the psychological costs and benefits of being highly persistent: personality profiles distinguish...
TRANSCRIPT

Journal of Affective Disorders 136 (2012) 758–766
Contents lists available at SciVerse ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r .com/ locate / jad
Research report
The psychological costs and benefits of being highly persistent: Personalityprofiles distinguish mood disorders from anxiety disorders
C. Robert Cloninger a,⁎, Ada H. Zohar b, Schmuel Hirschmann c,d, Dana Dahan b,e
a Center for Well-Being, Department of Psychiatry, Washington University School of Medicine, St. Louis, MO, USAb Psychology, Ruppin Academic Center, Emek Hefer, Israelc Department of Psychiatry, Technion, Haifa, Israeld Shaarei Menashe Medical Center, Israele Ariel University Center, Israel
a r t i c l e i n f o
⁎ Corresponding author. Tel.: +1 314 362 7005; faE-mail address: [email protected] (C.R. Clo
0165-0327/$ – see front matter © 2011 Elsevier B.V. Adoi:10.1016/j.jad.2011.09.046
a b s t r a c t
Article history:Received 27 September 2011Accepted 30 September 2011Available online 28 October 2011
Background: The personality trait of Persistence is highly valued by conscientious overachievers,but it has both psychological costs and benefits. The interactions among multiple personalityfactors influencing the development of mood and anxiety disorders have been confounded inprior clinical samples, but can be disentangled in terms of their underlying brain circuitry andinfluence on perception of emotional stimuli.Methods: 285 individuals who represented the full range of personality variation in a largesample of adult volunteers from the general community of Israel were selected for follow-upby psychiatric interviews, cognitive testing, and medical examinations. The Temperament andCharacter Inventory (TCI) measured profiles of traits that distinguished individuals with diagno-ses of mood and/or anxiety disorders using linear discriminant analysis and non-linear profileanalysis.Results: High Harm Avoidance and low Self-directedness strongly distinguished people withmood and/or anxiety disorders from those with neither. High Persistence distinguished peoplewith only anxiety disorders from those with mood disorders. High Persistence was associatedwith greater health and happiness overall, but also led to more negative emotions than in peoplewith low Persistence unless they were both unusually tolerant of frustration (i.e., low in HarmAvoidance) and self-accepting of personal limitations (i.e. high in Self-directedness).Limitations: Subjects were volunteers over 40 years of age at assessment.Conclusions: People who are highly persistent (i.e., persevering, ambitious, perfectionistic) aremore likely to have anxiety disorders than mood disorders, even when they have other traitsincreasing risk for both (i.e., high Harm Avoidance and low Self-directedness). High Persistenceincreases both positive and negative emotions in most people. However, high Persistencereduces negative emotions and increases positive emotions if a person is easy-going (i.e.,“happy-go-lucky” when low in both Harm Avoidance and Self-directedness).
© 2011 Elsevier B.V. All rights reserved.
Keywords:PersonalityBrain mappingAffectAnxietyDepressionHappiness
1. Introduction
Persistence is a basic dimension of personality that ischaracterized by the extent to which a person will continueto expect and seek rewards even when the expected outcome
x: +1 314 362 5594.ninger).
ll rights reserved.
is only rarely successful (Cloninger et al., 1993). Persistence isa heritable trait (Gillespie et al., 2003; Heath et al., 1994) thathas been well-defined in terms of its underlying brain circuitryand its role in information processing of affective stimuli(Gusnard et al., 2003) as well as the resulting individual differ-ences in behavioral characteristics (Svrakic et al., 1993). Never-theless, the influence of Persistence on mood and affect hasbeen unclear. Some work has shown that high Persistence is

759C.R. Cloninger et al. / Journal of Affective Disorders 136 (2012) 758–766
associatedwith resilience and positive emotionality (Cloningeret al., 1998; Garcia, 2011) whereas other work has associated itwith compulsiveness and negative emotionality (Bulik et al.,2000; Fassino et al., 2004; Mulder et al., 1996).
People who are highly Persistent are described behavior-ally as determined, conscientious, and ambitious becausetheir enthusiasm and perseverance in hard work often leadsthem to becoming overachievers in academic and occupa-tional roles. On the other hand, highly Persistent peoplealso tend to be perfectionists who are dissatisfied with any-thing less than perfection, or at least feel they need to bethe best at whatever they try to do (Fleet and Hewitt,2002), as is common among physicians (Gabbard, 1985;Myers and Gabbard, 2008). Such unrelenting ambition andexaggerated positive expectations can easily lead to compul-sive self-doubt and excessively harsh judgments of oneselfand others. Substantial clinical work suggests perfectionismleads to a variety of personal and social problems related toanxiety, compulsivity, and depression (Beevers and Miller,2004; Fleet and Hewitt, 2002; Hamilton and Schweitzer,2000).
At the other extreme, individuals who are low in Persis-tence are described behaviorally as changeable, irresolute,and easily discouraged (Cloninger et al., 1993). As a result,they tend to be under-achievers when rewards are intermit-tent (that is, when efforts are not continuously reinforced).Nevertheless, people low in Persistence may be more suc-cessful than those who are highly Persistent when rewardcontingencies are rapidly changing over time because thehighly persistent people are overly influenced by past condi-tioning that is no longer predictive of current outcomes(Cloninger et al., 1994). Some work has suggested that lowPersistence is characteristic of people with bipolar mood disor-ders evenwhen they are rated in a euthymic state (Osher et al.,1996; Osher et al., 1999). However, other studies have notobserved this effect in either unipolar or bipolar patient sam-ples (Farmer et al., 2003; Nery et al., 2008; Nery et al., 2009).
In order to understand the complex pattern of interac-tions by which Persistence modulates affect and relatedgoal-directed behavior, it is crucial to understand the braincircuitry by which Persistence regulates the information pro-cessing of affective stimuli (Gusnard et al., 2003). Individualdifferences in TCI Persistence have been found to be stronglycorrelated (r=0.79, Pb0.01) in adult human volunteers withactivity in a specific brain circuit involving ventral striatum,the anterior cingulate cortex (ACC), and the orbital frontalcortex (Brodmann area 47) bilaterally (Gusnard et al.,2003). This specific brain circuit is well-known to regulatethe behavioral conditioning of reward-seeking behavior inother mammals (Robbins and Everitt, 1996; Schoenbaumand Setlow, 2001; Schultz et al., 2000, 2003). The regulationof this reward-seeking brain circuit was evaluated in humanvolunteers by having people make judgments about whethera standardized set of pictures from the International AffectivePicture System were pleasant, neutral, or unpleasant (Langet al., 1997). When making these ratings, individual's highin Persistence had increased activity throughout the circuit,whereas those low in Persistence had decreased activity.Furthermore, the differences in circuit activity between highPersistence and low Persistence subjects increased as theproportion of neutral pictures increased. In other words, as
the proportion of neutral pictures increased, the activity ofthe circuit increased further in highly persistent people anddecreased further in less persistent people, revealing a pat-tern characteristic of a non-linear dynamic system regulatingthe overall activity of this multi-nodal circuit.
However, the tendency of subjects to rate pictures aspleasant, neutral, or unpleasant was independent of the pro-portion of neutral pictures. Instead, the tendency of subjectsto rate pictures as pleasant depended on a complex interac-tion of three personality variables: Persistence (r=.34,Pb0.05), Self-directedness (r=0.50, Pb0.01), and HarmAvoidance (r=−0.44, Pb0.05) (Gusnard et al., 2003). Inother words, people who were high in Persistence, high inSelf-directedness, and low in Harm Avoidance made morepleasant judgments at the expense of neutral ratings. Weobserved no correlations between any TCI traits and theproportion of pictures rated as unpleasant, but our subjectswere healthy volunteers selected by excluding anyone witha history of psychiatric or neurological disorder. Theseexclusion criteria restricted the range of Harm Avoidanceand Self-directedness, but not Persistence (Gusnard et al.,2003). The ventral striatum is known to play a role in theguidance of behavior by regulating expectations of bothpleasant and unpleasant outcomes (Schoenbaum and Setlow,2001, 2003, 2005).
