the scientific basis for and efficacy of optometric vision ... highlight o ptometric vision therapy...
TRANSCRIPT

ISSUE HIGHLIGHT
Optometric vision therapy for nonstrabismic accom-modative and vergence disorders involves highly spe-cific, sequential, sensory-motor-perceptual stimulation
paradigms and regimens. It incorporates purposeful, con-trolled, and scientifically based manipulations of target blur,disparity, and proximity, with the aim of normalizing theaccommodative system, the vergence system, and theirmutual interactions.1-3 In addition, other sources of sensoryinformation, such as kinesthesia4 (e.g., touching the near testobject) and audition5,6 (e.g., oculomotor auditory biofeedback)correlated to the accommodative and vergence states (e.g.,position, innervation, effort, etc.) can provide cue rein-forcement. Inclusion of related behavioral modification par-adigms,7-9 such as general relaxation,5 visual imagery,10,11
(e.g., “think far or near”), and attentional shaping12 may helpone learn to initiate (i.e., provide a “trigger” mechanism)and/or enhance the appropriate motor responses. However,the ultimate goal of optometric vision therapy is not simplyto impact positively on various aspects of the oculomotor sys-tem per se, in isolation, but to attain clear and comfortablebinocular vision at all times. It involves oculomotor inte-gration with the head (i.e., eye-head coordination),13 neck(i.e., proprioceptive information),14 limbs,15 and overallbody,16,17 with information from the other sensory modal-ities, producing temporally efficient, coordinated behavior18,19
within a context of harmonious spatial sense16,17,20 under avariety of external and internal conditions and states.
Prevalence of nonstrabismic accommodative and vergence disordersNonstrabismic accommodative and vergence disorders ofa non-organic, nonpathological nature (i.e., “functional” inorigin) are the most-common ophthalmic vision conditions(other than refractive error) that present in the general opto-
The scientific basis for and efficacy of optometric vision therapy in nonstrabismicaccommodative and vergence disorders
Kenneth J. Ciuffreda, O.D., Ph.D.
State University of New York, State College of Optometry, Department of Vision Sciences, New York, New York
Ciuffreda KJ. The scientific basis for and efficacy of optomet-ric vision therapy in nonstrabismic accommodative and ver-gence disorders. Optometry 2002;73:735-62.
735
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
Background: For nearly 75 years, optometric vision therapy hasbeen an important mode of therapy for both children andadults who manifested a range of nonstrabismic accom-modative and vergence disorders.
Methods: In this article, the scientific basis for, and efficacy of,optometric vision therapy in such patients will be discussed.Using bio-engineering models of the oculomotor system asthe conceptual framework, emphasis will be focused on stud-ies that used objective recording techniques to directlyassess therapeutically related changes in oculomotorresponsivity.
Results and Conclusions: The findings clearly support thevalidity of optometric vision therapy. Furthermore, the resultsare consistent with the tenets of general motor learning.
Key Words: Accommodation, behavior modification, motor learn-ing, oculomotor plasticity, oculomotor responsivity, vergence,vision therapy

ISSUE HIGHLIGHT
metric clinical practice. The specifically relatedsigns and symptoms may also initially bereported to, or uncovered by, the orthoptist, oph-thalmologist, neurologist, internist, or general pri-mary care medical practitioner, as well as othersin the allied health and educational professions(e.g., school nurses, remedial reading teachers,etc.). Failure to detect and diagnose these prob-lems may have grave consequences to somepatients and, hence, legal consequences.21
In symptomatic, nonpresbyopic clinic patients, theprevalence of accommodative dysfunction andcorrelated symptoms is estimated at: accom-modative insufficiency, 9.2%; accommodativeinfacility, 5.1%; and accommodative spasm,2.5%.22 However, as one might expect, in clinicpatients who are receiving treatment for manifestbinocular dysfunctions, the prevalence is muchhigher (60% to 80%).22,23 Thus, accommodative dis-orders are common in the general optometric clinicpopulation.
With respect to the prevalence of fusional ver-gence dysfunction, the most-common type is con-vergence insufficiency. The median prevalence is7%, in both children and adults.24 Other relativelyfrequent vergence dysfunctions include: conver-gence excess, 5.9% to 7.1%;22,25 basic exophoria,2.8%;26 fusional vergence dysfunction, <7%;27
and clinically significant vertical phoria, 9%.28
Thus, as was true for accommodative disorders, ver-gence disorders are also common in the general opto-metric clinic population.
Symptoms reported in patients who manifest nonstrabismic accommodative and vergence disordersThere are a wide range of symptoms reported inpatients who manifest nonstrabismic accom-modative and vergence disorders.26 With respectto accommodation, these include: blurred visionat distance and/or near during or immediately fol-lowing nearwork, headaches, poor concentration,and difficulty reading. With respect to vergence,these include: blurred vision, diplopia, ocular dis-comfort during or immediately following near-work, frontal headaches, nausea, sleepiness, lossof concentration, heavy lid sensation, generalfatigue, and “pulling” sensation of the eyes. Ofinterest, the symptom preventing tactic of task“avoidance” may be used by some, thus negativelyimpacting on overall quality of life—especiallywith respect to school and work performance.
Cure rates in patients who manifest nonstrabismic accommodative and vergence disordersThe cure rates in symptomatic patients who man-ifest nonstrabismic accommodative and fusionalvergence disorders are very high (also see‘Accommodative Therapy’ and ‘Vergence Ther-apy’ sections). Cure rates for accommodative dis-orders generally ranged from 80% to 100%,26 andcure rates for vergence disorders generallyranged from 70% to 100%.26 Thus, both theaccommodative and vergence systems are remark-ably remediable and exhibit considerable oculomo-tor plasticity, with concurrent marked reduction ofsymptoms.
The clinical practice of optometric vision ther-apy has had nearly 75 years to evolve to its pres-ent level within the optometric community.29,30
Before that, however, its more narrowly focusedcounterpart of orthoptics was founded inFrance by the ophthalmologist Javal in the mid-nineteenth century (1858) and is still practicedwidely—especially in Europe and the UnitedKingdom—in ophthalmological clinics.3 In 1915,in the United States, Duane31 reported that 10%of his ophthalmological clinic patients mani-fested nonpathological, functional, accom-modative disorders that he believed could beremediated by accommodative “exercises” heproposed. Both optometrically based vision ther-apy and ophthalmologically based orthopticshave had a long history, and are currentlyactively involved in the successful managementand treatment of a wide range of oculomotordysfunctions, including those with nonstrabis-mic accommodative and vergence disorders.From this rich background, well-developedand scientifically based treatment plans withcommon elements have evolved—especially inoptometry—to efficiently and cost-effectivelyremediate disorders of both of these oculomo-tor systems26 (see Figures 1 and 2). Clinicalguidelines and important conceptual notionsregarding these specific nonstrabismic accom-modative and vergence disorders have evolvedin optometry based on a wide range of labora-tory, clinical, and epidemiologic investigationsover the years.26,32-36 All of these factors havecontributed to keen insights and increasedunderstanding of functionally based, nonstra-bismic, accommodative and vergence disordersin clinical practice, resulting in the high successrates found following therapeutic intervention.
736
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
ISSUE HIGHLIGHT
The balance of this article will establish the sci-entific basis for, and efficacy of, optometric visiontherapy. It will have the following organizationalstructure. First, using bio-engineering models of
the oculomotor system as the conceptual frame-work, a detailed quantitative overview of variousstatic and dynamic models of accommodationand/or vergence having a direct bearing on opto-
737
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
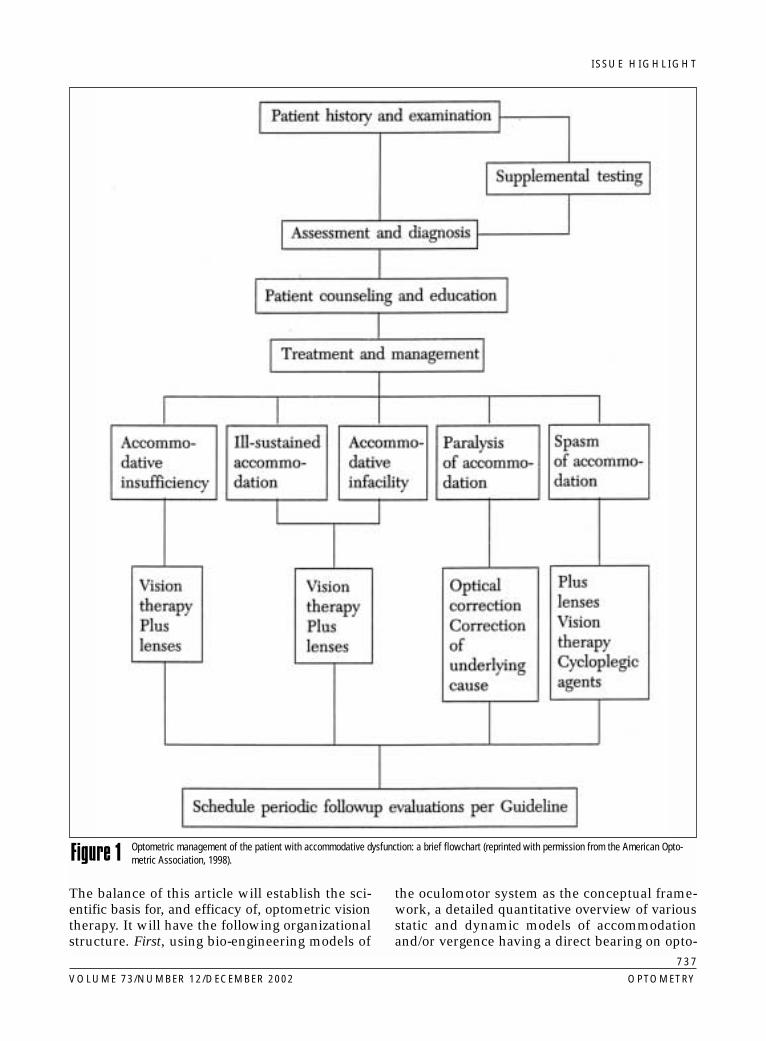
Optometric management of the patient with accommodative dysfunction: a brief flowchart (reprinted with permission from the American Opto-metric Association, 1998).Figure 1

ISSUE HIGHLIGHT
738
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
Optometric management of the patient with vergence dysfunction: a brief flowchart (reprinted with permission from the American OptometricAssociation, 1998).Figure 2

ISSUE HIGHLIGHT
metric vision therapy will be provided. In addi-tion to specifying and describing these directapplications, the importance of models will be fur-ther developed in subsequent sections. Second,selected research studies that provide support forthe scientific basis for and efficacy of optomet-ric vision therapy will be reviewed. The empha-sis will focus on objective findings, although theresults of other carefully conducted clinical inves-tigations will be considered. And third, moreglobal aspects will be considered, including therelationship between vision therapy, generalmotor learning, and oculomotor plasticity.
Models of the accommodative and vergence systemsVarious static and dynamic models of the accom-modative and vergence systems have been pro-posed over the past 50 years.37-53 Models providea comprehensive, organizational framework forlogical thinking and conceptual understanding ofa system’s elemental components within the con-
text of its overall structural framework, especiallyas the body of knowledge increases. By consid-ering individual components, one can understandwhen specific system aspects are abnormal priorto vision therapy, which aspects normalize sub-sequent to vision therapy, and how vision ther-apy itself may be specifically tailored based on theoverall model structure. All of these points willbe addressed to some extent in subsequent sec-tions of this article. Models also allow non-inva-sive, “dry dissection” and testing of a system andits underlying neurological control structure byperforming computer simulations incorporatinga variety of mathematical techniques. For exam-ple, sensitivity analysis49 allows one to ascertainthe likelihood of a specific oculomotor systemcomponent being responsible for the observedanomalous response pattern. As an illustration,it was found that the oculomotor gain controlcomponents were most sensitive to variation inmodel parameter values, as gain terms effectivelymultiply the incoming system error information.
739
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
Simplified, conceptual model of Hung et al., 1996 (reprinted with permission, from Ong and Ciuffreda, 1997).Figure 3
ISSUE HIGHLIGHT
Thus, small variations in, or deviations from, thenorm would be predicted to have large effects onsystem response amplitude—i.e., either beingexcessive or insufficient.
However, few models have met three basicrequirements:
1. model parameter values that agree withempirically derived physiologic data,
2. computer-simulated responses—especiallydynamically—to a variety of inputs (such aspulses, steps, ramps, and sinusoids) thatagree with the empirically derived physio-logic data, and
740
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
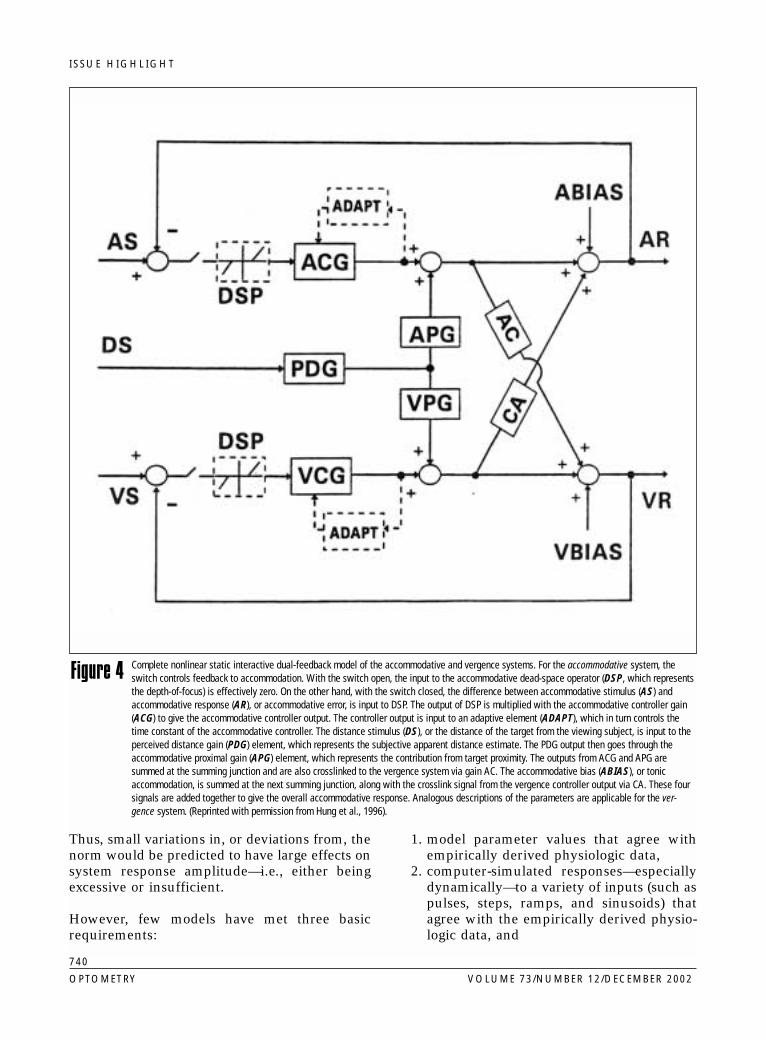
Complete nonlinear static interactive dual-feedback model of the accommodative and vergence systems. For the accommodative system, theswitch controls feedback to accommodation. With the switch open, the input to the accommodative dead-space operator (DSP, which representsthe depth-of-focus) is effectively zero. On the other hand, with the switch closed, the difference between accommodative stimulus (AS) andaccommodative response (AR), or accommodative error, is input to DSP. The output of DSP is multiplied with the accommodative controller gain(ACG) to give the accommodative controller output. The controller output is input to an adaptive element (ADAPT), which in turn controls thetime constant of the accommodative controller. The distance stimulus (DS), or the distance of the target from the viewing subject, is input to theperceived distance gain (PDG) element, which represents the subjective apparent distance estimate. The PDG output then goes through theaccommodative proximal gain (APG) element, which represents the contribution from target proximity. The outputs from ACG and APG aresummed at the summing junction and are also crosslinked to the vergence system via gain AC. The accommodative bias (ABIAS), or tonicaccommodation, is summed at the next summing junction, along with the crosslink signal from the vergence controller output via CA. These foursignals are added together to give the overall accommodative response. Analogous descriptions of the parameters are applicable for the ver-gence system. (Reprinted with permission from Hung et al., 1996).
Figure 4

