the dyspnea-anxiety-dyspnea cycle—copd patients’ stories of breathlessness: “it’s scary...
TRANSCRIPT

10.1177/1049732304265973QUALITATIVE HEALTH RESEARCH / July 2004Bailey / DYSPNEA-ANXIETY-DYSPNEACYCLE
The Dyspnea-Anxiety-Dyspnea Cycle—COPD Patients’ Stories of Breathlessness:“It’s Scary /When You Can’t Breathe”
Patricia Hill Bailey
Dyspnea, the major symptom associated with acute exacerbation events of chronic obstruc-tive pulmonary disease (COPD), is a subjective experience. Extensive research has beendone on the pathophysiology and affective components of dyspnea; however, the precisephysical mechanism of breathlessness remains elusive. One purpose of this narrativeresearch was to explore the affective component of dyspnea/anxiety as described by patientsliving with COPD characterized by acute illness events. Ten patient-family units partici-pated in interviews during an acute episode of the patient’s lung disease. They describedtheir understanding of acute dyspnea as an experience inextricably related to anxiety andemotional functioning. Their stories suggest that given the absence of clear objective mea-sures of illness severity, patient-reported anxiety might provide an important marker duringacute exacerbation events. Health care providers need to recognize anxiety as an importantand potentially measurable sign of invisible dyspnea for end-stage patients with COPD inacute respiratory distress.
Keywords: dyspnea; anxiety; COPD, AECOPD; narrative analysis; ethnography;discourse analysis
As chronic obstructive pulmonary disease (COPD) progresses, many individu-als experience frequent acute exacerbations of incapacitating dyspnea requir-
ing emergency admission to hospital (Anthonisen et al., 1987; Black & Curtis, 2001;McCory, Brown, Gelfand, & Bach, 2001). Dyspnea, the major symptom associatedwith acute exacerbation events of COPD (AECOPD), is defined as some form of dif-ficult breathing (Carrieri, Janson-Bjerklie, & Jacobs, 1984; Gift, 1990; Lynn et al.,2000; Runo & Ely, 2001; Schwartzstein & Cristiano, 1996; Schwartzstein, Manning,Weiss, & Weinberger, 1990). Dyspnea must not be confused with observed changesin either rate or depth of respiration that might not produce a subjective experienceof breathlessness (Gift, 1990, 1993). Extensive research has been done on thepathophysiological aspects of dyspnea, but to date, the precise physical mechanismof breathlessness is unclear (Adams, 1996; Adams, Lane, Shea, Cockcroft, & Guz,1985; Dahlén & Janson, 2003; Spector & Klein, 2001; Tobin, 1990). However,although the affective contribution to a perception of breathlessness has been
760
AUTHOR’S NOTE: The research project referred to in this article was supported by fellowship grantsfrom the Ontario Respiratory Care Society (a section of the Ontario Lung Association) and the CanadianNurses’ Research Society (a section of the Canadian Lung Association).
QUALITATIVE HEALTH RESEARCH, Vol. 14 No. 6, July 2004 760-778DOI: 10.1177/1049732304265973© 2004 Sage Publications
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from

examined, the nature of its contribution to dyspnea has been elusive (Burns &Howell, 1969; Carrieri-Kohlman, Gormley, Douglas, Paul, & Stulbarg, 1996a; Gift &Cahill, 1990). Does anxiety precipitate dyspnea, or is it the perception of dyspneathat provokes an overwhelming sense of anxiety?
Amid this uncertainty, nurse-researchers have conducted several studies relatedto the affective component of the experience of dyspnea in patients with COPDfocusing on the patient’s control of this perception. Their work has included exami-nation of the experience of dyspnea (DeVito, 1990; Janson-Bjerklie, Carrieri, &Hudes,1986), the relationship between the psychological and physical factors gen-erally associated with dyspnea in Patients with COPD (Gift & Cahill, 1990; Gift &Pugh, 1993; Gift & McCrone, 1993; Gift, Moore, & Soeken, 1992; Gift, Plaut, & Jacox,1986), the presence of depression and the administration of long-term low-dose ste-roid therapy (Gift, Wood, & Cahill, 1989), and the effect of alternate strategies suchas relaxation on the reduction of dyspnea and anxiety in individuals suffering fromCOPD (Carrieri & Janson-Bjerklie, 1986; Carrieri-Kohlman, Douglas, Gormley, &Stulbarg, 1993; Carrieri-Kohlman, Gormley, et al., 1996a, 1996b; Gift, Moore, et al.,1992; McBride, Graydon, Sidani, & Hall, 1999; Renfroe, 1988; Thornby, Haas, &Axen, 1995).
As anticipated, increased levels of anxiety were associated with more severedyspnea (Gift & Cahill, 1990; Gift, Plaut, et al., 1986). Contrary to expectations, norelationship has been found between respiratory rate and dyspnea and/or anxiety,and a relationship between depression and level of difficult breathing was not iden-tified. These researchers, however, suggest that there might be a relationshipbetween the administration of long-term low-dose steroid therapy and an increasein the levels of depression experienced by COPD individuals (Gift, Wood, et al.,1989). Furthermore, these studies have demonstrated that during non-acute phasesof the illness course, the use of alternate strategies can significantly reduce the sen-sation of dyspnea, respiratory rate, and levels of anxiety (Carrieri & Janson-Bjerklie,1986; Carrieri-Kohlman, Douglas, et al., 1993; Carrieri-Kohlman, Gormley, et al.,1996a, 1996b; Gift, Moore, et al., 1992; Renfroe, 1988; Thornby et al., 1995).
It is important to note that although these authors indicated that during non-acute episodes, anxiety contributes to the patient’s perception of increased short-ness of breath, the specific nature of this affective contribution to a perception ofmore or less severe breathlessness continues to remain enigmatic (DeVito, 1990;Killian & Campbell, 1996). In addition, a clear picture of the experience of the acuteevent of severe dyspnea describing the affective component of this experience fromthe perspective of the COPD sufferer and family caregiver is not yet available in theliterature.
The purpose of this research, in part, therefore, was to explore further the affec-tive component of dyspnea, more specifically anxiety, as described by patients andfamily caregivers living with an individual with COPD who have experiencedacute exacerbation events characterized by uncontrollable dyspnea.
METHOD
Between 1995 and 1996, I conducted a research study to develop an understandingof the relationship between anxiety (affective behavior) and the experience ofdyspnea (perception of shortness of breath) during the complex event of an acute
Bailey / DYSPNEA-ANXIETY-DYSPNEA CYCLE 761
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from

exacerbation of chronic obstructive lung disease (Bailey, 1998, 2001; Bailey & Tilley,2002). The study was conducted in Canada, in two general hospitals in anortheastern Ontario mining community of 160,000 people.
I interviewed 10 family-nurse units following the receipt of ethical approval.Over the 4-month period of data collection, the admission clerks in the hospitalemergency departments notified me daily of the admission of individuals with anAECOPD. The charts of all potential patient participants were reviewed within 24hours of their hospitalization to determine whether they met the study inclusioncriteria; that is, they were hospitalized because of an AECOPD characterized byextreme dyspnea, they had experienced at least two previous acute exacerbations ofCOPD necessitating hospitalization, and they had named family members as thenext of kin. I approached individuals who met these criteria and asked them to bepart of the study.
I explained the study aim to each identified patient. I asked patients to desig-nate two family members that had been involved in an acute exacerbation event andhad a commitment to their well-being on an ongoing basis (Gilgun, Daly, & Handel,1992; Johnson, 1998). After obtaining the patient’s informed consent, I asked onenurse who was assigned to the patient’s care on the in-patient unit to participate inthe study. I informed the 10 patients, 10 nurses, and 15 family caregivers who agreedto participate in the study that the information they shared might be published buttheir names would not be associated with the research.
For the purposes of this research, an acute exacerbation event of COPD wasdefined, according to Strauss and colleagues’ (1984) chronic illness model, as amedical crisis of a chronic illness. The interview questions were based on Strauss’smodel: “reading the signs,” “organizing for crisis,” “breakdown of organization:potential and actual,” and “ceding responsibility to the hospital.” Initially, I askedeach participant to talk about the circumstances surrounding the patient’s presentacute exacerbation event.
Narrative Analysis
I used a focused ethnographic research design for the study to uncover meanings ofthese acute events from the perspective of the participants. The main method ofdata collection was in-depth interviews conducted during the patients’ hospitaliza-tion. I used narrative analysis as an extension of ethnographic inquiry to examinethe interview data (Atkinson, 1992; Bailey, 2001; Bailey & Tilley, 2002; Mishler, 1986;Riessman, 1987, 1988, 1989, 1990a, 1990b, 1993, 1994a, 1994b; Wiltshire, 1995). Threegenres of stories were recognized in the stories identified in the interviews of the 10participating patient-family-nurse units. They included first-person event-specificstories, stories that “recreate[s]” a discrete moment in time (Riessman, 1990b,p. 1195); generic or habitual stories (Bennett, 1986; Polanyi, 1985, 1989; Riessman,1991; Schiffin, 1994); also first-person accounts, stories that “tell of the generalcourse of events over time, rather than what happened at a specific point in the past,and are constituted with verb tenses and adverbs that mark repetition androutinization” (Riessman, 1991, p. 53); and, finally, kernel stories (Kalcik, 1975),what Viney and Bousfield (1991) described as “stories-begun-but-not-told,” storyabstracts that suggest untold first-person event-specific personal stories (Connelly& Clandinin, 1990; Kermode, 1981).
