the vibrios are found in marine and surface waters
TRANSCRIPT

The vibrios are found in marine and surface waters
Vibrio: family Vibrionaceae Aeromonas: family Aeromonadaceae Plesiomonas: family Enterobacteriaceae
gastroenteritis, wound infection, septicemia
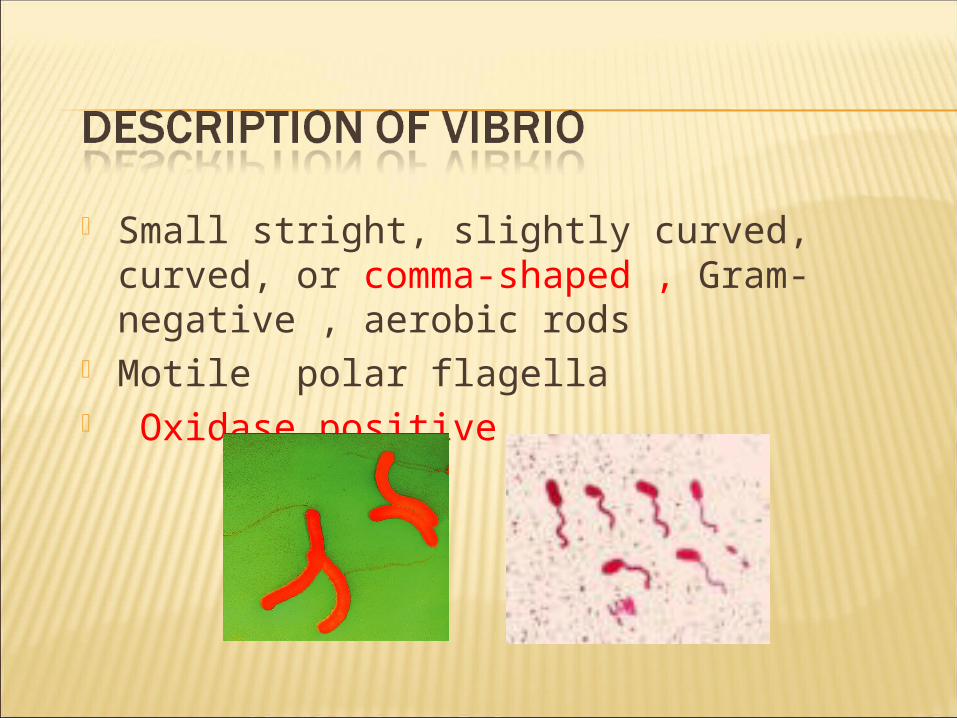
Small stright, slightly curved, curved, or comma-shaped , Gram-negative , aerobic rods
Motile polar flagella Oxidase positive

V.cholerae V.parahaemolyticus V.mimicus, V.vulnificus
Isolated from blood, wound, infected eyes and ears, and gallbladder

Taxonomy of Vibrio cholerae
>200 serogroups based on somatic O-antigen O1 and O139 serogroups are responsible for
classic epidemic cholera O1 serogroup subdivided into
Two biotypes: El Tor and classical (or cholerae)Three serotypes: ogawa, inaba, hikojima
3 major groups V.cholerae O1 V.cholerae non-O1 V.cholerae O139

2 biotypes Classical, El Tor,
3 subgroups or serotypes Ogawa : antigen A, B Inaba : antigen A, C Hikojima : antigen A, B, C

Pathogenesis of V.cholerae Incubation period: 1-4 days High infectious dose: >1010 CFU
102 -104 CFU with achlorhydria or hypochlorhydria
Vomiting and life-threatening watery diarrhea (20-30 liters/day), abdominal cramp
Rice-water stools Cholera toxin Dehydration , hypovolemic shock , Metabolic
acidosis, death Mortality rate reported 25-50% without treatment

