the homograft - postgraduate medical journalpmj.bmj.com/content/postgradmedj/35/401/131.full.pdfi3i...
TRANSCRIPT

I3I
THE HOMOGRAFTBy G. M. WYBURN, F.R.S.Ed., D.Sc., M.B., F.R.F.P.S.
Department of Anatomy, University of Glasgow
The penalty of the structural specialization,implying the increasing complexity in molecularconfigurations that has given man and mammalstop ranking in the animal order has been thediminution of the powers of tissue repair, and aspecific molecular 'fingerprint' inimical to themolecular patterns of all other organisms.
In simple forms such as hydra, the animal canbe cut into several pieces and each piece willregenerate into what is more or less a neworganism. Crabs, lizards, and salamanders canregrow appendages-limbs and tails-so can thetadpole but not the adult frog, although if thenerve from another limb is transplanted into anamputation stump in a frog a new limb grows, asthough the tissues were subsidized from thereserves of nerve growth potential (Singer, I958).While it is unlikely that such experiments would besuccessful at mammalian level, there is always thehope that whatever the nature of the regenerativefactor it might some day be possible to restore thislost capacity temporarily to mammalian tissuesso that they can replace destroyed limbs andorgans. Meanwhile, in man the skin, nerve fibreand connective tissues generally, including bone,repair the most readily and certain organs-liver,pancreas, salivary gland-can to some extentreplace lost tissue, but there is a limit to ourregenerative power, and extensive tissue losscannot be made good. Thus, inevitably there is along history of attempts to transplant tissues andorgans from one individual to another of the sameand of different species with sporadic claims ofdramatic successes, unfortunately never repeated.This rigid specificity is a characteristic of the adulttissues, and embryonic tissues are more plastic.Larval chimeras can be formed in the frog, forinstance, by grafting together different parts ofdifferent embryos and the composite organismbehaves physiologically as one unit.Loeb devoted his lifework to the study of tissue
transplantation consummated in his book 'TheBiological Basis of Individuality' (1945) andmany of his theories and conclusions expressed inmore modern terms are a good fit to those of today.
However, the real impetus for the attack on thehomograft problem was a wartime by-productwhich has since grown steadily in depth andbreadth. Nevertheless, despite the impressivevolume of work and the contributions of funda-mental biological significance such as 'activelyacquired tolerance,' ' enhancement' and ' radia-tion chimeras' the homograft problem remainsunsolved. The plastic surgeon or clinician stilllooks in vain for ' spare parts' and is little betteroff in this respect than he was before the greatonslaught of research ten or so years ago.The current concept of the homograft reaction
is that of antigen and antibody (Gibson andMedawar, 1943). From time to time variousparts and fractions of the cell have been indictedas the source of the tissue antigen including, in-evitably, the Nucleic acids. It is, however, un-likely that antigenicity resides exclusively in anyone cell substance or structure. DNA and RNAas the templates of the cellular proteins may wellcodify the molecular' fingerprints' that stamp thetissue specificity.The specificity of antigens is a property of the
chemi- al structure of the molecules and most goodantigens are proteins. The specificity of theprotein molecule 'Nature's noblest piece ofarchitecture' depends on the combination andarrangement of the amino acids and their sidegroups in the polypeptide chains. Other chemicalgroupings such as the conjugate combines mayalso provide specific determinants. While thespecificity of a tissue is not a single factor basedon any one particular molecular pattern, it is un-likely that all the varieties of protein found in anyone tissue or organ act as separate antigens. It istrue that antibodies are not rigidly specific for thetissue or organ against which they have beenprepared, but it is known that single antigens canproduce a number of antibodies, some of whichcombine with a substance in another organsimilar to but not identical in structure with thecausal antigen.
In contrast to infection immunity, in homo-logous tissue immunity no circulating antibodies
copyright. on 31 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.401.131 on 1 M
arch 1959. Dow
nloaded from
132 POSTGRADUATE MEDICAL JOURNAL March 1959
can be recovered from the bloodstream, althoughantisera can be prepared against heterologoustissues. In the homograft reaction the antibodiesare formed in special lymphocytes-the plasmacells-initially at any rate found in the regionallymph nodes draining the lymph from the graftedarea (Scothorne and McGregor, 1955) and oneaspect of tissue immunity which has received littleattention is the logistics of the immune reaction.Why, for instance, do the antibody-containingcells converge on the graft site and how do they getthere ? What is the method of attack once theyare in position?Up to the present there have been two main
lines of attack on the homograft problem: (i) theobjective-the prevention of the host reaction tothe homograft which in practice means the pre-vention of antibody formation; (2) the treatmentof the homograft so that it will cease to act as anantigen or in some way be rendered invulnerableto antibody action.
In respect of (i) there are only two procedureswhich have been successful in producing a lastingtolerance to homografts:
(a) The now well-known 'activity acquiredtolerance' following the injection of foreign tissueat or before birth, first demonstrated by ProfessorMedawar and his colleagues (Billingham, Brentand Medawar, 1953; 1956) and since repeated bythem and others in a variety of animals. Whilesuch acquired tolerance is long lasting it is, ofcourse, limited to homografts from the originaldonor or donor strain, and does not provide aworking solution to the homograft problem.A corollary of this kind of immunity with,
however, a different cause and effect, is the muchdiscussed 'enhancement.' The term was firstused to describe the growth of tumour homograftswhich normally regress, after pretreatment of thehost with doses of dead preparations of donortissues (Snell, 1952; Kaliss, 1955). Similar pre-treatment is said to prolong the life of skin andovarian homografts. One suggestion is that thepretreatment induces the formation of a' blocking'substance which will unite with the graft antigensand so prevent tissue antibody formation.