ISSUE HIGHLIGHT
3. homeomorphic model structure that there-fore reflects the underlying anatomy andphysiology. All of the models to be discussedfulfill these basic requirements.
Static model of the accommodative and vergence systemsA useful static, or steady-state, model of theaccommodative and vergence systems and itsmotor interactions by Hung and his col-leagues46,47,53 has evolved over the past 20 years.This model and its variations have been useful forfurthering our understanding of a wide range ofbasic mechanisms53 (e.g., vergence and accom-modative adaptation), as well as their applicationto a range of important clinical conditions (i.e.,amblyopia,54,55 strabismus,56 nystagmus,57
myopia,58 and vergence and accommodative dys-function49). For example, after completion of adynamic vergence response from far to near, thestatic model specifies the resultant steady-stateerror for accommodation (e.g., lag of accommo-dation as assessed clinically with the retinoscope)and vergence (e.g., fixation disparity as assessedclinically with a disparometer), and allows themodeller to vary the internal, neurologically basedcontrol parameters to predict and assess theimpact on system errors. A conceptual version oftheir latest model is presented in Figure 3.59
This latest version, transformed into the bio-engineering domain, is presented in Figure 4,47
with parameter values presented in Table 1. Pro-gressing from left to right in the figure, it may beseen that the accommodative (upper) and vergence(lower) negative feedback control loops have sim-ilar component structures.
InputThe input or stimulus change for accommodation(AS) (target distance in diopters) and disparity
vergence (VS) (target distance inmeter angles, MA) sum alge-braically with the negative feed-back response of the respectivesystem at that moment. Theresultant difference representsthe system’s initial error (AE orVE, respectively). The input forthe proximal branch is per-ceived target distance, withsuch perceptually derived prox-imal information not having aseparate feedback loop, butrather inputting directly and
simultaneously into both the accommodative andvergence feedback loops. Under normal binoc-ular, closed-loop (i.e., with blur and retinal dis-parity feedback present) viewing conditions, theproximal drive only adds 0.4% and 4% to thefinal steady-state vergence and accommodativeresponses, respectively.47 Hence, blur and disparityare the primary stimuli in their respective systems.Thus, appropriate manipulation of the blur (vialenses and target distance) and retinal disparity (viaprisms, mirrors, and target distance) used in visiontherapy will maximize the potential improvementsin system responsivity. Proximal informationenhances overall responsivity by providing importantcue reinforcement derived from the perceived depthinformation. However, without the constraintsimposed by feedback control (i.e., under open-loopconditions), the effect of proximal information on themotor response is substantial.47
Threshold “deadspace” operator (DSP)This represents the depth-of-focus for accom-modation and Panum’s fusional areas for disparityvergence. This component allows small neu-rosensory-based system error (i.e., retinal defo-cus and retinal disparity, respectively) to betolerated without adverse perceptual conse-quences (i.e., blur and diplopia, respectively). Ifthe input error exceeds its threshold level, thiserror information proceeds to drive the respectivesystem. However, even if the vergence error doesnot exceed the deadspace, a large residual fixationdisparity may adversely affect visual performanceor cause a small foveal binocular suppression sco-toma to develop. Therapeutic manipulations involv-ing the development of increased sensitivity to blurand disparity via lens and prism sorting procedures,55
respectively, will improve neurosensory sensitivity andincrease response amplitude in cases in which thishas been reduced.
741
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
Table 1. Static model values for accommodation and vergenceAccommodation Vergence
DSP = ± 0.15 D PFA = ± 5.0 min arcACG = 10.0 VCG = 150AC = 0.80 D/MA CA = 0.37 MA/DABIAS = 0.61 D VBIAS = – 0.29 MAADAPT = 4.0 ADAPT = 9APG = 2.10 VPG = 0.067PDG = 0.212 PDG = 0.212
(See text for explanation and description of abbreviations. Also see related figures/figure legends.)
ISSUE HIGHLIGHT
GainThe accommodative (ACG = AR – ABIAS) and
AE – DSP
vergence (VCG = VR – VBIAS) controller gains rep-VE – DSP
resent the experimentally derived, open-loop,internal neurological controller gains of the
respective systems. The final system error signal,which equals the initial system error minus thedeadspace threshold value, is multiplied by thisgain element. Its output provides the majority ofthe neurological control signal to formulate thefinal steady-state motor response. For example, anabnormally high accommodative controller gainwould result in accommodative excess, whereas
742
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
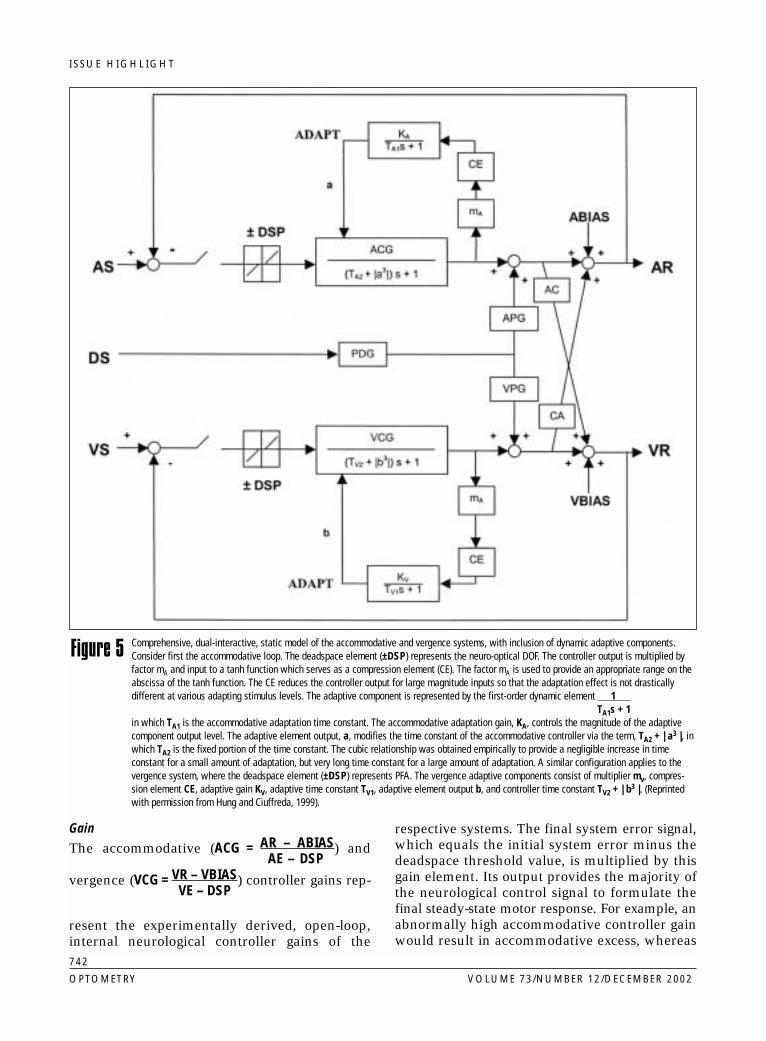
Comprehensive, dual-interactive, static model of the accommodative and vergence systems, with inclusion of dynamic adaptive components.Consider first the accommodative loop. The deadspace element (±DSP) represents the neuro-optical DOF. The controller output is multiplied byfactor mA and input to a tanh function which serves as a compression element (CE). The factor mA is used to provide an appropriate range on theabscissa of the tanh function. The CE reduces the controller output for large magnitude inputs so that the adaptation effect is not drasticallydifferent at various adapting stimulus levels. The adaptive component is represented by the first-order dynamic element 1
TA1s + 1in which TA1 is the accommodative adaptation time constant. The accommodative adaptation gain, KA, controls the magnitude of the adaptivecomponent output level. The adaptive element output, a, modifies the time constant of the accommodative controller via the term, TA2 + | a3 |, inwhich TA2 is the fixed portion of the time constant. The cubic relationship was obtained empirically to provide a negligible increase in timeconstant for a small amount of adaptation, but very long time constant for a large amount of adaptation. A similar configuration applies to thevergence system, where the deadspace element (±DSP) represents PFA. The vergence adaptive components consist of multiplier mv, compres-sion element CE, adaptive gain KV, adaptive time constant TV1, adaptive element output b, and controller time constant TV2 + | b3 |. (Reprintedwith permission from Hung and Ciuffreda, 1999).
Figure 5

ISSUE HIGHLIGHT
an abnormally low gain would result in accom-modative insufficiency. Thus, therapeutic manip-ulations that normalize gain will markedly improveresponse accuracy. The output of the controllergain is then input to three other components (seenext three components below).
Adaptive gain loopAlthough typically regarded to be a dynamicmodel element, following intense and pro-longed nearwork, it may bias the final, staticopen-loop or closed-loop system response.However, under nonsustained viewing condi-tions, its value is zero (see later dynamic modelsection).
Crosslink gainThe crosslink gain (AC for accommodation andCA for convergence) multiplies the output of thedirect ACG or VCG pathway, respectively. Foraccommodation, this new value represents theeffective accommodative-convergence to accom-modation (AC) ratio, whereas for convergence it
Arepresents the effective convergence-accommo-dation to convergence (CA) ratio. These gains have
Cbeen found to be highly sensitive to parameter valuevariations, and thus responsible for producing a rangeof clinical oculomotor imbalances.49 For example, anabnormally low AC crosslink gain value would resultin convergence insufficiency, whereas an abnormallyhigh value would result in convergence excess (see Fig-ures 3 and 4).
Tonic inputTonic input for accommodation (ABIAS) and ver-gence (VBIAS) has been speculated to reflectlow-level, stable midbrain baseline neuralinnervation, although other brain regions maybe involved. Although both the tonic vergenceand accommodative terms have substantialeffects on the response amplitude with both sys-tems rendered open-loop (i.e., with their visualfeedback rendered ineffective), they have neg-ligible influence on the overall closed-loop nearresponse and only modest influence on theclosed-loop far response.46 Thus, any abnormal-ity of or therapeutic effect on system responsivityunder normal viewing conditions would be minor.This is shown in the following equation andexample with respect to monocular blur-drivenaccommodation, in which:
AR = ACG × AS + [–DSP × ACG + ABIAS × 1 ]1+ACG 1+ACG 1+ACG
For a typical value of ABIAS = 1 diopter and ACG= 9, the effect of ABIAS on AR would only be0.1 diopter (D). This relative lack of effect is evenmore dramatic for disparity vergence (with itsmuch higher controller gain value) with accom-modation open-loop, in which:
VR = VCG × VS + [–DSP × VCG + VBIAS × 1 ]1+VCG 1+VCG 1+VCG
For a typical value of VBIAS = 1 MA and VCG= 149, the effect of VBIAS on VR would only be0.007 MA.
Summing junctionThe direct gain output is also sent to the neuro-logical summing junction, where it adds with thecrosslink output and the tonic input, both ofwhich have only modest-to-moderate influence onthe fellow system, to formulate the final com-bined signal to drive the respective system. Thissumming junction may reside in the midbrain.
Peripheral apparatusThe output of the summing junction proceeds tocortical and subcortical centers related to accom-modation60,61 and vergence51 to formulate theaggregate neural signal. It then advances to inner-vate the appropriate peripheral apparatus—the cil-iary muscle and lens complex for accommodationand the extraocular muscles for vergence.
OutputThese motor changes are then fed back to the ini-tial summing junction via the negative-feedbackpathways. If a relatively large residual errorremains, the cycle is repeated, until an acceptablysmall and stable steady-state error for both sys-tems is attained. If the error cannot be reducedfor whatever reason, such as low vergence con-troller gain, however, then diplopia would result;for accommodation, the outcome would be sus-tained blur.
Incorporation of adaptive dynamic components into the modelIn addition to the basic dual-interactive static com-ponents described above, adaptive dynamic gaincomponents were more-recently incorporated intothe accommodative and vergence controllers for
743
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY

