. have stated that color Doppler sonography for the diagnosis of acute cholecystitis Is nonspecific as thicken-ing of the wall.[18] On the other hand, with the use of power Doppler sonography, a significant diagnostic superiority was put forward in previous reports.[5,17] However, the quantitive measurement of GB wall vascularity and its association with pathologically proven acute cholecystitis has been reported by only one study.[5] To the best of our knowledge, this is the first prospective comparative study aiming to evaluate the as-sociation between preoperative sonographic (gray-scale and power Doppler) findings and intraoperative adhesion grade, quantitively.
According to some authors, gray-scale sonography have re-vealed up to 99% specificity and 97% sensitivity.[19,20] In this study, for the purpose of excluding the inter-observer vari-ability, the sensitivity and specificity of the diagnostic tools were calculated according to quantitive parameters, increased GB wall thickness (≥3 mm) for gray-scale and severe vascular-ity for power Doppler sonography. Increased wall thickness showed 96.9% sensitivity and 68% specificity in our patients. With the use of power Doppler sonography, Soyer et al. have shown remarkable increase in sensitivity and specificity of gray-scale sonography, 86%, 99%; and 95%, 100%, respective-ly.[4] Uggowitzer et al. have defined a scoring system for power Doppler sonography aiming to score the vascularity of the GB wall on a scale of 0 to +++. They have stated severe vascular-ity (++, +++) in 96% of all acute cholecystitis patients while this study indicated 72.8%. Additionally, they have reported 95% sensitivity and 86% specificity with severe vascularity.[5] In the present study, severe vascularity was 72.7% sensitivity and 87.2% specificity for the diagnosis of acute cholecystitis. In spite of the low sensitivity and specificity rate of our study, it must be noted that whole features of both modalities were used for primary diagnosis and decision making; however, the most objective and less operator-dependent findings of the diagnostic tools were analyzed. Besides, all of our patients were examined by one radiologist. From this aspect, our re-sults were similar to the sub-classified result of Uggowitzer et al., 73% sensitivity and 67% specificity, for only GB wall thickness.[5] When both diagnostic measurements were taken into account, sensitivity was calculated 69.7% and specificity reached up to 97.6%.
Despite the importance of the association between diagnos-tic tool and pathological proof of the diagnosis, from a sur-geon’s perspective, predicting the difficulty of the operation is uppermost valuable.[21] A number of previous studies have reported a relation between increased GB wall thickness and dissection difficulty.[21-23] Pehlivan et al. have indicated high postoperative complication rate with increased wall thick-ness.[20] In acute cholecystitis patients, a moderate correla-
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 154
Çetinkünar et al. Evaluation of power Doppler sonography in acute cholecystitis to predict intraoperative findings: a prospective clinical study
Figure 1. GraphshowsthatROCanalysisofpowerDopplerso-nography detected severe vascularity (++, +++), Gray-scale so-nography detected increased wall thickness (≥3mm), and bothmodalitieshadpositiveconditions fordifferentiatingpatientswithacutecholecystitis.
0.0 0.2 0.4 0.6 0.8 1.0
1.0
0.8
0.6
0.4
0.2
Sensitivity(T
rue-Positiverate)
Specificity(False-Positiverate)
0.0
Variable
WT+SVWTSV
Area
.838
.825
.800
Increasedwallthicknessandseverevascularity(WT+SV)Increasedwallthickness(WT)
Severevascularity(SV)
Referenceline

tion was found between severe vascularity and severe intra-operative adhesion grade but increased wall thickness was not correlated with the presence of adhesion. The positive correlation between severe vascularity and severe adhesion formation did not affect the difficulty of the operation in our patients by means of GB perforation, conversion rate and op-eration time. Drain usage increased in the presence of severe vascularity and severe adhesion. Postoperative pain did not increase in severe vascularity but it increased in the patients developing severe adhesions.
It must be noted that our study had some strong and weak points. For the elimination of inter-operator changes, one radiologist examined all patients, one surgeon assessed GB adhesion score in all operations, and all measurements were based on quantitive scoring systems. Additionally, in order to overcome heterogeneities in previous studies, regarding the sample size and the time frame between diagnosis to operation, patients with confirmed diagnosis of acute cho-lecystitis were operated in the first 24 hours. On the other hand, the difficulties of laparoscopic cholecystectomy were indirectly assessed in terms of GB perforation, conversion rate and operation time; however, all relevant factors affect-ing the difficulty of the operation, such as body mass index (BMI), symptom duration, number of right-upper quadrant pain attack, were not evaluated. Moreover, our sample size was relatively small, especially for the evaluation of rare com-plications of surgery.
ConclusionOur results indicated that GB wall vascularity correlated with adhesion formation but failed to predict difficulties in the dis-section of the operation. The diagnostic specificity of gray-scale sonography for acute cholecystitis could be improved with additional power Doppler examination. However, de-sired diagnostic accuracy of preoperative sonography could not be obtained with only quantitive measurements.
Conflict of interest: None declared.
REFERENCES
1. Carroll BA. Preferred imaging techniques for the diagnosis of cholecysti-tis and cholelithiasis. Ann Surg 1989;210:1-12.
2. Laing FC, Federle MP, Jeffrey RB, Brown TW. Ultrasonic evaluation of patients with acute right upper quadrant pain. Radiology 1981;140:449-55.
3. Ralls PW, Colletti PM, Lapin SA, Chandrasoma P, Boswell WD Jr, Ngo C, et al. Real-time sonography in suspected acute cholecystitis. Prospec-tive evaluation of primary and secondary signs. Radiology 1985;155:767-71.
4. Soyer P, Brouland JP, Boudiaf M, Kardache M, Pelage JP, Panis Y, et al. Color velocity imaging and power Doppler sonography of the gallbladder wall: a new look at sonographic diagnosis of acute cholecystitis. AJR Am J Roentgenol 1998;171:183-8.
5. Uggowitzer M, Kugler C, Schramayer G, Kammerhuber F, Gröll R,
Hausegger KA, et al. Sonography of acute cholecystitis: comparison of color and power Doppler sonography in detecting a hypervascularized gallbladder wall. AJR Am J Roentgenol 1997;168:707-12.
6. Akoğlu M, Ercan M, Bostanci EB, Teke Z, Parlak E. Surgical outcomes of laparoscopic cholecystectomy in scleroatrophic gallbladders. Turk J Gastroenterol 2011;22:183-9.
7. Hunter JG. Acute cholecystitis revisited: get it while it’s hot. Ann Surg 1998;227:468-9.
8. Lo CM, Liu CL, Fan ST, Lai EC, Wong J. Prospective randomized study of early versus delayed laparoscopic cholecystectomy for acute cholecysti-tis. Ann Surg 1998;227:461-7.
9. Phillips EH, Carroll BJ, Fallas MJ. Laparoscopically guided cholecystec-tomy: a detailed report of the first 453 cases performed by one surgical team. Am Surg 1993;59:235-42.
10. Zhou MW, Gu XD, Xiang JB, Chen ZY. Comparison of clinical safety and outcomes of early versus delayed laparoscopic cholecystec-tomy for acute cholecystitis: a meta-analysis. ScientificWorldJournal 2014;2014:274516.
11. Assaff Y, Matter I, Sabo E, Mogilner JG, Nash E, Abrahamson J, et al. Laparoscopic cholecystectomy for acute cholecystitis and the conse-quences of gallbladder perforation, bile spillage, and “loss” of stones. Eur J Surg 1998;164:425-31.
12. Sakpal SV, Bindra SS, Chamberlain RS. Laparoscopic cholecystectomy conversion rates two decades later. JSLS 2010;14:476-483.
13. Kiviluoto T, Sirén J, Luukkonen P, Kivilaakso E. Randomised trial of laparoscopic versus open cholecystectomy for acute and gangrenous cho-lecystitis. Lancet 1998;351:321-5.
14. Sikora SS, Kumar A, Saxena R, Kapoor VK, Kaushik SP. Laparo-scopic cholecystectomy--can conversion be predicted? World J Surg 1995;19:858-60.
15. Bawahab MA, Abd El Maksoud WM, Alsareii SA, Al Amri FS, Ali HF, Nimeri AR, et al. Drainage vs. non-drainage after cholecystectomy for acute cholecystitis: a retrospective study. J Biomed Res 2014;28:240-5.
16. Martínez A, Bona X, Velasco M, Martín J. Diagnostic accuracy of ultra-sound in acute cholecystitis. Gastrointest Radiol 1986;11:334-8.
17. Draghi F, Ferrozzi G, Calliada F, Solcia M, Madonia L, Campani R. Power Doppler ultrasound of gallbladder wall vascularization in inflam-mation: clinical implications. Eur Radiol 2000;10:1587-90.
18. Paulson EK, Kliewer MA, Hertzberg BS, Paine SS, Carroll BA. Diag-nosis of acute cholecystitis with color Doppler sonography: significance of arterial flow in thickened gallbladder wall. AJR Am J Roentgenol 1994;162:1105-8.
19. Ji W, Li LT, Li JS. Role of laparoscopic subtotal cholecystectomy in the treatment of complicated cholecystitis. Hepatobiliary Pancreat Dis Int 2006;5:584-9.
20. Pehlivan T, Alper Cevik A, Ateş E. Relationships among ultrasonograph-ic and demographic, clinical, laboratory findings of patients with acute cholecystitis. Ulus Travma Acil Cerrahi Derg 2005;11:134-40.
21. Stanisic V, Milicevic M, Kocev N, Stojanovic M, Vlaovic D, Babic I, et al. Prediction of difficulties in laparoscopic cholecystectomy on the base of routinely available parameters in a smaller regional hospital. Eur Rev Med Pharmacol Sci 2014;18:1204-11.
22. Fried GM, Barkun JS, Sigman HH, Joseph L, Clas D, Garzon J, et al. Factors determining conversion to laparotomy in patients undergoing laparoscopic cholecystectomy. Am J Surg 1994;167:35-41.
23. Sakuramoto S, Sato S, Okuri T, Sato K, Hiki Y, Kakita A. Preopera-tive evaluation to predict technical difficulties of laparoscopic cholecys-tectomy on the basis of histological inflammation findings on resected gallbladder. Am J Surg 2000;179:114-21.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 55
Çetinkünar et al. Evaluation of power Doppler sonography in acute cholecystitis to predict intraoperative findings: a prospective clinical study

Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 156
OLGU SUNUMU
Akut kolesistitte intraoperatif bulguları öngörmede power Doppler ultrasonundeğerlendirilmesi: İleriye yönelik klinik çalışmaDr. Süleyman Çetinkünar,1 Dr. Hasan Erdem,1 Dr. Recep Aktimur,3 Dr. Gokhan Soker,2
Dr. Hilmi Bozkurt,1 Dr. Enver Reyhan,1 Dr. Selim Sozen,1 Dr. Oktay İrkorucu1
1AdanaNumuneEğitimveAraştırmaHastanesi,GenelCerrahiKliniği,Adana;2AdanaNumuneEğitimveAraştırmaHastanesi,RadyolojiKliniği,Adana;3SamsunEğitimveAraştırmaHastanesi,GenelCerrahiKlinigi,Samsun
AMAÇ: Akut kolesistit tanısında gri-skala ve power Doppler ultrasonografinin değerini belirlemek için kantitatif sonografik ve intraoperatif bulgular arasındaki ilişkiyi göstermek amaçlandı.GEREÇ VE YÖNTEM: Kırk kronik, 40 akut kolesistit hastası değerlendirildi. Akut kolesistit hastalarına erken laparoskopik kolesistektomi uygulandı. Demografik özellikler, sonografik bulgular ve adezyon skoru incelendi. Veriler ileriye yönelik olarak toplandı (clinicaltrials.gov: NCT02156947).BULGULAR: Duvar kalınlığı (≥3 mm) ve vaskülarite akut kolesistitte artmıştı (p<0.01 ve <0.01). Vaskülarite ile adezyon arasında orta düzey ilişki saptanmasına rağmen (p<0.01, r=0.59) perforasyon, konversiyon ve operasyon süresi açısından ilişki saptanmadı. Duvar kalınlığı adezyon gelişimi ile ilişkili değildi (p=0.36). Duvar kalınlığı ve vaskülarite için duyarlılık ve özgüllük sırasıyla: %96.9, %72.7 ve %68, %87.2 idi. Her iki tanısal değerlendirme birleştirildiğinde duyarlılık %69.7 iken, özgüllük %97.6’ya çıkmaktaydı.TARTIŞMA: Vaskülarite, adezyon gelişimi ile ilişkili, ancak operasyon zorluğunu belirlemede yetersiz idi. Gri-skala ultrasonografinin özgüllüğünün power Doppler inceleme ile artırılabileceği görüldü, ancak istenilen tanısal doğruluğa sadece kantitatif ultrasonografik bulgular ile ulaşılamayacağı anlaşıldı.Anahtar sözcükler: Akut; kolesistit; kronik; power Doppler; vaskülarite.
Ulus Travma Acil Cerrahi Derg 2015;21(1):51-56 doi: 10.5505/tjtes.2015.64505
KLİNİK ÇALIŞMA - ÖZET
Çetinkünar et al. Evaluation of power Doppler sonography in acute cholecystitis to predict intraoperative findings: a prospective clinical study
Ciddi yanık travması olan hastalarda hastane kaynaklı idrar yolu enfeksiyonu sıklığı ve risk faktörlerinin araştırılmasıDr. Sıtkı Ün,1 Dr. Yüksel Yılmaz,1 Dr. Mehmet Yıldırım,2
Dr. Fırat Akdeniz,3 Dr. Hakan Türk,4 Dr. Osman Koca5
1KatipÇelebiÜniversitesi,AtatürkEğitimAraştırmaHastanesi,ÜrolojiKliniği,İzmir;2İzmirBozyakaEğitimveAraştırmaHastanesi,GenelCerrahiKliniği,İzmir;3GaziemirDevletHastanesi,ÜrolojiKliniği,İzmir;4İzmirTepecikEğitimveAraştırmaHastanesi,ÜrolojiKliniği,İzmir;5HorasanDevletHastanesi,ÜrolojiKliniği,Erzurum
ÖZET
AMAÇ: Ciddi yanık travması olan hastalarda hastane kaynaklı idrar yolu enfeksiyon sıklığı ve risk faktörlerini araştırmayı amaçladık.
GEREÇ VE YÖNTEM: Bu çalışmada Ağustos 2009-Nisan 2012 tarihleri arasında Bozyaka Eğitim ve Araştırma Hastanesi Yanık Merkezi’nde %20 ve üzerinde yanık yaralanması nedeni ile tedavi gören hastaları kapsayacak şekilde geriye dönük olarak değerlendirme yapıldı. Çalışmaya 69 hasta alındı. Çalışmadaki hastaların 30’u erkek (%43.5), 39’u kadındı (%56.5). Hastaların yaş ortalaması 40.1±16.7 idi.
BULGULAR: DM, sondalı kalma süresi ve sonda bakımı ile hastane kaynaklı idrar yolu enfeksiyon arasında istatistiksel olarak anlamlı korelasyon saptandı (p<0.005).
SONUÇ: Hastane kaynaklı idrar yolu enfeksiyonlarıın büyük bir kısmı üriner kateterizasyonla ilişkilidir. Bu şartlarda takılan üriner kateterin mümkün olduğunca kısa sürede sonlandırılması hastane kaynaklı idrar yolu enfeksiyonu gelişiminin önlenmesi açısından dikkat edilmesi gereken önemli bir noktadır. Hastanın sondalı kalması zorunlu ise düzenli olarak sonda bakımının yapılmasını önermekteyiz.
Anahtar sözcükler: İdrar yolu enfeksiyonu; üriner kateterizasyon; yanık travması.
GİRİŞ
Ciddi yanık travmalı hastalarda ortaya çıkan hastane kaynaklı enfeksiyonlar en sık gözlenen ölüm nedenlerinden birisidir.[1] Yetişkinlerde toplam vücut yüzey alanı’nın (TVYA) %20’den fazlasında yanık olması, %5’den fazla tam kat yanık olması, yük-sek voltaj yaralanması, bilinen inhalasyon yanığı olması, yüz-el gibi bölgelerde yanık olması ciddi yaralanma olarak tanımlan-mıştır.[2] Deri bütünlüğünün bozulması, yanık sonrası gelişen immün süpresif etki, tanı ve tedavi için girişim yapılması, has-tanede uzun süre yatış gerektirmesi nedeniyle yanıklı hastalar
hastane kaynaklı enfeksiyonlara daha açıktırlar. Gelişen enfek-siyonlar önemli morbidite ve mortaliteye yol açmaktadır.[2]
Yanık hastalarında yoğun antibiyotik kullanımı floranın bozul-masına ve enfeksiyonların oluşmasına neden olabilmektedir.[2]
Günümüzde tüm hasta gruplarında da hastane kaynaklı enfek-siyonlar önemli bir morbidite ve mortalite sebebidir. Sağlık hizmetlerinde iyileşme, hastanede bakım hizmetlerindeki ge-lişme ve yeni antibiyotiklerin geliştirilmesine rağmen hastane enfeksiyonları insidansı azalmış değildir.[3]
İdrar yolu enfeksiyonları (İYE) tüm hastane enfeksiyonlarının %30-40’ını oluştururken, yoğun bakımda meydana gelen İYE ise tüm hastane enfeksiyonlarının %8-21’ini oluşturmaktadır.[4,5] Yoğun bakım hastalarında yapılan geniş bir surveyans ça-lışmasında İYE en sık üçüncü enfeksiyon olarak saptanmış.[6]
Hastane kaynaklı idrar yolu enfeksiyonlarının (HKİYE) önde gelen nedeni bir kalıcı kateter varlığıdır. HKİYE insidansı kalıcı kateter kullanan hastalarda yaklaşık olarak %15’dir.[7] Yoğun bakım hastalarında idrar çıkışı takibi sık yapıldığı için bu has-
K L İ N İ K Ç A L I Ş M A
Sorumlu yazar: Dr. Sıtkı Ün,
Katip Çelebi Üniversitesi, Atatürk Eğitim ve Araştırma Hastanesi,
Üroloji Kliniği, İzmir
Tel: +90 232 - 243 43 43 E-posta: [email protected]
Ulus Travma Acil Cerrahi Derg2015;21(1):57-62doi: 10.5505/tjtes.2015.35920
Telif hakkı 2015 TJTES
Ulus Travma Acil Cerrahi Derg, Ocak 2015, Cilt. 21, Sayı. 1 57

