transitional care pharmacist / medication therapy ...c.ymcdn.com/sites/ · transitional care...
TRANSCRIPT
Transitional Care Pharmacist / Medication Therapy Management
(MTM)
Mimi Nguyen. Pharm.D.
Sr. Director, Corporate Pharmacy
Scripps Health
Pharmacy
Transitions of Care
Scripps Health
• 5 Acute Care Hospital Campuses
– About 1400 beds
• 2 Medical Foundation Groups
– Scripps Medical Clinic
•12 + locations
– Scripps Coastal Medical Clinic
•8 + locations
• 2,600 affiliated physicians throughout all our facilities
Scripps Mission Statement
Current National Issues
Published Articles: – Institute of Medicine (IOM) reported that 1.5 million injuries per year
were caused by preventable prescription error, which cost $3.5 billion to manage them.
– World Health Organization (WHO) reported that only 50% of patients
with Chronic diseases adhere to medication therapy. Non-adherence cost health care $290 Billion annually due to disease progression, reduced functional status, lower quality of life, and premature death.
– New England Journal of Medicines (NEJM) states that 20% of Medicare
patients are readmitted within 30days and 34% within 90 days of discharge. Costing $17 billion annually. CMS to begin penalizing hospitals for excessive readmissions in FY2013.
– Annals of Internal Medicine, 2003 states that 20-30% of older patients suffer an adverse event within 30 days of discharge. Medication errors being the most prevalent and nearly half were believed to be preventable.