ISSUE HIGHLIGHT
establishment of a new dynamic, time-dependent,nearwork oculomotor model,53 which was specif-ically developed to gain insight into the clinical enti-ties of nearwork-induced transient myopia andpermanent myopia59 (see Figure 5). The adaptiveloops function to sustain the motor response fora prolonged period (i.e., several seconds or min-utes); for example, during reading. The adaptivegain element in each feedback loop receives itsinput signal from the controller (ACG or VCG)output, with the adaptive loop output in turnmodifying the time constant of the controller viaterms ‘a’ and ‘b’ for the accommodative and ver-gence loops, respectively. For example, theaccommodative controller output (ACG) is inputto a multiplier (mA) and compression element (CE)to drive the adaptive element having gain (KA) andtime constant (TA1). Of considerable clinicalimportance was the finding that this accommodativeadaptive gain, KA, was the primary model componentrelated to nearwork-induced transient myopia(NITM):59 high adaptive gain, as found in myopes,produced significantly slowed decay of accommoda-tion to pre-task baseline distance levels. Andaccommodative vision therapy normalized thismodel parameter value62 (see ‘Accommodative Ther-
apy’ section). The multiplier and compressionelements are necessary to provide a saturationeffect for large inputs that are found in the var-ious adaptation experiments. The adaptive ele-ment output, ‘a’, is incorporated into andmodifies the overall time constant of the accom-modative controller via the term, TA2 + |a3| , inwhich TA2 is the fixed portion of the time con-stant. The cubic relationship was obtainedempirically to provide negligible increase in thetime constant for smaller amounts of adaptation,but a larger increase in the time constant forgreater amounts of adaptation. Similar to theaccommodative adaptive element, the vergenceadaptive component consists of multiplier, mV,compression element, CE, adaptive gain, KV,adaptive time constant, TV1, adaptive element out-put, ‘b’, and controller time constant, TV2 + |b3|.
Neurophysiological version of static model of the accommodative and vergence systemsRecently, a neurophysiologically based configu-ration of the basic Hung and et al.’s45,47 staticmodel of the accommodative and vergence sys-tem has been proposed63 (see Figure 6; compare
744
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
Neurophysiological version of static accommodative and vergence model of Hung and colleagues. Symbols: BA = blur-driven accommodation, DC= disparity-driven convergence, NR = midbrain near response cells, G = midbrain near response cell gains, AR = accommodative response, andVR = vergence response. (Reprinted with permission from Mays and Gamlin, 2000). For Figures 3, 4, 5, and 6, see text for explanation of symbols.
Figure 6
ISSUE HIGHLIGHT
with Figure 4). All of the intermediary block ele-ments of the earlier static control system modelsdescribed have been replaced by their neurolog-ical analogs—namely, gains (G), near responsecells (NR), and neural averagers (AVG). Hence, thebioengineering models described earlier areindeed homeomorphic, and thus have true neu-rophysiological representation, albeit somewhatspartan at the present time. However, no simu-lations have been performed using this model.
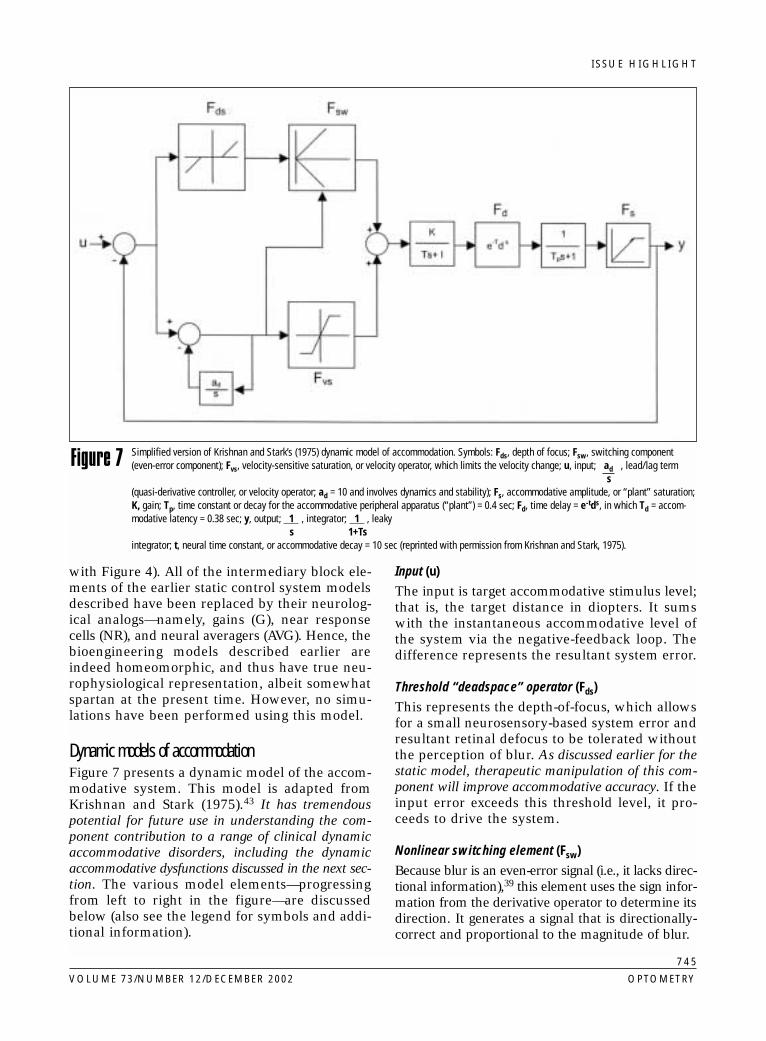
Dynamic models of accommodationFigure 7 presents a dynamic model of the accom-modative system. This model is adapted fromKrishnan and Stark (1975).43 It has tremendouspotential for future use in understanding the com-ponent contribution to a range of clinical dynamicaccommodative disorders, including the dynamicaccommodative dysfunctions discussed in the next sec-tion. The various model elements—progressingfrom left to right in the figure—are discussedbelow (also see the legend for symbols and addi-tional information).
Input (u)The input is target accommodative stimulus level;that is, the target distance in diopters. It sumswith the instantaneous accommodative level ofthe system via the negative-feedback loop. Thedifference represents the resultant system error.
Threshold “deadspace” operator (Fds)This represents the depth-of-focus, which allowsfor a small neurosensory-based system error andresultant retinal defocus to be tolerated withoutthe perception of blur. As discussed earlier for thestatic model, therapeutic manipulation of this com-ponent will improve accommodative accuracy. If theinput error exceeds this threshold level, it pro-ceeds to drive the system.
Nonlinear switching element (Fsw)Because blur is an even-error signal (i.e., it lacks direc-tional information),39 this element uses the sign infor-mation from the derivative operator to determine itsdirection. It generates a signal that is directionally-correct and proportional to the magnitude of blur.
745
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
Simplified version of Krishnan and Stark’s (1975) dynamic model of accommodation. Symbols: Fds, depth of focus; Fsw, switching component(even-error component); Fvs, velocity-sensitive saturation, or velocity operator, which limits the velocity change; u, input; ad , lead/lag term
s(quasi-derivative controller, or velocity operator; ad = 10 and involves dynamics and stability); Fs, accommodative amplitude, or “plant” saturation;K, gain; Tp, time constant or decay for the accommodative peripheral apparatus (“plant”) = 0.4 sec; Fd, time delay = e-tds, in which Td = accom-modative latency = 0.38 sec; y, output; 1 , integrator; 1 , leaky
s 1+Tsintegrator; t, neural time constant, or accommodative decay = 10 sec (reprinted with permission from Krishnan and Stark, 1975).
Figure 7
ISSUE HIGHLIGHT
Derivative controller (ad)s
This parallel, pseudo-derivative (i.e., a mathe-matical approximation to a true derivative) con-troller component is a velocity operator. It
generates the derivative of the error signal (i.e.,the instantaneous velocity) for use by its controlprocess. Such a controller improves the transientstability, as well as the speed, of the response. Spe-cific therapy (e.g., low-power lens flippers creating
746
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
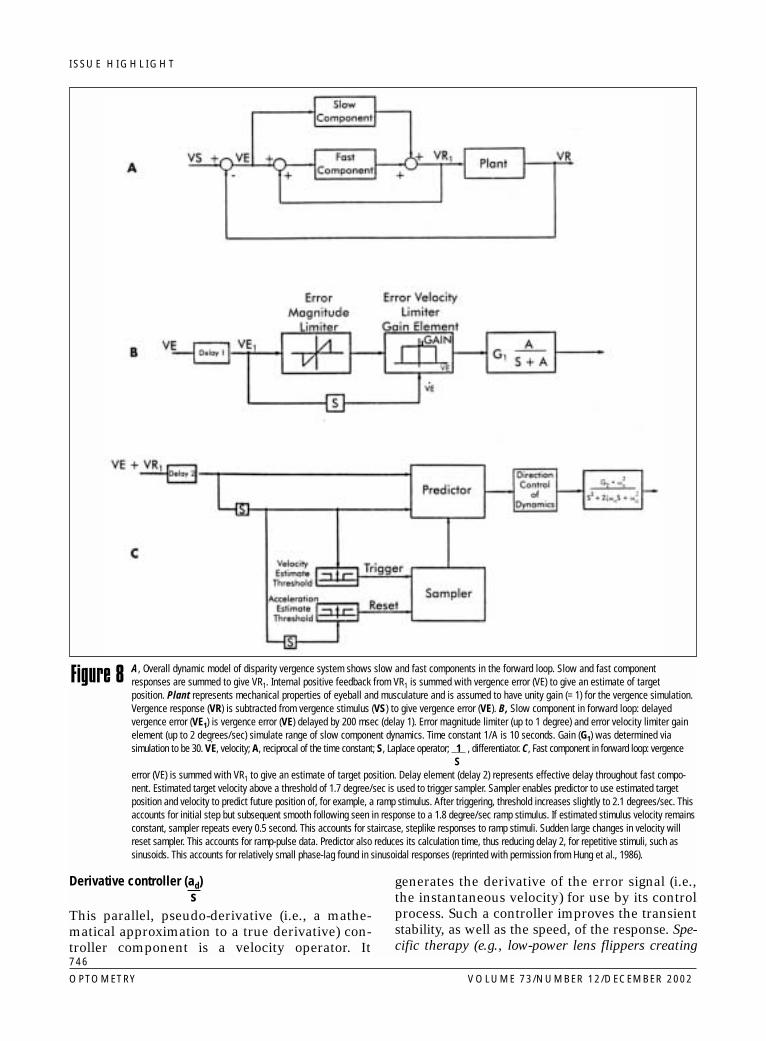
A, Overall dynamic model of disparity vergence system shows slow and fast components in the forward loop. Slow and fast componentresponses are summed to give VR1. Internal positive feedback from VR1 is summed with vergence error (VE) to give an estimate of targetposition. Plant represents mechanical properties of eyeball and musculature and is assumed to have unity gain (= 1) for the vergence simulation.Vergence response (VR) is subtracted from vergence stimulus (VS) to give vergence error (VE). B, Slow component in forward loop: delayedvergence error (VE1) is vergence error (VE) delayed by 200 msec (delay 1). Error magnitude limiter (up to 1 degree) and error velocity limiter gainelement (up to 2 degrees/sec) simulate range of slow component dynamics. Time constant 1/A is 10 seconds. Gain (G1) was determined viasimulation to be 30. V
·E, velocity; A, reciprocal of the time constant; S, Laplace operator; 1 , differentiator. C, Fast component in forward loop: vergence
Serror (VE) is summed with VR1 to give an estimate of target position. Delay element (delay 2) represents effective delay throughout fast compo-nent. Estimated target velocity above a threshold of 1.7 degree/sec is used to trigger sampler. Sampler enables predictor to use estimated targetposition and velocity to predict future position of, for example, a ramp stimulus. After triggering, threshold increases slightly to 2.1 degrees/sec. Thisaccounts for initial step but subsequent smooth following seen in response to a 1.8 degree/sec ramp stimulus. If estimated stimulus velocity remainsconstant, sampler repeats every 0.5 second. This accounts for staircase, steplike responses to ramp stimuli. Sudden large changes in velocity willreset sampler. This accounts for ramp-pulse data. Predictor also reduces its calculation time, thus reducing delay 2, for repetitive stimuli, such assinusoids. This accounts for relatively small phase-lag found in sinusoidal responses (reprinted with permission from Hung et al., 1986).
Figure 8