Other work has shown that Harm Avoidance influencesthe functional connectivity between the amygdala and ACCin response to anxiety-provoking stimuli (Pezawas et al.,2005), whereas Self-directedness is strongly related to theactivation of the medial prefrontal cortex (Brodmann areas8/9) when a person is consciously evaluating internal stimuli,such as whether a stimulus is felt to be pleasant, neutral, orunpleasant (Cloninger, 2004; Gusnard et al., 2001). Fear andother negative emotions reduce the ability of the prefrontalcortex to guide goal-directed behavior rationally by short-circuiting communication via the ACC (Pezawas et al.,2005). The ACC serves as a cross-road where conscious inten-tions interface with emotional drives to guide behavior basedon expectations of unpleasant or unpleasant outcomes (Paus,2001). In functional terms, TCI Persistence can be consideredto function as a modulator of the functional connectivity ofthe emotional brain (i.e., limbic system regulating the emo-tional drives measured by a person's temperament) and therational brain (i.e., prefrontal cortex regulating goals andvalues measured by a person's character) by holding incen-tive information in representational memory during delayperiods in the guidance of goal-directed behavior.
In order to evaluate the psychological advantages and dis-advantages associated with Persistence and its interactionswith Harm Avoidance and Self-directedness, we need toevaluate a sample representative of both the healthy and un-healthy extremes of a general community sample. A generalsample is needed to understand the complex interactionsamong multiple personality traits that regulate a person'swell-being across its full range from resilient health to disease.Such a study was undertaken in Israel, which is particularlyappropriate for the evaluation of the role of Persistence in themodulation of affect. Israel has a long cultural tradition ofencouraging achievement and persistent productivity understressful conditions (Brooks, 2010; Pease, 2009; Senor andSinger, 2009). Our study participants were highly diverse

760 C.R. Cloninger et al. / Journal of Affective Disorders 136 (2012) 758–766
adults and included representative numbers of active workersin highly successful businesses, farms, and professions as wellas individuals with clinically significant physical, emotional,and social disabilities (Cloninger and Zohar, 2011).
2. Methods
2.1. Participants
A base sample of 1102 adult volunteers in the community ofthe Sharon region of Israel completed a comprehensive self-report, which included extensivemeasures of personality, emo-tion, health and health behavior. The baseline sample and themeasures taken at initial participation are described in detailelsewhere (Cloninger and Zohar, 2011; Zohar and Cloninger,2011; Zohar et al., 2011). A mean 18 months later, a subset ofthe base sample, was invited to participate in the secondstudy phase (N=285). The phase-two-sample was selected torepresent the full range of personality traits measured in thebaseline sample. Out of those approached to participate inphase-two, 9.9% (30 out of 303) refused. The phase-two-sample included 142 women and 143 men. The mean age ofthe group was 56.5 years, ranging from 40 to 89. 70.1% weremarried, 18.2% divorced, 7.4% were widowed, and the remain-der single. They had a mean of 2.8 children, and a range ofeducation: 1.8% primary school, 16.5% high-school, 33.7% hadprofessional post-high-school training, and 31.2% were collegegraduates, 14.4% had MAs, and 2.1% Ph.D.s. The majority,83.7% defined themselves as non-religious Jews. The phase-two sample was no different from the base sample for any ofthe demographic variables described, nor were there any sig-nificant sex differences for these variables.
2.2. Participant review board
The research schedule was approved by Institutional EthicsCommittee, as well as by a regional Helsinki Medical ReviewBoard (permission number 42/2007), who reviewed andapproved the study annually over the four years until its com-pletion. Signed consent was requested at initial recruitment,and again for phase II of the study. Any additional procedure(e.g. audio-recording of the interview, reviewing medicalfiles) was preceded by an additional informed consent proce-dure. Privacy of the participants was rigorously protected.Participants were encouraged to discuss their concerns withthe research team and the PIs throughout and beyond thestudy period.
2.3. Phase-two measures
The structured clinical interview for DSM axis I disorders,text revised, non-patient version (SCID-I/NP) (First et al.,2002) was translated into Hebrew (with the permission ofthe authors), by translation, independent back-translation,and comparison with the original. The text was then line-edited for language and punctuation. Several formats werepiloted, until a user friendly, color tabbed version was pro-duced, which served as the diagnostic tool for the study. TheHebrew version of the SCID-I/NP is available to researchersupon request.
2.3.1. SCID-I/NP interviewsOver the duration of the study 6 interviewers were
employed. All interviewers were college graduates of abehavioral sciences program, and in addition, two were psy-chology graduate students. The interviewers were trained bysimulation interviews, in person and on-line, and then byinterviewing in pairs. Mean reliability between all pairs ofinterviewers was 0.89. The interviews were audio-recorded.The interview schedule was preceded by about half an hourof discussion, during which a life-story framework was eli-cited from the interviewee. The SCID-I/NP was then adminis-tered, and the life-story was used by the interviewer as areference for times of particular stress or crisis. The interviewprocess lasted between half an hour and 3 h, depending onthe amount of psychopathology reported. The interviewerthen wrote a brief summary of the life-story and psychiatricfindings and summarized the DSM axes I, III, IV and V diagno-ses on a suitable score sheet.
2.3.2. Best estimate diagnosis procedure (BEDP)The training of the interviewers, and the BEDP, was over-
seen by a board-certified senior psychiatrist, S.H. In caseswhere there were relevant medical files (hospital or outpa-tient) they were requested and compared to the SCID-I/NPresults. In all cases in which the SCID-I/NP results were lessthan certain, S.H. reviewed the SCID, referred to the audio-recording, and a BEDP meeting was held, attended by theinterviewer, S.H., and A.H.Z. (a senior clinical psychologist),C.R.C. participated in a BEDP meeting as an additional mea-sure of quality control. Diagnoses were scored as definite,probable, possible, or absent. Only definite life-time diagno-ses are reported in the subsequent results. Interviewersscored the SCID-I/NP for axis I diagnoses, as well as axis IIImedical conditions, axis IV socio-economic stressors, andaxis V general assessment of functioning (GAF). GAF wasscored in all interviews, even in the absence of axis I diagno-ses. Since this was a non-clinical sample, the general level offunctioning was high, and all those with GAF scores below 51(N=11) were combined with those between 51 and 60 toform a moderate or worse impairment category. The GAF wasfurther truncated to a 5-point Likert-like scale: superior func-tioning (5), satisfactory functioning with minimal symptoms(4), slightly impaired functioning with transient symptoms (3),mildly impaired functioning and symptoms (2), moderately im-paired functioning orworse symptoms (1). The truncated GAF isreferred to in the subsequent analyses as adaptive function.
Mean reliability between SCID interviewer and BEDP was0.91, when axis I diagnoses were present and 0.98 when theywere not. By diagnostic category agreement between SCIDinterviewer and BEDP were: 0.90 for mood disorders, 0.89for anxiety disorders, 0.73 for somatization disorders, 0.93for Eating Disorders, and 0.83 for all other diagnoses, includ-ing adjustment disorder.
