thromboembolism in pregnancy - health collaborative in pregnancy subhashini ladella, md, facog...
TRANSCRIPT
Thromboembolism in pregnancy
Subhashini Ladella, MD, FACOG Associate Professor, UCSF
Department of Ob/Gyn, UCSF, Fresno Medical Director
Maternal Fetal Medicine Community Medical Centers, Fresno
Objectives
1. Overview of VTE in pregnancy
2. Diagnosis of VTE in pregnancy
3. Risk assessment of VTE in pregnancy
4. Management of VTE in pregnancy
5. Risk reduction with thrombo-prophylaxis during pregnancy?
6. Treatment of Thrombophilia in pregnancy?
RCOG: Guidance questions to be considered
1. What are the risks of anticoagulant use during pregnancy?
2. What are the risks of anticoagulation in breastfeeding women?
3. How is venous thromboembolism during pregnancy treated?
4. How is pregnancy-associated VTE prevented?
5. How is peripartum anticoagulation managed?
California Toolkit
The major components of the California Toolkit to Improve Health Care Response to Maternal Venous Thromboembolism (VTE) include:
1. Risk assessment
2. Suggested prophylaxis and treatment regimens
3. Anesthesia and Analgesia considerations
4. Patient, provider and nursing education materials
5. Implementation strategies
CMQCC Guidelines Resources
• National Partnership for Maternal Safety (NPMS),
• American College of Obstetricians and Gynecologists (ACOG),
• Safe Motherhood Initiative (SMI),
• American College of Chest Physicians (ACCP),
• Royal College of Obstetricians and Gynaecologists (RCOG)
• American Society of Regional Anesthesia and Pain Medicine (ASRA).
Background
• VTE is a leading cause of severe maternal morbidity and mortality.
• PE accounts for approximately 15% of maternal deaths in developed countries worldwide according to the World Health Organization, while accounting for 9.3% of maternal deaths in the United States
• Nearly all these deaths (97%) had at least some chance of preventability and more than half of them (52%) had a good-to-strong chance.
(Khan, Wojdyla et al. 2006, Creanga, Berg et al. 2015).
Mortality Rates Venous thromboembolism (VTE) is the most common cause of maternal mortality.
• VTE contributes to 14.9% of maternal deaths in developed countries. WHO analysis of causes of maternal death: a systematic review. Lancet 2006;367:1066-74.
• VTE related deaths in pregnancy was 31.1% based on UK Confidential Enquiries into Maternal Deaths in the United Kingdom.
BJOG : an international journal of obstetrics and gynaecology 2011;118 Suppl 1:1-203.
• CDC data: 9.3% of pregnancy related deaths from VTE Pregnancy-Related Mortality in the United States, 2006-2010.
Obstet Gynecol 2014;125:5-12.
Prevalence
Prevalence of venous thromboembolism and has increased due to increasing rates of obesity, advanced maternal age and major medical comorbidities complicating pregnancy.
Trends in venous thromboembolism among pregnancy-related hospitalizations, United States, 1994-2009.
American journal of obstetrics and gynecology 2013;209:433 e1-8.
Venous thromboembolism (VTE)
• Two potentially life threatening conditions:
(i) deep vein thrombosis (DVT)
(ii) pulmonary embolism (PE)
• Incidence is 2-4 in 1000 pregnancies
• DVT 80% and PE 20%
• 2/3 of DVT are antepartum
• Cesarean section increases the risk 3-5 fold than vaginal delivery
Thromboembolism (VTE) in pregnancy
• Pregnant women are at an increased risk for venous thromboembolic disease (VTE / DVT)
– 2-4 in 1000 pregnancies
– 2-4 fold increase compared to non-pregnant state
– Cesarean delivery > vaginal delivery
– 2/3 of DVT occur antepartum (equally distributed among all three trimesters)
– 43-60% of pulmonary embolism (PE) occur 4-6 weeks after delivery
– Risk per day of PE and DVT: highest following delivery than antepartum period.
• PE is the major non-obstetric cause of maternal mortality
– 2/100 000 pregnancies, 10-20% of VTEs are PEs.
90% of DVT during pregnancy occurs on the left side.
DVT in pregnancy can also occur in the pelvic veins –diagnostic challenge with routine testing.
Ovarian vein thrombosis 0.025%.
VTE in pregnancy
Pathogenesis of VTE
• Virchow’s triad
-hypercoagulability,
-stasis, and
-endothelial vascular damage
All 3 components are exacerbated by the physiologic and hormonal changes associated with pregnancy resulting in a greater than 5 fold increased risk of VTE during pregnancy (Bourjeily, Paidas et al. 2010).
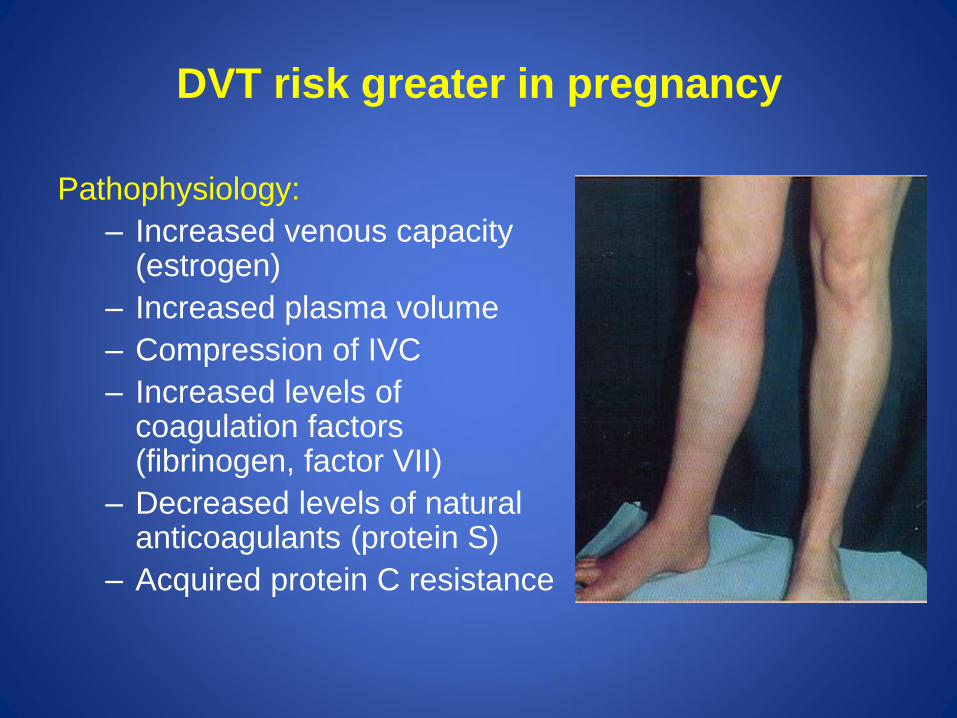
DVT risk greater in pregnancy
Pathophysiology:
– Increased venous capacity (estrogen)
– Increased plasma volume
– Compression of IVC
– Increased levels of coagulation factors (fibrinogen, factor VII)
– Decreased levels of natural anticoagulants (protein S)
– Acquired protein C resistance
CMQCC VTE Toolkit
The national VTE bundle is organized into 4 domains:
• readiness
• recognition and prevention
• response
• reporting/system learning
Each facility/unit will then be able to individualize the specific components of the CMQCC VTE toolkit to fit their particular culture and available resources.
