the lung cancer epidemic in australia, 1910 to 1989
TRANSCRIPT

BRIEF REPORT
The lung cancer epidemic in Australia, 1910 to 1989
Graham G. Giles, David J. Hill and Bronwyn Silver Anti-Cancer Council of Victoria, Melbourne
Abstract: Deaths that occurred in Australia between 1985 and 1989 that were ascribed to cancers of the respiratory tract and intrathoracic organs were obtained to update Australian lung cancer mortality trends. The age-standardised mortality rate from lung cancer in males decreased significantly from 49/100 000 in 1980-1984 to 46.4/100 000 in 1985-1989 (-5.5%). Lung cancer mortality in females increased significantly to 12.3/100 000 in 1985- 1989 from an average of 10.7/100 000 in 1980-1984 (+ 15%). We conclude that lung cancer mortality in males is declining and although mortality in females continues to increase, there is evidence that the rate of increase has started to slow. The decline in male mortality has been anticipated from their trends in smoking cessation. The slowing increase in women cannot be ascribed to similar patterns of cessation. It is considered more likely to be due to decreasing trends in tar consumption linked to the tar content of preferred brands. (AwtJ Public Health 1991; 15: 245-7)
rends in cancer mortality in Australia have been previously reported for 19 10-1 9 14 to T 1975-1979' and for 1980-1984.' The major
upward trend observed has been for increased mor- tality from cancer of the lower respiratory tract in both males and females. In the most recent quinquennium, 1980-1 984, mortality rates were continuing to increase in both sexes. Although the rate of increase in males had slowed considerably since the 1970s, no comparable trend was apparent for females. An examination of trends by age, sex and year of birth showed evidence of a cohort-based peak in mortality after 30 years of age in males born around 1930 and a cross-sectional levelling out of mortality in older men beginning about 1965-1969. In women, cohort-based increases in mortality began in those born around 1900. A steady increase in mor- tality was observed since 1960-1964 but this slowed in women aged under 65 since 1975-1979. This report updates lung cancer mortality trends by an extra quinquennium, 1985-1989.
Data and methods To maintain comparability over time with published data, the sources and methods used were identical to those of previous analyses.'.' Mortality tabulations of International Classification of Diseases (ICD) three- digit rubrics, by sex and age in five-year age groups 0-4 to 85+ , were obtained from the Australian Bureau of Statistics for 1985 to 1989, as were the annual Australian population estimates by age and sex. As before, ICD rubrics 162 to 165 were aggre- gated into a group described as respiratory and intrathoracic organs (lung). Age- and sex-specific lung cancer mortality rates per 100 000 person-years
Correspondence to Dr G.C. Giles, Cancer Epidemiology Centre, Anti-Cancer Council of Victoria, 1 Rathdowne Street, Carlton South, VIC 3053
were calculated and the summary rates were directly age-adjusted to the World Standard Population. Standard errors were calculated using a Poisson formula.'
Results Lung cancer killed over 30 000 Australians between 1985 and 1989; 23 120 men and 7137 women. The age- and sex-specific rates and the age-standardised rates per 100 000 person-years are given in Table 1 with the proportional changes between 1980-1 984 and 1985-1989. Changes in age-specific rates were not uniform with age. Large relative decrements in male age-specific rates were observed in males born since 1925-1 929 and smaller reductions in men born 1900-1924. Rates in men born before 1900 con- t inued to rise. Statistically significant interquinquennial changes were observed in men aged 45 to 59 and 70 to 74. In women, age-specific rates virtually all increased between the two quinquennia, the largest relative increments being observed in women born between 1900 and 1915 and between 1935 and 1949. Statistically significant increases were restricted to women aged 70 to 84.