ISSUE HIGHLIGHT
relatively small blur magnitudes) directed to sensi-tizing this component will produce more-rapid, oscil-lation-free, and time-optimal responsivity.
Nonlinear saturation element (Fvs)This element is a velocity-sensitive componentthat prevents the resultant response velocity fromexceeding a specified limit. This, too, facilitatesdynamic response stability and limits the amplitudeof instability oscillations of the accommodativeresponse.
”Leaky” integrator ( 1 )1 + Ts
The “leaky” integrator is a “charge/discharge” ele-ment. It represents a central neurological inte-grating circuit that is rapidly activated (“charged”like a capacitor) by the visual input which then“stores” this information, thus providing steady-state maintenance of the response. “Discharge” ofthis element is reflected in the decay rate, orreciprocal of the time constant, of the systemdynamics.64 Abnormally slow decay may result intransient blur and diplopia for the accommodativeand vergences systems, respectively.
Time delay (Fd)This represents the combined neural and bio-mechanical transmission time delays, orlatency/reaction time. As discussed in the next sec-tion, accommodative vision therapy has beendemonstrated to reduce this delay by a modestamount in cases in which it is abnormally long, withthis perhaps also involving attentional and/or pre-dictive aspects.
Ciliary muscle/lens dynamics ( 1 ) TPs + 1
This represents the biomechanical responsecharacteristics of the combined ciliary muscle/lenszonules/lens/lens capsule complex, or “plant”.
Saturation element (Fs)The saturation element limits the accommodativeresponse imposed by the lens elasticity andrelated structures. In effect, it represents the ampli-tude of accommodation.
Output (y)This represents the accommodative system’s finaloutput. It is transmitted back to the input via thenegative feedback loop, where it is subtractedfrom the current input level. If a relatively large
residual error remains, the cycle is repeated untilan acceptable error is attained.
A different dynamic model, one in which thedual-mode control characteristics were empha-sized, was developed by Hung and Ciuffreda(1988).48 The rationale for a system having “dual-mode” control—i.e., having “fast” and “slow”dynamic control components—is to provideoverall system stability in a feedback loop that hasa relatively long latency (i.e., equal to or longerthan the dynamic step response latency). Thismodel provides the scientific basis and justificationfor use of both step and ramp stimuli in accom-modative vision therapy paradigms.
Based on monocular accommodative trackingresponses to ramps (i.e., constant velocity blur-only stimuli), as well as computer simulations, itwas concluded that the accommodative systemoperated in two basic modes, “fast” and “slow”,and hence the term dual-mode control. The “fast”component is used to track rapidly moving (> 2.0D/sec), constant-velocity ramp stimuli, as well asinstantaneous steps of blur. This “fast” componentis preprogrammed and thus open-loop in nature,and does not use visual feedback related to blurof the retinal image during its initial dynamic tra-jectory. By contrast, the “slow” component is usedto track slowing-moving (≤ 0.5 D/sec) ramp stim-uli, as well as to correct small, residual errorsremaining in the step tracking response. This“slow” component is closed-loop in nature, andthus uses visual feedback related to blur of theretinal image during its dynamic trajectory. Andfor intermediate velocity ramps of blur stimuli,a mixture of ramp-like and step-like motorresponses are intermingled.
Thus, for a typical blur-driven, accommodativestep response, the “fast” component is responsi-ble for the initial (300 to 500 msec) and largeopen-loop, exponentially characterized portion ofthe motor response, whereas the “slow”, visualfeedback-driven, closed-loop component isresponsible for completion of the response (500to 700 msec) to attain clear retinal-imagery lyingwithin the depth-of-focus of the eye.
Dynamic model of disparity (fusional) vergenceA dynamic model45 of disparity vergence is pre-sented in Figure 8. This model provides the scien-tific basis and justification for use of both step andramp stimuli in the vergence vision therapy para-
747
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY

ISSUE HIGHLIGHT
digms. The current model hastwo major subdivisions or com-ponents analogous to those pro-posed earlier for accommodation:
1. The “fast component” is usedto track perceived targetvelocity (with a latency/reaction time or delay of200 msec) of rapidly movingtargets (> ~2 degrees/sec),such as occurs with rapidramps, fast sinusoids,pulses, and the more-com-mon and naturalistic stepsof disparity input. Ratherthan using continuousvisual feedback—as earliersimple servomechanism-based models hadassumed—the fast compo-nent is preprogrammed oropen-loop, and it is trig-gered by, and then samples,the rapidly moving target.Its direct feed-forward path-way dynamically representsthe “fast” subsystem. That is, this complexis responsible for generating the initial 300to 500 msec or so of the response to a dis-parity input and accounts for most of theoverall response amplitude. A predictor oper-ator then predicts future target position, suchas where it will be 500 msec later based onestimated target position and velocity at thetime of sampling, and subsequently sends acommand to make such a motor response.The fast component’s motor responseapproximates an exponential.
2. The “slow component” is used to track slowly-moving targets (<~2 degrees/sec), as wellas small residual errors remaining in the steptracking response. It is driven by vergenceerror (with a delay of 50 msec for pre-dictable stimuli and 200 msec for nonpre-dictable stimuli). Thus, in contrast to theopen-loop, nonvisual feedback neurologicalcontrol structure and response of the initialfast component described above, the slowcomponent incorporates a closed-loopresponse. Since the slow component usescontinuous visual feedback, it functions tocorrect any slow and small residual or accu-mulating vergence error (<1 degree ampli-tude, <1.8 degrees/sec velocity), especially
following slightly inaccurate and rapidopen-loop fast component step responses, oralso fast-ramp responses. Note that this slowcomponent is not to be confused with the“slow” adaptive dynamic gain element dis-cussed earlier, which is responsible for long-term decay following prolonged nearwork.
Thus, in a typical step disparity vergenceresponse, the “fast”, preprogrammed, open-loopcomponent is responsible for the initial and largeportion of the response, whereas the “slow,” small,visual feedback-driven, closed-loop component isresponsible for completion of the response toattain bi-fixation and fusion within foveal Panum’sfusional areas.
Accommodative therapyPrimary studiesThere have been three primary studies conductedover the past 20 years or so that have clearlydemonstrated the efficacy of accommodativetherapy in patients who manifested combinedaccommodative insufficiency (i.e., reducedresponse amplitude) and infacility (i.e., sloweddynamics). These investigations used objectiverecording techniques to assess therapeutically
748
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
Accommodation responses of subject. Upper records show slow response dynamics forpositive accommodation and slow, multiphasic response dynamics for relaxation ofaccommodation before orthoptic training. Bottom records show the patient’s improvementafter training with faster velocities in both directions of accommodation. Note twodiscontinuous spikes in the upper record when the patient blinked; stimuli for each areunpredictable step changes between targets set at 1.5 and at 4.5 D (reprinted withpermission from Liu et al., 1979).
Figure 9

ISSUE HIGHLIGHT
related anatomical and physiological changes inthe accommodative system, which reflect systemneuroplasticity, as well as appropriate statisticalanalyses whenever possible.
The earliest study was performed by Liu et al.65
in 1979. Three young adult patients with symp-toms of blur during and/or immediately follow-ing short periods of nearwork were tested. Adynamic optometer integrated within a clinicalslit-lamp, which directly measured anatomicalcrystalline lens movement and physiologically-related luminous flux changes in the central ante-rior region of the crystalline lens and anteriorchamber, was used in the laboratory environmentto assess accommodative dynamics pre- and post-accommodative vision therapy. Conventional
home therapy was institutedover periods that ranged from 4to 7 weeks for 20 minutes perday. The therapy consisted ofstep dioptric blur stimuli (i.e.,jump focus and lens flippers) andramp dioptric blur stimuli (i.e.,pencil push-ups),1-3 which isconsistent with the dynamicaccommodative model and dual-mode accommodative controldescribed earlier. Direct changesin crystalline lens responsedynamics pre- and post-therapyare presented in Figures 9 and10. Clearly, the overall lens dynam-ics became more-rapid and normalized following the accom-modative therapy. The primarychange was in the innervationaland biomechanical aspect of thecrystalline lens response time.This can be described and quan-tified using the bioengineeringmeasure of “time constant,”which refers to the time for anexponential response to attain63% of its final steady-stateamplitude.64 Clearly, the timeconstant for both increasing anddecreasing accommodationreduced and normalized (seeFigure 10). The reduction in timeconstant suggested revision andimprovement in the neuromotorcontrol program,66 thereby lead-ing to a more-efficient and time-
optimal response. Furthermore, a reduction intime constant means a greater rate of change ofthe anterior curvature of the lens with increasingor decreasing accommodation. That in turnimplies either a greater rate of force output pro-duced by the neuromuscular system of the ciliarymuscle67 and/or more-synchronized innervation.The accommodative latency, or reaction time—thetime from stimulus onset to crystalline lensresponse onset—also normalized (see Figure 10),although this parameter was only slightly abnor-mal (i.e., prolonged) initially. Reduction oflatency means a shorter reaction time of the sys-tem, which may indicate more-efficient signal pro-cessing at the cortical level. Specifically, withrespect to the dynamic accommodative model (seeFigure 7), these findings reflect changes in the
749
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
Change of accommodative characteristics in the three subjects as measured weeklythrough changes in time constants (TC), latencies (L), and flipper rates during theiraccommodative therapy program. Mean values are plotted for time constant and latencygraphs, with standard errors denoted by the error bars. Flipper rates are self-reported byeach subject (reprinted with permission from Liu et al., 1979).
Figure 10