The final toolkit is currently in process. Updates will be posted to the website when available.
Readiness
Every Unit
Use a standardized thromboembolism risk assessment tool for VTE during:
• Outpatient prenatal care
• Antepartum hospitalization
• Hospitalization after cesarean or vaginal deliveries
• Postpartum period (up to 6 weeks after delivery)
Council on Patient Safety in Women’s Health Care
ACOG
Recognition and prevention
Every Patient
• Apply standardized tool to all patients to assess VTE risk at time points designated under “Readiness”
• Apply standardized tool to identify appropriate patients for thromboprophylaxis
• Provide patient education
• Provide all healthcare providers education regarding risk assessment tools and recommended thromboprophylaxis
Council on Patient Safety in Women’s Health Care
ACOG
Response Every Unit
• Use standardized recommendations for mechanical thromboprophylaxis
• Use standardized recommendations for dosing of prophylactic and therapeutic pharmacologic anticoagulation.
• Use standardized recommendations for appropriate timing of pharmacologic prophylaxis with neuraxial anesthesia
Council on Patient Safety in Women’s Health Care
ACOG
Reporting/systems learning
• Every Unit
• Review all thromboembolism events for systems issues and compliance with protocols
• Monitor process metrics and outcomes in a standardized fashion
• Assess for complications of pharmacologic thromboprophylaxis
Council on Patient Safety in Women’s Health Care
ACOG
Risk factors for VTE
• Pregnancy itself is a risk factor
• Previous VTE in patient on hormonal contraception
• Previous VTE during pregnancy (risk is 12%)
• Rheumatic heart disease in patients with heart prosthesis
• Thrombophilias (congenital and acquired)
VTE risk assessment
• A standardized VTE risk assessment is recommended at the following times:
– During the first prenatal visit
– During any antepartum hospital admission including birth hospitalization
– During the immediate postpartum period (just after the birth)
– Upon discharge home after the birth
Independent risk factors of a higher
VTE risk in pregnancy • Bedrest and physical immobility
• Advanced maternal age (>35 yrs)
• Personal or family history of VTE
• Obesity; BMI > 30
• Multiparity; parity > 4
• Preeclampsia
• Hyperemesis gravidarum
• Shock and dehydration
• Infections
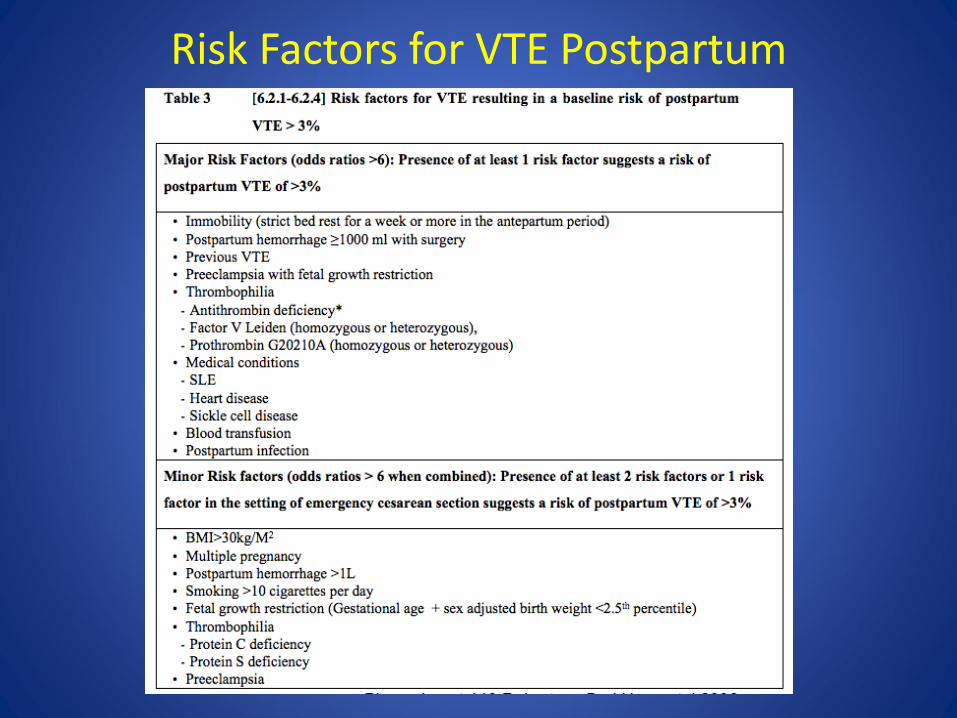
Risk Factors for VTE Postpartum
VTE Risk- CMQCC
• Low
• Medium
• High
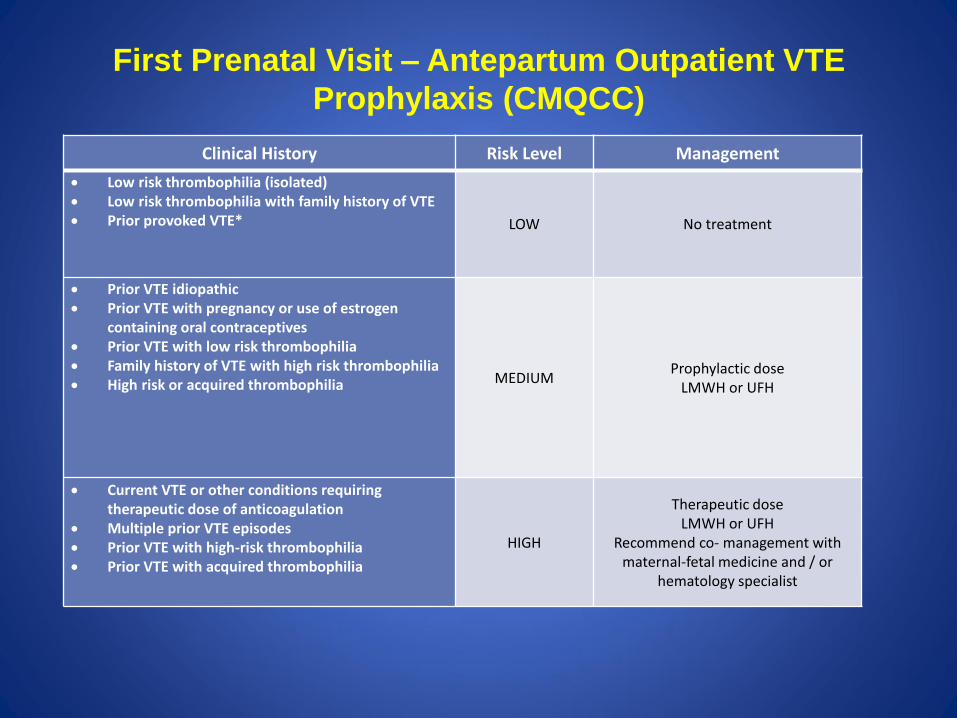
First Prenatal Visit – Antepartum Outpatient VTE
Prophylaxis (CMQCC)
Clinical History Risk Level Management
Low risk thrombophilia (isolated) Low risk thrombophilia with family history of VTE Prior provoked VTE* LOW No treatment
