the development of acute myelomonocytic leukemia in a patient with acute lymphocytic leukemia
TRANSCRIPT

The Development of Acute Myelomonocytic Leukemia in a Pa tien t with A c u te Lymph o c y tic Le u ke m ia
LEONARD MADOFF, MD, FREDERICK R. DAVEY, MD, GERALD 8. GORDON, MD, NANCY L. DOCK, MS, AND JACK GOLDERG. MD
A diagnosis of acute lymphocytic leukemia (ALL) was made from a peripheral blood and bone marrow specimen from a 59-year-old woman. Typical-appearing lymphoblasts were positive for periodic acid-Schiff (PAS) reaction, but negative for peroxidase, Sudan black B (SBB) and non-specific esterase (NSE) stains. Lymphoblasts failed to form non-immune rosettes and had no surface membrane immunoglobulins. However, lymphoblasts exhibited a n “Ia-like” mem- brane antigen and markedly stimulated allogeneic lymphocytes in a mixed lymphocyte reac- tion (MLR). These cytochemical and immunologic studies were considered characteristic of null-cell subtype of ALL. Thirteen months later, the peripheral blood and bone marrow speci- mens contained numerous myelomonoblasts characterized by a weak or negative PAS stain and strongly positive peroxidase, SBB, and NSE reactions. Electron micrographs of the bone marrow suggested that the majority of leukemic cells were myelomonocytic and a minority of cells were lymphoblasts. In addition, myelomonoblasts in liquid cultures appeared to differ- entiate into mature macrophages. These data suggest the development of acute myelomono- cyte leukemia in a previous case of ALL.
Cancer 48:1157-1163, 1981.
C U T E M Y E L O M O N O C Y T I C (AMML) or acute A myelogenous leukemia (AML) has been observed with increased frequency in patients with Hodgkin’s d i ~ e a ~ e , ~ ~ , ~ ~ , ~ ~ , ~ ~ multiple polycythe- mia v e ~ a , ~ ~ and chronic myelogenous leukemia. 12jz5
Several cases of AML have been reported in patients previously diagnosed with chronic lymphocytic leuke- mia18,21,26,38 and non-Hodgkin’s lymphoma.24 How- ever, AMML or AML rarely develops in patients with acute lymphocytic leukemia (ALL).
We report the morphologic, cytochemical, im- munologic and ultrastructural studies on the neoplastic cells from a patient who initially presented with ALL, and thirteen months later developed AMML.
Case Report
In September 1978, a 59-year-old woman complained of weakness, fatigue, and a low-grade fever of three weeks’ duration. Her physical examination was unremarkable ex-
From the Departments of Pathology and Medicine, State Univer- sity of New York, Upstate Medical Center, Syracuse, New York 13210.
Address for reprints: Dr. Frederick R. Davey, Department of Pa- thology, State University of New York, Upstate Medical Center, 750 East Adams Street, Syracuse, NY 13210.
Accepted for publication August 29, 1980.
cept for pallor. The initial pertinent laboratory studies in- cluded hemoglobin of 5.5 gdl, platelet count of 185,0OO/p1 and a leukocyte count of 2900/p1 with 34.5% lymphoblasts. The bone marrow was hypercellular with 81.2% lympho- blasts. A diagnosis of ALL was made and the patient was treated with induction chemotherapy with vincristine and daunorubicin administered intravenously and prednisone administered orally. Bone marrow remission was achieved three weeks after the initial diagnosis. The patient then re- ceived L-asparaginase intravenously. Maintenance therapy included vincristine, prednisone, 6-mercaptopurine, and methotrexate. Craniospinal irradiation and methotrexate, administered intrathecally, were given as central nervous system prophylaxis.
A bone marrow relapse occurred nine months later with a bone marrow lymphoblast count of 60%. The patient was readmitted for induction chemotherapy, now with cytosine arabinoside, daunorubicin, vincristine, and prednisone. Re- mission was achieved within three weeks and maintenance therapy reinstituted. Two months later, a 20% lymphoblast count in the bone marrow indicated a second relapse which was treated with cyclophosphamide, vincristine, and predni- sone. The patient returned five weeks later, in November 1979, complaining of bilaterial hip pain and abdominal cramps.
