town of lantana - amazon web services · town of lantana employee benefit ... look up the status of...
TRANSCRIPT

TTown of Lantana Employee Benefit Guide 2016-2017
�
�
�
������������������������������ ������
In this booklet you will find important information pertaining to your employee benefits as an employee of Town of Lantana
Please retain this booklet for future use.

ContentsYour Benefit Plans………………………………………………………………………………………………………………………………………3
Online Enrollment……………………………………………………………………………………………………………………………………….4
Eligibility and Enrollment Guidelines ............................................................................................................... .…….5-6
IRS Code, Section 125 & Qualifying Events ............................................................................................................... 7
Holidays ........................................................................................................................................................................ 8
Medical Insurance – Aetna ................................................................................................................................. 10-14
GAP Insurance - American Public Life ………………………………………………….………………………………….……15-17
Dental Insurance – Guardian .............................................................................................................................. 18-19
Vision Insurance – EyeMed……………………………………………………………………………………………………………………..…20
Flexible Spending Account – Eagles Benefits by Design, Inc. ........................................................................... 21-22
Supplemental Insurance – Aflac & Liberty Mutual. ................................................................................................. 22
Life and AD&D Insurance – Mutual of Omaha ......................................................................................................... 23
Voluntary Life Insurance - Mutual of Omaha ……………..……….…………………………………………………………..………23-24
Short Term Disability / Long Term Disability - Mutual of Omaha…………………………………………………………………..24
Employee Assistance Program……………………………………………………………………………………………………………………25
Compliance Notices ......................................................................................................................................... … 26-27
CHIP Notice………………………………………………………………………………………………………………….………….……..…….28-30
Medicare Part D Credible Coverage Disclosure Notice ……………………………………………………….……….………...31-32
Health Insurance Marketplace Coverage………………………………………………………………………………….....….…33
Notes ................................................................................................................................................................ ….34-35
Contact Contact InformationHuman Resources� Myila Young� �������������
�� ���myoung�������������Medical Insurance� ����� �������������
����������� ����������Medical GAP Insurance ��� ������ � ��! "� �������������
������#� � ������Dental Insurance� $���% ��� �������������
��������% ����&� ������Vision Insurance� '&(%� �����������)�
����&�%� * ����������Flexible Spending Account� '���*�+�" �*� &�,* ��� �����������)�
�������* �" �*�����Life Insurance (�������"�-��.��
�����������������������"���.������
Short Term Disability� (�������"�-��.���
������������������������"���.������
Long Term Disability� (�������"�-��.���
������������������������"���.������
Liberty National /�*���(�0��&� �������������
AFLAC 1�� %��2�� ���� ��������)����
EAP – Employee Assistance Program� 0���*� ���/�� �*��**�� ��*� ���������������������������������*� ��*�� �*�**������ ������

3 | P a g e
Benefit Plans for Employees of Town of Lantana 2�����"�!��������""�*���"����������"� �" �*������ ���&����.��##����� �&����#��������%�����"���&�����%�&����"�� �&��-���"��.���*�� �#���������%������ ���*����*� *�&����#�*����� �" �*�#�����-�������� *����#��� %��� �" �*�#��������.����*#��%*����&�����%*���%���� � #��*��.���3#��%��4����#�*����� �" �*�#���� *���*��#�����"�&��������������#�*�� ���"����2�����"�!�����������
�
�� (% ����0��������� ,�����0�������� 5 * ���6�*�������� +�* ��2���! "���%��,7,�6�*�������� 5�������&�! "���%��,7,�6�*�������� /.���2���, *� � �&�6�*�������� 5�������&�!���2���, *� � �&�6�*�������� ,#�%���0���8 � ��*�������������� 1���.����9�3 ��/#�% ������������� '�#��&��** *��������������� 5�������&�0� � ����0�����%�8����&�6�*��������� 5�������&���� %�����%�1�*# ����6�*�������� 5�������&�0�����0����� 8� ����������
�6���.�"����� ���#��*:�&��;������������� �����.� �" �*��.����.�2�����"�!��������""�*��4���� �����*��*�.����.��* ����.�� �.����� ��� ����"� �" �*�����.�#�#������&�����%�&����"�� �&;*�.���.���%�" ����*�<���%�&����"�� �&;*�"����.
KKey Benefit Terms
CCOBRA – A Federal law that allows workers and dependents who lose their medical, dental, or vision coverage to continue any of these coverages for a specified length of time by electing and paying for continuation benefits.
Deductible – The amount you pay toward medical and dental expenses each calendar year before the plan begins paying benefits.
Out of Pocket Maximum – The maximum amount you will pay in coinsurance during the calendar year
Co-insurance – The percentage of the medical or dental charge that you pay after the deductible has been met.
Copayment – A flat fee that you pay for medical services, regardless of the actual amount charged by your doctor or another provider. This generally applies to physicians’ office visits and prescription drugs�

4 | P a g e
OOnline Benefit Enrollment through PlanSource 2.�2�����"�!�������� ����*�PlanSource��*�������� �����������*&*����9����.�������#�����������&���%������.������������� ��&����#������� ��*��������"�&����#�*�����%������%� �" ����� ��*�"������*��&������ ���.�*&*����1������.�2����*������&�*���*�*��.���&����� ��&���� �" ����� ��*���%��#%���&���� �" � ��&=*>��
About PlanSource
PlanSource� *�����#��&�*�"*�� ��#�������.���� ���������&���������**������.� �"����� �������%����&���� �" �*��4��������*���&�� � ���*����&�.�� ���.�����%�������**�����/�������? �.�����/����:�&���.�������� �����**��������&���� �" �*����%��#��&���� �"����� ������.���*���%�&:���%�&*����@����
Logging In
2�����**��.�* �:�#� ���&����� � ���*�����.��#�AA �" �*�����/����������2����� ��&�����*������� ��� �" �*�� � � ����"�&����" �*�����:�&������*��������%���*����% � �*��"�&����/�� ���/��� �&�B�� ��� �.������&�%�*.*�="���3��#��C��/� �.:���)�������� ��� �D*� �.����>��
B3��&���� �������&����#�**���%���4����#�**���%�� ��� �&����%����"� ��.� ������ ��"������� �.������&�*��*.*:�YYYYMMDD��0� �@��.�E!���6�F� ��������4���� ��� �#���#�%�����.����&����#�**���%��#���&������� ������*� ����%���. ��� "��� &���*�"� �� �.����� &��� "����� &����#�**���%� =?�%������ ������%�����% ���&�����������#�**���%:����&���. ����.���� ���.�#�&������ �� �>�
G*��B����HHHHHHHHHHHHHHHHHHHHHHHHHHH���**���%�1 ����HHHHHHHHHHHHHHHHHHHHHHHHHH�
2�������.����������&���0� �@����“Make a change to my Benefits”���� � ���6"�&�����������. ���. *�� �@�� ���*�&�“New Hire –�Enroll”���%�%�� ����#�����������“Enroll – Annual”
?.�����#��%�&�����&��� ��&�������" ���� ���*�����&����&���*�"����
�
2��re-enroll� ��&���� �" �*�%�� ����#����������:�&���� ����%������� ���
��� $�����.��#�AA �" �*�����/������������ '����&��������*�������%�#�**���%�)�� 0� �@� �" ����� ��*���� 0� �@������� �� �" �*���� 2.��"���������*��������������#���&������� ��*�����
�
�
PlanSource� *���� �� �����.���*���%�&:���%�&*����@�%�� ����#�������������4���� ���.������**�����.�#����%* ��*�"����.�% ""����������*:�#�� ��*���%��.�% ����� �@*�����.�6�*������0��#��&;*�� * �*����
,�� ����.�&���&���������� ��������**�&���� �" �*���%� �*���������#��&�� �@*��
9�����*�����*�##���:�&������������Myila�4������������������:�(��%�&��.����.�9� %�&:�%�� ���������� �* �**�.���*:������ ���&������������������
5 | P a g e
EEligibility and Enrollment Guidelines Eligible Employees
2�� �� � ��"���.���.�������:��*������*���.�� �" ��#������*��""�%��.����.��.�2�����"�!������:�&�����*�� ���"���� ���#��&���0������� ��� �""�� ������.��*���"��.�����.�"����� ������%�&*��
Eligible Dependents
,#�%��*��.������� � ��"����% ������%�%���������
�� 2.��#��&;*�*#��*��*�%" �%� &����:���� 0. �%����.���������"��.�"����� ����� �� ���
o� �� ���� �����. �%I����o� �����"���&��%�#�%��. �%I����o� ��*�#�. �%��"��.��#��&I����o� ���. �%�"����.����.��#��&����*#��*�.�*� �������&��##� ��%�*�������% ���"���
��� �%" � ��#� �%��"�� ���� ,#�%��*��������.����.����)���
o� ,#�%���0������ *���� �� ���.����.�������� �.�����*�� �� ��*���0������ *���%���� �� ������%�**��"���� ���:�*��%������%#�%���*����*��
o� ,#�%����������������)��<�9��� %��!� *��� ���������� *���� �� �������*����� ���.��%��"��.�����%���&��� ���. �.��.��. �%����.*����)��#��� %%�.A*.� *������� %:����%#�%��*��B,� *����* %����"�9��� %��-8���"�������#����� ��*��%����B,�
o� 6*�����#��� %%�.���.�������� &���&���.������#���� �% � %���� �" ��#�����B,� *������� ��%���� �" �*���%���.�/�� ���/��� �&������
����"��.������ �% � %���� *���J��� " %�%#�%���=���� ������ ��.���� " ���:�����% ��*. #���%�*:��*��##� �� �>� *��J� �%�����.�� ���"� � � ��������������%�#� �% ����&��.��"����
Disabled Child Eligibility
0��� �� �#��&;*� =������ %>� ����%� %#�%��;*��% ���� ���������&� � ���� ��%� &��%� �.�� � � �������"���:� "��.�%#�%�����
o� 6*� ���#� ���"�*�"*�##����%����������� ���**������&���.�����������#.&* ����.��% ��#I��
o� 6*�.��% ��##%�prior to attainment of the limiting age���%� *��. "�&�%#�%�������.��#��&�"���*�##��������.���%�����
o� 6*���������%���%�����% ����3#�*������* ���#�� �&:���%I��o� 8�� �*�%#�%����#����.� �*��%�#������������% ���"���*�##������%��� ���������
����"��.����.��. �%� *�"���&�% *� �%���*�� �*� � ��%� ���� � ������������.���)��%�&*�#� �������.�%����.����.� %#�%��;*� �����������%� ��*�� � 2.� 2���� �"� !�������.�*� �.� � �.�� ��� �J� �:� ��� ��*��� �� ������*:�#���"��.����.��. �%���� �*�"���&�% *� �%:� *�%#�%�������.��#��&�"���" ���� ���*�##���:���%���.�� *�*�� *" *��.�68/��� �� ���*���%#�%���"��� �.�#��#�*��"�3���% ���2�����"�!������;*������ �� ��*���%��.�������"�����%�*�� �*�"�����.��#��&;*����**� ����������*���������1�����8*����*� "�"���.������ " ��� �������% �������#� �*������� � � �&� *��J� �%���

6 | P a g e
Adding and Dropping Dependents Mid-Year
-��* %�-#��'��������:���%#�%������� �%��##%�����%%%����&� "��.��#��&�3#� ��*����68/%" �%�0.���� ��/����*:�"���3��#�I����� ��:�% ����:������**��"����������%���.�*#��*;*�.���.�#������0.���*���*�� ���%�� �. ��)��%�&*��"��.�0.���� ��/����*����"����.���� �:��.��#��&���*���� ����� ���.��3��-#��'�����������See Qualified Events Section for a detailed list of events
Coverage Periods & Election Timeline
0������� ��� �""�� ���.�" �*���"��.�����.�"����� ������%�&*��"��#��&�����9���3��#�:�&������. �%����9 ����&����.I�&������������ ��� �""�� �����(�&��*�����
0������ *�������� ���%���� �� �.� �#��&K*�.���.�#������������� *� �� �%���%�#���**%��G�� ��.���.�#����������� *���� ���%��.��#��&���&��%����#�&�.���.�������*�*�����"#��@����%�" ����� �*������������ *���� ���%��
For new employees, you have 15 days from your date of hire to complete the online benefit enrollment with PlanSource.
Note:� 6"� *#���� ��� �"� �#��&���� �����*�� �.� �.�2�����"� !������:� �*������ �������� ��� ���� ����.����.��.��%��"��.�����.� ���. �.��.��#��&�#.&* ����&����@%��

7 | P a g e
IRS Code, Section 125 and Qualifying Events
Cafeteria Plans
�*��� �" �:��.�#�� ��*�"���.���.:�%����:�� * �����%�9�3 ��/#�% ��������������%%���%�"����&�������**� ����� "���&���� ����� *���3%���+���*��.*� �" �*����"��"����"%������3*:�&������3� �� ����� *��%��%:��. �.� ����**��.�#��������"�&������@.���#�&���2. *� *�@������*���0�"�� ����������/�� ���������%� *�������%� &��.�68/���
6�� *� �#���������������.���68/������� ��*��J� ���.���������=*>���� �� ��""���"����.��� ��#����&���=-��� ���*���.����.�/#�� ��)��.>���2. *����*��.���&�����%�&����%#�%��*���������� ���� �&��
�� 0.����.���.�#���*��� �%%���������%#�%��*��� 0������������
4�����*���� ����� ���.�"����� ����#�����������#� �%������@��.*��.���*����**�&���3#� �����J��� "& ���������2. *� *������%� &��.�68/�0�%:�/�� ���������
Qualifying Events
'�#��&*���%��. ��%#�%��*��.���3#� ������� ���.���*� ���. ��"�� �&�*����*�����#��&�������� � ��"����.���*����* %��.��#�����������#� �%��0.���*�� ��� ������%�� �.�#��#��%�������� ����"� �.�*����*��.������%����#�� ����"� �.�#��#��#�#����@�within 30 days of the qualifying event. +&��%�)��%�&*:����*�� ��� �%� %���%��.��#��&���&� ��*#��* �� ��.������&���%�" ���� ���&�"�����&���� ����%A���3#�*� �����%��*����*�����"��.��#��&������%#�%����.������ ��*���� ������%� ��������������*�� � � �&��J� ����*��6"�&�����J�*�� *��##���%:��%% � ��*�� �����@�#��������.�" �*���"��.�����.�"����� ����.�J��� "& ������:�3�#��"��� ��.���%�%��.�����&��������� ��*�� ��� �#���**%�����.��%��"��.�����.������*�*� ���������#�.�* ��� *� ����"�J��� " %����*���
�� 0.���� ���������� ����*����*��� ���.���� ���.���� ���"�%#�%��*��� ���.���� ���#��&����*����*��"��.��#��&����*#��*����%#�%����� �� %#�%��� ��* ��� ��� *�� *"&� � � � �&� �J� ����*� "��� ������� %�� ��� ���� ����� �"� ��:�
*��%���*����*:���� ����*����*:������.��* � ����� ����*����*���� ���.���� ��#�����"� �* %����"� �.��#��&:� �� ����� �. �� *#��*����%#�%�����%� �.�
����������� �� *�������� �� ����� / �� " �������*�������������.���*�= ����% ��������������� �������%��.��%% � ����"��� �" ��
#��@��>���� 9�� �&�(% ����!�������=9(!�>�������� C�%����*:�%��*������%�*���� ���.���� ����������"���*#��*����%#�%�����%������.���#��&�;*�#������� -#�������������%���.�#�����"�����.���#��&����� 1���.� 6�*������ ����� � �&� ��%� �������� � �&� ���� =16���>� *#� ��� ��������� � �.�*� "��� ���
%#�%��*���%� ���.���*��"���**��"���.�� �*���������������� ��0-+8��J��� "& ���������� !�**��"����������%���.�����#�.���.�#�����"�����������������%���� ����� �*� ��� ���=��*���;*�
�. �%��;*�.���.� �*������#������:��% ��������#��������"����6�% ����� �����������:�*����.���.� �" �*�� *@�#���:����"�� ����������������#�.���.�#���>��
�� '�� ���������(% �������(% �� %����016����������

8 | P a g e
Holidays 2.�.�� %�&*��� ���%� &��.�2�����"�!����������#��� %%� ������6"��.�.�� %�&�"���*������/����%�&:��.�.�� %�&�� ��� �� *��%�����.�#�� ��*�9� %�&I� "��.�.�� %�&�"���*������/��%�&:��.�"����� ���(��%�&�� ��� �� *��%��
�������
�
�TTown of Lantana Holiday Schedule�
�� B��4��;*�,�&��� (��� ��!��.��L ��:�C���,�&��� ��* %��;*�,�&��� (��� ���,�&��� 6�%#�%���,�&��� ��*�����,�&���� �,* ����%�����.�
'�#��&;*�, *��� ���� �.�#��#���##������
�� !� ���,�&��� 5����;*�,�&��� 2.��@*� � ���,�&��� ,�&��"���2.��@*� � ����� 0.� *���*�,�&�

9 | P a g e

10 | P a g e
Health Network Only Plan - Aetna
Health Maintenance Organization – HMO
2.�2�����""�*�����.���.�#�����#� ��*��.����.����������
2.�1(-������ *�-#�����**� ��%� %�*����� �J� �� &��� ��� �.��*����� ���&�0����.&* � ���=�0�>����
9��� ������@�#.&* � ���*�� �*:���M�����#�&� *� �J� �%� �.�� � * � ��� �� �0�I� �.�/#� �� *����#�&� *�M�����2.�%%��� ������. *�#����"���* ���� *�M�:������%�M��:����"���"�� �&���2.�-���"���@��(�3 ����"���* ����������� *�M�:������%�M��:����"���"�� �&���2.��� �*������ *����N���There are no benefits for going out of network.���
All co-pays, including prescription drugs go towards meeting your Out-of -Pocket Maximum. Once you meet your Out-of-Pocket Maximum, all covered services will be paid at 100% by Aetna
Health Network Option Plan – PPO
2.� -#�� ���**� ��-� �����*� &��� ����� �� �% ���� *�� �*� without� " �*������% ��� ���&���������.����.����� ���&�0��� �.&* � ��� =�0�>�� 4��� .��� �.�"�3 � �&� ��� ��� �� ��%� ���� �"� �����@�� �.�������"�������
M�����#�&� *��J� �%��.��� * � ������0����%��.�*#� �� *����#�&� *�M�����2.�%%��� ������. *�#����"��� ������@�#��� %�*�"���* ���� *�M�:������%�M��:����"���"�� �&��2.�%%��� ������. *�#����"��������"������@�#��� %�*�"���* ���� *�M��:������%�M��:����"���"�� �&���2.�-���"���@��(�3 ����"��� ������@�#��� %�*� "���* ����������� *�M�:������%�M��:���� "��� "�� �&��2.�-���"���@��(�3 ���� "��������"������@�#��� %�*�"���* ����������� *�M��:������%�M)�:����"���"�� �&��
The deductible, co-pays and co-insurance go towards meeting your out-of-pocket maximum.�6"�&����.��*� �����������"������@:� &�������%� �“balanced billed”��. �.� *� �.�% ""���� ��������;*������� ��"���%��.�#.&* � ������.�*# ����"����
-���&������&��������"#��@����3 ���:���������%�*�� �*�� ��� �#� %�������N� &��������
The HMO and the PPO plans include prescription drug coverage. Emergencies are covered nationwide and 24/7. A description of the plan benefits for both plans are outlined side by side on the following pages.
The networks for Aetna plans are:
Tier of Coverage� Employee Cost�'�#��&�-��&� M�����'�#��&�O�/#��*� M�������'�#��&�O�0. �%=��>� M�������9�� �&� M�)���)�
Tier of Coverage� Employee Cost�'�#��&�-��&� M�)�)��'�#��&�O�/#��*� M����)��'�#��&�O�0. �%=��>� M�)��)��9�� �&� M�������
2016– 2017 Premium per Pay Period
2016– 2017 Premium per Pay Period