– Journal of Hospital Medicine and Archives of Internal Medicine states
discharge education were inadequate thus cause poor retention of instructions and inconsistent follow up on pending tests and non-compliance.
4
Accountable Care
• Requires coordination of care and communication across multiple providers, including pharmacist.
• Accountable for quality, cost and care
What are we doing about it?
Scripps Goals
• Reduce Hospital Readmissions
• Reduce Length of Stay
• Improve Patient Satisfaction
• Provide consistent care
• Safe transition across the continuum of care
OutptInptOutpt+/-SNF
Issues that we face
• Poor communication among healthcare professionals
• Incomplete and/or Inaccurate Medication Reconciliation
• Inadequate discharge education
• Preventable medication errors or adverse events
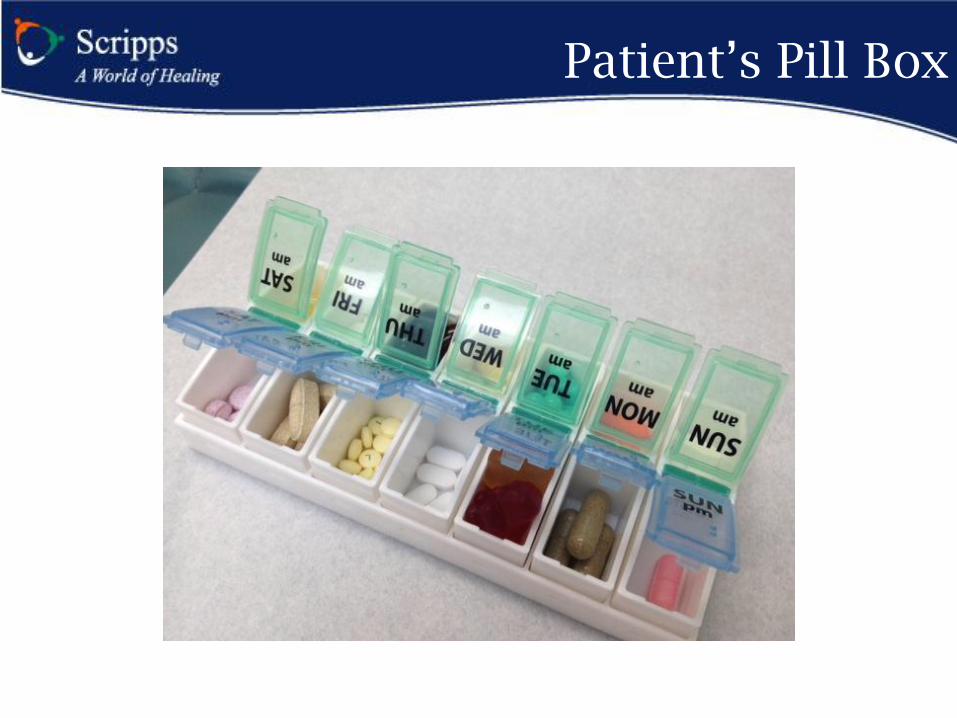
Patient’s Pill Box
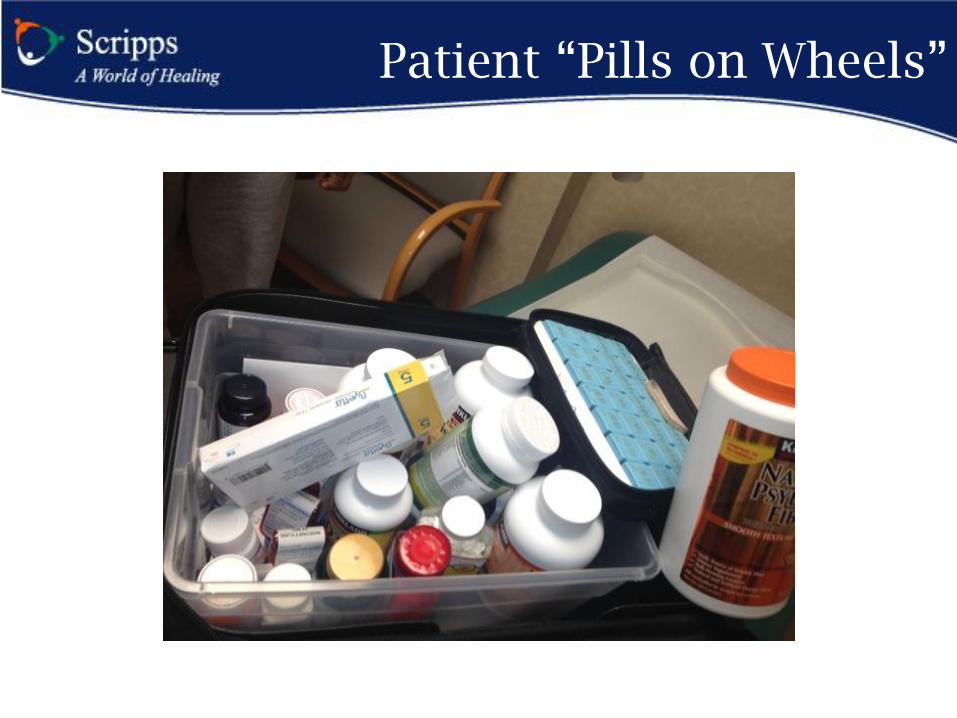
Patient “Pills on Wheels”
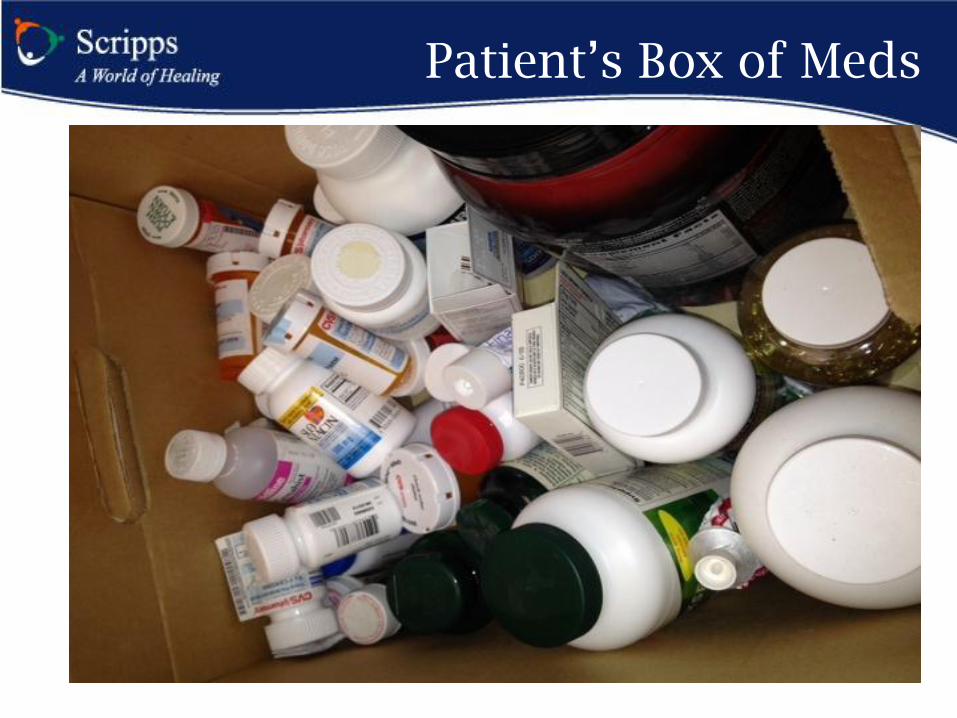
Patient’s Box of Meds
Case Study #1
• 76 y/o female with history of Chronic Kidney Disease, Hypertension, Transient Ischemic Attack. Referred to Pharmacist due to incomplete Admission Medication List
• What was discovered?
– Aggrenox were in a metoprolol bottle
– Pill box were filled three times daily for hydralazine, aggrenox and metoprol
– OTC aspirin was a 325mg tablet, instead of 81mg
• Patient complaints of headache
• Patient found to have ulcer during this stay