(b) Animals which have been heavily irradiatedso that there is an almost complete destruction ofthe antibody forming cells will survive if injectedwith homologous or heterologous suspensions ofbone marrow or splenic cells (Ford, Hamilton,Barnes and Loutit, 1956). In such radiationchimeras the grafted cells survive, multiply, andrepopulate the bone marrow and lymph nodes, ashas been confirmed by using marker cells dis-tinguished by characteristic chromosomes. Skingrafts from the original donor of the grafted cellswill survive in these radiation chimeras. While
such procedures provide a rather desperate remedyfor the late stages of leukaemia or severe radiationdisease, like acquired tolerance they are of littlepractical value in the homograft problem.An interesting observation arising from such
experiments is the onset of secondary diseasecausing the death of a proportion of the radiationchimeras within 20 to 20o days after the initialtreatment. Evidence is accumulating that thissecondary disease is due to antibody formationby the donor tissue against recipient antigens(Barnes, Ford, Ilbery and Loutit, 1958) and todaythis antigen antibody reaction in reverse is attract-ing the attention of the pathologist.Another method of treating the host which can
claim to prolong the survival of homografts, is theadministration of cortisone (Billingham, Krohnand Medawar, I95I). In the opinion of Scothorne(1956) cortisone acts by reducing the effectiveantigenicity of the homograft, although how this isaccomplished is not known.
Pre-treatment of GraftsThe aim of such treatment is to destroy the
antigens while retaining the viability of the graft,and this poses the question' Is tissue antigenicity abuilt-in component of the living molecules of adultmammalian tissue which can only be neutralizedby denaturation and so precluding any pos-sibility of processing non-antigenic viable tissueout of normally antigenic substance ?' Whileof the many methods of pretreatment of grafts,freezing, culturing in vitro, and membrane pro-tection merit mention, none of them has offeredto the replacement surgeon a promise of lastingand successful homografts.Freezing
Polge, Smith and Parkes (I949), first describedthe protective properties of glycerol against thebiological effects of low temperature, in particularthe control of ice crystallization, and so introducedan ideal method for the long term preservation oftissues. The preservation, unfortunately, alsoapplies to the tissue antigens of a treated homo-graft, and although, for instance, frozen gonadalhomografts may take and function for varyingperiods of time, there is no suggestion that theimmunological reaction evoked by the homograftis decreased by freezing it (Parkes, 1957). Thesame is true for frozen skin homografts.Tissue CultureLiver cells lose most of their enzymatic activityafter prolonged culture, possibly from lack of
substrate. Theoretically, therefore, there is theargument that isolated from all humoral in-fluences even the nucleic acids might shed some of
copyright. on 31 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.401.131 on 1 M
arch 1959. Dow
nloaded from
March 1959 WYBURN: The Homograft 33
their finer shades of specificity to the extent ofproducing a neutral brand of protein molecule.If this were so, it would then be possible to havelarge scale synthetic plants producing culturedgrafts of wanted tissues and organs. An effort hasin fact been made to acclimatize host and homo-graft by growing the necessary tissue in culturemedium to which has been added the serum fromthe prospective host. This has been done, forexample, with the parathyroids (Galliard, I954).Similarly, the endocrines of infantile rats-thyroids, parathyroids, adrenals-have been ex-planted for periods of three or four months andthen grafted into adult rats from which the cor-responding gland has been removed. There iscertainly evidence of an increased survival periodduring which such grafts appear to function, andthyroid grafts for example take up radioactiveiodine, indicating they are elaborating theirsecretion. Although there are interesting pos-sibilities in this type of experiment, on the wholethe results have been equivocal and it cannot besaid that tissue culture has provided the solutionto the homograft problem. One of the moredramatic tissue culture experiments recentlyreported was the combination of the kidney cellsof the mouse and the chicken to form a chimerakidney capable, it was said, of partial function.