762 QUALITATIVE HEALTH RESEARCH / July 2004
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from

I analyzed all three types of stories systematically, within the context of theinterviews, using an analysis strategy developed that I have developed (Bailey,2001; Bailey & Tilley, 2002). This process included a combination of two narrativeanalysis strategies: Labov and Waletzky’s functional model (Labov, 1982; Labov &Waletzky, 1972) and Agar and Hobbs’s (1982, 1983) coherence model. In addition,analysis was informed by attention to discursive and rhetorical aspects of the sto-ries (Antaki, 1994; Bennett, 1986; Gee, 1991; Gee, Michaels, & O’Connor, 1992;Labov, 1982; Labov & Fanshel, 1977; Potter & Wetherell, 1987; Widdicombe, 1993).
I identified 503 stories across the transcribed database. As a first step in a sys-tematic analysis process (Bailey, 1996), I parsed the identified stories into the vari-ous story elements—abstract, orientation, complicating action, resolution, evalua-tion, and coda—as described by Labov and Waletzky (1972). Subsequently, Iidentified story events and meanings from the story elements. Within the interviewcontexts, I examined the stories with similar meanings (evaluation elements) forcontent and structure, and described the story meanings and functions.
VULNERABILITY STORIES
In their conversations about acute exacerbation events, patients and family care-givers in this study told numerous stories that described the relationship betweenacute dyspnea and the patient’s physical and emotional functioning as they livedwith the patient’s chronic lung disease. Stories about the patient’s emotional func-tioning, situations in which the patient and/or family member experienced over-whelming anxiety, were the most frequently told stories across the interviews. Allpatients and all but one family caregiver told stories of emotional functioning. Seg-ments from the 145 stories told by patients and their family caregivers addressingemotional functioning will be highlighted in this article. The stories told by nursesin which they talked about the patient’s anxious behaviors are addressed elsewhere(Bailey, Colella, & Mossey, 2003).
In these stories, patients and family caregivers represented emotional functionas a sense of disability or vulnerability, a vulnerability expressed as anxiety andexperienced during and in anticipation of episodes of increasing or intractablebreathlessness, situations they were unable to avoid or manage effectively. I havecategorized these stories of anxiety or emotional disability as Emotional Vulnerabil-ity Stories describing a dyspnea-anxiety-dyspnea cycle.
In several stories, the relationship between emotional functioning and unusualbreathlessness was unclear. Where the cause of breathlessness was ambiguous, par-ticipants talked of emotional dysfunction as a sign of intractable breathlessness. Inthese stories, patients and family caregivers represented the relationship betweenemotional functioning and breathlessness as both circular and complex. In a num-ber of stories, these participants talked of emotional dysfunction as being a result ofboth chronic breathlessness and increased physical or emotional activity.
It became apparent that the telling of stories of patient anxiety—stories describ-ing the patient’s inability to cope emotionally with everyday experiences because ofintractable breathlessness—functioned to make the subjective invisible experienceof breathlessness visible. This process of giving concrete expression to the dyspneicexperience also functioned to legitimize the illness (physical and emotional disabil-ity) and help-seeking behavior of both the patients and their family caregivers.
Bailey / DYSPNEA-ANXIETY-DYSPNEA CYCLE 763
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from

STORY STRUCTURE AND CONTENT
In the following analysis, vulnerability was understood as the individuals’ (patients’)perceptions of their lessened potential or capacity for interacting with perceivedchallenging or threatening environments (Clarke & Driever, 1983). The conceptual-ization of vulnerability as the innate or acquired capacity to be injured or hurt isdescribed by other nurse-researchers in their work with adolescents (Hogan &DeSantis, 1994), psychiatric patients (Zubin & Spring, 1977), women’s health issues(Steven, Hall, & Meleis, 1992), families (Demi & Warren, 1995), and geriatricpatients (Good & Rodrigues-Fisher, 1993). It is a subjective and invisible experience(Anthony, 1989; Cohler, 1989; Rose & Killien, 1983).
Although the dyspneic behavior described in the vulnerability stories appearsto have different causes (one physical activity, the other emotional distress), the nar-rative phrases share a common structure. Patients and family caregivers usuallyincluded a description of the patient’s experience of dyspnea or its sequellae, theiremotional functional limitations or anxiety, and an account of the resolution of thestory events. The resolution segments commonly included help-seeking behaviorsuch as emergency hospitalization. They talked of their experience of severeemotional disability as a distressing event.
Dyspnea and Emotional Functioning
In emotional vulnerability stories, the relationship between emotional actions anddyspnea was presented as circular. In some stories, unusual emotional reactions toeveryday situations were understood as a sign, or marker, of the onset of unusualbreathlessness. The increasing dyspnea then evoked other emotional reactions and,as a result, more severe breathlessness. In addition, several stories told by both thepatient and family caregiver described everyday circumstances in which emotionalfeelings unwittingly experienced by the patient played a part in the initiation of anacute exacerbation event. The psychological tasks described in these stories includedactivities such as arguing with a relative, getting angry, waiting for a late visitor, get-ting frustrated, or being in a crowd. These normal emotional reactions occasionedan increase in shortness of breath.
Some stories clearly demonstrated that these patients and family caregiverswere aware of the patient’s emotional vulnerability, that is, they recognized emo-tional dysfunction as a part of this chronic illness. Because of their experience of pre-vious episodes of increased breathlessness patients and family caregivers now rec-ognized any increase or change in the patient’s emotional response to an everydayexperience, an unexplained sense of panic, for example, as a sign of potentiallyintractable dyspnea.
The Resolution
Emotional vulnerability stories generally concluded with an acknowledgment ofthe patient’s emotional disability, a decrease in the patient’s activity, an increase inthe patient’s experience of dyspnea, further emotional distress, and/or, often, someform of help-seeking action. The help-seeking behavior described often includedemergency admission to hospital.
764 QUALITATIVE HEALTH RESEARCH / July 2004
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from
MEANING OF EMOTIONAL VULNERABILITY STORIES
The participants presented several analogous explanations across the patients’ andfamily caregivers’ vulnerability stories. The most frequently identified explanationwas to communicate that the patients, because of their chronic lung disease, wereemotionally vulnerable and that acute episodes of breathlessness or the threat ofincreased dyspnea further exacerbated this emotional dysfunction. In these stories,it was clear that patients who were already emotionally disabled were unable toundertake normal physical or emotional activities because of the threat of increasedbreathlessness and its sequellae, or experienced increased emotional dysfunctionduring episodes of increased dyspnea.
These complex circular understandings were included by both patients andfamily caregivers. The participants’ use of rhetorical devices such as repeatedwords and phrases—“gotta,” “he can’t do anything,” “he’ll force himself to do it”—intensifiers—“just,” “even”—and attention to detail—“three or four stairs,” “ablock”—emphasized the degree of functional disability normally experienced bythe patient. These participants also found the circumstances of potentially unman-ageable breathlessness distressing. Indeed, patients concluded their stories by say-ing that the anticipation and experience of such limited functioning because of inca-pacitating dyspnea was emotionally difficult. Their sense of distress was expressedas emotional vulnerability—it was “too hard,” “too much,” “very scary.” They“cannot die/cannot live.”
Family caregivers on the other hand, when recounting stories of the patient’sphysical and emotional vulnerability, concluded their accounts by expressing theirsense of helplessness—“you cannot do nothing,” “you feel sort of helpless”—andfear when present during an episode of acute dyspnea—“it’s it’s scared me,” “youpanic.” They not only found it difficult to watch an acute experience of breathless-ness but also talked about the seriousness of future dyspneic events—their “biggestfear.” Family caregivers suggested through their stories that the patient would ulti-mately die—“choke,” “not gonna make it”—during one of these events.
Finally, in another group of evaluation segments from vulnerability stories,family caregivers talked of their sense of relief and security once they decided toseek help or the patient arrived at the hospital emergency department. On occasion,these participants suggested that the patients shared this sense of relief. This feelingof safety was sometimes coupled with talk of an improvement in the patient’sphysical condition.
VISIBILITY FUNCTION OF EMOTIONALVULNERABILITY STORIES
In the identified stories, emotional dysfunction was often presented either as thevisible expression of the patient’s subjective experience of breathlessness or as thesequella of unusual dyspnea. In stories of emotional vulnerability, patients werepresented as individuals who normally could not express common emotions(anger, sadness, fear, frustration) without either precipitating breathlessness orexacerbating already existing dyspnea potentially to the point of physical collapse.The representation of breathlessness as emotional disability made this subjective,
Bailey / DYSPNEA-ANXIETY-DYSPNEA CYCLE 765
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from

invisible experience visible. When participants talked of patients’ panic behavior orinappropriate tears, they provided concrete images of the reality of invisibledyspnea.
THE LEGITIMIZATION FUNCTION OFEMOTIONAL VULNERABILITY STORIES
Such vulnerability stories give the subjective experience of breathlessness an inter-pretable form. In their stories, patients measured the seriousness of their dyspneaconcretely, by how they felt and by what they were able to do. Patients and familycaregivers communicated how they understood unmanageable breathlessness;emotional dysfunction and anxiety were part of their experience of living withchronic lung disease characterized by acute exacerbation events. By giving dyspneaa visible form, they also inherently legitimized the patients’ complaints of this invis-ible experience (feeling short of breath) and their help-seeking behavior. Breathless-ness concretely represented as emotional dysfunction and vulnerability, that is,anxiety, functioned to legitimize the experience of dyspnea.