11 | P a g e
This is only a brief overview of your medical benefits and should not be relied upon to fully determine your coverage. Pleaserefer to your Benefit Summary for a detailed description of the services and supplies that are covered and those that are excluded or limited.
HMO Health Network OnlyPPO Health Network Option
AAetna Plan Features AAetna HMO AAetna PPO Calendar Year Deductible (CYD) 6��B����@�-��&� 6��B����@� -��-"B����@�
Single M�:���� M�:���� M��:����Family M��:���� M��:���� M��:����
Out-of-Pocket Maximum � � �Single M�:���� M�:���� M��:����Family M��:���� M��:���� M)�:����
Coinsurance �N� �N� ���N�Physician Services � � �
Primary Care Physician (PCP) M�����#�&� M�����#�&� ��N��"���%%��� ��Specialist M�����#�&� M�����#�&� ��N��"���%%��� ��
Prenatal OB Care (excluding delivery and postpartum care) 0���%����N� 0���%����N� ��N��"���%%��� ��
Preventative Care � � �Routine Well Child
Exams/Immunizations1 Exam every 12 months
0���%����N� 0���%����NI�%%��� ���� �%� ��N��"���%%��� ��
Routine Gynecological Care1 Exam every 12 months 0���%����N� 0���%����NI�
%%��� ���� �%� ��N��"���%%��� ��
Routine mammograms 0���%����N� 0���%����NI�%%��� ���� �%� ��N��"���%%��� ��
Hospital Services � � �
Inpatient 0���%����N���"���%%��� ���
0���%����N���"���%%��� ��
��N�#���%� ** ��I��"���%%��� ��
Outpatient 0���%����N���"���%%��� ��
0���%����N���"���%%��� ��
��N�#���%� ** ��I��"���%%��� ��
Emergency Room 0���%����N���"���%%��� ���
0���%����N���"���%%��� ���
0���%����N���"���%%��� ��
Urgent Care M�����#�&� M�����#�&I�%%��� ���� �%� ��N���"���%%��� ��
Diagnostic Procedures � � �
Diagnostic Laboratory Covered 100% after deductible
Covered 100%after deductible
50% after deductible
Diagnostic X-ray Covered 100% after deductible�
Covered 100%after deductible� 50% after deductible
Diagnostic X-ray for Complex Imaging Services (MRI, etc)
Covered 100% after deductible
Covered 100% after deductible
50% after deductible
PPrescription Drug Benefits ((RX) Retail (30 day supply)
Aetna HMO Aetna PPO
In Network In Network����������� Out of Network�Generic� 2����M)I�2��M��� 2����M)I�2���M��� B���0���%�
Brand Name� M��� M��� B���0���%�Non-Preferred Brand Name� M��� M��� B���0���%�
Specialty Drugs, includes self-injectable, infused, and oral specialty drugs (��� ����%��� ����%���#������)��%�&�*�##�&:�3���%*� �*�� �>��
��"��%��)�N�� �.�����3��"�M)���#��#�*�� #� ��I�B����"��%����N�� �.�����3��"�M����#��#�*�� #� ���
B�������%�
Mail Order Program (90 day supply)*� ���3�8�� ��0�#�&� ���3�8�� ��0�#�&� B���0���%�*You will receive a 90 day supply for the cost of a 75 day supply of medication by using the mail order option.
12 | P a g e
Aetna’s mail-service pharmacy for the medications you take every day
�����83�1���,� ��&P� *��.�#�*�� #� ����� ��*�� ��"��������#.�����&� �" ���� �*��G*� �������%��&������ ��������% � �*� &��� ���2.*��&#*��"�%���*�������.��� �����% � ��*�*��.��*����.� � *:��*�.��:�% � �*:�. �.��.��*����:�.�������% � ��*:�.&#���* �����%���.�*���
A money-saving option
,#�% ������&���������#.�����&� �" �*���� �*������#���:�&�������%�*������&� &��* ��������83�1���,� ��&������;*�*�� �*��""���
�� Savings��4�������*������&� &��* ��������83�1���,� ��&� &���%� ���)�����.*�"����.�#� ���"���������.*:���%�*���%��%�*. ## ��� *�����&*�"���!��������������B�� ��������%�� * ������%����#� � ���*�� ������" �%�����.������.�&�������*������*#� " ��%���*��
�� Privacy��0��" %�� ���*. ## ����"�&����#�*�� #� ��*�� �.�����&����.��:����@#���������&���.������� ���&����.��*��
�� Convenience��8��%�����&�������&��.������.*���� Peace of mind��8� *��%�#.����� *�*��.�@���%�*�"����������&���%������� �� �����.���*���
%�&:�*���%�&*����@� ����*��"������&��
Get started today
/����� &���� �����)�%�&�*�##�&��"�&������ �������%���������������#.�����&��2.�:�*���� ����%����&� &���%� ���&����#�*�� #� ��*��.����.������83�1���,� ��&��9����� ����.*������*&�*�#*��
�� Step 1��$����#�*�� #� ���"����&����%������"�����.��� �������%����=�&# ����&�����%�&�*�##�&>����� Step 2��0��#�����%��� �������%��"����������� �.�&�������#�*�� #� ��=*>���%�#�&������������
83�1���,� ��&��-����1���&����%������"�3�&����#�*�� #� ��=*>�� �.����#��%���%��"����
Learn more
6"�&���������������� �:�&����������������� ���������83�1���,� ��&:����**������%��"���:���%����� &����� ��� �����&����*���������B�� ������=����������� ���������>��� ��� * �:���%��� �@��.� ����� �����.��"��* %��"��.�#����.���*�&*:�E-�%���% ��� ��*F��
�
�

13 | P a g e
Aetna Navigator
�����B�� ������ *�����;*��� ����%����*����*�"*�� ��� * ���.���#��� %*���single source�"������ ��.���.���%� �" �*� �"����� ������.���*���%�&:���%�&*����@���2.����.������B�� �����:��*�*�����" �%�#��� � #�� ���#��� %�*:��#�������6,����%:��*���.�����;*�#��%���*���%�#������*:��������������% ����&:���%����**�����*����������"���% ��.���.���%�����**� �"����� ����������B�� ��������*�� ����%*�*���:�#�*���� Q%�"����*:� ����% ������**������� ����%� �" ��*����*��
Log on to Aetna Navigator today!
Find a Doctor
�� 2��" �%����6�B����@�,���������9�� � �&�� �. ��&�������:�������������������A%��" �%������ -�������. *�#��:�&���� ��� �� �����*���.� &�#.&* � ��;*�������%������� ������@�
#��� %�*A"�� � � *� ��&����������� 4���� �����*��.����.�� � �&����*���.�"���.���.�����#��"** ����*��.��������*#� " �����% � ��*�
��%�#�"�������� ��#���%��*����� ?.��&������#���#�%����*������#���:��� �#��*�*�������������"Aetna Open Access Plans"�
��%� "�&��K����@ ����.�1(-����1���.�B����@�-��&�*�����.�"Aetna Health Network Only"��6"��.��� �� *���@ ����.�1���.�B����@�-#� ��������-�#����#��*�*�����.�"Aetna Health Network Option"��
�� 6"�&��K%�� @�����������&����*���.�"��� �.���.�%�����*����%�� *�*���%����@�"���%�����K*� &���*�����:�#��*�D��#�%�������R/���.� &�B��:�/#� ���&����-�.��-#� ��*R��
Aetna Mobile, convenince “on the go”
Use your web enabled phone or mobile device to:
�� View your ID card information �� Look up the status of a claim �� Find doctors, hospitals, specialists, or walk in clinics �� Check the price of prescription drugs
Log on to Aetna Navi
Find a Doctor
�� 2��" �%����6�B����@�,����� -�������. *�#��:�&���� �
#��� %�*A"�� � � *� ��&������� 4���� �����*��.����.�� � �
��%�#�"�������� ��#���%� ?.� &�� �� #���#�% ��

14 | P a g e
AAetna Discount Programs
6"�&����.���.� �" �*����.���.� �*������#��������*���&��"��.*�*�� �*:��*�&����#����" �*�����
4�������%�#�&��**������"�#��@�����
Aetna Fitness(sm) Discount Program�<�$���.��������%����*���������&�����.� ���"�������:�����&�*� ���.�$�� ��" �������@��2��D� �����&�:������ ����$�� ��" �����A" ��**��
Home Exercise Products and Equipment< , *�����*�*��.��*����%� ��*���%���.��.���3�� *�#��%���*���
Natural Products & Services –Save on a natural path to health living. You will pay less for massages, therapy, acupuncture, chiropractic care, dietetic counseling, vitamins, herbal supplements and more through American Specialty Health (ASH), Inc. a leader in this market. Log onto www.aetna.com and follow link to discounts. .
Weight Management Discount Programs – Lose weight, feel great and save! Enroll online at www.aetna.com and follow the link to discount programs. Enroll in an online diet plan that is convenient and personalized to you. Discounts at Jenny Craig, Nutrisystem and Calorie king.
Vision Discount Program – Save on what you need to see better, like eye exams, glasses, contact lenses…even LASIK.
Hearing Discount Program - Pay less for hearing aids, exams and more through Amplifon Hearing Health Care, a leading provider of hearing supplies. With over 1,900* locations in the U.S., it’s easy to find one near you. Log in to www.aetna.com for further information/
Other Savings – Save on dental products, Sonic Toothbrushes, Epic Dental products like gum, toothpastes, and mouth rinses. Discounts on books and other items from the American Cancer Society Bookstore. Just go to www. Aetna.com and choose “Health Programs” , then “See the Discounts”
Aetna Health Information Hot Line – Nurses available 24/7 call 1-800-556-1555. Have a sick child at 2 am in the morning call the Aetna Health Information Hot line for advice.