Recent experiments (Algire, Weaver and Prehn,I957) have shown that homograft tissue can beprotected from host reaction if enclosed inMillipore filters with a porosity small enough toprevent transport of cells, but large enough to letthrough protein molecules. Such homograftssurvive in immune as well as non-immune hosts,indicating that they are protected against hostantibodies, and according to Woodruff (i957) arenot effectively antigenic. Such protected graftsare useful biological tools, but as they arenourished by diffusion only, they are of limitedpractical application.Leob (I945) emphasised the variation in the
behaviour of tissues and organs as homografts withregard to survival time and the histological andfunctional history of the graft. Through thework of Medawar, Billingham and their colleagues(I956), there is a very complete record of allaspects of the skin homograft, and to this has beenadded details of histochemical analyses, revas-cularization, and lymphatic regeneration (Scot-horne, I953a, I953b, I958) and re-innervation(Hutchison, Tough and Wyburn, I949; Adeymoand Wyburn, 1957).The position with regard to the long term
survival of homocrafts of endocrine glands is byno means clear (Rob, I954). In a recent report,Coupland (I958) claims a Ioo per cent. survival ofsix-months-old intraocular homografts of chro-
maffin and cortical adrenal cells. More long-termgenetically controlled studies of endocrine graftsare required to provide sufficient data for a finalverdict in respect of the different glands. Atpresent it can be said that there is evidence, as faras the endocrines are concerned, that the homo-graft reaction is a variable factor determined by thespecies of animal used as donor and host, and thephysiological conditions at the time of grafting.Within the scope of one article it is only possible
to deal in detail with the behaviour of a few kindsof homograft and subsequent remarks will beconfined to those on which personal observationsare available, namely cartilage, cornea, bone, andnerve.While there may be some difference of opinion
about the details of the histological fate of cartilageand corneal homografts, there is complete agree-ment that they are clinically a success and able tosurvive permanently as a functioning replacementof the relevant host tissue. They share a commondenominator of cause and effect-an abundantground substance of mucopolysaccharides andavascularity.There is now ample evidence that cartilage
homografts survive, probably permanently, bothin man and in animals. This has been confirmedin man by Gibson, Davis and Curran (1958), whoreport the survival of human cartilage implantsremoved at intervals of from two weeks to twoyears and examined histologically and tested forviability by the uptake of 36S in vitro. Theirmaterial also includes 22-year-old cartilage graftinserted by Sir Harold Gillies. Craigmyle (I955,1958) confirms long-term survival up to two yearsin rabbits (a relatively large proportion of therabbit life span). Bacsich and Wyburn (I947,1956) investigated the histology of short-termcartilage homografts in the guinea pig (up to threeweeks) and found no evidence of any degenerativechange either in the cells or the matrix. In thesestudies the host animals were given injections of35S, and autoradiographed sections of three-weeks-old grafts showed a normal cellular uptake of theisotope. We feel convinced that the survival ofcartilage and corneal homografts is an attribute ofthe mucoproteins of their ground substance.The major constituent of the cartilage matrix isthe mucopolysaccharide-chondroitin sulphate.The uptake of 3S by healthy cartilagenous cellsindicates an active turnover with a continuouscycle of break down and formation of chondroitinsulphate. This cycle presumably involves adepolymerization of high-grade molecules and thepossible diffusion of the degraded non-antigenicmolecules into the host tissue. The depoly-merization also liberates chondrosamine which ismade available for the nutrition of the tissues.
copyright. on 31 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.401.131 on 1 M
arch 1959. Dow
nloaded from
134 POSTGRADUATE MEDICAL JOURNAL March 1959
Is the survival of these homografts merely becausea successful' take ' is not vascularized ? Does theground substance simply act like the Milliporemembrane as a barrier to the penetration of anti-body-containing cells ? Are cartilage homograftsin virtue of their ground substance non-antigenic ?Heterografts, although avascular, are destroyed bythe immune reaction. Moreover, Craigmyle(I956) found that whereas there was considerableincrease in the weight of regional lymph nodeswith heterografts there was no significant changewith homografts, indicating the absence of anantigenic stimulus. In the large number ofcartilagenous homografts of all ages which we haveexamined over a number of years, there has neverbeen any evidence of the host reaction in the formof the aggregation of lymphocytes around the graft,to be expected with the formation of antibody.The conclusion from present available evidence isthus that cartilage does not in fact exite a homo-graft reaction. It has been stated that it is theimmunologically inert ground substance thatconfers survival value on cartilage homografts,and that deprived of this protection the cartilagecells die. We have found, however (Bacsich andWyburn, I955), that growing cartilage with a highcell content and little ground substance not onlysurvives but shows active cell proliferation anddeposition of ground substance. This is inter-preted to imply that it is the active production ofthe mucopolysaccharides by the cells which givesprotection against or prevents host reaction, ratherthan the quantitative characteristics of the tissue,although little is known concerning the chemicalmechanism of this intracellular process. Nor dowe know very much about the life span of normalchondrocytes, whether they are renewed from timeto time, or last throughout the life of the cartilage,but it seems improbable that the graft chondrocytescould synthetise a chondroitin sulphate antigenicto the host tissue. In this respect it can thereforebe argued that if there is' replacement' it is not byhost tissue, but by material elaborated by the nativecells of the graft. There is some clinical evidenceof the protective nature of the mucoproteins andtheir influence on both the local and general hostreactions to living foreign elements. In 1936,Nungster, Jourdonais, and Wolf reported that thesimultaneous injection of gastric mucin andbacteria of low virulence into the peritoneal cavityincreased the virulence of meninococci, strepto-cocci, and staphylococci, by in some way or otheraffording them protection from the host reaction,and again there is the well known increased fatalityrate associated with the presence of circulatingcapsular polysaccharides in the blood of patientswith pneumococcal pneumonia.