Ün ve ark. Ciddi yanık travması olan hastalarda hastane kaynaklı idrar yolu enfeksiyonu sıklığı ve risk faktörlerinin araştırılması
talarda kalıcı kateter kullanımı daha sıktır. Ayrıca yoğun bakım hastaları metabolik instabiliteleri nedeniyle diğer hastalara göre enfeksiyona daha açıktırlar.[7,8] Günümüzde HKİYE tanısı genel kabul olarak Centers for Disease Control and Preven-tion (CDC) tarafından belirlenen semptomlu ve semptomsuz HKİYE tanı kriterleri ile yapılmaktadır.[9]
Çalışmamızda majör yanık yaralanması nedeniyle yoğun bakım ünitesinde takip edilen hastalarda HKİYE sıklığı ve risk faktör-lerini araştırmayı amaçladık.
GEREÇ VE YÖNTEM
Bu çalışmada Ağustos 2009-Nisan 2012 tarihleri arasında Bozyaka Eğitim Araştırma Hastanesi Yanık Merkezi’nde %20 ve üzerinde yanık yaralanması nedeni ile tedavi gören hastaları kapsayacak şekilde geriye dönük olarak değerlendirme yapıl-mıştır. İnhalasyon yanığı olan ve genital bölge yanığı olan has-talar çalışma dışı bırakılmıştır. Çalışmaya 69 hasta dahil edil-miştir. Hastaların demografik verileri, boy, kilo, foley kateter kalış süreleri, profilaksi durumu, sonda bakım sıklığı, operas-yon durumu, eşlik eden hastalıkları, fizik muayene bulguları, la-baratuvar sonuçları, yanık yüzdeleri kaydedildi. %20 ve üzerin-de yanık yaralanması olan hastalarda bilinç durumunun yeterli olmaması, erken dönem sık idrar çıkışı takibi, immobilizasyon ihtiyacı gibi durumlar olması nedeniyle, tümüne üriner katete-rizasyon uygulaması yapıldı. Kültür için idrar örnekleri, steril şartlarda kateterin üretraya yakın olan kısmından ucunda 21 no’lu bir iğne bulunan enjektörle alınmıştır. Steril tüplere alı-nan örnek en geç 30 dakika içerisinde labaratuvara ulaştırıl-mıştır. HKİYE tanısı CDC tanı kriterlerine göre konuldu.
Veriler bilgisayar ortamında SPSS 15.0 istatistik programına girilerek değerlendirildi. p<0.05 istatistiksel anlamlılık düzeyi olarak kabul edildi.
BULGULAR
Çalışmadaki hastaların 30’u erkek (%43.5), 39’u kadındı (%56.5). Hastaların yaş ortalaması 40.1±16.7 olarak hesaplan-dı. Hastaların toplam yanık yüzey alan ortalaması %33.6±15 olarak hesaplandı. Hastaların hastanede yatış süreleri ortala-ma 33.9±18.8 gün olarak hesaplandı. 12 hastada (%17.4) eşlik eden Diabetes Mellitus (DM) tespit edildi. CDC kriterlerine göre değerlendirildiğinde yedi hastada (%10.1) idrar yolu en-feksiyonu saptandı. Bu hastalarda ateş, pollaküri, dizüri veya suprapubik duyarlılık bulgularından birisine ek olarak idrar kültüründe >105 koloni/ml üreme saptandı.
Hastaların 32’si (%46.4) profilaktik antibiyoterapi alırken, 37 hastanın (%53.6) ise profilaktik tedavi almadığı görüldü. Profi-laktik antibiyotik tedavisi yanık yarası eksizyonu, otogreftleme gibi cerrahi girişim yapılacak olan hastalara ve yoğun kontami-ne yarası olan hastalara yapıldı. Profilaktik antibiyoterapi ön-cesi yara kültürü alındı. Profilaktik tedavi olarak Amoksisilin Klavulonat 1 gr 2x1 İV olarak verildi.
Hastanın tümüne foley sonda takılmış, mobilizasyon ve bilinç durumu değerlendirilmelerinin sonrası foley kateterleri çekil-miştir. Sonda kalma süreleri en az bir gün, en çok 40 gün ola-rak tespit edildi. Ortalama sonda kalış süreleri ise 9.3±8.4 gün olarak tespit edildi. Sonda kalış süreleri 10 günün üzerinde 19 hasta (%27.5), 10 günün altında 50 hasta (%72.5) mevcuttu. Hastalardan 37’sine (%53.6) düzenli günlük sonda bakımı ya-pıldı. 32 hastaya (%46.4) ise hasta uyumsuzluğu ve personel yetersizliği gibi çeşitli sebeplerden dolayı düzenli günlük sonda bakımı yapılamadı.
Yattığı süre içerisinde 25 hastaya (%36.2) eskaratomi veya otogreftleme yapıldı, 44 hastaya (%63.8) ise cerrahi girişim yapılmadı. Böbrek fonksiyonları değerlendirildiğinde ilk başvu-ru anında 12 hastada (%17.4) kreatinin değeri 1.5 ve üzerinde tespit edildi.
Hastaların yaş, cinsiyet, yanık oranı, hastanede kalış süresi, profilaktik antibiyotik kullanımı, sondalı kalma süresi, sonda bakımı, geçirilmiş cerrahi girişim öyküsü, DM varlığı, başvuru anında böbrek fonksiyonlarında bozukluk olması şeklindeki değişkenleri tek değişkenli analiz ile değerlendirildi. Cinsiyet, DM varlığı, sondalı kalma süresi, sonda bakımı ve hastane-de kalma süresi ile HKİYE arasında tek değişkenli analizde istatistiksel olarak anlamlı korelasyon saptandı (p<0.005). Çok değişkenli analiz ile değerlendirildiğinde ise DM varlı-ğı, sondalı kalma süresi ve sonda bakımı ile HKİYE arasında istatistiksel olarak anlamlı korelasyon saptandı (p<0.005) (Tablo 1).
TARTIŞMA
Ciddi yanık travmalı hastalar deri bütünlüğünün ve immün ya-nıtın bozulması nedeni ile enfeksiyona oldukça açık durumda-dırlar. Yanıklı hastalarda enfeksiyonlar en sık ölüme neden olan yanık komplikasyonudur.[10] Yanık hastaları; deri bütünlüğünün bozulması sonucu ortaya çıkan artmış damaryolu girişimleri, idrar çıkış takibi için uzamış mesane kateterizasyonunun ve çeşitli sebeplerle gerekli olan sık cerrahi girişimlerin yapıldığı bir hasta grubudur. Literatüre baktığımızda invaziv girişimlerin enfeksiyon açısından risk faktörü olduğunu görülmektedir.[11] İdrar kataterizasyonunun uzaması bakteriyel kolonizasyon ve enfeksiyon riskini artırdığı bilinmektedir.[12] Yanık hastalarında en sık görülen enfeksiyonlar yara yeri enfeksiyonu, pnömoni ve idrar yolu enfeksiyonlarıdır.[13]
Hastane kaynaklı idrar yolu enfeksiyonlarının tanısı için genel-likle CDC kriterleri kullanılmaktadır.[9] Bizde çalışmamızda bu kriterleri kullanarak değerlendirme yaptık.
Hastane kaynaklı idrar yolu enfeksiyonlarının etiyolojisinde mesaneye kateter uygulaması, yaş, kadın cinsiyet, diabet, im-münsupresyon, üriner sistemin fonksiyonel ve anatomik bo-zukluğu, genetik nedenler, konakçının yatkınlığı, uzun hasta-nede kalış süresi gibi faktörler bulunmakla birlikte en önemlisi üriner kateterizasyondur.[6,14]
Ulus Travma Acil Cerrahi Derg, Ocak 2015, Cilt. 21, Sayı. 158
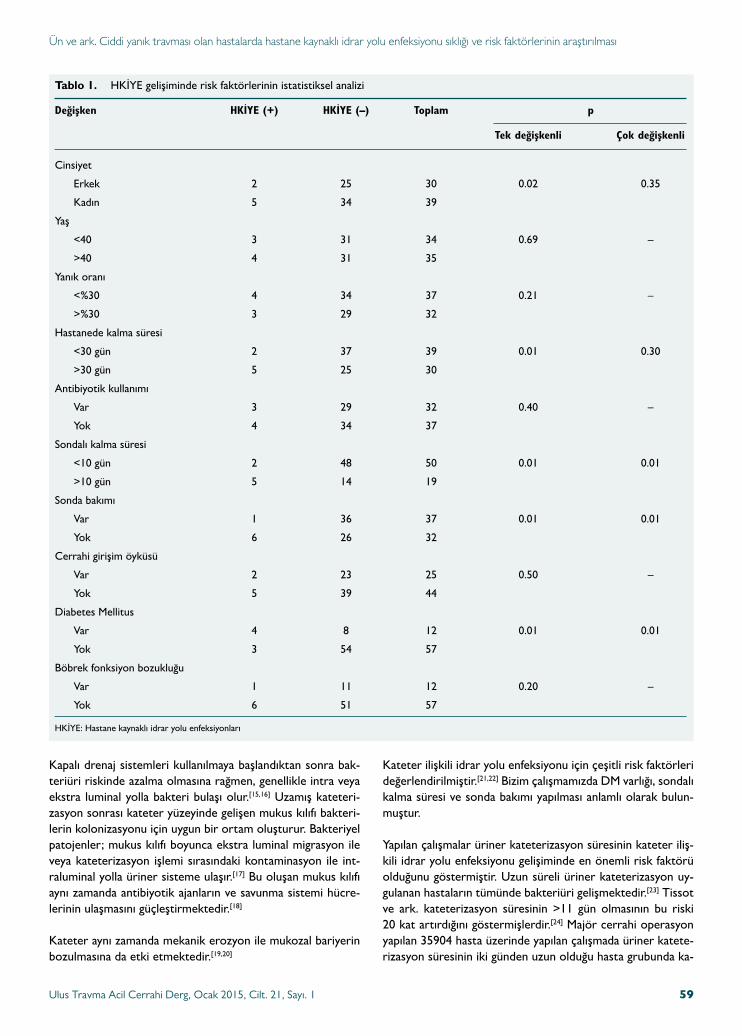
Ün ve ark. Ciddi yanık travması olan hastalarda hastane kaynaklı idrar yolu enfeksiyonu sıklığı ve risk faktörlerinin araştırılması
Kapalı drenaj sistemleri kullanılmaya başlandıktan sonra bak-teriüri riskinde azalma olmasına rağmen, genellikle intra veya ekstra luminal yolla bakteri bulaşı olur.[15,16] Uzamış kateteri-zasyon sonrası kateter yüzeyinde gelişen mukus kılıfı bakteri-lerin kolonizasyonu için uygun bir ortam oluşturur. Bakteriyel patojenler; mukus kılıfı boyunca ekstra luminal migrasyon ile veya kateterizasyon işlemi sırasındaki kontaminasyon ile int-raluminal yolla üriner sisteme ulaşır.[17] Bu oluşan mukus kılıfı aynı zamanda antibiyotik ajanların ve savunma sistemi hücre-lerinin ulaşmasını güçleştirmektedir.[18]
Kateter aynı zamanda mekanik erozyon ile mukozal bariyerin bozulmasına da etki etmektedir.[19,20]
Kateter ilişkili idrar yolu enfeksiyonu için çeşitli risk faktörleri değerlendirilmiştir.[21,22] Bizim çalışmamızda DM varlığı, sondalı kalma süresi ve sonda bakımı yapılması anlamlı olarak bulun-muştur.
Yapılan çalışmalar üriner kateterizasyon süresinin kateter iliş-kili idrar yolu enfeksiyonu gelişiminde en önemli risk faktörü olduğunu göstermiştir. Uzun süreli üriner kateterizasyon uy-gulanan hastaların tümünde bakteriüri gelişmektedir.[23] Tissot ve ark. kateterizasyon süresinin >11 gün olmasının bu riski 20 kat artırdığını göstermişlerdir.[24] Majör cerrahi operasyon yapılan 35904 hasta üzerinde yapılan çalışmada üriner katete-rizasyon süresinin iki günden uzun olduğu hasta grubunda ka-
Ulus Travma Acil Cerrahi Derg, Ocak 2015, Cilt. 21, Sayı. 1 59
Tablo 1. HKİYE gelişiminde risk faktörlerinin istatistiksel analizi
Değişken HKİYE (+) HKİYE (–) Toplam p
Tek değişkenli Çok değişkenli
Cinsiyet
Erkek 2 25 30 0.02 0.35
Kadın 5 34 39
Yaş
<40 3 31 34 0.69 –
>40 4 31 35
Yanık oranı
<%30 4 34 37 0.21 –
>%30 3 29 32
Hastanede kalma süresi
<30 gün 2 37 39 0.01 0.30
>30 gün 5 25 30
Antibiyotik kullanımı
Var 3 29 32 0.40 –
Yok 4 34 37
Sondalı kalma süresi
<10 gün 2 48 50 0.01 0.01
>10 gün 5 14 19
Sonda bakımı
Var 1 36 37 0.01 0.01
Yok 6 26 32
Cerrahi girişim öyküsü
Var 2 23 25 0.50 –
Yok 5 39 44
Diabetes Mellitus
Var 4 8 12 0.01 0.01
Yok 3 54 57
Böbrek fonksiyon bozukluğu
Var 1 11 12 0.20 –
Yok 6 51 57
HKİYE: Hastane kaynaklı idrar yolu enfeksiyonları