I now present one patient’s accounts of three emotional vulnerability stories.Like other participants in the study, Paul (pseudonym) recounted Emotional Vul-nerability Stories and described his understanding of acute dyspnea as being anexperience inextricably related to emotional functioning. His narratives demon-strate the identification of vulnerability stories and explicate the analytical utility ofthese vulnerability story structures in interpreting the participants’ understandingof acute exacerbation events. Most important, these examples illustrate the functionof vulnerability stories in making dyspnea visible and as a way of legitimizing thehelp-seeking behavior of patients during experiences of acute breathlessness.
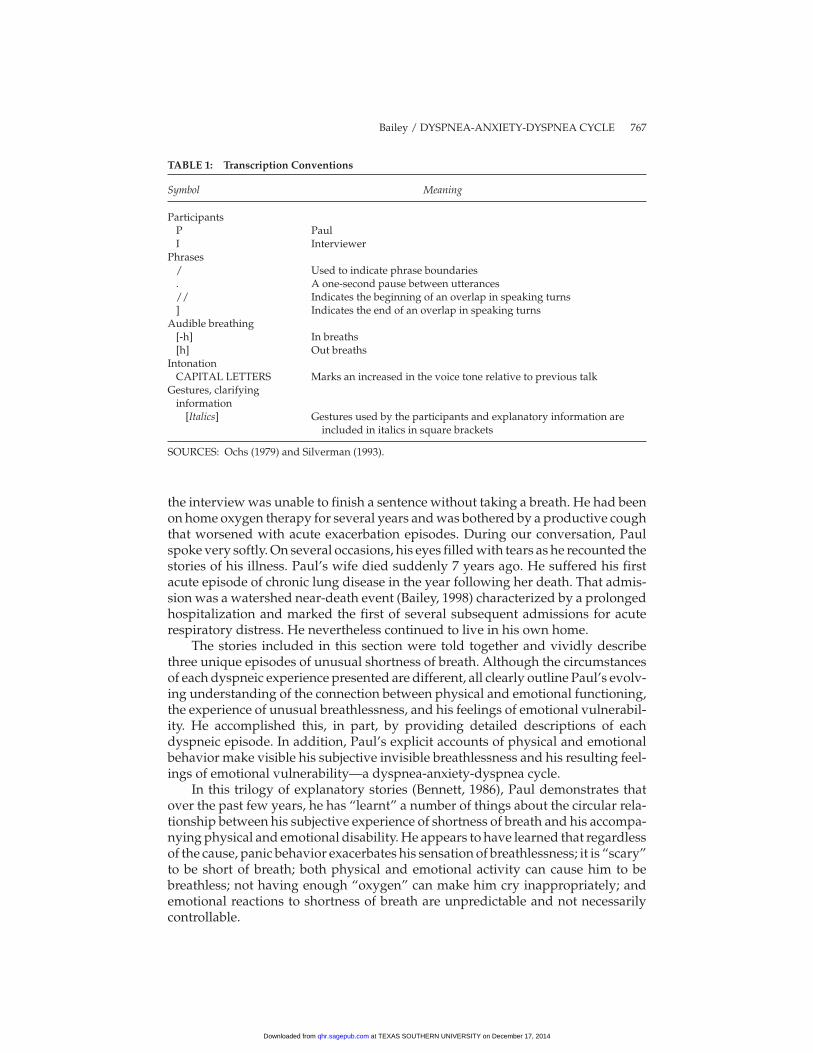
In the following stories, the patient describes three unrelated episodes of acutebreathlessness. I have presented the stories using Labov’s (1972) structural catego-ries and method of transcription. In the written text, I made a conscious effort to“reveal [rather than] conceal aspects of meaning and intent” as presented by thisparticipant’s talk (Gee et al., 1992, p. 240). For example, I made notations on the tran-scriptions to indicate aspects of oral text such as pitch/loudness, pauses andnonlexical expressions, overlaps in speech, dialect, and discourse markers (seeTable 1 for transcription conventions). I also attempted to ensure that the textreflected the breathlessness of the patient, particularly when this difficulty inter-rupted the flow of the interview. The transcript was not tidied. All the conversationthat occurred during the interaction was incorporated into the transcript, includingspeech interruptions, false starts, and overlaps in speaking turns. The phrasing wasmarked and each line of the transcribed text was sequentially numbered to allow forthe identification of sections of interview text.
CASE EXAMPLE
Paul, a 73-year-old retired miner, had been admitted to hospital frequently over thepast 6 years with acute dyspnea. He had the characteristically barreled chest of anindividual with long-standing chronic obstructive pulmonary disease and during
766 QUALITATIVE HEALTH RESEARCH / July 2004
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from
the interview was unable to finish a sentence without taking a breath. He had beenon home oxygen therapy for several years and was bothered by a productive coughthat worsened with acute exacerbation episodes. During our conversation, Paulspoke very softly. On several occasions, his eyes filled with tears as he recounted thestories of his illness. Paul’s wife died suddenly 7 years ago. He suffered his firstacute episode of chronic lung disease in the year following her death. That admis-sion was a watershed near-death event (Bailey, 1998) characterized by a prolongedhospitalization and marked the first of several subsequent admissions for acuterespiratory distress. He nevertheless continued to live in his own home.
The stories included in this section were told together and vividly describethree unique episodes of unusual shortness of breath. Although the circumstancesof each dyspneic experience presented are different, all clearly outline Paul’s evolv-ing understanding of the connection between physical and emotional functioning,the experience of unusual breathlessness, and his feelings of emotional vulnerabil-ity. He accomplished this, in part, by providing detailed descriptions of eachdyspneic episode. In addition, Paul’s explicit accounts of physical and emotionalbehavior make visible his subjective invisible breathlessness and his resulting feel-ings of emotional vulnerability—a dyspnea-anxiety-dyspnea cycle.
In this trilogy of explanatory stories (Bennett, 1986), Paul demonstrates thatover the past few years, he has “learnt” a number of things about the circular rela-tionship between his subjective experience of shortness of breath and his accompa-nying physical and emotional disability. He appears to have learned that regardlessof the cause, panic behavior exacerbates his sensation of breathlessness; it is “scary”to be short of breath; both physical and emotional activity can cause him to bebreathless; not having enough “oxygen” can make him cry inappropriately; andemotional reactions to shortness of breath are unpredictable and not necessarilycontrollable.
Bailey / DYSPNEA-ANXIETY-DYSPNEA CYCLE 767
TABLE 1: Transcription Conventions
Symbol Meaning
ParticipantsP PaulI Interviewer
Phrases/ Used to indicate phrase boundaries. A one-second pause between utterances// Indicates the beginning of an overlap in speaking turns] Indicates the end of an overlap in speaking turns
Audible breathing[-h] In breaths[h] Out breaths
IntonationCAPITAL LETTERS Marks an increased in the voice tone relative to previous talk
Gestures, clarifyinginformation
[Italics] Gestures used by the participants and explanatory information areincluded in italics in square brackets
SOURCES: Ochs (1979) and Silverman (1993).