The admission laboratory findings included leukocyte count 27,900lp1, hemoglobin 9.5 ddl , and a platelet count of 28,00O/pl. The peripheral blood differential count now showed 62% myelomonoblasts and the bone marrow con-
0008-543)</8 1 /0901 / I 157 $0.90 0 American Cancer Society
1157
1158 CANCER September 1 1981 Vol. 48
TABLE 1. Allogeneic Mixed Lymphocyte Reaction
Responding Date cell
9/79 Patient Normal Normal
11/79 Patient Normal Normal
Stimulating cell
Normal Patient Normal
Patient N orma1
Normal
Mean net cpm (AEm-AAm)*
32,677 163,827 78,374
9,067 7,744
27,129
Percentage of normal
41.7 209.0 100.0
33.4 28.5
100.0
* A, responding cell; Bm, stimulating cell pretreated with mitomycin C; Am, responding cell pretreated with mitomycin C.
tained 67.8% myelomonoblasts as well. However, 29.2% of the bone marrow cells were morphologically similar to the lymphoblasts seen at the patient's initial presentation. The patient began reinduction chemotherapy with hydroxy- daunorubicin and cytosine arabinoside, but died several days after admission. A postmortem examination was not performed.
Materials and Methods
A 500-cell differential count was performed on each bone marrow aspirate previously stained with Wright-Giemsa material.
Cytochemical Stuins
Bone marrow aspirates and peripheral blood air- dried smears were stained for the presence of peroxidase;" neutral lipids (Sudan black B);3" ASD chloroacetate e s t e r a ~ e ; ~ ~ alpha-naphthyl butyrate es- terase;17 alpha-naphthyl acetate e s t e ra~e ; '~ acid phos- phatase;17 and periodic acid-Schiff (PAS) material.8
Immunologic Studies
Two milliliters of aspirated bone marrow or ten mil- liliters of peripheral blood were obtained in preservative-free heparin. Mononuclear cells were separated from other blood elements by centrifugation and a gradient composed of Ficoll and diatrizoate salts lymphocyte separation medium, (Litton Bionetics, Kensington, MD). Mononuclear cell suspensions were tested for non-immune rosette formation with sheep erythrocytes (E) according to the methods of Jondal et d . ' O and Wybran et al.,"j surface membrane immuno- globulin,'" and "Ia-like" antigen.*
Mixed lymphocyte reactions (MLR) were performed in triplicate according to the method of Bach and Voy- now.' Cultures were established using 2 x lo5 mitomycin C treated stimulating cells and 2 x lo5 re- sponding cells in volume of 0.20 ml culture medium. Sufficient normal human serum was added to the cul- ture medium to give a final concentration of 20%. One microcurie of tritiated thymidine was added to cultures
on the fifth day, cells were harvested 24 hours later, and incorporated radioactivity was measured in an ambient temperature liquid scintillation counter. The results are expressed as net counts (average counts per minute of stimulated culture minus average counts per minute of unstimulated culture) as a percentage of normal allogeneic MLR.
Liquid Culture
For liquid culture, 10 x lo6 blood mononuclear cells were suspended in 10 ml of McCoy's 5A medium, containing 15% fetal bovine serum, 100 unitdm1 penicillin, 50 pg/ml streptomycin and 40% conditioned medium and placed in a loosely capped 15 cm' (30-ml) tissue culture flask.6 Conditioned medium was pre- pared by incubating normal adherent blood cells for seven days in McCoy's 5A medium and 10 p~ 2- mer~aptoethanol.~ The liquid cultures were incubated for up to 25 days at 37 C in a humidified 5% C02-95% air atmosphere. Aliquots were removed every 48 to 72 hours for cell counts. Cell suspensions (1 x lo6 cells) underwent cytocentrifugation onto glass slides and stained with Wright-Giemsa and alpha-naphthyl ace- tate esterase. A 500-cell differential count was per- formed on each preparation.
Electron Microscopy
Small fragments of marrow aspirate or peripheral blood buffy coat preparations were fixed overnight in cold 2.5% phosphate-buffered isotonic glutaraldehyde, pH 7.35. After washing in an isotonic phosphate buffer, the tissue was sliced into 1 mm3 blocks and postfixed in phosphate-buffered osmium tetroxide. Dehydration through a graded series of ethanol and propylene oxide was followed by embedding in Aral- dite. Sections were cut with an LKB ultramicrotome and stained with uranyl acetate and lead citrate and examined in a Philips EM 300 electron microscope.
Results
Studies Performed on Neoplastic Cells Collected at Initia 1 Present a t ion
Studies performed on the bone marrow aspirates at the time of the patient's initial presentation demon- strated 81 2% lymphoblasts. The neoplastic cells con- tained a very high nuclear-to-cytoplasmic ratio and were less than 12 pm in diameter. The nuclei were often cleft and the nuclear chromatin was intermediate between fine and course. Auer rods were not observed in any cell.