2.3.3. Brief Symptom InventoryThe Brief Symptom Inventory (BSI) is a 53-item, empiri-
cally derived inventory of psychiatric symptoms and associ-ated distress (Derogatis, 1993). The Hebrew version waspreviously validated on a large community sample (Bacharet al., 1997). In the current study, the BSI global distressscale had an internal reliability estimate of α=0.93.

761C.R. Cloninger et al. / Journal of Affective Disorders 136 (2012) 758–766
2.3.4. Temperament and Character InventoryThe 140 Item Temperament and Character Inventory (TCI-
140; Zohar and Cloninger, 2011) includes 140 items whichare answered on a 5 point Likert-scale from definitely falseto definitely true. It measures four dimensions of tempera-ment (Novelty Seeking (NS), Harm Avoidance (HA), RewardDependence (RD), and Persistence (PS)) and three dimen-sions of character (Self-Directedness (SD), Cooperativeness(CO), and Self-Transcendence (ST)). There are 20 items foreach of the 7 dimensions except for Self-Transcendence,which has 16 allowing for the inclusion of 4 validity itemsto assess carelessness. The TCI-140 was translated intoHebrew for the current study by a process of translation,independent back translation and revision, and extensivelypiloted. The TCI-140 in Hebrew's scale reliability, structuralvalidity, as well as discriminant and convergent validityproved to be satisfactory (Zohar and Cloninger, 2011).
2.3.5. PANASThe positive and negative affect scale (PANAS) was used
for measuring affect (Watson et al., 1988). It includes 20items, half of which describe negative affective states andhalf positive, which are endorsed on a Likert-like scale. Ityields two subscales, one of negative affect and one of posi-tive affect. In the current study, scale reliability estimateswere α=0.79 and α=0.83 respectively. The sub-scalescores were transformed to standard distributions, with amean of 0 and a standard deviation of 1. Then the HI wascomputed as the difference between the positive and nega-tive affect scores. The HI is positively related to measures oflife satisfaction, social support, and emotional awareness(Cloninger and Zohar, 2011).
2.3.6. Social supportPerceived social support was measured with the multi-
dimensional perceived social support scale (MPSS) (Zimetet al., 1990). The MPSS has 12 items that relate to the per-ceived support given by friend, family, and intimate partner.It has been used extensively in Hebrew translation. Scalereliability in the current study was α=0.93.
2.3.7. AlexithymiaAlexithymia was measured using the Toronto Alexithymia
Scale-20 (TAS-20; Bagby, Parker, & Taylor, 1994). This 20item scale reduces to three subscales, Difficulty in IdentifyingAffect; Difficulty in Describing Affect, and External Attribu-tion of Affect. The TAS-20 was translated into Hebrew forthe current study by a process of translation, independentback translation, comparison and revision. Scale reliabilityfor the total TAS-20 was α=0.84, and for the three sub-scales α=0.83, 0.70 and 0.66 respectively.
2.3.8. Cognitive testingParticipants were evaluated on two tests of cognitive
function:
1. The Shipley Institute of Living Scale (SILS) (Shipley, 1940;Zachary, 1986). The SILS is composed of two timed sub-tests: the first is a multiple choice vocabulary test and thesecond an abstract reasoning (i.e., rule-inference comple-tion) test. The vocabulary sub-test is ameasure of crystallized
intelligence, while the rule-inference test measures fluidintelligence. The reasoning subtest score tends to declinearound middle age, while the vocabulary subtest is stable inadults (Mason et al., 1991). The SILS score is strongly corre-lated (i.e, 0.8–0.9) with the full scale WAIS-R score (Weissand Schell, 1991). The SILS was translated into Hebrew(Gilboa and Kave, 2007), taking into accountword frequencyin Hebrew as well as cultural considerations. The Hebrewversion has been found to discriminate between patientswith neurological deficits and normal controls (Gilboa,personal communication, 2010).
2. The California Verbal Learning Test II (Delis et al., 2000).The CVLT-II is a test of the ability to learn a list of words.It is individually administered by a trained tester andthen computer scored. It supplies information on manyaspects of verbal learning and memory processes, and issensitive to cognitive decline due to normal aging as wellas brain injury or illness. The CVLT-II was translated intoHebrew (Gilboa and Kave, 2008) and is in clinical use inneuropsychological assessment of normal aging, mild cog-nitive impairment, brain injury and illness.
2.3.9. AttachmentAdult attachment was assessed by a standardized self-
report (Hazan and Shaver, 1987), which includes 15 items,5 for each attachment style, and a 16th forced choice itemin which the respondent has to choose one of three descrip-tions of the three attachment styles. In the current study,the secure subscale had internal reliability of α=0.62, theanxious α=0.67, and the ambivalent α=0.76. Three groupswere formed by the forced choice of item 16 (secure, anxious,ambivalent), and analysis of variance of the three subscalemeans showed powerful discrimination of the groups(F=42.3, 27.9, and 62.4 pb0.0001 for secure, anxious, andambivalent respectively).
2.4. Blinded assessment procedures
The research design called for independent unbiasedassessment of each of the domains measured. Thus the diag-nostic interviewers who administered the SCID, did not haveaccess to the initial self-report, and the cognitive testing wasconducted by research assistants who were blind to theinitial self-report as well as to diagnostic status as reportedin the SCID.
2.5. Data management and statistical analysis
Data was entered by optically scanning the researchinstruments, and reading them into data sets by using OfficeRemark (version 10). After scanned documents were backedup, originals were shredded and recycled. Thus the privacy ofthe participants and the safety of the data were ensured. Allanalyses were carried out in SPSS for Windows version 18.0.
3. Results
All axis I diagnoses were assessed for lifetime prevalence.Table 1 summarizes the results by diagnostic groups, in orderof their frequency. Lifetime diagnoses of mood and anxiety dis-orders each occurred in about one third of subjects. Other
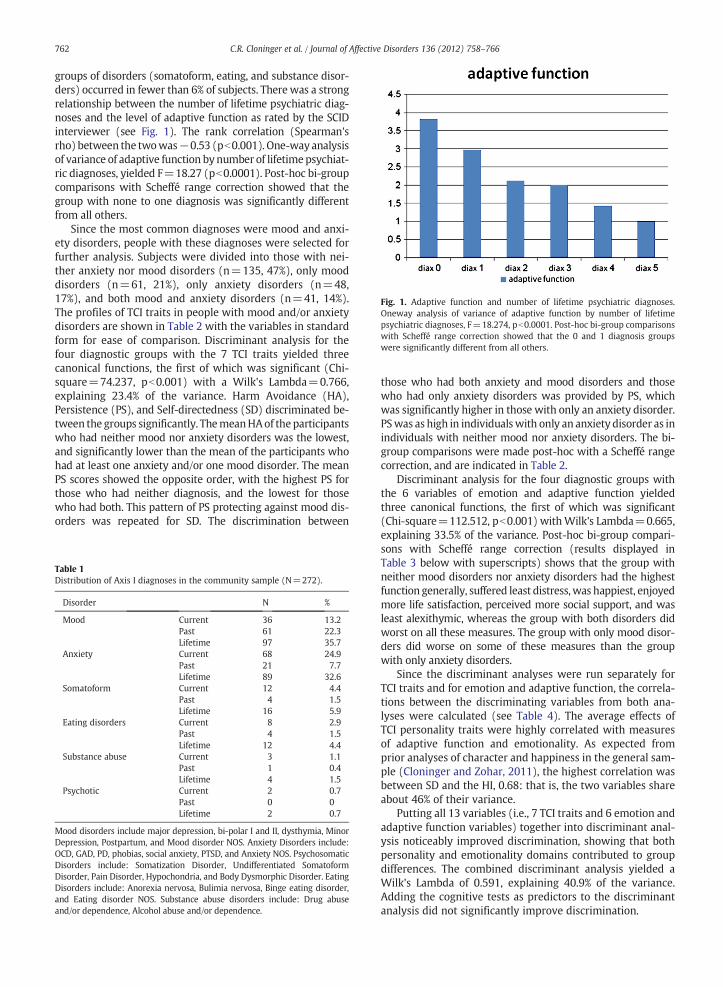
Fig. 1. Adaptive function and number of lifetime psychiatric diagnoses.Oneway analysis of variance of adaptive function by number of lifetimepsychiatric diagnoses, F=18.274, pb0.0001. Post-hoc bi-group comparisonswith Scheffé range correction showed that the 0 and 1 diagnosis groupswere significantly different from all others.