Prior VTE idiopathic Prior VTE with pregnancy or use of estrogen
containing oral contraceptives Prior VTE with low risk thrombophilia Family history of VTE with high risk thrombophilia High risk or acquired thrombophilia MEDIUM
Prophylactic dose LMWH or UFH
Current VTE or other conditions requiring therapeutic dose of anticoagulation
Multiple prior VTE episodes Prior VTE with high-risk thrombophilia Prior VTE with acquired thrombophilia
HIGH
Therapeutic dose LMWH or UFH
Recommend co- management with maternal-fetal medicine and / or
hematology specialist
First trimester risk factors Identification and Management
• Women admitted with hyperemesis should be considered
for thromboprophylaxis with LMWH and can discontinue thromboprophylaxis when the hyperemesis resolves.
• Women with ovarian hyperstimulation syndrome should be considered for thromboprophylaxis with LMWH in the first trimester.
• Women with an IVF pregnancy and three other risk factors should be considered for thromboprophylaxis with LMWH starting in the first trimester.
RCOG Green-top Guideline No. 37a, 2015
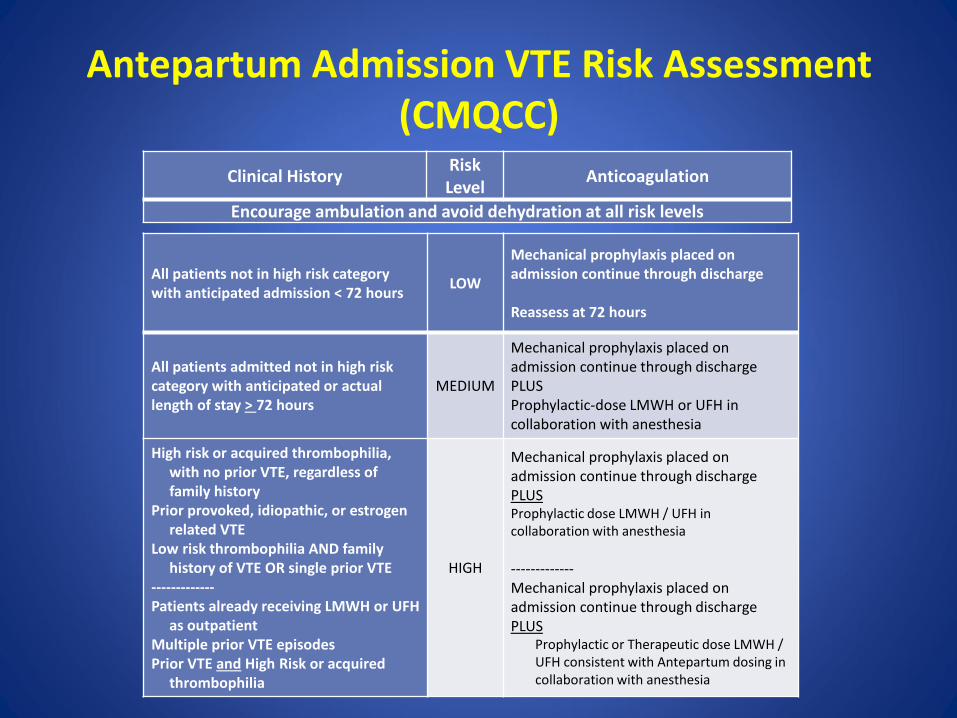
Antepartum Admission VTE Risk Assessment
(CMQCC) Clinical History
Risk Level
Anticoagulation
Encourage ambulation and avoid dehydration at all risk levels
All patients not in high risk category with anticipated admission < 72 hours
LOW
Mechanical prophylaxis placed on admission continue through discharge Reassess at 72 hours
All patients admitted not in high risk category with anticipated or actual length of stay > 72 hours
MEDIUM
Mechanical prophylaxis placed on admission continue through discharge PLUS Prophylactic-dose LMWH or UFH in collaboration with anesthesia
High risk or acquired thrombophilia, with no prior VTE, regardless of family history
Prior provoked, idiopathic, or estrogen related VTE
Low risk thrombophilia AND family history of VTE OR single prior VTE
------------- Patients already receiving LMWH or UFH
as outpatient Multiple prior VTE episodes Prior VTE and High Risk or acquired
thrombophilia
HIGH
Mechanical prophylaxis placed on admission continue through discharge PLUS Prophylactic dose LMWH / UFH in collaboration with anesthesia
------------- Mechanical prophylaxis placed on admission continue through discharge PLUS
Prophylactic or Therapeutic dose LMWH / UFH consistent with Antepartum dosing in collaboration with anesthesia
Diagnosis of VTE in pregnancy:
challenges
• Clinical diagnosis alone is unreliable.
• DVT and PE are less prevalent in symptomatic
pregnant patients compared to non-pregnant patients.
• Anticoagulant treatment though highly effective carries
significant risks.
• Untreated VTE: can be life-threatening, can result in
fatal and non fatal PE.