teter ilişkili idrar yolu enfeksiyonu gelişimi riskinin diğer has-talara oranla anlamlı olarak yüksek olduğunu göstermişlerdir.[22] Bizim çalışmamızda da 10 gün ve üzerinde kateterizasyonu devam eden hasta grubu ile, kateter ilişkili idrar yolu enfeksi-yonu arasında anlamlı korelasyon saptandı.
Pek çok çalışmada bakteriüri gelişimi ile cinsiyetin rolü de-ğerlendirilmiş, erkeklerle karşılaştırıldığında kadınlarda kate-ter ilişkili idrar yolu enfeksiyonunun daha sık geliştiği göste-rilmiştir. Kateterize hastalarda yaptılan bir çalışmada kateter ilişkili idrar yolu enfeksiyonu gelişen hastaların %66’sının kadın olduğunu göstermiştir.[22,25] Yoğun bakımda tedavi alan hasta-larda yapılan bir çalışmada kadın cinsiyeti kateter ilişkili idrar yolu enfeksiyonu gelişimi için bağımsız bir risk faktörü olarak bulmuşlardır.[26,27] Çeşitli hasta grupları üzerinde yapılan çalış-malarda kadın cinsiyet ile kateter ilişkili idrar yolu enfeksiyonu gelişimi arasındaki ilişkiyi gösterilmiştir.[28,29] Bizim çalışmamız-da tek değişkenli analizde kadın cinsiyet ile kateter ilişkili idrar yolu enfeksiyonu arasında anlamlı korelasyon saptandı. Ancak çok değişkenli analizde anlamlı olarak saptanmadı. Literatürle çalışmamız arasındaki bu farklılığın, bizim çalışmamızın sadece yanık nedeniyle yoğun bakımda tedavi alan hastaları içermesi ve hasta sayımızın daha az olmasından kaynakalabileceğini dü-şünüyoruz.
Yapılan bazı çalışmalarda ileri yaş kateter ilişkili idrar yolu en-feksiyonu gelişimi için bir risk faktörü olarak tanımlanmıştır. İleri yaşın kateter ilişkili idrar yolu enfeksiyonu gelişimi için bir risk faktörü olduğunu öne sürülmüştür.[29] Bunların aksine bir çalışmada yaş ile kateter ilişkili idrar yolu enfeksiyonu gelişim arasında istatistiksel olarak anlamlı bir ilişki saptamamıştır.[30] Çalışmamızda yaş ile HKİYE arasında anlamlı bir ilişki saptan-madı. Bu farklılık; çalışmamızdaki hastaların yanık maruziyeti-ne daha müsait olan nispeten daha genç yaş grubunda hasta-lardan oluşmasından kaynaklanabilir.
Üriner kateterli hastalarda antibiyotik kullanımının bakteriüri gelişimine etkisi konusunda yapılan çalışmalarda farklı sonuç-lar bildirilmektedir. Antibiyotik kullanan hastalarda idrar yolu enfeksiyonu gelişme oranını daha düşük bulan çalışmalar oldu-ğu gibi, antibiyotik kullanımının katetere bağlı enfeksiyonları önlemediği hatta daha dirençli patojenlerle enfeksiyon gelişi-mine yol açtığını gösteren çalışmalarda mevcuttur. Üriner ka-teterize hastalarda sistemik antimikrobiyal kullanılmamasının kateter ilişkili idrar yolu enfeksiyonu gelişimi için bir risk fak-törü olduğunu saptanmıştır.[28] Öte yandan kateter çıkarıldık-tan sonra ilk 48 saatte antibiyotik kullanımının idrar yolu en-feksiyonu insidansını düşüreceğini öne sürülmüştür.[31] Bizim çalışmamızda ise profilaktik antibiyotik kullanımı ile kateter ilişkili idrar yolu enfeksiyonu arasında korelasyon saptanmadı.Yapılan bazı çalışmalarda meatusun mikroorganizmalarca ko-lonize edilmesi kateterize hastalarda enfeksiyon riskini artır-dığı gösterildiyse de kapalı sistem kateterize hastalarda gün-lük meatus bakımının HKİYE riskini azaltmada etkili olmadığı gösterilmiştir.[32] Bizim çalışmamızda ise bunun aksine kate-ter bakımının düzenli yapılmaması enfeksiyon açısından risk
olarak saptandı. Bunun majör yanık travmalı hasta grubunun kontaminasyon riskinin daha yüksek olmasından kaynaklanabi-leceğini düşünmekteyiz.
Yoğun bakımda kalış süresinin uzaması idrar yolu enfeksiyo-nu gelişme riskini artırmaktadır.[33] Bizim çalışmamızda yatış süresi ile HKİYE arasında tek değişkenli analizde anlamlı ko-relasyon saptandı. Çoklu analizde ise bu korelasyon saptan-madı. Bu farklılık çalışmamızın sadece yanık nedeniyle yoğun bakımda tedavi alan hastaları içermesi ve hasta sayımızın daha az olmasından kaynaklabileceğini düşünüyoruz.
Pek çok çalışmada DM ile HKİYE arasındaki ilişki gösterilmiş-tir.[34,35] Bizim çalışmamızda da DM ile HKİYE arasında anlamlı bir korelasyon saptanmıştır.
Literatürde yanık oranı ile HKİYE arasındaki ilişkiye yönelik net bir veri yoktur. Bizim çalışmamızda yanık oranı ile HKİYE ara-sında korelasyon saptanmamıştır. Ancak yanık oranı arttıkça bu hastaların sistemik komplikasyonlara daha açık olması ve mor-talitenin artması nedeniyle HKİYE saptanması zorlaşmaktadır.
Hastalarda başvuru anında böbrek fonksiyonlarında bozukluk ile HKİYE arasında korelasyon saptanmadı. Böbrek fonksiyon-larındaki bozukluğun çoğunlukla sıvı kaybından kaynaklanması nedeniyle hidrasyon ile tedavisi sonrası biyokimyasal paramet-relerin kontrolünün sağlanabilmesi nedeniyle olduğunu düşü-nüyoruz. Cerrahi girişim ise sondalı kalma süresini artırmakla birlikte anlamlı bir korelasyon saptanmamıştır.
Hasta sayısının az olması ve net sınırlarla sonda bakım kriter-lerinin belirli olmaması çalışmamızı sınırlandırmaktadır. Daha geniş seriler ile yapılacak çalışmalara ihtiyaç vardır.
Sonuçlarİdrar yolu enfeksiyonları hastane enfeksiyonlarının önemli bir kısmını oluşturur. HKİYE morbidite, mortalitede artışla bera-ber hasta sağaltım giderlerinde önemli artışlara sebep olduk-larından gün geçtikçe daha da önem kazanmaktadır ve büyük bir kısmı üriner kateterizasyonla ilişkilidir.
Sonuç olarak, üriner kateterizasyonun uygun endikasyonlarda, eğitilmiş personel tarafından asepsi koşullarına riayet edilerek uygulanması gereklidir. Bu şartlarda takılan üriner kateterin mümkün olduğunca kısa sürede sonlandırılması nozokomiyal idrar yolu enfeksiyonu gelişiminin önlenmesi açısından dikkat edilmesi gereken önemli bir noktadır. Şayet hastanın sondalı kalması zorunlu ise düzenli olarak sonda bakımının yapılmasını önermekteyiz.
Kateter lümeni içinde mikroorganizmaların kolonizasyonu ile nozokomiyal idrar yolu enfeksiyonu arasındaki ilişki henüz tam olarak aydınlatılamamış olmakla beraber bakteriüri geli-şiminde öncül gösterge olabilir. Kateter ilişkili idrar yolu en-feksiyonu tanısı alan ve uygun antimikrobiyal tedaviye rağmen
Ün ve ark. Ciddi yanık travması olan hastalarda hastane kaynaklı idrar yolu enfeksiyonu sıklığı ve risk faktörlerinin araştırılması
Ulus Travma Acil Cerrahi Derg, Ocak 2015, Cilt. 21, Sayı. 160
yeterli klinik yanıt alınamayan hastalarda üriner kateter içinde biyofilm gelişmiş olabileceği de göz önüne alınarak üriner ka-teterizasyonun sonlandırılması veya üriner kateterin değişimi mutlaka değerlendirilmelidir.
Çıkar örtüşmesi: Çıkar örtüşmesi bulunmadığı belirtilmiştir.
KAYNAKLAR
1. Al B, Yildirim C, Coban S, Aldemir M, Güloğlu C. Mortality factors in flame and scalds burns: our experience in 816 patients. Ulus Travma Acil Cerrahi Derg 2009;15:599-606.
2. Garmel, edited by Mahadevan SV, Gus M. An introduction to clinical emergency medicine. 2nd ed. Cambridge: Cambridge University Press; 2012. p. 216-9.
3. Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Dis Mon 2003;49:53-70.
4. Eriksen HM, Iversen BG, Aavitsland P. Prevalence of nosocomial infec-tions in hospitals in Norway, 2002 and 2003. J Hosp Infect 2005;60:40-5.
5. Lizioli A, Privitera G, Alliata E, Antonietta Banfi EM, Boselli L, Panceri ML, et al. Prevalence of nosocomial infections in Italy: result from the Lombardy survey in 2000. J Hosp Infect 2003;54:141-8.
6. Vincent JL, Bihari DJ, Suter PM, Bruining HA, White J, Nicolas-Cha-noin MH, et al. The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in In-tensive Care (EPIC) Study. EPIC International Advisory Committee. JAMA 1995;274:639-44.
7. Parida S, Mishra SK. Urinary tract infections in the critical care unit: A brief review. Indian J Crit Care Med 2013;17:370-4..
8. Saint S. Clinical and economic consequences of nosocomial catheter-related bacteriuria. Am J Infect Control 2000;28:68-75.
9. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC defini-tions for nosocomial infections. In: Olmsted RN, editor. APIC Infection Control and Applied Epidemiology: Principles and Practice. St. Louis: Mosby; 1996. p. 1-20.
10. Taneja N, Emmanuel R, Chari PS, Sharma M. A prospective study of hospital-acquired infections in burn patients at a tertiary care referral cen-tre in North India. Burns 2004;30:665-9.
11. Oncul O, Yüksel F, Altunay H, Açikel C, Celiköz B, Cavuşlu S. The evalu-ation of nosocomial infection during 1-year-period in the burn unit of a training hospital in Istanbul, Turkey. Burns 2002;28:738-44.
12. Isikgoz Tasbakan M, Durusoy R, Pullukcu H, Sipahi OR, Ulusoy S; 2011 Turkish Nosocomial Urinary Tract Infection Study Group. Hospi-tal-acquired urinary tract infection point prevalence in Turkey: differenc-es in risk factors among patient groups. Ann Clin Microbiol Antimicrob 2013;12:31.
13. Peck MD. Epidemiology of burns throughout the world. Part I: Distribu-tion and risk factors. Burns 2011;37:1087-100.
14. Neal DE Jr. Complicated urinary tract infections. Urol Clin North Am 2008;35:13-22.
15. Chenoweth C, Saint S. Preventing catheter-associated urinary tract infec-tions in the intensive care unit. Crit Care Clin 2013;29:19-32.
16. Tambyah PA, Halvorson KT, Maki DG. A prospective study of patho-genesis of catheter-associated urinary tract infections. Mayo Clin Proc 1999;74:131-6.
17. Saint S, Chenoweth CE. Biofilms and catheter-associated urinary tract infections. Infect Dis Clin North Am 2003;17:411-32.
18. Nickel JC, Costerton JW, McLean RJ, Olson M. Bacterial biofilms: influ-ence on the pathogenesis, diagnosis and treatment of urinary tract infec-tions. J Antimicrob Chemother 1994;33 Suppl A:31-41.
19. Hakuno H, Yamamoto M, Oie S, Kamiya A. Microbial contamination of disinfectants used for intermittent self-catheterization. Jpn J Infect Dis 2010;63:277-9.
20. Kurosaka Y, Ishida Y, Yamamura E, Takase H, Otani T, Kumon H. A non-surgical rat model of foreign body-associated urinary tract infection with Pseudomonas aeruginosa. Microbiol Immunol 2001;45:9-15.
21. Saint S, Chenoweth CE. Biofilms and catheter-associated urinary tract infections. Infect Dis Clin North Am 2003;17:411-32.
22. Tambyah PA, Maki DG. Catheter-associated urinary tract infection is rarely symptomatic: a prospective study of 1,497 catheterized patients. Arch Intern Med 2000;160:678-82.
23. Bhatia N, Daga MK, Garg S, Prakash SK. Urinary catheterization in medical wards. J Glob Infect Dis 2010;2:83-90.
24. Tissot E, Limat S, Cornette C, Capellier G. Risk factors for catheter-as-sociated bacteriuria in a medical intensive care unit. Eur J Clin Microbiol Infect Dis 2001;20:260-2.
25. Wald HL, Ma A, Bratzler DW, Kramer AM. Indwelling urinary catheter use in the postoperative period: analysis of the national surgical infection prevention project data. Arch Surg 2008;143:551-7.
26. Leone M, Albanèse J, Garnier F, Sapin C, Barrau K, Bimar MC, et al. Risk factors of nosocomial catheter-associated urinary tract infection in a polyvalent intensive care unit. Intensive Care Med 2003;29:1077-80.
27. Laupland KB, Zygun DA, Davies HD, Church DL, Louie TJ, Doig CJ. Incidence and risk factors for acquiring nosocomial urinary tract infection in the critically ill. J Crit Care 2002;17:50-7.
28. Johnson EN, Marconi VC, Murray CK. Hospital-acquired device-associated infections at a deployed military hospital in Iraq. J Trauma 2009;66(4 Suppl):157-63.
29. Puri J, Mishra B, Mal A, Murthy NS, Thakur A, Dogra V, et al. Catheter associated urinary tract infections in neurology and neurosurgical units. J Infect 2002;44:171-5.
30. Piljic D, Porobic-Jahic H, Piljic D, Ahmetagic S, Jahic R. Chateter-associ-ated Urinary Tract Infections in Adults. Mater Sociomed 2013;25:182-6.
31. Nicolle LE. Catheter-related urinary tract infection. Drugs Aging 2005;22:627-39.
32. Jacobsen SM, Stickler DJ, Mobley HL, Shirtliff ME. Complicated cathe-ter-associated urinary tract infections due to Escherichia coli and Proteus mirabilis. Clin Microbiol Rev 2008;21:26-59.
33. Aygen B, Kayabaş Ü, Güven M. Erciyes Üniversitesi Tıp Fakültesi yoğun bakım üniteleri nozokomiyal enfeksiyon sürveyansı: Epidemiy-oloji, risk faktörleri ve prognozu etkileyen faktörler. Yoğun Bakım Dergisi 2001;1:122-30.
34. Medina M, Martínez-Gallego G, Sillero-Arenas M, Delgado-Rodríguez M. Risk factors and length of stay attributable to hospital infections of the urinary tract in general surgery patients. [Article in Spanish] Enferm Infecc Microbiol Clin 1997;15:310-4. [Abstract]
35. Hooton TM, Bradley SF, Cardenas DD, Colgan R, Geerlings SE, Rice JC, et al. Diagnosis, prevention, and treatment of catheter-associated uri-nary tract infection in adults: 2009 International Clinical Practice Guide-lines from the Infectious Diseases Society of America. Clin Infect Dis 2010;50:625-63.
Ün ve ark. Ciddi yanık travması olan hastalarda hastane kaynaklı idrar yolu enfeksiyonu sıklığı ve risk faktörlerinin araştırılması
Ulus Travma Acil Cerrahi Derg, Ocak 2015, Cilt. 21, Sayı. 1 61