762 C.R. Cloninger et al. / Journal of Affective Disorders 136 (2012) 758–766
groups of disorders (somatoform, eating, and substance disor-ders) occurred in fewer than 6% of subjects. There was a strongrelationship between the number of lifetime psychiatric diag-noses and the level of adaptive function as rated by the SCIDinterviewer (see Fig. 1). The rank correlation (Spearman'srho) between the twowas−0.53 (pb0.001). One-way analysisof variance of adaptive function bynumber of lifetimepsychiat-ric diagnoses, yielded F=18.27 (pb0.0001). Post-hoc bi-groupcomparisons with Scheffé range correction showed that thegroup with none to one diagnosis was significantly differentfrom all others.
Since the most common diagnoses were mood and anxi-ety disorders, people with these diagnoses were selected forfurther analysis. Subjects were divided into those with nei-ther anxiety nor mood disorders (n=135, 47%), only mooddisorders (n=61, 21%), only anxiety disorders (n=48,17%), and both mood and anxiety disorders (n=41, 14%).The profiles of TCI traits in people with mood and/or anxietydisorders are shown in Table 2 with the variables in standardform for ease of comparison. Discriminant analysis for thefour diagnostic groups with the 7 TCI traits yielded threecanonical functions, the first of which was significant (Chi-square=74.237, pb0.001) with a Wilk's Lambda=0.766,explaining 23.4% of the variance. Harm Avoidance (HA),Persistence (PS), and Self-directedness (SD) discriminated be-tween the groups significantly. ThemeanHAof the participantswho had neither mood nor anxiety disorders was the lowest,and significantly lower than the mean of the participants whohad at least one anxiety and/or one mood disorder. The meanPS scores showed the opposite order, with the highest PS forthose who had neither diagnosis, and the lowest for thosewho had both. This pattern of PS protecting against mood dis-orders was repeated for SD. The discrimination between
Table 1Distribution of Axis I diagnoses in the community sample (N=272).
Disorder N %
Mood Current 36 13.2Past 61 22.3Lifetime 97 35.7
Anxiety Current 68 24.9Past 21 7.7Lifetime 89 32.6
Somatoform Current 12 4.4Past 4 1.5Lifetime 16 5.9
Eating disorders Current 8 2.9Past 4 1.5Lifetime 12 4.4
Substance abuse Current 3 1.1Past 1 0.4Lifetime 4 1.5
Psychotic Current 2 0.7Past 0 0Lifetime 2 0.7
Mood disorders include major depression, bi-polar I and II, dysthymia, MinorDepression, Postpartum, and Mood disorder NOS. Anxiety Disorders include:OCD, GAD, PD, phobias, social anxiety, PTSD, and Anxiety NOS. PsychosomaticDisorders include: Somatization Disorder, Undifferentiated SomatoformDisorder, Pain Disorder, Hypochondria, and Body Dysmorphic Disorder. EatingDisorders include: Anorexia nervosa, Bulimia nervosa, Binge eating disorder,and Eating disorder NOS. Substance abuse disorders include: Drug abuseand/or dependence, Alcohol abuse and/or dependence.
those who had both anxiety and mood disorders and thosewho had only anxiety disorders was provided by PS, whichwas significantly higher in those with only an anxiety disorder.PSwas as high in individualswith only an anxiety disorder as inindividuals with neither mood nor anxiety disorders. The bi-group comparisons were made post-hoc with a Scheffé rangecorrection, and are indicated in Table 2.
Discriminant analysis for the four diagnostic groups withthe 6 variables of emotion and adaptive function yieldedthree canonical functions, the first of which was significant(Chi-square=112.512, pb0.001) withWilk's Lambda=0.665,explaining 33.5% of the variance. Post-hoc bi-group compari-sons with Scheffé range correction (results displayed inTable 3 below with superscripts) shows that the group withneither mood disorders nor anxiety disorders had the highestfunction generally, suffered least distress,was happiest, enjoyedmore life satisfaction, perceived more social support, and wasleast alexithymic, whereas the group with both disorders didworst on all these measures. The group with only mood disor-ders did worse on some of these measures than the groupwith only anxiety disorders.
Since the discriminant analyses were run separately forTCI traits and for emotion and adaptive function, the correla-tions between the discriminating variables from both ana-lyses were calculated (see Table 4). The average effects ofTCI personality traits were highly correlated with measuresof adaptive function and emotionality. As expected fromprior analyses of character and happiness in the general sam-ple (Cloninger and Zohar, 2011), the highest correlation wasbetween SD and the HI, 0.68: that is, the two variables shareabout 46% of their variance.
Putting all 13 variables (i.e., 7 TCI traits and 6 emotion andadaptive function variables) together into discriminant anal-ysis noticeably improved discrimination, showing that bothpersonality and emotionality domains contributed to groupdifferences. The combined discriminant analysis yielded aWilk's Lambda of 0.591, explaining 40.9% of the variance.Adding the cognitive tests as predictors to the discriminantanalysis did not significantly improve discrimination.
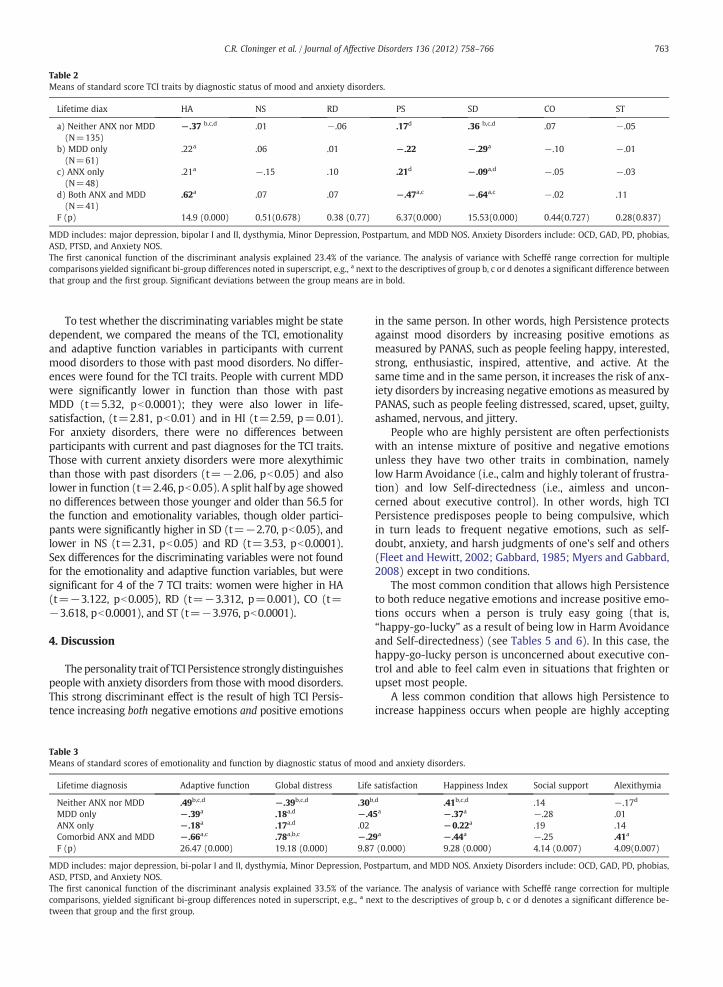
Table 2Means of standard score TCI traits by diagnostic status of mood and anxiety disorders.
