the surfactant positive airway pressure and pulse oximetry randomized controlled trial ... round...
TRANSCRIPT

The Surfactant Positive Airway Pressure and Pulse Oximetry Randomized Controlled Trial
(SUPPORT) in Extremely Preterm Infants
Wally Carlo, MD University of Alabama at Birmingham
for the SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network


Stevie Wonder
Famous former preemie; blind from retinopathy

History of Supplemental Oxygen in Preterm Babies
● 1940s - Excessive O2 use in preemies; retinopathy in premature infants was first observed
● 1950s - Uncontrolled restriction O2 (<50% FiO2, severe hypoxia allowed) trials led to reduced retinopathy (not blindness) but trends for increased mortality (4% increase)
● 1960s - Uncontrolled O2 restriction practice was estimated to result in 16 deaths per case of blindness prevented
● 2010 - SUPPORT trial: O2 titration to keep saturations 85-89% in preemies resulted in decreased retinopathy (not blindness) but increased death (3.7%)
● 2013 - BOOST II trials confirm SUPPORT trial results

Objectives
1. Know the background and results of the SUPPORT RCT arm of lower versus high oxygen saturation targeting
2. Post SUPPORT, are there new data that support or refute the findings?
3. Did SUPPORT result in changes in practice recommendations?

Outline
1. Background 2. The SUPPORT Trial 3. Post SUPPORT
Background
• No consensus on oxygen saturation targets • Published “acceptable” levels in neonates
were initially 88-98% and more recently 85-95%
• No standards for assessing “need” for oxygen supplementation in infants

Does oxygen saturation targeting matter?
Previous Trials of Oxygenation Targets
STOP-ROP Trial BOOST I Trial

SaO2 Targets: STOP-ROP Trial
STOP-ROP Multicenter Study Group. Pediatrics 105:295, 2000
Sats 96 to 99%
Sats 89 to 94%
p value
Threshold ROP 41% 48% <0.05 Pneumonia/BPD exacerbations 13% 8% = 0.07 Prolonged hospitalization* 13% 7% <0.05 Prolonged oxygen* 47% 37% <0.05
Prolonged diuretics* 36% 24% <0.05 Death 3% 2% NS
* At 3 months corrected age

SaO2 Targets: BOOST Trial Sats
95-98% Sats
91-94% p value
Dev abnormality 23% 24% NS
Weight < 10% tile 33% 37% NS
Death 5% 3% NS
O2 at 36 w 64% 46% <0.001
Home O2 30% 17% <0.001
Askie et al. NEJM 349:959, 2003
Previous Trials of Oxygen Saturation Targets
1. Both targeted oxygen saturation at upper limits of practice (high 90s)
2. Both were post-neonatal interventions 3. Both reported pulmonary harms of targets
above 95%
STOP-ROP Trial BOOST I Trial

How about studies of oxygen saturation targets below 90%?
Before SUPPORT, there had not been randomized controlled
trials of oxygen saturation targets below 90%

Mortality in Liberal Versus Restricted Oxygen Saturation RCT
500-1250 gm >1250 gm
Liberal (PaO2 < 80 mmHg) 69% 9%
Restricted (PaO2 < 40 mmHg) 68% 2%
Usher R and Avery ME. Pediatric Research 4:469, 1970

How about observational studies of oxygen saturation targeting?

SaO2 Targets: Retrospective Study
Methods • Retrospective review • Population study - All babies < 28 weeks in
several referral units • Data analyzed by SaO2 targets
Tin et al. Arch Dis Child. 84:F106, 2001

SaO2 Targets: Retrospective Study
0
20
40
60
70-90% 84-94% 85-95% 88-98%
SurvivorsCerebral palsyThreshold ROP
Oxygen Saturation
Perc
ent (
%)
Tin et al. Arch Dis Child. 84:F106, 2001

Incidence of ROP Stages 3 to 4 for Infants with Birth Weight of 500-1500 g
Chow LC et al. Pediatrics 111:339, 2003
Hospital VON
(targets 85-93%)
�Survival rates showed a trend toward improvement� with lower oxygen saturation targets

Outline
1. Background 2. The SUPPORT Trial 3. Post SUPPORT

Background - SUPPORT Oxygen Saturation Trial
• Retinopathy of prematurity (ROP) continues to be an important cause of blindness in preterm infants
• Recent observational data suggest that oxygen saturations in the lower limits of common clinical practice (83 or 85%) may reduce ROP but this has not been tested in RCTs
• While RCTs of oxygen restriction of oxygen supplementation without oxygenation measurements in the 1950s resulted in an increased mortality in infants in the lower oxygen group, a RCT in 1970 reported lower mortality with lower oxygenation targeting