Ün ve ark. Ciddi yanık travması olan hastalarda hastane kaynaklı idrar yolu enfeksiyonu sıklığı ve risk faktörlerinin araştırılması
Ulus Travma Acil Cerrahi Derg, Ocak 2015, Cilt. 21, Sayı. 162
OLGU SUNUMU
Investigation of prevalance and risk factors for hospital-acquired urinary tractinfections in patients with severe burn injurySıtkı Ün, M.D.,1 Yüksel Yılmaz, M.D.,1 Mehmet Yıldırım, M.D.,2 Fırat Akdeniz, M.D.,3 Hakan Türk, M.D.,4 Osman Koca, M.D.5
1DepartmentofUrology,KatipÇelebiUniversityAtatürkTrainingandResearchHospital,Izmir;2DepartmentofGeneralSurgery,IzmirBozyakaTrainingandResearchHospital,IzmirarchHospital,Izmir;3DepartmentofUrology,GaziemirStateHospital,Izmir;4DepartmentofUrology,IzmirTepecikTrainingandResearchHospital,Izmir;5DepartmentofUrology,HorasanStateHospital,Erzurum
BACKGROUND: This study aimed to investigate the prevalence and risk factors for hospital-acquired urinary tract infections in patients with severe burn injuries.METHODS: In this study, patients treated due to their burn injuries of greater than 20% between August 2009 and April 2012 in Bozyaka Training and Research Hospital Burn Center were assessed retrospectively. Sixty nine patients (30 [43.5%] males, 39 [56.5%] females; mean age 40.1±16.7 years) were included into the study.RESULTS: DM, duration of the catheter and catheter care showed a statistically significant correlation with hospital-acquired urinary tract infections (p<0.005).DISCUSSION: A large number of hospital-acquired urinary tract infections are associated with urinary catheterization. In addition, removing urinary catheter within the shortest time possible is another issue to be considered for the prevention of these infections. If the catheter has to remain for a longer time, regular catheter care is recommended.Key words: Burn injury; urinary catheterization; urinary tract infection.
Ulus Travma Acil Cerrahi Derg 2015;21(1):57-62 doi: 10.5505/tjtes.2015.35920
ORIGINAL ARTICLE - ABSTRACT
Closed reduction of traumatic bilateral anteriorhip dislocations with sedation: a case reportand review of the literatureChee Kidd Chiu1, M.B.B.S., M.S.Orth., Tiong Soon Ng2, M.D., Nayyer Naveed Wazir3, M.B.B.S. M.S.Orth.,Kareem Abdul Bhurhanudeen3, M.B.B.S., M.S.Orth.
C A S E R E P O R T
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 63
1DepartmentofOrthopaedicSurgery,FacultyofMedicine,UniversityofMalaya,KualaLumpur,Malaysia;2DepartmentofOrthopaedicSurgery,HospitalTuankuJaafar,Seremban,Malaysia;3DepartmentofOrthopaedicSurgery,InternationalMedicalUniversity,Seremban,Malaysia
ABSTRACT
A rare case of bilateral anterior hip dislocation reduced under sedation was reported in this study. A 47-year-old man was knocked down by a car and sustained bilateral anterior hip dislocation which was reduced successfully with sedation using titrated dose of intravenous Midazolam in combination with Pethidine. A modified Lefkowitz maneuver using the manipulator’s thigh as a fulcrum was used. Patient started weight bearing in the second month after injury and was walking without any hip pain at the twenty-fourth month follow-up. Thirteen case reports describing bilateral anterior hip dislocations were found while reviewing the literature and it was no-ticed that only one author had reported the usage of intravenous sedation (Propofol) for the reduction procedure. However, no author reported the use of Lefkowitz maneuver for this purpose. Consequently, reduction of a bilateral anterior hip dislocation is possible with sedation using a modified Lefkowitz maneuver.
Key words: Bilateral anterior hip dislocation; modified Lefkowitz maneuver; sedation.
INTRODUCTION
Traumatic bilateral anterior dislocation of the hip joints is a rare condition. In 1951, Thompson and Epstein surveyed two hundred and four cases of hip dislocations over a period of twenty-one years and found only eighteen (9%) anterior dislocations, none bilateral.[1] As with other types of dislo-cations, prompt reduction of the hip joint is crucial to pre-vent potential complications of a delayed reduction, such as avascular necrosis of the femoral head. A case of traumatic bilateral anterior hip dislocations reduced successfully under sedation using intravenous Midazolam and Pethidine with a modified Lefkowitz maneuver was reported in this study.
CASE REPORT
The patient, a 47-year-old man, was knocked down from the back by a moving vehicle while standing behind a stationary car. Prior to the accident, he lost control of his car and skid-ded, and crash into a road divider. He was trying to inspect the car damage when he was knocked down from the back. He was unable to remember what happened from the time of the accident until he awoke in the emergency department. He complained about bilateral hip pain and inability to move both his hips.
Clinical assessment revealed tenderness over both of the patient’s hips. Patient resisted moving his hips due to pain. The hip joints were held in a flexed, abducted and external rotated position (Fig. 1a). Radiograph of the pelvis showed anterior dislocation of both his hip joints (Fig. 1c). The pa-tient also sustained a displaced fracture of the right medial malleolus and a Lisfranc fracture of the left foot.
A closed reduction was planned to be carried out under se-dation and analgesia in the ward, which was carried out in less than six hours from time of injury. Five milligrams of in-travenous Midazolam in 1mg/ml dilution in a 10mls syringe
Address for correspondence: Chee Kidd Chiu, M.D.
Department of Orthopaedic Surgery, Faculty of Medicine,
University of Malaya, 50603 Kuala Lumpur, Malaysia
Tel: +60 379492446 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):63-67doi: 10.5505/tjtes.2015.27475
Copyright 2015TJTES
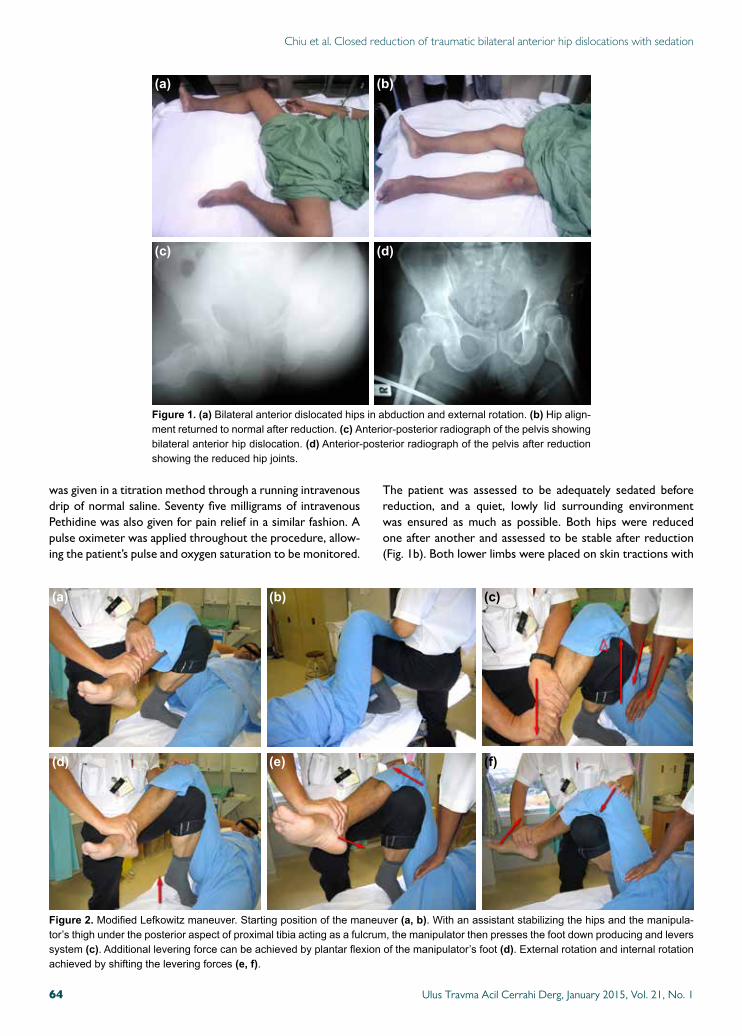
Chiu et al. Closed reduction of traumatic bilateral anterior hip dislocations with sedation
was given in a titration method through a running intravenous drip of normal saline. Seventy five milligrams of intravenous Pethidine was also given for pain relief in a similar fashion. A pulse oximeter was applied throughout the procedure, allow-ing the patient’s pulse and oxygen saturation to be monitored.
The patient was assessed to be adequately sedated before reduction, and a quiet, lowly lid surrounding environment was ensured as much as possible. Both hips were reduced one after another and assessed to be stable after reduction (Fig. 1b). Both lower limbs were placed on skin tractions with
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 164
Figure 2. ModifiedLefkowitzmaneuver.Startingpositionofthemaneuver(a, b).Withanassistantstabilizingthehipsandthemanipula-tor’sthighundertheposterioraspectofproximaltibiaactingasafulcrum,themanipulatorthenpressesthefootdownproducingandleverssystem(c).Additionalleveringforcecanbeachievedbyplantarflexionofthemanipulator’sfoot(d).Externalrotationandinternalrotationachievedbyshiftingtheleveringforces(e, f).
(a)
(d)
(b)
(e)
(c)
(f)
Figure 1. (a)Bilateralanteriordislocatedhipsinabductionandexternalrotation.(b)Hipalign-mentreturnedtonormalafterreduction.(c) Anterior-posteriorradiographofthepelvisshowingbilateralanteriorhipdislocation.(d)Anterior-posteriorradiographofthepelvisafterreductionshowingthereducedhipjoints.
(a)
(c)
(b)
(d)
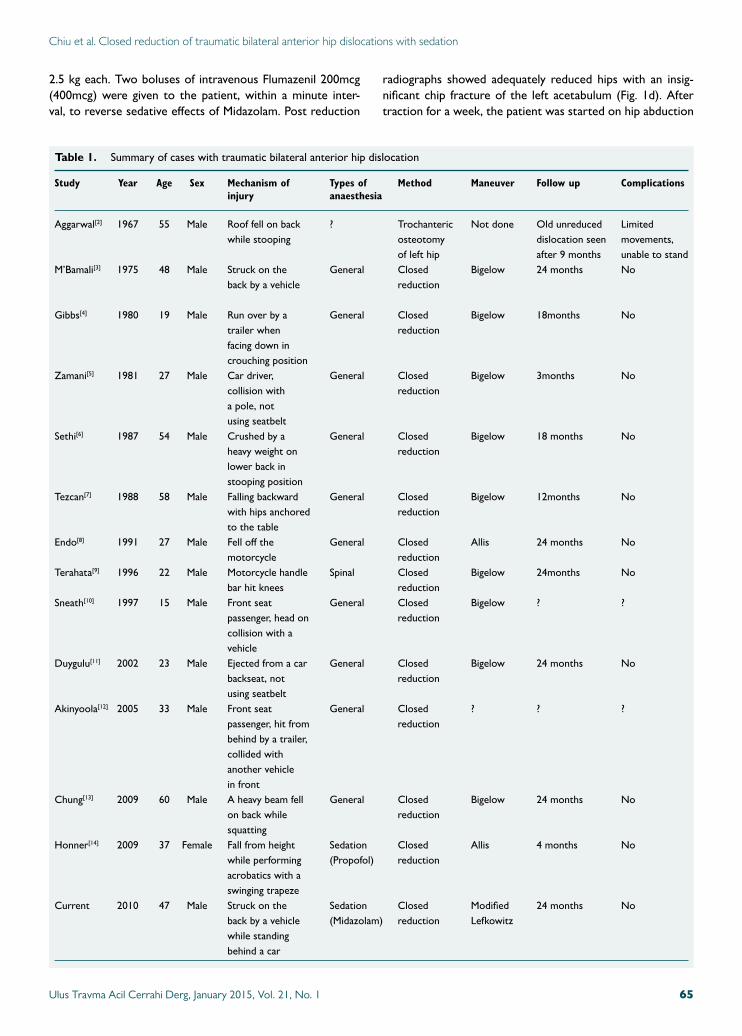
Chiu et al. Closed reduction of traumatic bilateral anterior hip dislocations with sedation
2.5 kg each. Two boluses of intravenous Flumazenil 200mcg (400mcg) were given to the patient, within a minute inter-val, to reverse sedative effects of Midazolam. Post reduction
radiographs showed adequately reduced hips with an insig-nificant chip fracture of the left acetabulum (Fig. 1d). After traction for a week, the patient was started on hip abduction
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 65
Table 1. Summary of cases with traumatic bilateral anterior hip dislocation
Study Year Age Sex Mechanism of Types of Method Maneuver Follow up Complications injury anaesthesia
Aggarwal[2] 1967 55 Male Roof fell on back ? Trochanteric Not done Old unreduced Limited while stooping osteotomy dislocation seen movements, of left hip after 9 months unable to standM’Bamali[3] 1975 48 Male Struck on the General Closed Bigelow 24 months No back by a vehicle reduction Gibbs[4] 1980 19 Male Run over by a General Closed Bigelow 18months No trailer when reduction facing down in crouching positionZamani[5] 1981 27 Male Car driver, General Closed Bigelow 3months No collision with reduction a pole, not using seatbeltSethi[6] 1987 54 Male Crushed by a General Closed Bigelow 18 months No heavy weight on reduction lower back in stooping positionTezcan[7] 1988 58 Male Falling backward General Closed Bigelow 12months No with hips anchored reduction to the table Endo[8] 1991 27 Male Fell off the General Closed Allis 24 months No motorcycle reductionTerahata[9] 1996 22 Male Motorcycle handle Spinal Closed Bigelow 24months No bar hit knees reductionSneath[10] 1997 15 Male Front seat General Closed Bigelow ? ? passenger, head on reduction collision with a vehicleDuygulu[11] 2002 23 Male Ejected from a car General Closed Bigelow 24 months No backseat, not reduction using seatbelt Akinyoola[12] 2005 33 Male Front seat General Closed ? ? ? passenger, hit from reduction behind by a trailer, collided with another vehicle in frontChung[13] 2009 60 Male A heavy beam fell General Closed Bigelow 24 months No on back while reduction squattingHonner[14] 2009 37 Female Fall from height Sedation Closed Allis 4 months No while performing (Propofol) reduction acrobatics with a swinging trapezeCurrent 2010 47 Male Struck on the Sedation Closed Modified 24 months No back by a vehicle (Midazolam) reduction Lefkowitz while standing behind a car

