the behavioural effects of testosterone undecanoate in adult men with klinefelter's syndrome: a...
TRANSCRIPT

Clinical Endocrinology (1982) 16,489497
THE BEHAVIOURAL EFFECTS OF TESTOSTERONE UNDECANOATE IN ADULT MEN WITH KLINEFELTER’S
SYNDROME: A CONTROLLED STUDY
F. C. W. WU, J . BANCROFT, D . W. DAVIDSON AND K . NICOL
Royal InJirmary, Lauriston Place, Edinburgh EH3 9 Y W; MRC Reproductive Biology Unit, Centre for Reproductive Biology, 37 Chalmers Street, Edinburgh EH3 9E W and Imrnunoassay Section, Department of Clinical Chemistry, Royal InJirmary, Edinburgh
(Received 27 July 1981; revised 10 Nouember 1981; accepted 3 December 1981)
SUMMARY
The behavioural effects of exogenous testosterone in men with marginally low circulating androgen levels were investigated. Four adult men with Klinefelter’s syndrome, low normal testosterone levels and normal sexual activity and interest were given testosterone undecanoate (TU 160 mg daily by mouth; Organon International) and placebo using a double blind cross-over design. A modest increase in sexual interest was observed during TU administration compared to placebo, though there were no effects on self-reported mood or energy, or on erectile responsiveness in the laboratory. Increase in circulating hormone levels during TU administration was more marked for DHT than for testosterone. The possible implications of this are discussed.
Adults with 47 XXY karyotype show varying degrees of Leydig cell failure and plasma testosterone concentrations are usually in the lower part of the normal range. Some are clearly hypogonadal. The sexual activity of one group of Klinefelter men did not differ significantly from a normal group although their testosterone was significantly lower (Raboch & Starka, 1973). Others have reported that low sexual appetite is common in these men (Paulsen et al., 1968; Becker, 1972) who are likely to benefit from exogenous androgens. Two studies have shown that 47 XXY males have impaired or at least delayed psychosexual development (Raboch et al., 1979; Bancroft et af., 1982). Obviously there is considerable variability in how this chromosomal abnormality manifests itself. The discrepancy between the numbers of such men who present clinically (e.g. in an infertility or endocrine clinic) and the incidence found in screening studies (0.1% live births, Jacobs et a/., 1974) indicates that many such men must exist in the community relatively free from problems.
As yet there is no controlled evidence of the effects of exogenous androgens on the
Correspondence: Dr J. Bancroft, MRC Reproductive Biology Unit, 37 Chalmers Street, Edinburgh EH3 9EW.
0300-0664/82/0500-0489$02.00 0 1982 Blackwell Scientific Publications
489

490 F. C. Wu et al.
behaviour of Klinefelter men. With severe hypogonadism, the effects of exogenous androgens on sexual behaviour and interest is striking (Davidson et ul., 1979; Skakkebaek et id., 1980). Whether exogenous androgens have any behavioural effects in men whose endogenous testosterone levels are just below or within the normal range remains uncertain. We report here the results of a double blind controlled evaluation of testosterone administration on the sexual interest, behaviour and mood in four such men. The results are therefore of clinical relevance to the management of Klinefelter’s syndrome, but also of theoretical interest for the behavioural effects of exogenous testosterone at various levels of circulating endogenous androgens.
SUBJECTS
Details of the four subjects are given in Table 1 . For cosmetic reasons subject 4 underwent right-sided orchidectomy with implantation of bilateral testicular prosthesis 3 years previously. He presented with ill-defined problems in establishing relationships with women and some anxiety about his sexual ability. Each subject was asked if he would enter the study, having the full procedure explained in detail to him. It was stated that whereas our primary purpose was to investigate the effects of androgens on their behaviour, they may find the results of personal benefit as far as their future clinical management was concerned. To the three patients who presented with infertility, it was emphasized that we did not expect hormone treatment to have any effect on their infertility but that i t may have effects on their sexuality and general well-being.