Figure 1 illustrates the trends by sex in the age- standardised rates from 1910-1914 to 1985-1989. The proportional changes between quinquennia in the age-standardised rates over time are not obvious from the figure. Overall, the male rate dropped by about 5 per cent between 1980-1984 and 1985- 1989 and the female rate rose by about 15 per cent in the same interval. These changes were statistically sig- nificant at the 5 per cent level. Table 2 gives the stan- dardised quinquennial rates by sex with their standard errors and the percentage change between quinquennia beginning with 1960-1964. It is appar- ent that the rate of increase in males slowed dramati- cally before it stopped. The rate of increase in the
AUSTRALIAN JOURNAL OF PUBLIC HEALTH 1991 VOL. 15 NO. 3 245
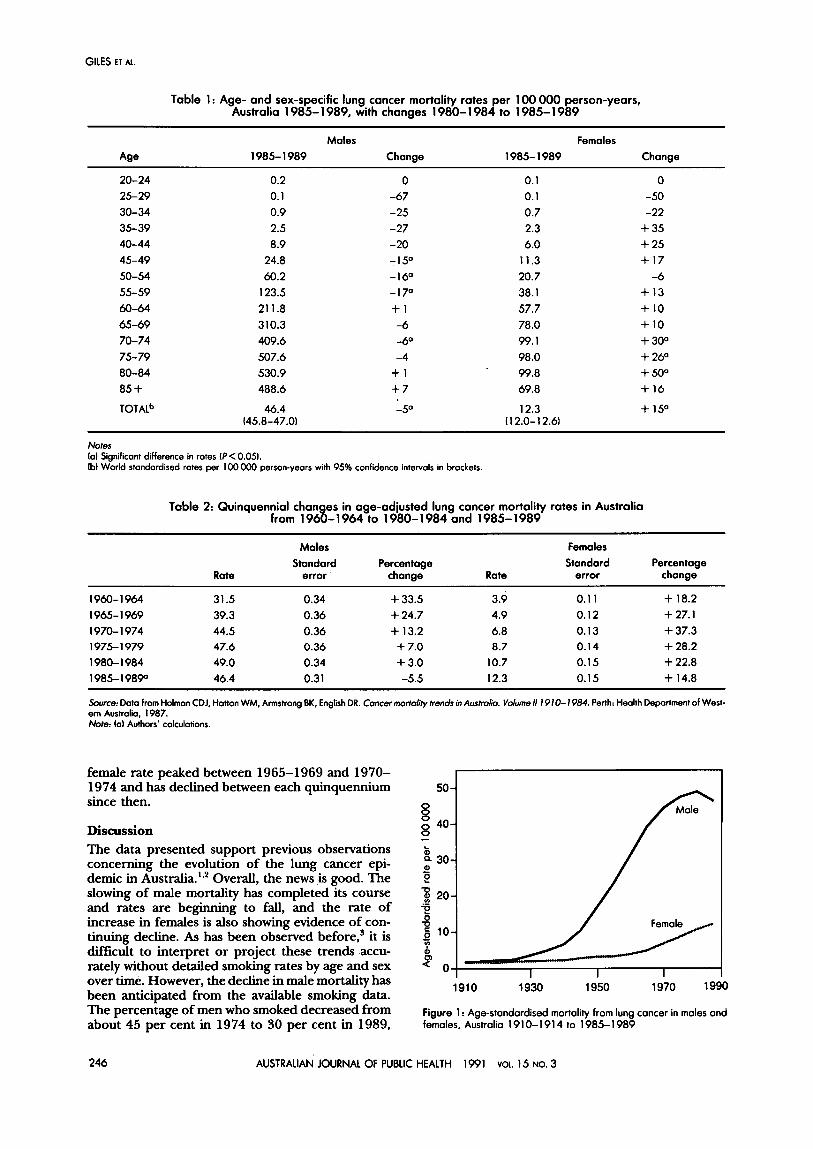
Table 1 : Age- and sex-specific lung cancer mortality rates per 100 000 person-years, Australia 1985- 1989, with changes 1980- 1 984 to 1 985- 1989
Males Females Age 1985- 1989 Change 1985- 1989 Change
female rate peaked between 1965-1969 and 1970- 1974 and has declined between each quinquennium 50 - since then. 0
0 ; 40- - Discussion The data presented support previous observations concerning the evolution of the lung cancer epi- demic in Australia.'.' Overall, the news is good. The slowing of male mortality has completed its course and rates are beginning to fall, and the rate of increase in females is also showing evidence of con-
t, 30-
Z 2 20- ; u 6 10-
: 2 0
c
tinuing decline. As has been observed before,3 it is difficult to interpret or project these trends accu-
*
rately without detailed smoking rates by age and sex over time. However, the decline in male mortality has
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85 +
I I I
0.2 0.1 0.9 2.5 8.9 24.8 60.2 123.5 21 1.8 3 10.3 409.6 507.6 530.9 488.6
0 -67 -25 -27 -20 -15' -16' -17' + 1 -6 -6' -4
+ 1 +7
0.1 0.1 0.7 2.3 6.0 11.3 20.7 38.1 57.7 78.0 99.1 98.0 99.8 69.8
0 -50 -22
+ 35 + 25 + I7 -6
+ I3 + 10 + 10 + 30' + 26' + 50' + 16
TOTALb 46.4 -5' 12.3 + 15' (45.8-47.01 (1 2.0-1 2.61
Notes la1 Significant difference in rotes I f < 0.051. lb) World standardised rotes per 100 OOO person-yeors with 95% confidence intervals in brackets.
Table 2: Quinquennial chon es in age-adiusted lung cancer mortality rates in Australia from 1968-1 964 to 1980- 1984 and 1985- 1989
Males Females
Rate error change Rate error change Standard Percentage Standard Percentage
1960-1964 31.5 0.34 + 33.5 3.9 0.1 1 + 18.2 1965- 1 969 39.3 0.36 + 24.7 4.9 0.12 + 27.1 1970- 1 974 44.5 0.36 + 13.2 6.8 0.13 + 37.3 1 975- 1 979 47.6 0.36 + 7.0 8.7 0.14 + 28.2 1980- 1984 49.0 0.34 + 3.0 10.7 0.15 + 22.8 1985- 19890 46.4 0.31 -5.5 12.3 0.15 + 14.8 Source: Doto from Holman CDJ, Hatton WM, Anstrang BK, English DR. Cancer morfa/ity trends in Australia. Volume /I I91 0- 1984. Perth: Health Deportment of West- ern Austrolia. 1987. Note: lo) Authors' calculations.