Chiu et al. Closed reduction of traumatic bilateral anterior hip dislocations with sedation
and exercises. He was discharged a week later and was asked to ambulate with a wheelchair for another six weeks. At the twelfth and twenty-fourth follow-up after the injury, he was walking without any hip pain.
Literature ReviewA search was performed on MEDLINE from January 1966 to December 2012, aiming to identify all publications reporting traumatic bilateral anterior hip dislocation. Key words used were “traumatic”, “bilateral”, “anterior” and “hip disloca-tion”. Sixteen reports were found in which thirteen were in English[2-14] (Table 1).
DISCUSSION
Hip dislocations are frequently encountered in an accident and emergency department. Prompt reduction of the hip is desirable as it has been documented to reduce potential long term complications of hip dislocations, such as avascular ne-crosis of the femoral head.
Reduction of the hip joint can be done under sedation or gen-eral anaesthesia. Our review showed that general anaesthesia was mostly preferred since it can provide substantial pain re-lief and good muscle relaxation. However, general anaesthesia preparation may lead to a delay for the reduction procedure. In patients with risk factors for general anaesthesia, the delay may occur during work-up and optimization of the patient. In some centres, especially in less-developed countries, al-location for general anaesthesia is limited and a delay may be unavoidable while waiting for its availability. In addition, patients with pre-existing medical conditions may be exposed to anaesthetic risks and complications.
The use of intravenous sedation in reduction of the hip is a good alternative for general anaesthesia. Intravenous sedation can easily be administered bedside at the accident and emer-gency room or in the ward. If titrated well, it can provide a level of sedation adequate for procedures with mild muscle relaxation. The fear of using sedation for this procedure may arise from its lack of predictability of sedative duration and the incomplete muscle relaxation leading to a difficult reduc-tion and a failed procedure. In our review, only one author has reported the use of intravenous sedation to reduce the hip joints. Honner[14] has used intravenous Propofol to sedate the patient before reducing both anterior hip dislocations. In our center, Propofol is not freely available in the emergency department or in the wards. It was shown in our study that the reduction of bilateral anterior hip dislocation is possible using a cheaper and more available sedative agent.
Our review noted that most authors had used Bigelow ma-neuver to reduce hip joints. Two authors, Endo[8] and Hon-ner,[14] used the Allis maneuver. All early closed reductions were successful and none needed operation. An adapted ver-sion of thigh fulcrum maneuver described by Lefkowitz[15] was
used in our case to reduce the dislocated hip joints. With a fulcrum maneuver, a consistent and controlled force could be applied throughout the reduction procedure, preventing the risk of excessive stress to the hip joint which may lead to the impairment of femoral head blood supply and damage of the surface of the joint cartilage (Fig. 2). This is particularly useful if a potentially strong muscular resistance is anticipated during the reduction procedure, especially in a brawny man. All case reports in our review revealed good outcome on follow-up except for a patient reported by Aggarwal,[2] who neglected his hip dislocations for nine months. He developed limited hip movements preventing him from standing and a trochanteric osteotomy was done to improve his function. In our case, the patient was able to walk after two months and continued to walk without any pain at the twenty-fourth month follow-up after injury.
ConclusionClosed reduction of traumatic bilateral anterior hip disloca-tion can be done successfully under sedation using intrave-nous Midazolam with a modified Lefkowitz maneuver. Early reduction of hip dislocation will ensure a better long term outcome.
ConsentWritten informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for the review by the Editor-in-Chief of this journal.
Authors’ ContributionCKC performed the procedure, took care of the patient, col-lected the clinical data, and drafted the manuscript. TSN as-sisted in collecting the clinical data and drafting of the manu-script. NNW and BAK revised the manuscript. All authors read and approved the final manuscript.
Competing InterestThe authors declare that they have no competing interests.
REFERENCES1. Thompson VP, Epstein HC Traumatic dislocation of the hip; a survey of
two hundred and four cases covering a period of twenty-one years. J Bone Joint Surg Am 1951;33-A:746-78.
2. Aggarwal ND, Singh H. Unreduced anterior dislocation of the hip. Re-port of seven cases. J Bone Joint Surg Br 1967;49:288-92.
3. M’Bamali EI. Unusual traumatic anterior dislocation of the hip. Injury 1975;6:220-4.
4. Gibbs A. Bilateral obturator dislocation of the hip joint. Injury 1980;12:250-1.
5. Zamani MH, Saltzman DI. Bilateral traumatic anterior dislocation of the hip: case report. Clin Orthop Relat Res 1981;161:203-6.
6. Sethi TS, Mam MK, Kakroo RK. Bilateral traumatic anterior dislocation of the hip. J Trauma 1987;27:573-4.
7. Tezcan R, Erginer R, Babacan M. Bilateral traumatic anterior dislocation
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 166

Chiu et al. Closed reduction of traumatic bilateral anterior hip dislocations with sedation
of the hip: brief report. J Bone Joint Surg Br 1988;70:148-9.8. Endo S, Hoshi S, Takayama H, Kan E. Traumatic bilateral obturator dis-
location of the hip joint. Injury 1991;22:232-3.9. Terahata N, Matsui H, Makiyama N. Bilateral anterior dislocation of the
hips. A case report. Int Orthop 1996;20:125-6.10. Sneath RJ, Morgan NP. Bilateral traumatic anterior dislocation of the hip
joint. J Accid Emerg Med 1997;14:391.11. Duygulu F, Karaoglu S, Kabak S, Karahan OI. Bilateral obturator dislo-
cation of the hip. Arch Orthop Trauma Surg 2003;123:36-8.
12. Akinyoola AL, Abiodun AA. Bilateral traumatic anterior hip dislocation-a case report. West Afr J Med 2005;24:272-3.
13. Chung KJ, Eom SW, Noh KC, Kim HK, Hwang JH, Yoon HS, et al. Bi-lateral traumatic anterior dislocation of the hip with an unstable lumbar burst fracture. Clin Orthop Surg 2009;1:114-7.
14. Honner S, Taylor SM. Bilateral anterior traumatic hip dislocation. J Emerg Med 2012;42:306-8.
15. Lefkowitz M. A new method for reduction of hip dislocations. Orthop Rev 1993;22:253-6.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 67
OLGU SUNUMU - ÖZET
Travmatik çift taraflı anterior kalça çıkıklarında sedasyon ile kapalı redüksiyon:Bir olgu sunumu ve literatürün gözden geçirilmesiDr. Chee Kidd Chiu,1 Dr. Tiong Soon Ng,2 Dr. Nayyer Naveed Wazir,3 Dr. Kareem Abdul Bhurhanudeen3
1MalayaÜniversitesiTıpFakültesi,OrtopedikCerrahiAnabilimDalı,KualaLumpur,Malezya;2TuankuJaafarHastanesi,OrtopedikCerrahiKliniği,Malezya;3UluslararasıUluslararasıTıpÜniversitesi,OrtopedikCerrahiAnabilimDalı,Malezya
Sedasyon altında redükte edilmiş nadir bir çift taraflı anteriyor kalça çıkığı olgusunu sunuyoruz. Kırk yedi yaşındaki erkek bir araç tarafından çarpılıp yere düşürüldü. Petidinle kombine titre edilmiş intravenöz midazolam dozuyla birlikte petidin kullanarak sedasyon altında çift taraflı anteriyor kalça kırığını başarıyla redükte ettik. Manipülasyon yapanın uyluğunu bir dayanak noktası olarak kullanıp modifiye Lefkowitz manevrası uyguladık. Hasta travmadan iki ay sonra yük bindirmeye başladı. Yirmi dört ay sonra ise kalça ağrısı olmaksızın yürüyordu. Literatür gözden geçirildiğinde 12 adet çift taraflı anteriyor kırığı olgu sunumu saptadık. Yalnızca bir yazar redüksiyon işlemi için intravenöz sedasyon (propofol) kullandığını bildirmişti. Hiçbir yazar bu amaçla Lefkowitz manevrası kullandığını bildirmemişti. Sonuçta, modifiye Lefkowitz manevrasını kullanarak sedasyon altında çift taraflı anterior kalça çıkığının redüksiyonu mümkündür.Anahtar sözcükler: Çift taraflı anteriyor kalça çıkığı; modifiye Lefkowitz manevrası; sedasyon.
Ulus Travma Acil Cerrahi Derg 2015;21(1):63-67 doi: 10.5505/tjtes.2015.27475