15 | P a g e
MEDICAL SECONDARY INSURANCE (GAP)
2. *�#�� �&� *���/G��!'('B2�!�6B/G8�B0'��!�B���%� *� ���%% � �������.��'2B���% ����#������
� When you have a claim for a service that is covered by APL you must submit the claim to AETNA first, your primary medical insurance carrier.
In-Hospital Benefit� �
6�1�*# ����+�" �*�(�3 ����(�3 �����"�M�:����#������%�#�*���#������%���&����(�3 �����"�M��:����#������%���&���"�����������%�#�*��*���� �%��
6��1�*# ����+�" ���
+�" �*� ����%� �.�*# �������" ����:��� ��������%� �.�*# ������������"��������������� �����% *��%��=*� D����������3 �����"�)��%�&*��"������������� �����% *��%����������#������%�#�*���#������%���&��>������ �" �*����*� D�������.���� �%� �.�*# ������%����#�� ��� �" ����3 �����
Outpatient Benefit� �
-������ ���+�" �*�(�3 ����(�3 �����"�M�:����#������%�#�*���#������%���&���"�������%����#�� ���*�� �*��(�3 �����"�M��:����#������%���&���"�����������%�#�*��*���� �%��
-��#�� ���+�" �*��
0���%����#�� ���*�� �*� ����%�.�*# ���������&�����:�����������"�� � �&:�*����&� ����.�*# �������#�� ���"�� � �&����"�*���% ������#�� ���*����&�����:�% ����*� ���*� ��� ����.�*# �������#�� ���"�� � �&����(86�"�� � �&:�#.&* �����.��#&�"�� � �&:��� ��������%����#�� �����������"��������������� �����% *��%��=*� D����������3 �����"�)��%�&*��"������������� �����% *��%����������#������%�#�*���#������%���&���>����� �" �*����*� D�������.����#�� ��� �" ����3 �����
Covered Out Patient Services� �
1�*# ����'�����&�8���� ��&� ���#�����.���3 �������#�� ��� �" �:�*� D�����������&������#�����������%%��� �:��*�*.����� ����
G�����0���9�� � �&��� ��&� ���#�����.���3 �������#�� ��� �" �:��"���*�� *"��� ����"���&��##� �� �����#�� ���%%��� ���*�*���%� ���.����#�� ���#�� �&�� ����
-��#�� ���/����&�
-��#�� ���*����&� ����.�*# �������#�� ���"�� � �&����"�*���% ������#�� ���*����&���������&� ���#�����.���3 �������#�� ��� �" �:��"���*�� *"��� ����"���&��##� �� �����#�� ���%%��� ���*�*���%� ���.����#�� ���#�� �&�� ����
, ����*� ��2*� �����, ����*� ���*� ��� ����.�*# �������#�� ���"�� � �&����(86�"�� � �&����&� ���#�����.���3 �������#�� ��� �" ���"���*�� *"��� ����"���&��##� �� �����#�� ���%%��� ���*�*���%� ���.����#�� ���#�� �&�� ����
�.&* ����2.��#&�9�� � �&� ��&� ���#�����.���3 �������#�� ��� �" �:��"���*�� *"��� ����"���&��##� �� �����#�� ���%%��� ���*�*���%� ���.����#�� ���#�� �&�� ����
Outpatient Riders� �-"" ��2�������8 %�� ���� �" �*����*� D�������.����#�� ��� �" ����3 ����
0�����-��#�� ���2�������8 %�� ���� �" �*����*� D�������.����#�� ��� �" ����3 ����
6�%#�%���!� �9�� � �&�8 %�� ���� �" �*����*� D�������.����#�� ��� �" ����3 ����
,��� ��(% ����'J� #����8 %�� ���� �" �*����*� D�������.����#�� ��� �" ����3 ����
Amendment Riders� �
,#�%���0. �%�(���� �&����%����8 %�� 6����%%�

APSB-22417
Underwritten by American Public Life Insurance Company. This product may have limitations and exclusions. This product is inappropriate for people who are eligible for Medicaid coverage.
Two Easy Ways to File a Claim!
• Simply present your ID card to your medical provider so they may file your claim and accept the assignment of benefits.
• If your medical provider is unable to accept assignment of benefits, you may file a claim directly with APL.
1. Present your ID card to the Provider
2. Submit a claim to APL• Find claim forms on ampublic.com under “Claims & Forms.” Select MEDlink® from the list of products, then click “download.”
• Using the MEDlink® claim form (Form C101), complete the section entitled “Claimant’s Statement.” Please be sure to sign and date in the blanks provided at the bottom of the form.
• Include the Explanations of Benefits from your primary insurance carrier
• For in-hospital and outpatient hospital claims, please include a uniform itemized hospital bill from your provider (Form UB-04)
• For treatment in a physician’s office, please include the physician’s itemized statement of services from your provider (Form CMS-1500)
Claims may be submitted to us by fax at 877.365.9423 or by mail to:
APL ClaimsP.O. Box 925Jackson, MS 39205-0925
Need assistance? Call 800.256.8606, option 2. We’re happy to help!
Filing MEDlink® Series Policy Claims Instructions for the Insured
Submit Your Claim
If the provider is unable to accept assignment of benefits, please obtain a walk out statement (Form CMS-1500) or an itemized hospital bill (Form UB-04) so that you can file your claim with APL. In order for APL to consider benefits, the itemized bill or walkout statement must list the claimant’s name, date of service, charge, procedure code, diagnosis code, name and NPI number of the attending physician.

APSB-22418
Underwritten by American Public Life Insurance Company. This product may have limitations and exclusions. This product is inappropriate for people who are eligible for Medicaid coverage.
Assignment of BenefitsAPL accepts assignment of benefits. Claims submitted with an assignment of benefits will allow any payable benefits to be made directly to the Provider of Services. Ask your patient for a copy of his/her ID card.
Filing MEDlink® Series Policy Claims Instructions for the Provider
Claims may be submitted to us by fax at 877.365.9423 or by mail to:
APL ClaimsP.O. Box 925Jackson, MS 39205-0925
Need assistance? Call 800.256.8606, option 2. We’re happy to help!
Submit Your Claim
As a healthcare service provider for APL’s insured customer, you are an important customer to us. We are here to assist you in getting the information you need to provide service to your patient, our customer.
Unable to Accept Assignment of BenefitsIf you are unable to accept assignment of benefits, please provide the patient with a walk out statement (Form CMS-1500) or a uniform itemized hospital bill (Form UB-04) so that the patient can file the claim with APL and receive his/her benefit. To file the claim, the patient needs a statement providing the name and NPI number of the attending physician, the name of the patient, the date of service, the procedure and diagnosis codes, and the charge.
Confirm CoverageTo confirm coverage, simply call APL at 800.256.8606, option 2, from 8 a.m. to 7 p.m. EST to speak with a claims customer service representative.
File a Claim• The Explanations of Benefits from the primary insurance carrier must be submitted.• A uniform itemized hospital bill (Form UB-04) must be submitted for inpatient and outpatient hospital claims.• The physician’s itemized statement of services rendered must accompany the claim form when filing for treatment in a physician’s office (Form CMS-1500).

18 | P a g e
DDental Insurance – Guardian Guardian Dental DMO & PPO
�
2.� 2���� �"� !��������""�*� �.�� �� ,(-� �����-� %����� #���� �#� ����.����.� $���% ���� � 2.���-� � ��� ������ &��� �.�"�3 � �&����*������.����)�:������"��%����� %�*���%�� * ����&�� ��*%�%�� *��� �.�������"�������2.�#��������*�#���� ������������N���G�%���.�,�������"��%����� %��-���� Q�� ���=��->�#���:�&�����&��.��*�����.�� ���"�*�� �� �.������-�#��� � #�� ���%�� *�������&����#��� � #�� ���%�� *����? �.��.���-�#���:�*�� ��*���� #�** �� ���*� �.� #��� � #�� ��� %�� *�*� .��� ���%� ��� #��� %� ���� "��� ����%� *�� �*� ������� ��%� ���*�� � � B��#��� � #�� ��� �" �*� ��� *� D��� ��� �*���� ��%� #��� � ��� �.���� � � �*:� �*�%��� �%� &�$���% �����
2.� ,(-� �#� ��� *� ��%* ����%� �����@� �"�%�� *�*� �.����.�$���% ���� 2. *� #��������*�#���� ������������N� �*� ���� ��%� .�*���#�&*� �**�� ��%� � �.��.� *�� �*� ��%�%��.����.��.�%* ����%�%�� *���
Dental insurance plan features
�� 4�������� * ����&�� ��*%�%�� *��� �.�������"�������� 0������"���#���� �:� �* ����%���D���*�� �*�SS��� /�� ��*��""�%� &������@�%�� *�*����*�� �*���������%� &��.�#�������� $���% ���.�*���������%����*�� �.������@�%�� *�*��.�������"������.�������.����. ���������
"*��2.������*�&�����&�*������&� &�*��& ��� ��$���% ��;*������@��
To Find a Dentist
�� $�������������% ����&� �������� 0� �@�'�#��&*���%��.���� �@�,����� ���.�%��#�%���� �3��� 0� �@�����.�E9 �%������� %�F�� �@�����.���#��"��.�#����� 0� �@��.�E9 �%���,�� *�F�� �@�����.�� �.���"��.�#����� 0� �@����,�� *����� /����&����#���:�,1(-������-���� 4����� ����.��.����.�� � �&����*���.� &�!���� ��:�,�� *�;*�������%�-"" ������� ��������� ��*�� ���� ��� � �����J�*� ���&���*����&���������@��. �.�"����.���-�#���� *�,����$���%�
��"��%�B����@��2.�,(-�#���� *� ���.�(����%�,����$���%������@���� �"����.������@� *�*���%:�&�������*���.� &��%%�**����" �%��. �.�%�� *�*�������**�����&���
��� &�*������%������&� "��. *� *�#�"�� ���
PPO Option� Employee Cost�Employee Only*� $0.00Employee + Family� $12.57*No cost for Employee Coverage if enrolled in the health plan
DMO Option� Employee Cost�Employee Only*� $0.00Employee + Spouse� $2.60Employee + Child(ren)� $3.19Employee + Family $5.78*No cost for Employee Coverage if enrolled in the health plan
2016 – 2017 Premium per Pay Period

