the cardiorespiratory system. size of a fist weighs
TRANSCRIPT
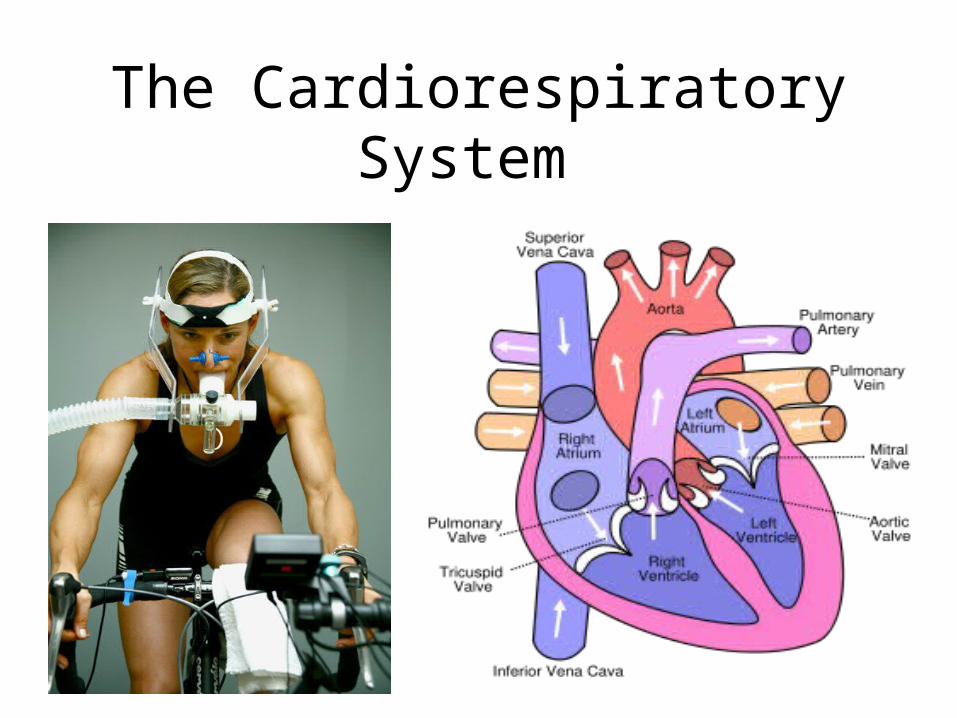
The Cardiorespiratory System
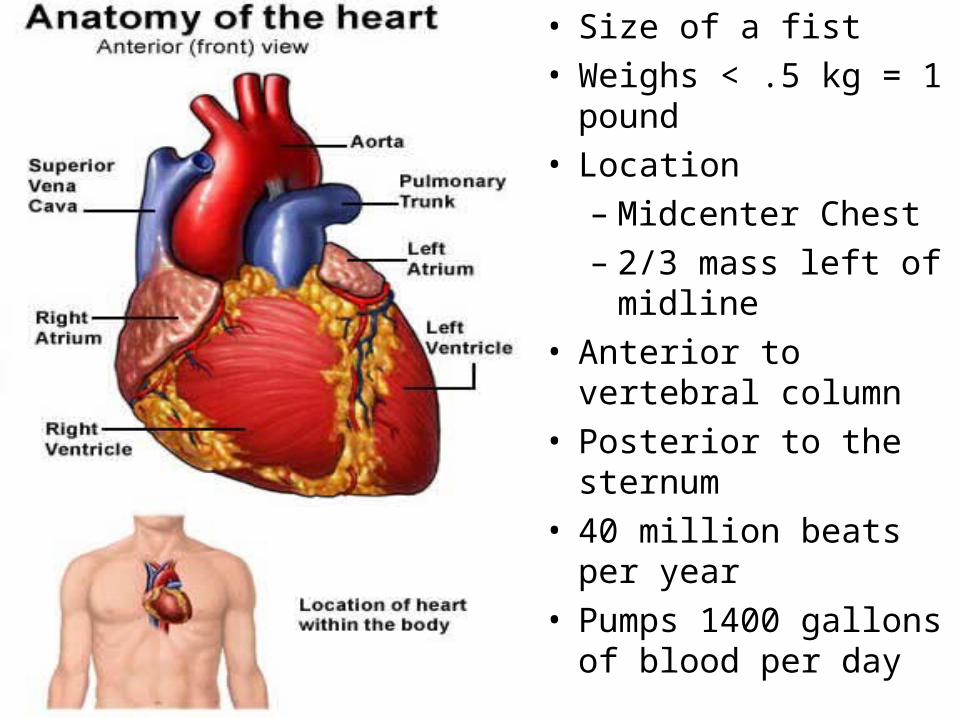
• Size of a fist
• Weighs < .5 kg = 1 pound
• Location
– Midcenter Chest
– 2/3 mass left of midline
• Anterior to vertebral column
• Posterior to the sternum
• 40 million beats per year
• Pumps 1400 gallons of blood per day
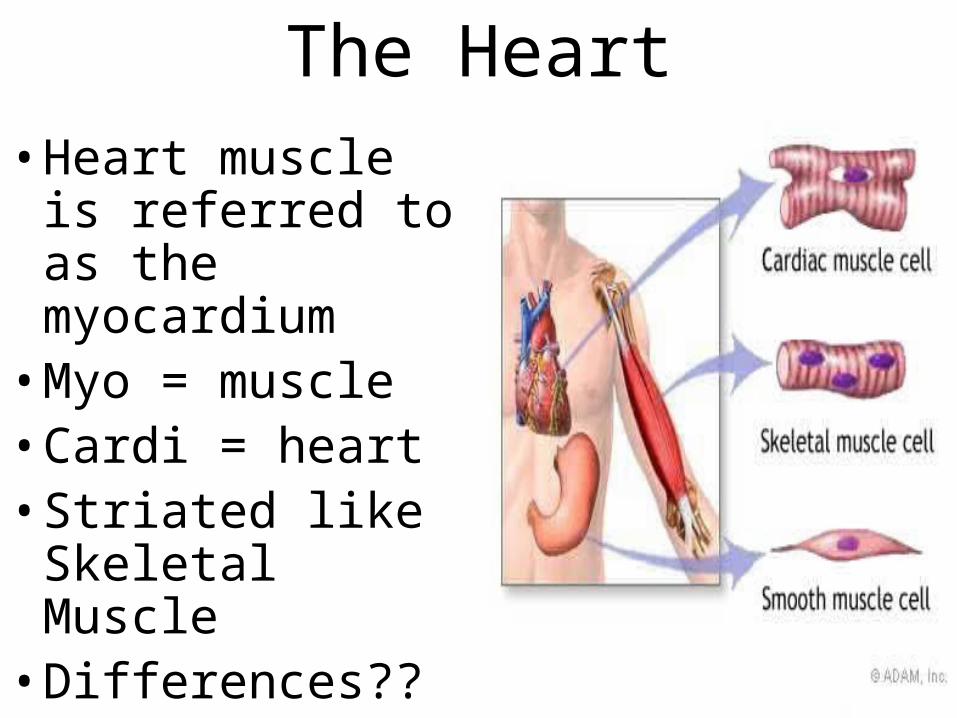
The Heart• Heart muscle is
referred to as the myocardium
• Myo = muscle• Cardi = heart• Striated like
Skeletal Muscle• Differences??