Carotid blowout syndromeYung-Shang Lin, M.D.,1 Chia-Ti Wang, M.D.,2 Yen Ting Chen, M.D.,2 Kuo-Tai Chen, M.D.3
1DepartmentofNeurosurgery,Yuan’sGeneralHospital,Kaohsiung;2DepartmentofEmergency,Chi-meiMedicalCenter,Tainan;3DepartmentofEmergencyMedicine,TaipeiMedicalUniversity,Taipei
ABSTRACT
Carotid blowout syndrome refers to the rupture of the carotid artery and its branches. Carotid blowout syndrome is a dangerous medical emergency typically resulting from complications of treatments for head and neck cancer. A patient without a prior history of head or neck cancer presented to the emergency department with a painless, enlarging neck mass was reported in this study. The mass progressed to acute airway obstruction during imaging of the lesion and necessitated emergency cricothyrotomy to secure the airway. The patient underwent four endovascular treatments to manage repeated bleeding thus producing the neurological complica-tion of right middle cerebral artery infarction. Clinical manifestations, varied treatments, and common complications of carotid blowout syndrome were discussed.
Key words: Carotid blowout syndrome; difficult airway; emergency cricothyrotomy.
INTRODUCTION
Carotid blowout syndrome (CBS) refers to the rupture of the carotid artery or one of its major branches and is a rare, devastating medical emergency.[1-4] The majority of CBS cases are complications of therapies for head and neck cancers and physicians are aware of the development of the disease.
Herein, a case of CBS was reported in a patient without a history of cancer or prior treatments on the head or neck regions. The patient presented with a rapidly enlarging neck mass progressing to acute airway obstruction which required emergency airway management.
CASE REPORT
A 60-year-old man found an enlarging lump on the right side of his neck and came to the emergency department one hour later. The lump was painless and did not influence his ability
to eat or breath or his articulation. The patient denied any systemic disease but reported that he had undergone gastric surgery several years ago. Additionally, he could not recall any events of trauma, fever, or upper respiratory tract infection symptom within the previous month. At the time of arrival, his vital signs were as follows: body temperature, 36.8°C; pulse, 107 beats/min; respiratory rate, 19/min; and blood pressure, 174/134 mmHg. Physical examination revealed a soft, non-movable and non-tender round mass on the right side of the patient’s neck.
The emergency physician arranged a computed tomography scan of the neck, which revealed a pseudo-aneurysm of the right internal carotid artery (Fig. 1). Soon after the comple-tion of the scan, the patient experienced dyspnea and lost consciousness. The physician performed an emergency cri-cothyroidotomy to secure the patient’s airway. A subsequent following angiography confirmed the presence of a pseudo-an-eurysm of the right internal carotid artery, which was treated via embolization of right internal carotid artery (Fig. 2).
Additionally, the radiologist identified an osteolytic lesion in the patient’s right middle skull base suspected to be a na-sopharyngeal carcinoma. Unfortunately, recurrent bleeding in the neck and oropharyngeal regions was observed one day, ten days, and twenty-three days after the first angiographic embolization attempt, and the patient underwent repeated embolization of the branches of the right internal carotid artery, right occipital artery, and right ascending pharyngeal
C A S E R E P O R T
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 168
Address for correspondence: Yen Ting Chen, M.D.
2f, No. 16, North District, Yude 1st Road 704 Tainan, Taiwan
Tel: +886987509108 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):68-70doi: 10.5505/tjtes.2015.76992
Copyright 2015TJTES
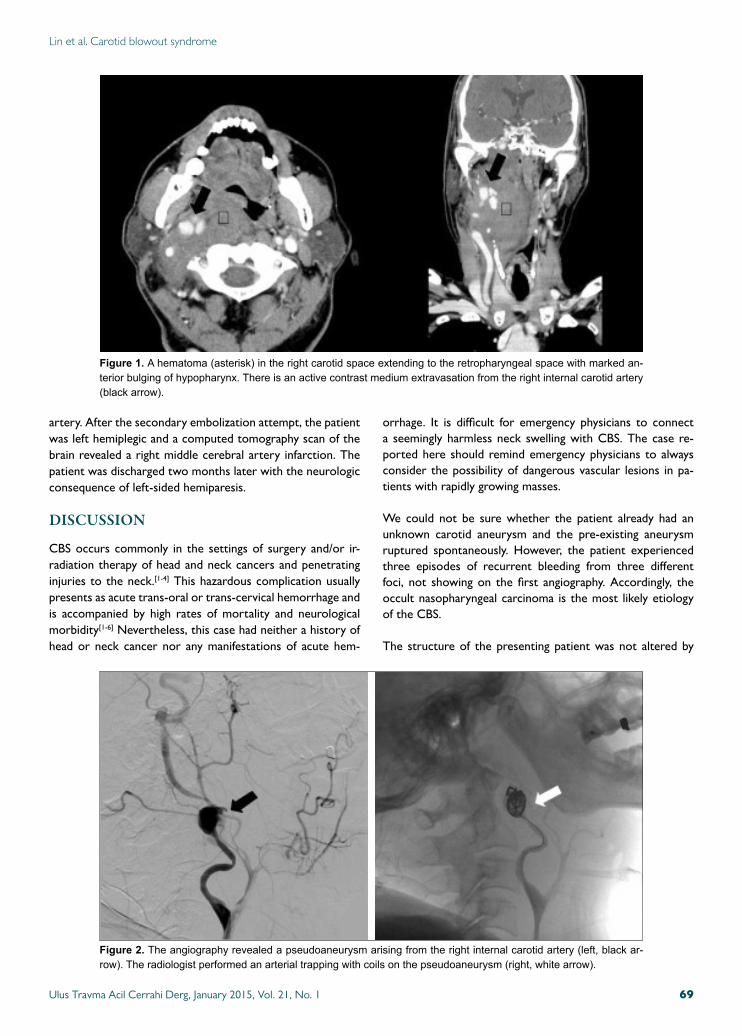
Lin et al. Carotid blowout syndrome
artery. After the secondary embolization attempt, the patient was left hemiplegic and a computed tomography scan of the brain revealed a right middle cerebral artery infarction. The patient was discharged two months later with the neurologic consequence of left-sided hemiparesis.
DISCUSSION
CBS occurs commonly in the settings of surgery and/or ir-radiation therapy of head and neck cancers and penetrating injuries to the neck.[1-4] This hazardous complication usually presents as acute trans-oral or trans-cervical hemorrhage and is accompanied by high rates of mortality and neurological morbidity[1-6] Nevertheless, this case had neither a history of head or neck cancer nor any manifestations of acute hem-
orrhage. It is difficult for emergency physicians to connect a seemingly harmless neck swelling with CBS. The case re-ported here should remind emergency physicians to always consider the possibility of dangerous vascular lesions in pa-tients with rapidly growing masses.
We could not be sure whether the patient already had an unknown carotid aneurysm and the pre-existing aneurysm ruptured spontaneously. However, the patient experienced three episodes of recurrent bleeding from three different foci, not showing on the first angiography. Accordingly, the occult nasopharyngeal carcinoma is the most likely etiology of the CBS.
The structure of the presenting patient was not altered by
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 69
Figure 1. Ahematoma(asterisk)intherightcarotidspaceextendingtotheretropharyngealspacewithmarkedan-teriorbulgingofhypopharynx.Thereisanactivecontrastmediumextravasationfromtherightinternalcarotidartery(blackarrow).
Figure 2. Theangiographyrevealedapseudoaneurysmarisingfromtherightinternalcarotidartery(left,blackar-row).Theradiologistperformedanarterialtrappingwithcoilsonthepseudoaneurysm(right,whitearrow).

Lin et al. Carotid blowout syndrome
prior cancer or trauma therapy. The intact skin presumably limited the outward expansion of the hematoma. The enlarg-ing neck hematoma, resulted from a pseudo-aneurysm of the carotid artery, likely extended rapidly inward to occlude the oropharynx or the trachea. Therefore, once a CBS is recog-nized, it is crucial to first secure the airway and then perform surgical or endovascular management of the CBS.
Surgical ligation of the common carotid artery or internal carotid artery is the traditional treatment for CBS. However, this approach is accompanied by unacceptably high rates of neurological complications and mortality.[5-7] The high mor-bidity and mortality rates of this treatment are attributable to the following factors. First, the surgical exploration of a field with previous irradiation and operation is technically dif-ficult. Second, without pre-surgical evaluation of the intra-cranial collateral circulation, surgical ligation of the carotid artery often results in thromboembolic events. Finally, CBS often causes massive hemorrhages leading to hypovolemia and the depletion of coagulation factors. Global cerebral isch-emia and uncontrolled re-bleeding can be encountered during the subsequent operation and increase the surgical risk.
Endovascular management with either permanent occlusion or stent deployment has become a practical alternative to surgical treatment. Two case series from Hong Kong and Taiwan have reported that immediate hemostasis is achieved in all cases.[3,4] Cerebral ischemia has been found in 15-20% of the patients with CBS treated with permanent occlusion.[4,7] Some authors advocate the examination of the availability of collateral circulation with the balloon occlusion test to identify patients with a high risk of stroke after endovascular management. However, this test is not usually possible in patients with acute massive hemorrhage and a small subset of cases develop cerebral ischemia despite the completion of balloon occlusion test.[1,4] Additionally, a significant por-tion of patients undergoing endovascular management of CBS exhibit delayed complications that include re-bleeding, thromboembolic events, stent migration, and intracranial in-fection.[1,3,4]
After the establishment of a patent airway and treatment for CBS, emergency physicians or neurosurgeons should look for occult lesions in the head and neck region. Since the major-ity of CBS cases result from the sequelae of head and neck cancer, meticulous studies of the underlying etiology are im-portant for further therapeutic planning.
ConclusionAlthough rare, CBS can occur in patients without histories of head and neck cancer or prior irradiation or surgical therapy on the neck. The disease may lead to acute airway obstruc-tion, necessitating emergency airway intervention. Surgical or endovascular managements are available as treatments for CBS; however, both treatments are accompanied by signifi-cant mortality and neurologic complications.
Conflict of interest: None declared.
REFERENCES1. Chaloupka JC, Roth TC, Putman CM, Mitra S, Ross DA, Lowlicht RA,
et al. Recurrent carotid blowout syndrome: diagnostic and therapeutic challenges in a newly recognized subgroup of patients. AJNR Am J Neu-roradiol 1999;20:1069-77.
2. Chang FC, Lirng JF, Luo CB, Guo WY, Teng MM, Tai SK, et al. Carotid blowout syndrome in patients with head-and-neck cancers: reconstruc-tive management by self-expandable stent-grafts. AJNR Am J Neurora-diol 2007;28:181-8.
3. Chaloupka JC, Putman CM, Citardi MJ, Ross DA, Sasaki CT. Endovas-cular therapy for the carotid blowout syndrome in head and neck surgical patients: diagnostic and managerial considerations. AJNR Am J Neuro-radiol 1996;17:843-52.
4. Wan WS, Lai V, Lau HY, Wong YC, Poon WL, Tan CB. Endovascular treatment paradigm of carotid blowout syndrome: review of 8-years ex-perience. Eur J Radiol 2013;82:95-9.
5. Razack MS, Sako K. Carotid artery hemorrhage and ligation in head and neck cancer. J Surg Oncol 1982;19:189-92.
6. Porto DP, Adams GL, Foster C. Emergency management of carotid ar-tery rupture. Am J Otolaryngol 1986;7:213-7.
7. Verhaeghe JL, Montagne S, Belotzerkovski I, Bracard S, Henneton C, Lapeyre M, et al. Is carotid resection a valuable option in advanced head and neck squamous cell carcinomas. [Article in French] Bull Cancer 2003;90:607-13. [Abstract]
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 170
OLGU SUNUMU - ÖZET
Karotis patlama sendromuDr. Yung-Shang Lin,1 Dr. Chia-Ti Wang,2 Dr. Yen Ting Chen,2 Dr. Kuo-Tai Chen3
1YuanGenelHastanesi,BeyinCerrahisiKliniği,Kaohsiung;2Chi-meiTıpMerkezi,AcilTıpKliniği,Tainan;3TaipeiTıpÜniversitesi,AcilTıpAnabilimDalı,Taipei
Karotis patlama sendromu karotis arter ve dallarının yırtılmasına işaret eder. Karotis patlaması sendromu tipik olarak baş veya boyun kanserleri için uygulanan tedavilerin komplikasyonları sonucu oluşan tehlikeli bir tıbbi acildir. Daha önce baş veya boyun kanseri öyküsü olmayan ve acil servise ağrısız büyümüş bir boyun kitlesiyle gelen bir hastayı raporluyoruz. Lezyonun görüntülenmesi sırasında kitle büyüyerek akut hava yolu tıkanmasına neden olmuş ve hava yolunu korumak için acil krikotirotomi gerekmiştir. Hastanın yinelenen kanamalarını kontrol altına almak için dört kez endovas-küler tedavi uygulanmış ve bu tedavi sağ orta serebral arter infarktına bağlı nörolojik komplikasyona neden olmuştur. Karotis patlama sendromunun klinik belirtileri, değişik tedavilerini ve sık görülen komplikasyonlarını tartıştık.Anahtar sözcükler: Acil krikotirotomki; karotis patlama sendromu; sorunlu hava yolu.
Ulus Travma Acil Cerrahi Derg 2015;21(1):68-70 doi: 10.5505/tjtes.2015.76992

The care of a patient with Fournier’s gangreneEsma Özşaker, Asst. Prof.,1 Meryem Yavuz, Prof.,1 Yasemin Altınbaş, MSc.,1
Burçak Şahin Köze, MSc.,1 Birgül Nurülke, MSc.2
C A S E R E P O R T
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 71
1DepartmentofSurgicalNursing,EgeUniversityFacultyofNursing,Izmir;2DepartmentofUrology,EgeUniversityFacultyofMedicineHospital,Izmir
ABSTRACT
Fournier’s gangrene is a rare, necrotizing fasciitis of the genitals and perineum caused by a mixture of aerobic and anaerobic microor-ganisms. This infection leads to complications including multiple organ failure and death. Due to the aggressive nature of this condition, early diagnosis is crucial. Treatment involves extensive soft tissue debridement and broad-spectrum antibiotics. Despite appropriate therapy, mortality is high. This case report aimed to present nursing approaches towards an elderly male patient referred to the urology service with a diagnosis of Fournier’s gangrene.
Key words: Case report; Fournier’s gangrene; nursing diagnosis; patient care.
INTRODUCTION
Rarely observed in the peritoneum, genital and perianal re-gions, necrotizing fasciitis is named as Fournier’s gangrene.[1-5] It is an important disease, following an extremely insidious beginning and causing necrosis of the scrotum and penis by advancing rapidly within one-two days.[1] The rate of mortal-ity in the literature is between 4 and 75%[6] and it has been reported that advanced age and delay in diagnosis and treat-ment of the condition increase the rate of mortality.[3,4,6] The disease is observed more frequently in men than in women at a ratio of 10:1 and the frequency of occurrence gradually increases between 50 and 60 years of age.[1,4,6]
In terms of etiology, it is a polymicrobial disease. Gram nega-tive bacteria, gram positive bacteria, anaerobics, and fungi can be the causes of the disease.[3,6] Even though the disease can appear with symptoms such as necrosis, pain, erythema, dis-charge, sensitivity, swelling, redness, and crepitation in the
perineal and genital regions, it is observed in a majority of cases with general symptoms, such as fever related infection and weakness, and without symptoms in the perineal region, negatively influencing the prognosis by causing a delay in diag-nosis and treatment.[2,3] Consequently, anamnesis and physical examination are extremely important. A very careful exami-nation of the peritoneum in patients with general symptoms of infection, such as fever and weakness, is important for the diagnosis of Fournier’s gangrene and the start of the treat-ment on time.[4] Hypocalcemia is also a significant finding in early diagnosis. Diagnosis is made with CT and MR imaging, subcutaneous, dermis, fascia and muscle biopsies, and surgical drainage. Imaging techniques are also used during follow-up after surgery.[3,4] The foundation of treatment consists the de-bridement of necrotic tissues, along with aggressive surgical intervention and broad-spectrum antibiotics.[1,4]
The role of the nurse in the care of patients with Fournier’s gangrene is to plan and implement suitable care of the pa-tient,[2] and educate the patient and family on the seriousness of the disease. Nurses should be sensitive towards their pa-tients since their body image may change.[6]
The objective of this case study was to emphasize the impor-tance of suitable care for Fournier’s gangrene, which occurs rarely but has a high rate of mortality. Nursing care was given according to Gordon’s Functional Health Patterns model (1982) and the North American Nursing Diagnosis Associa-tion (NANDA).
Address for correspondence: Esma Özşaker, Asst. Prof.
Ege Üniversitesi Hemşirelik Fakültesi, Cerrahi Hastalıkları
Hemşireliği Anabilim Dalı, Bornova, 35100 İzmir, Turkey
Tel: +90 232 - 311 56 23 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):71-74doi: 10.5505/tjtes.2015.22735
Copyright 2015TJTES