Case Study #2
• 89 year old man came in due to weakness caused by chronic diarrhea/constipation.
• Patient on 20 different prescription.
• When patient does not have a bowel movement, he takes 2 capsule of stool softener, a few doses of Milk of Magnesium, then escalates to a few enemas.
• Thus, causing diarrhea and bowel incontinence.
• He treats this with 4-5 capsules of Loperamide (imodium)
daily until he has constipation..
Transition Care Team
• Multi-Disciplinary Team
– Physicians – Hospitalist
– Navigators – Case Management
•Inpatient
•Outpatient
– Bedside Nurses
– Pharmacists
Patient Risk Stratification
•Diagnosis
•Capacity to manage their care as outpatient
•Ability to comprehend teach back
•Medication compliance
•Complexity of Drug Regimen
•Discharge location
Problem existing today around Medication Management
Academy of Managed Care Pharmacy 2011 • 32% of patients are hospitalized due to adverse
events
• 33-50% of patients are non compliant with chronic medications
• 58% of physicians complain that patients have difficulty affording medications
• Typical multi-chronic disease on average – see 13 physicians,
– fill 50 prescriptions,
– Account for 76% of hospitalization
– 100 times more likely to have a preventable hospitalization

Pharmacist’s Role
• Interdisciplinary bedside rounds
• Validate admission medication list reconciliation (AML)
• Review medication therapy for effectiveness, safety and compliance.