The Heart• 3 Areas of Heart Tissue
– Atrial – Mechanical Contraction
– Ventricular – Mechanical Contraction
– Conductive – Electrical Transmitter
• Conductive tissue – Lies between the atria and ventricles
– Facilitates rapid transmission of electrical impulses
– Transmission allows coordinated actions between atria and ventricles to pump
Heart Circulation Video• http://www.youtube.com/watch?v=D3ZDJgFD
dk0&feature=related

2 Separate Pumps That Serve 2 Circulations
• Pulmonary Circuit: –The right side of the heart–Receives blood from all parts of the body –Pumps deoxygenated blood to the lungs
• Systemic Circuit: –The left side of the heart –Receives oxygenated blood from the lungs–Pumps it out to all body tissues
Atria and Ventricles• Left and Right Atria:
– Superior 2 chambers where blood enters the heart
– Function as blood reservoirs, delivering blood into the right and left ventricles
• Left and Right Ventricles:
– Inferior 2 chambers which pump blood away from the heart
– Thick musculature – Athletes vs. Sedentary
– Forceful contraction powers ejection of blood through the entire body
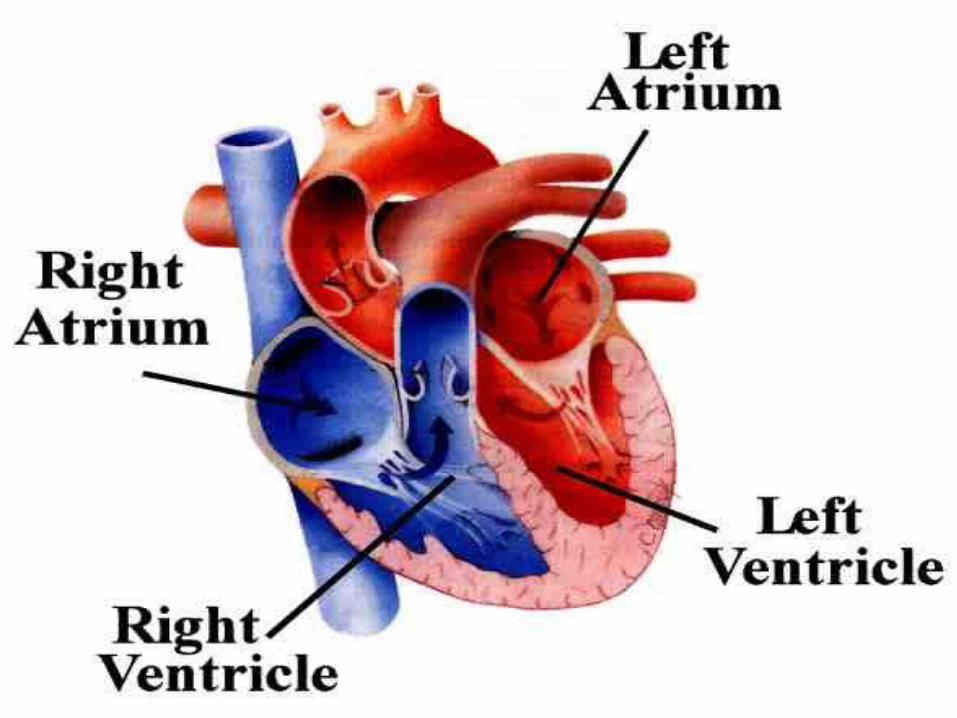
Right Atrium• 3 large veins return blood from the body to the Right
atrium: – Superior Vena Cava– Inferior Vena Cava– Coronary Sinus
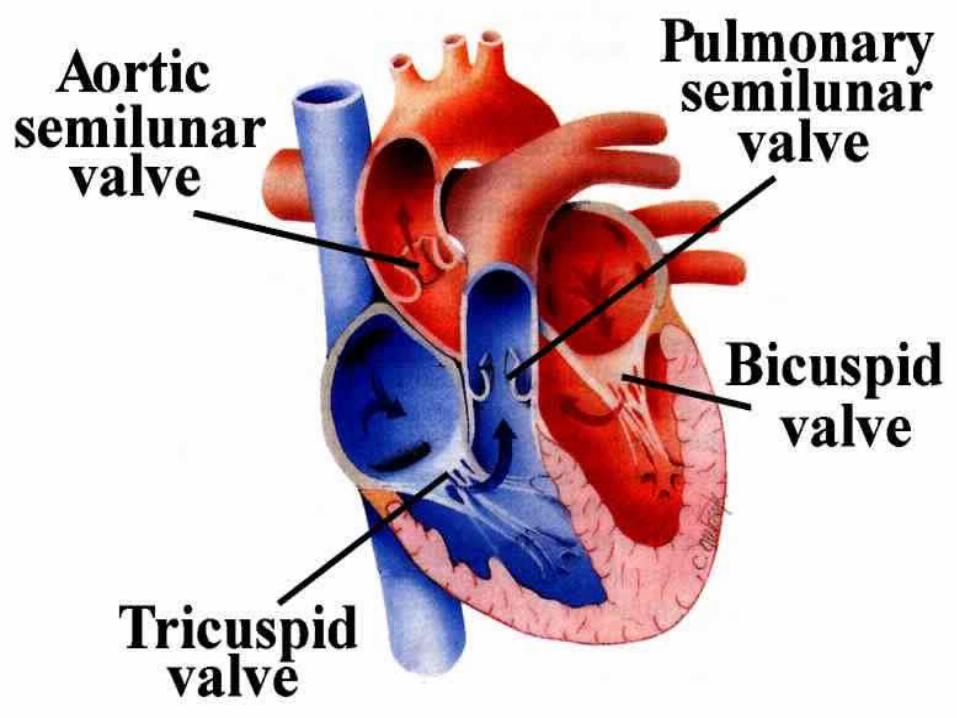
• Blood flows R atrium to R ventricle through the Tricuspid valve:
– Three cusps that allow only uni-directional flow – Prevents backflow of blood from the right ventricle
to the right atrium when the ventricles contract (systole)
• As the ventricles contract, blood is forced behind the 3 valve flaps forcing them upward and together to close the valve
Left Atrium• Receives Oxygenated blood from
the lungs by the Pulmonary Veins
• Blood flows into the L ventricle through the L bicuspid or mitral valve.
• Bicuspid (Mitral) valve prevents backflow of blood from the L ventricle to the L atrium during L ventricular contraction
Right and Left Ventricles
• Actual pumps of the heart
• Right ventricle pumps deoxygenated blood to the lungs
– Gas exchange occurs at lungs (respiration)
• The left ventricle ejects oxygenated blood into the aorta via the systemic circuit to all body tissues
2 Semilunar Valves• Located on the arterial walls on the outside of the
ventricles• Prevent blood from flowing back into the heart
between contractions• Aortic Semilunar Valve: Left