Lifetime diax HA NS RD PS SD CO ST
a) Neither ANX nor MDD(N=135)
−.37 b,c,d .01 −.06 .17d .36 b,c,d .07 −.05
b) MDD only(N=61)
.22a .06 .01 −.22 −.29a −.10 −.01
c) ANX only(N=48)
.21a −.15 .10 .21d −.09a,d −.05 −.03
d) Both ANX and MDD(N=41)
.62a .07 .07 −.47a,c −.64a,c −.02 .11
F (p) 14.9 (0.000) 0.51(0.678) 0.38 (0.77) 6.37(0.000) 15.53(0.000) 0.44(0.727) 0.28(0.837)
MDD includes: major depression, bipolar I and II, dysthymia, Minor Depression, Postpartum, and MDD NOS. Anxiety Disorders include: OCD, GAD, PD, phobias,ASD, PTSD, and Anxiety NOS.The first canonical function of the discriminant analysis explained 23.4% of the variance. The analysis of variance with Scheffé range correction for multiplecomparisons yielded significant bi-group differences noted in superscript, e.g., a next to the descriptives of group b, c or d denotes a significant difference betweenthat group and the first group. Significant deviations between the group means are in bold.
763C.R. Cloninger et al. / Journal of Affective Disorders 136 (2012) 758–766
To test whether the discriminating variables might be statedependent, we compared the means of the TCI, emotionalityand adaptive function variables in participants with currentmood disorders to those with past mood disorders. No differ-ences were found for the TCI traits. People with current MDDwere significantly lower in function than those with pastMDD (t=5.32, pb0.0001); they were also lower in life-satisfaction, (t=2.81, pb0.01) and in HI (t=2.59, p=0.01).For anxiety disorders, there were no differences betweenparticipants with current and past diagnoses for the TCI traits.Those with current anxiety disorders were more alexythimicthan those with past disorders (t=−2.06, pb0.05) and alsolower in function (t=2.46, pb0.05). A split half by age showedno differences between those younger and older than 56.5 forthe function and emotionality variables, though older partici-pants were significantly higher in SD (t=−2.70, pb0.05), andlower in NS (t=2.31, pb0.05) and RD (t=3.53, pb0.0001).Sex differences for the discriminating variables were not foundfor the emotionality and adaptive function variables, but weresignificant for 4 of the 7 TCI traits: women were higher in HA(t=−3.122, pb0.005), RD (t=−3.312, p=0.001), CO (t=−3.618, pb0.0001), and ST (t=−3.976, pb0.0001).
4. Discussion
Thepersonality trait of TCI Persistence strongly distinguishespeople with anxiety disorders from those with mood disorders.This strong discriminant effect is the result of high TCI Persis-tence increasing both negative emotions and positive emotions
Table 3Means of standard scores of emotionality and function by diagnostic status of moo
Lifetime diagnosis Adaptive function Global distress Life
Neither ANX nor MDD .49b,c,d −.39b,c,d .30b
MDD only −.39a .18a,d −.4ANX only −.18a .17a,d .02Comorbid ANX and MDD −.66a,c .78a,b,c −.2F (p) 26.47 (0.000) 19.18 (0.000) 9.87
MDD includes: major depression, bi-polar I and II, dysthymia, Minor Depression, PoASD, PTSD, and Anxiety NOS.The first canonical function of the discriminant analysis explained 33.5% of the vacomparisons, yielded significant bi-group differences noted in superscript, e.g., a netween that group and the first group.
in the same person. In other words, high Persistence protectsagainst mood disorders by increasing positive emotions asmeasured by PANAS, such as people feeling happy, interested,strong, enthusiastic, inspired, attentive, and active. At thesame time and in the same person, it increases the risk of anx-iety disorders by increasing negative emotions as measured byPANAS, such as people feeling distressed, scared, upset, guilty,ashamed, nervous, and jittery.
People who are highly persistent are often perfectionistswith an intense mixture of positive and negative emotionsunless they have two other traits in combination, namelylow Harm Avoidance (i.e., calm and highly tolerant of frustra-tion) and low Self-directedness (i.e., aimless and uncon-cerned about executive control). In other words, high TCIPersistence predisposes people to being compulsive, whichin turn leads to frequent negative emotions, such as self-doubt, anxiety, and harsh judgments of one's self and others(Fleet and Hewitt, 2002; Gabbard, 1985; Myers and Gabbard,2008) except in two conditions.
The most common condition that allows high Persistenceto both reduce negative emotions and increase positive emo-tions occurs when a person is truly easy going (that is,“happy-go-lucky” as a result of being low in Harm Avoidanceand Self-directedness) (see Tables 5 and 6). In this case, thehappy-go-lucky person is unconcerned about executive con-trol and able to feel calm even in situations that frighten orupset most people.
A less common condition that allows high Persistence toincrease happiness occurs when people are highly accepting
d and anxiety disorders.
satisfaction Happiness Index Social support Alexithymia
,d .41b,c,d .14 −.17d
5a −.37a −.28 .01−0.22a .19 .14
9a −.44a −.25 .41a
(0.000) 9.28 (0.000) 4.14 (0.007) 4.09(0.007)
stpartum, and MDD NOS. Anxiety Disorders include: OCD, GAD, PD, phobias,
riance. The analysis of variance with Scheffé range correction for multiplext to the descriptives of group b, c or d denotes a significant difference be-
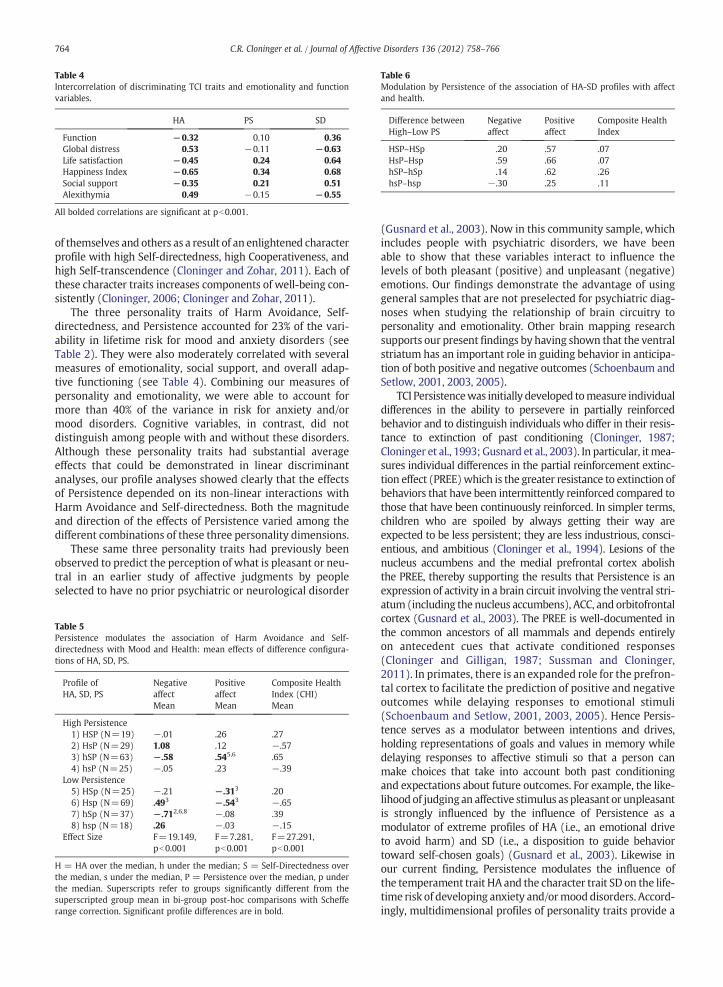
Table 4Intercorrelation of discriminating TCI traits and emotionality and functionvariables.