• Provide patient education on medications
• Assess barriers in patient compliance (financial, ADR, regimen, social)
• Create Medication Discharge planning
• 30 day post discharge follow-up- if needed
Referral Criteria
1. Medication related admission (e.g adverse event or non-compliance)
2. Potential financial barriers to obtaining medications
3. High risk med and requires drug education
4. Polypharmacy: >10 home medications at admission or discharge
5. Multiple chronic medication changes during inpatient stay
6. Newly diagnosed/uncontrolled high risk disease state
– Diabetes, CHF, acute MI, stroke, asthma, COPD, pneumonia, CABG, Percutaneous Translumenal Coronary Angiography (PTCA), or other vascular conditions
Hospital Medication Reconciliation
• Nurses use one of the following to gather information:
•Pill bottles
•Patient list
•Outpatient EHR
•Last hospital discharge summary
• Based on this information, nurses will compose an admissions medication list (AML)
Validation of AML
• Check to see if meds match disease state
• Check appropriate dose
• Check for duplicate therapy
• Check for interactions
• Check for missing meds
• Contact patient, family, pharmacy, and MD office if warranted
Outcomes from the Pilot on Accuracy of AML
• N= 26 AMLs (234 medications, average is 9 prescriptions/pt)
• 3 AMLs were complete & accurate
• 96% of the patients had AML on the chart – 8% contained incomplete or inaccurate doses
– 14% had incomplete or inaccurate frequencies
– 71% had unknown administration time and date of last dose given
• Pharmacy Intervention: – Removed 5 meds (2%)
– Added 27 meds (10%)
– Corrected doses and frequencies for 42 meds (21%)
Categories of Drug Therapy Problems
• Indications: • Unnecessary • Additional drug therapy required
• Effectiveness: • Not Effective at producing desired response • Dose too low to produce desired outcome
• Safety: • Adverse Reaction • Dose too high, resulting in undesirable effects
• Compliance • Patient prefers not to take • Patient forgets to take • Patient cannot swallow/administer • Drug product not available • Patient cannot afford the medication • Patient did not understand the instructions
Patient Education 101