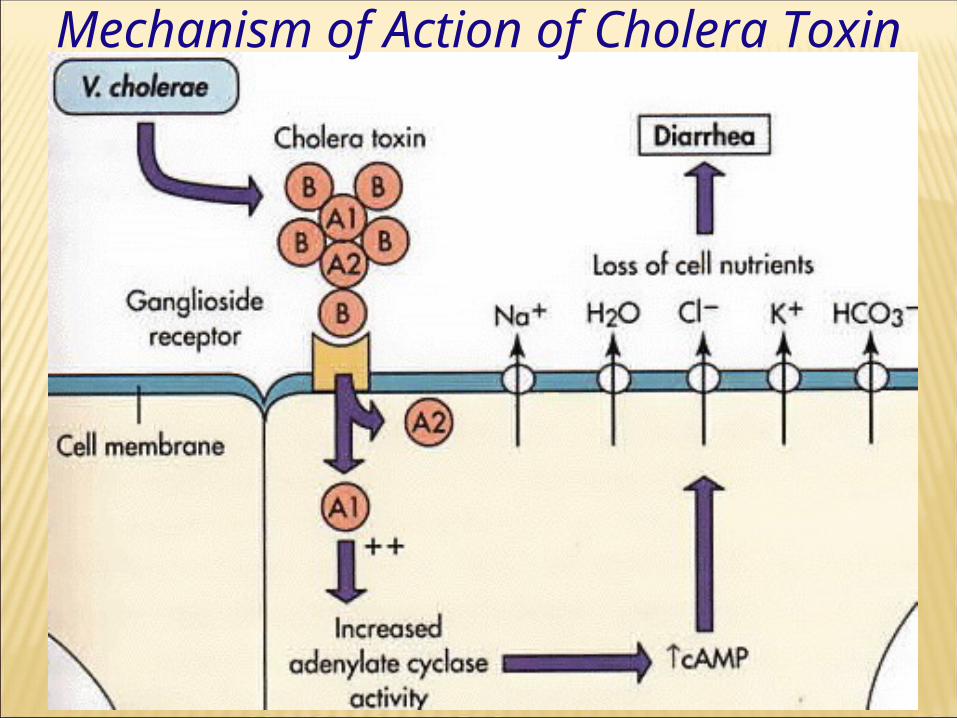
Cholera toxin, Choleragen Exotoxin, Enterotoxin
1 A subunit (peptide A1, peptide A2) 5 B subunits
Mechanism of Action of Cholera Toxin

Phenotypically similar to toxigenic V.cholerae O1
Lack of cholera toxin Cholera-like disease Extraintestinal infection
Ear infections, cellulitis and septicemia Contaminated raw-seafood
Specimen : stool or rectal swab Thiosulfate Citrate Bile-salt Sucrose
agar (TCBS) :selective medium Alkaline Peptone Water (pH 8.4-
8.6) :enrichment medium Biotyping , Biochemical tests Serotyping , Antiserum O1, O139

Epidemiology of Vibrio cholerae
Cholera recognized for more than two millennia with sporadic disease and epidemics
Endemic in regions of Southern and Southeastern Asia; origin of pandemic cholera outbreaks
Generally in communities with poor sanitation Eight pandemics since 1817 attributable to
increased world travel Cholera spread by contaminated water and food Human carriers and environmental reservoirs

First recognized in Japan Food-poisoning Halophilic bacteria (1-8% NaCl) Colony on TCBS is green
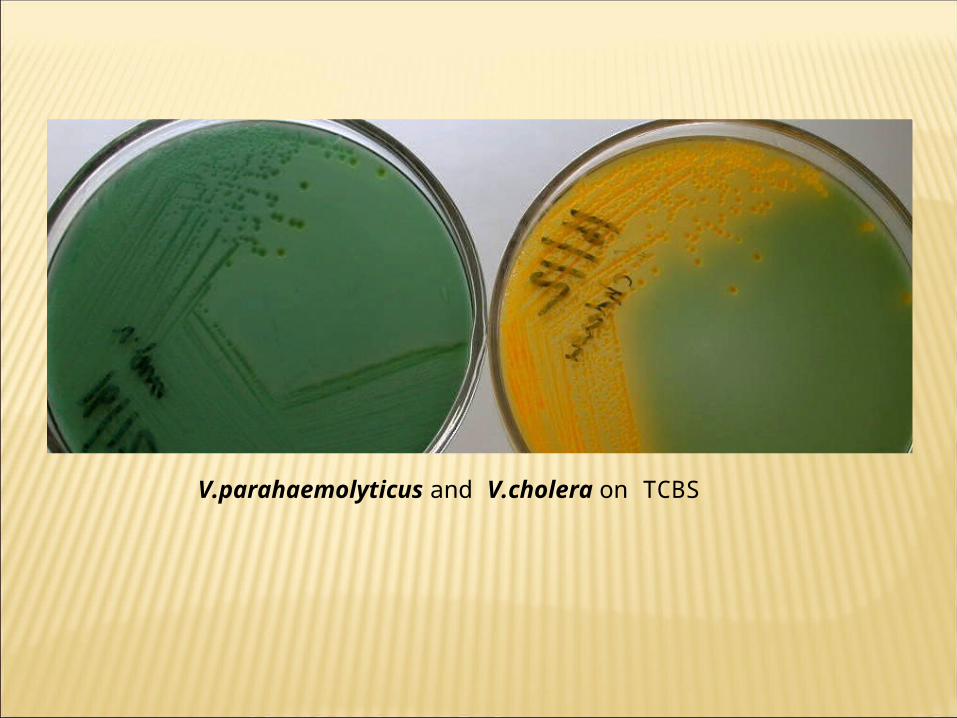
V.parahaemolyticus and V.cholera on TCBS