SUPPORT Hypothesis
P Among infants of 24 0/7 to 27 6/7 weeks gestational age
I a lower O2 saturation target range (85 to 89%)
compared to
C a higher O2 saturation target range (91 to 95%) reduces
O the incidence of the composite outcome of severe
ROP or death

Methods – Intervention • Infants were randomized to:
– lower saturation targeting (85 to 89%) or; – higher saturation targeting (91 to 95%)
• Oxygen saturations were monitored with electronically-altered Masimo Radical Pulse Oximeters
SpO2 Group Displayed Actual Target Alarm Values Low SpO2 88-92% 85-89% <85 and >95% High SpO2 88-92% 91-95% <85 and >95%

Recent Trials of Oxygenation Targets
Experimental
Control
SUPPORT, BOOST II, COT 85-89% 91-95%
STOP-ROP 96-99% 89-94%
BOOST I 95-98% 91-94%
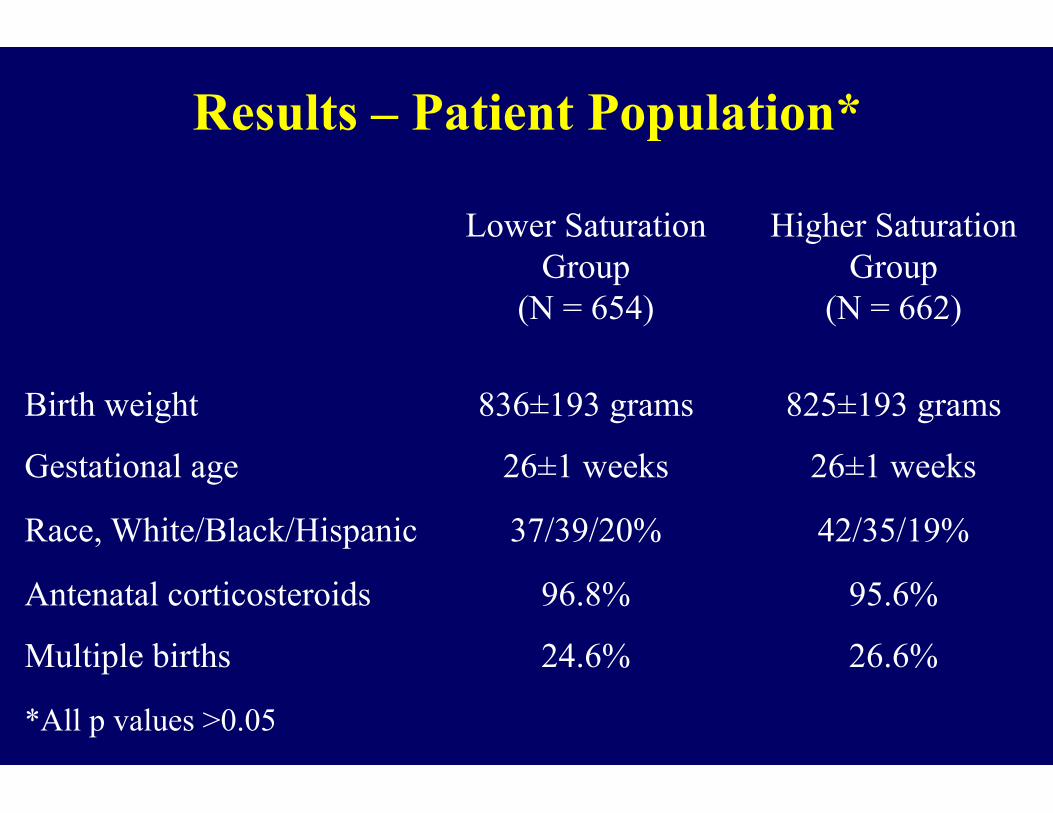
Results – Patient Population*
Lower Saturation Group
(N = 654)
Higher Saturation Group
(N = 662)
Birth weight 836±193 grams 825±193 grams
Gestational age 26±1 weeks 26±1 weeks
Race, White/Black/Hispanic 37/39/20% 42/35/19%
Antenatal corticosteroids 96.8% 95.6%
Multiple births 24.6% 26.6%
*All p values >0.05