Table I . Characteristics of four males with Klinefelter’s syndrome
Previous Age Presenting Marital sexual Eunuchoidal Gynaeco- Previous
Subject (years) problem status function featurcs mastia treatment
I 30 Infertility Married Normal High pitched Right and Nil voice. Beard left growth started age 21
and facial hair. Fluoxymesterone Shaving from age 18. 10 mg bd 2 years Eunuchoid body previously proportions
Eunuchoid body proportions
4 48 Problems in Single Intermittent Eunuchoid body
2 31 Infertility Married Normal Diminished body Right only 2 month course of
3 32 Infertility Married Normal Diminished body hair. Nil Nil
Nil Mesterelone
with for previous
terminating 2 months before entering study right orchidectomy
establishing problems proportions 25 mg qid a sexual relationship erection 3 years
-~

Testosterone undecanoate in Klinefelter ’s syndrome 49 1
METHOD Design
A double blind cross-over design was used. After a period of ‘no treatment’ (minimum 8 weeks) during which no hormone preparations were taken and baseline behaviour and hormonal assessment was carried out, there followed 8 weeks of placebo and 8 weeks of testosterone undecanoate (TU), a new oral androgen which is principally absorbed by the lymphatics (Nieschlag et al., 1975). The order was randomized, two men having TU followed by placebo and two men having the reverse.
Methods of Assessment Behavioural self-ratings
Each subject was asked to complete diary forms and weekly self-rating scales throughout the period of the study. The diaries provided the following information:-
1 Sexual acts. The occurrence of different types of sexual activity (i.e. sexual
2 Ejaculation. Whether a sexual act resulted in ejaculation. 3 Frequency of sexual thoughts. Weekly self-ratings were made. (M; O=not at all,
4 Feelings of sexual excitement associated with sexual thoughts (0-2). 5 Mood, using the Lorr & McNair Mood Adjective Check List (McNair et al., 1964)
intercourse, petting or masturbation) on a day-to-day basis.
4 =at least daily).
providing scales for: a anxiety/tension; b depression; c anger; d vigour; e fatigue.
Psychophysiological assessment Erectile responsiveness to erotic fantasies and films was measured according to the
method described by Bancroft & Wu (1982). This provides a measure of maximum erection and latency of erection (i.e. to 5 mm increase in diameter of the penis. If the 5-mm criterion was not reached, the latency was recorded as 180 s, the length of the trial period). The order of stimuli was erotic fantasy, three sequences of erotic film and a second erotic fantasy. Each stimulus lasted 3 min with a minimum of 3 min neutral film in between each. Erections were measured by a mercury in rubber strain gauge placed around the shaft of the penis and recorded on a Grass polygraph. This assessment was carried out twice during the no treatment period (with 8 weeks interval between) and once at the end of each treatment period (i.e. four times in all).
Hormonal assessments Once a month during the study, three to four blood samples were collected at 30 min to
l-h intervals during the morning. Plasma was separated and stored at -20°C until analysis. Each sample was assayed for testosterone, 5a-dihydrotestosterone (DHT), oestradiol, sex hormone binding globulin (SHBG), FSH and LH. DHT and testosterone were measured by RIA following separation by chromatography on celite columns using a modification of a method previously described (Thorneycroft et al., 1973). Testosterone was assayed as described by Corker & Davidson (1978). The DHT was assayed using antisera raised to 5a-DHT-BSA.