HA PS SD
Function −0.32 0.10 0.36Global distress 0.53 −0.11 −0.63Life satisfaction −0.45 0.24 0.64Happiness Index −0.65 0.34 0.68Social support −0.35 0.21 0.51Alexithymia 0.49 −0.15 −0.55
All bolded correlations are significant at pb0.001.
Table 6Modulation by Persistence of the association of HA-SD profiles with affectand health.
Difference betweenHigh–Low PS
Negativeaffect
Positiveaffect
Composite HealthIndex
HSP–HSp .20 .57 .07HsP–Hsp .59 .66 .07hSP–hSp .14 .62 .26hsP–hsp −.30 .25 .11
764 C.R. Cloninger et al. / Journal of Affective Disorders 136 (2012) 758–766
of themselves and others as a result of an enlightened characterprofile with high Self-directedness, high Cooperativeness, andhigh Self-transcendence (Cloninger and Zohar, 2011). Each ofthese character traits increases components of well-being con-sistently (Cloninger, 2006; Cloninger and Zohar, 2011).
The three personality traits of Harm Avoidance, Self-directedness, and Persistence accounted for 23% of the vari-ability in lifetime risk for mood and anxiety disorders (seeTable 2). They were also moderately correlated with severalmeasures of emotionality, social support, and overall adap-tive functioning (see Table 4). Combining our measures ofpersonality and emotionality, we were able to account formore than 40% of the variance in risk for anxiety and/ormood disorders. Cognitive variables, in contrast, did notdistinguish among people with and without these disorders.Although these personality traits had substantial averageeffects that could be demonstrated in linear discriminantanalyses, our profile analyses showed clearly that the effectsof Persistence depended on its non-linear interactions withHarm Avoidance and Self-directedness. Both the magnitudeand direction of the effects of Persistence varied among thedifferent combinations of these three personality dimensions.
These same three personality traits had previously beenobserved to predict the perception of what is pleasant or neu-tral in an earlier study of affective judgments by peopleselected to have no prior psychiatric or neurological disorder
Table 5Persistence modulates the association of Harm Avoidance and Self-directedness with Mood and Health: mean effects of difference configura-tions of HA, SD, PS.
Profile ofHA, SD, PS
NegativeaffectMean
PositiveaffectMean
Composite HealthIndex (CHI)Mean
High Persistence1) HSP (N=19) −.01 .26 .272) HsP (N=29) 1.08 .12 −.573) hSP (N=63) −.58 .545,6 .654) hsP (N=25) −.05 .23 −.39
Low Persistence5) HSp (N=25) −.21 −.313 .206) Hsp (N=69) .493 −.543 −.657) hSp (N=37) −.712,6,8 −.08 .398) hsp (N=18) .26 −.03 −.15
Effect Size F=19.149,pb0.001
F=7.281,pb0.001
F=27.291,pb0.001
H = HA over the median, h under the median; S = Self-Directedness overthe median, s under the median, P = Persistence over the median, p underthe median. Superscripts refer to groups significantly different from thesuperscripted group mean in bi-group post-hoc comparisons with Schefferange correction. Significant profile differences are in bold.
(Gusnard et al., 2003). Now in this community sample, whichincludes people with psychiatric disorders, we have beenable to show that these variables interact to influence thelevels of both pleasant (positive) and unpleasant (negative)emotions. Our findings demonstrate the advantage of usinggeneral samples that are not preselected for psychiatric diag-noses when studying the relationship of brain circuitry topersonality and emotionality. Other brain mapping researchsupports our present findings by having shown that the ventralstriatum has an important role in guiding behavior in anticipa-tion of both positive and negative outcomes (Schoenbaum andSetlow, 2001, 2003, 2005).
TCI Persistencewas initially developed tomeasure individualdifferences in the ability to persevere in partially reinforcedbehavior and to distinguish individuals who differ in their resis-tance to extinction of past conditioning (Cloninger, 1987;Cloninger et al., 1993; Gusnard et al., 2003). In particular, itmea-sures individual differences in the partial reinforcement extinc-tion effect (PREE)which is the greater resistance to extinction ofbehaviors that have been intermittently reinforced compared tothose that have been continuously reinforced. In simpler terms,children who are spoiled by always getting their way areexpected to be less persistent; they are less industrious, consci-entious, and ambitious (Cloninger et al., 1994). Lesions of thenucleus accumbens and the medial prefrontal cortex abolishthe PREE, thereby supporting the results that Persistence is anexpression of activity in a brain circuit involving the ventral stri-atum (including the nucleus accumbens), ACC, and orbitofrontalcortex (Gusnard et al., 2003). The PREE is well-documented inthe common ancestors of all mammals and depends entirelyon antecedent cues that activate conditioned responses(Cloninger and Gilligan, 1987; Sussman and Cloninger,2011). In primates, there is an expanded role for the prefron-tal cortex to facilitate the prediction of positive and negativeoutcomes while delaying responses to emotional stimuli(Schoenbaum and Setlow, 2001, 2003, 2005). Hence Persis-tence serves as a modulator between intentions and drives,holding representations of goals and values in memory whiledelaying responses to affective stimuli so that a person canmake choices that take into account both past conditioningand expectations about future outcomes. For example, the like-lihoodof judging an affective stimulus as pleasant or unpleasantis strongly influenced by the influence of Persistence as amodulator of extreme profiles of HA (i.e., an emotional driveto avoid harm) and SD (i.e., a disposition to guide behaviortoward self-chosen goals) (Gusnard et al., 2003). Likewise inour current finding, Persistence modulates the influence ofthe temperament trait HA and the character trait SD on the life-time risk of developing anxiety and/ormooddisorders. Accord-ingly, multidimensional profiles of personality traits provide a

765C.R. Cloninger et al. / Journal of Affective Disorders 136 (2012) 758–766
powerful way to describe the motivations, strengths, andvulnerabilities of a person across diverse life situations.
The major limitation of this study is that the subjects werealready 40 years of age or older at the time of their baselineassessment. This age group was selected in phase 1 of thestudy in order to be able to identify substantial numbers ofpeople with medical disorders like hypertension and heartdisease within a few years. Then in phase 2 we selectedgroups of people predicted to be high and low in well-beingon the basis of personality traits, including HA, RD, and SD.There was no selection on PS because of uncertainty aboutwhether its overall impact on well-being was positive ornegative. Hence the phase 2 sample provided an excellentopportunity to assess the interactions of Persistence withextremes of HA and SD. However, because of the age ofsubjects, personality was assessed after subjects had alreadypassed through most of their period of lifetime risk for com-mon psychiatric disorders. Consequently it will be useful forus to replicate findings from this study in other prospectivestudies in which personality is measured at an early ageand then people are followed over many years to assess thedynamics of their health and well-being, as is being doneelsewhere (Hintsanen et al., 2009).