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from
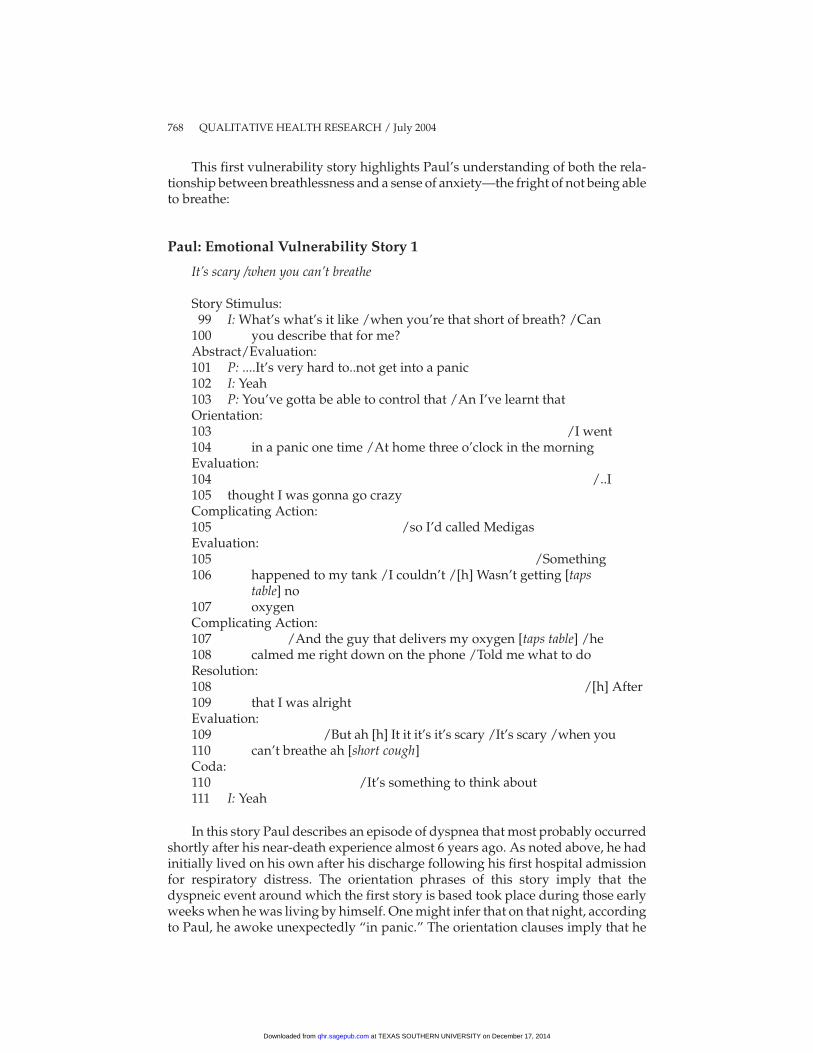
This first vulnerability story highlights Paul’s understanding of both the rela-tionship between breathlessness and a sense of anxiety—the fright of not being ableto breathe:
Paul: Emotional Vulnerability Story 1
It’s scary /when you can’t breathe
Story Stimulus:99 I: What’s what’s it like /when you’re that short of breath? /Can
100 you describe that for me?Abstract/Evaluation:101 P: ....It’s very hard to..not get into a panic102 I: Yeah103 P: You’ve gotta be able to control that /An I’ve learnt thatOrientation:103 /I went104 in a panic one time /At home three o’clock in the morningEvaluation:104 /..I105 thought I was gonna go crazyComplicating Action:105 /so I’d called MedigasEvaluation:105 /Something106 happened to my tank /I couldn’t /[h] Wasn’t getting [taps
table] no107 oxygenComplicating Action:107 /And the guy that delivers my oxygen [taps table] /he108 calmed me right down on the phone /Told me what to doResolution:108 /[h] After109 that I was alrightEvaluation:109 /But ah [h] It it it’s it’s scary /It’s scary /when you110 can’t breathe ah [short cough]Coda:110 /It’s something to think about111 I: Yeah
In this story Paul describes an episode of dyspnea that most probably occurredshortly after his near-death experience almost 6 years ago. As noted above, he hadinitially lived on his own after his discharge following his first hospital admissionfor respiratory distress. The orientation phrases of this story imply that thedyspneic event around which the first story is based took place during those earlyweeks when he was living by himself. One might infer that on that night, accordingto Paul, he awoke unexpectedly “in panic.” The orientation clauses imply that he
768 QUALITATIVE HEALTH RESEARCH / July 2004
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from
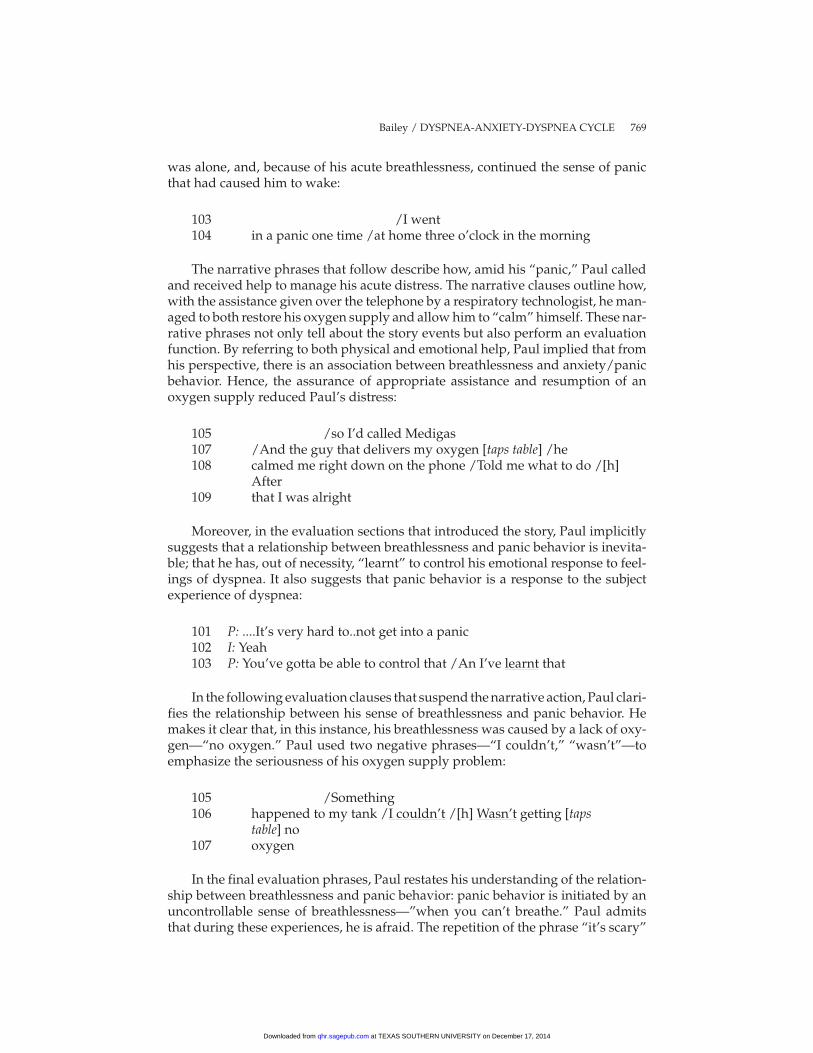
was alone, and, because of his acute breathlessness, continued the sense of panicthat had caused him to wake:
103 /I went104 in a panic one time /at home three o’clock in the morning
The narrative phrases that follow describe how, amid his “panic,” Paul calledand received help to manage his acute distress. The narrative clauses outline how,with the assistance given over the telephone by a respiratory technologist, he man-aged to both restore his oxygen supply and allow him to “calm” himself. These nar-rative phrases not only tell about the story events but also perform an evaluationfunction. By referring to both physical and emotional help, Paul implied that fromhis perspective, there is an association between breathlessness and anxiety/panicbehavior. Hence, the assurance of appropriate assistance and resumption of anoxygen supply reduced Paul’s distress:
105 /so I’d called Medigas107 /And the guy that delivers my oxygen [taps table] /he108 calmed me right down on the phone /Told me what to do /[h]
After109 that I was alright
Moreover, in the evaluation sections that introduced the story, Paul implicitlysuggests that a relationship between breathlessness and panic behavior is inevita-ble; that he has, out of necessity, “learnt” to control his emotional response to feel-ings of dyspnea. It also suggests that panic behavior is a response to the subjectexperience of dyspnea:
101 P: ....It’s very hard to..not get into a panic102 I: Yeah103 P: You’ve gotta be able to control that /An I’ve learnt that
In the following evaluation clauses that suspend the narrative action, Paul clari-fies the relationship between his sense of breathlessness and panic behavior. Hemakes it clear that, in this instance, his breathlessness was caused by a lack of oxy-gen—“no oxygen.” Paul used two negative phrases—“I couldn’t,” “wasn’t”—toemphasize the seriousness of his oxygen supply problem:
105 /Something106 happened to my tank /I couldn’t /[h] Wasn’t getting [taps
table] no107 oxygen
In the final evaluation phrases, Paul restates his understanding of the relation-ship between breathlessness and panic behavior: panic behavior is initiated by anuncontrollable sense of breathlessness—”when you can’t breathe.” Paul admitsthat during these experiences, he is afraid. The repetition of the phrase “it’s scary”
Bailey / DYSPNEA-ANXIETY-DYSPNEA CYCLE 769
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from
underscores his fear. The coda phrase suggests that this sense of anxiety, emotionalvulnerability, is something that now occupies his thoughts:
109 /But ah [h] It it it’s it’s scary /It’s scary /when you110 can’t breathe ah [short cough] /It’s something to think about
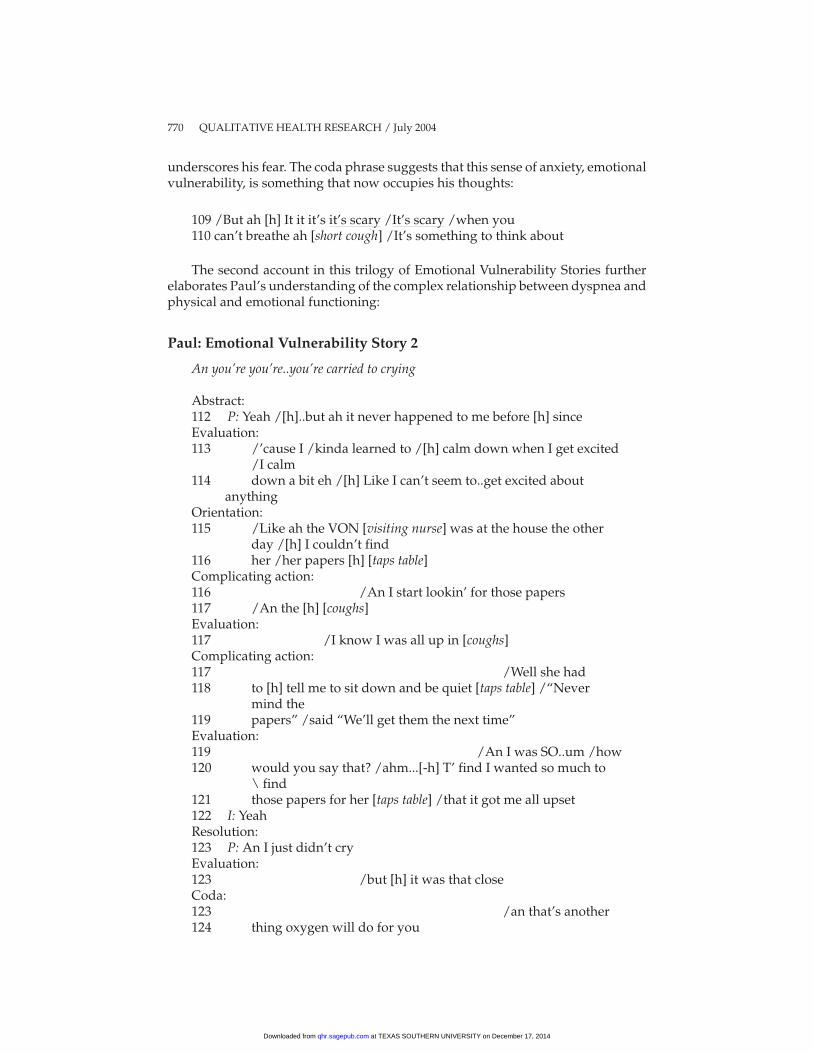
The second account in this trilogy of Emotional Vulnerability Stories furtherelaborates Paul’s understanding of the complex relationship between dyspnea andphysical and emotional functioning:
Paul: Emotional Vulnerability Story 2