Cytochemical stains of blasts were negative for peroxidase, Sudan black B, ASD chloroacetate es-
No. 5 AML DEVELOPING I N ALL . Madof le t al. 1159
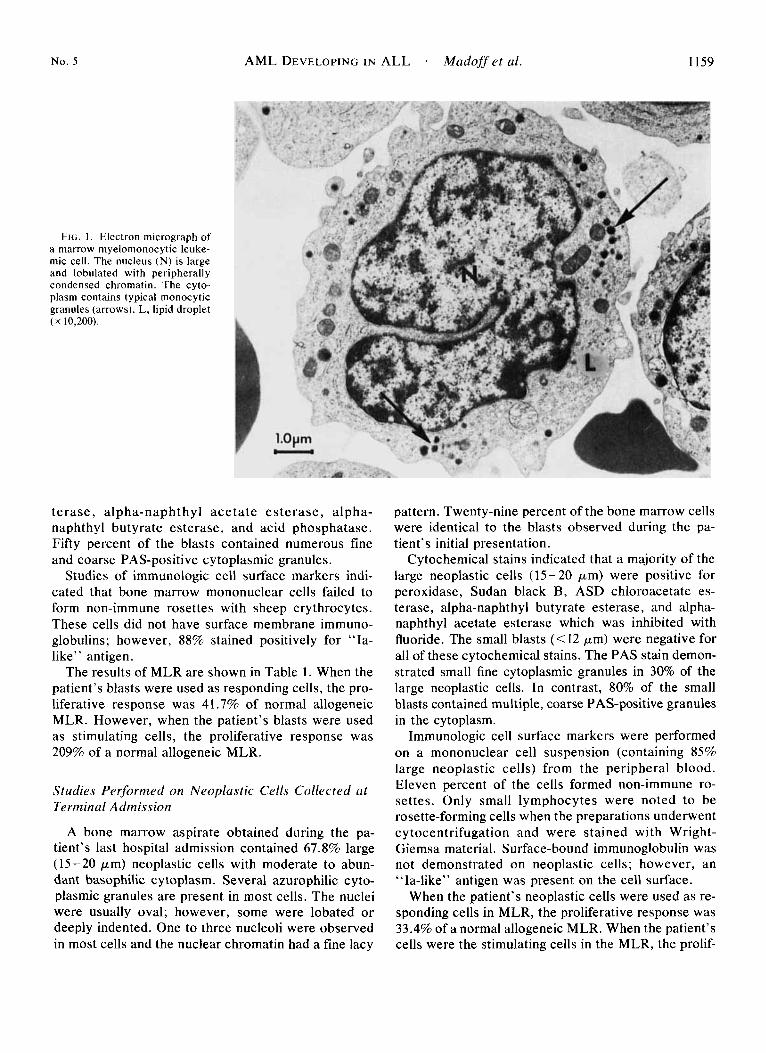
FIG. 1. Electron micrograph of a marrow myelomonocytic leuke- mic cell. The nucleus (N) is large and lobulated with peripherally condensed chromatin. The cyto- plasm contains typical rnonocytic granules (arrows). L, lipid droplet ( X 10,200).
terase, alpha-naphthyl ace ta te es terase, alpha- naphthyl butyrate esterase, and acid phosphatase. Fifty percent of the blasts contained numerous fine and coarse PAS-positive cytoplasmic granules.
Studies of immunologic cell surface markers indi- cated that bone marrow mononuclear cells failed to form non-immune rosettes with sheep erythrocytes. These cells did not have surface membrane immuno- globulins; however, 88% stained positively for “Ia- like” antigen.
The results of MLR are shown in Table 1. When the patient’s blasts were used as responding cells, the pro- liferative response was 41.7% of normal allogeneic MLR. However, when the patient’s blasts were used as stimulating cells, the proliferative response was 209% of a normal allogeneic MLR.
Studies Performed on Neoplastic Cells Collected at Terminal Admission
A bone marrow aspirate obtained during the pa- tient’s last hospital admission contained 67.8% large (15-20 pm) neoplastic cells with moderate to abun- dant basophilic cytoplasm. Several azurophilic cyto- plasmic granules are present in most cells. The nuclei were usually oval; however, some were lobated or deeply indented. One to three nucleoli were observed in most cells and the nuclear chromatin had a fine lacy
pattern. Twenty-nine percent of the bone marrow cells were identical to the blasts observed during the pa- tient’s initial presentation.
Cytochemical stains indicated that a majority of the large neoplastic cells (15-20 pm) were positive for peroxidase, Sudan black B, ASD chloroacetate es- terase, alpha-naphthyl butyrate esterase, and alpha- naphthyl acetate esterase which was inhibited with fluoride. The small blasts (< 12 pm) were negative for all of these cytochemical stains. The PAS stain demon- strated small fine cytoplasmic granules in 30% of the large neoplastic cells. In contrast, 80% of the small blasts contained multiple, coarse PAS-positive granules in the cytoplasm.