Our findings show clearly that human personality is com-prised of multiple dimensions that interact as a complex adap-tive system, rather than as a collection of separate components.Because of the non-linear dynamics of personality development,methods that assume linearity, such as linear actor analysis andlinear regression analyses with independent predictors, may beill-suited for assessing the number and content of personalitycomponents or the way the personalities of people influencetheir health and other important life outcomes (Cloninger,2004, 2008). Models of personality structure must considerextra-statistical information about the complex psychobiologyof personality in order to be realistic, as has been done indeveloping the seven-factor model used here. Likewise profileanalyses are more appropriate and sensitive to detecting non-linear interactions, as we have shown here and elsewhere(Cloninger and Zohar, 2011). Fortunately, profiles also allowclinicians and researchers to adopt a person-centered perspec-tive, rather than focusing on the average effects of separatedimensions between groups of people (Cloninger andCloninger,2011). In this way, personality profiles provide a way torecognize personality types, such as Akiskal's dysthymics andhyperthymics (Maremmani et al., 2005). Profiles, therefore,havemany of the advantages of categorical diagnoses and typol-ogies, while preserving information on meta-stable configura-tions of component processes. As noted by Insel (Insel et al.,2010), our results illustrate how helpful it is to understandbrain circuitry as a basis for understanding the dynamics ofpersonality, emotionality, and psychopathology.
Clinically, our findings indicate that high TCI Persistence hasboth costs and benefits. Persistence is neither good nor bad; itsvalue depends on a complex set of adaptive processes, bothinternal and external, and how well these forces that pushand pull on the person are integrated and balanced. Beinghighly persistent is likely to lead to intensemixtures of positiveand negative emotions, which can lead to high achievement,much anxiety, or both. Paradoxically, trying to be perfect is aself-defeating goal, and trying to be irreproachable leadsinevitably to harsh judgments of guilt and shame. Fortunately,
Persistence also can help a person to let go of self-defeatingdrives and intentions by becoming self-aware of them andthen learning how to let go of fighting with one's self byusing the principles and practices of the science of well-being(Cloninger and Cloninger, 2011; Cloninger et al., 2010).
Role of the funding sourceThis research was supported by the United States Israel Binational Science
Foundation (BSF). The BSF provided funding for the four year researchdescribed in the current paper, including paying for the laboratory personneland procedures, the medical examinations, all the expenses of data gatheringand data maintenance. The BSF did not pay the salaries of any of the authors,save Dana Dahan, who was project manager for three of the four years of theproject.
Conflict of interestNo conflict of interest is present for any of the authors.
AcknowledgmentThis research was supported by the United States Israel Binational Sci-
ence Foundation, grant #2005-48 to AHZ and CRC.
References
Bachar, E., Canetti, L., Bonne, O., DeNour, A.K., Shalev, A.Y., 1997. Physicalpunishment and signs of mental distress in normal adolescents. Adoles-cence 32, 945–958.
Bagby, R.M., Parker, J.D.A., Taylor, G.J., 1994. The twenty-item Toronto Alex-ithymia Scale. Journal of Psychosomatic Research 38 (1), 23–32.
Beevers, C.G., Miller, I.W., 2004. Perfectionism, cognitive bias, and hopeless-ness as prospective predictors of suicidal ideation. Suicide & Life-Threatening Behavior 34, 126–137.
Brooks, D., 2010. The Tel Aviv Cluster. New York Times. New York Times,New York.
Bulik, C.M., Sullivan, P.F., Fear, J.L., Pickering, A., 2000. Outcome of anorexianervosa: eating attitudes, personality, and parental bonding. Interna-tional Journal of Eating Disorders 28, 139–147.
Cloninger, C.R., 1987. A systematic method for clinical description andclassification of personality variants. A proposal. Archives of GeneralPsychiatry 44, 573–588.
Cloninger, C.R., 2004. Feeling Good: The Science of Well-Being. OxfordUniversity Press, New York.
Cloninger, C.R., 2006. The science of well-being: an integrated approach tomental health and its disorders. World Psychiatry 5, 71–76.
Cloninger, C.R., 2008. The psychobiological theory of temperament andcharacter: comment on Farmer and Goldberg. Psychological Assessment20, 292–299 discussion 300-294.
Cloninger, C.R., Cloninger, K.M., 2011. Person-centered therapeutics. Interna-tional Journal of Person-centered Medicine 1 (1), 43–52.
Cloninger, C.R., Gilligan, S.B., 1987. Neurogenetic mechanisms of learning:a phylogenetic perspective. Journal of Psychiatric Research 21,457–472.
Cloninger, C.R., Zohar, A.H., 2011. Personality and the perception of healthand happiness. Journal of Affective Disorders 128, 24–32.
Cloninger, C.R., Svrakic, D.M., Przybeck, T.R., 1993. A psychobiological modelof temperament and character. Archives of General Psychiatry 50,975–990.
Cloninger, C.R., Przybeck, T.R., Svrakic, D.M., Wetzel, R.D., 1994. The Tempera-ment and Character Inventory (TCI): A Guide to its Development andUse. Washington University Center for Psychobiology of Personality, St.Louis.
Cloninger, C.R., Bayon, C., Svrakic, D.M., 1998. Measurement of tempera-ment and character in mood disorders: a model of fundamental statesas personality types. Journal of Affective Disorders 51, 21–32.
Cloninger, C.R., Zohar, A.H., Cloninger, K.M., 2010. Promotion of well-being inperson-centered mental health care. Focus 8, 165–179.
Delis, D.C., Kramer, J.H., Kaplan, E., Ober, B.A., 2000. California Verbal LearningTest (CVLT-II). Pearson, Bloomington, MN.
Derogatis, L.R.B., 1993. Brief Symptom Inventory Administration ScoringProcedure Manual. National Computer Systems Research, Minneapolis,MN.
Farmer, A., Mahmood, A., Redman, K., Harris, T., Sadler, S., McGuffin, P., 2003.A sib-pair study of the Temperament and Character Inventory scales inmajor depression. Archives of General Psychiatry 60, 490–496.
766 C.R. Cloninger et al. / Journal of Affective Disorders 136 (2012) 758–766
Fassino, S., Amianto, F., Gramaglia, C., Facchini, F., Abbate Daga, G., 2004.Temperament and character in eating disorders: ten years of studies.Eating and Weight Disorders 9, 81–90.
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 2002. Structured ClinicalInterview for DSM-IV-TR Axis I Disorders Research Version, Non-patientEdition (SCID-I/NP). Biometrics Research, New York State PsychiatricInstitute, New York.
Fleet, G.L., Hewitt, P.L. (Eds.), 2002. Perfectionism: Theory, Research, andTreatment. American Psychological Association, Washington, DC.
Gabbard, G.O., 1985. The role of compulsiveness in the normal physician.JAMA 254, 2926–2929.
Garcia, D., 2011. Two models of personality and well-being among adoles-cents. Personality and Individual Differences 50, 1208–1212.
Gilboa, A., Kave, G., 2007. The Shipley Institute of Living Scale (SILS) inHebrew. Haifa University, Haifa.
Gilboa, A., Kave, G., 2008. The California Verbal Learning Test II (CVLT-II) inHebrew. Haifa University, Haifa.
Gillespie, N.A., Cloninger, C.R., Heath, A.C., Martin, N.G., 2003. The geneticand environmental relationship between Cloninger's dimensions oftemperament and character. Personality and Individual Differences 35,1931–1946.
Gusnard, D.A., Akbudak, E., Shulman, G.L., Raichle, M.E., 2001. Medial pre-frontal cortex and self-referential mental activity: relation to a defaultmode of brain function. Proceedings of the National Academy of Sciencesof the United States of America 98, 4259–4264.