The “What?, Why?, How?” – What are your medications goal? – What are these medications indicated for? – What are the potential side effects? – Why is compliance so important? – How do you take your medications? – What signs/symptoms do you look for while on this
medication?
Customize teaching for the individual – Weekly pill container, if needed – Involve patient’s family or caregiver – Using pictures to illustrate – Tip Sheets – Teach back
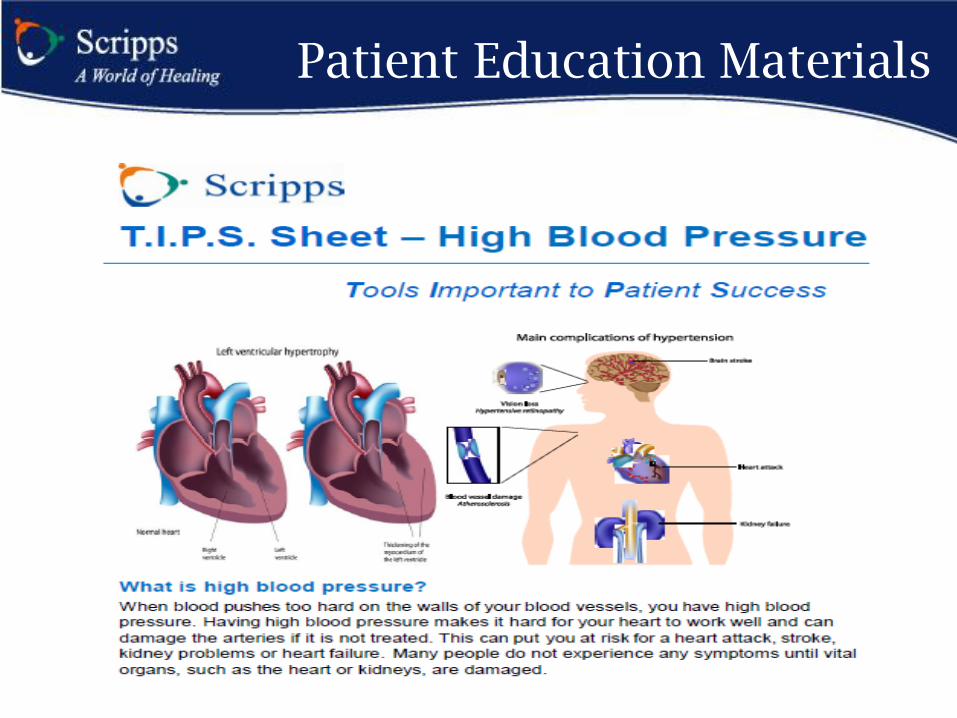
Patient Education Materials
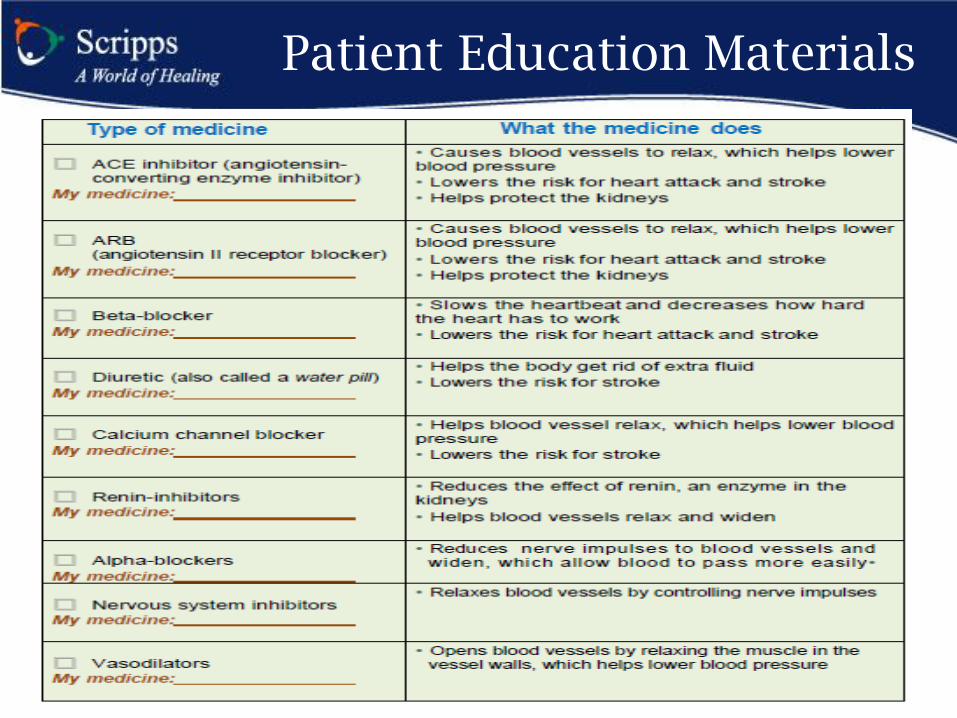
Patient Education Materials
Patient’s Expectations of Pharmacy Services
• Day 1: Validate admission medication reconciliation list (AML), interview patient/caregiver/family, start patient education, and start discharge planning
• Day 2: Continue patient education on disease state(s) and medication(s)
• Day 3: Continue education on new medication(s) and discharge planning
• Day 3 post discharge: Follow-up phone call
Discharge Planning
• Develop an affordable medication which is cost-effective and safe
• Provide counseling on new, changed, discontinued medications
• Work with insurance and get prior authorization, if needed.
• Work with patient’s pharmacy as needed. • Coordinate medication delivery for patient at home
or bedside to improve compliance. • $4 / $10 Generic plans, if and where available. • Patient Assistance Program for indigent patients, if
available. • Provide Drug Discount Cards, if available
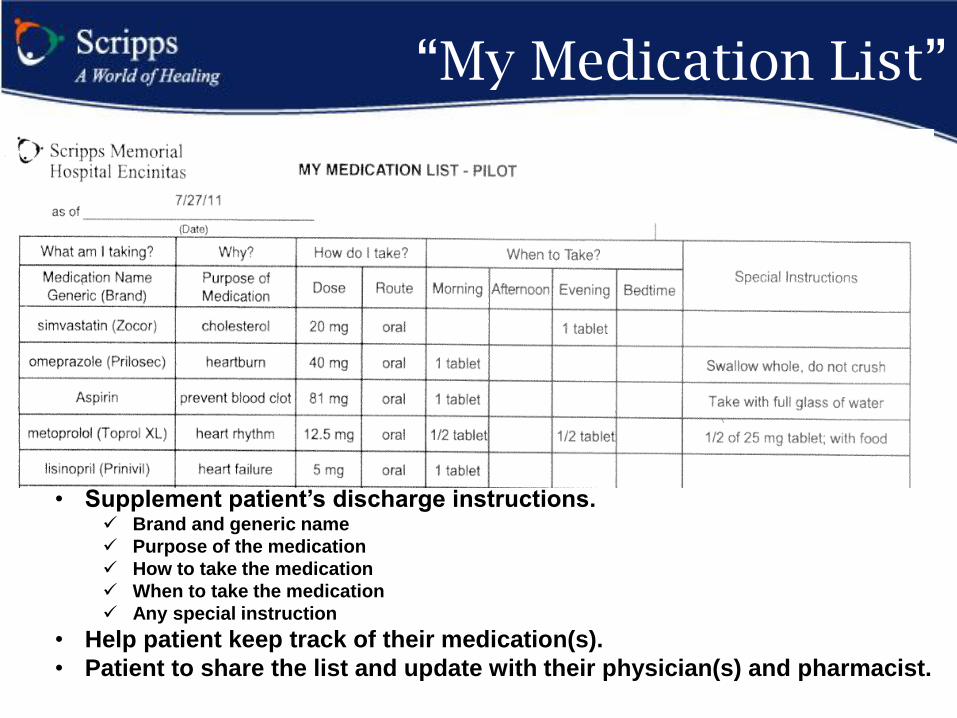
“My Medication List”
• Supplement patient’s discharge instructions. Brand and generic name
Purpose of the medication
How to take the medication
When to take the medication
Any special instruction
• Help patient keep track of their medication(s).
• Patient to share the list and update with their physician(s) and pharmacist.
MTM Post Discharge Follow-up
• Work with outpatient navigator – Determine if treatment goals achieved
• Call patients to assess if: – Medication comprehension was achieved
– Compliance was achieved
– Potential side effects or adverse events were noted
– Medication-related issues or questions were resolved
• Contact patient’s PCP or hospitalist for interventions as needed
Case Study #1
• 76 y/o female with hx of CKD, HTN, TIA. Referred to MTM due to incomplete AML
• What was discovered?
– Aggrenox were in a metoprolol bottle
– Pill box were filled three times daily for hydralazine, aggrenox and metoprol