Immunologic cell surface markers were performed on a mononuclear cell suspension (containing 85% large neoplastic cells) from the peripheral blood. Eleven percent of the cells formed non-immune ro- settes. Only small lymphocytes were noted to be rosette-forming cells when the preparations underwent cytocentrifugation and were stained with Wright- Giemsa material. Surface-bound immunoglobulin was not demonstrated on neoplastic cells; however, an “Ia-like” antigen was present on the cell surface.
When the patient’s neoplastic cells were used as re- sponding cells in MLR, the proliferative response was 33.4% of a normal allogeneic MLR. When the patient’s cells were the stimulating cells in the MLR, the prolif-
1160 CANCER September I 1981 Vol. 48
erative response was only 28.5% of a normal al- logeneic MLR.
Liquid Cultures
Total cell counts remained unchanged ( 1 x lo6 cells/ml) for the first five days in culture, decreased by 50% (0.5 x lofi cells/ml) after eleven days, and no cells were observed in culture after 25 days. Prior to cul- ture, 85% of the cells were myelomonoblasts and 15% were mature lymphocytes. The cytoplasm of all the blasts stained diffusely with alpha-naphthyl acetate esterase. After eight days in culture, less than 1% of the cells were blasts, 70% were small (8-9 pm) lym- phocytes and 28% were large (30 pm) macrophages with mature nuclei and cytoplasm-containing phagocytized debris. These macrophages were adher- ent to the bottom of the tissue culture flask and stained strongly positive with alpha-naphtyl acetate esterase. After 1 1 to 25 days of culture, the majority (>75%) of the cells were macrophages.
Electron Microscopic Studies
Ultrastructural examination of the marrow and peripheral blood buffy coat from the last hospital ad- mission demonstrated that the majority of cells were large, immature cells having the typical electron mi- croscopic appearance of myelomonocytic leukemic
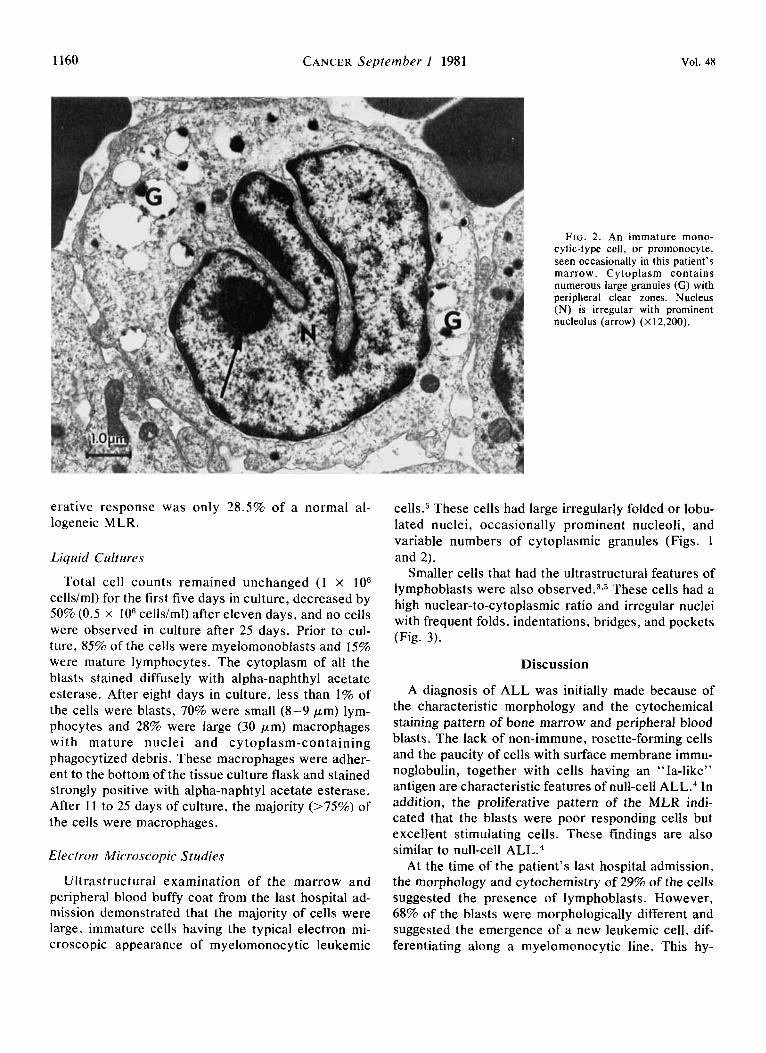
FIG. 2. An immature mono- cytic-type cell, or promonocyte, seen occasionally in this patient’s marrow. Cytoplasm contains numerous large granules (G) with peripheral clear zones. Nucleus (N) is irregular with prominent nucleolus (arrow) (X12,200).
cells5 These cells had large irregularly folded or lobu- lated nuclei, occasionally prominent nucleoli, and variable numbers of cytoplasmic granules (Figs. 1 and 2).