ISSUE HIGHLIGHT
threshold deadspace operator, derivative con-troller, time delay, and ciliary muscle/lensdynamics components. These objectively basedmeasures, as well as the clinical lens flipper accom-modative facility measure1-3 —which are correlatedwith objective measures of overall accommoda-tive dynamic responsivity (i.e., dynamic facil-ity)68—were themselves positively correlatedwith marked reduction in the patients’ nearworksymptoms. Thus, for the first time, it was clearly andconvincingly demonstrated that accommodativeoptometric vision therapy produced true physiologi-cal alterations in the accommodative system, reflect-ing the underlying oculomotor plasticity, withcorrelated reduction in symptoms.
In tandem with the above study, control experi-ments were independently performed.69 Subjectsincluded optometry students with accommodativeinsufficiency, patients with accommodative insuf-ficiency who elected not to receive vision ther-apy, and visually normal individuals whounderwent accommodative therapy. None exhib-ited any change in accommodative dynamics.
Four years later, the landmark Liu et al. (1979)investigation65 was confirmed and extended byBobier and Sivak70 (1983) in five young adultpatients who manifested nearwork-related blursymptoms and accommodative infacility. Theyused the objective laboratory technique of pho-torefraction, which assesses refractive-related, opti-cal changes in the retinal reflection as observedin the plane of the pupil, similar to the standardclinical technique of retinoscopy. Patients received20 minutes of daily home therapy for 3 to 6weeks, which consisted of monocular and binoc-ular accommodative therapy (step dioptric blurstimuli). In addition to confirming the types ofobjective changes reported by Liu et al.65 (asdescribed earlier), they also found lack ofregression of the positive therapy effect over the4.5-month follow-up test period. Over the sameperiod, no changes in accommodative dynamicswere found in their control subject. Clearly, thepositive physiologically based therapeutic effects per-sisted.
Three years later (1986), Hung, Ciuffreda, andSemmlow44 assessed static (i.e., steady-statechanges rather than the dynamic changesassessed in both the Liu et al.,65 and Bobier andSivak,70 investigations described above) in 21 col-lege students who reported visual symptoms of
blur and intermittent diplopia after short periodsof nearwork. They used a Hartinger coincidencerefractometer to measure accommodation objec-tively via the Scheiner principle of optical ver-gence at the retina, and used a bioengineeringmodel approach (see Figures 3, 4, 5, and 6) toassess the individual component contributionchanges versus overall global changes in accom-modative responsivity resulting from the accom-modative vision therapy. Accommodative therapywas performed both daily in the home (15 min-utes/day; step dioptric blur stimuli) and weeklyin the laboratory (30 minutes/session; ramp diop-tric blur stimuli) for an average of 12 weeks. Allof the model-based accommodative components testednormalized immediately following the accommoda-tive therapy in 15 of the subjects, with 2 of the 3 com-ponents normalizing in the others. These includedtonic accommodation (system bias), slope of theaccommodative stimulus/response function (the
closed-loop system gain = ACG ) and the con-1 + ACG
vergence-accommodation to convergence ratio ( CA ratio; related to crosslink system gain CA).
CAll of the above changes improved accuracy ofthe steady-state accommodative responses at alldistances. Furthermore, there was long-term (i.e., 6to 9 months) maintenance of the positive accom-modative training effects. There was also mainte-nance of the markedly reduced nearwork symptomsbased on a rating-scale questionnaire, as well as clin-ical lens flipper accommodative facility improve-ment, which has been found to correlate wellwith overall lens dynamic responsivity deter-mined objectively in both young adults65 and chil-dren.68 Thus, on a larger population scale, this studyconfirmed and extended the two earlier investiga-tions65,70 using objective measures of accommodation,statistical analyses, and, for the first time, a math-ematically based bioengineering control systemsmodel.
Other studiesMany patients with accommodative dysfunctionnot only have symptoms at near, but also transient(5 seconds to 5 minutes) blur at distance follow-ing relatively short periods (≤ 15 minutes) of near-work.59 This has been termed nearwork-inducedtransient myopia (NITM).53,59 This anomalousaccommodative after effect results from aninability to relax accommodation fully and rap-idly in the distance in a time-optimal and efficientmanner. This appears to reflect physiologically an
750
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
ISSUE HIGHLIGHT
abnormality of the sympathetic system59,71 andneurologically increased gain (KA) of the adaptiveloop.53 This transient myopia has been linked topermanent myopia.53,59 NITM can be conceptu-alized in clinical terms as reflecting a very mildaccommodative spasm,59 and in bioengineeringterms as reflecting nonlinear accommodative
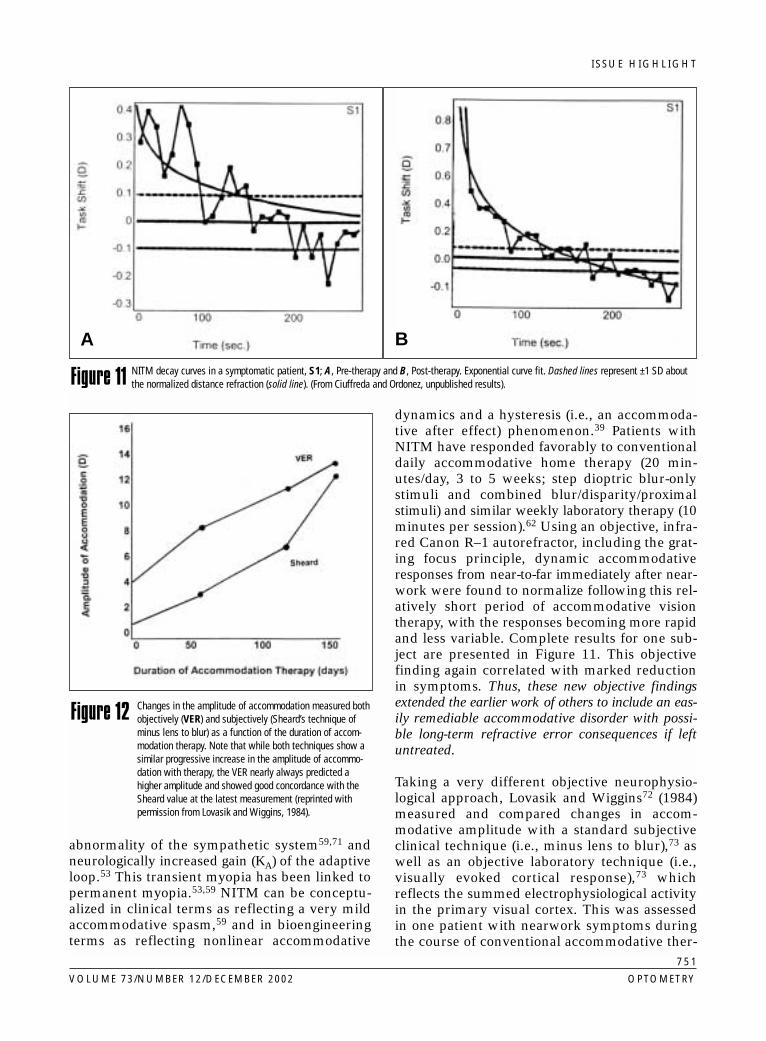
dynamics and a hysteresis (i.e., an accommoda-tive after effect) phenomenon.39 Patients withNITM have responded favorably to conventionaldaily accommodative home therapy (20 min-utes/day, 3 to 5 weeks; step dioptric blur-onlystimuli and combined blur/disparity/proximalstimuli) and similar weekly laboratory therapy (10minutes per session).62 Using an objective, infra-red Canon R–1 autorefractor, including the grat-ing focus principle, dynamic accommodativeresponses from near-to-far immediately after near-work were found to normalize following this rel-atively short period of accommodative visiontherapy, with the responses becoming more rapidand less variable. Complete results for one sub-ject are presented in Figure 11. This objectivefinding again correlated with marked reductionin symptoms. Thus, these new objective findingsextended the earlier work of others to include an eas-ily remediable accommodative disorder with possi-ble long-term refractive error consequences if leftuntreated.
Taking a very different objective neurophysio-logical approach, Lovasik and Wiggins72 (1984)measured and compared changes in accom-modative amplitude with a standard subjectiveclinical technique (i.e., minus lens to blur),73 aswell as an objective laboratory technique (i.e.,visually evoked cortical response),73 whichreflects the summed electrophysiological activityin the primary visual cortex. This was assessedin one patient with nearwork symptoms duringthe course of conventional accommodative ther-
751
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
A B
NITM decay curves in a symptomatic patient, S1; A, Pre-therapy and B, Post-therapy. Exponential curve fit. Dashed lines represent ±1 SD aboutthe normalized distance refraction (solid line). (From Ciuffreda and Ordonez, unpublished results).Figure 11
Changes in the amplitude of accommodation measured bothobjectively (VER) and subjectively (Sheard’s technique ofminus lens to blur) as a function of the duration of accom-modation therapy. Note that while both techniques show asimilar progressive increase in the amplitude of accommo-dation with therapy, the VER nearly always predicted ahigher amplitude and showed good concordance with theSheard value at the latest measurement (reprinted withpermission from Lovasik and Wiggins, 1984).
Figure 12

ISSUE HIGHLIGHT
apy. There was a large and progressive correlatedincrease in both measures over the 4-month visiontherapy period (see Figure 12). Thus, direct andobjective measures of visual cortical activity revealedmarkedly increased responsivity concurrent with theimprovement of accommodation, both during andimmediately following the course of accommodativevision therapy.
An investigation by Cooper et al.74 focused onchanges in nearwork-related asthenopia with con-ventional accommodative vision therapy.1-3 Eightyoung adult patients with combined accom-modative insufficiency and infacility underwentcomputer-automated, monocular accommodativefacility therapy in the clinic (6 weeks, 2times/week for 30 minutes; steps of dioptric blurstimuli) using a matched-subjects, cross-overexperimental design to control for placeboeffects. All patients exhibited a marked reductionin nearwork-related asthenopia as assessed by a5-point symptom rating scale questionnaire (seeFigure 13, A), as well as correlated increases inboth clinical static accommodative amplitude (seeFigure 13, B) and dynamic accommodative facil-ity. Hence, this relatively short period of accom-modative vision therapy was sufficient to remedyboth the patients’ nearwork-related signs andsymptoms. Statistically significant results werefound that demonstrated true performanceimprovement related to the accommodativetherapy. Furthermore, there was no such changeduring the cross-over control phase. Thus, those
who received the control phase first exhibited nochange, while those who received the controlphase second exhibited maintenance of the ini-tial positive therapeutic effect. Attaining statisti-cally significant changes with such a relatively smallsample size and short therapy duration attests to therobustness of the accommodative therapeutic para-digm.
In a recent clinical study conducted in a Swedishophthalmology department, Sterner et al.75 testedand trained school-age children (n = 38; ages 9 to13 years) who manifested accommodative dys-function. Symptoms included asthenopia,headaches, blurred vision, and avoidance of near-work. Accommodative facility therapy (i.e., lensflippers) was performed at home (15 minutes/day,typically for 8 weeks or less). Relative accom-modation improved in all children, and all werenow asymptomatic. In a two-year followup, 20 ofthe original 38 children agreed to participate in atelephone interview. All remained asympto-matic. Thus, both short- and long-term efficacy ofaccommodative vision therapy was once againdemonstrated, but now in younger school-age children.
In summary, the above findings clearly and sci-entifically demonstrate the efficacy of accom-modative vision therapy. This is reflected in theobjective measures of accommodation andrelated cortical control structures, formal quan-titative and informal symptom surveys, and stan-dard clinical optometric/ophthalmologic test
752
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
A, Mean asthenopia scores are presented on the ordinate, whereas phases of testing are presented on the abscissa. Open circles (� ) repre-sent patients who received experimental therapy first; closed circles (� ) represent those patients who received placebo therapy first (reprintedwith permission from Cooper et al, 1983). B, The abscissa depicts the three phases of testing, i.e., baseline, phase 1, and phase 2. Meanaccommodative amplitude for all patients in each phase (determined by minus lens to blur) is plotted on the ordinate. Open circles (� ) repre-sent patients who received experimental, accommodative training during phase 1 and placebo during phase 2. Closed circles (� ) representpatients who received the opposite condition, i.e., phase 1, control (placebo); phase 2, accommodative training (reprinted with permission fromCooper et al., 1983).
Figure 13
A B
ISSUE HIGHLIGHT
findings. The results are in agreement with aconstellation of clinical case reports and caseseries, as well as retrospective and prospectiveclinical studies, found in the optometric, oph-thalmologic, and orthoptic literatures over thepast several decades demonstrating modifiabil-ity (i.e., visual system neurosensory and neuro-motor plasticity) and normalization ofaccommodative responsivity, subsequent to rel-atively short durations of accommodative visiontherapy.26,32-36
Fusional vergence therapyTherapy for fusional (i.e., disparity) vergence dis-orders has been recognized clinically for decadesby both optometrists and ophthalmologists:
“Most recognized textbooks in the treatmentof binocular vision disorders, including thoseof Duke–Elder, von Noorden and Burian,Hugonnier and Hugonnier, Lyle and Wybar,Dale, and Griffin recommend vision therapy,or orthoptics, as the preferred treatmentoption in cases of symptomatic convergenceinsufficiency. This unanimity of opinion is jus-tified on the basis of over 1900 reported clin-ical cases assimilated during the last 47 yearsin which the average cure rate is 72%.”76
Primary studiesThe seminal work in this area based on objectivedocumentation was conducted by Grisham et al.77,78 over the past two decades in two pri-mary investigations. In both studies, objectiverecordings of horizontal fusional vergence eye
movements were made that reflected the actualoculomotor physiology related directly to the under-lying neurological control structure. In addition,appropriate statistical analyses were incorporatedwhenever possible.
In the first study (1980), Grisham77 differentiatedbetween asymptomatic normal patients (n = 4)and those with symptoms related to fusional ver-gence dysfunction (n = 4 to 14, depending on theexperiment) based on statistically significant dif-ferences in their objectively based, dynamicfusional vergence oculomotor parameters. Testand therapy stimuli consisted of small steps (2prism diopters) of convergent (10 prism diopterrange) and divergent (10 prism diopter range) dis-parity centered about the heterophoria positionwith a variable rate of step input change, thus pro-ducing variable frequency “staircases” of disparatestimuli. Overall vergence tracking rate (analogousto clinical prism flipper vergence facility1), per-cent completion of step responses, response veloc-ity, and divergence response latency discriminatedstatistically between the two groups; only con-vergence response latency did not. Thus, this inves-tigation clearly demonstrated that most of theobjectively measured dynamic fusional vergenceresponse parameters were abnormal in young adultpatients with symptomatic convergence insuffi-ciency.
Given the above critical information, the keyquestion remained to be answered in the labo-ratory environment using objective measures:
753
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
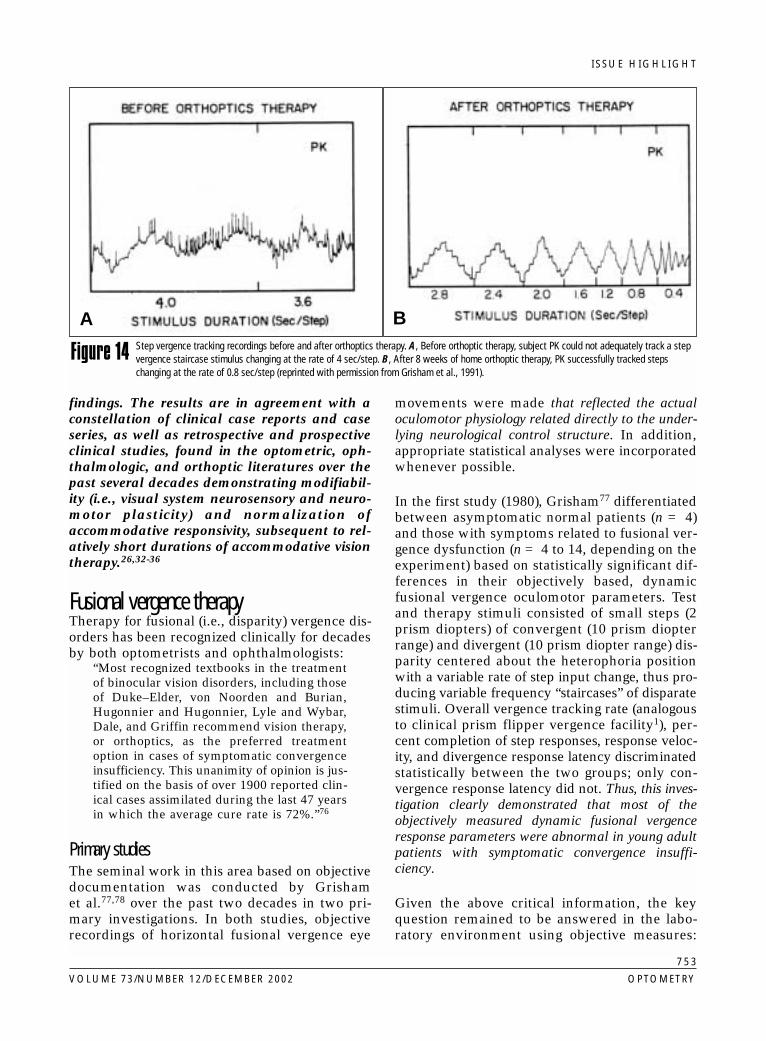
Step vergence tracking recordings before and after orthoptics therapy. A, Before orthoptic therapy, subject PK could not adequately track a stepvergence staircase stimulus changing at the rate of 4 sec/step. B, After 8 weeks of home orthoptic therapy, PK successfully tracked stepschanging at the rate of 0.8 sec/step (reprinted with permission from Grisham et al., 1991).
Figure 14
A B