An you’re you’re..you’re carried to crying
Abstract:112 P: Yeah /[h]..but ah it never happened to me before [h] sinceEvaluation:113 /’cause I /kinda learned to /[h] calm down when I get excited
/I calm114 down a bit eh /[h] Like I can’t seem to..get excited about
anythingOrientation:115 /Like ah the VON [visiting nurse] was at the house the other
day /[h] I couldn’t find116 her /her papers [h] [taps table]Complicating action:116 /An I start lookin’ for those papers117 /An the [h] [coughs]Evaluation:117 /I know I was all up in [coughs]Complicating action:117 /Well she had118 to [h] tell me to sit down and be quiet [taps table] /“Never
mind the119 papers” /said “We’ll get them the next time”Evaluation:119 /An I was SO..um /how120 would you say that? /ahm...[-h] T’ find I wanted so much to
\ find121 those papers for her [taps table] /that it got me all upset122 I: YeahResolution:123 P: An I just didn’t cryEvaluation:123 /but [h] it was that closeCoda:123 /an that’s another124 thing oxygen will do for you
770 QUALITATIVE HEALTH RESEARCH / July 2004
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from
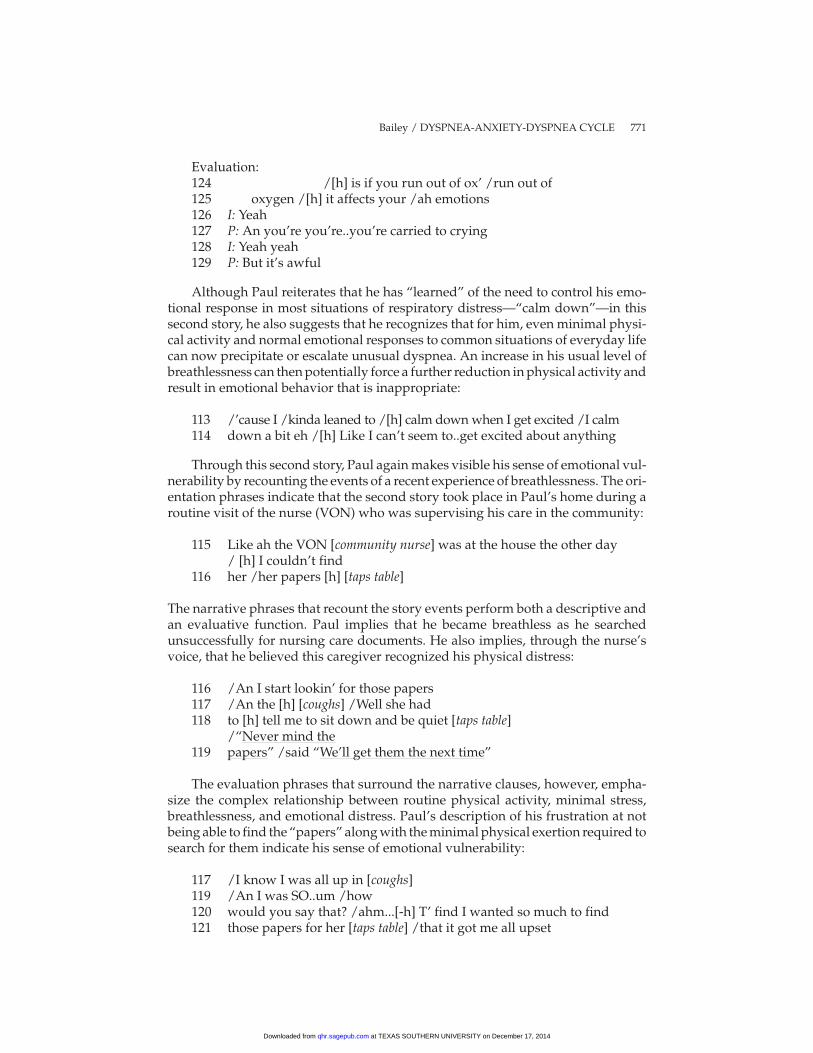
Evaluation:124 /[h] is if you run out of ox’ /run out of125 oxygen /[h] it affects your /ah emotions126 I: Yeah127 P: An you’re you’re..you’re carried to crying128 I: Yeah yeah129 P: But it’s awful
Although Paul reiterates that he has “learned” of the need to control his emo-tional response in most situations of respiratory distress—“calm down”—in thissecond story, he also suggests that he recognizes that for him, even minimal physi-cal activity and normal emotional responses to common situations of everyday lifecan now precipitate or escalate unusual dyspnea. An increase in his usual level ofbreathlessness can then potentially force a further reduction in physical activity andresult in emotional behavior that is inappropriate:
113 /’cause I /kinda leaned to /[h] calm down when I get excited /I calm114 down a bit eh /[h] Like I can’t seem to..get excited about anything
Through this second story, Paul again makes visible his sense of emotional vul-nerability by recounting the events of a recent experience of breathlessness. The ori-entation phrases indicate that the second story took place in Paul’s home during aroutine visit of the nurse (VON) who was supervising his care in the community:
115 Like ah the VON [community nurse] was at the house the other day/ [h] I couldn’t find
116 her /her papers [h] [taps table]
The narrative phrases that recount the story events perform both a descriptive andan evaluative function. Paul implies that he became breathless as he searchedunsuccessfully for nursing care documents. He also implies, through the nurse’svoice, that he believed this caregiver recognized his physical distress:
116 /An I start lookin’ for those papers117 /An the [h] [coughs] /Well she had118 to [h] tell me to sit down and be quiet [taps table]
/“Never mind the119 papers” /said “We’ll get them the next time”
The evaluation phrases that surround the narrative clauses, however, empha-size the complex relationship between routine physical activity, minimal stress,breathlessness, and emotional distress. Paul’s description of his frustration at notbeing able to find the “papers” along with the minimal physical exertion required tosearch for them indicate his sense of emotional vulnerability:
117 /I know I was all up in [coughs]119 /An I was SO..um /how120 would you say that? /ahm...[-h] T’ find I wanted so much to find121 those papers for her [taps table] /that it got me all upset
Bailey / DYSPNEA-ANXIETY-DYSPNEA CYCLE 771
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from
Paul’s sense of frustration (emotional distress) caused by such a seemingly trivialproblem not only necessitated stopping all physical activity but also resulted inwhat Paul intimates was an inappropriate emotional reaction:
123 P: An I just didn’t cry /but [h] it was that close
Furthermore, this story suggests that Paul is emotionally vulnerable. From hisperspective, the relationship between dyspnea and emotional functioning was bothcomplex (i.e., breathlessness caused anxiety, and anxiety caused increased breath-lessness and more anxiety) and circular, that is, breathlessness, apparently exacer-bated by both emotional feelings such as frustration and minimal physical activity,resulted in not only physically incapacitating dyspnea but also disproportionateemotional distress. In addition, on occasion the experience of an emotional responsewas both a contributing factor in Paul’s increased respiratory distress and a sign ofan impending episode of unmanageable dyspnea.
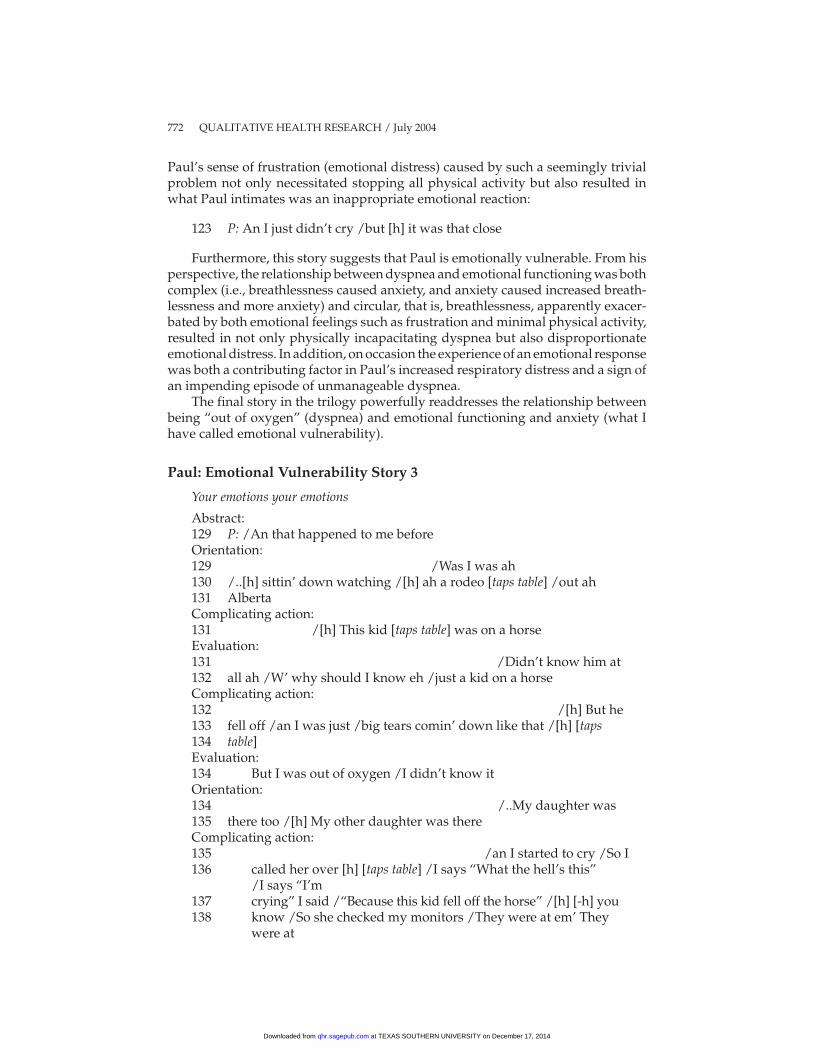
The final story in the trilogy powerfully readdresses the relationship betweenbeing “out of oxygen” (dyspnea) and emotional functioning and anxiety (what Ihave called emotional vulnerability).