19 | P a g e
��**Dental benefits and dental insurance plans contain exclusions and limitations. Deductible, coinsurance and annual plan maximums may apply.
Summary of Benefits Guardian DMO
Guardian PPO
� ManagedDentalGuard
Network�
DentalGuard Preferred Network
� Designated Network Participating
Non-Participating
Annual Deductible*� � �Individual� None $50* $50*Family� None $150 $150
Annual Benefit Maximum� None $1,000 $1,000 Orthodontic Services� $2,500-$2,800 50%** 50%**Orthodontic Deductible� None None NoneOrthodontic Lifetime Maximum� None $1,000 $1,000
*The deductible applies to: Basic & Major services only� ��**Orthodontia is covered only for children (appliance must be placed prior to age 19).��
��
Partial List of Services Guardian PPOManaged
DentalGuardNetwork
DentalGuard Preferred Network
Preventive Designated Network Participating
Non-Participating
��
Oral examinations � $5 100% 90% ��Cleanings Adult/Child� $0 100% 90% ��Fluoride � $0 100% 90% ��Bitewing X-rays � $0 100% 90% ��Full mouth series X-rays � $0 100% 90% ��Sealants (per tooth)� $0 100% 90% ��
Basic ��Anesthesia**� Exclusions
Apply80% 70% ��
Root canal therapy, molar teeth� $120-$270 80% 70% ��Amalgam fillings � $0 80% 70% ��Scaling and Root Planing (per Quadrant) � $0 80% 70% ��Surgical and Simple Extractions� $0 -$30 80% 70% ��Repair & Maint. Of Crowns, Bridges &
Dentures�$36-$155 80% 70% ��
Major �� ��Crowns� $375-$395 50% 40% ��Full & partial dentures� $381-$575 50% 40% ��Inlays, Onlays and Veneers+� $265-$370/Unit 50% 40% ��
Certain services may be covered under the Medical Plan. Contact Member Services for more details.**General Anesthesia – restrictions apply. +Covered when needed for decay or injury and amalgam cannot be used. The DMO copay is per unit placed.�

20 | P a g e
VVision Insurance – EyeMed 0�*�����/�� ���=���>�������)�������� � � �����www.eyemedvisioncare.com�
2.�2�����"�!��������""�*�����������&�� * ��� �*������#�����.����.�'&(%�5 * ���0�����2.�+�" �*�������� �%� ���� ���#��*�*��.�'&(%�*�����&��"� �" �*�"�����"����%*�� #� ����"��.���#�&*:���������*:�% *�����*:�3���* ��*���%�� � ��� ��*����
�
���*������.����.����������"����.��������� ��**� ��� "���*� ��*�� ��� � Q%������� � ���2.���������� *����&� ��� �� �� ���� �� �� ��� ����.�#� �%��2.�+�" �*�������� �*%������#����&����������%���&���
Network for Providers is Advantage; Retailers include Lens Crafters, Pearle Vision, Target and more!
Visit www.eyemed.com and click on “Find a Provider” select your network “ADVANTAGE” and add the zip.
Frequency
Examination Lenses or Contact Lenses Frame
-�����&��������.*� � �-�����&��������.*� � � -�����&��������.*� ��
�
���
�
Tier of Coverage� Employee Cost�'�#��&�-��&� M)�)��'�#��&�O�/#��*� M��)��'�#��&�O�0. �%=��>� M�����9�� �&� M�����
Exams and Frames In Network Out of Network -Reimbursement
'&�'3���� �.�, ��� ����*�B�**��&� M���0�#�&� G#����M)���/���%��%�0�������!�*�9 ��7�9������G#� G#����M��� BA����� ���0�������!�*�9 ��7�9�����G#� ��N��""���� ��#� �� BA��
�9���*� M��0�#�&�M������������I���N��""���� ��
#� ������M����G#����M���
Lenses � �/ ����5 * ��� M���0�#�&� G#����M���+ "����� M���0�#�&� G#����M���2� "����� M���0�#�&� G#����M���Lens Options � �G5�2������� M��� BA��/���%��%����&��� ����� M)�� BA��Contact Lenses � �0����� ����� M�)����������I���N��""���� ��#� ������
M�)��G#����M����
, *#�*� �� M�)����������I�#��*� ����������M�)�� G#����M���(% ����&�B�**��&� M��0�#�&:��� %� ��9���� G#����M����Laser Vision Correction � �!�/6L�����8L�"����G�/��!�*��B����@� ��N��""���� ��#� ������N��""�#����� �����#� �� B��
2016 – 2017 Premium per Pay Period

21 | P a g e
FFlexible Spending Account – Eagles Benefits by Design, Inc.
The Town of Lantana offers a Flexible Spending Account (FSA) administered by Eagles Benefit’s by Design. An FSA is an Employer-sponsored benefit that enables you to pay for eligible medical expenses on a pre-tax basis, such as deductibles co-pays, vision and dental. An FSA saves you money by reducing your income taxes. And contributions you make to your flex spending account are deducted from your check before any of your taxes are calculated and are never reported to the IRS. The overall result? You decrease your taxable income and increase your disposable income which can save you hundreds or even thousands of dollars a year.
If you expect to incur medical expenses not reimbursed by your current health insurance, you should definitely think about participating in an FSA.
The IRS regulates the rules that surround FSAs and the money that can be used from them. A short list of eligible expenses is provided on the following page.
There are two types of FSAs offered by the Town of Lantana:
Health Care Flexible Spending Account Dependent Care Reimbursement Account
���.���.�����9/������� � ��*�&������.�#�&���#�&�"���� � ��.���.�����3#�**���������%� &�&����.���.�#�����2.�#��� ����"�&����#�&�.�@�&���#��� ����&����9/�� *���@������ "���&���#�&�"%���� �������3*:�/�� ���/��� �&� ��3*���%���*��*������3*��6�K*����������&����*������&����$�����&:������ �� ��*�&�����@� ���&����9/���������*� D������"%���� �������3*����*�� ���*��� �&���3*��6�� ��*�� �*����*:� �.�� ��� ��� *���� ��3*� ��@�� ���� �.���2.��������&�����&�*���%#�%*��#����2.��������&���#��� ����&����9/��2.� ��3� #������� &��� ����%� �������&� #�&� ��� �.������&�=��3� ���@�>��2. *���������� ���������&������*���* %������������#����������������3 �����"�M�:����#���#��&�%�� ��� � � ���=���. �>������������#������������������'� � ��'3#�**��1�� ��� D�*�� *��� 3#�**� &��� ���� #�&� � �.� &����.���.�����9/����
�� 1���.�#������#�&*���%������� ,��������@���%����.�%��� ���� ,�����K*�"*��� '&�3��*���%�&���***��� 0���������**���%�*�� ��*���� ���
���%#�%�������9/�� *����������&����#�&�%#�%������� 3#�**� ��%� ����� &���� ��3� �� ������ 1�K*�.��� �����@*����4��� % ���� #���� �"� &���� "����3� #�&� ���� �� *#� ��������������.�#�#�&����@����%�%#�%���������*�*�4��������*�&�������������.����.�����.�&������.�#�#�&�"���� � ��3#�**�4����3#�*���*�� � "��� �.�#��#�*��"������ ��� &�����%:� "����� %:�&����*#��*���� ��#��&*�������%#�%�������9/��.�#*�� � ��*�&���"����.����@����%� ��*�� �"� ���� "��� �� J��� "& ��� %#�%���� ��J��� "& ���%#�%��� *��
�� ����3�%#�%����"�&���*��.�� *���%������)�:����
�� ��&� ��.�� ��3� %#�%��� �"� &���*:� *��.� �*� ����%��&� #����:� �.�� *� #.&* ����&� ��� ������&� ���#� ���"�*�"������%�.�*��.�*���#� �� #���* %����*�&���
�� ��*#��*��.�� *�#.&* ����&����������&� ���#� ���"�*�"������%�.�*��.�*���#� �� #���* %����*�&���
������

22 | P a g e
�� 1�� ���� %*��� 0. ��#���� ������������ !� ������&�"*��� ������ ��-���.������� ��*��� ��*�� #� ��*��� (�����.���.�����*� ���
�����3#�**���*�� �J��� " %��% ���:�� * ��:�#.�����&����%����� �" ��3#�**:��*�%" �%� ��/�� �����)=%>��"��.�6�������8����0�%�����
2.�6�������8����/�� ��� � �*��.��������&�������#��� ������%#�%�������9/�:��#�����
�� M�:����#��&��:� "� &���������� %���%� " � �����D� ��������:���� "�&��������* ����#�����
�� M�:���� #�� &��:� "� &��� ��� ���� %� ��%� " � ���*#�����&�
�
*NOTE: �G�� @���.���.�0���9/�:�&���� ������&� �� � ��*%��#�����.���������.���.�*� ��%%���%�"����&����#�&�.�@�"���,#�%���0���3#�**��
�
4�����&��������#��� � #��� �� �.�����9/����� ��.�* ��������*�&���2�����������&����#��#�&������ �� ��:�* �#�&���@�&����������#����&���9/����� ��=*>����������%�% � %��.��� &��.���� ���"� �" ��#�&�����%%��� ��*�=��>����
Just remember this: FSA dollars are "use-it-or-lose-it" funds. Account balances cannot be carried over from year to year. If you have any unused funds at the end of the plan year, or at the end of any applicable grace period, those funds will be forfeited. That is an IRS requirement. So be careful when estimating how much you want to be deposited into your FSA.
SSupplemental Insurance – Aflac & Liberty National The Town of Lantana offers supplemental insurance through Aflac and Liberty National. Supplemental insurance is extra or additional insurance that you can purchase to help you pay for services and out-of-pocket expenses that your regular insurance does not cover.
Some supplemental insurance plans will pay for out-of-pocket medical expenses, such as deductibles, copayments, and coinsurance. Other supplemental plans may provide you with a cash benefit paid out over a period of time or given to you in one lump sum. The cash can be used to cover lost wages, transportation related to your health condition, or used to pay for food, medication, and other unexpected expenses you have due to an illness or injury. For more information or to enroll in our supplemental programs, contact the representatives below:
Hamida Trainor - Aflac Susan McCray - Liberty National
561.718.3577/[email protected] 954.562.7618/[email protected]