492 F. C. Wu et al.
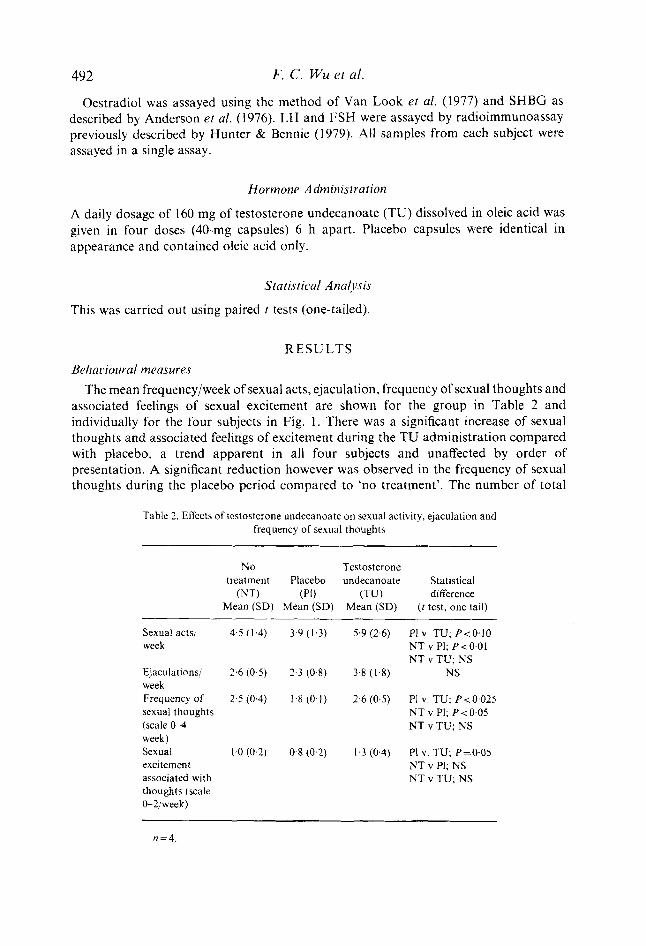
Oestradiol was assayed using the method of Van Look ef al. (1977) and SHBG as described by Anderson et al. (1976). LH and FSH were assayed by radioimmunoassay previously described by Hunter & Bennie (1 979). All samples from each subject were assayed in a single assay.
Hormone Administration
A daily dosage of 160 mg of testosterone undecanoate (TU) dissolved in oleic acid was given in four doses (40-mg capsules) 6 h apart. Placebo capsules were identical in appearance and contained oleic acid only.
Staristical Attalysis
This was carried out using paired t tests (one-tailed).
RESULTS BehaLiioural measures
The mean frequency/week of sexual acts, ejaculation, frequency of sexual thoughts and associated feelings of sexual excitement are shown for the group in Table 2 and individually for the four subjects in Fig. 1. There was a significant increase of sexual thoughts and associated feelings of excitement during the TU administration compared with placebo, a trend apparent in all four subjects and unaffected by order of presentation. A significant reduction however was observed in the frequency of sexual thoughts during the placebo period compared to ‘no treatment’. The number of total
Table 2. Ellects of testosterone undecanoate on sexual activity, ejaculation and frequency of sexual thoughts
NO Testosterone treatment Placebo undecanoate Statistical
(NT) (Pi) (TU) difference Mean (SD) Mean (SD) Mean (SD) ( t test, one tail)
Sexual acts/ 4.5 (1.4) 3.9 (1.3) 5.9 (2.6) PI V. TU; P<O.lO week N T v P1; P < 0.01
N T v TU; NS Ejaculations/ 2.6 (0.5) 2.3 (0.8) 3.8 (14) NS week Frequency of 2.5 (0.4) 1.8 (0-1) 2-6 (0.5) PI v. TU; P<0,025 sexual thoughts (scale W week) Sexual 1.0 (0.2) 0.8 (0.2) 1.3 (0.4) PI V . TU; P=0.05 excitement N T v PI; NS associated with thoughts (scale O-Z!week)
N T v PI; P < 0.05 N T v TU; NS
N T v TU; NS
n = 4 .

Testosterone undecanoate in Klinefelter 's syndrome
2
&.I--- z
493
2 C' T /
No Placebo TU No Placebo TU treatment treatment
Fig. 1. The mean frequency/week of sexual acts (a), frequency of sexual thoughts (b) (W self-rating scales/week) and sexual excitement associated with sexual thoughts (c) (0-2 self-rating scaleiweek) in four men with Klinefelter's syndrome on no treatment, followed by treatment with placebo and testosterone undecanoate (subjects 2 and 4) or testosterone undecanoate and placebo (subjects 1 and 3). (0) Subject I ; (0) subject 2; (0) subject 3; (W) subject 4.
sexual acts increased in all four men during TU administration compared to placebo, though the difference was only significant at the 10% level. The degree of change was also variable in extent (59, 58,23, and 2% respectively). Furthermore, in two men, subjects 1 and 4, the level of sexual activity during TU administration was close to that during the no-treatment period. There were no significant differences in any of the subscales of mood (Table 3).