Paul: Emotional Vulnerability Story 3
Your emotions your emotions
Abstract:129 P: /An that happened to me beforeOrientation:129 /Was I was ah130 /..[h] sittin’ down watching /[h] ah a rodeo [taps table] /out ah131 AlbertaComplicating action:131 /[h] This kid [taps table] was on a horseEvaluation:131 /Didn’t know him at132 all ah /W’ why should I know eh /just a kid on a horseComplicating action:132 /[h] But he133 fell off /an I was just /big tears comin’ down like that /[h] [taps134 table]Evaluation:134 But I was out of oxygen /I didn’t know itOrientation:134 /..My daughter was135 there too /[h] My other daughter was thereComplicating action:135 /an I started to cry /So I136 called her over [h] [taps table] /I says “What the hell’s this”
/I says “I’m137 crying” I said /“Because this kid fell off the horse” /[h] [-h] you138 know /So she checked my monitors /They were at em’ They
were at
772 QUALITATIVE HEALTH RESEARCH / July 2004
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from
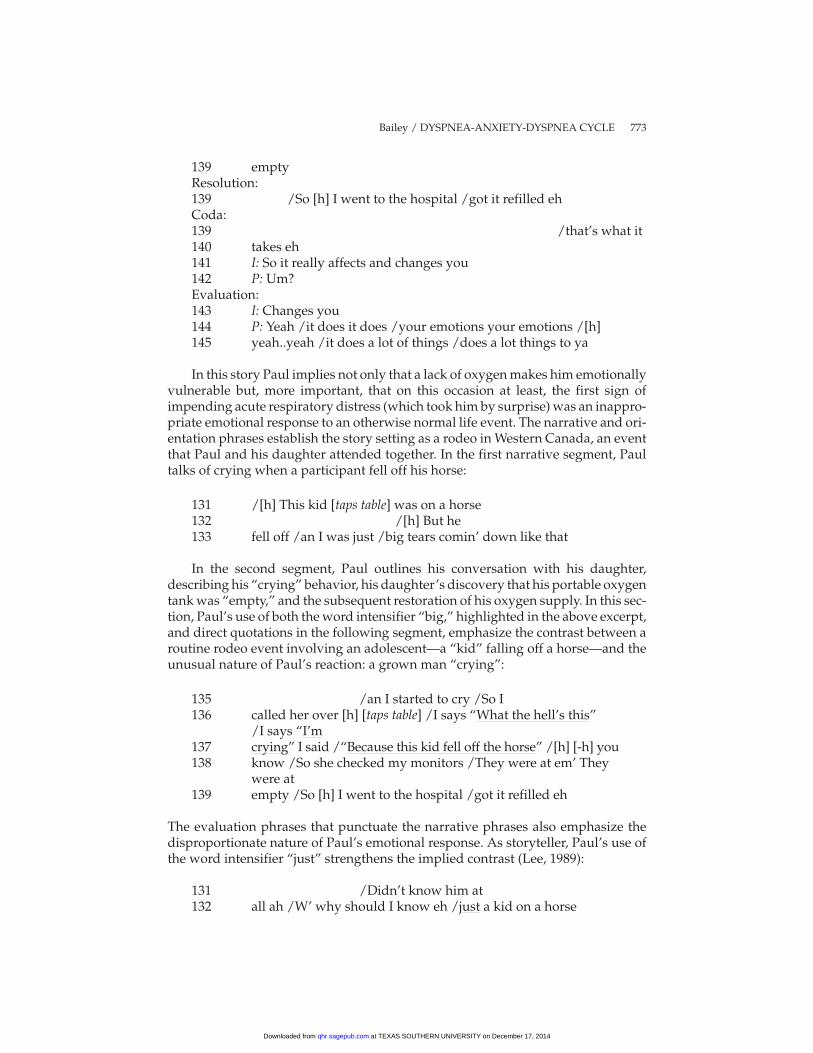
139 emptyResolution:139 /So [h] I went to the hospital /got it refilled ehCoda:139 /that’s what it140 takes eh141 I: So it really affects and changes you142 P: Um?Evaluation:143 I: Changes you144 P: Yeah /it does it does /your emotions your emotions /[h]145 yeah..yeah /it does a lot of things /does a lot things to ya
In this story Paul implies not only that a lack of oxygen makes him emotionallyvulnerable but, more important, that on this occasion at least, the first sign ofimpending acute respiratory distress (which took him by surprise) was an inappro-priate emotional response to an otherwise normal life event. The narrative and ori-entation phrases establish the story setting as a rodeo in Western Canada, an eventthat Paul and his daughter attended together. In the first narrative segment, Paultalks of crying when a participant fell off his horse:
131 /[h] This kid [taps table] was on a horse132 /[h] But he133 fell off /an I was just /big tears comin’ down like that
In the second segment, Paul outlines his conversation with his daughter,describing his “crying” behavior, his daughter’s discovery that his portable oxygentank was “empty,” and the subsequent restoration of his oxygen supply. In this sec-tion, Paul’s use of both the word intensifier “big,” highlighted in the above excerpt,and direct quotations in the following segment, emphasize the contrast between aroutine rodeo event involving an adolescent—a “kid” falling off a horse—and theunusual nature of Paul’s reaction: a grown man “crying”:
135 /an I started to cry /So I136 called her over [h] [taps table] /I says “What the hell’s this”
/I says “I’m137 crying” I said /“Because this kid fell off the horse” /[h] [-h] you138 know /So she checked my monitors /They were at em’ They
were at139 empty /So [h] I went to the hospital /got it refilled eh
The evaluation phrases that punctuate the narrative phrases also emphasize thedisproportionate nature of Paul’s emotional response. As storyteller, Paul’s use ofthe word intensifier “just” strengthens the implied contrast (Lee, 1989):
131 /Didn’t know him at132 all ah /W’ why should I know eh /just a kid on a horse
Bailey / DYSPNEA-ANXIETY-DYSPNEA CYCLE 773
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from

The second notable point of this story is Paul’s recognition that his inappropri-ate emotional response of crying was the initial sign that he was experiencing respi-ratory distress. Paul’s sense of dyspnea presented initially as an inappropriate emo-tional reaction to a normal life event. The story centers on a puzzle. Paul attempts tounderstand why he would cry in such an unlikely situation—“just a kid on a horse.”The explanation suggests Paul’s recognition of a dyspnea-anxiety-dyspnea cyclerelated to an oxygen deficit:
134 But I was out of oxygen /I didn’t know it
Paul, through his story, implies that he has now learned that not having enough“oxygen” makes him emotionally vulnerable (crying inappropriately). Althoughhe does not understand it, this emotional reaction or anxiety, associated withdyspnea (caused by a lack of oxygen), is unpredictable and outside of voluntarycontrol.
DISCUSSION
My initial intention in this research, in part, was to understand the affective compo-nent of AECOPD from the patient’s perspective. As represented in the precedingstories, patients described a dynamic relationship between dyspnea and emotionalfunctioning or anxiety. Through their accounts, they illustrated their emotional vul-nerability as they lived with chronic lung disease. The narrative phrases of their sto-ries revealed their understanding of the complex relationship between physicalactivity, emotional behavior, and intractable breathlessness. The underlying experi-ence of the patient-participants was shortness of breath, an experience that wasessentially subjective and invisible. The stories told by Paul made visible the subjec-tive nature of this dyspnea. These accounts also represented the emotional vulnera-bility and interaction between the sensations of breathlessness and anxiety experi-enced by all patients across the interview data during their dyspneic episodes.
It is important to note that individuals with apparently comparable lung dis-ease report varying levels of respiratory distress (O’Donnell & Webb, 1992; Lareau,Meek, Press, Anholm, & Roos, 1999; Traver, 1988). As Adams and colleagues(Adams, Chronos, Lane, & Guz, 1986; Adams, Lane, et al., 1985) have demon-strated, there are differences in the perception of respiratory sensory stimuli amonghealthy adults that as yet remain unexplained. Therefore, some researchers havefocused on the psychological differences among people with COPD and/orbetween COPD sufferers and nondiseased individuals to explain disparity in theexperience of breathlessness severity reported by patients with COPD with similarlevels of respiratory pathophysiology.