– Prevents backflow of blood from atria into ventricles left side of heart during ventricular relaxation (diastole)
• Pulmonary Semilunar Valve: Right– Prevents backflow of blood from atria into
ventricles from right side of heart during ventricular relaxation (diastole)
Heart Valves Video
• http://www.youtube.com/watch?v=H04d3rJCLCE&feature=related

Path of Blood Through The Heart• Deoxygenated blood enters R atrium from veins thru
Superior vena cava and Inferior vena cava– Where has this blood come from and why no 02?
• R atrium → tricuspid valve → R ventricle → pulmonary semilunar valve → pulmonary arteries → lungs
• Blood exchanges CO2 for fresh O2 in lungs – Blood returns to heart via pulmonary veins → L
atrium• L atrium → bicuspid valve → L ventricle → aortic
semilunar valve → aorta → all arteries of the body delivering 02, nutrients and carrying away CO2, waste products
• Back to Step 1…Deoxygenated blood enters R atrium…..
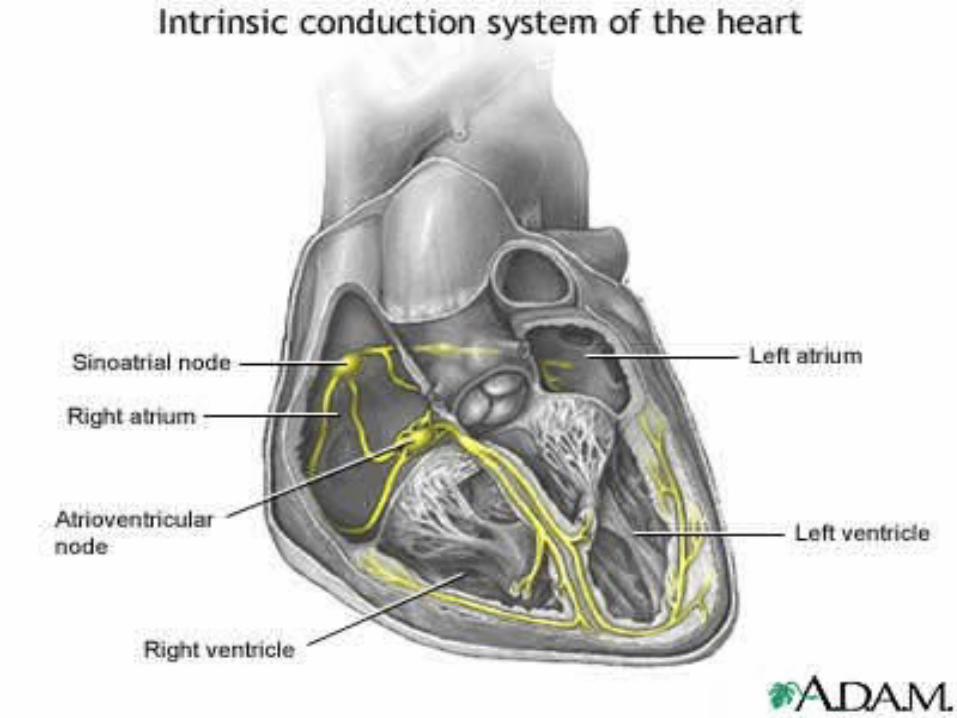
Conduction System• The Sinoatrial (SA) Node:
– Pacemaker of heart – sets rhythm– Normal heart beat begins with an electrical impulse
from the SA (sinoatrial) node– SA Node located in Upper right atrium– The impulse spreads throughout the atria, causing them to
contract
• Atrioventricular (AV) Node: – Electrical impulse travels through the AV
(atrioventricular) node into the conduction fibers located in ventricles
– Located in lower right atrium – As the impulse travels down the fibers, the
ventricles contract. The cycle repeats
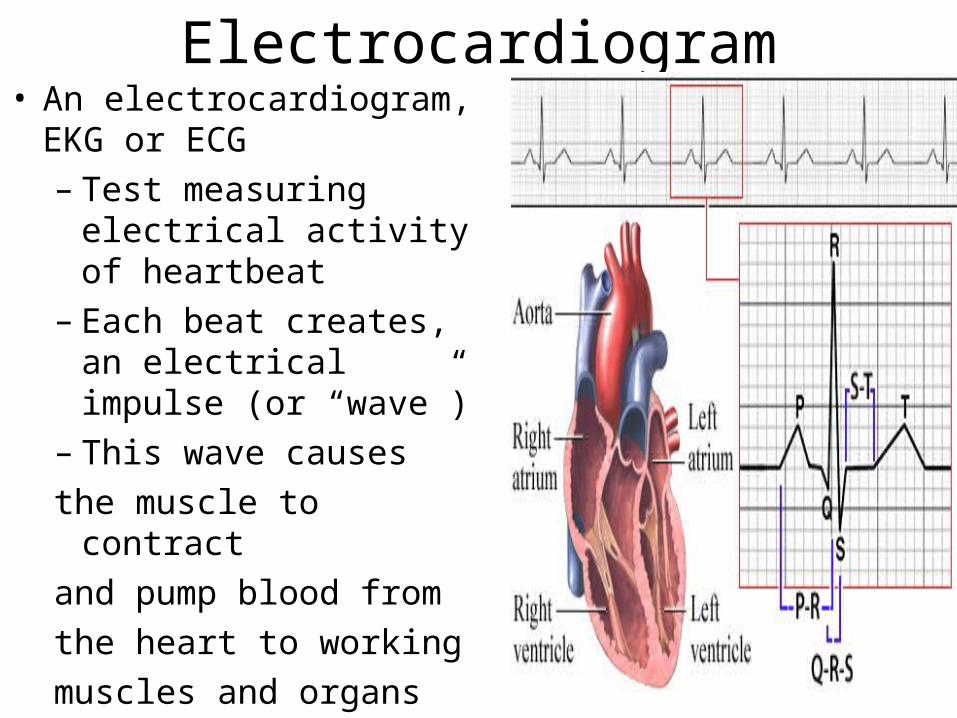
Electrocardiogram• An electrocardiogram, EKG
or ECG– Test measuring
electrical activity of heartbeat
– Each beat creates, an electrical impulse (or “wave”)
– This wave causes
the muscle to contract
and pump blood from
the heart to working
muscles and organs
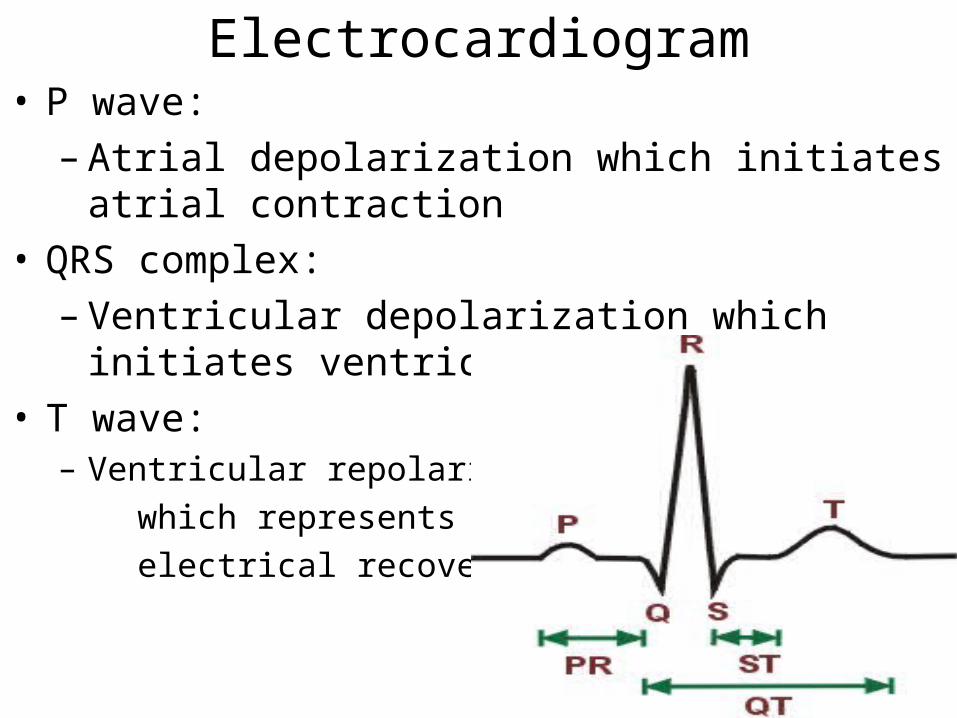
Electrocardiogram• P wave:
– Atrial depolarization which initiates atrial contraction
• QRS complex:
– Ventricular depolarization which initiates ventricular contraction
• T wave: – Ventricular repolarization
which represents
electrical recovery
Conduction System Video
• http://www.youtube.com/watch?v=nK0_28q6WoM&feature=related

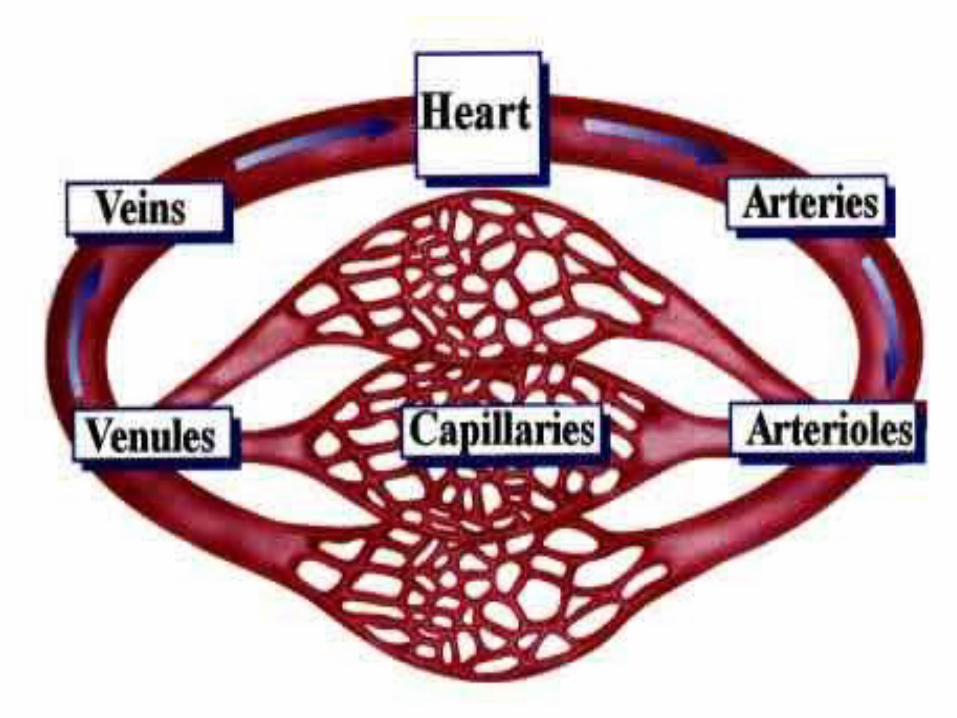
Blood Vessels• Arteries: Transporters
– Transport blood AWAY from the heart. Transport oxygenated blood only. (*except* in the case of the pulmonary artery).