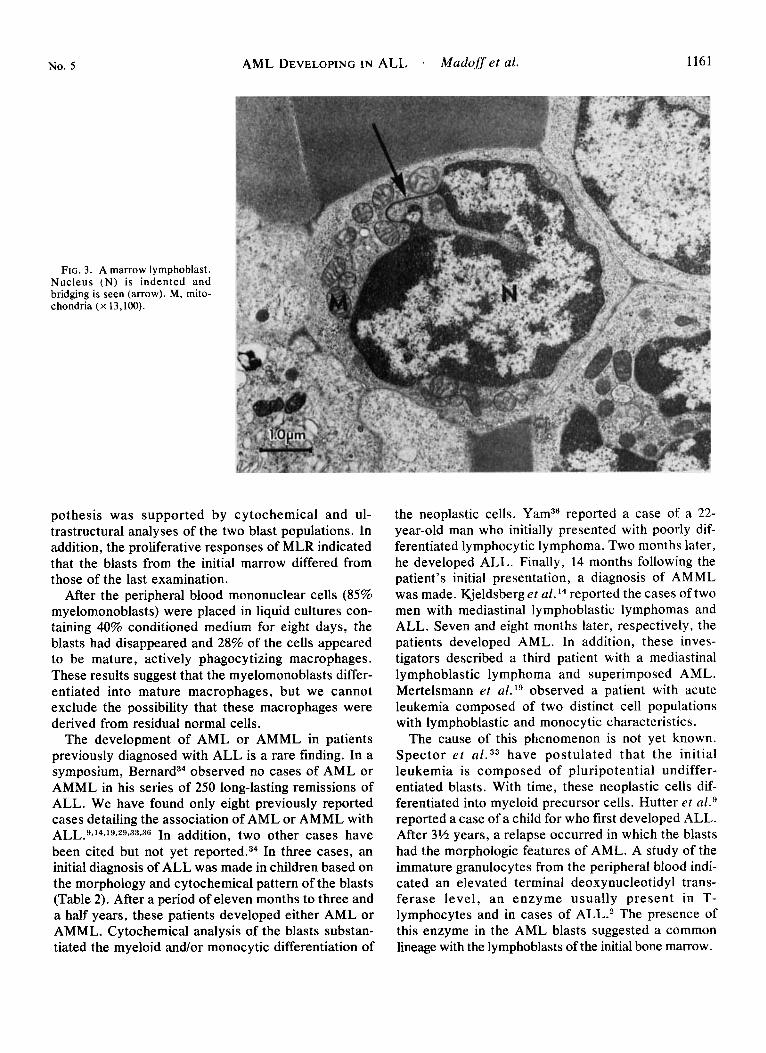
Smaller cells that had the ultrastructural features of lymphoblasts were also o b s e r ~ e d . ~ , ~ These cells had a high nuclear-to-cytoplasmic ratio and irregular nuclei with frequent folds, indentations, bridges, and pockets (Fig. 3).
Discussion
A diagnosis of ALL was initially made because of the characteristic morphology and the cytochemical staining pattern of bone marrow and peripheral blood blasts. The lack of non-immune, rosette-forming cells and the paucity of cells with surface membrane immu- noglobulin, together with cells having an “Ia-like” antigen are characteristic features of null-cell ALL.4 In addition, the proliferative pattern of the MLR indi- cated that the blasts were poor responding cells but excellent stimulating cells. These findings are also similar to null-cell ALL.4
At the time of the patient’s last hospital admission, the morphology and cytochemistry of 29% of the cells suggested the presence of lymphoblasts. However, 68% of the blasts were morphologically different and suggested the emergence of a new leukemic cell, dif- ferentiating along a myelomonocytic line. This hy-
No. 5 AML DEVELOPING IN ALL . Madoffet al. 1161
FIG. 3 . A marrow lymphoblast. Nucleus (N) is indented and bridging is seen (arrow). M, mito- chondria (x 13,100).
pothesis was supported by cytochemical and ul- trastructural analyses of the two blast populations. In addition, the proliferative responses of MLR indicated that the blasts from the initial marrow differed from those of the last examination.
After the peripheral blood mononuclear cells (85% myelomonoblasts) were placed in liquid cultures con- taining 40% conditioned medium for eight days, the blasts had disappeared and 28% of the cells appeared to be mature, actively phagocytizing macrophages. These results suggest that the myelomonoblasts differ- entiated into mature macrophages, but we cannot exclude the possibility that these macrophages were derived from residual normal cells.