ISSUE HIGHLIGHT
“Does the fusional vergence sys-tem have sufficient plasticity toalter and normalize its dynamicneuromotor response character-istics?” The second study (1991)by Grisham et al.78 clearly pro-vided a positive answer to thisimportant question, which hadits origins in the pioneeringwork of Javal (1858), an oph-thalmologist and the “father oforthoptics.”
Using a stimulus system andobjective infra-red eye movementsystem similar to that used in theaforementioned study, they firsttested patients (n = 3 to 6,depending on the experiment)with nearwork-related visual dis-comfort and clinical signs ofconvergence insufficiency. Avariety of standard clinical ver-gence and accommodative ther-apy techniques1-3 that involvedboth step and ramp disparitystimuli were assigned to eachpatient (8 weeks, 30 minute/dayat home). Post-therapeutic objec-tive changes in their fusionalvergence eye movements werestriking. Figure 14 shows overallfusional vergence tracking tosmall steps of disparity beforeand after therapy. Before fusionalvergence therapy, only a veryslow stimulus rate of changecould be followed, and that waspoorly executed using small andvariable amplitude responses. By contrast, fol-lowing therapy, the fusional vergence responseswere full, and tracking rate was remarkablyincreased (about 10-fold). These improvementsreflected changes in dynamic vergence modelparameters analogous to those suggested earlierwith respect to accommodation dynamics. Thestriking vergence improvements were correlatedwith marked reduction in symptoms, as well asnormalization of related clinical findings. Positivetherapy results did not show evidence of regres-sion over the 6- to 9-month follow-up period inmost cases (see Figure 15). And there were nochanges in the control group monitored over asimilar time course (see Figure 16).
Hence, based on objective measurements and sta-tistical analyses, the above two investigations clearlydemonstrated deficient dynamic fusional vergenceoculomotor parameters in patients with symptomaticconvergence dysfunction, considerable vergence ocu-lomotor plasticity, and relatively long-term retentionof the fusional vergence therapeutic effects, along withcorrelated reduction of symptoms.
Other studiesAnother model-based fusional vergence parameteris “vergence adaptation”79 (see Figures 4 and 5).It is believed to be critical for a range of vergencefunctions,79 (e.g., maintaining a stable phoria posi-
754
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
The tracking rate of vergence-deficient subjects as a function of weeks of training andpost-training monitoring. All subjects initially showed slow tracking rates that increasedto maximum levels in 2 to 8 weeks of orthoptics therapy. All subjects, except for RM,maintained their maximum tracking rate over the post-therapy period of monitoring. The bar ( | ) indicates the measurement standard error (reprinted with permission fromGrisham et al., 1991).
Figure 15
ISSUE HIGHLIGHT
tion80 in the presence of changes in disparity stim-ulation, fatigue effects, illness, etc.). Such changesmay occur either transiently or over more-sustained periods of time, such as during pro-longed nearwork. Using oculomotor model-driveninvestigations that incorporated psychophysicaltest procedures, North and Henson81 found thatvergence adaptation discriminated well betweensymptomatic and asymptomatic patients whomanifested nonstrabismic vergence dysfunc-tions. In a later study, they—like Grisham et al.77,78—assessed vision therapy-related plas-ticity of this specific oculomotor component.82,83
Seven young adult patients with symptomatic con-vergence insufficiency and abnormal vergence
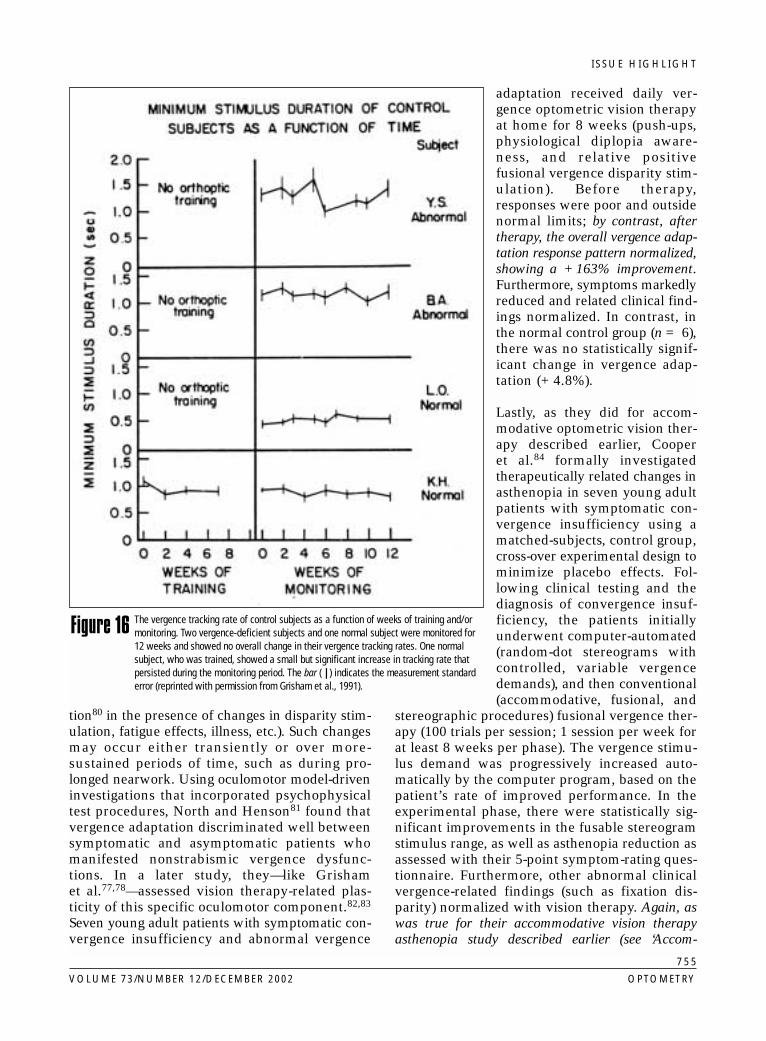
adaptation received daily ver-gence optometric vision therapyat home for 8 weeks (push-ups,physiological diplopia aware-ness, and relative positivefusional vergence disparity stim-ulation). Before therapy,responses were poor and outsidenormal limits; by contrast, aftertherapy, the overall vergence adap-tation response pattern normalized,showing a +163% improvement.Furthermore, symptoms markedlyreduced and related clinical find-ings normalized. In contrast, inthe normal control group (n = 6),there was no statistically signif-icant change in vergence adap-tation (+4.8%).
Lastly, as they did for accom-modative optometric vision ther-apy described earlier, Cooper et al.84 formally investigatedtherapeutically related changes inasthenopia in seven young adultpatients with symptomatic con-vergence insufficiency using amatched-subjects, control group,cross-over experimental design tominimize placebo effects. Fol-lowing clinical testing and thediagnosis of convergence insuf-ficiency, the patients initiallyunderwent computer-automated(random-dot stereograms withcontrolled, variable vergencedemands), and then conventional(accommodative, fusional, and
stereographic procedures) fusional vergence ther-apy (100 trials per session; 1 session per week forat least 8 weeks per phase). The vergence stimu-lus demand was progressively increased auto-matically by the computer program, based on thepatient’s rate of improved performance. In theexperimental phase, there were statistically sig-nificant improvements in the fusable stereogramstimulus range, as well as asthenopia reduction asassessed with their 5-point symptom-rating ques-tionnaire. Furthermore, other abnormal clinicalvergence-related findings (such as fixation dis-parity) normalized with vision therapy. Again, aswas true for their accommodative vision therapyasthenopia study described earlier (see ‘Accom-
755
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
The vergence tracking rate of control subjects as a function of weeks of training and/ormonitoring. Two vergence-deficient subjects and one normal subject were monitored for12 weeks and showed no overall change in their vergence tracking rates. One normalsubject, who was trained, showed a small but significant increase in tracking rate thatpersisted during the monitoring period. The bar ( | ) indicates the measurement standarderror (reprinted with permission from Grisham et al., 1991).
Figure 16

ISSUE HIGHLIGHT
modative Therapy’ section), attain-ing statistically significant changeswith such a relatively small samplesize attests to the robustness of thefusional vergence therapeutic par-adigm.
In summary, the findings clearlydemonstrate the scientific effi-cacy of fusional vergence visiontherapy. This is reflected in theobjective measures of fusionalvergence, formal quantitativeand informal symptom surveys,and standard clinical optomet-ric/ophthalmological test find-ings. The results are inagreement with a constellation of clinical casereports and case series, as well as retrospectiveand prospective clinical studies, in the optomet-ric, ophthalmologic, and orthoptic literatures overthe past several decades demonstrating modifi-ability (i.e., neuroplasticity) and normalization ofvergence responsivity, subsequent to relativelyshort durations of fusional vergence vision ther-apy.26,32-36
DiscussionIn this article, selected literature has been reviewedthat provides supportive evidence of the scientificbasis for and efficacy of optometric vision therapyin the areas of nonstrabismic accommodative andvergence disorders. The supporting evidence is man-ifold, including objective physiological measures,symptom rating-scale questionnaire confirmation,statistical verification, oculomotor model-based bio-engineering quantitative approaches, cross-overexperimental designs in clinical studies, and corre-lated and positive clinical test findings. Furthermore,when the above information is combined with thenumerous case reports/case studies, and retro-spective/prospective investigations summarizedand reviewed in the optometric, ophthalmologic, andorthoptic literatures,26,32-36 and if one adopts a moreglobal meta-analysis approach,85 the evidence in sup-port of optometric vision therapy in patients whomanifest symptomatic, nonstrabismic vergence andaccommodative disorders is even stronger.
How models of the accommodative and vergence systems can be helpful to the clinicianNumerous examples of how these models havebeen used to provide new insights regarding diag-
nostic aspects of static and dynamic accom-modative and vergence oculomotor anomalies andtheir specific abnormal model-based subcompo-nents, as well as the effectiveness of specific ther-apeutic subcomponent targeting, have beenenumerated and detailed.
Let us reinforce this notion using a specific caseexample. Suppose an adolescent patient exhibitsreduced (by 1 D) steady-state accommodation atnear under binocular viewing conditions asassessed by dynamic retinoscopy.73 Several pos-sible individual static model components may beinvolved (see Figures 3, 4, and 5), such as thedepth-of-focus, accommodative controller gain,adaptive gain, tonic accommodation, proximalaccommodation, and convergence accommoda-tion. First, the magnitude of vergence accom-modation is typically relatively minor, as most ofa system’s response output is derived from thespecific stimulus drive (i.e., blur) within its ownnegative feedback control loop. Second, under nor-mal binocular viewing conditions—with both theaccommodative and vergence negative feedbackcontrol loops in their closed-loop mode, such thatblur and disparity information, respectively, areeffective—the proximal and tonic terms are neg-ligible, especially at near. Third, since one is notdealing with sustained (i.e., minutes) accommo-dation at near, the adaptive loop would not beactivated. Thus, one is left with two components;namely, depth-of-focus and accommodative con-troller gain. It can be difficult to disentangle theirindividual component effects on steady-stateaccommodation, as their typical abnormaldynamic accommodative retinoscopy responsewould independently result in reduced static
756
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
Table 2. Neurophysiological analogs of static and dynamic model components of accommodation and vergence
Model component Probable neural sites
Depth-of-focus (DF) Areas V1, V2 visual cortex(sensory; contrast detectors)
Panum’s fusional areas (PFA) Areas V1, V2 visual cortex(sensory; disparity detectors)
Controller gain (ACG; VCG) Midbrain(motor near response cells)
Crosslink gain (AC; CA) Midbrain
Adaptive gain (ADAPT) Cerebellum;neuroreceptors of ciliary body
Tonic innervation (TA; TV) Midbrain