• Arterioles: Regulators– Transport blood from arteries to capillaries.– Main regulators of blood flow and blood
pressure• Capillaries: Exchangers
– Exchange of 02, CO2, H2O, hormones, electrolytes, and other nutrients between the blood and the surrounding body tissues
– Remove waste products from surrounding cells
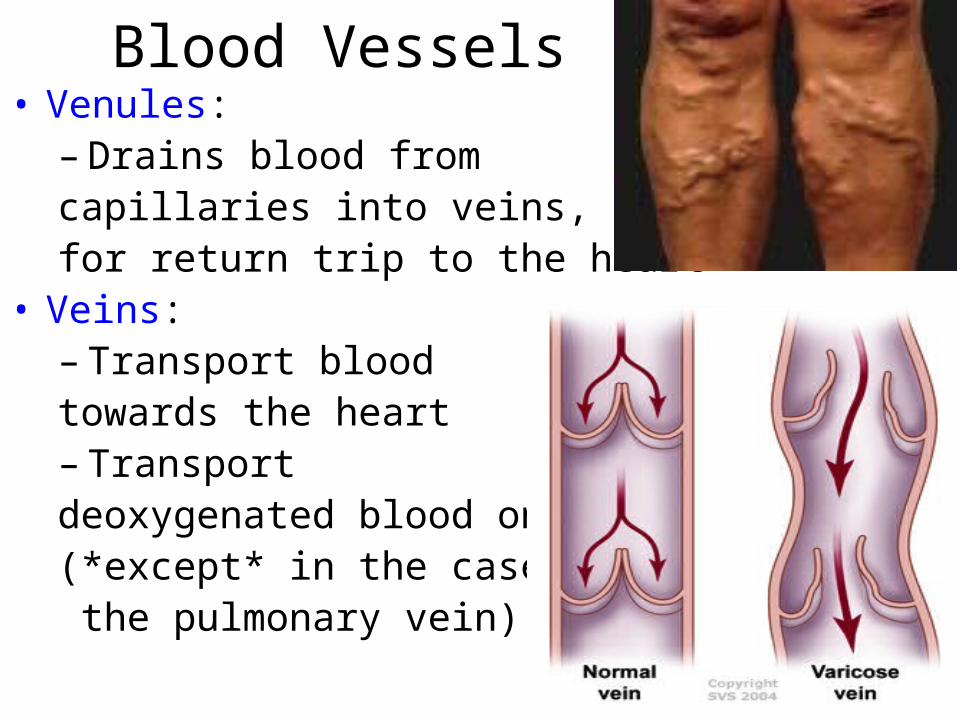
Blood Vessels• Venules:
– Drains blood from capillaries into veins, for return trip to the heart
• Veins: – Transport blood towards the heart– Transport deoxygenated blood only (*except* in the case of the pulmonary vein)
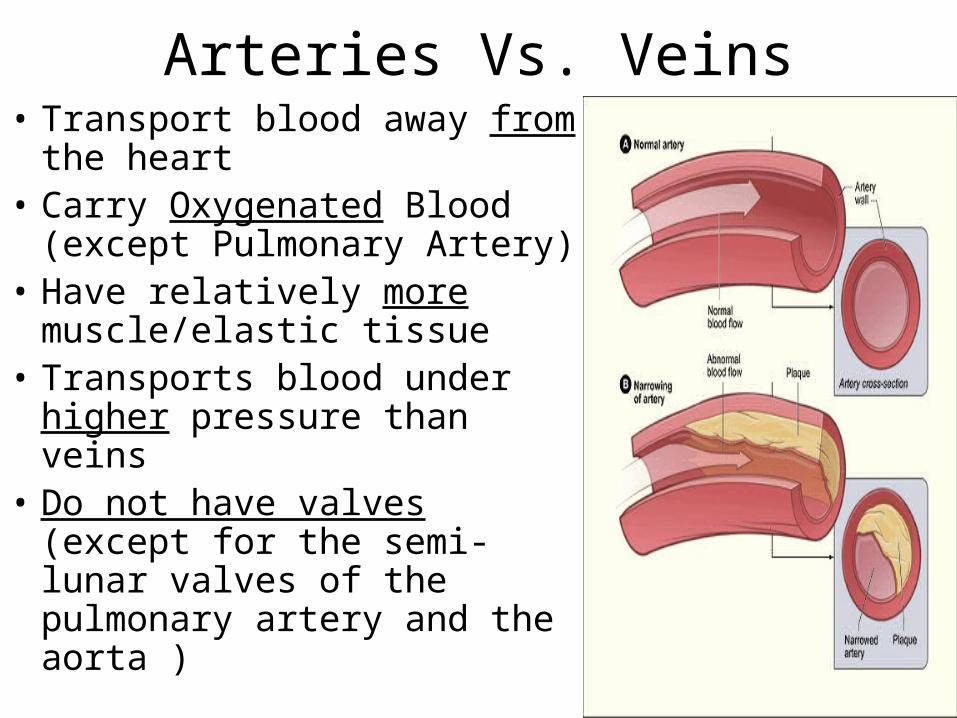
Arteries Vs. Veins• Transport blood away from
the heart • Carry Oxygenated Blood
(except Pulmonary Artery)• Have relatively more
muscle/elastic tissue• Transports blood under
higher pressure than veins • Do not have valves (except
for the semi-lunar valves of the pulmonary artery and the aorta )
Veins vs. Arteries• Transport blood towards the heart• Carry De-oxygenated Blood
Exception -- Pulmonary Vein• Have relatively less muscle/elastic tissue • Transports blood under lower pressure (than
arteries)• Have one-way valves throughout the main
veins of the body• Valves prevent blood flowing in the wrong
direction, as this could (in theory) return waste materials to the tissues
Cardiac Output (Q)• Total volume (amount) of blood
pumped by the heart in one minute
• Measured in liters (L) or milliliters (ml)
• Typically males have about 5.5 L of blood and females 5 L of blood
• Why the gender difference??
• Product of heart rate (HR) and stroke volume (SV)

Measuring Cardiac Output (Q)• Cardiac Output depends on:
– Heart rate (HR): number of times the heart contracts per minute (60-80 bpm)
– Stroke Volume (SV): the volume of blood ejected with each stroke or beat (60-80ml)
– Cardiac output computes as follows:
• Cardiac output = Heart rate x Stroke volume
• A-VO2 Difference:
– The difference in the oxygen content of arterial blood versus venous blood and is expressed in ml of O2 per 100 ml of blood
Stroke Volume• SV is determined by:
–End Diastolic Volume (EDV): how much blood your heart can accommodate
–End Systolic Volume (ESV): how completely it can empty
• Both EDV and ESV are a result of the number, size, and the strength of the muscle fibers –Left ventricular mass –Maximal contractility–How large the blood volume (preload) –How much the arteries can dilate (afterload)–Size of the pericardium.
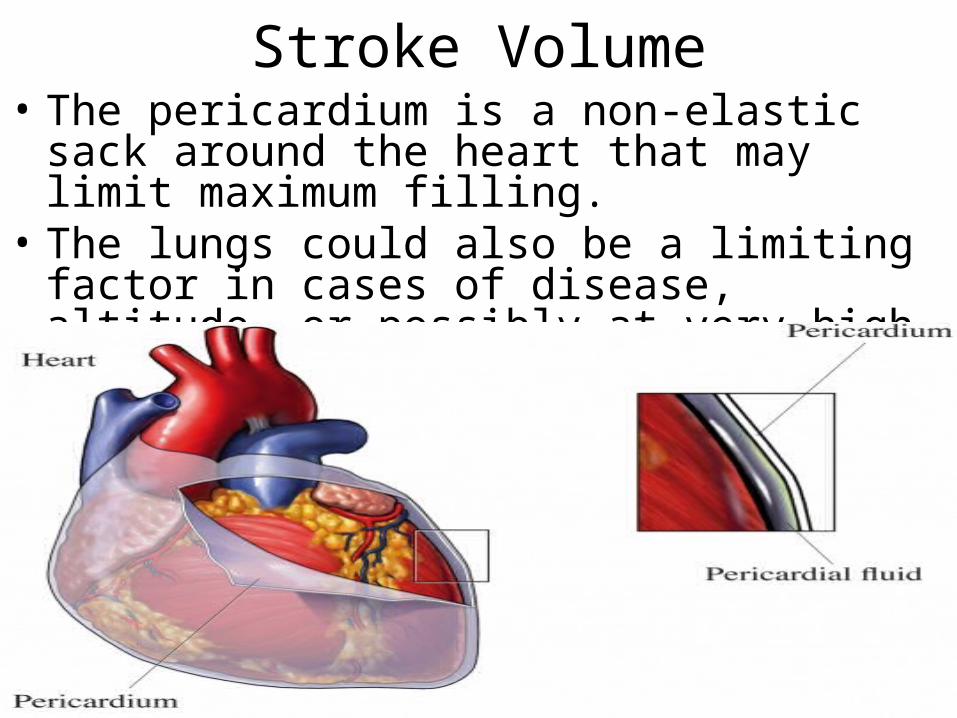
Stroke Volume• The pericardium is a non-elastic sack around
the heart that may limit maximum filling. • The lungs could also be a limiting factor in
cases of disease, altitude, or possibly at very high work loads.