Cartilage autografts are not readily available, so
an important practical point is the storage andpreservation of homograft material. Unfortu-nately, glycerol does not protect cartilage from thelethal effects of freezing (Wyburn and Bacsich,1956; Curran and Gibson, 1956; Alexander,1957). According to Smith (I954) ' the optimumrate of cooling for preserving the viability of anycell depends on conflicting factors. The occur-rence of thermal shock must be avoided withoutcooling so slowly as to prolong the harmful effectsof concentrated salt solutions during the separationof ice, or to allow the coagulation and loss ofsolubility of colloidal substances or any other formof intracellular disorganisation.' There is acritical range of temperature in which this harmfulaction occurs. If cells remain more than a fewseconds within this critical range they are irre-versibly damaged (Lovelock, 1953). The pro-tective action of glycerol in freezing is due to anarrowing of this range of critical temperature(Lovelock, I954). The eutectic temperature forthe mixture of salts and other substances withinthe cells determines the lower limit of the criticalrange for any tissue. Obviously, the final storagetemperature must lie beyond the critical zone.There are differences of opinion about the histo-
logical progress of the corneal homograft, but aunanimous verdict concerning its clinical successunder proper conditions. Its behaviour as anorthotopic homograft is therefore quite differentfrom the skin homograft and whether, as is main-tained by Maumenee (I953) its epithelium isfinally replaced by host epithelium or not, asuccessful' take ' does not slough off leaving a rawarea as it would if a homograft reaction wereelicited with antibody-containing cells marshalledto the graft site and the invasion of its substance.It would be surprising if a delicate operation likecorneal grafting, often dealing with unhealthyrecipient tissue, could mark up Ioo per cent.successes. The argument that, because of the in-evitable odd failure or delayed clouding of a graft,corneal tissue is therefore antigenic surely qualifiesas post hoc ergo propter hoc (Nelken Michaelsonand Gurevitch, I958). Again, the plea that theavascularity of the clinical corneal graft is re-sponsible for the absence of any homograft re-action is not valid. Intraocular grafts and hetero-logous corneal grafts readily become vascularizedMoreover, according to Craigmyle a subcutaneouscorneal graft elicits no response from the regionallymph nodes.
If the clinical success of the corneal homograftwere merely a fortuitous result of place and cir-cumstance, heterotopic grafts of whole cornea, notjust the epithelium, should be destroyed.Our personal observations have been made on a
large series of subcutaneous corneal homografts
copyright. on 31 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.401.131 on 1 M
arch 1959. Dow
nloaded from

March 1959 WYBURN: The Homograft 35
l l-- - - --- --
........ ..... ..
.···:I·'1'·srleslaaeamsEaa·~
:·. 5..^j:';, :!:..}E*·:e..i..:.i. .j :... ;:;:·fi:i
-i;i;ii-::-'--. ........ -- - .. Ui - ,. ,,,,,, .,
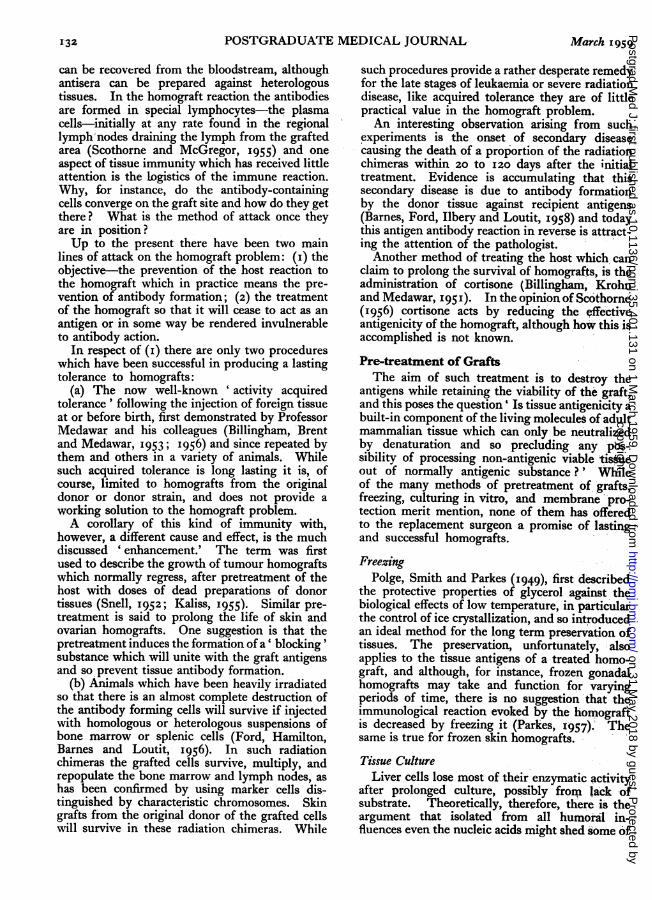
FIG. i.-A 21-day-old cystic corneal homograft. x i8.TEXT FIG. i.-After Sobel.
NiN''...::"
......
:4' ....
FIG. 2.-A 2I-day-old cystic corneal homograft showingepithelium and ground substance. x 135.
in the guinea pig, examined histologically, andtested for viability by the uptake of 35S from thehost at intervals ranging from three weeks to fivemonths (Bacsich and Wyburn, I955, I957). Theexperiments also included examination of secondsets of corneal grafts from the same donor.Healthy viable grafts were recovered up to threemonths. After three months most of the graftswere absorbed, as indeed may happen to manysoft tissue non-glandular autografts. The majorityof the recovered grafts formed inverted cysts witha lining of intact corneal epithelium, Figs. I and 2).In the non-cystic grafts the epithelium had disap-peared by three weeks, but there was no evidenceof host reaction, and the ground substance wasnormal and viable. Cystic formation does not byitself confer protection from a host reaction, as thebehaviour of skin homografts which form cystswhen implanted subcutaneously is identical withthat of orthotopic controls and after three weeks theepithelium has degenerated. The behaviour ofthe second set of homografts was no different fromthat of the first set, with no evidence of donor
i.