ISSUE HIGHLIGHT
accommodative levels. Assuming a high state ofattention and motivation during the diagnostictesting—and in the absence of more-severe ocu-lar conditions such as amblyopia and nystagmus—the anticipated increased amount ofdepth-of-focus might only be 0.25 D or so, whichis considerably less than the 1.0 D lag of accom-modation uncovered at near clinically. Hence, theaccommodative controller gain component wouldbe responsible for contributing the residualamount. Thus, vision therapy would incorporateblur discrimination techniques (e.g., sequentiallens sorting55) to sensitize and normalize the neu-rosensory aspects of the depth-of-focus. How-ever—and perhaps even more importantly—monocular and binocular lens flipper therapyusing slightly-above-threshold visual acuity lettertargets (or perhaps low-contrast gratings) wouldalso be used to force more-accurate accommo-dation (and thus larger response amplitudes),which translates into normalization of theaccommodative controller gain parameter. Whileadditional therapeutic procedures would still beused, only specific ones would be emphasized,perhaps with various degrees of “weighting.” Suchmodel-based clinical logic and specific componenttherapeutic targeting may result in even-better finaloutcomes.
Homeomorphic nature of the modelsAs mentioned at the beginning of the model sec-tion, a good model should have neuroanatomicand neurophysiologic under-pinnings. Thus, itshould be homeomorphic in nature. At this time,some of this information is not fully understood.With recent advances in brain-imaging technol-ogy, however, answers to these critical questionsshould be forthcoming. Within these constraints,an attempt has been made to relate the static anddynamic model components to possible sensoryand motor neural sites of involvement (see Table2). However, additional brain areas are probablyinvolved in dissemination of this information ina more-complex and comprehensive neural net-work.51,61,62
A primary thrust of this article has been on thosestudies that have used objective measures ofaccommodative and vergence responsivity beforeand after therapy, as well as in some cases dur-ing specific therapeutic phases. In the future, anadditional and important objective measure shouldinclude neural imaging: first, to document the affectedsite and its cerebral pervasiveness and second, to
assess directly the neurological therapeutic changesand effectiveness.
Motor learning and motor planningMotor learning (i.e., perceptual-motor skill acqui-sition) involves describing and explaining changesin motor performance and motor control thatoccur with specific practice paradigms.19 Acquir-ing new (or altering old) motor skills takes placein three well-defined phases.
1. Verbal-cognitive phase: This primarilyinvolves conscious thinking and planning ofmovement strategies; hence, one eitherlearns new movement patterns, or reshapesold ones, via a trial-and-error approach. Ini-tial performance varies considerably as arange of movement strategies is attempted,with most being discarded in favor of themost-effective and efficient one.
2. Associative phase: This single, new movementpattern is practiced repeatedly and “fine-tuned.” When the movement pattern islearned reasonably well, increases in task com-plexity and changes in prevailing conditions areinstituted to ensure task success and system-atic continuation of motor skill development.
3. Autonomous phase: The highly practicedmovement pattern, or motor skill, hasbecome automatic and below the level ofconsciousness. Motor performance is con-sistent, precise, efficient, “time-optimal,” andaccurate. Hence, the motor pattern becomes“pre-programmed” and, in essence, “open-loop” (i.e., without the need to consciouslymonitor its feedback). This is in contrast tothe earlier two phases, in which feedback isessential and continuously monitored (i.e.,closed-loop) to improve motor performance.
The above description of motor skill acquisitionmust be learned for each new motor skill. Thereis relatively little transfer. Thus, if this basic tenetof motor learning is related specifically to optomet-ric vision therapy for nonstrabismic accommodativeand vergence disorders, it provides justification fortraining of a series of oculomotor learning skillsencompassing a wide range of stimuli and test con-ditions to ensure development of the full complementof motor skills that can then be used in one’s every-day environment.
These principles of motor learning can be con-ceptualized mechanistically in a global manner (asshown in Figure 17, which presents the classical
757
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY

ISSUE HIGHLIGHT
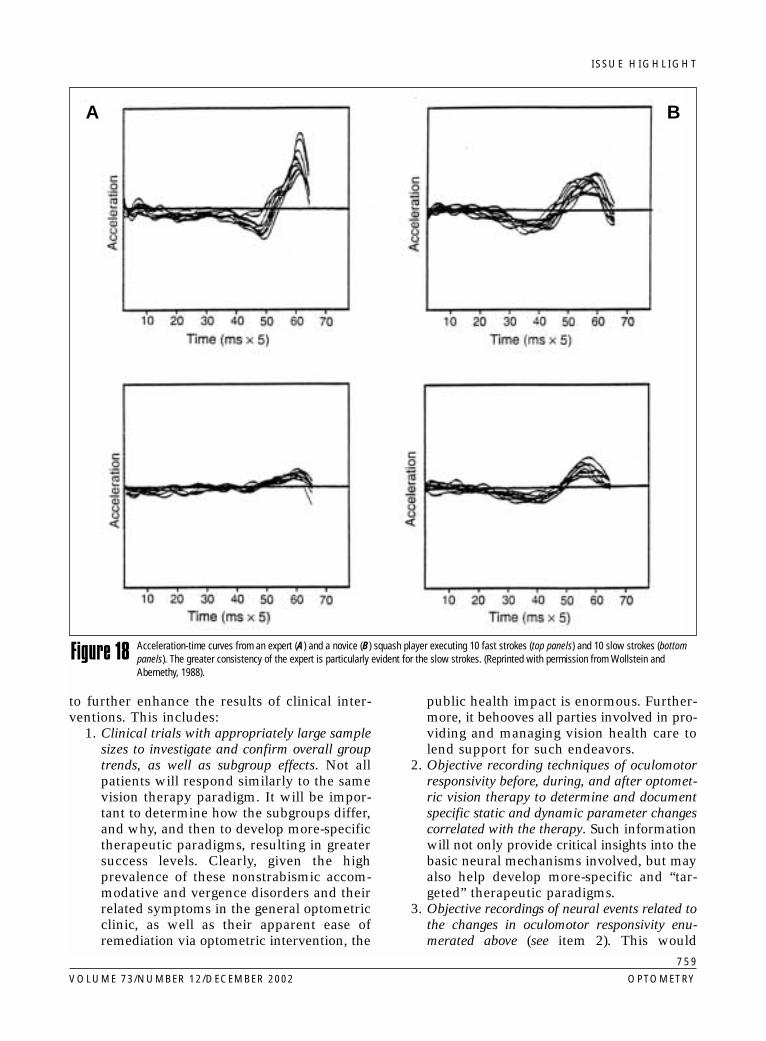
psychology “stimulus-response” paradigm).86 Itcan be further appreciated in the dynamic motorresponse patterns (response acceleration as a func-tion of time) comparing a novice versus expertsquash player (see Figure 18).87 What is referredto as greater “consistency” for the expert playercan be translated into the more-general neuro-logical principle of neural signal “synchroniza-tion.”19,88-90 With appropriate practice andrepetition, there is more synchronous firing in thegroup of motor neurons controlling the musclesinvolved in a specific movement. Greater massneuronal synchrony translates into greater motorresponse consistency and time optimality.67
Clearly, this idea can be transferred to optomet-ric vision therapy for nonstrabismic accom-modative and vergence disorders. One would usemonocular lens flipper techniques, whereinonly monocular accommodative neural control isconditioned and shaped, then fusional vergencein isolation using prism flippers and a blur-freeDOG (difference of Gaussians) stimulus,60,61 fol-lowed by a similar process involving binocularinteractive closed-loop aspects of the accom-modative and vergence systems in the dynamicfree-space environment. Thus, in such therapy, syn-chronization of motor neurons within each systemwould first be conditioned, followed by synchro-nization of motor neurons between each system.
Lastly, one can proceed to the synaptic and molec-ular level of motor learning. This was first enun-ciated by Hebb in 194991 within the context of his
now-classic notion of “cell assemblies,” the pred-ecessor to contemporary “neural networks.”92 Hestated, “...when an axon of Cell A is near enoughto Cell B and repeatedly or persistently takes partin firing it, some growth processes or metabolicchanges take place in one or both cells such thatA’s efficiency, as one of the cells firing B, isincreased.” Hence, by repetition, patterns of neu-ral activation of specific neurons and their inter-connections are enhanced, whereas those withoutsuch correlated patterns of activity are weakened.This neural enhancement, in effect, produces rel-atively long-term neural “potentiation,” such thata certain level of neural activation now producesincreased cell responsivity, which suggests theefficiency of synapses has been enhanced via therepetitive motor learning process. Currentresearch is focused on determining which neu-roreceptor is involved in such learning, with theN-methyl-D-asparate (NMDA) receptor appearingto be a likely candidate.92 Clearly, such synapticplasticity and conditioning could account for themotor improvements found during the course of opto-metric vision therapy for nonstrabismic accom-modative and vergence disorders.
Future directionsWhile there is considerable evidence for the sci-entific basis and efficacy of optometric visiontherapy, as in any clinical discipline, moreresearch and advances are welcome to understandthe basic mechanisms more comprehensively, and
758
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
Schematic view of the different types of learning examined by neurophysiologists (Reprinted with permission from Carlson, 1994).Figure 17
ISSUE HIGHLIGHT
to further enhance the results of clinical inter-ventions. This includes:
1. Clinical trials with appropriately large samplesizes to investigate and confirm overall grouptrends, as well as subgroup effects. Not allpatients will respond similarly to the samevision therapy paradigm. It will be impor-tant to determine how the subgroups differ,and why, and then to develop more-specifictherapeutic paradigms, resulting in greatersuccess levels. Clearly, given the highprevalence of these nonstrabismic accom-modative and vergence disorders and theirrelated symptoms in the general optometricclinic, as well as their apparent ease ofremediation via optometric intervention, the
public health impact is enormous. Further-more, it behooves all parties involved in pro-viding and managing vision health care tolend support for such endeavors.
2. Objective recording techniques of oculomotorresponsivity before, during, and after optomet-ric vision therapy to determine and documentspecific static and dynamic parameter changescorrelated with the therapy. Such informationwill not only provide critical insights into thebasic neural mechanisms involved, but mayalso help develop more-specific and “tar-geted” therapeutic paradigms.
3. Objective recordings of neural events related tothe changes in oculomotor responsivity enu-merated above (see item 2). This would
759
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
Acceleration-time curves from an expert (A) and a novice (B) squash player executing 10 fast strokes (top panels) and 10 slow strokes (bottompanels). The greater consistency of the expert is particularly evident for the slow strokes. (Reprinted with permission from Wollstein andAbernethy, 1988).
Figure 18
A B