23 | P a g e
LLife and AD&D Insurance – Mutual of Omaha
Basic Life and Accidental Death & Dismemberment 2.�2�����"�!�������#��� %*�+�* ��! "� �*�������.����.�(�������"�-��.���������� � ���#��&*���������*������.��#��&���2.� �* ��� "� �*������ �" �� *�M��:����"�������� � ��"���� ���#��&*��2.�2�����"�!���������*��#��� %*���� %�����,��.�7�, *�� �����=�,7,>�� "� �*�������. �.�#�&*� ���%% � ��� ��� �.� �* �� �" ���.��%��.������*��*��� �*�����"������� %���� �2.��,7,� �" �������������.*��.� �* ��� "� �" �����������%���#��� ��� *���*��#�&� �� �*%�����.�*�.%��� �����
The AD&D benefit will be paid for the loss of:� One half the AD&D benefit will be paid for the loss of:��
�� ! "�=��� %����>I������ +��.�.��%*���� ��.�"�I������ / �.���"� ��.�&*:������ ��&�����������I����"���:����.��%:�����.�
* �.���"����&�
��� -��.��%:������ -��"���I������ / �.���"����&I������ 2.�� ���%� �%3�" �����"��.�*���.��%�
The Basic Life and AD&D life insurance benefit amount reduces 35% at age 65, and reduces an additional 25% at age 70 and further reduces an additional 15% at age 75. �
Voluntary Life Insurance – Mutual of Omaha 2�����"�!��������#��&*���&��������#���.�*��%% � ������ "� �*�������������������&� �* *��.����.�(�������"�-��.��� ��#�&�����%%��� ������%% � ������ "� �*��������&� �#���.�*%���������&���*�"����% ""���� �" �����*��*�%*�� %� ������8��*�"����%% � ������ "� �*���������&�"����.��#��&� �*%���������%���#�� ��������� ����&� �� �� �%�"����1�����8*����*���� ������� �%� ������/��������
�� 4�����&�*�����%% � ����:��#��&#� %�� "� �*������J�����#������� �*�&�����������*����&� ��M��:���� ������*��������3 �����"�M���:�����
�� G#����M���:�����"�������� *��������%� **�:�����% ����J�*� ���� ���%%�=���. �*����&>��6"�&���% %�����������������.�� ����*�" �*���""�%:�&���� ����%�������#������% ����J�*� ���� ����%����*� D��������%��� � ���'� %����"�6�*��� � �&�='-6>���
�� 0�������%��*� &�)�N���������:�����%% � �������N������������%�����%% � �������N�����������
6"�&���� *.�������������#���.�*���. �.����������"����������%�&������#�*��&���� � � ������������� � � �&�#� �%:�&�����*�����#������% ����J�*� ���� ���. �.�&�������� �� ��"����1�����8*����*����
� � ��������������� � � � � �� �
24 | P a g e
Voluntary Dependent Life Insurance – Mutual of Omaha 2.�2�����"�!��������#��&*���&���*���������#���.�*�%#�%���� "� �*�������������������&� �* *��.����.�(�������"�-��.��� ��#�&�����%%��� ���� �,#�%��� � "� �*��������&� �#���.�*%���������&����*#��*���%A����. �%������% ""���� �" �����*��*�%*�� %� �������
�� 4�����&�*�����%% � ����:��#��&#� %��%% � ������ "� �*������"���&����*#��*� ��M�:���� ������*�
�� 2.� �" ����������������3�%���N��"��.��#��&�#���.�*%� �" �����������'3��#�I� "��.��#��&�#���.�*%�����%% � �����M��:�����"�������:��.� �" ���������"����.�*#��*��������3�%�M��:����
�� G#����M)�:���� *��������%� **��"����.�*#��*�=���. �*����&>���6"�&���% %�����������������.�� ����*�" �*���""�%:�&���� ����%�������#������% ����J�*� ���� ����%����*� D������'� %����"�6�*��� � �&�='-6>�
�� 0. �%������%�&*����������.*����� �����%�"���M������ 0. �%���������.*�������&��*����� �����%� ��M�:���� ������*��������3 �����"�M��:����
6"�&���������* %��"�&���� � � ���� � � �&�#� �%:�&����*#��*���*�����#������% ����J�*� ���� ������J�*�������������
Short Term Disability – Mutual of Omaha 2.�2���� �"� !������� #��� %*�/.���2���, *� � �&� =/2,>� �*������ �.����.�(������ �"�-��.�� ��� ����� � ���#��&*���������*�� ��� �.��#��&�� �2.�/2,� �" ��#�&*�&�����#��������"� &�������**��@�&���� ��*� "�&��� ����% *� �%�%����� �D��&����* �@�**�� ���*�����&��"� �.�#���;*� �" �*� *�#��� %%� �����
�� 2.�/2,� �" ��#�&*���N��"�&�����@�&���� ��*��#�������@�&���3 �����"�M�:������ ����#��&���*�� �% *� �%�"�����%�&*�#� ������ ��� ���� � ��"����.�/2,� �" ���� 2.�/2,� �" �� � �*�����.���.�%�&��"����.��#��&�3#� ��*��.�% *� � ��������� 2.�/2,� �" �� *�#�&� ��"����#�����)��@*�
Voluntary Long Term Disability – Mutual of Omaha 5�������&�!���2���, *� � �&�=!2,>� �*������ *��""�%��.����.�(�������"�-��.����%���� �� ���������� � ���#��&*��2.�!2,� �" ��#�&*�&�����#��������"�&�������**��@�&���� ��*� "�&��� ����#�������&�% *� �%�%����� �D��&����* �@�**��8��*�"����#� �����!2,� �*���������&�"����.��#��&� �*%��������������� ���"��.� �" �� *� �����
�� 2.�!2,� �" ��#�&*���N��"�&�����@�&���� ��*��#����������.�&���3 �����"�M�:������ ����#��&���*�� �% *� �%�"������%�&*�#� ������ ��� ���� � ��"����.�!2,� �" ���� 2.�!2,� �" �� � �*�����.���*��%�&��"����.��#��&�3#� ��*��.�% *� � ��������� 2.�!2,� �" �� *�#�&� �����������

25 | P a g e
EEmployee Assistance Program through Counseling Services Associates
2.�2�����"�!�������#��� %*���������*�:������#�.�* ��'�#��&��** *�������������='��>�� 6�� *���� �� �����&�����%���.��� ���"�&����"�� �&��.����.�0���*� ���/�� �*��**�� ��*���2.�'����""�*�&������**����#��� %�*��.������ ��*%������� " %� ���. ��*#� ���&�" �%*���%�� ���*�&���� �. �����������.���*��"��.������%#�% �������.�*�� �&��"��.�#�� ������****������%��"�����*�� �*������*����� �� �����&����"�� �&��� �*��'����.���.�'��� *�#� %� &��.�2�����"�!������:�'���#��� %�*���*��"���������" %�� �� �&��� %� �*I���&� �"����� ���&���% *���*�� ������ �����" %�� ������**�&������.�� Q� �*����*���'���*�� �*� ����%��
�� 2.���"" ��� * �*�#���#��&��� -���"" ��� * ��"���%#�%��*��� ��������.�����%�%���������� ��*��������.������ / 3���.����*��**����������*** ��*�#��&����� ���**��������.�&�%���� �����#������*��� (�� ��� ����"���������������%�� � *�"������&����� /���/�/�6������� ��*�"�������.��A%����� �*�,G6��"����*��� 8"�����*�� �*������*��J��� �&�� ��%A��*��""�� �����* %�#������*��.����**��&��� 8%��%�"*�"���#*&�. ��� ����%�*� *����*�� �*�#������*���%�%�����*���� '�%��0���6**�*��� (�D���� "����*� ����% ��� ��.*:���� %��*:���%�%��.*�
��Contact information: Call (561) 272-8880 �Visit website at���������*� ��*�� �*�**�������������
����������������� ���

26 | P a g e
Compliance Notices 2016-2017
Patient Protection:
�6"��.�$���#�1���.������������&��J� �*��.�%* ���� ����"���#� ���&�����#��� %�:�&���.����.�� �.�����%* �������&�#� ���&�����#��� %���.��#��� � #��*� ���.������@���%��.�� *���� �� ��������#��&������&����"�� �&��� �*��9����. �%��:�&�����&�%* �������#% ��� � ����*��.�#� ���&�����#��� %�����4���%�������%�#� ������.�� Q�� ���"�����.����� �����"������&���.��#�*���= ����% �����#� ���&�����#��� %�>� ����%������ �� �����**����� *��� ��������&������ ��������"������.���.�����#��"** ����� ���.������@��.��*#� �� Q*� ��� *��� �*�����&������&��2.�.���.�����#��"** ����:�.����:���&� ��J� �%�������#�&�� �.����� ��#���%��*:� ����% ���� �� � ���#� ������.�� Q�� ���"������� ��*�� �*:�"����� �����#��##���%���������#���:����#���%��*�"�����@ ����"����*����9������ *���"�#��� � #�� ���.���.�����#��"** ����*��.��*#� �� Q� ��� *��� �*�����&������&:����"��� �"����� ������.������*������#� ���&�����#��� %�:���%�"������ *���"��.�#��� � #�� ���#� ���&�����#��� %�*:����������.�������%� � *�����������"������.����� ��� * �����6�� *�&�����*#��* � �&�����*����.����.� �"����� ���#��� %%����&�����##� ��� ���"���������� *�����������%����#������&��� ** ��*���� ��������*������*���%� &�&������&�����##� ��� �����&� ���� %���&������������2.����� ��.�*��.�� �.������*� �%������������.� �* *��"�"���%����� *�#�*���� ����
HIPAA Special Enrollment Rights:
6"�&������%�� � ������������"���&���*�"���%�&����%#�%��*�= ����% ���&����*#��*>� ���*��"���.��.���.� �*�������������#�.���.�������:�&�����&� �� �����������&���*�"���%�&����%#�%��*� ���. *�#���� "�&������&����%#�%��*���*�� � � �&�"����.�����.���������=��� "��.��#��&��*��#*������ �� ��������%�&�������&����%#�%��*;���.��������>��1����:�&�����*���J�*������������ �. ��)��%�&*��"���&�������&����%#�%��*;���.����������%*�=����"����.��#��&��*��#*������ �� ��������%��.�.���.�������>���
The Newborn’s and Mother’s Health Protection Act:
$���#�.���.�#���*���%�.���.� �*������ **��*�������&���&����:���%��9%�������:��*�� ��� �" �*�"�����&�.�*# ��������.��"�*��&� �������� ���� �.��. �% ��.�"����.����.������� �����. �%�����**��.������.���*�"����� �������� ����%� ��&:�����**��.������.���*�"����� ������*�����*�� ����1����:�9%��������������&�%�*�����#��. ���.����.�K*������ ���K*�����% ���#��� %�:��"������*��� ���� �.��.����.�:�"����% *�.��� ����.����.�����.���� ������� ���.������.���*�=������.���*��*��##� �� �>��6����&���*:�#���*���%� �*���*���&����:���%��9%�������:��J� ���.�����#��� %��� �� �����.�� Q�� ���"�����.�#��������.� �*����"���#�*�� ���������.��"�*��&����������.������.���*�=������.���*>��
����������

27 | P a g e
����������� ������2.����������*�"������� ��%��������"���%#�%����. �%����.���������%���%��&��������#�.���.�#�����*���*��%��� "��.&���*��. ��*��%���*����*� ���*��"����% ����&���**��&������"�� *���"����*�.�����2. *������##� *�����% ����&���**��&����*��"�� *����.��� � ���������"���C�����&��:��������6"�&�����. �%� *������������*��%��:��*�%" �%� ��&����0�� " �����"�0�����:� ���*�.����*.� *�������% ����&���**��&������"�� *��:�&�����. �%���&����� ������ �����%���%���.�#����"����#�������&���"�����.� � �� ����"��.������"�� *����2. *����� ��%���������##� *� "�&�����. �%���*�=�>�����%���%���.�#������%�=�>������%��*���*��%��������#�*�*���%��&�%���� ����� �*� ��� ���= ����%*������*:��� ��* � *:�*������%�*�.���*���%����� ����.��#�*�*���%��&� �*� ��� ��*>����2.�2�����"�!�������� ����J� ������ ������� " ��� ���"�����.��. �%K*�#.&* � ����.���*���*��.����.��. �%� *�*�""� ���"������*� ��*� ���**���� �D��&���%��.����.������"�� *��� *��% ����&���**��&���������������������������������������������
�������������� � �������������������������������������������������� ����������������� �������������������������� ������������������ �!�����"#�$� ����������� �����������������% ������������������� ���&�������' �������������� ����� ���������������������&�����������������'���������������'��������� (���
�� ������������� ������ ��������������� �������&�������������������&��'� �� ������� )� �� ����� ������ ������������������ �� �������' ������������� ����''� ������� * ������������ + ����������'����������'����������������������������������������'�����#��
�+��������������&�������' ���������,������������������������������������ ����''�������������� ������������� ��������������' ���������� ������'��#�
������������� ���

28 | P a g e
�Premium Assistance under Medicaid and the Children’s Health Insurance Program (CHIP)
6"�&������&�����. �%������� � ��"���(% �� %����016����%�&��;��� � ��"���.���.��������"����&�����#��&�:�&����*������&�.�����#�� ����** *�����#��������.�������.�#�#�&�"���������:��* ���"��%*�"�����. ��(% �� %����016��#������*��6"�&������&�����. �%������;��� � ��"���(% �� %����016�:�&������;�� �� � ��"����.*�#�� ����** *�����#������*� ���&�����&� �� ����� �&� �% � %���� �*��������������.����.��.�1���.�6�*������(��@�#�����9������� �"����� ��:�� * � www.healthcare.gov��
6"�&������&����%#�%��*��������%&������%� ��(% �� %����016����%�&���� �� ����/����� *�%� ���:���������&����/����(% �� %����016���"" �����" �%����� "�#�� ����** *����� *���� �� ���
6"�&������&����%#�%��*����B-2��������&������%� ��(% �� %����016�:���%�&����. �@�&��������&��"�&����%#�%��*�� �.�� �� � ��"��� �.���"��.*�#������*:���������&����/����(% �� %����016���"" �����% �� 1-877-KIDS NOW��� www.insurekidsnow.gov����" �%�����.�������##�&��6"�&���J��� "&:��*@�&����*���� "� ��.�*���#��������.���� �.��.�#�&���#�&��.�#�� ��*�"�������#��&�*#��*��%�#�����
6"�&������&����%#�%��*����� � ��"���#�� ����** *�������%��(% �� %����016�:��*������*�� � ����%��&�����#��&��#���:�&�����#��&����*��������&������������ ��&�����#��&��#���� "�&������;������%&������%��2. *� *�����%���E*#� �����������F��##����� �&:���%�you must request coverage within 60 days of being determined eligible for premium assistance��6"�&���.���J�*� ��*�� ��������� ��� ��&�����#��&��#���:����������.�,#��������"�!� ����� www.askebsa.dol.gov�������� 1-866-444-EBSA (3272)��
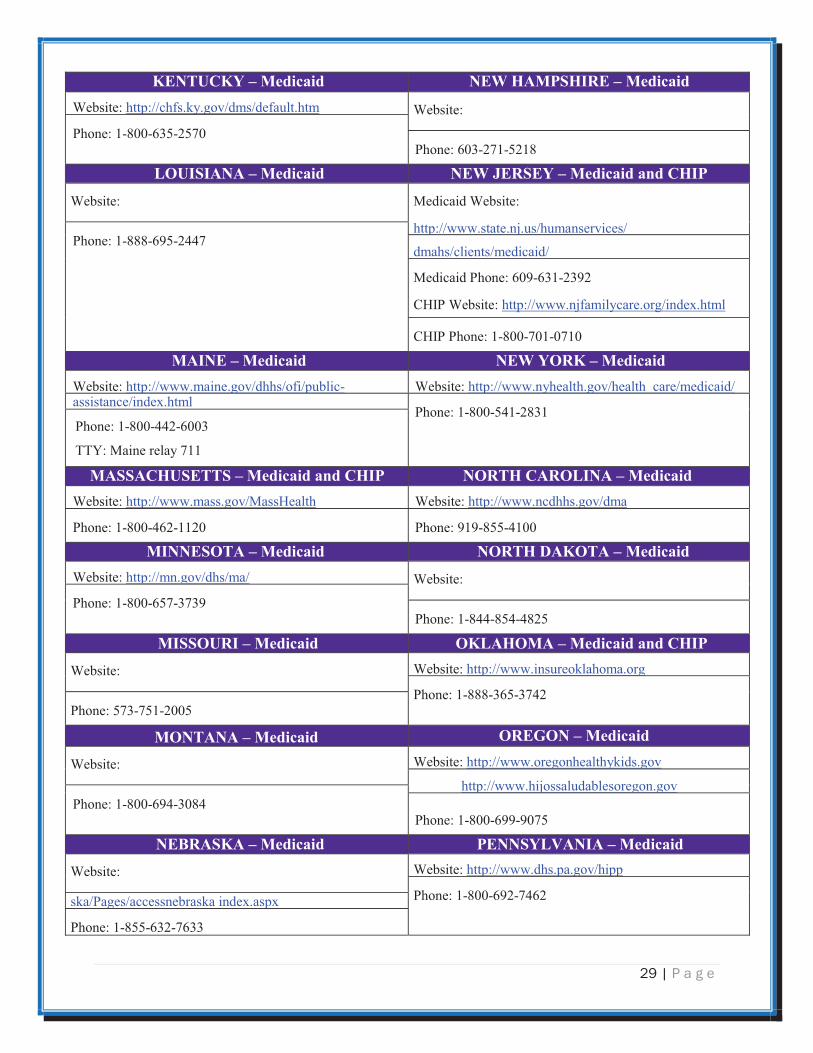
If you live in one of the following states, you may be eligible for assistance paying your employer health plan premiums. The following list of states is current as of January 31, 2016. Contact your State for more information on eligibility –
�������� ���������� !"#�!$�� ����������? * ���.��#�AA�&��. ##����A� ? * ���.��#�AA%�.����� �����A�% �� %��
�.���������������� �0� �@����1���.�6�*��������� �����&����
=16��>��.������������������%&�� ���������� $'($�'�� ����������
? * ���.��#�AA.���.�.**�*�����@��*A%#�A#������*A�% �� %A��
1���.&�6�% ���������"������ ������%���*�
�����? * ���.��#�AA����. #� �������
�.���=-��* %��"����.����>������)��
������.���=���.����>��������������.���������)������
������.��(% �� %�? * ���.��#�AA���� �% ����% �� %������
�.���������)������#�#��(#� ���������� $#��� ����������
-��������������(����'(..&&&#���� ��#��.��'��� �������(����'(..&&&#���#����#�#��.��''.��
-�������������� ������������� (��% //%00�%1�21� *����(��% %123%�430�
)�#�$(�� ���������� &�'%�%� ����������
�������(����'(..����������'� ���� �#���.��''.�� �������(����'(..&&���5�#��.���.��
*����(��% 66%146%103 � *����(��%6 4%0�3%14�0�
29 | P a g e
�&"'*+�&,� ��������� '"�����-%�$�"� ���������
�������(����'(..����#5�#��.���.������#���� �������(
*����(��% //%314%046/ *����(�3/1%06�%40�
�#+$%$�'�� ��������� '"��."�%",� ����������������$-
�������( -��������������(
���'(..&&&#����#�,#��.������ ����.� *����(��% %3�4%0226
����.�������.�������.
-�������*����(�3/�%31�%01�0
���*��������(����'(..&&&#�,������ �#� �.����7#�����
���*�*����(��% //%6/�%/6�/
��$'"� ��������� '"��,#�&� ��������� �������(����'(..&&&#����#��.����.���.'�����%� �������(����'(..&&&#�������#��.����� � �.�������.� ��������.����7#����
*����(��% //%42�%0 1� *����(��% //%220%3//1��
++9(�-���� ����6��
��%%���+%"**%� ����������������$- '#�*�����#�$'�� ��������� �������(����'(..&&&#���#��.-�������� �������(����'(..&&&#������#��.���
*����(��% //%230%��0/ *����(����% 44%2�//
�$''"%#*�� ��������� '#�*��(�&#*�� ��������� �������(����'(..��#��.���.�.� �������(
*����(��% //%346%161� *����(��% 22% 42%2 04
�$%%#+�$� ��������� #&���#��� ����������������$- �������( �������(����'(..&&&#���� ��5����#� ��
*����(��% %134%1620 *����(�461%64�%0//4
�#'*�'�� ��������� #�"!#'� ���������
�������( �������(����'(..&&&#� ����������5���#���
���'(..&&&#��,����������� ����#��� *����(��% //%3�2%1/ 2
*����(��% //%3��%�/64
'"���%&�� ��������� -"''%,�/�'$�� ��������� �������( �������(����'(..&&&#���#'#��.��''�
*����(��% //%3�0%6230 �5.*���.�������� �5�����7#�'7
*����(��% 44%310%6311