Gusnard, D.A., Ollinger, J.M., Shulman, G.L., Cloninger, C.R., Price, J.L.,Van Essen, D.C., Raichle, M.E., 2003. Persistence and brain circuitry.Proceedings of the National Academy of Sciences of the United Statesof America 100, 3479–3484.
Hamilton, T.K., Schweitzer, R.D., 2000. The cost of being perfect: perfectionismand suicide ideation in university students. The Australian and NewZealand Journal of Psychiatry 34, 829–835.
Hazan, C., Shaver, P., 1987. Romantic love conceptualized as an attachmentprocess. Journal of Personality and Social Psychology 52, 511–524.
Heath, A.C., Cloninger, C.R., Martin, N.G., 1994. Testing a model for the geneticstructure of personality: a comparison of the personality systems of Cloningerand Eysenck. Journal of Personality and Social Psychology 66, 762–775.
Hintsanen, M., Pulkki-Raback, L., Juonala, M., Viikari, J.S., Raitakari, O.T.,Keltikangas-Jarvinen, L., 2009. Cloninger's temperament traits andpreclinical atherosclerosis: the Cardiovascular Risk in Young Finns Study.Journal of Psychosomatic Research 67, 77–84.
Insel, T., Cuthbert, B., Garvey, M., Heinssen, R., Pine, D.S., Quinn, K., Sanislow, C.,Wang, P., 2010. Research domain criteria (RDoC): toward a new classifica-tion framework for research on mental disorders. The American Journal ofPsychiatry 167, 748–751.
Lang, P.J., Bradley, M.M., Cuthbert, B.N., 1997. International Affective PictureSystem (IAPS): Technical Manual and Affective Ratings. National Insti-tute of Mental Health Center for the Studyof Emotion and Attention,Gainesville, FL.
Maremmani, I., Akiskal, H.S., Signoretta, S., Liguori, A., Perugi, G., Cloninger,R., 2005. The relationship of Kraepelian affective temperaments (asmeasured by TEMPS-I) to the tridimensional personality questionnaire(TPQ). Journal of Affective Disorders 85, 17–27.
Mason, C.F., Lemmon, D., Wayne, K.S., Schmidt, R., 1991. Shipley Institute ofLiving Scale (SILS): formulas for abstraction quotients from a normativesample of 580. Sex and SES considered as additioinal moderating variables.Psychological Assessment 3, 412–417.
Mulder, R.T., Joyce, P.R., Sellman, J.D., Sullivan, P.F., Cloninger, C.R., 1996.Towards an understanding of defense style in terms of temperamentand character. Acta Psychiatrica Scandinavica 93, 99–104.
Myers, M.F., Gabbard, G.O., 2008. The Physician as Patient: A Clinical Hand-book for Mental Health Professionals. American Psychiatric AssociationWashington, DC.
Nery, F.G., Hatch, J.P., Glahn, D.C., Nicoletti, M.A., Monkul, E.S., Najt, P., Fonseca,M., Bowden, C.L., Cloninger, C.R., Soares, J.C., 2008. Temperament andcharacter traits in patients with bipolar disorder and associations withcomorbid alcoholism or anxiety disorders. Journal of Psychiatric Research42, 569–577.
Nery, F.G., Hatch, J.P., Nicoletti, M.A., Monkul, E.S., Najt, P., Matsuo, K., Cloninger,C.R., Soares, J.C., 2009. Temperament and character traits in major depres-sive disorder: influence of mood state and recurrence of episodes. Depres-sion and Anxiety 26, 382–388.
Osher, Y., Cloninger, C.R., Belmaker, R.H., 1996. TPQ in euthymic manic-depressive patients. Journal of Psychiatric Research 30, 353–357.
Osher, Y., Lefkifker, E., Kotler, M., 1999. Low persistence in euthymic manic-depressive patients: a replication. Journal of Affective Disorders 53, 87–90.
Paus, T., 2001. Primate anterior cingulate cortex: where motor control, driveand cognition interface. Nature Reviews Neuroscience 2, 417–424.
Pease, S.L., 2009. The Golden Age of Jewish Achievement: The Compendiumof a Culture, a People, and Their Stunning Performance. Deucalion,Sonoma Valley, USA.
Pezawas, L., Meyer-Lindenberg, A., Drabant, E.M., Verchinski, B.A., Munoz, K.E.,Kolachana, B.S., Egan,M.F., Mattay, V.S., Hariri, A.R.,Weinberger, D.R., 2005.5-HTTLPR polymorphism impacts human cingulate–amygdala interac-tions: a genetic susceptibility mechanism for depression. Nature Neurosci-ence 8, 828–834.
Robbins, T.W., Everitt, B.J., 1996. Neurobehavioural mechanisms of rewardand motivation. Current Opinion in Neurobiology 6, 228–236.
Schoenbaum, G., Setlow, B., 2001. Integrating orbitofrontal cortex intoprefrontal theory: common processing themes across species and subdi-visions. Learning and Memory 8, 134–147.
Schoenbaum, G., Setlow, B., 2003. Lesions of nucleus accumbens disruptlearning about aversive outcomes. Journal of Neuroscience 23, 9833–9841.
Schoenbaum, G., Setlow, B., 2005. Cocaine makes actions insensitive tooutcomes but not extinction: implications for altered orbitofrontal–amygdalar function. Cerebral Cortex 15, 1162–1169.
Schultz, W., Tremblay, L., Hollerman, J.R., 2000. Reward processing in primateorbitofrontal cortex and basal ganglia. Cerebral Cortex 10, 272–284.
Schultz, W., Tremblay, L., Hollerman, J.R., 2003. Changes in behavior-relatedneuronal activity in the striatum during learning. Trends in Neurosciences26, 321–328.
Senor, D., Singer, S., 2009. Start-Up Nation: The Story of Israel's EconomicMiracle. The Hachette Book Group, New York, Twelve.
Shipley, W.C., 1940. A self-administering scale for measuring intellectualimpairment and defoliation. Journal of Psychology 9, 371–377.
Sussman, R.W., Cloninger, C.R. (Eds.), 2011. Origins of Cooperation andAltruism. Springer, New York.
Svrakic, D.M., Whitehead, C., Przybeck, T.R., Cloninger, C.R., 1993. Differentialdiagnosis of personality disorders by the seven-factor model of tempera-ment and character. Archives of General Psychiatry 50, 991–999.
Watson, D., Clark, L.A., Carey, G., 1988. Positive and negative affectivity andtheir relation to anxiety and depressive disorders. Journal of AbnormalPsychology 97, 346–353.
Weiss, J.L., Schell, R.E., 1991. Estimating WAIS-R IQ from the Shipley Instituteof Living Scale: a replication. Journal of Clinical Psychology 47, 558–562.
Zachary, R.A., 1986. Shipley Institute of Living Scale-Revised manual.Western Psychological Services, Los Angeles.
Zimet, G.D., Powell, S.S., Farley, G.K., Werkman, S., Berkoff, K.A., 1990.Psychometric characteristics of the Multidimensional Scale of PerceivedSocial Support. Journal of Personality Assessment 55, 610–617.
Zohar, A.H., Cloninger, C.R., 2011. The psychometric properties of theTCI-140 in Hebrew. European Journal of Psychological Assessment 27,73–80.
Zohar, A.H., Denollet, J.K., Lev Ari, L., Cloninger, C.R., 2011. The psychometricproperties of the DS14 in Hebrew and the prevalence of Type D in Israeliadults. European Journal of Psychological Assessment 27, 274–281.