Actual Median Oxygen Saturation (%)
80 85 90 95 100
Perc
ent o
f Inf
ants
(%)
16
12
4
0
8
91 - 95% oxygen saturation target 85 - 89% oxygen saturation target
Percent of O2 saturation (%)

Results – Primary Outcome
Lower Saturation
Group N=654
Higher Saturation
Group N=662
Adjusted Relative Risk
(95% CI)
Severe ROP/death 28.3% 32.1% 0.90 (0.76, 1.06)
Severe ROP 8.6% 17.9% 0.52 (0.37, 0.73) NNT=11
Death 19.9% 16.2% 1.27 (1.01, 1.60) NNH=27

100
Perc
ent o
f Inf
ants
Sur
vivi
ng
80
0 100 200 300 400
High SpO2 Group
Low SpO2 Group
70
90
Day of Life
Survival Curve

Results – BPD and Other Pulmonary Outcomes
Lower Saturation
Group N=654
Higher Saturation
Group N=662
Adjusted Relative Risk
(95% CI)
BPD (O2 use at 36 w) 37.6% 46.7% 0.82 (0.72, 0.93) BPD (O2 use) or death, 36 w 48.5% 54.2% 0.91 (0.83, 1.01) BPD (phys), 36 w 38.0% 41.7% 0.92 (0.81, 1.05) BPD (phys) or death, 36 w 48.8% 50.0% 0.99 (0.90, 1.10) Pneumothorax 7.2% 6.5% 1.12 (0.74, 1.68) Any air leaks (14 days) 7.8% 6.3% 1.23 (0.83, 1.83) Postnatal steroids for BPD 9.6% 10.7% 0.91 (0.67, 1.24)

Results – Other Major Outcomes
Lower Saturation
Group N=654
Higher Saturation
Group N=662
Adjusted Relative Risk
(95% CI)
IVH, grade 3 or 4 13.2% 12.7% 1.06 (0.80, 1.40)
PVL 3.8% 4.7% 0.83 (0.49, 1.42)
NEC, stage ≥ 2 11.9% 10.8% 1.11 (0.82, 1.51)
Late onset sepsis 36.5% 35.6% 1.03 (0.89, 1.18)

Neurodevelopmental Impairment at 18 to 22 Months
Viable
Lower Oxygen
Saturation
Higher Oxygen
Saturation
Adjusted Relative Risk
(95% CI)
P Value
Primary outcome determined 94% 94% 1.00 (0.97-1.03) 0.79
Death or NDI 30% 28% 1.12 (0.94-1.32) 0.21
Death 22% 18% 1.25 (1.00-1.55) 0.046
NDI 10% 11% 0.87 (0.60-1.28) 0.49
Bilateral blindness 1% 1% 0.90 (0.28-2.90) 0.86
Vaucher et al. N Engl J Med, 2013
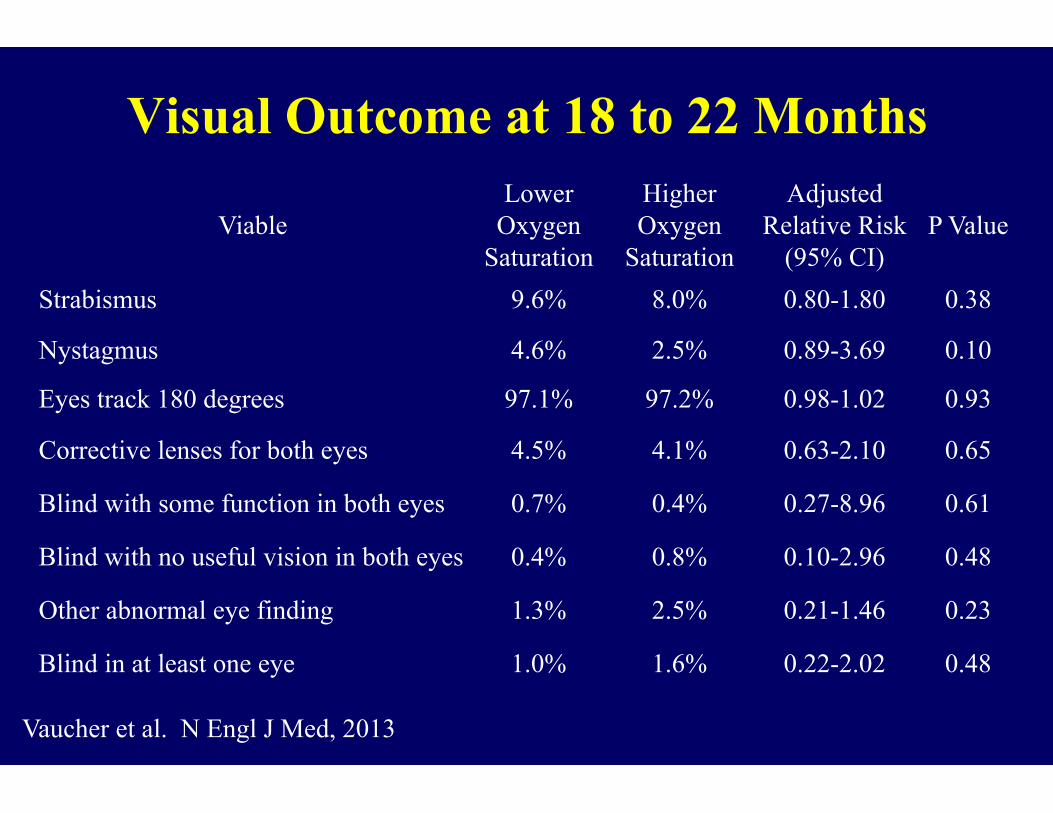
Visual Outcome at 18 to 22 Months
Viable Lower
Oxygen Saturation
Higher Oxygen
Saturation
Adjusted Relative Risk
(95% CI)
P Value
Strabismus 9.6% 8.0% 0.80-1.80 0.38
Nystagmus 4.6% 2.5% 0.89-3.69 0.10
Eyes track 180 degrees 97.1% 97.2% 0.98-1.02 0.93
Corrective lenses for both eyes 4.5% 4.1% 0.63-2.10 0.65
Blind with some function in both eyes 0.7% 0.4% 0.27-8.96 0.61
Blind with no useful vision in both eyes 0.4% 0.8% 0.10-2.96 0.48
Other abnormal eye finding 1.3% 2.5% 0.21-1.46 0.23
Blind in at least one eye 1.0% 1.6% 0.22-2.02 0.48
Vaucher et al. N Engl J Med, 2013