· .".!:;:%?:.. '. ? '1
..'E ~ '.- 2·:i·:i·
':'::
di%Ei'i':::i·::'..:::.:::~i~i::i.~~..~~~~. "::,iI%l~~!il;~:.::? alW%x~''~.ii:::iii?'~"~;.::':~i:<~ii ·:"~'?' ·i;lii"<' '~ . ,:~-~~~
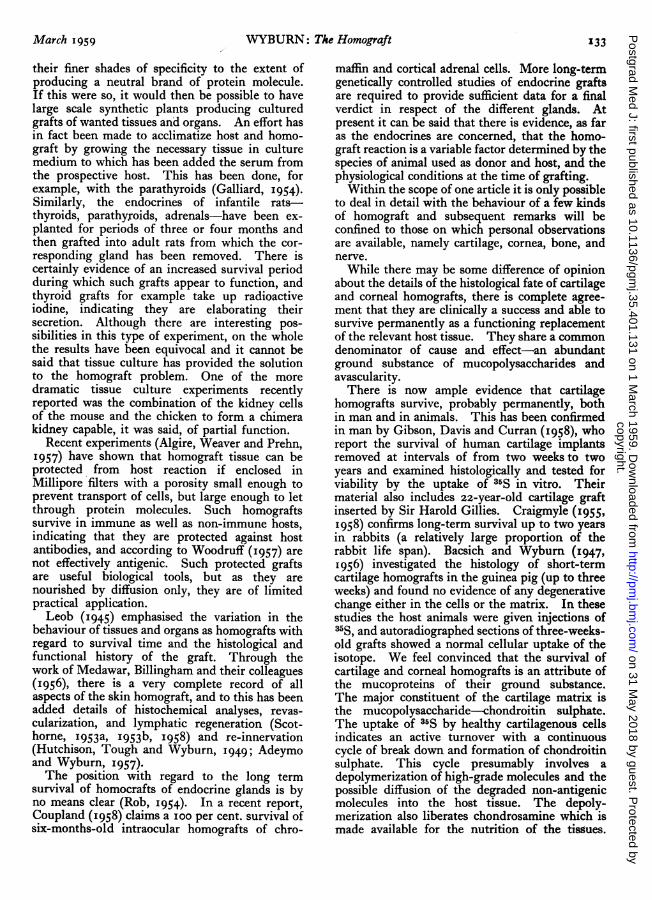
FIG. 3.-A 21-day-old second-set cystic cornealhomograft. x i8.
L. .. . .*.:r· *·:·---·"·--·*:::~·*:
:;::";:.........iiii·-:l~:i:
. 1H: "'2.'iiiil~tiii;i
::": iiliiiii&t8-i:il;tii
L .s·7:i1-:'
FIG. 4.-A 21-day-old cystic second-set cystic cornealhomograft showing epithelium and ground sub-stance. x 135.
recipient reaction, Figs. 3 and 4. The muco-polysaccharides which form the bulk of the groundsubstance of cornea and cartilage have a low pro-tein content and are predominantly carbohydrates.Antigenicity is not a 'sine qua non' of all thegiant molecules of living substance. It is not un-reasonable to suppose that the carbohydratepolymers are not individually specific, and theyare in sufficient quantity in these tissues to conferneutrality.As with cartilage, the question of the preserva-
tion of the cornea and an available ' bank' ofmaterial is of importance. Rob and Eastcott (I954)had successful corneal homografts with glycerol-treated material stored at -79°C. for a perfod oimonths. The fact that such grafts remain trans-luscent is evidence of their viability, and this wasfurther confirmed by the uptake of 35S from thehost by grafts previously stored in this way(Bacsich and Wyburn, 1954). On the other hand,
Cl
copyright. on 31 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.401.131 on 1 M
arch 1959. Dow
nloaded from
136 POSTGRADUATE MEDICAL JOURNAL March x959
grafts stored by freeze-drying do not survive(Bacsich and Wyburn, I954).The purpose of a nerve graft is not to provide a
functioning replacement, but a tissue bridge forthe regenerating nerve fibres to cross from thecentral to the peripheral stump. What is asked ofa homograft is that it should remain viable untilthe crossing is complete. Once the gap is bridgedby the regenerating fibres the support of the grafttissue appears to be no longer essential. Sheathcells can spread from the central stump and thehost connective tissue elements replace the fibrousframework of the reconstituted nerve. Nervehomografts are equal to this limited task inrabbits (Sanders and Young, I942) and in cats(Bentley and Hill, 1936), but despite a spate ofexperimental work during and immediately afterthe recent war, there is no reliable report of asuccessful human nerve homograft. Perhaps be-cause of this dismal record there is today only atrickle of work on nerve grafts, and yet it shouldnot be an insuperable problem to keep the homo-graft alive for a limited time. The explanationthat the failure of the human nerve homograft ismerely a question of relative size-a larger gap, alonger homograft, more difficult to vascularize,and a greater length of regenerating nerve fibres-is not wholly satisfactory. Quite large humannerve autografts ' take' and are repopulated withregenerating fibres (Barnes, Bacsich and Wyburn,1945a). The tempo of events in an organism isgenerally geared to the dimensions of the task inspace and time, and it is thus doubtful if it isaltogether justified to assume that the rate of re-generation of nerve fibres is the same for man andthe rabbit.