Measuring Cardiac Output• For an untrained person who has a resting
heart rate of 72 bpm and a stroke volume of 70 ml the resting cardiac output is:
– Cardiac output = HR x SV
– Cardiac output = 72 x 70
– Cardiac output = 5040 ml/min
– Cardiac output = 5.04 L/min
– (Note: 1000ml = 1L)
• At rest average heart pumps about 5 liters of blood per minute
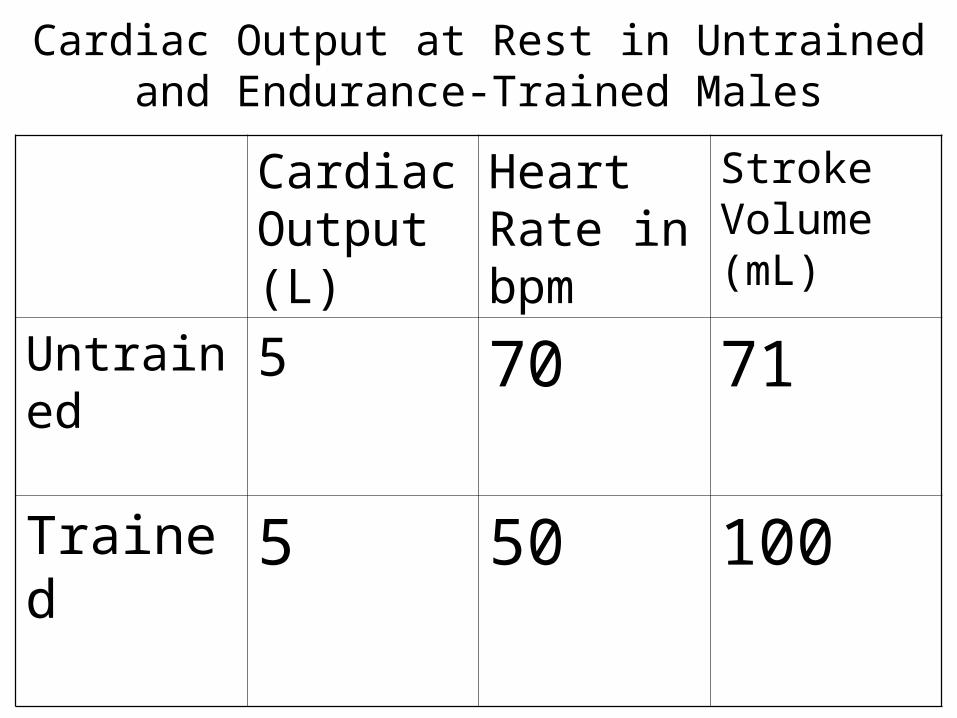
Cardiac Output at Rest in Untrained and Endurance-Trained Males
Cardiac Output (L)
Heart Rate in bpm
Stroke Volume (mL)
Untrained 5 70 71
Trained 5 50 100
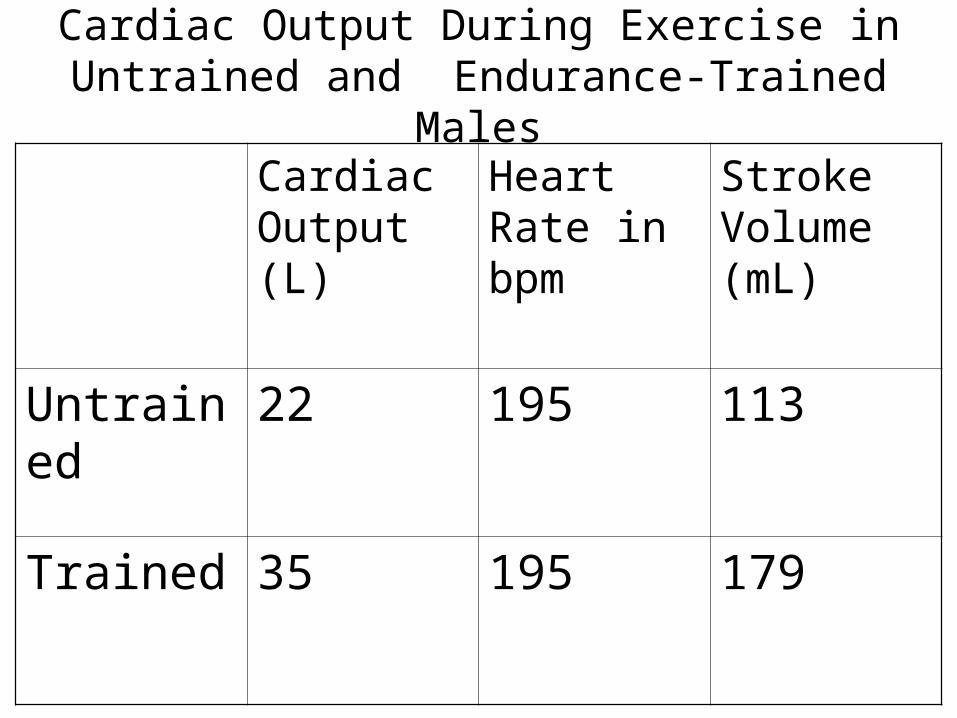
Cardiac Output During Exercise in Untrained and Endurance-Trained Males
Cardiac Output (L)
Heart Rate in bpm
Stroke Volume (mL)
Untrained 22 195 113
Trained 35 195 179
Cardiac Output• Initial Stages of Exercise
cardiac output is due heart rate and stroke volume
• When level of exercise exceeds 40% to 60% of the individual's capacity, stroke volume has either plateaued or begun to increase at a much slower rate
• Further in cardiac output are largely the result of in heart rate.
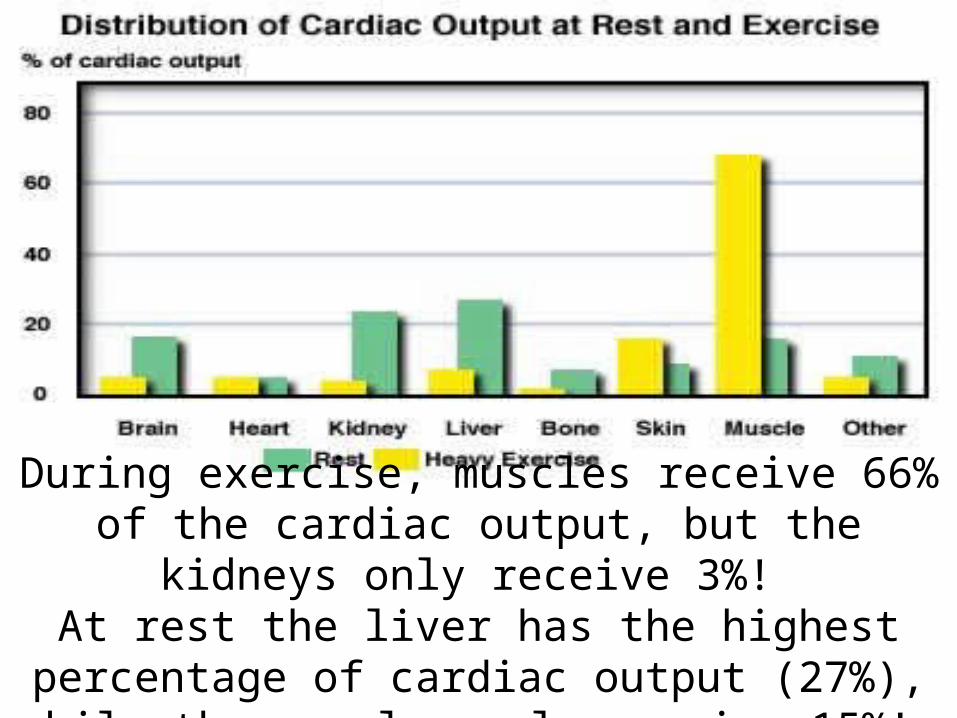
During exercise, muscles receive 66% of the cardiac output, but the kidneys only receive 3%!
At rest the liver has the highest percentage of cardiac output (27%), while the muscles only
receive 15%!
Oxygen Uptake• Oxygen Uptake (VO2):
–Amount of oxygen utilized by the tissues of the body
–Measured in liters per minute (L/min)
–Function of cardiac output• Maximal Oxygen Uptake is VO2 max:
–Greatest amount of oxygen that can be utilized at the cellular level for the entire body
Oxygen Uptake• Metabolic Equivalent (MET):
–3.5 ml O2/kg/min at rest• Peak oxygen uptake ranges from
35-80 ml/kg/min or 10-22.9 METS• Capacity to utilize oxygen is
described by Cardiac Output:–HR x Stroke Volume and Arteriovenous Oxygen Difference (a-vO2 difference)
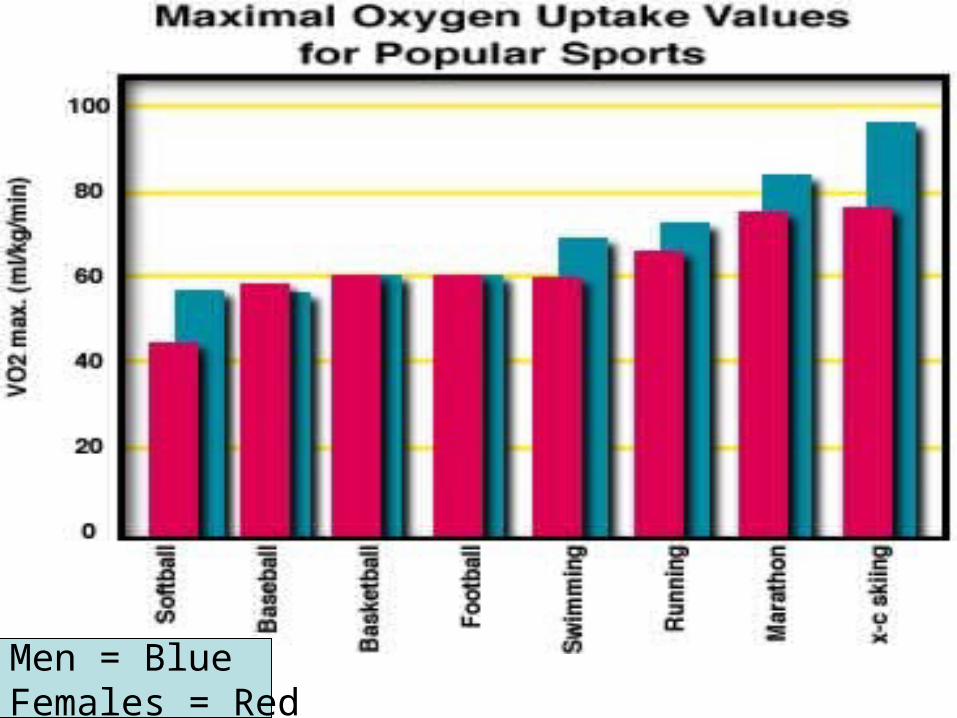
Men = BlueFemales = Red
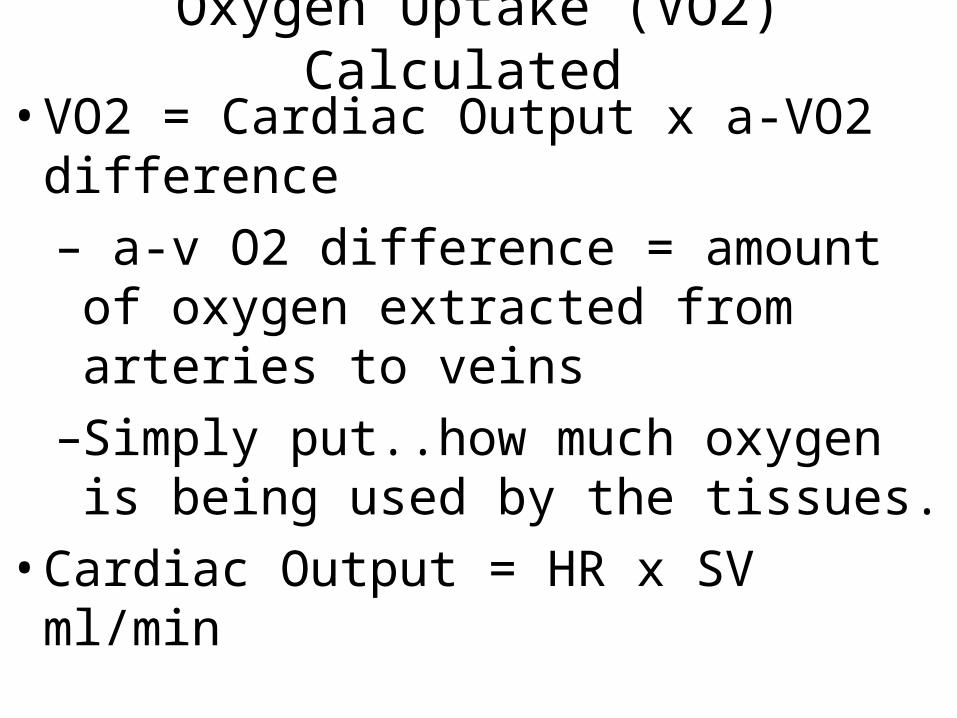
Oxygen Uptake (VO2) Calculated
• VO2 = Cardiac Output x a-VO2 difference
– a-v O2 difference = amount of oxygen extracted from arteries to veins
–Simply put..how much oxygen is being used by the tissues.