Summary • O2 saturation targeting in the range of 85-89%
did not affect severe ROP/death • O2 saturation targeting in the range of 85-89%
resulted in a significant reduction in severe ROP (17.9 to 8.6%, NNT = 11)
• However, mortality was significantly increased in the 85-89% target group (19.9 versus 16.2%, NNH = 27)
• The mortality effect persisted to 18-22 months corrected age
Outline
1. Background 2. The SUPPORT Trial 3. Post SUPPORT

BOOST ll UK and Aus/NZ Trials Enrollment Stopped
�Preterm babies who were having their oxygen targeted to keep them in the range 91-95% were surviving more often than preterm babies who were having their oxygen targeted to keep them in the range 85-89%.�
https://www.npeu.ox.ac.uk/boost

BOOST ll UK and Aus/NZ Trials Enrollment Stopped
“The difference was so clear that it was extremely unlikely to change if the trial continued to the end.”
“Because of this it was decided that no further babies should be entered into the trial and that babies currently in the trial should not continue in their allocated groups.”
https://www.npeu.ox.ac.uk/boost

Meta-analysis of SaO2 Targets Trials Death (latest age)
Lower SaO2 Higher SaO2 SUPPORT 140/663 111/648 BOOST II 235/1221 202/1220 COT 97/584 88/577
472/2439 409/2445 Risk increase 2.6% 19.3% 16.7%
RR 1.16 (1.03, 130) , p=0.018 NNH 38

Recommendations: Expert Opinion Given the increase in mortality at lower oxygen saturation targets in BOOST II and similar trials, it now appears prudent to aim to maintain an oxygen saturation level in the 90-95% range. “Until the remaining questions raised by these studies are answered by the combined meta-analysis or new evidence becomes available, minimizing extreme oxygenation levels by targeting saturations between 90-95% appear to be a reasonable approach.” Bancalari E and Claure N. JAMA 309:2161, 2013
Polin RA and Bateman D. NEJM 368:2141, 2013

European Association of Perinatal Medicine Consensus Guidelines on RDS - 2013
“In preterm infants receiving oxygen, the saturation target should be between 90 and 95%”.
Sweet DG, et al. Neonatology 103:353-68, 2013

NeOPRoM
International collaboration on a prospective meta-analysis

Thanks to the many infants, parents, and NICU staff
Thanks to the members of the Neonatal Research Network