• Clinical suspicion of DVT or VTE: follow up with
accurate diagnose to rule in or rule out.
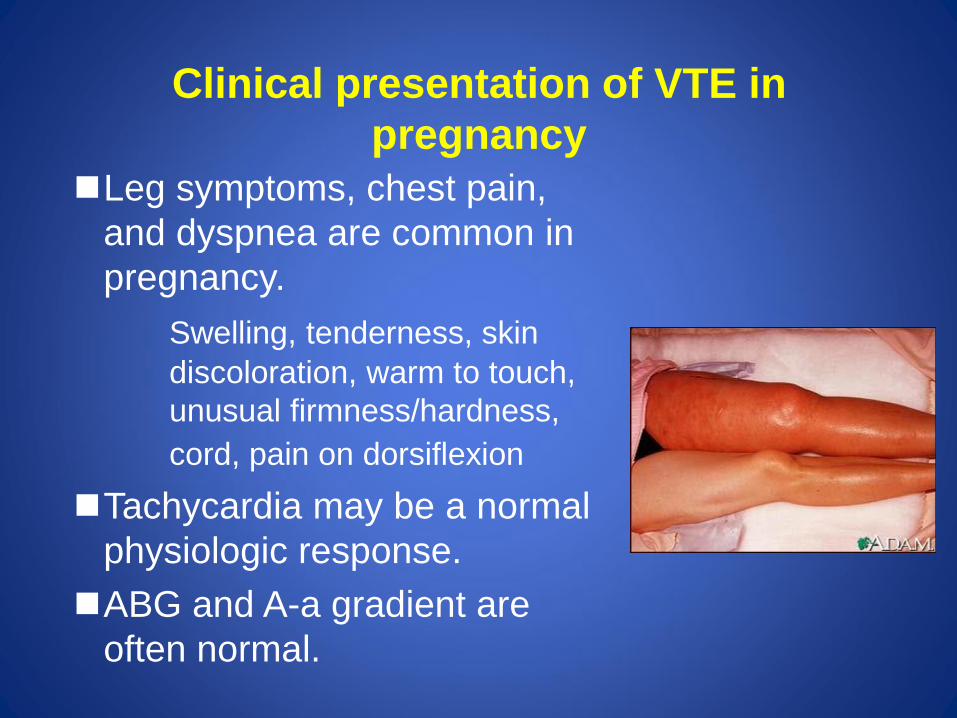
Clinical presentation of VTE in
pregnancy
Leg symptoms, chest pain,
and dyspnea are common in
pregnancy.
Swelling, tenderness, skin
discoloration, warm to touch,
unusual firmness/hardness,
cord, pain on dorsiflexion
Tachycardia may be a normal
physiologic response.
ABG and A-a gradient are
often normal.
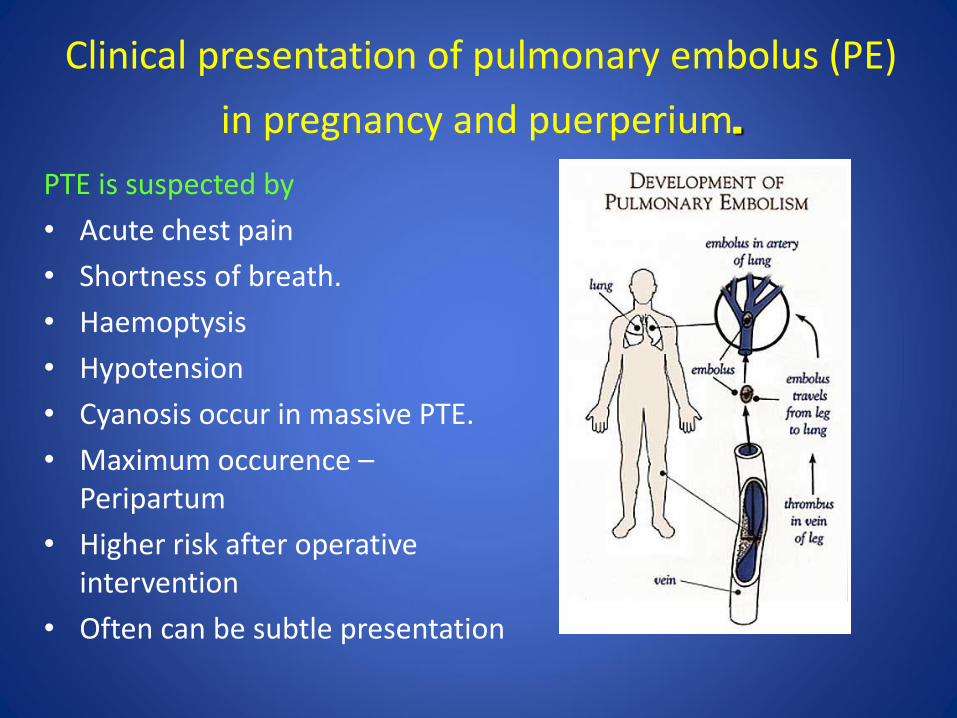
PTE is suspected by
• Acute chest pain
• Shortness of breath.
• Haemoptysis
• Hypotension
• Cyanosis occur in massive PTE.
• Maximum occurence – Peripartum
• Higher risk after operative intervention
• Often can be subtle presentation
Clinical presentation of pulmonary embolus (PE)
in pregnancy and puerperium.
Diagnosis of VTE in pregnancy:
challenges
• The common diagnostic tests: in adequately studied and
not appropriately validated in pregnant women.
• D-dimer assays and DVT/PE clinical prediction rules
have not been validated in the pregnant population.
• Concerns with radiation exposure to the fetus with
certain diagnostic testing.
Diagnosis of VTE in pregnancy:
challenges
• While it is important to avoid ionizing radiation
exposure whenever possible during pregnancy,
the risks of undiagnosed PE are much greater
than any theoretical risk to the fetus from use of
diagnostic testing with radiation exposure.