Table 3. Effects of testosterone undecanoate on self-rating of mood (Lorr & McNair mood adjective check list)
No treatment Placebo TU
Mean (SD) Mean (SD) Mean (SD)
Tension/anxiety 12.4 (1.6) 12.1 (2.4) 11.9 (1.3) NS Anger 8.8 (0.9) 8.9 (1.0) 8.7 (0.3) NS Depression 13.6 (1.9) 13.5 (2.2) 13.3 (1.5) NS Vigour 11.8 (6.1) 11.8 (6.7) 12.1 (6.0) NS Fatigue 8.4 (1.4) 7.7 (1.9) 8.0 (1.5) NS
n=4 .

494 F. C. Wu et al.
Table 4. Effects of testosterone undecanoate on latency and degree of erectile response to erotic fantasy and film
No N o treatment treatment session I session I1 Placebo TU
Mean (SD) Mean (SD) Mean (SD) Mean (SD)
Funfosj, I Latency I80 s (0) 176 s (9) 142 s (45) 139 s (49) NS Maximum erection as increase in diameter 0.9 mm (0.4) 2.7 mm (2.1) 5.1 mm (4.1) 4.3 mm (3.5) NS
Funtasy I I Latency I80 s (0) 153 s (51) 122 s (72) 146 s (68) NS Maximum erection as increase in diameter 1.2 mm (0.7) 5.2 mm (3.1) 7.4 mm (7.0) 3.9 mm (5.1) NS
Frilnis Latency 76 s (29) 34 s (6) 62 s (44) 37 s (12) NS Maximum erection as increase in diameter 8.6 mm (3.5) 13.8 mm (4.6) 10.6 mm (3.8) 11.1 mm (2.3) NS
n = 4
Table 5. Effects on plasma hormone levels. Comparison of testoster- one undecanoate and placebo
No TU TU Plasma treatment Placebo 1st month 2nd month
hormone Mean (SD) Mean (SD) Mean (SD) Mean (SD) ~
Testosterone 3071 (882) 2976 (732) 3777 (1540) 3558 (717) (Pg/ml)
(pg/ml)
(pgiml)
(nmolil) LH 32 0 (6.2) 32 8 (12 2) 23 9 (7 4) 23 0** (1 1 2)
(u/l)
(u/l?
DHT 361 (47) 375 (69) 1083* (314) 1043** (223)
Oestradiol 49 6 (22 1) 31 1 (6 4) 46 5 (31 6) 38 3* (6 2)
SHBG 3 26 (0 69) 2 7 (0.7) I 68** (0.5) I 72** (0 6)
FSH 39 5 (4 6) 39 9 (6 9) 35 4* (6 3) 29 6* (12 5 )
n = 4 Comparison of placebo and TU t test. * P < 0.05. ** P<O.Ol.

Testosterone undecanoate in Klinefelter 's syndrome 495
Psychophysiological measures Maximum erection and latency of response to fantasy and film for the three conditions
are shown in Table 4. There was no evidence that TU either increased the maximum response or reduced the latency of response to either fantasy or film.
Hormones Mean concentrations of testosterone, DHT, oestradiol, SHBG, LH and FSH for the
no-treatment, placebo and TU periods are shown in Table 5 . The levels for the first and second months of TU administration are shown separately. Plasma testosterone concentrations were not significantly raised by TU administration, whereas DHT levels rose substantially. There was also a highly significant drop in SHBG which would indicate that free testosterone did increase and free DHT even more so. Basal LH and FSH were lowered to a modest extent by TU administration.
DISCUSSION
The principal effect of TU administration was observed in measures of sexual interest and associated excitement. This is compatible with previous results in severely hypogonadal men suggesting that androgens mainly affect sexual appetite (Skakkebaek et al., 1981).