30 | P a g e
�
'"/�(�� ��������� ��#("�$%��'(� ��������� -��������������(����'(..�&��#�#��. �������(����'(..&&&#�����# �#��.
-�������*����(��% //%��0%/�// *����(�2/�%230%41//
%#+*�����#�$'�� ��������� /$�!$'$�� ����������������$- �������(����'(..&&&#������#��� -��������������(
*����(��% %42�%/ 0/ -�������*����(��% //%210%4�02
���*��������(
���*�*����(��% 44%020% 0 0
%#+*��(�&#*��0��������� ��%�$'!*#'� ��������� �������(����'(..���#��#��� �������(
*����(��% % 0 %//4� 7#�'7
*����(��% //%430%1/00��7�#��4261
*"1�%� ��������� �"%*�/$�!$'$�� ��������� �������(����'(..�����''��7�#���. �������(
*����(��% //%22/%/2�1 �.������#�'7
*����(��% 66%4� %4 0/���-)�+�� ��* ���=�������
+*��� ����������������$- �$%�#'%$'� ����������������$-
�������(
-������(����'(..�����#���#��.��������
�������(
���'�(..&&&#���#&��������#��.'����������.'�.'�//�4#'���
���*(����'(..�����#���#��.���'� *����(��% //%130%1//0
*����(��% 66%421%633�
/"��#'* ��������� �,#�$'!� ��������� �������(����'(..&&&#� ����������� �#� �. �������(����'�(..&��>������ �#��%���#���.
*����(��% //%04/% 206 *����(�1/6%666%641�
+���������������� ����������������' ���������������' �� ��������?�� ��1���0/�3��� ��� ��� ������ ����������'������� �������� ������������������� (
@#)#�A�' ���������=�� � @#)#�A�' �����������������������)� ����
<�'������B��������)��� ������������ ����� ����� ���� �-���� ��C�-�������)� ����
2���2��34�5�� 2��2��2��3�

31 | P a g e
MODEL INDIVIDUAL CREDITABLE COVERAGE DISCLOSURE NOTICE LANGUAGE OMB0938-0990 FOR USE ON OR AFTER APRIL 1, 2011
$�6�������'�����������*� ��������������5�7��,�7��-�����6�����(�7����3�������������������
�*����� ���������������� ����������5��'����&�� ����������������#�+������������������ �������������� ��� ����' ��� �'������ ������ ���&�����<+:������������� ��'���������� �-���� ����' ��� �'������ ������ ��#�+�������� ������������'������������&����� �� ���������&������,�����-���� ��� ���'��#�������� ��������� ����,����������������������' ����� ��� ������� ��������������&������ ���� ����� �����&���������&����������� �������������������'�������� ����-���� ��' ��� �'������ ������ ��������� � �#����� �����������&�� ����������������'�����5�������������������� �' ��� �'������ ������ ������������������������������#���*���������� ����6�������������8�7���������9�� ��5�7��8�7���7��������3�������������������6�����6�������7����3����������#�-���� ��' ��� �'������ ������ ������������������0//3������ �����&����-���� �#�9������������������ ����������,�����-���� ��* ��� �'�����A ���*���� �,�����-���� ���������*���!��5�����-D�� �**D"��������� ��' ��� �'������ ������ ��#�����-���� ��� ���'����' ����������������� ������������� ����������-���� �#�)����'��������������� ��� ����� ����� ������� ���������' �����#���0#�+���+�&�����=����������� ��������������' ��� �'������ ������ ������� �������<+:���������� ����� ����'���' ����'������7'���������'������������������� ��-���� ��' ��� �'������ ������ ���'������������ ��� ��������� ���� ����������� ��#�B��������� ��7���������� ������� ����������� �����������5��'��������� ����������'�������� �' ������!�'�����"����������� �����������,�����-���� ��� ���'��#������������,�7�.���������������(�7��-���:���9������,�����-���� ��� ���'���&���������� ��������������������� �-���� ����������� �� ���D����� ��4����� �����A������ �6��#����&�� ����������������� ��� ����� ��������' ��� �'������ ������ ������ ������������������� ��&�������&���������������������� ���&��!0"�������)'�����<� ��������*� ����!)<*"����,�����-���� ��� ���'��#����������66���*��,�7���7��������3������$��,�7�(���������.���������������(�7��-���:��������������������,�����-���� ��� ���'������� ��� �����<+:����� ���&������������������#����������������������,�����-���� ��� ���'������� �'���� ��� �����<+:����� �������& ���������������� ���'������������������������������������� �����5#�������������,�7�-�8����������-����7��;-�����8<�*��.���������������(�7��-���:��9��������������5��&������������� �'�� ��������� ��� ������� ���&�����<+:�����������,�����-���� ��� ���'���&������31������������������� ���� ��� ������� ����������������'�������� �' ������!�'�����"����,�����-���� ��� ���'������ #�

32 | P a g e
$�6�������'�����������*� ��������������5�7��,�7��-�����6�����(�7����3�������������������;������7��<�
�����������31����������������� ������ �&�������� ��������' ��� �'������ ������ ������� ���������' �������������'������������;��������-���� �������������� ��' ������'� ��������� ��� ���������������������������������� ��#�$� ��7�'������������������������������&�������� ����������� ������� �' ����������������������������������;������ ���������-���� �������������� ��' �����#�9������������'������������ �' ������!�'�����"�����������������-���� ��' ��� �'������ ������ ��#��������������������������&������������������&����D����� ����,���#���)��������$������������5�7��*���'������#��,�7���7������-�����6�����(�7����3�����=��������������'� ���������������&��� ��� ��� ����� �����#�'#*"��9���������������������������� #�9���&������������������� ��������7��'� �����������,�����-���� ��� ���'������������������ ����� ������<+:��������#�9���������� �>��������'��������������������������#���)��������$������������5�7��,�7��#6�����+��������������-�����6�����(�7����3�����=���-� �������������� �����������-���� ��'������������ �' ��� �'������ ������ �������������E-���� ��C�9��F�������5#�9�������������'���������������5�������������� ���� �� ���-���� �#�9������������������������ ���������-���� ��� ���'���#��)���������������������5�7�����������6�����6�������7����3��������
�� G����� 2��������2��3���� ������� �)�������������� ��������������* �� ��!�����������������5���� ������� ���'�����
����E-���� ��C�9��F�������5��� ����� �����'���������� "��� �'� �����H������'���� �����% //%-<A����<�!�% //%311%2006"#�++9���� ��������������% 66%2 3%0/2 #���� ���������������������������� ���� ������7� ����'�'������� �-���� ��' ��� �'������ ���
��� �����������#�$� ����� �����������������7� ����'�������)�����)��� �����������&����� 2�������7���82��3��� �������������% //%660%�0�1�!++9��% //%104%/66 "#��
�����5����&��6������������5�����3������������2�$��8�7�����������>��������������������������7��6���?�8�7���8�5����@7��������6��3��������68��������������� ����8�7�>��������� � ��������������8�7���3��������������������5�����3���������?����������?� ��������������8�7�������@7��������6�8����������6����7��;��6�����8<2���
A��(�D����� ������0/�3��������.D�����(�-����9�����
:������<�����.)���� (*� ���������������� ���(�ABB�!��8��������������������)���(���������?�)��*�����:���� (�AC�0ADB0ABB��
CMS Form 10182-NC Updated April 1, 2011
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0938-0990. The time required to complete this information collection is estimated to average 8 hours per response initially, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. If you have comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.

33 | P a g e
New Health Insurance Marketplace Coverage Options and Your Health Coverage�� � ��
PART A: General Information :
What is the Health Insurance Marketplace?
Can I Save Money on my Health Insurance Premiums in the Marketplace?
Does Employer Health Coverage Affect Eligibility for Premium Savings through the Marketplace?
How Can I Get More Information?
�
Form Approved
OMB No. 1210-0149 (expires 1-31-2017)

34 | P a g e
Notes:
_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

35 | P a g e
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________�
�

36 | P a g e
�
�
�
����������
�
�
�
�
����
�
��#��%� &��
�
�����B�������
3//��� '� ���A ����)�����1/4�
$� ��=��� �����$=#�11112�
+����$ ��(��# //# 33#6/06�
$7(��42#660#// /�
���������������&&&#����������#����
�
�
����