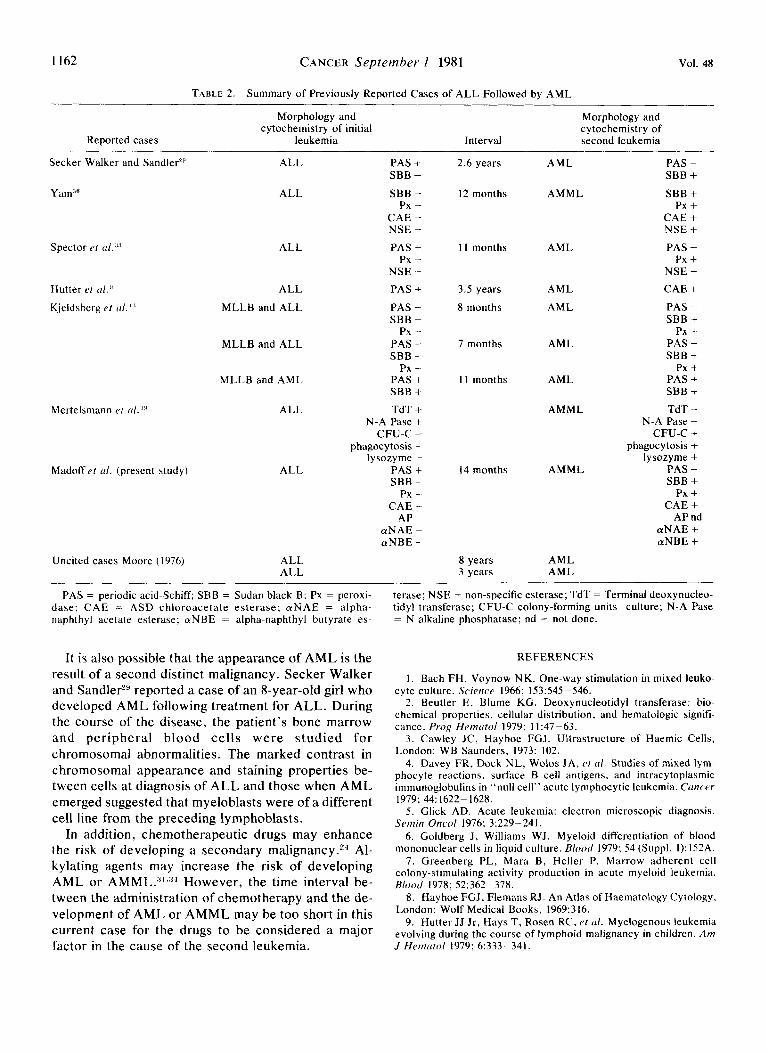
The development of AML or AMML in patients previously diagnosed with ALL is a rare finding. In a symposium, Bernard34 observed no cases of AML or AMML in his series of 250 long-lasting remissions of ALL. We have found only eight previously reported cases detailing the association of AML or AMML with ALL.9,14,19,29,33*36 In addition, two other cases have been cited but not yet In three cases, an initial diagnosis of ALL was made in children based on the morphology and cytochemical pattern of the blasts (Table 2). After a period of eleven months to three and a half years, these patients developed either AML or AMML. Cytochemical analysis of the blasts substan- tiated the myeloid andor monocytic differentiation of
the neoplastic cells. Yam36 reported a case of a 22- year-old man who initially presented with poorly dif- ferentiated lymphocytic lymphoma. Two months later, he developed ALL. Finally, 14 months following the patient’s initial presentation, a diagnosis of AMML was made. Kjeldsberg et al. l4 reported the cases of two men with mediastinal lymphoblastic lymphomas and ALL. Seven and eight months later, respectively, the patients developed AML. In addition, these inves- tigators described a third patient with a mediastinal lymphoblastic lymphoma and superimposed AML. Mertelsmann et a1.19 observed a patient with acute leukemia composed of two distinct cell populations with lymphoblastic and monocytic characteristics.
The cause of this phenomenon is not yet known. Spector e t have postulated that the initial leukemia is composed of pluripotential undiffer- entiated blasts. With time, these neoplastic cells dif- ferentiated into myeloid precursor cells. Hutter et ~ 1 . ~ reported a case of a child for who first developed ALL. After 3% years, a relapse occurred in which the blasts had the morphologic features of AML. A study of the immature granulocytes from the peripheral blood indi- cated an elevated terminal deoxynucleotidyl trans- ferase level, an enzyme usually present in T- lymphocytes and in cases of ALL.* The presence of this enzyme in the AML blasts suggested a common lineage with the lymphoblasts of the initial bone marrow.
1162 CANCER September 1 1981 Vol. 48
TABLE 2. Summary of Previously Reported Cases of ALL Followed by AML
Reported cases
Morphology and cytochemistry of initial
leukemia
Morphology and cytochemistry of
Interval second leukemia
Secker Walker and Sandier'!'