• Cardiac Output = HR x SV ml/min
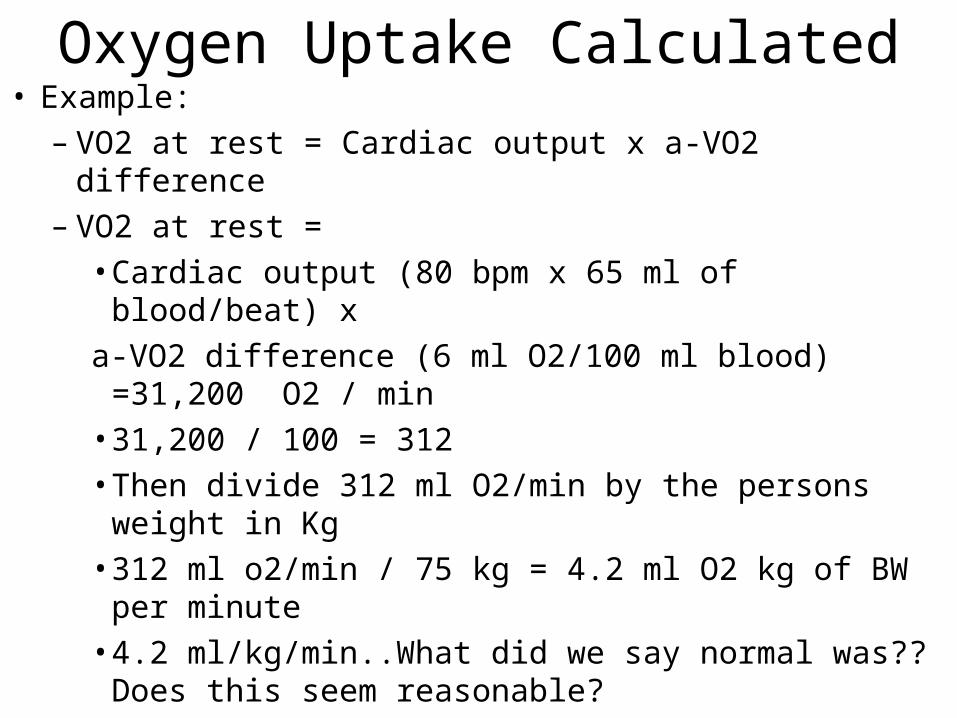
Oxygen Uptake Calculated• Example:
– VO2 at rest = Cardiac output x a-VO2 difference – VO2 at rest =
• Cardiac output (80 bpm x 65 ml of blood/beat) x
a-VO2 difference (6 ml O2/100 ml blood) =31,200 O2 / min
• 31,200 / 100 = 312 • Then divide 312 ml O2/min by the persons weight
in Kg• 312 ml o2/min / 75 kg = 4.2 ml O2 kg of BW per
minute• 4.2 ml/kg/min..What did we say normal was??
Does this seem reasonable?
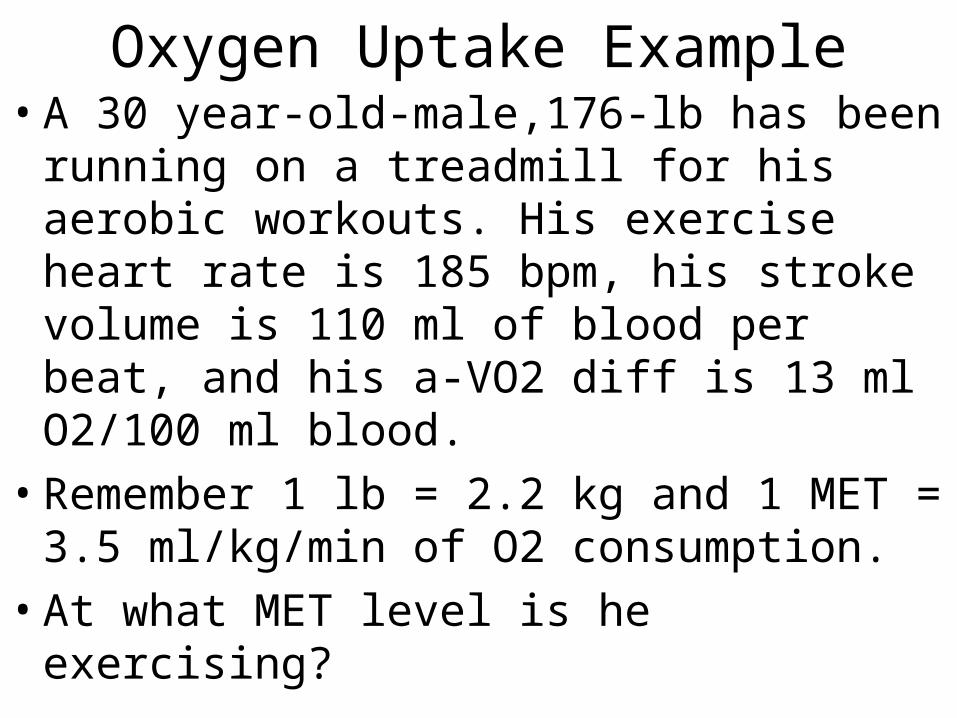
Oxygen Uptake Example• A 30 year-old-male,176-lb has been
running on a treadmill for his aerobic workouts. His exercise heart rate is 185 bpm, his stroke volume is 110 ml of blood per beat, and his a-VO2 diff is 13 ml O2/100 ml blood.
• Remember 1 lb = 2.2 kg and 1 MET = 3.5 ml/kg/min of O2 consumption.
• At what MET level is he exercising?