In all the human nerve homografts which havebeen examined histologically, the regeneratingfibres have penetrated some distance into thegraft which here retains the structural frameworkof a nerve. It has been suggested (Sanders, 1954)that the length of graft innervated is correlated tothe total size of the graft, indicating a dosage effect-the longer the graft the bigger the antigen doseand so the more rapid the onset of the immunereaction. Out of a series of eight nerve homo-grafts, three of which were examined histologi-cally (Barnes, Bacsich, Wyburn and Kerr, i945b),the proportions were-25 mm. in i8-cm. graft,12 mm. in a 9-cm. graft, and I5 mm. in a 7-cm.graft. There are likely to be many variables inindividual host reactions, the most significant thegenetic rather than the size factor. It is agreed thatthere is complete replacement of graft by hosttissue elements, but what is interesting is that thestructural architecture of the non-innervated partof the graft is retained for a long time. In ourseries, the fibrous framework of a typical nerve
was recognizable after a year, although some of thebundles had a necrotic centre and others werepartially filled with a cellular connective tissue.After 955 days there was no longer any fascicularorganization, only a homogeneous fibrous mass.Obviously a ' ghost ' skeleton of the graft survivedthe immediate homograft reaction and organizedthe replacing host connective tissue in the firstinstance. One incidental observation emergingfrom nerve-graft work is the latent regenerativecapacity of neurons. In our series, fibres re-generated from the central stump after two years.Presumably, isolation from peripheral or muscularconnection does not necessarily mean the death ofthe neuron, and the viable nerve cell can alwaysregenerate its processes. In what way the mechani-cal stimulus of freshening a central stump stirs upthe distant nerve cell is not known.There is, obviously, worthwhile work still to be
done in nerve homografts, particularly in respectof the pre-treatment of the graft.The bone homograft, whether implanted into
bone, muscle, or intraocularly, dies and can be re-covered as a sequestrum up to a year or later. Thebehaviour of the bone graft is unique in two ways.The graft never takes. Examined within a fewdays the cortical lacunae are empty both in auto-grafts and homografts, but in the homograft thereis no sign of living bone cells, whereas in the auto-graft there are living bone cells subperiosteally andlining haversian canals and marrow spaces(Hutchison, I952). By 14 days these cells areactive in new bone formation, while the homograftis a sequestrum. Secondly, bone is the only trans-plant which as autograft or homograft can inducethe host tissue to reproduce the grafted tissue.Host osteogenesis commences about io days afteran implant of homogeneous bone into muscle andceases, in rabbits at any rate, after 42 days. Inorle experiment when the bone homograft wasextruded after three days there was new host boneat the graft site examined two weeks later (Wyburnand Bacsich, 1956). The use of the bone graft,autograft or homograft, is mainly as a stimulus tonew bone formation by the host tissues, andmaybe in future the answer to bone loss and repairwill not be the bone graft, but the local inductionof new bone formation. As previously noted(Wyburn, 1957), certain general conclusions aboutthe induction of host osteogenesis by bone homo-grafts can be stated:
(I) The inductive factor or factors is not specificas it is effective although delayed in homogeneoustransplants;
(2) Induction is not exclusively the function ofbone cells, as the cells of homogeneous grafts dieand, moreover, host osteogenesis has been re-
copyright. on 31 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.401.131 on 1 M
arch 1959. Dow
nloaded from
March 1959 WYBURN: The Homograft 137
-ported with frozen grafts after an interval of 30days;
(3) The more immediate and greater inductiveresponse to fresh autogenous grafts suggests aquantitative or qualitative difference in inductivecapacity, probably related to the presence ofliving osteoblasts.
There are, as is well known, many conditions,experimental, pathological, other than bone graft-ing that can induce osteogenesis not only in bonebut in the soft tissues. Over the years there havebeen a great many theories as to the nature of theosteogenetic stimulus and we still await the rightone.
In this connection, recent work by Sobel (I955)gives promise of a new starting point for anexperimental approach to osteogenesis. Sobelused the technique of reversible in vitro calcifica-tion to demonstrate that the first step in mineraliza-tion is the combination of Ca++ with someconstituent in the calcifiable tissue. He showedthat other ions (e.g. strontium) can compete withthe calcium ions in the calcifying fluid, and bycombining reversibly with this substance canprevent calcification, i.e. can inactivate the tissue.Re-activation of the calcifiable tissue is a functionof the ratio of activator to inactivator ions, TextFig. i. The mineral element of bone, smallcrystals of hydroxyapatite a few hundred Angstromunits in length are first deposited in ossifying tissuearound the repeating bands of the collagen fibres.There is some evidence that the mucopolysac-charide, chondroitin sulphate, is an integral partof the calcifying mechanism. Sulphur-containingmucopolysaccharides appear wherever calcificationoccurs in normal or abnormal situations. Calci-fication in vitro of rachitic cartilage is inhibited bytoluidine blue which competes with Ca++ in thesame way as inactivator ions, and so in this case aspecific target-the chondroitin sulphate can beassumed to be the calcifying factor. Moreover,Ca++ up to a certain concentration causes achange in the polymerization of the chondroitinsulphate complex so that metachromatically itbecomes more active.