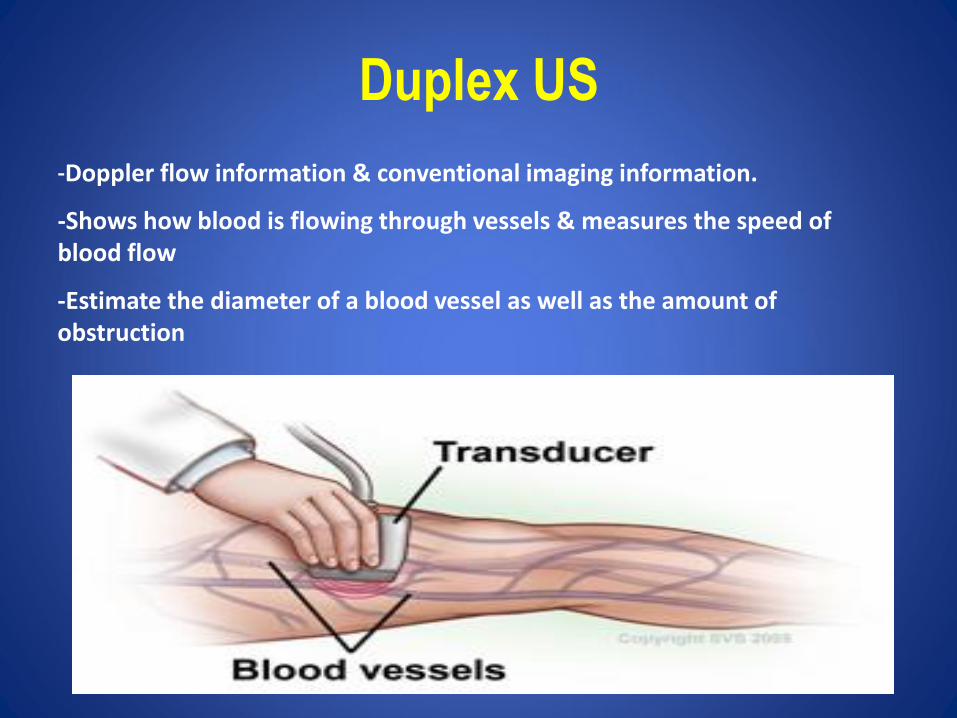
Duplex US
-Doppler flow information & conventional imaging information.
-Shows how blood is flowing through vessels & measures the speed of blood flow
-Estimate the diameter of a blood vessel as well as the amount of obstruction
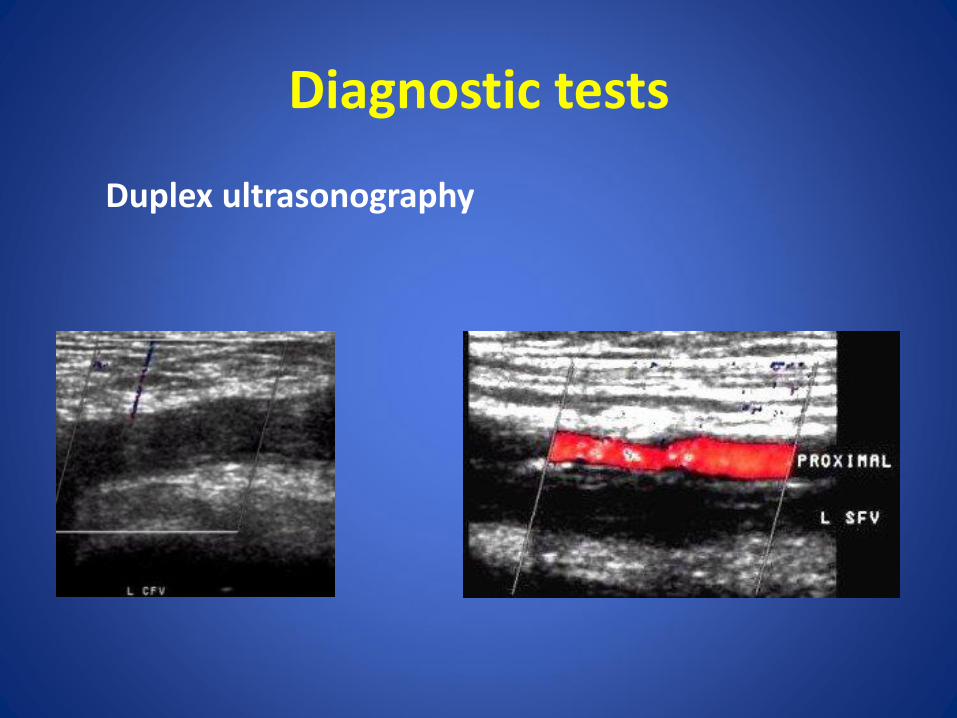
Diagnostic tests
Duplex ultrasonography
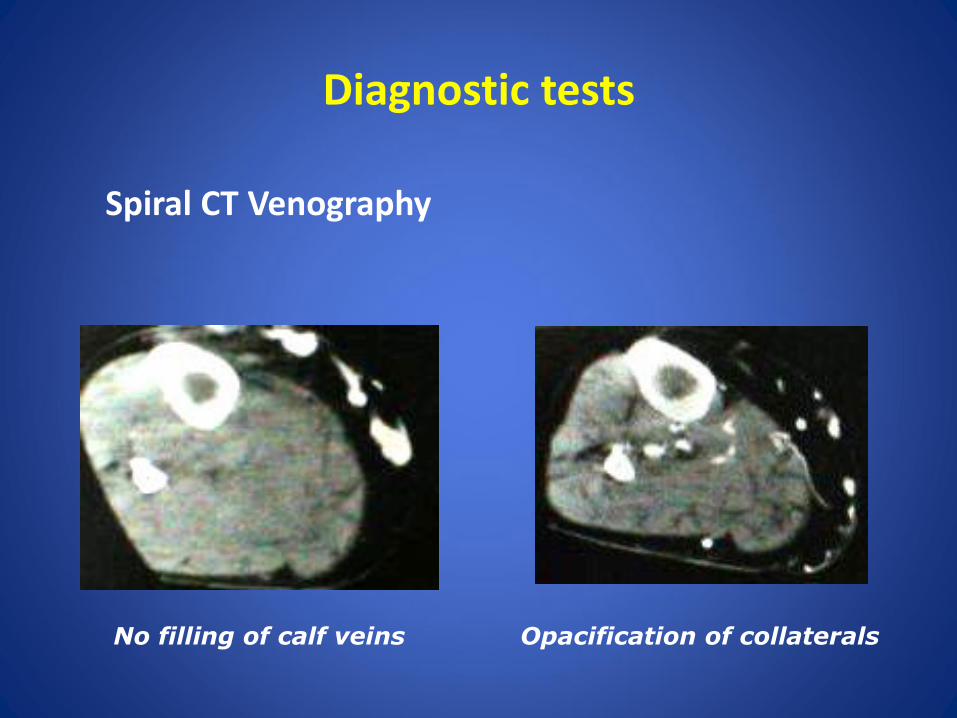
Diagnostic tests
Spiral CT Venography
No filling of calf veins Opacification of collaterals
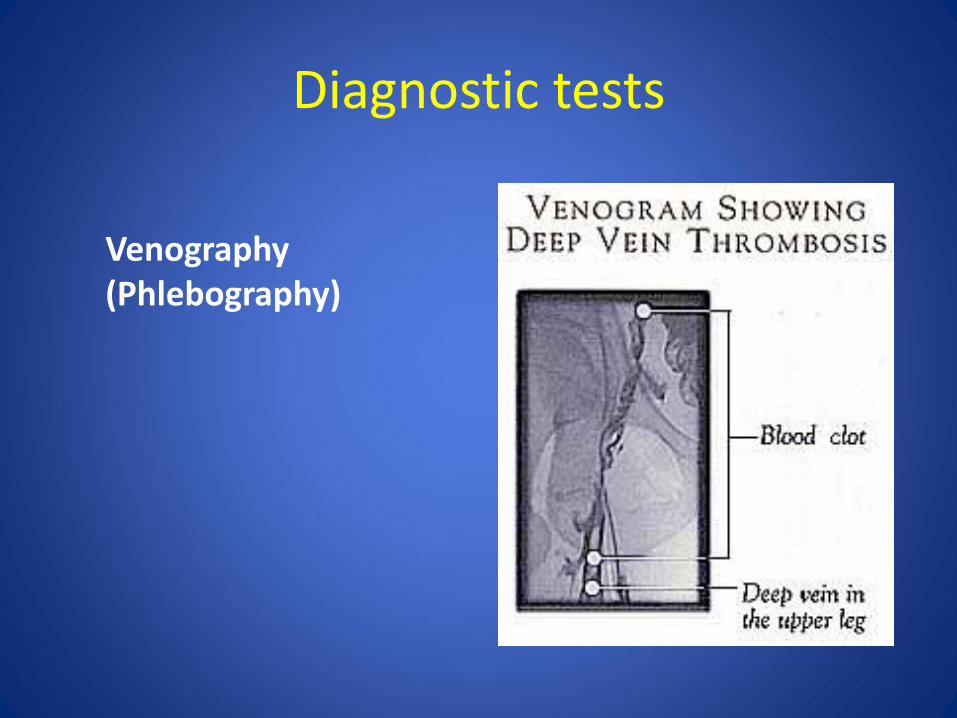
Diagnostic tests
Venography (Phlebography)
Consequences of VTE
• Complications of PE that are non-fatal include chronic thromboembolic pulmonary hypertension and/or cardiac compromise (Vazquez and Kahn 2010)
• DVT during pregnancy is usually proximal in location, i.e. popliteal, deep femoral or iliac that often manifests as a large thrombus. This is associated with an increased risk of late term sequelae such as chronic venous insufficiency and stasis ulcers, i.e. post thrombotic syndrome (Wik, Jacobsen et al. 2012, Skuterud Wik, Flem Jacobsen et al. 2015).
• VTE events require prolonged anticoagulation and are a major risk factor for future events.
VTE Prophylaxis
•Venous thromboembolism (VTE) is a leading cause of maternal mortality and severe morbidity
•Maternal death from VTE is amenable to prevention “single cause of death most amenable to reduction by systematic change in practice” Clark, SL. SeminPerinatol2012;36(1):42-7
•Protocols in the UK have led to significant reduction in maternal death from VTE
•Strategies for preventing VTE require minimal resources and are easily implementable
ANTICOAGULATION REGIMENS