Diarrhea Consumption of
uncooked seafood Raw oysters
Clinical and epidemiologal are similar toV.cholerae non-O1
Wound infection- cellulitis, necrosis Trauma and exposure to marine
environment Bacterimia , Septicemia- fatality rate
50% Alcoholism , Preexisting liver disease
Gastroenteritis
All cases of diarrhea required measures for the prevention and treatment of dehydration and minerals
T reatment with antimicrobials: Tetracycline, chloramphenicol,
trimetroprim-sulfamethoxasole and norfloxacin
11 species isolated from clinical specimen
Gram-negative rod, motile (polar flagella) Facultative anaerobes , Oxidase, catalase
positive -hemolysis on BA Resistance to Vibriostatic compound
O/129

Gastroenteritis Acute diarrhea with vomiting or bloody stool Chronic persist more than 2 weeks A. hydrophila, A.veronii, A.caviae, and
A.trota Wound infection
Traumatic injury that occurs in contact water A.hydrophila, A.veronii biovar veronii and
A.schubertii

Plesiomonas shigelloides Gram-negative rod Lophotrichous flagella (2-5) Oxidase, catalase positive Growth in 0-5% NaCl, pH 4-9, 8-45 0C Susceptible to Vibriostatic compound
O/129 No hemolysis on BA
CLINICAL SIGNIFICANCECLINICAL SIGNIFICANCE Ingesting contaminated foods, raw fish, and
handling of infected cold-blooded animals Diarrheal disease Abdominal pain, watery and bloody diarrhea Extraintestinal infection
Septicemia, meningitis S : S : gentamicin, chloramphenicol,
cephalothin, trimetroprim-sulfamethoxasole, imipenam, quinolone
R : ampicillin, erythromycin, piperacillin

?

• convex, smooth, round colonies ,• 37 °C mineral salts and asparagine as sources
of carbon and nitrogen. thiosulfate-citrate-bile-sucrose (TCBS) agar, yellow colonies
• oxidase-positive, which differentiates them from enteric gram-negative bacteria.
• high pH (8.5–9.5) and are rapidly killed by acid.
• In areas where cholera is endemic, direct cultures of stool on selective media such as TCBS, and enrichment cultures in alkaline peptone water are appropriate.
• single heat-labile flagellar H antigen• O lipopolysaccharides that confer
serologic specificity. There are at least 139 O antigen groups.
• O group 1 and O group 139 cause classic cholera;
• non-O1/non-O139 V cholerae causes cholera-like disease.
• Antibodies to the O antigens tend to protect laboratory animals against infections with V cholerae.

• O1 antigen has determinants that make possible further typing; the serotypes are Ogawa, Inaba, and Hikojima
• Two biotypes of epidemic V cholerae have been defined, classic and El Tor.
• The El Tor biotype produces a hemolysin, gives positive results on the Voges-Proskauer test, and is resistant to polymyxin B. Typing is used for epidemiologic studies, and tests generally are done only in reference laboratories.
• V cholerae O139 is very similar to V cholerae O1 El Tor biotype. V cholerae O139 does not produce the O1 lipopolysaccharide and does not have all the genes necessary to make this antigen. V cholerae O139 makes a polysaccharide capsule like other non-O1 V cholerae strains, while V cholerae O1 does not make a capsule.

• heat-labile enterotoxin with a molecular weight of about 84,000, consisting of subunits A (MW 28,000) and B . Genes on the bacterial chromosome
• Ganglioside GM1 serves as the mucosal receptor for subunit B, which promotes entry of subunit A into the cell. Activation of subunit A1 yields increased levels of intracellular cAMP and results in prolonged hypersecretion of water and electrolytes
• Diarrhea occurs—as much as 20–30 L/d—with resulting dehydration, shock, acidosis, and death.
• V cholerae is pathogenic only for humans• normal gastric acidity may ingest as many as
1010 V cholerae to become infected when the vehicle is water, because the organisms are susceptible to acid. When the vehicle is food, as few as 102–104 organisms are necessary because of the buffering capacity of food.
• Any medication or condition that decreases stomach acidity makes a person more susceptible to infection with V cholerae.
Cholera is not an invasive infection. The organisms do not reach the bloodstream but remain within the intestinal tract. Virulent V cholerae organisms attach to the microvilli of the brush border of epithelial cells. There they multiply and liberate cholera toxin and perhaps mucinases and endotoxin.
• About 60% of infections with classic V cholerae are asymptomatic• about 75% of infections with the El Tor biotype• incubation period is 1–4 days for persons • symptoms, depending largely upon the size of the inoculum ingested. • sudden onset of nausea and vomiting and profuse diarrhea with
abdominal cramps. • Stools, "rice water," contain mucus, epithelial cells, and large
numbers of vibrios. • There is rapid loss of fluid and electrolytes, dehydration, circulatory
collapse, and anuria. • The mortality rate without treatment is between 25% and 50%. • The diagnosis of a full-blown case of cholera presents no problem in
the presence of an epidemic. • However, sporadic or mild cases are not readily differentiated from
other diarrheal diseases. • The El Tor biotype tends to cause milder disease than the classic
biotype.