Sobel suggests that the significant event in theformation of a calcifiable tissue is an alteredpolymerization which promotes a complex ofchondroitin sulphate with collagen in a criticalconfiguration. Given the necessary calcium andphosphate ions in the circulating fluids, thiscomplex acts as a template and provides a possiblemechanism for the epitactic (seeding) growth ofbone crystals. The next step is to experiment withcomplexes obtained by condensing chondroitinsulphate from different varieties of collagen and totest them for mineralization by the method ofin vitro calcification.
It may be that with the homograft problem, aswith the problem of malignant disease, or with thestill more intractable enigma, the translation ofnerve impulses into conscious sensations, we havereached a barrier and require a new set of conceptsbefore we can break through, just as Pasteur'smicrobes, Miiller's mutations, and the physicist'snon-conservation of parity have in their turnbroken through to new frontiers. The lessons ofhistory encourage the conviction that sooner orlater the homografter will achieve his break-through to a successful solution of the problem-asuccess that will rank along with insulin andpenicillin as one of the great advances in medicine.
BIBLIOGRAPHYADEYMO, O., and WYBURN, G. M. (I957), Trans. Bull., 4, 152.ALEXANDER, S. (1957), Brit. J. plast. Surg., o1, I, 36.ALGIRE, G. H., WEAVER, J. M., and PREHN, R. T. (1957),
Ann. N.Y. Acad. Sci., 64, IOO9.BACSICH, P., and WYBURN, G. M. (1947), Proc. roy. Soc.
Edinb. B, 72, 321.BACSICH, P., and WYBURN, G. M. (1954), Trans. Bull., i, 5, I99.BACSICH, P., and WYBURN, G. M. (I955), Ibid., 2, 2, 44.BACSICH, P., and WYBURN, G. M. (i955), Ibid., 2, 4, 144.BARNES, R., BACSICH, P., and WYBURN, G. M. (1945a),
Brit. J. Surg., 32, 130.BARNES, R., BACSICH, P., WYBURN, G. M., and KERR, A. S.
(I945b), Ibid., 34, 34.BARNES, D. W. H., FORD, C. E., ILBERY, G. L. T., and
LOUTIT, J. F. (1958), Trans. Bull., 53, lor.BENTLEY, F. H., and HILL, M. (I936), Brit. J. Surg., 24, 368.BILLINGHAM, R. E., KROHN, P. L., and MEDAWAR, P. B.
(1951), Brit. med. J., i, 1157.BILLINGHAM, R. E., BRENT, L., and MEDAWAR, P. B. (1953),
Nature (Lond.), 172, 603.BILLINGHAM, R. E., BRENT, L., and MEDAWAR, P. B. (1956),
Philos. Trans. B, 666, 239.COUPLAND, R. E. (1957), J. Endocr., 15, 2, i62.CRAIGMYLE, M. B. L. (I955), Brit. J. plast. Surg., 8, 2, 93.CRAIGMYLE, M. B. L. (I958a), J. Anat. (Lond.), 92, 174.CRAIGMYLE, M. B. L. (1958b), Ibid., 92, 346.CURRAN, R. C., and GIBSON, T. (1956), Proc. roy. Soc. B, x44,
572.FORD, C. E., HAMILTON, J. L., BARNES, D. W. H., and
LOUTIT, J. F. (I956), Nature (Lond.), 177, 452.GALLIARD, P. J. (I954), Ciba Foundation Symposium, 'The
Preservation and Transplantation of Normal Tissues,' J. & A.Churchill, London, p. o00.
GIBSON, T., and MEDAWAR, P. B. (I943), J. Anat. (Lond.),77, 299.
GIBSON, T., DAVIS, W. B., and CURRAN, R. C. (1958),Brit. J. plast. Surg., II, 3, I77.
HUTCHISON, J., TOUGH, J. S., and WYBURN, G. M. (I949),Ibid., 2, 82.
HUTCHISON, J. (1952), Ibid., 39, 158, 2.KALISS, N. (I955), Ann. N.Y. Acad. Sci., 59, 385.LOEB, L. (I94S), 'The Biological Basis of Individuality,'
C. Thomas, Baltimore.LOVELOCK, J. W. (I953), Biochim. biophys. Acta.LOVELOCK, J. W. (I954), 'In Preservation and Transplantation
of Normal Tissues,' Ciba Foundation Symposium, J. & A.Churchill, London.
MAUMENEE, A. E. (1953), Trans. Bull., I, II7.NELKEN, E., MICHAELSON, I. C., and GUREVITCH (I958),
Ibid., 5, I, 9.NUNGSTER, W. J., JOURDONAIS, L. F., and WOLF, A. H.
(1936), J. infect. Dis., 59, 2.PARKES, A. S. (1957), 'A Discussion on Viabilitv of Mammalian
Cells and Tissues after Freezing,' Proc. roy. Soc. B, 147, 520.POLGE, C., SMITH, A. U., and PARKES, A. S. (1949), Nature
(Lond.), I64, 666.ROB, C. (1954), Lancet, August 7, 255.ROB, C., and EASTCOTT, H. H. G. (I954), Ciba Foundation
Svmposium,' The Preservation and Transplantation of NormalTissues, J. & A. Churchill, London, p. I90.