Yam:’fi
ALL
ALL
Spector e f ~ 1 : ’ : ’ ALL
Hutter ei (ti.!’
Kjeldsberg e f ( I / . I.‘
Mertelsmann ei (11 . ‘!I
Madoff e f d. (present study)
Uncited cases Moore (1976)
ALL
MLLB and ALL
MLLB and ALL
MLLB and AML
ALL
ALL
ALL ALL
PAS + SBB -
SBB - Px -
CAE - NSE - PAS +
Px - NSE - PAS + PAS - SBB -
Px - PAS - SBB -
Px - PAS + SBB + TdT +
N-A Pase +
phagocytosis - lysozyme -
PAS + SBB -
Px - CAE -
AP - aNAE - aNBE -
CFU-C -
2.6 years
12 months
1 1 months
3.5 years
8 months
7 months
1 1 months
14 months
8 years 3 years
AML
AMML
AML
AML
AML
AML
AML
AMML
AMML
AML AML
.-
PAS - SBB + SBB +
Px + CAE + NSE + PAS -
Px + NSE - CAE + PAS - SBB +
Px + PAS - SBB +
Px + PAS + SBB +
N-A Pase -
phagocytosis + lysozyme +
PAS - SBB +
Px + CAE +
AP nd aNAE + aNBE +
TdT -
CFU-C +
PAS = periodic acid-Schiff; SBB = Sudan black B: Px = peroxi- dase; CAE = ASD chloroacetate esterase: a N A E = alpha- naphthyl acetate esterase; aNBE = alpha-naphthyl butyrate es-
terase; NSE = non-specific esterase; TdT = Terminal deoxynucleo- tidy1 transferase; CFU-C colony-forming units-culture; N-A Pase = N alkaline phosphatase: nd = not done.
It is also possible that the appearance of AML is the result of a second distinct malignancy. Secker Walker and SandlerL9 reported a case of an 8-year-old girl who developed AML following treatment for ALL. During the course of the disease, the patient’s bone marrow and peripheral blood cells were s tudied for chromosomal abnormalities. The marked contrast in chromosomal appearance and staining properties be- tween cells at diagnosis of ALL and those when AML emerged suggested that myeloblasts were of a different cell line from the preceding lymphoblasts.
In addition, chemotherapeutic drugs may enhance the risk of developing a secondary m a l i g n a n ~ y . ~ ~ Al- kylating agents may increase the risk of developing AML or AMML.:”.:’4 However, the time interval be- tween the administration of chemotherapy and the de- velopment of AML or AMML may be too short in this current case for the drugs to be considered a major factor in the cause of the second leukemia.
REFERENCES
1 . Bach FH, Voynow NK. One-way stimulation in mixed leuko- cyte culture. Scierrre 1966; 153:545-546.
2. Beutler E, Blume KG. Deoxynucleotidyl transferase: bio- chemical properties, cellular distribution, and hematologic signifi- cance. Prog Heintrfol 1979: 11:47-63.
3. Cawley JC, Hayhoe FGJ. Ultrastructure of Haemic Cells, London: WB Saunders, 1973: 102.
4 . Davey FR, Dock NL, Wolos JA, et r i l . Studies of mixed lym- phocyte reactions, surface B cell antigens, and intracytoplasmic immunoglobulins in “null cell” acute lymphocytic leukemia. Cancer
5. Glick AD. Acute leukemia: electron microscopic diagnosis. Semin Oncol 1976; 3:229-241.
6. Goldberg J , Williams WJ. Myeloid differentiation of blood mononuclear cells in liquid culture. Blood 1979; 54 (Suppl. 1): 152A.
7 . Greenberg PL, Mara B, Heller P. Marrow adherent cell colony-stimulating activity production in acute myeloid leukemia.
8. Hayhoe FGJ, Flemans RJ. An Atlas of Haematology Cytology, London: Wolf Medical Books, 1969:316.
9. Hutter JJ Jr, Hays T. Rosen RC, r f (11. Myelogenous leukemia evolving during the course of lymphoid malignancy in children. Am J Hemnfol 1979; 6:333-341.
1979; 44: 1622- 1628.
R l ~ d 1978; 52:362-378.

No. 5 AML DEVELOPING IN ALL . Madoffet al. 1163
10. Jondal M, Holm G, Wigzell H. Surface markers on human T and B lymphocytes. 1. A large population of lymphocytes forming non-immune rosettes with sheep red blood cells. J Exp Med 1972;
1 I . Kaplow LS- Substitute for benzidine in myeloperoxidase stains. Am J Clin Pathol 1975; 63:451.
12. Karanas A, Silver RT. Characteristics of the terminal phase of chronic granulocytic leukemia. Blood 1968; 32:445-459.