Özşaker et al. The care of a patient with Fournier’s gangrene
Ethical ConsiderationsThe objective of the case report was explained to the patient and a written consent was obtained. Patient name was not mentioned in the case report.
CASE REPORT
A 69-year-old male patient, married with three children, came to the emergency service of a university hospital with com-plaints of dyspnea, lack of appetite, difficulty in swallowing, weakness, fatigue, and jaundice and was admitted to the gas-troenterology clinic with cirrhosis of the liver. While receiv-ing treatment in the gastroenterology clinic, complaints of skin defects and discharge from the scrotum and perineum started, and the patient was diagnosed with Fournier’s gan-grene and referred to the urology clinic.
Physical examination of the patient in the clinic showed a fever of 36.0ºC, a pulse rate of 98/min., blood pressure of 140/100 mmHg, and a respiration rate of 26/min. The patient had complaints of dyspnea, lack of appetite, and weakness and was diagnosed with ineffective respiratory patterns and activity intolerance. Along with a height and weight of 1.75 cm and 120 kg, respectively, the Body Mass Index (BMI) of the patient was calculated as 39.1 (obese). Due to excessive weight, internal acid and Fournier’s gangrene, a diagnosis of breakdown in physical activity, risk of situational low self-es-teem, and nutrition exceeding body requirements was made. Laboratory findings of the patient were low for PLT (93 mm³), Hb (10.9 g/dl) and Htc (31.6%), but high for Gamma-GT (492 u/L), CRP (13.51) and FBG (133 mg/dL). It was found out that the patient had been consuming alcohol since the age of fifteen and had hypertension. There was a breakdown in health, which the patient connected to the use of alcohol, and lack of knowledge on the damaging effects of alcohol, and nursing interventions were applied. Anti-hypertension drugs, Cardopan Plus 2x1 and Amlodipin 1x1, and others including Pannet Tablet 1x1 as a stomach protector, Antiviral Zeflix 1x1, Hepamerz Granules 3x1 for liver treatment and the anti-biotics, Seftiriakson Sodium 1000 mg and Flacon + Ornidazol 500 mg injections were started in the clinic. These were given on time and vital findings were monitored regularly.
Patient was taken into an emergency operation in the clinic and an extensive debridement was made. After the proce-dure, infectious diseases physician started Tazocin for the patient. The width of the wound was 5 cm and the depth was 3-4 cm. Daily dressings were made with 4x1 Rivanol. On the twelfth day after surgery, the patient consulted a plastic surgeon and his dressings and antibiotic therapy continued. The patient had a re-consultation with the plastic surgeon on the twentieth day and daily dressings and Rivanol continued. Care and treatment of the patient continued under isolation conditions. The patient was evaluated for risk of situational low self-esteem connected to social isolation and the disease.The patient was anxious and tense and his level of anxiety
in relation to the treatment was high. He was informed on the issues he was anxious about throughout his treatment and inaccurate information was corrected. The patient could not go to the bathroom and a pad was used under him for his need for defecation, and a urinary catheter was attached for urinary evacuation and monitoring what he ingested and evacuated. Due to the fact that the place of the wound was close to the anus of the patient, he was monitored for risk of infection after extensive tissue debridement and the use of an intravenous/urinary catheter. Hyper-hydration was deter-mined in the follow-up of the 24-hour ingestion and evacua-tion of liquids by the patient. The patient’s skin was dry and there was +2 degrees edema in his lower extremities and acid was present internally. Nursing interventions were made for the risk of breakdown of skin integrity connected to an excessive volume of liquids and edema, a decrease in second-ary tissue nutrition/bleeding of acid, itching and anemia. An R2 diet (a liquid, soft diet) was implemented in the patient since he had an excessive volume of liquid and difficulty in swallowing hard and unsalted foods. The patient was moni-tored for risk of aspiration owing to difficulty in swallowing. Patient nutrition was followed closely as it is important to meet the nutritional needs of the body to provide for the re-granulation of tissues in patients on whom extensive tissue debridement has been made.
The patient experienced trembling during sleep, causing a breakdown in his sleep pattern. He could not fulfill his role as a father because of his treatment process and hospital stay and a breakdown in intra-family processes and caretaking role were considered. There was a breakdown in verbal commu-nication with lack of harmony between verbal and nonver-
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 172
Table 1. Nursing diagnosis
• Activity intolerance
• Anxiety
• Breakdown in physical activity
• Breakdown in the caretaking role
• Breakdown in the continuation of health
• Breakdown in the intra-family processes
• Breakdown in the pattern of sleep
• Breakdown in verbal communications
• Excessive volume of liquids
• Ineffective respiratory patterns
• Lack of knowledge
• Lack of self-care syndrome
• Nutrition exceeding body requirements
• Risk of aspiration
• Risk of breakdown of skin unity
• Risk of infection
• Risk of situational low self-esteem

Özşaker et al. The care of a patient with Fournier’s gangrene
bal communications connected to difficulty in speaking and pronouncing words. In terms of fulfilling daily activities, the patient was included into dependent patient category in the categories of standing, eating, walking and hygiene. In terms of general hygienic pattern, the patient had bad breath as he did not brush his teeth. He was given nursing care for lack of self-care syndrome. Table 1 shows nursing diagnosis for Gor-don’s Functional Health Patterns model and NANDA accord-ing to the findings obtained when the patient was evaluated for nursing care.
Treatment was planned in light of the findings obtained from the patient and was continued in an isolated room with a nursing care over a 28-day period covering the pre- and post-operative periods, and the patient was moved to the plastic surgery service on the twenty-eighth day to undergo a graft.
DISCUSSION
Even with the use of broad-spectrum antibiotics, aseptic and antiseptic conditions in the operating rooms, developed sur-gical techniques and intensive care conditions, Fournier’s gan-grene still exists in Turkey as a pathology with a high mortal-ity.[7] Generally, diagnosis is frequently made at a late period since patients with Fournier’s gangrene do not completely describe their complaints or permit a complete examination of the genital region due to embarrassment.
Early diagnosis, early radical surgical debridement/s, the use of suitable antibiotics, and when needed, long-term hemody-namic support is required to decrease the high rate of mor-tality in Fournier’s gangrene.[8] Dressing the wound debrid-ed surgically in a suitable manner,[7] meeting the nutritional requirements of the body for re-granulation of the tissues, monitoring the nutritional status of the patient, and giving supportive food supplements are all important.[6]
In spite of the fact that Fournier’s gangrene was first described as a gangrene of the penis and scrotum spreading rapidly in young male adults, it has been shown in the recent literature as occurring predominantly in cases of an advanced age and having predisposing factors.[4] In a study by Unalp et al. car-ried out in 2008 on patients with Fournier’s gangrene, it was determined that the average age of the patients was 54.7 and that 10% of the patients died. They found that the average age of the patients who died was 66.7, whereas the average age of the patients who survived was 53.3 and that the rate of mortality was higher in those who were 60 years of age and older.[8] It is stated in the literature that old age is not a predisposing factor; however, elderly patients with poor self-care and nutritional status are more susceptible to Fourni-er’s gangrene and the prognosis is worse in elderly patients.[9] Consequently, slightest complaints in the perineal, genital and perianal regions, especially in elderly patients, should be evaluated carefully.
Among the predisposing factors playing a role in the develop-ment of Fournier’s gangrene are poor perfusion, hyperten-sion, renal insufficiency, trauma, primary anorectal infections, diabetes mellitus, cirrhosis, malnutrition, immunosuppres-sion, cigarette smoking, alcohol, dependence on intravenous drugs, malignities, inadequate nutrition, morbid obesity, and spinal cord injuries.[1,2,4,8-10]
In this case study, the patient had been consuming alcohol for fifty-four years since the age of fifteen, had liver cirrhosis and a history of hypertension, and was excessively overweight (BMI: 39.1). Alcohol, cirrhosis, excessive overweight and hy-pertension in our case study suggested that these were pre-disposing factors for Fournier’s gangrene, as also suggested in the literature.
People receiving Fournier’s gangrene treatments are con-fronted with many serious concerns. When the medical team has made a diagnosis of a life-threatening condition and it is necessary for the patient to undergo a series of surgical interventions, including debridement, breakdowns in shape and function caused by extensive debridements can create anxiety in the person to varying degrees.[6] Consequently, it is necessary to keep the patient and family informed on the seriousness of the disease from the beginning. The patient and family can be directed to a psychologist to receive con-sultation for loss of body image, weakness, and feelings of change in family dynamics. Nurses/health personnel should be sensitive and aware of the feelings in the patient on the breakdown in their body image.[6] Patients should be encour-aged to discuss their feelings on the disease, the treatment and their self-conception. Wrong information, if any, should be corrected.
ConclusionFournier’s gangrene is a rarely occurring, life-threatening emergency situation and delays in its diagnosis and treatment increase the rate of mortality. In order to keep the patient alive, it is of critical importance to make a diagnosis as soon as possible, start broad-spectrum antibiotics, perform emer-gency surgical debridement, support the nutrition of the pa-tient, and carry out suitable wound care. Consequently, the smallest complaints in the perineal, genital and perianal re-gions, especially in elderly patients, should be evaluated with care. These complaints should be considered within the pre-diagnoses of Fournier’s gangrene and suitable care should be given to the patient.
Conflict of interest: None declared.
REFERENCES
1. Çelen MK, Uluğ M, Tekin R, Geyik MF, Ayaz C. Fetal Seyirli Fournier Gangreni: Bir Olgu Sunumu. ANKEM Derg 2008;22:39-41.
2. Soares RSA, Saul AR, Farão EMD, Lima SBS, Silva FS, Finger A. Nurs-ing care systematization for patient with Fournier syndrome. Available at
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 73