• Anticoagulation during pregnancy is complex -Teratogenic risk to the fetus -Alteration of pharmacokinetics -Management at time of delivery -Neuraxial anesthesia • Heparins are preferred agents of choice: safe in pregnancy as
they donot cross the placenta, have no teratogenic and anticoagulation effects on the fetus.
• Warfarin and oral anticoagulants (Rivaroxaban, Apixaban,
Dabigatran) contraindicated due to limited or unfavorable data
VTE treatment • LMWH preferred based on better safety profile, reliable
pharmacokinetics, more practical, and as effective as UFH
– Largely based on studies in non-pregnant population
– Widespread use over the last 10-15 years in pregnant women have shown that LMWHs are as effective and safer than UFH (less HIT and less osteoporosis than UFH)
– Does not cross placenta!
VTE treatments: other options • UFH
– Initial IV UFH therapy followed by UFH bid sc dosing (adjusted weekly to achieve target PTT (60-80 sec) 6H after injection). Weekly surveillance
• VKA – Teratogenicity (coumarin embryonopathy: nasal hypoplasia and/or stippled
epiphyses); observed only duirng 6-12 weeks of gestation (Chan et al, studied 549 live births; VKA through out preg vs. UFH 6-12 weeks then VKA vs. UFH throughout pregnancy)
– CNS abnormalities during any trimester (corpus callosum agenesis; midline cerebellar atrophy); very rare and questionable association
– Fetal hemorrhagic complications especially at delivery due to prolonged anticoagulant effect of warfarin as a result of fetal liver being immature and hence fetal levels of vit K dependent coag factors are low.
– ?role in pregnant women with mechanical prosthetic valves at high risk for embolization (i.e. previous CVA)
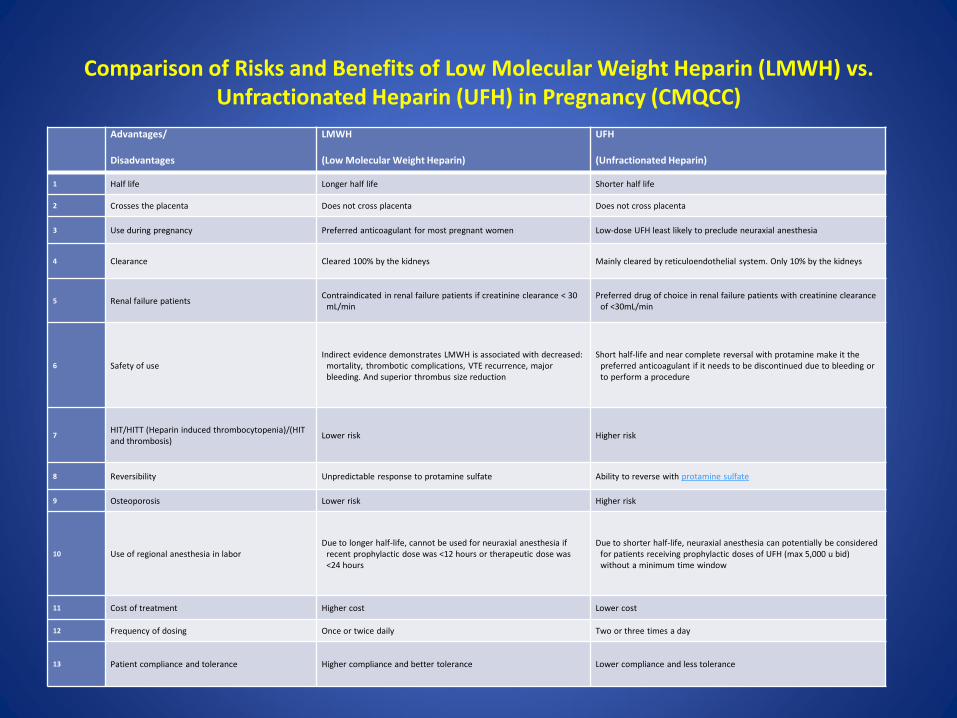
Comparison of Risks and Benefits of Low Molecular Weight Heparin (LMWH) vs.