• Specimens : Specimens for culture consist of mucus flecks from stools.
• Smears : The microscopic appearance of smears made from stool samples is not distinctive. Dark-field or phase contrast microscopy may show the rapidly motile vibrios.
• Culture• Growth is rapid in peptone agar, on blood agar with a pH
near 9.0, or on TCBS agar, and typical colonies can be picked in 18 hours. For enrichment, a few drops of stool can be incubated for 6–8 hours in taurocholate-peptone broth (pH 8.0–9.0); organisms from this culture can be stained or subcultured.
• Specific Tests• V cholerae organisms are further identified by slide
agglutination tests using anti-O group 1 or group 139 antisera and by biochemical reaction patterns.
• water and electrolyte replacement to correct the severe dehydration and salt depletion.
• Many antimicrobial agents are effective against V cholerae.
• Oral tetracycline tends to reduce stool output in cholera and shortens the period of excretion of vibrios.
• In some endemic areas, tetracycline resistance of V cholerae has emerged; the genes are carried by transmissible plasmids.

• Six pandemics (worldwide epidemics) of cholera occurred between 1817 and 1923, caused most likely by V cholerae O1 of the classic biotype and largely originating in Asia, usually the Indian subcontinent.
• The seventh pandemic began in 1961 in the Celebes Islands, Indonesia, with spread to Asia, the Middle East, and Africa. This pandemic has been caused by V cholerae biotype El Tor. Starting in 1991, the seventh pandemic spread to Peru and then to other countries of South America and Central America. Cases also occurred in Africa. Millions of people have had cholera in this pandemic. Some consider the cholera caused by the serotype O139 strain to be the eighth pandemic that began in the Indian subcontinent in 1992–1993, with spread to Asia. The disease has been rare in North America since the mid 1800s, but an endemic focus exists on the Gulf Coast of Louisiana and Texas.

The disease is spread by contact involving individuals with mild or early illness and by water, food, and flies. In many instances, only 1–5% of exposed susceptible persons develop disease. The carrier state seldom exceeds 3–4 weeks, and the importance of carriers in transmission is unclear. Vibrios survive in water for up to 3 weeks.

• Control rests on education• and on improvement of sanitation, particularly
of food and water. • Patients should be isolated, their excreta
disinfected, and contacts followed up. • Chemoprophylaxis with antimicrobial drugs may
have a place. • Repeated injection of a vaccine containing
either lipopolysaccharides extracted from vibrios or dense vibrio suspensions can confer limited protection to heavily exposed persons (eg, family contacts) but is not effective as an epidemic control measure.
• halophilic bacterium • acute gastroenteritis , seafood such as raw fish or
shellfish. • incubation period of 12–24 hours, nausea and vomiting,
abdominal cramps, fever, and watery to bloody diarrhea occur.
• spontaneously in 1–4 days with no treatment other than restoration of water and electrolyte balance.
• No enterotoxin worldwide, with highest incidence in areas where
people eat raw seafood. grow well on blood agar. It also grows well on TCBS, where
it yields green colonies. V parahaemolyticus is usually identified by its oxidase-positive growth on blood agar.

• the new family Aeromonadaceae ; Based on DNA hybridization
• three groups are of primary clinical importance
• Aeromonas hydrophila complex, • Aeromonas caviae complex, • Aeromonas veronii biovarsobria• Aeromonas species are differentiated from
vibrios by showing resistance to compound O/129 (see above) and lack of growth on media containing 6% NaCl.

• Plesiomonas shigelloides is a gram-negative rod with polar flagella.
• Plesiomonas is most common in tropical and subtropical areas.
• It is a water and soil organism and has been isolated from freshwater fish and many animals.
• stool cultures of patients with diarrhea. • Some plesiomonas strains share antigens with Shigella
sonnei, and cross-reactions with shigella antisera occur. • Plesiomonas can be distinguished from shigellae in
diarrheal stools by the oxidase test: Plesiomonas is oxidase-positive and shigellae are not.
• Plesiomonas is positive for DNase; this and other biochemical tests distinguish it from aeromonas