Özşaker et al. The care of a patient with Fournier’s gangrene
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 174
OLGU SUNUMU - ÖZET
Fournier gangrenli hastanın bakımıYrd. Doç. Dr. Esma Özşaker,1 Prof. Dr. Meryem Yavuz,1 Uzm. Hem. Yasemin Altınbaş,1
Uzm. Hem. Burçak Şahin Köze,1 Uzm. Hem. Birgül Nurülke2
1EgeÜniversitesiHemşirelikFakültesi,CerrahiHastalıklarıHemşireliğiAnabilimDalı,İzmir;2EgeÜniversitesiTıpFakültesiHastanesi,ÜrolojiAnabilimDalı,İzmir
Fournier gangreni genital bölgenin ve perinenin aerobik ve anaerobik bakterilere bağlı olarak gelişen ve nadir görülen nekrotizan fasiitidir. Bu enfek-siyon çoklu organ işlev bozukluğu ve ölüm gibi ciddi komplikasyonlara yol açmaktadır. Bu hastalığın agresif tedavisi için öncelikli olan tanının erken konmasıdır. Tedavideki asıl nokta, geniş doku debridmanı ile birlikte geniş spektrumlu antibiyoterapinin uygulanmasıdır. Tedaviye rağmen mortalite yüksek seyretmektedir. Bu olguda, Fournier gangreni tanısıyla üroloji servisine yatırılan yaşlı bir erkek hastaya yönelik hemşirelik yaklaşımları yer almaktadır.Anahtar sözcükler: Fournier gangreni; hasta bakımı; hemşirelik tanısı; olgu sunumu.
Ulus Travma Acil Cerrahi Derg 2015;21(1):71-74 doi: 10.5505/tjtes.2015.22735
November 15, 2012 http://www.unifra.br/eventos/jornadadeenferma-gem/Trabalhos/4190.pdf.
3. Sökmen S. Fournier gangreni. ANKEM Derg 2012;26(Ek 2):331-6.4. Sümer A, Onur E, Altınlı E, Çelik A, Senger S, Köksal N. Ateş etyolojisi
nedeni ile araştırılan hastalarda tanısı gecikmiş mortal bir neden: Fourni-er gangreni. Bakırköy Tıp Dergisi 2005;1:57-9.
5. Thwaini A, Khan A, Malik A, Cherian J, Barua J, Shergill I, et al. Fournier’s gangrene and its emergency management. Postgrad Med J 2006;82:516-9.
6. Champion SE. A case of Fournier’s gangrene. Urol Nurs 2007;27:296-9.
7. Şen Z, Yomruk E, Kaya B, Can Z, Serel S, Ersoy A. Fournier gangren-inde tedavi prensipleri. Ankara Üniversitesi Tıp Fakültesi Mecmuası 2003;56:249-58.
8. Unalp HR, Kamer E, Derici H, Atahan K, Balci U, Demirdoven C, et al. Fournier’s gangrene: evaluation of 68 patients and analysis of prognostic variables. J Postgrad Med 2008;54:102-5.
9. Neary E. A case of Fournier’s gangrene. Trinity student. Medical Journal 2005;6:68-73.
10. Akgün Y, Yilmaz G. Factors affecting mortality in Fournier’s gangrene. Ulus Travma Acil Cerrahi Derg 2005;11:49-57.
Late onset brachial artery thrombosis and totaltemporary peripheral neuropathy in a child withhumerus supracondylar fracture: a case reportTolga Ege, M.D.,1 Selim Türkkan, M.D.,2 Celalettin Günay, M.D.,3
Yalçın Külahçı, M.D.,2 Mustafa Kürklü, M.D.2
1DeparmentofOrthopedicsandTraumatolgy,GülhaneMilitaryMedicalAcademy,Ankara;2DeparmentofHandSurgery,GülhaneMilitaryMedicalAcademy,Ankara;3DeparmentofCardiovascularSurgery,GülhaneMilitaryMedicalAcademy,Ankara
ABSTRACT
Pediatric supracondylar fractures of the humerus are generally associated with neurovascular complications due to the deformity and sharp nature of bone fragments. When treated inadequately, these injuries may result in catastrophic complications, such as Volkmann’s contracture and amputation. To our knowledge, late onset brachial arterial thrombosis and total temporary peripheral neuropathy after surgery of pediatric supracondylar fracture in the setting of normal preoperative vascular examination has not been reported yet. In this study, a 2-year and 6- month-old girl, who had delayed brachial arterial thrombosis after a displaced humerus supracondylar frac-ture surgery treated with embolectomy, was reported. Total lesion of median, ulnar and radial nerves completely resolved four months after surgery. Close neurovascular monitoring on the postoperative phase especially in severely displaced supracondylar fractures is strongly emphasized even in the setting of well-perfused hand.
Key words: Brachial artery; supracondylar fracture; thrombosis.
INTRODUCTION
Vascular complications associated with pediatric humerus supracondylar fractures are still common problems despite much has been written about the incidence and their man-agement.[1] When managed inappropriately, these injuries may result in catastrophic complications, such as Volkmann’s con-tracture and amputations which are extremely rare situations an orthopedic surgeon may face once in his entire career. Vascular pathologies such as thrombosis, intimal tear, and rupture associated with bone fractures generally give symp-toms in the acute phase of the fracture. However, late on-
set arterial occlusion after bony fractures are extremely rare situations.[2-4] To our knowledge, there is no reported data in the literature consisting late onset vascular occlusion after surgical treatment of supracondylar fracture with preopera-tive and postoperative good palpable radial pulse.
CASE REPORT
A 2-year and 6-month old girl was admitted to our emer-gency department from another tertiary trauma center with severely displaced Gartland type-III supracondylar fracture. The fracture was due to a fall from 1.5 meter-high kitchen bench. The patient was consulted by an orthopedic surgeon at 3’ o clock in the morning and her parents stated that she ate just before being admitted to our emergency department (ED). On physical exam, there was large ecchymosis on the ante-cubital fossa with brachialis sign. Radial pulse was pal-pable and on motor neurologic exam, median nerve was in-tact; however, ulnar, radial, and anterior interosseous nerves were not evaluated optimally. On sensory exam, ulnar radial and median nerve distributions were intact. With palpation,
C A S E R E P O R T
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 75
Address for correspondence: Tolga Ege, M.D.
Gülhane Tıp Akademisi, Ortopedi ve Travmatoloji Kliniği,
Etlik, Ankara, Turkey
Tel: +90 312 - 304 55 01 E-mail: [email protected]
Qucik Response Code Ulus Travma Acil Cerrahi Derg2015;21(1):75-78doi: 10.5505/tjtes.2015.92072
Copyright 2015TJTES
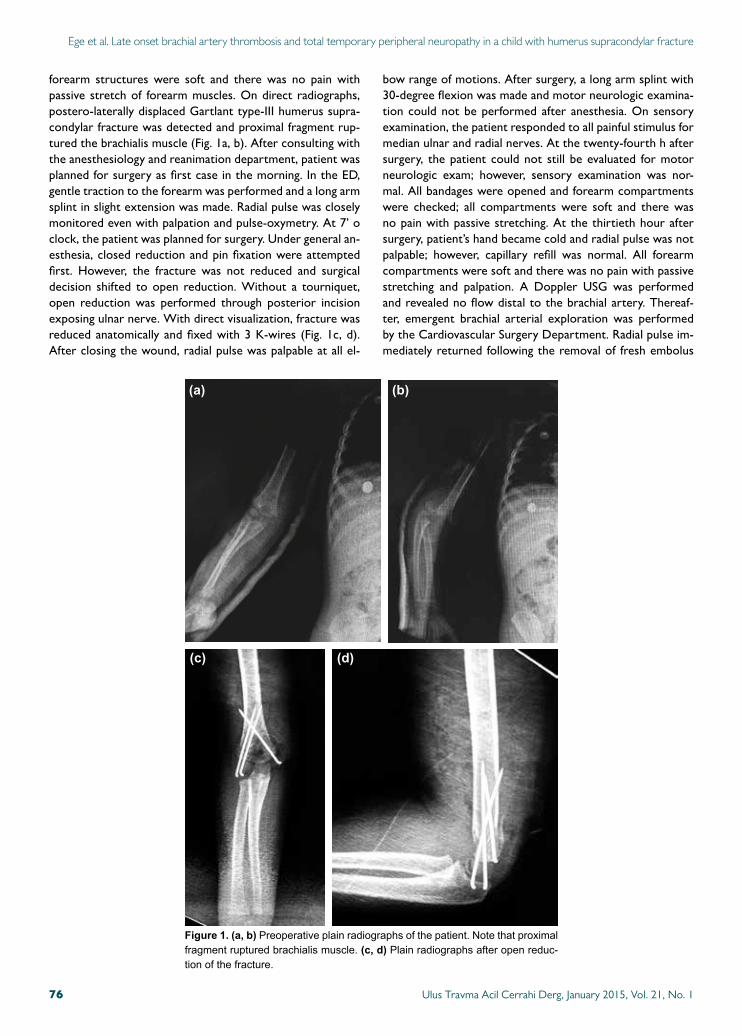
Ege et al. Late onset brachial artery thrombosis and total temporary peripheral neuropathy in a child with humerus supracondylar fracture
forearm structures were soft and there was no pain with passive stretch of forearm muscles. On direct radiographs, postero-laterally displaced Gartlant type-III humerus supra-condylar fracture was detected and proximal fragment rup-tured the brachialis muscle (Fig. 1a, b). After consulting with the anesthesiology and reanimation department, patient was planned for surgery as first case in the morning. In the ED, gentle traction to the forearm was performed and a long arm splint in slight extension was made. Radial pulse was closely monitored even with palpation and pulse-oxymetry. At 7’ o clock, the patient was planned for surgery. Under general an-esthesia, closed reduction and pin fixation were attempted first. However, the fracture was not reduced and surgical decision shifted to open reduction. Without a tourniquet, open reduction was performed through posterior incision exposing ulnar nerve. With direct visualization, fracture was reduced anatomically and fixed with 3 K-wires (Fig. 1c, d). After closing the wound, radial pulse was palpable at all el-
bow range of motions. After surgery, a long arm splint with 30-degree flexion was made and motor neurologic examina-tion could not be performed after anesthesia. On sensory examination, the patient responded to all painful stimulus for median ulnar and radial nerves. At the twenty-fourth h after surgery, the patient could not still be evaluated for motor neurologic exam; however, sensory examination was nor-mal. All bandages were opened and forearm compartments were checked; all compartments were soft and there was no pain with passive stretching. At the thirtieth hour after surgery, patient’s hand became cold and radial pulse was not palpable; however, capillary refill was normal. All forearm compartments were soft and there was no pain with passive stretching and palpation. A Doppler USG was performed and revealed no flow distal to the brachial artery. Thereaf-ter, emergent brachial arterial exploration was performed by the Cardiovascular Surgery Department. Radial pulse im-mediately returned following the removal of fresh embolus
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 176
Figure 1. (a, b) Preoperativeplainradiographsofthepatient.Notethatproximalfragmentrupturedbrachialismuscle.(c, d) Plainradiographsafteropenreduc-tionofthefracture.
(a) (b)
(c) (d)

Ege et al. Late onset brachial artery thrombosis and total temporary peripheral neuropathy in a child with humerus supracondylar fracture
with Fogarty catheter from the thrombosed segment (Fig. 2). After surgery, there was slight edema on the forearm region but compartments were soft. EMG study, performed on the third week after surgery, revealed total axonal de-generation on median, radial and ulnar nerves. Afterwards, aggressive physical therapy was started. On the thirtieth day after surgery, there was slight contracture on flexor muscles of second, third, fourth, and fifth digits. Static splint for the fingers and wrist was ordered. At the fifth week after the initial trauma, median and ulnar nerves began to heal. EMG study in the third month showed complete healing of radial nerve and partial axonal degeneration of medial and ulnar nerves. In the fourth month after surgery, all nerves healed without sensory deficit and motor loss and all of the con-tractures resolved completely. Patient revealed slight elbow flexion deficit in last 20 degrees.
DISCUSSION
Careful neurovascular examination must be the first step in the evaluation of a child with supracondylar fracture. How-ever, frightened child may cause a delay in detecting vascular pathologies in preoperative and even in postoperative phases. Vascular pathologies associated with supracondylar fractures may be classified into three types including first type, acute vascular occlusion; second type, sub-acute occlusion; and third type, Volkmann’s ischemia.[5] Fortunately, acute ischemic events are extremely low as the collateral circulation around elbow joint is good enough even in the case of brachial ar-tery rupture. Most authors indicate that non-palpable radial pulse with warm hand is not an indication for routine arterial exploration as most of the cases return to normal after re-duction and pinning of the fracture.[5,6] Absence of the pulse with palpation and by Doppler USG is important, meaning an arterial injury is probably present. At this situation, routine brachial arterial exploration must be considered.[7]
The other but rare cause of ischemia after supracondy-lar fracture is compartment syndrome which may result in Volkmann’s contracture and amputation when treated inad-
equately. Historically, it was generally due to casting after closed reduction and flexion of the elbow greater than 90 degrees. However, the incidence of compartment syndrome was diminished by routine closed reduction and percutane-ous pinning of the displaced supracondylar fractures. It gen-erally has 5P (pain, pallor, pulselessness, paresthesias, and paralysis) signs but the most obvious sign is pain out of pro-portion and pain with passive stretching of the wrist and fin-gers. However, pain can be masked in patients with median nerve lesion, which called silent compartment syndrome. Thus, in this group of patients, compartment pressures must be measured as soon as possible and early fasciatomies must be considered.
When the literature is reviewed, late onset vascular lesions associated with bony fractures are extremely rare and con-sist several cases.[2-4] The main reason in these cases is inti-mal tear after trauma of the artery by fractured bone frag-ments.[2,3] Copley et al.[1] have reported two cases with late onset brachial arterial occlusion after surgical treatment of displaced supracondylar fracture in their study. However, in these cases, radial pulses were diminished or absent before surgery. It is to our belief that our case was unique as the patient had good pulses before and after the reduction of the fracture. Thrombosis at the fracture site was thought to be due to intimal tear caused by sharp proximal fracture frag-ment. Therefore, thrombosis at the intimal tear site aroused gradually at postoperative phase. In our case, compartment syndrome, which may mask acute arterial occlusion, was not considered since all forearm compartments were checked with physical exam throughout the hospital stay. Further-more, patient’s sensation over median nerve distributions were normal as we ruled out silent compartment syndrome. Again, immediate return of pulses after embolectomy ruled out probable compartment syndrome. Additionally, our case had total neurologic deficit involving median, ulnar and radial nerves, which was extremely rare in this type of fracture, and completely resolved in the fourth month after surgery. It was probably due to traction injury resulting from severe displacement of the fractured bone fragments after the high fall and transient ischemic situation due to brachial artial oc-clusion.
We strongly emphasize that patients with severely displaced supracondylar fractures should be carefully monitorized for neurovascular status even at the postoperative phase. One should consider that acute compartment syndrome might in-terfere with acute arterial conclusion, and therefore, in case of suspicion, compartment pressures must be checked even with physical exam or invasive techniques. Good capillary refill does not exclude arterial occlusion or compartment syndrome. A routine follow-up for at least forty-eight hours after surgery must be preferred with severely displaced su-pracondylar fractures.
Conflict of interest: None declared.
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 1 77
Figure 2. Intraoperativeviewofthethrombosedbrachialartery.

Ege et al. Late onset brachial artery thrombosis and total temporary peripheral neuropathy in a child with humerus supracondylar fracture
Ulus Travma Acil Cerrahi Derg, January 2015, Vol. 21, No. 178
REFERENCES1. Copley LA, Dormans JP, Davidson RS. Vascular injuries and their se-
quelae in pediatric supracondylar humeral fractures: toward a goal of pre-vention. J Pediatr Orthop 1996;16:99-103.
2. Roper BA, Provan JL. Late thrombosis of the femoral artery complicating fracture of the femur. J Bone Joint Surg Br 1965;47:510-3.
3. Porter MF. Delayed arterial occlusion in limb injuries. Report of three cases. J Bone Joint Surg Br 1968;50:138-40.
4. Gallucci G, Ranalletta M, Gallucci J, De Carli P, Maignon G. Late onset of axillary artery thrombosis after a nondisplaced humeral neck fracture:
a case report. J Shoulder Elbow Surg 2007;16:e7-8. 5. Ramesh P, Avadhani A, Shetty AP, Dheenadhayalan J, Rajasekaran S.
Management of acute ‘pink pulseless’ hand in pediatric supracondylar fractures of the humerus. J Pediatr Orthop B 2011;20:124-8.
6. Matuszewski L. Evaluation and management of pulseless pink/pale hand syndrome coexisting with supracondylar fractures of the humerus in chil-dren. Eur J Orthop Surg Traumatol 2013 Oct 15.
7. Tomaszewski R, Gap A, Wozowicz A, Wysocka P. Analysis of early vas-cular and neurological complications of supracondylar humerus fractures in children. Pol Orthop Traumatol 2012;77:101-4.
OLGU SUNUMU - ÖZET
Pediatrik humerus suprakondiler kırıklı bir hastada geç gelişenbrakiyal arter trombozu ve total geçici sinir paralizisi: Olgu sunumuDr. Tolga Ege,1 Dr. Selim Türkkan,2 Dr. Celalettin Günay,3 Dr. Yalçın Külahçı,2 Dr. Mustafa Kürklü2
1GülhaneAskeriTıpAkademisi,OrtopediveTravmatolojiKliniği,Ankara;2GülhaneAskeriTıpAkademisi,ElCerrahisiKliniği,Ankara;3GülhaneAskeriTıpAkademisi,KalpDamarCerrahisiKliniği,Ankara
Çocukluk çağı humerus suprakondiler kırıkları hem kırıktan kaynaklanan deformite hem de kırık uçlarının keskin yapısı nedeni sıklıkla nörovasküler komplikasyonlara yol açmaktadır. Yeterli tedavi edilmedikleri takdirde Volkmann iskemik kontraktürü veya amputasyon gibi katastrofik kompli-kasyonlara yol açabilmektedirler. Bilgimize göre literatürde ameliyat öncesi dönemde normal nörovasküler muayenesi olup ameliyat sonrası geç dönemde brakiyal arter trombozu ile birlikte total sinir paralizisi henüz bildirilmemiştir. Çalışmamızda iki yaş altı aylık olan çocuk hastada kaymış humerus suprakondiler kırğının ameliyat sonrası döneminde gelişen brakiyial arter trombozunun embolektomi yapılarak tedavisini sunmayı amaç-ladık. Total median, ulnar ve radial sinir lezyonları, ameliyat sonrası dördüncü ayda tamamen düzeldi. Sonuç olarak, özellikle ciddi olarak kaymış pediatrik humerus suprakondiler kırıklarında ameliyat öncesi dönemde elin dolaşımı iyi olsa dahi, ameliyat sonrası dönemde nörovasküler inceleme yakınen yapılmalıdır.Anahtar sözcükler: Brakiyal arter trombozu; geç dönem; humerus; kırık; suprakondiler; total paralizi.
Ulus Travma Acil Cerrahi Derg 2015;21(1):75-78 doi: 10.5505/tjtes.2015.92072