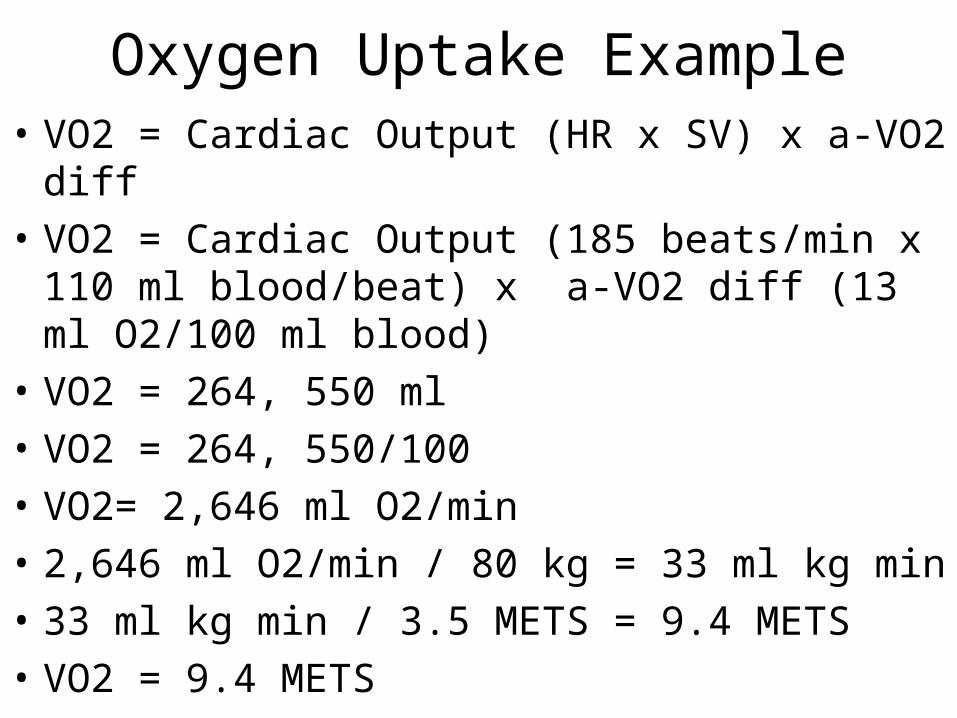
Oxygen Uptake Example• VO2 = Cardiac Output (HR x SV) x a-VO2 diff
• VO2 = Cardiac Output (185 beats/min x 110 ml blood/beat) x a-VO2 diff (13 ml O2/100 ml blood)
• VO2 = 264, 550 ml
• VO2 = 264, 550/100
• VO2= 2,646 ml O2/min
• 2,646 ml O2/min / 80 kg = 33 ml kg min
• 33 ml kg min / 3.5 METS = 9.4 METS
• VO2 = 9.4 METS
Blood Pressure• Systolic Blood Pressure:
–Pressure exerted against the arterial walls as blood is forcefully ejected during ventricular contraction
–Systole
• Diastolic Blood Pressure: –Pressure exerted against the arterial
walls when no blood is being forcefully ejected through the vessels
–Diastole
Blood Pressure• Blood pressure increases with
dynamic exercise (e.g., walking, jogging, rowing…)
• In healthy individuals it is only seen in the systolic response
• During upper extremity exercise both systolic and diastolic pressures are higher than compared with lower extremity exercises
Blood Pressure• Hypertension:
–High blood pressure commonly defined as 140/90
• With aerobic exercise systolic pressure can rise to as much as 220-260 mmHg
• Diastolic pressure remains at resting levels
• Pressure is highest in the aorta and arteries and rapidly falls in the veins
Cardiovascular Adaptations to Prolonged Training
• Cardiac Output initially increases rapidly, then more gradually, and reaches a plateau
• There is no cardiac output change with resistance training
• Aerobic and resistance training increases heart rate
Respiratory System
• Primary function of the respiratory system is the basic exchange of oxygen and carbon dioxide
• The respiratory pump:–located in the thoracic cavity (chest and
abdomen)
–Composed of skeletal structures and muscles
–Works together with the nervous system
Respiratory System Video
• http://www.youtube.com/watch?v=HiT621PrrO0&feature=related

Structures of the Respiratory System• Bones:
– Sternum– Ribs– Vertebrae
• Muscles of Inspiration:– Diaphragm– External intercostals– Scalenes– Sternocleidomastoid– Pectoralis Minor
• Expiration:– Internal intercostals– Abdominals
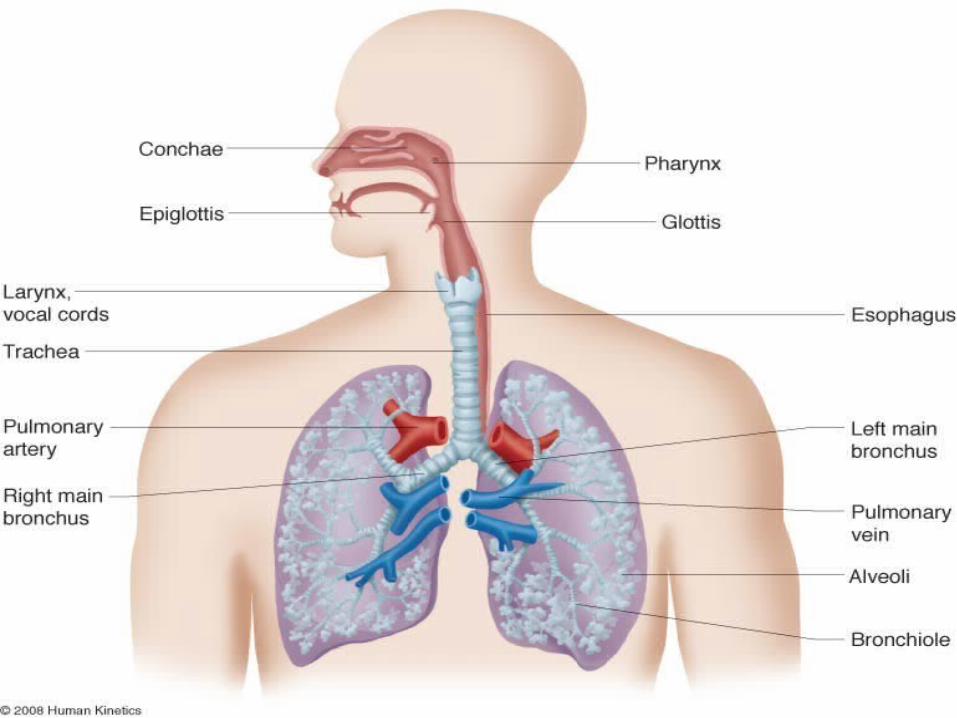
Structures of the Respiratory System• Conduction:
–Nasal cavity–Oral cavity–Pharynx–Larynx–Trachea–Right and left pulmonary bronchi–Bronchioles
• Respiratory:–Alveoli–Alveolar Sacs
Inspiration• Diaphragm:
– Large, dome-shaped sheet of striated muscle
– Primary muscle of ventilation
– Creates an airtight separation between the abdominal and thoracic cavities
– During inspiration the muscle contracts, flattens, and moves downward toward the abdominal cavity
– Elongation and enlargement of the chest cavity expands the air in the lungs
– The lungs inflate as air literally becomes sucked in through the nose and mouth
Inspiration• Contraction of the scalenes and external
intercostal muscles between the ribs causes the ribs to rotate and lift up away from the body (i.e., handle lifted up and away from the side of a bucket)
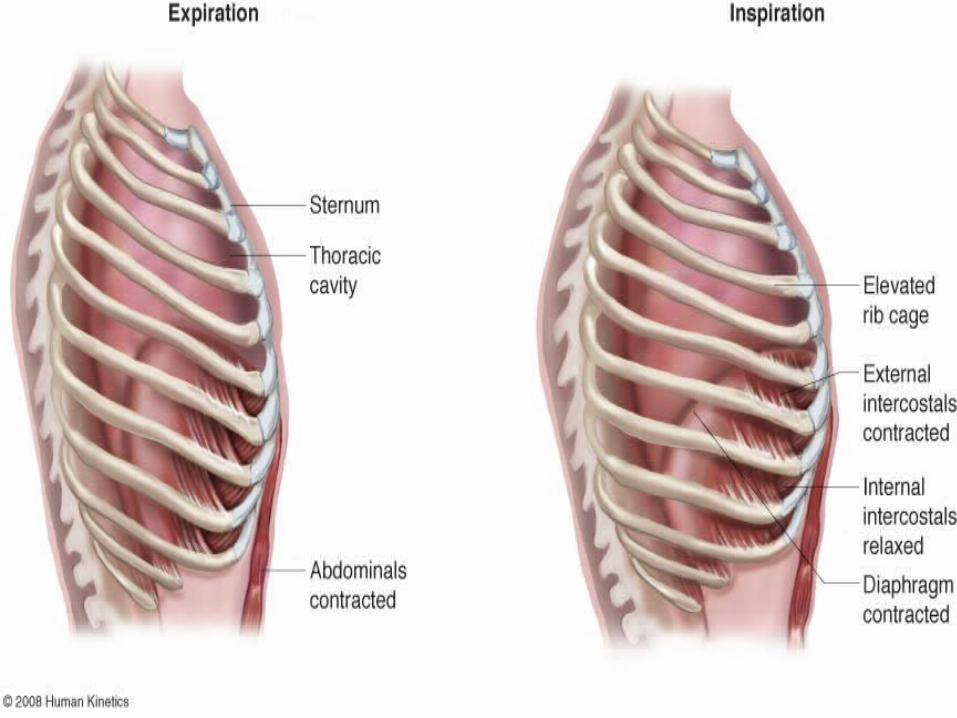
• During exercise:
– The diaphragm descends, the ribs swing upward, sternum thrusts outward
– Athletes often bend forward from the waist to facilitate breathing after exhausting exercise to promote blood flow back to the heart and minimize effects of gravity
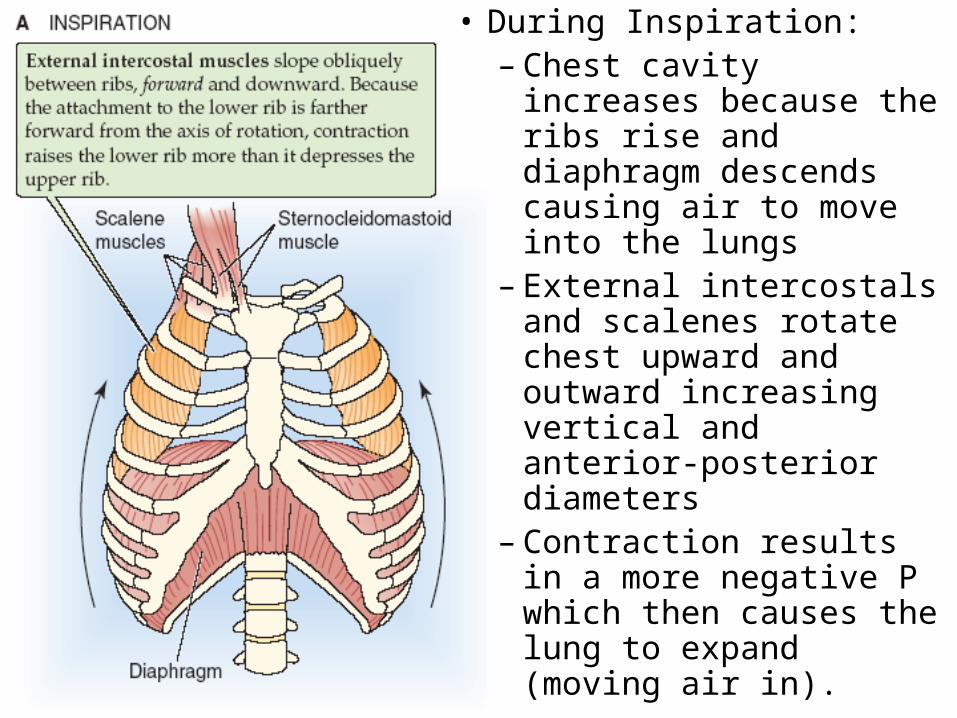
• During Inspiration:– Chest cavity increases
because the ribs rise and diaphragm descends causing air to move into the lungs
– External intercostals and scalenes rotate chest upward and outward increasing vertical and anterior-posterior diameters
– Contraction results in a more negative P which then causes the lung to expand (moving air in).