– OTC aspirin was a 325mg tablet, instead of 81mg
• Patient complaints of headache may have been aggravated by overdosage of aggrenox
• Patient found to have ulcer during this stay which may have been aggravated by excessive aspirin and aggrenox
• Interventions - Clarified with cardiologist and PCP to determine what medications patient should be on.
– Discovered that cardiologist did not have an updated list
Post Discharge
• Patient’s family was educated on importance of compliance and encouraged to help fill out the pill box. Family was very appreciative of all the help and bringing this to their awareness.
• Post discharge follow up, patient’s family has been filling the pill box and found the chart to be useful. Patient responding well.
• 89 year old man came in due to weakness caused by chronic diarrhea/constipation.
• Patient on 20 different prescription.
• When patient does not have a bowel movement, he takes 2 capsule of stool softener, a few doses of Milk of Magnesium, then escalates to a few enemas.
• Thus, causing diarrhea and bowel incontinence.
• He treats this with 4-5 capsules of Loperamide (imodium) daily until his he has constipation.
• Interventions:
– Rearrange dosing time of 20 medications to prevent drug-drug interactions. Discussed bowel symptoms and suggested natural method of pro-biotic yogurt and increased fiber and water.
Case Study #2
Post Discharge
• 1st Post discharge call, patient complained of not having bowel movement for 2 days. RPh reviewed the regimen again and emphasized increase of intake of water from 1-2 glasses a day to 6 glasses a day.
• 2nd post discharge call, patient admits normal daily bowel movement and is happy with new natural regimen.
Outcomes
• Reduce Hospital Readmissions
– Gradual reduction, more significant with Pharmacist
• Reduce Length of Stay
– Reduce by about 0.5 days
• Improve Patient Satisfaction
– Significant increase initially but gradually tapering off.
• Provide consistent care
• Safe transition across the continuum of care
What can you all do to help?
• Help us create education materials we can use on our patients that relates to disease and drugs.
• Provide more drug discount cards
• Provide easier process for Patient assistance program.
• Provide process for us to get prior approval.
Questions ???