246 AUSTRALIAN JOURNAL OF PUBLIC HEALTH 1991 VOL. I5 NO. 3

LUNG CANCER EPIDEMIC I N AUSTRALIA
when almost 30 per cent of Australian males were ex smoker^.^
The downturn in male lung cancer mortality is con- sistent with trends in other countries5 and gives room for optimism about future improvement. Data from England and Wales5 and the United States' show similar trends in levelling off of male lung cancer mortality. In United States white males there is evi- dence of a fall in incidence rates but this is not seen for blacks.' Similar ethnic and/or socioeconomic dif- ferences can be obtained from Australian data where British-Irish migrants have been observed to have higher rates of smoking and lung cancer.' In Mel- bourne, significant differentials in lung cancer inci- dence and mortality have been shown across socioeconomic strata, those in the lowest decile hav- ing 40 per cent more lung cancer than those in the highest decile.' There are also Australian socioeconomic differences in smoking prevalence largely due to members of higher status groups and white-collar occupations never taking up the
Twenty-seven per cent of Australian women cur- rently smoke and a further 19 per cent are exsmokers. The fall in smoking prevalence in females has been from about 30 per cent in 1974 to about 27 per cent in 1989, a nonsignificant decrease com- pared to that in males. The reducing rate of increase in lung cancer mortality in females may be due more to their reduced tar intake than to a reduction in the number of smokers. Hill et aL4 estimated that between 1986 and 1989 male smokers reduced their tar intake by 10 per cent and female smokers by 19 per cent as a result of changes in tar content of brands smoked.
Structural changes, such as price increases, tar decreases and advertising reforms, and behavioural change linked to smoking cessation programs have combined to bring about recent declines in male lung cancer mortality in Australia and similar changes appear to be slowing the female epidemic. Yet thou- sands of Australians living today will die of lung can- cer before the end of the century. Within the 1990s it could be possible to achieve even greater reductions and save hundreds of lives by stepping up health pro-
motion and smoking cessation programs, as it is known that changes in lung cancer mortality can be observed within a relatively short time after smoking cessation." The trends illustrated above should encourage public health workers but should not allow complacency. As prefaced in the US Surgeon General's report" on 25 years of progress in reduc- ing the health consequences of smoking, the remain- ing challenges include children and adolescents, women, minorities and blue-collar workers. It is not going to be easy to control smoking in these groups most at risk of taking up and continuing the smoking habit, particularly in the face of targeting by tobacco advertising.
References 1 . Holman CDJ, Armstrong BK. Cancer mottality trends in Aur-
tralia 1910-1976. Perth: Cancer Council of Western Aus tralia, 1982.
2. Holman CDJ, Hatton WM, Armstrong BK, English DR. Can- cer mmlality trends in Australia. Volume I1 1910-1984. Perth: Health Department of Western Australia, 1987.
3. Winstanley M. Tobacco in Australia: f i and issues. Sydney: ASH (Action for Smoking and Health) Australia, 1989.
4. Hill DJ, White VM, Gray NJ. Australian patterns of tobacco smoking in 1989. Med J Awl. In press.
5. Davis Dl, Hoe1 D, Fox J, Lopez A. International trends in can- cer mortality in France, West Germany, Italy, Japan, England and Wales and the U.S.A. Lancet 1990; 336: 474-81.
6. Centers for Disease Control. Trends in lung cancer incidence and mortality-United States, 1980-1987. MMWR 1990;
7. McMichael AJ, Giles GG. Cancer in migrants to Australia: extending the descriptive epidemiological data. C a w Rcs
8. Williams J, Clifford C, Hopper J. Gies G. Socioeconomic status and cancer mortality and incidence in Melbourne. Eur J C a m . In press.
9. McMichaeI AJ. Social class (as estimated by occupational prestige) and mortality in Australian males in the 1970s. Com- munity Health Stud 1985; 9: 220-30.
10. United States Department of Health and Human Services. The health benefits of smoking cessation. Rockville, MA: US Department of Health and Human Services, Public Health Service, 1990.
11 . United States Department of Health and Human Services. Reducing the health consequences of smoking: 25 years of progress. A repolt ofthe Surgeon General. Rockville, MA: US Department of Health and Human Services, 1989.
39(48): 875-83.
1988; 48: 751-6.
AUSTRALIAN JOURNAL OF PUBLIC HEALTH 1991 VOL. 15 NO. 3 247