13. Khaleeli M, Keane WM, Lee GR. Sideroblastic anemia in multiple myeloma: a preleukemic change. Blood 1973; 41: 17-25.
14. Kjeldsberg CR, Nathwani BN, Rappaport H. Acute myelo- blastic leukemia developing in patients with mediastinal lympho- blastic lymphoma. Cancer 1979: 44:2316- 2323.
15. Kyle RA, Pierre RV, Bayrd ED. Multiple myeloma and acute myelomonocytic leukemia. N Engl J Med 1970; 283:I 121-1 125.
16. Li CY, Yam LT, Lam KW. Acid phosphatase isoenzyme in human leukocytes in normal and pathologic conditions. J Histochem Cytochem 1970, 18:473-481.
17. Li CY, Lam KW, Yam LT. Esterase in human leukocytes. J Hisfochem Cytochem 1973; 21:l- 1 1 .
18. McPhedran P, Heath CW. Acute leukemia occurring during chronic lymphocytic leukemia. Blood 1970; 35:7-1 I .
19. Mertelsmann R, Koziner B, Ralph P, et al. Evidence for dis- tinct lymphocytic and monocytic populations in a patient with ter- minal transferase-positive acute leukemia. Blood 1978;
20. Newman DR, Maldonado JE , Harrison EG, e t a / . Myelomonocytic leukemia in Hodgkin’s disease. Cancer 1970;
21. O’Neill BJ, McCredie KB, Raik E, et a/ . Mixed leukemia: a report of three cases. Med J Aust 1970: 2:586-591.
22. Osserman EF. Monocytic and monomyelocytic leukaemia with increased serum and urine lysozyme as a late complication in plasma cell myeloma. Br Med J 1971; 2:327.
23. Papamichail M, Brown JC, Holborow EJ. Immunoglobulins on the surface of human lymphocytes. Lancet 1971; 2:850-851.
24. Penn I: Leukemias and lymphomas associated with the use of cytotoxic and immunosuppressive drugs. Recent ReJults Cancer
136:207 -2 15.
51:1051- 1056.
25:128- 140.
R ~ s 1979: 69:7-13.
25. Peterson LC, Bloomfield CD, Brunning RD. Blast crisis as an initial or terminal manifestation of chronic myeloid leukemia. A study of 28 patients. Am J Med 1976; 60:209-220.
26. Roberts PD, Forster PM. Chronic lymphocytic leukaemia as- sociated with acute myelomonocytic leukaemia. Br J Haemafol
27. Rosner F, Grunwald H . For acute leukemia group B: Hodgkin’s disease and acute leukemia. Report of eight cases and review of the literature. Am J Med 1975; 58:339-353.
28. Sahakian GJ, Al-Mondhiry H , Lacher MJ, et a / . Acute leukemia in Hodgkin’s disease. Cancer 1974; 33: 1369- 1375.
29. Secker Walker LM, Sandler RM. Acute rnyeloid leukaemia with monosomy-7 follows acute lymphoblastic leukaemia. Br J Haematol 1978; 38:359-366.
30. Sheehan HL, Storey GW. An improved method of staining leukocyte granules with Sudan black B. J Pathol Bact 1947;
31. Sieber SM. Cancer chemotherapeutic agents and carcino- genesis. Cancer Chemorher Rep 1975; 59:915-918.
32. Silverstein MN, Goldberg JD, Balcerzak SP, et a/. The inci- dence of acute leukemia in a randomized clinical trial for polycythemia Vera. Blood 1979; 54 (Suppl 1):209A.
33. Spector G, Youness E, Gulbert J . Acute lymphoblastic leukemia followed by acute granulocytic leukemia in a pediatric pa- tient. Am J Clin Pathol 1979; 72~242-245.
34. Tchernia G, Mielot F, Subtil E, ef al. Acute myeloblastic leu- kemia after irnmunodepressive therapy for primary nonmalignant dis- ease. Blood Cells 1979; 2:67-80.
35. Wybran J , Carr MC, Fudenberg HH. The human rosette- forming cell as a marker of a population of thymus-derived cells. J Clin Invest 1972; 51~2537-2543.
36. Yam LT. Acute myelomonocytic leukemia: coexistent cytochemical markers for monocytes and granulocytes in leukemic cells. South Med J 1979; 72:670-672.
37. Yam LT, Li CY, Crosby WH. Cytochemical identification of monocytes and granulocytes. Am J Clin Puthol 1971; 55:283-290.
38. Zarrabi MH, Grunwald HW, Rosner F. Chronic lymphocytic leukemia terminating in acute leukemia. Arch Intern Med 1977;
1973; 25:203 - 206.
54:336-337.
137:1059- 1064.