In studies involving the measurement of psychological and behavioural variables, the effect of order must be taken into account. In the experimental design of this study, order was only balanced for placebo and TU treatment. Thus only the comparisons between TU and placebo are statistically valid. Nevertheless, the effects of TU and placebo compared with no treatment are worthy of comment. In all four subjects, sexual activity and frequency of sexual thoughts were higher during the no-treatment period than during placebo administration. For none of the variables was this difference between TU and no treatment significant. It is not unusual to find that self-monitoring initially increases the behaviour that is being monitored, particularly if there are no important constraints on the behaviour in the first place. This could well be the case in this study where each of the four subjects were showing quite normal levels of sexual interest and activity to begin with. The potentially confounding effect of measurement emphasizes the importance of balancing order in the experimental design.
The overall effect must therefore be seen as modest in degree, only marked in two men, and less striking than that observed in men who start with low levels of testosterone and behaviour (Skakkebaek et al., 198 1).
The finding that in two men (subjects 2 and 3) the behavioural effects of TU were substantial whilst in the other two they were minimal (subjects 1 and 4) may indicate that there is variable sensitivity of behaviour to androgens. This could apply to men with Klinefelter's syndrome as to men in general. There was no obvious distinguishing characteristic of the high responders in terms of baseline androgen levels or order of presentation, although they did undergo a longer period of no-treatment assessment.
Changes in androgen at this level did not affect erectile responsiveness as measured. Elsewhere we have shown that with lower testosterone levels, the administration of TU may increase the erectile response to erotic fantasies but not to erotic films (Bancroft & Wu, 1982). It may be that erectile function requires less androgens than other aspects of sexuality, but more evidence will be required before we can be certain on that point.

496 F. C. Wu rt al.
The relatively greater increase in circulating DHT than testosterone is consistent with previous studies involving TU (Hirschhauser et ul., 1975; Franchi et al., 1978; Franchimont etal., 1978; Skakkebaek et ul., 1981). It is not known whether thispattern is observed with other forms of exogenous testosterone administration or whether it is peculiar to the undecanoate ester. Previous reports of plasma levels of testosterone achieved with exogenous androgens have employed assays with a high degree of cross-reactivity between testosterone and DHT (at least 30%, Nieschlag et ul., 1976; Aakvaag & Vogt, 1969; Coppage & Cooner, 1965).
I t has been suggested that TLJ is converted to dihydro-TU during absorption in bowel mucosa (Hirschhauser et al., 1975). Considerable 5%-reductase activity of human jejunal mucosa has recently been demonstrated (Farthing et ul., 1980). Further work is needed to clarify this point as far as TU is concerned and studies are currently in progress to establish to what extent DHT administration is responsible for the behavioural effects of TU .
These results suggest that some men with Klinefelter’s syndrome may benefit from androgen therapy, even when their endogenous levels are within the normal range. It would be clinically desirable in such cases to test the hormone against placebo before embarking on long-term hormone administration. Although one should be cautious in generalizing from effects in men with abnormal sex chromosome constitution to normal males. it seems possible that at least some androgen-dependent aspects of male sexuality may be enhanced by augmenting the androgen supply in this lower part of the normal range. Further studies of this kind are needed in normal men to clarify this point.
A C K N O W L E D G E M E N T S
We are grateful to Organon International, Oss for their support and the supply of testosterone undecanoate and placebo.
R E F E R E N C E S
AAKVAAG. A. & VOGT. J.H. (1969) Plasma testosterone values in different fornls of testosterone treatment. Acfu Endocr-inologica. 60, 537-542.
AWFRSOK. D. C.. LESLEY. B.L.. FISHER. R.A.. SHEPHERD. J.H.. NEWMAN. L. & HENDKICKX, A.G. (1976) Transplacental gradients of sex-hormone-binding-globulin in human and Simian pregnancy. Clinical Endocrinolog!.. 5, 657-669.
BANCKOFT. J.. AXWORTHY. D. & RATCLIFFE. S. ( 1982) The personality and psychosexual development of boys with 47 XXY chromosome constitution. Joitrnal uf Child P . ~ j d i o l o g ~ and Psychiatry, In Press.
BANCROFT. J . & WU, F.C. (1982) Changcs in erectile responsiveness during androgen replacement therapy. Archives of Sesiral Behavior. In Press.