Work by Burns and Howell (1969) in the 1960’s unequivocally demonstratedthat individuals concurrently suffering from psychological illnesses, includingdepression, anxiety, or hysteria, could present with breathlessness disproportionateto their underlying lung pathology as measured by pulmonary function testing.However, it is important to note that these researchers reported that treatment of theunderlying psychopathology relieved the complaints of dyspnea. Although subse-quent research has shown that individuals with COPD as a group do report
774 QUALITATIVE HEALTH RESEARCH / July 2004
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from

substantially higher levels of reactive depression than other medical patients, in theabsence of psychiatric illness, there is no correlation or causal relationship betweenthe perceived severity of dyspnea and the degree of depression (Light, Merrill,Despars, Gordon, & Mutalipassi, 1985; McSweeny, Grant, Heaton, Adams, &Timms, 1982; Yellowlees, Alpers, Bowden, Bryant, & Ruffin, 1987).
Finally, as outlined initially, nurse-researchers describe a positive relationshipbetween anxiety and levels of dyspnea and have conceptualized this relationship asthe “anxiety-dyspnea-anxiety cycle” (Carrieri-Kohlman, Douglas, et al., 1993,p. 230), suggesting that patients’ emotional reaction to a sense of breathlessnessexacerbates their perception of breathlessness. However, I would suggest thathealth care providers must consider an alternate understanding of the dyspnea-anxiety relationship. From the perspective of the patients living with COPD in thisstudy, anxiety is not usually the underlying cause of distressing dyspnea but, rather,a sign of longstanding or acute respiratory failure—what might, from the sufferersemic perspective more accurately be labeled a dyspnea-anxiety-dyspnea cycle.Indeed, over the course of their illness, these patients have learned to control theiremotional reactions. Hence, when they feel anxious, they realize that at this stage oftheir illness, this emotion is an indicator that they are actually breathless.
Janson-Bjerklie, Ferketich, Benner, and Becker’s (1992) work with acutely illasthmatic patients supports this alternate interpretation. These researchers studiedasthmatics who presented themselves to the emergency department during acuteexacerbations of their disease characterized by severe dyspnea. They discoveredthat individuals who became highly anxious during these asthmatic episodes wereaccurate in their assessment of the severity of their illness, that is, correctly knowingwhen they required emergency hospitalization. These researchers contended thatthe patients’ levels of anxiety in this study positively correlated with objectivemeasures of airway obstruction.
Hence, in the absence of clear, objective measures of illness severity for patientsexperiencing acute exacerbations of COPD characterized by dyspnea, and given thefindings reported by Janson-Bjerklie, Ferketich, et al. (1992), the insights uncoveredin this study suggest that anxiety might provide an important indicator of actual ill-ness severity and assist nurses in determining the support and care that thesepatients require. It is essential that nurses recognize anxiety as an emic sign and notnecessary the cause of dyspnea for patients with COPD in acute respiratorydistress.
REFERENCES
Adams, L. (1996). Reflex respiratory stimulation and respiratory sensation. In L. Adams & A. Guz (Eds.),Respiratory sensation (pp. 201-211). New York: Marcel Dekker.
Adams, L., Chronos, N., Lane, R., & Guz, A. (1986). The measurement of breathlessness induced in nor-mal subjects: Individual differences. Clinical Science, 70, 131-140.
Adams, L., Lane, R., Shea, S. A., Cockcroft, A., & Guz, A. (1985). Breathlessness during different forms ofventilatory stimulation: Astudy of mechanisms in normal subjects and respiratory patients. ClinicalSciences, 69, 663-672.
Agar, M., & Hobbs, J. R. (1982). Interpreting discourse: Coherence and the analysis of ethnographic inter-views. Discourse Process, 5, 1-32.
Agar, M., & Hobbs, J. R. (1983). Natural plans: Using AI planning in the analysis of ethnographic inter-views. Ethos, 11(1/2), 33-48.
Bailey / DYSPNEA-ANXIETY-DYSPNEA CYCLE 775
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from
Antaki, C. (1994). Exploring and arguing: The social organization of accounts. London: Sage.Anthonisen, N. R., Hershfield, E. S., Harding, G. K. M., Manfred, J., Nelson, N. A., & Warren, C. P. W.
(1987). Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Annals ofInternal Medicine, 106, 196-204.
Anthony, E. J. (1989). Risk, vulnerability and resilience: An overview. In E. J. Anthony & B. J. Cohler(Eds.), The invulnerable child (pp. 3-48). London: Guilford.
Atkinson, P. (1992). The ethnography of a medical setting: Reading, writing, and rhetoric. QualitativeHealth Research, 2(4), 451-474.
Bailey, P. H. (1996). Assuring quality in narrative analysis. Western Journal of Nursing Research, 18(2), 186-194.
Bailey, P. H. (1998). Patients’, family caregivers’, and nurses’ stories of acute exacerbation events of chronicobstructive pulmonary disease [Doctoral dissertation]. Edinburgh, UK: Edinburgh University Press.
Bailey, P. H. (2001). Death stories: Acute exacerbations of chronic obstructive pulmonary disease. Qualita-tive Health Research, 11(3), 322-337.
Bailey, P. H., Colella, T., & Mossey, S. (in press). Intuition or template: Nurses’ stories of AECOPD.Bailey, P. H., & Tilley, S. (2002). Storytelling and the interpretation of meaning in qualitative research.
Journal of Advanced Nursing, 38(6), 574-583.Bennett, G. (1986). Narrative as expository discourse. Journal of American Folklore, 99, 415-434.Black, A. L., & Curtis, J. R. (2001). Treating dyspnea in a patient with advanced chronic obstructive pul-
monary disease. Western Journal of Medicine, 175, 197-201.Burns, B. H., & Howell, J. B. L. (1969). Disproportionately severe breathlessness in chronic bronchitis.
Quarterly Journal of Medicine, 38(151), 277-294.Carrieri, V., & Janson-Bjerklie, S. (1986). Strategies patients use to manage the sensation of dyspnea. West-
ern Journal of Nursing Research, 8(3), 284-305.Carrieri, V., Janson-Bjerklie, S., & Jacobs, S. (1984). The sensation of dyspnea: A review. Heart & Lung,
13(4), 436-447.Carrieri-Kohlman, V., Douglas, M. K., Gormley, J. M., & Stulbarg, M. S. (1993). Desensitization and
guided mastery: Treatment approaches for the management of dyspnea. Heart & Lung, 22, 226-234.Carrieri-Kohlman, V., Gormley, J. M., Douglas, M. K., Paul, S. M., & Stulbarg, M. S. (1996a). Differentia-
tion between dyspnea and its affective components. Western Journal of Nursing Research, 18(6), 626-642.
Carrieri-Kohlman, V., Gormley, J. M., Douglas, M. K., Paul, S. M., & Stulbarg, M. S. (1996b). Exercise train-ing decreases dyspnea and the distress and anxiety associated with it. Chest, 110(6), 1526-1535.
Clarke, H. F., & Driever, M. J. (1983). Vulnerability: The development of a construct for nursing. In P. L.Chinn (Ed.), Advances in nursing theory development (pp. 207-220). Rockville, MD: Aspen Systems.
Cohler, B. J. (1989). Adversity, resilience, and the study of lives. In E. J. Anthony & B. J. Cohler (Eds.), Theinvulnerable child (pp. 363-424). London: Guilford.
Connelly, F. M., & Clandinin, D. J. (1990). Stories of experience and narrative inquiry. EducationalResearcher, 19(5), 2-14.
Dahlén, I., & Janson, C. (2003). Do anxiety and depression impact patients with COPD? American FamilyPhysician, 67(6), 1378.
Demi, A. S., & Warren, N. A. (1995). Issues in conducting research with vulnerable families. Western Jour-nal of Nursing Research, 17(2), 188-202.
DeVito, A. J. (1990). Dyspnea during hospitalisation for acute phase of illness as recalled by patients withchronic obstructive pulmonary disease. Heart & Lung, 12(2), 186-191.
Gee, J. P. (1991). A linguistic approach to narrative. Journal of Narrative and Life History, 1(1), 15-39.Gee, J. P., Michaels, S., & O’Connor, M. C. (1992). Discourse analysis. In M. D. LeCompte, W. L. Millroy, &
J. Preissle (Eds.), The handbook of qualitative research in education (pp. 227-291). Toronto, Canada: Aca-demic Press.
Gift, A. G. (1990). Dyspnea. Nursing Clinics of North America, 25(4), 955-965.Gift, A. G. (1993). Therapies for dyspnea relief. Holistic Nursing Practice, 7(2), 57-63.Gift, A. G., & Cahill, C. A. (1990). Psychophysiologic aspects of dyspnea in chronic obstructive pulmo-
nary disease: A pilot study. Heart & Lung, 19, 252-257.Gift, A. G., & McCrone, S. H. (1993). Depression in patients with COPD. Heart & Lung, 22(4), 289-297.Gift, A. G., Moore, T., & Soeken, K. (1992). Relaxation to reduce dyspnea and anxiety in COPD patients.
Nursing Research, 41(4), 242-246.Gift, A. G., Plaut, S. M., & Jacox, A. K. (1986). Psychologic and physiologic factors related to dyspnea in
subjects with chronic obstructive pulmonary disease. Heart & Lung, 15, 595-601.