Bibliography continued on page 155
copyright. on 31 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.401.131 on 1 M
arch 1959. Dow
nloaded from

March 1959 PROBERT: Traumatic Diaphragmatic Hernia 155The literature contains many reports of cases in
which a symptom-free interval between injury andstrangulation of a traumatic diaphragmatic herniacan be measured in months. The latent period inthis case was over 33 years. Mild bowel symptomsculminating in acute intestinal obstruction sug-gested a diagnosis of carcinoma of the colon. Thecorrect diagnosis was not made because the smallscars on the chest wall were not deemed relevant;because the shadow of the metallic fragment inthe abdominal radiograph was likewise disre-garded; and because the original injury was lookedupon as an unimportant fact of remote history.SummaryA case of traumatic herniation of the left hemi-
diaphragm due to penetrating injury is described.
Following wounding in I918 there was a longinterval without symptoms.
Acute obstruction of the colon developed 331years later preceded only by a few months of mildpremonitory symptoms.Acknowledgments
I wish to thank Mr. Ralph H. Gardiner forpermission to report this case, and the ChiefMedical Officer of the Ministry of Pensions forconfirmation of essential dates and for permissionfor publication.
BIBLIOGRAPHYBELCHER, J. R. (1956), personal communication.CARTER, B. N., and GIUSEFFI, J. (1948), Ann. Surg., 128, 210.HAVARD, C., and PROBERT, W. R., to be published.WINDSOR, H. M. (I957), Brit. med. J., i, I344.
Bibliography continuedfrom page 137-The Homograft, C. M. WyburnSANDERS, F. K., and YOUNG, J. Z. (1942), J. Anat. (Lond.),
76, I43.SANDERS, F. K. (1954), 'Preservation and Transplantation of
Normal Tissues,' Ciba Foundation Symposium, J. & A.Churchill, London.
SCOTHORNE, R. J., and TOUGH, J. S. (1952), Brit. J. plast.Surg., 5, i6I.
SCOTHORNE, R. J., and McGREGOR, I. A. (19S3), J. Anat.(Lond.), 87, 379.
SCOTHORNE, R. J., and McGREGOR, I. A. (1955), Ibid., 89, 283.SCOTHORNE, R. J. (1956), Ibid., 93, 4I7.
SCOTHORNE, R. J. (1958), Ann. N.Y. Acad. Sci., 73, 673.SINGER, M. (1958), Sci. Amer., 199, 4, 79.SNELL, J. D. (1952), Cancer Res., 12, 543.SOBEL, A. E. (1955), Ann. N.Y. Acad. Sci., 60, 713.WYBURN, G. M., and BACSICH, P. (1955), Brit. J. plast. Surg.,8, I77.WYBURN, G. M., and BACSICH, P. (I956a), Trans. Bull., 3, I, 3.WYBURN, G. M., and BACSICH, P. (I9g6b), Ibid., 3, 3, 79.WYBURN, G. M. (1957), J. roy. Coll. Surg. (Edin.), 2i 3I5.WOODRUFF, M. F. A. (1957), Ann. N.Y. Acad. Sci., 64, 1014.
THE NEUROLOGIC EXAMINATIONRUSSELL N. DEJONG
Professor of Neurology, University of Michigan Medical SchoolThe second edition of a Well-knoWn Work,completely revised in the light of modernresearch, clinical experience and methods oftherapy. The book is a complete coverage ofthe structure and functioning of the normal aswell as the diseased nervous system.
1096 pages 300 illus. £7 0 0 net
ILLUSTRATED PRE-OPERATIVE ANDPOST-OPERATIVE CARE
PHILIP THOREK, M.D., F.A.C.S., F.I.C.S.Drawings by CARL LINDEN
A clear, concise and dogmatic little book. Ofthe previous book by Thorek and Linden,Surgical Diagnosis, the B.M.J. said "The authorhas a quite exceptional power of compressingall the essentials of description in the briefestpossible space; the artist has an equal power... It is a very rare and happy combination."
100 pages 60 illus. 30s. net
PITMAN MEDICAL PUBLISHING Co. Ltd.39 PARKER STREET, LONDON, W.C.2
RECENTLY PUBLISHED
Modern TreatmentYearbook 1959.
Edited bySIR CECIL WAKELEY, Bt., K.B.E., C.B., LL.D., M.Ch.,D.Sc., F.R.C.S., F.R.S.E., F.R.S.A., F.A.C.S., F.R.A.C.S.
Specially written to keep the general practitionerinformed on the latest therapeutic methods and onthe practical applications of the latest research.Thirty-one articles on many of the conditionscommonly encountered by general practitioners intheir daily work, with the accepted methods ofdiagnosis and treatment, each thoroughly testedand the result of hospital experience.25th issue 320 pages. 16 plates and manyother illustrations. 30s. Postage ls. 9d.
Publishedfor the Medical Press by
BAILLIERE, TINDALL & COX7 & 8 Henrietta Street, London W.C.2
copyright. on 31 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.401.131 on 1 M
arch 1959. Dow
nloaded from