ISSUE HIGHLIGHT
include functional MRI,93 magnetoen-cephalography (MEG),67 and positron emis-sion tomography (PET)94,95 non-invasivebrain-imaging techniques to localize the basicneural sites involved in the clinical abnor-mality, as well as those that contribute to theoculomotor therapeutic changes reflectingoculomotor learning and plasticity.
4. Investigations into the synaptic and molecularbasis of vision therapy and cortical plastic-ity,86,92,96,97 as pioneered by the classic Heb-bian notion.91
5. Development of new instrumentation andclinical procedures to assess oculomotor per-formance in infants and very young childrenwho are “at risk” for development of a binoc-ular vision disorder.
6. Further development of computerized technol-ogy to standardize training procedures, as wellas to provide more controlled home therapy.98,99
7. Expansion of the oculomotor models to incor-porate such important aspects as attention andproprioception, as well as visual stress-relatedcomponents and correlated neuropharmaco-logical mechanisms.36
AcknowledgmentsThis document was funded in part by a grant from the Mountain States Congressof Optometry, in association with the American Optometric Association.I wish to thank Drs. Jeffrey Cooper, Sue Cotter, Esther Han, George Hung, NeeraKapoor, Leonard Press, Michael Rouse, Mitchell Scheiman, Irwin Suchoff, BarryTannen, and Gary Williams for their helpful and insightful discussions and com-ments.
References1. Griffin JR, Grisham JD. Binocular anomalies, 3rd ed.
Boston: Butterworth–Heinemann, 1995.2. Rutstein RP, Daum KM. Anomalies of binocular vision: diag-
nosis and management. St. Louis: Mosby, 1998.3. Press LJ, ed. Applied concepts in vision therapy. St. Louis:
Mosby, 1997.4. Cornell E, Mitchell R. An evaluation of proximal con-
vergence by the use of infra-red photography. AustOrthopt J 1979-1980;17:24-9.
5. Ciuffreda KJ, Goldrich SG. Oculomotor biofeedback ther-apy. Int Rehab Med 1983;5:111-7.
6. Scheiman MM, Peli E, Libassi D. Auditory biofeedbackused to enhance convergence insufficiency. J AMOPTOM ASSOC 1983;54:1001-3.
7. Groffman S. Operant conditioning and vision training.Am J Optom Arch Am Acad Optom 1969;46:583-94.
8. Letourneau JE. Application of biofeedback and behaviormodification technique in visual training. Am J OptomPhysiol Optics 1976;53:187-90.
9. Feldman J. Behavior modification in vision training: facil-itating prerequisite behaviors and skills. J AM OPTOMASSOC 1981;52:329-40.
10. Malmstrom FV, Randle RJ. Effects of visual imagery onthe accommodative response. Percept Psychophys 1976;19:450-3.
11. Forrest EB. Visual imagery: an optometric approach. Dun-can, Okla.: OEP Foundation, 1981.
12. Richman JE. The influence of visual attention and auto-maticity on the diagnosis and treatment of clinical oculo-motor, accommodative, and vergence dysfunctions. J Optom Vis Dev 1999;30:132-41.
13. Lie I, Watten R, Fostervold KI. Accommodation/ver-gence/fixation disparity and synergism of head, neck andshoulders. In: Franzen O, Richter H, Stark L, eds. Accom-modation and vergence mechanisms in the visual system.Basel, Switzerland: Birkhauser Verlag, 2000:303-12.
14. Han Y, Lennerstrand G. Effect of neck muscle proprio-ceptive activation on the dynamics of monocularly-drivenhorizontal vergence movements. Acta Ophthalmol Scand1998;76:283-8.
15. Servos P, Goodale MA, Jakobson LS. The role of binoc-ular vision in prehension: a kinematic analysis. Vision Res1992;32:1513-21.
16. Howard IP, Templeton WB. Human spatial orientation.London: Wiley and Sons, 1966.
17. Suchoff IB. Visual-spatial development in the child: an opto-metric theoretical and clinical approach. New York:SUNY/State College of Optometry, 1974.
18. Kelso JAS, ed. Human motor behavior. Hillsdale, N.J.:Lawrence Erlbaum Assoc. Pub., 1982.
19. Abernathy B, Kipper V, Mackinnon LT, et al. The bio-physical foundations of human movement. Champaign, Ill.:Human Kinetics Pub., 1997:269-352.
20. Kephart NC. The slow learner in the classroom. Columbus,Ohio: C.E. Merrill Books, 1960.
21. Classé JG, Rutstein RP. Binocular vision anomalies: anemerging cause of malpractice claims. J AM OPTOMASSOC 1995;66:305-9.
22. Hokoda SC. General binocular dysfunction in an urbanoptometry clinic. J AM OPTOM ASSOC 1985;56:560-2.
23. Hoffman L, Cohen AH, Feuer G. Effectiveness of opto-metric vision therapy/orthoptics in a private practice. AmJ Optom Arch Am Acad Optom 1973;50:813-6.
24. Cooper J, Duckman R. Convergence insufficiency; inci-dence, diagnosis, and treatment. J AM OPTOM ASSOC1978;49:673-80.
25. Scheiman M, Gallaway M, Goutler M, et al. Prevalenceof vision and ocular disease conditions in a clinical pedi-atric practice. J AM OPTOM ASSOC 1996;67:193-202.
26. American Optometric Association Concensus Panelwith Accommodative and Vergence Dysfunction. Care ofthe Patient with Accommodative and Vergence Dys-function. Optometric Clinical Practice Guidelines. St.Louis: AOA, 1998.
27. Scheiman MM, Wick B. Clinical management of binocu-lar vision: heterophoric, accommodative, and eye movementdisorders. Philadelphia: JB Lippincott, 1994.
28. Amos JF, Rutstein RP. Vertical deviations. In: Amos JF,ed. Diagnosis and management of vision care. Boston: But-terworth, 1987:515-83.
29. Skeffington AM. Procedure in ocular examination. Chicago:AJ Fox Co., 1928.
30. Peckham RH. The modern treatment of binocular imbalance.New York: Shur-On Standard Optical, 1928.
31. Duane A. Anomalies of the accommodation, consideredclinically. Trans Am Ophthalmol Soc 1915;14:386-402.
760
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002
ISSUE HIGHLIGHT
32. American Optometric Association. Position statement onvision therapy. J AM OPTOM ASSOC 1985;56:782-3.
33. The 1986/87 Future of Visual Development/PerformanceTask Force. The efficacy of optometric vision therapy. J AM OPTOM ASSOC 1988;59:95-105.
34. Joint Organizational Policy Statement of the American Acad-emy of Optometry and the American Optometric Associ-ation. Vision therapy. J Behav Optom 1999;10:109-10.
35. Suchoff IB, Petito GT. The efficacy of visual therapy:accommodative disorders and nonstrabismic anomalies ofbinocular vision. J AM OPTOM ASSOC 1986;57:119-25.
36. Birnbaum MH. Optometric management of nearpoint visiondisorders. Boston: Butterworth–Heinemann, 1993:381-93.
37. Westheimer G. Amphetamine, barbiturates, and accom-modative vergence. Arch Ophthalmol 1963;70:830-6.
38. Toates FM. Accommodation and convergence in thehuman eye. Measurement and Control 1969;3:29-33.
39. Stark L. Neurological control systems. New York: PlenumPress, 1968.
40. Saladin JJ. Interpretation of divergent oculomotorimbalance through control systems analysis. Am J OptomPhysiol Optics 1988;65:439-47.
41. Jiang BC. A modified control model for steady-stateaccommodation. In: Franzen O, Richter H, Stark L, eds.Accommodative and vergence mechanisms in the visual sys-tem. Basel, Switzerland: Birkhauser Verlag, 2000:235-43.
42. Krishnan VV, Stark L. A heuristic model of the humanvergence eye movement system. IEEE Trans Biomed Engn1977;24:44-9.
43. Krishnan VV, Stark L. Integral control in accommodation.Comp Prog Biomed 1975;4:237-45.
44. Hung GK, Ciuffreda KJ, Semmlow JL. Static vergence andaccommodation: population norms and orthoptics effect.Doc Ophthalmol 1986;62:165-79.
45. Hung GK, Semmlow JL, Ciuffreda KJ. A dual-modedynamic model of the vergence eye movement system.IEEE Trans Biomed Engn 1986;33:1021-8.
46. Hung GK, Semmlow JL. Static behavior of accommo-dation and vergence: computer simulation of an inter-active dual feedback system. IEEE Trans Biomed Engn1980;27:439-47.
47. Hung GK, Ciuffreda KJ, Rosenfield M. Proximal contri-bution to a linear static model of accommodation andvergence. Ophthalmic Physiol Opt 1996;16:31-41.
48. Hung GK, Ciuffreda KJ. Dual-mode behavior in thehuman accommodation system. Ophthalmic Physiol Opt1988;8:327-32.
49. Hung GK, Ciuffreda KJ. Sensitivity analysis of relativeaccommodation and vergence. IEEE Trans Biomed Engn1994;41:241-8.
50. Schor C, Horner D. Adaptation disorders of accommo-dation and vergence in binocular dysfunction. OphthalmicPhysiol Opt 1989;9:264-8.
51. Schor C, Ciuffreda KJ, eds. Vergence eye movements: basicand clinical aspects. Boston: Butterworth, 1983.
52. Schor CM. The relationship between fusional vergenceeye movements and fixation disparity. Vision Res 1979;19:1359-67.
53. Hung GK, Ciuffreda KJ. Adaptation model of nearwork-induced transient myopia. Ophthalmic Physiol Opt 1999;19:151-8.
54. Hung GK, Ciuffreda KJ, Semmlow JL, et al. Model ofstatic accommodative behavior in human amblyopia.IEEE Trans Biomed Engn 1983;30:665-72.
55. Ciuffreda KJ, Levi D, Selenow A. Amblyopia: basic andclinical aspects. Boston: Butterworth, 1991.
56. Ciuffreda KJ, Hokoda SC, Hung GK, et al. Accom-modative stimulus/response function in human ambly-opia. Doc Ophthalmol 1984;56:303-26.
57. Ong E, Ciuffreda KJ, Tannen B. Static accommodation incongenital nystagmus. Invest Ophthal Vis Sci 1993;34:194-204.
58. Hung GK, Ciuffreda KJ. A unifying theory of refractiveerror development. Bull Math Biol 2000;62:1087-108.
59. Ong EO, Ciuffreda KJ. Accommodation, nearwork, andmyopia. Santa Ana, Calif.: OEP Foundation Press, 1997.
60. Ciuffreda KJ. Accommodation and its anomalies. In: Char-man WN, ed. Vision and visual dysfunction: visual opticsand instrumentation. New York: MacMillan, 1991:231-79.
61. Ciuffreda KJ. Accommodation, the pupil, and presbyopia.In: Benjamin WJ, ed. Borish’s clinical refraction. Philadel-phia: WB Saunders Co., 1998:77-120.
62. Ciuffreda KJ, Ordonez X. Vision therapy to reduce abnor-mal nearwork-induced transient myopia. Optom Vis Sci1998;75:311-5.
63. Mays LE, Gamlin PDR. Neuronal circuits for accom-modation and vergence in the primate. In: Franzen O,Richter H, Stark L, eds. Accommodation and vergence mech-anisms in the visual system. Basel, Switzerland: BirkhauserVerlag, 2000:1-9.
64. Bogart TF Jr. Laplace transforms and control systems the-ory and technology. New York: John Wiley and Sons,1982:73-4.
65. Liu JS, Lee M, Jang J, et al. Objective assessment ofaccommodation orthoptics: dynamic insufficiency. Am JOptom Physiol Optics 1979;56:285-94.
66. Gottlieb GL, Corcos DM, Jarie S, et al. Practiceimproves even the simplest movements. Exp Brain Res1988;73:436-40.
67. Takeda T, Endo H, Hashimoto K. Research on dynamicaccommodation using TDO III (three dimensionaloptometer III) and MEG (magneticoencephalography). In:Franzen O, Richter H, Stark L, eds. Accommodative andvergence mechanisms in the visual system. Basel, Switzer-land: Birkhauser Verlag, 2000:51-66.
68. Mah MM, Pope RS, Wong JH. Testing of accommodationfacility in school age children. University of California(Berkeley): School of Optometry, O.D. thesis, 1981.
69. Liu J, Lee M, Jang J. An objective assessment of accom-modation orthoptics. University of California (Berkeley):School of Optometry, O.D. thesis, 1978.
70. Bobier WR, Sivak JG. Orthoptic treatment of subjectsshowing slow accommodative response. Am J Optom Phys-iol Optics 1983;60:678-87.
71. Rosenfield M, Gilmartin B. Temporal aspects of accom-modative adaptation. Optom Vis Sci 1989;66:229-34.
72. Lovasik JV, Wiggins R. Cortical indices of impaired ocu-lar accommodation and associated convergence mecha-nisms. Am J Optom Physiol Optics 1984;61:150-9.
73. Benjamin WJ, ed. Borish’s clinical refraction. Philadelphia,WB Saunders Co., 1998.
74. Cooper J, Feldman J, Selenow A, et al. Reduction ofasthenopia after accommodative facility training. Am JOptom Physiol Opt 1987;64:430-6.
75. Sterner B, Abrahamsson M, Anders S. Accommodativefacility training with a long-term followup in a sampleof school-aged children showing accommodative dys-function. Doc Ophthalmol 1999;99:93-101.
761
VOLUME 73/NUMBER 12/DECEMBER 2002 OPTOMETRY
ISSUE HIGHLIGHT
76. Grisham JD. Visual therapy results for convergence insuf-ficiency: a literature review. Am J Optom Physiol Optics1988;65:448-54.
77. Grisham JD. The dynamics of fusional vergence eyemovements in binocular dysfunction. Am J Optom Phys-iol Optics 1980;57:645-55.
78. Grisham JD, Bowman MC, Owyang LA, et al. Vergenceorthoptics: validity and persistence of the training effect.Optom Vis Sci 1991;68:441-51.
79. Cooper J. Clinical implications of vergence adaptation.Optom Vis Sci 1992;69:300-7.
80. McCormack GL. Vergence adaptation maintains het-erophoria in normal binocular vision. Am J Optom Phys-iol Opt 1985;62:555-61.
81. North R, Henson DB. Adaptation to prism-induced het-erophoria in subjects with abnormal binocular vision orasthenopia. Am J Optom Physiol Opt 1981;58:746-52.
82. North R, Henson DB. The effect of orthoptic treatmentupon the ability of patients to adapt to prism-induced het-erophoria. Am J Optom Physiol Opt 1982;59:983-6.
83. North R, Henson DB. The effect of orthoptic treatmentupon the vergence adaptation mechanism. Optom Vis Sci1992;69:294-9.
84. Cooper J, Selenow A, Ciuffreda KJ, et al. Reduction ofasthenopia in patients with convergence insufficiencyafter fusional vergence training. Am J Optom Physiol Opt1983;60:982-9.
85. Glass GV. Primary, secondary, and meta-analysis ofresearch. Educational Researcher 1976;5:3-8.
86. Carlson NR. Physiology of behavior. Boston: Allyn andBacon Inc., 1997:576-608.
87. Wollstein JJ, Abernethy B. Timing structure in squashstrokes: further evidence for the operational timinghypothesis. J Hum Mov Studies 1988;15:70-1.
88. Smith KU, Schmidt J, Putz V. Binocular coordination:feedback synchronization of eye movements for spaceperception. Am J Optom Arch Am Acad Optom 1970;47:679-89.
89. Singer W. Synchronization of cortical activity and its puta-tive role in information processing and learning. Ann RevPhysiol 1993;55:349-74.
90. Singer W. Time as coding in neocortical processing. In:Buzsaki G, Llinas R, Singer W, et al., eds. Temporal cod-ing in the brain. Berlin: Springer Verlag, 1994:51-79.
91. Hebb DO. The organization of behavior. New York: JohnWiley and Sons Inc., 1949.
92. Rauschecker JP. Mechanisms of visual plasticity: Hebbsynapses, NMDA receptors, and beyond. Physiol Rev1991;71:587-615.
93. Ellermann JM, Siegal JD, Strupp JP, et al. Activation ofvisuomotor systems during visually-guided movements:a functional MRI study. J Magn Reson 1998;131:272-85.
94. Richter H, Lee JT, Pardo JV. Neuroanatomical correlatesof the near response: voluntary modulation of accom-modation in the human visual system. In: Franzen O,Richter H, Stark L, eds. Accommodative and vergence mech-anisms in the visual system. Basel, Switzerland: BirkhauserVerlag, 2000:67-78.
95. Pardo JV, Sponheim SR, Costellow P, et al. Functional neu-roanatomy of the human near/far response of the visualsystem to blur cues: fixation to point targets at differentviewing distances. In: Franzen O, Richter H, Stark L, eds.Accommodative and vergence mechanisms in the visual sys-tem. Basel, Switzerland: Birkhauser Verlag, 2000:79-90.
96. Daw NW. Visual development. New York, Plenum Press1995:155-92.
97. Windhorst U. Specific networks of the cerebral cortex:functional organization and plasticity. In: Greger R,Windhorst U, eds. Comprehensive human physiology, Vol.1. Berlin: Springer-Verlag, 1996:1105-36.
98. Cooper J. Review of computerized orthoptics with spe-cific regard to convergence insufficiency. Am J OptomPhysiol Opt 1988:65:455-63.
99. Cooper J. Diagnosis and treatment of accommodative andvergence anomalies using computerized vision therapy.Practical Optometry 1998;9(1):6-11.
Corresponding author:
Kenneth J. Ciuffreda, O.D., Ph.D.State University of New York
State College of Optometry33 West 42nd Street
New York, New York 10036
762
OPTOMETRY VOLUME 73/NUMBER 12/DECEMBER 2002