776 QUALITATIVE HEALTH RESEARCH / July 2004
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from

Gift, A. G., & Pugh, L. C. (1993). Dyspnea and fatigue. Nursing Clinics of North America, 28(2), 373-384.Gift, A. G., Wood, R. M., & Cahill, C. A. (1989). Depression, somatization and steroid use in chronic
obstructive pulmonary disease. International Journal of Nursing Studies, 26(3), 281-286.Gilgun, J. F., Daly, K., & Handel, G. (1992). Qualitative methods in family research. London: Sage.Good, B. A. V., & Rodrigues-Fisher, L. (1993). Vulnerability: An ethical consideration in research with
older adults. Western Journal of Nursing Research, 15(6), 780-783.Hogan, N. S., & De Santis, L. (1994). Things that help and hinder adolescent sibling bereavement. Western
Journal of Nursing Research, 16(2), 132-153.Janson-Bjerklie, S., Carrieri, V. K., & Hudes, M. (1986). The sensations of pulmonary dyspnea. Nursing
Research, 35(3), 154-159.Janson-Bjerklie, S., Ferketich, S., Benner, P., & Becker, G. (1992). Clinical markers of asthma severity and
risk: The importance of subjective as well as objective factors. Heart & Lung, 21, 265-272.Johnson, M. A. (1998). Who is the family? In B. Vaughan-Cole, M. A. Johnson, J. A. Malone, & B. Walker
(Eds.), Family nursing practice (pp. 3-18). Philadelphia: W. B. Saunders.Kalcik, S. (1975). “ . . . like Ann’s gynaecologist or the time I was almost raped”: Personal narrative in
women’s rap groups. In C. R. Farrer (Ed.), Women and folklore (pp. 3-11). Austin: University of Texas.Kermode, F. (1981). Secrets and narrative sequence. In W. J. T. Mitchell (Ed.), On narrative (pp. 79-97). Chi-
cago: University of Chicago Press.Killian, K. J., & Campbell, E. J. M. (1996). Historical aspects of dyspnea. In L. Adams & A. Guz (Eds.),
Respiratory sensation (pp. 1-17). New York: Marcel Dekker.Labov, W. (1972). Language in the inner city: Studies in the Black English vernacular. Philadelphia: University
of Pennsylvania Press.Labov, W. (1982). Speech actions and reactions in personal narrative. In E. Tannen (Ed.), Analyzing dis-
course: Text and talk (pp. 219-247). Washington, DC: Georgetown University Press.Labov, W., & Fanshel, D. (1977). Therapeutic discourse: Psychotherapy as conversation. London: Academic
Press.Labov, W., & Waletzky, J. (1972). Narrative analysis: Oral versions of personal experience. In J. Helms
(Ed.), Essays on the verbal and visual arts (pp. 12-44). Seattle: University of Washington Press.Lareau, S. C., Meek, P. M., Press, D., Anholm, J. D., & Roos, P. J. (1999). Dyspnea in patients with chronic
obstructive pulmonary disease: Does dyspnea worsen longitudinally in the presence of declininglung function? Heart & Lung, 28, 65-73.
Lee, D. (1989). The semantics of just. Journal of Pragmatics, 11, 377-398.Light, R. W., Merrill, E. J., Despars, J. A., Gordon, G. H., & Mutalipassi, L. R. (1985). Prevalence of depres-
sion and anxiety in patients with COPD: Relationship to functional capacity. Chest, 87(1), 35-38.Lynn, J., Ely, E. W., Zhong, Z., McNiff, K. L., Dawson, N. V., Connors, A., et al. (2000). Living and dying
with chronic obstructive pulmonary disease. Journal of the American Geriatrics Society, 48, S91-S100.McBride, S., Graydon, J., Sidani, S., & Hall, L. (1999). The therapeutic use of music for dyspnea and anxi-
ety in patients with COPD who live at home. Journal of Holistic Nursing, 17(3), 229-250.McCory, D. C., Brown, C., Gelfand, S. E., & Bach, P. B. (2001). Management of acute exacerbations of
COPD: A summary and appraisal of published evidence. Chest, 119(4), 1190-1209.McSweeny, A. J., Grant, I., Heaton, R. K., Adams, K. M., & Timms, R. M. (1982). Life quality of patients
with chronic obstructive pulmonary disease. Archives of Internal Medicine, 142, 473-478.Mishler, E. G. (1986). Research interviewing context and narrative. London: Harvard University Press.Ochs, E. (1979). Transcription as theory. In E. Ochs & B. B. Schieffenn (Eds.), Developmental pragmatics
(pp. 43-72). New York: Academic Press.O’Donnell, D. E., & Webb, K. A. (1992). Breathlessness in patients with chronic airflow limitation. Chest,
106, 904-912.Polanyi, L. (1985). Conversational storytelling. In T. A. Van Dijk (Ed.), Handbook of discourse analysis (Vol.
3, pp. 183-201). London: Academic Press.Polanyi, L. (1989). Telling the American story: A structural and cultural analysis of conversational storytelling.
London: MIT Press.Potter, J., & Wetherell, M. (1987). Discourse and social psychology: Beyond attitudes and behaviour. London:
Sage.Renfroe, K. L. (1988). Effect of progressive relaxation on dyspnea and state anxiety in patients with
chronic obstructive pulmonary disease. Heart & Lung, 17, 408-413.Riessman, C. K. (1987). When gender is not enough: Women interviewing women. Gender & Society, 1,
172-207.
Bailey / DYSPNEA-ANXIETY-DYSPNEA CYCLE 777
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from

Riessman, C. K. (1988). Worlds of difference: Contrasting experience in marriage and narrative style. InA. D. Todd & S. Fisher (Eds.), Gender and discourse: The power of talk (pp. 151-173). Norwood, NJ:Ablex.
Riessman, C. K. (1989). Life events, meaning and narrative: The case of infidelity and divorce. Social Sci-ence & Medicine, 29(6), 743-751.
Riessman, C. K. (1990a). Divorce talk: Women and men make sense of personal relationships. London: RutgersUniversity Press.
Riessman, C. K. (1990b). Strategic uses of narrative in the presentation of self and illness: Aresearch note.Social Science & Medicine, 30(11), 1195-1200.
Riessman, C. K. (1991). Beyond reductionism: Narrative genres in divorce accounts. Journal of Narrativeand Life History, 1(1), 41-68.
Riessman, C. K. (1993). Narrative analysis. London: Sage.Riessman, C. K. (1994a). Making sense of marital violence: One women’s narrative. In C. K. Riessman
(Ed.), Qualitative studies in social work research (pp. 113-132). London: Sage.Riessman, C. K. (1994b). Narrative approaches to trauma. In C. K. Riessman (Ed.), Qualitative studies in
social work research (pp. 67-71). London: Sage.Rose, M. H., & Killien, M. (1983). Risk and vulnerability: A case for differentiation. Advances in Nursing
Science, 5(3), 60-73.Runo, J. R., & Ely, E. W. (2001). Treating dyspnea in a patient with advanced chronic obstructive pulmo-
nary disease. Western Journal of Medicine, 175, 197-201.Schiffin, D. (1994). Approaches to discourse. Oxford, UK: Blackwell.Schwartzstein, R. M., & Cristiano, L. M. (1996). Qualities of respiratory sensation. In L. Adams & A. Guz
(Eds.), Respiratory sensation (pp. 125-154). New York: Marcel Dekker.Schwartzstein, R. M., Manning, H. L., Weiss, W., & Weinberger, S. E. (1990). Dyspnea: A sensory experi-
ence. Lung, 168, 185-199.Silverman, D. (1993). Interpreting qualitative data: Methods for analysing, talk, text and interaction. London:
Sage.Spector, N., & Klein, D. (2001). Chronic critically ill dyspneic patients: Mechanisms and clinical measure-
ment. AACN Clinical Issues: Advanced Practice in Acute & Critical Care, 12(2), 220-233.Stevens, P. E., Hall, J. M., & Meleis, A. I. (1992). Examining vulnerability of women clerical workers from
five ethnic/racial groups. Western Journal of Nursing Research, 14(6), 754-774.Strauss, A., Corbin, J., Fagerhaugh, S., Glaser, B. G., Maines, D., Suczek, B., et al. (1984). Chronic illness and
the quality of life. Toronto, Canada: C. V. Mosby.Thornby, M. A., Haas, F., & Axen, K. (1995). Effect of distractive auditory stimuli on exercise tolerance in
patients with COPD. Chest, 107(5), 1213-1217.Tobin, M. J. (1990). Dyspnea: Pathophysiological basis, clinical presentation, and management. Archives
of Internal Medicine, 150, 1604-1613.Traver, G. A. (1988). Measures of symptoms and life quality to predict emergent use of institutional health
care resources in chronic airway disease. Heart & Lung, 17, 689-697.Viney, L. L., & Bousfield, L. (1991). Narrative analysis: A method of psychological research for AIDS-
affected people. Social Science & Medicine, 32(7), 757-765.Widdicombe, S. (1993). Autobiography and change: Rhetoric and authenticity of “Gothic” style. In E.
Burman & I. Parker (Eds.), Discourse analytic research: Repertoires and readings of texts in action (pp. 95-113). London: Routledge.
Wiltshire, J. (1995). Telling a story, writing a narrative: Terminology in health care. Nursing Inquiry, 2, 75-82.
Yellowlees, P. M., Alpers, J. H., Bowden, J. J., Bryant, G. D., & Ruffin, R. E. (1987). Psychiatric morbidity inpatients with chronic airflow obstruction. Medical Journal of Australia, 146, 305-307.
Zubin, J., & Spring, B. (1977). Vulnerability: A new look at schizophrenia. Journal of Abnormal Psychology,86, 103-126.
Patricia Hill Bailey, R.N., B.N., M.H.Sc., Ph.D., is a professor of nursing at Laurentian University,Sudbury, Ontario, Canada.
778 QUALITATIVE HEALTH RESEARCH / July 2004
at TEXAS SOUTHERN UNIVERSITY on December 17, 2014qhr.sagepub.comDownloaded from