Expiration• Passive process of movement out of lungs (during
rest and light exercise) due to natural recoil of lungs and relaxation of inspiratory muscles
• Sternum and ribs swing down
• Diaphragm rises toward thoracic cavity
• This decreases chest cavity volume and compresses alveolar gas so air moves out of the respiratory tract into the atmosphere
• During strenuous exercise, internal intercostals and abdominal muscles act on the ribs to reduce thoracic dimensions and exhalation is rapid and extensive
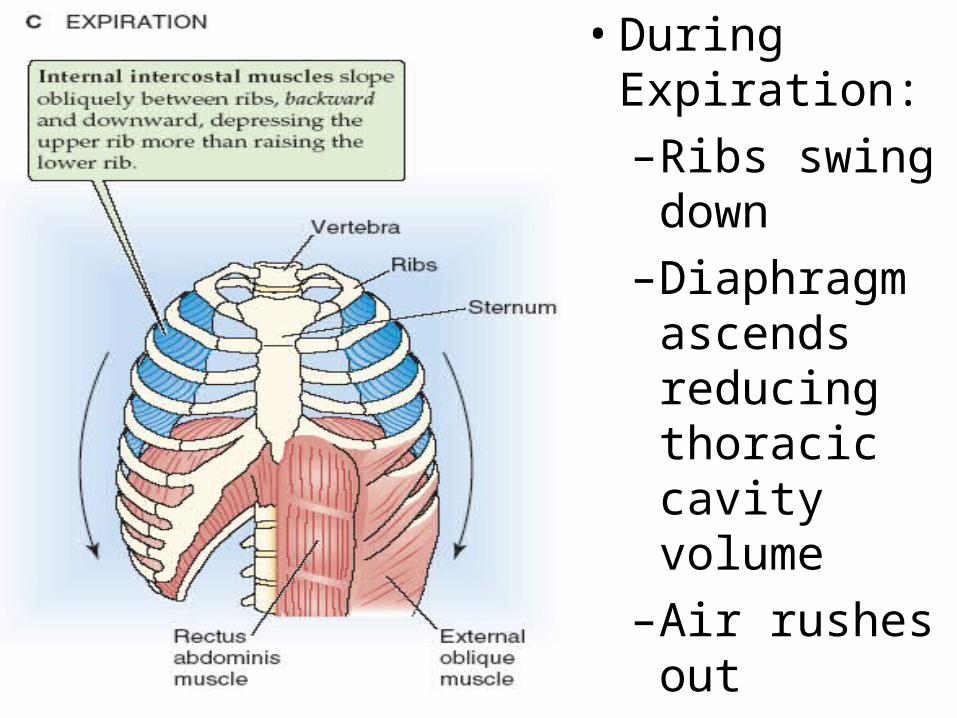
• During Expiration:
–Ribs swing down
–Diaphragm ascends reducing thoracic cavity volume
–Air rushes out
Inspiration and Expiration
• Inspiration:– Contraction of the diaphragm creates
negative pressure (vacuum) in the chest cavity, and air is drawn into the lungs
• Expiration:– The diaphragm relaxes; and the elastic
recoil of the lungs, chest wall, and abdominal structures compresses the lungs and air is expelled
Diaphragm Video
• http://www.youtube.com/watch?v=hp-gCvW8PRY&feature=related

Control of Respiration
• The nervous system controls the rate of ventilation by adjusting the rate and depth of breathing
• The body’s respiratory center is composed of neurons located in the lower portion of the brain stem (pons and medulla oblongata)
Respiratory Responses• Minute Ventilation:
– The volume of air breathed per minute.– With aerobic exercise it is increased. – During exercise it increases from 12-15
breaths per minute at rest to 35-45 breaths per minute during exercise.
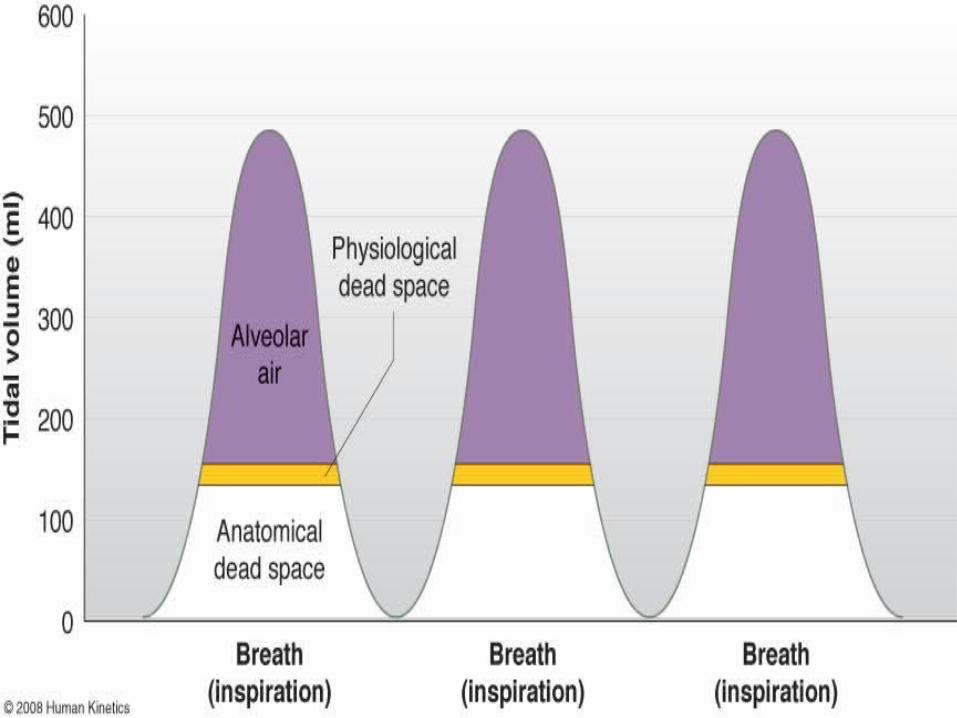
• Tidal Volume: – The amount of air inhaled and exhaled with
each breath. – It increases from .4 to 1L at rest to as much
as 3L during aerobic exercise.
Respiratory Responses• Anatomical Dead Space:
–Air entering and occupying respiratory passageways that is not useful for gas exchange. It is about 150 ml in adults and increases with age.
• Physiological Dead Space: –Poor blood flow, poor ventilation, or
other problems with the alveoli impair gas exchange (smoking).
External Influences on Cardiorespiratory Response
Altitude• Ventilation rate:
– Total amount of air moving in and out of the lungs is stimulated at high elevations by an increase in breath frequency.
• This serves to raise oxygen availability to the alveoli in the lungs (site of oxygen extraction from the pulmonary system into the bloodstream).
Altitude• Altitude stimulates an increase in heart
rate and cardiac output to increase blood circulation by the muscles to unload oxygen and pick up carbon dioxide and back to the alveoli to reverse these exchanges.
• The composition of the blood changes after about 2 weeks of altitude exposure by producing more red blood cells and hemoglobin (the iron-protein compound that transports oxygen).
Altitude• The benefits of blood adaptation in
the weeks following exposure includes:–Reducing the cardiac output required for
oxygen delivery during rest and submaximal exercise
– Increasing maximal oxygen transport during strenuous exertion and providing a larger fluid reserve for sweating.
Physiological Changes With Long-Term (3-6 months) Aerobic Exercise:
• Bradycardia: –Slower resting heart rate ranging from 40-
60 bpm• Lower maximal heart rate during exercise• Increase in stroke volume at rest and during
exercise• Increase in cardiac output at rest and during
exercise
Physiological Changes With Long-Term (3-6 months) Aerobic Exercise
• Increase in heart volume
• Increase in blood volume
• Increase in systolic blood pressure during exercise (no change in diastolic)
• Decrease in blood pressure at rest
• Increase in breathing rate (breaths per minute) during exercise
• Decrease in breathing rate at rest
Physiological Changes With Long-Term (3-6 months) Aerobic Exercise
• Increase in maximal oxygen uptake
• Onset of blood lactate accumulation (OBLA) occurs at a higher percentage
• More rapid rate of lactic acid removal
• Increased mitochondrial density and capillary density
• Improved aerobic enzyme activity
• Decrease in percent body fat