Unfractionated Heparin (UFH) in Pregnancy (CMQCC) Advantages/
Disadvantages
LMWH
(Low Molecular Weight Heparin)
UFH
(Unfractionated Heparin)
1 Half life Longer half life Shorter half life
2 Crosses the placenta Does not cross placenta Does not cross placenta
3 Use during pregnancy Preferred anticoagulant for most pregnant women Low-dose UFH least likely to preclude neuraxial anesthesia
4 Clearance Cleared 100% by the kidneys Mainly cleared by reticuloendothelial system. Only 10% by the kidneys
5 Renal failure patients Contraindicated in renal failure patients if creatinine clearance < 30
mL/min Preferred drug of choice in renal failure patients with creatinine clearance
of <30mL/min
6 Safety of use Indirect evidence demonstrates LMWH is associated with decreased:
mortality, thrombotic complications, VTE recurrence, major bleeding. And superior thrombus size reduction
Short half-life and near complete reversal with protamine make it the preferred anticoagulant if it needs to be discontinued due to bleeding or to perform a procedure
7 HIT/HITT (Heparin induced thrombocytopenia)/(HIT and thrombosis)
Lower risk Higher risk
8 Reversibility Unpredictable response to protamine sulfate Ability to reverse with protamine sulfate
9 Osteoporosis Lower risk Higher risk
10 Use of regional anesthesia in labor Due to longer half-life, cannot be used for neuraxial anesthesia if
recent prophylactic dose was <12 hours or therapeutic dose was <24 hours
Due to shorter half-life, neuraxial anesthesia can potentially be considered for patients receiving prophylactic doses of UFH (max 5,000 u bid) without a minimum time window
11 Cost of treatment Higher cost Lower cost
12 Frequency of dosing Once or twice daily Two or three times a day
13 Patient compliance and tolerance Higher compliance and better tolerance Lower compliance and less tolerance
Clinical situations favoring UFH over LMWH
-LMWH is primarily cleared by renal excretion as opposed to UFH, and therefore is relatively contraindicated in patients with significant renal impairment (GFR < 30 ml/min).
-In renal failure, UFH is the preferred anticoagulant in pregnancy.
-Additional clinical situations in which UFH may be favored over LMWH may relate to the need for rapid reversal and/or regional anesthesia concerns.
Timing of initiation of thromboprophylaxis
When should thromboprophylaxis be started?
• Antenatal thromboprophylaxis for those with previous VTE should begin as early in pregnancy as practical.
• Women without previous VTE and without particular first trimester risk factors or admission to hospital, but with four other risk factors, should be considered for antenatal prophylaxis throughout pregnancy.
• Women without previous VTE and without particular first trimester risk factors or admission to hospital, but with three other risk factors, can start antenatal prophylaxis at 28 weeks of gestation.
RCOG Green-top Guideline No. 37a, 2015
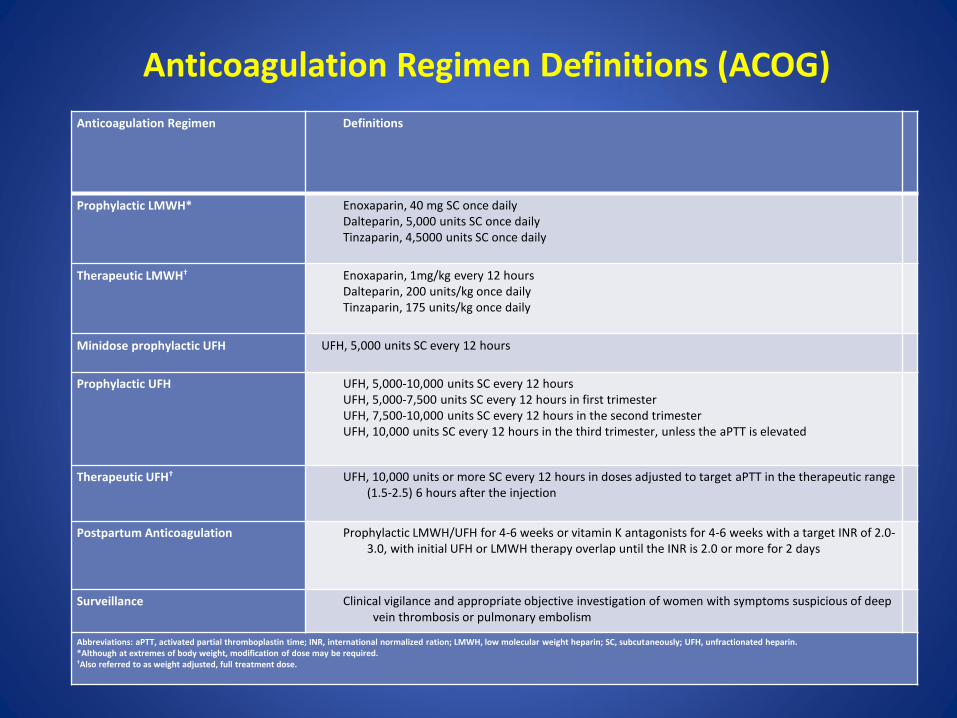
Anticoagulation Regimen Definitions (ACOG)
Anticoagulation Regimen Definitions
Prophylactic LMWH* Enoxaparin, 40 mg SC once daily Dalteparin, 5,000 units SC once daily Tinzaparin, 4,5000 units SC once daily
Therapeutic LMWH† Enoxaparin, 1mg/kg every 12 hours Dalteparin, 200 units/kg once daily Tinzaparin, 175 units/kg once daily
Minidose prophylactic UFH UFH, 5,000 units SC every 12 hours
Prophylactic UFH UFH, 5,000-10,000 units SC every 12 hours UFH, 5,000-7,500 units SC every 12 hours in first trimester UFH, 7,500-10,000 units SC every 12 hours in the second trimester UFH, 10,000 units SC every 12 hours in the third trimester, unless the aPTT is elevated
Therapeutic UFH† UFH, 10,000 units or more SC every 12 hours in doses adjusted to target aPTT in the therapeutic range (1.5-2.5) 6 hours after the injection
Postpartum Anticoagulation Prophylactic LMWH/UFH for 4-6 weeks or vitamin K antagonists for 4-6 weeks with a target INR of 2.0-3.0, with initial UFH or LMWH therapy overlap until the INR is 2.0 or more for 2 days
Surveillance Clinical vigilance and appropriate objective investigation of women with symptoms suspicious of deep vein thrombosis or pulmonary embolism
Abbreviations: aPTT, activated partial thromboplastin time; INR, international normalized ration; LMWH, low molecular weight heparin; SC, subcutaneously; UFH, unfractionated heparin. *Although at extremes of body weight, modification of dose may be required. †Also referred to as weight adjusted, full treatment dose.