BECKEK, K.L. (1972) Clinical and therapeutic experiences with Klinefelter’s syndrome. FertilityundSlrrility, 23,
COPPAGE, W.S. & C(X)NEK, A.E. ( 1965) Testosterone in human plasma. New England Journal of’Mrtlic,inr, 273,
CORKER. C.S. & DAVIDSON. D.W. (1978) A radioimmunoassay for testosterone in various biological fluids with
DAVIDSON. J.M., CAMARGO. C.A. & SMITH, E.R. (1979) Effects of androgens on sexual behaviour in
FARTHING. M.J.G.. VINSON. G.P.. EDWAKDS, C.R.W. & DAWSON. A.M. (1980) Androgen metabolisni and
FKAVTHI, F., LuiSl. M. & KITOVK. P.M. (1978) Long-term study of ordl testosterone undecdnoate in
568-578.
902.
chromatography. Journul of Slrr-oid Bioch~vnistr-,~~. 9, 373-374.
hypogonadal men. Journal of Cliniccii Etiriocrinolog~~ c m c i Metttholi.vm. 48, 955 %R.
transport by the gut. Proceedings of r h c ~ 160th M i v t N i g o f ’ t l i ~ Society.for- Endocrinologj,. May.
hypogonadal males. Inter-n~itionul Juitrnul of Anclr-olog~., 1, 270- 278.
Testosterone undecanoate in Klinefelter j . syndrome 497 FRANCHIMONT, P., KICOVIC, P.M., MATTIER, A. & ROULIER, R. (1978) Effects of oral testosterone undecanoate
in hypogonadal male patients. Clinical Endocrinology, 9, 3 13-320. HIRSCHHAUSER, C., HOPKINSON, C.R.N., STURN, G. & COERT, A. (1975) Testosterone undecanoate: a new orally
active androgen. Acta Endocrinologica, 80, 179-187. HUNTER, W.M. & BENNIE, J.G. (1979) Reduction of non-specific serum response in human pituitary
gonadotrophin radioimmunoassays. Journal of Endocrinology, 80, 59-68. JACOBS, P.A., MELVILLE, M., RATCLIFFE, S., KEAY, A.J. & SYME, J. (1974) A cytogenetic survey of 11,680
newborn infants. Annals of Human Genetics, London, 37, 359-376. MCNAIR, L., DOUGLAS, M. & LORR, M. (1964) An analysis of mood in neurotics. Journal of Abnormaland Sociul
Psychology, 69, 620-627. NIESCHLAG, E., CUPPERS, H.J., WIEGELMAN, W. & WICKINGS, E.J. (1976) Biovailability and LH-suppressing
effect of different testosterone preparations in normal and hypogonadal men. Hormone Research. 7, 138-145.
NIESCHLAG, E., MANSS, J., COERT, A. & KICOVIC, P.M. (1975) Plasma androgen levels in men after oral administration of testosterone or testosterone undecanoate. Acia Endocrinologica, 79, 366.
PAULSEN, C.A., GORDON, D.L., CARPENTER, R.W., GANDY, H.M. & DRUCKER, W.D. (1968) Klinefelter’s syndrome and its variants: a hormonal and chromosomal study. Receni Progress in Hormone Research. 24, 4, 321.
RABOCH, J. MELLAN, J. & STARKA, L. (1979) Klinefelter’s syndrome: sexual development and activity. Archives of Sexual Behavior, 8, 3 3 3-3 3 9.
RABOCH, J. & STARKA, L. (1973) Reported coital activity of men and levels of plasma testosterone. Archires qj’ Sexual Behaviour, 2,309-3 16.
SKAKKEBAEK, N., BANCROFT, J., DAVIDSON, D.W. & WARNER, P. (1981) Androgen replacement with oral testosterone undecanoate in hypogonadal men: a double blind controlled study. Clinical Endocrinology. 14,
THORNEYCROFT, I.H., RIBEIRO, W.O., STONE, S.C. & TILLSON, S.A. (1973) A radioimmunoassay of
VAN LOOK, P.F.A., HUNTER, W.M., CORKER, C.S. & BAIRD, D.T. (1977) Failure of positive feedback in intact
49-6 1.
androstenedione. Steroids, 21, 1 1 1-122.
normal men and subjects with testicular feminisation. Clinical Endocrinology, 7, 353-366.