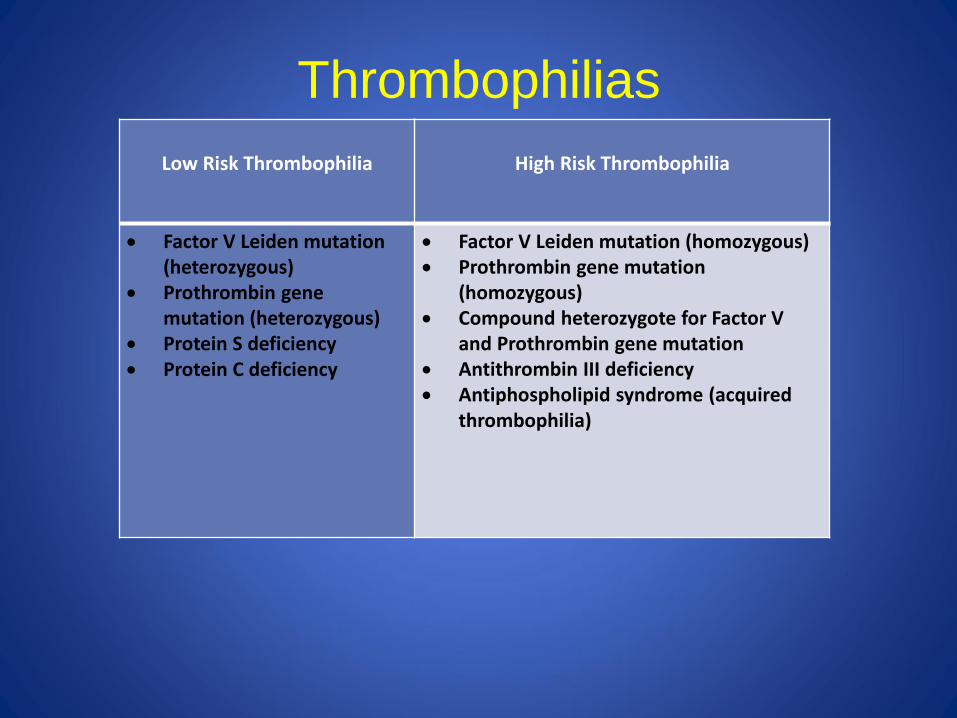
Thrombophilias
Low Risk Thrombophilia
High Risk Thrombophilia
Factor V Leiden mutation (heterozygous)
Prothrombin gene mutation (heterozygous)
Protein S deficiency Protein C deficiency
Factor V Leiden mutation (homozygous) Prothrombin gene mutation
(homozygous) Compound heterozygote for Factor V
and Prothrombin gene mutation Antithrombin III deficiency Antiphospholipid syndrome (acquired
thrombophilia)
Aspirin and concurrent antepartum heparin administration
For patients receiving antepartum pharmacologic VTE prophylaxis along with low dose aspirin for the prevention of preeclampsia, the small theoretical risks of aspirin use past 36 weeks in combination with heparin prophylaxis justify discontinuation of aspirin at that time given unclear benefits of continuing the medication (Ruff and Dougherty 1981, Horlocker 2011).
Warfarin use in pregnancy
Warfarin is primarily limited to select cases of mechanical heart valves only in consultation with cardiologist and maternal fetal medicine and in the postpartum period. Warfarin is considered compatible with breastfeeding and therefore is a valid option for anticoagulation in the postpartum period.
(Bates, Greer et al. 2012)
Newer Anticoagulants
• Oral direct thrombin inhibitors (Dabigatran), • Oral direct factor Xa inhibitors (Rivaroxaban, apixaban,
edoxaban) and Fondaparinux which is a heparinoid are NOT recommended for pregnant or breastfeeding mothers as they most likely cross placenta and their effects on human fetal development are unknown (Tang and Greer 2013).
• Patients should be advised to discontinue oral anticoagulants either prior to the anticipated pregnancy or at the time pregnancy is diagnosed.
• These should only be used in exceptional circumstances when no other anticoagulant option is available (Bates, Greer et al. 2012).
Preventive measure
• Thrombo-prophylaxis is the most readily available and implementable intervention that has shown to reduce maternal mortality from VTE
• The obstetric thromboembolism safety bundle evolved as a result of a national multidisciplinary work group addressing maternal safety
References
• American College of Obstetricians and Gynecologists (2012). "Practice Bulletin No. 132: Antiphospholipid syndrome." Obstet Gynecol 120(6): 1514-1521.
• American College of Obstetricians and Gynecologists (2013). "ACOG Practice Bulletin No. 138: Inherited thrombophilias in pregnancy." Obstet Gynecol 122(3): 706-717.
• American College of Obstetricians and Gynecologists and A. James (2011). "Practice bulletin no. 123: Thromboembolism in pregnancy." Obstet Gynecol 118(3): 718-729.
• American Society of Regional Anesthesia and Pain Medicine (2016). • American College of Chest Physicians Evidence-Based Clinical Practice Guidelines."
Chest 141(2 Suppl): e691S-736S. • Bates, S. M., I. A. Greer, I. Pabinger, S. Sofaer, J. Hirsh and P. American College of
Chest (2008). "Venous thromboembolism, thrombophilia, antithrombotic therapy, and pregnancy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition)." Chest 133(6 Suppl): 844S-886S.