testosterone and Δ4-androstenedione in the saliva of patients with klinefelter's syndrome
TRANSCRIPT

Clinical Endocrinology (1983) 18, 5 1-59
TESTOSTERONE AND A,-ANDROSTENEDIONE IN THE SALIVA OF PATIENTS WITH KLINEFELTER’S SYNDROME
J . J . WELLEN, A. G. H. SMALS, J. C. W. RIJKEN, P. W. C. KLOPPENBORG A N D TH. J. BENRAAD
Department of Experimental and Chemical Endocrinology and Division of Clinical Endocrinology, Department of Medicine, University of Nijmegen, The Netherlands
(Received 14 April 1982; revised 22 June 1982; accepted 8 July 1982)
S U M M A R Y
This study compares salivary and total plasma levels of testosterone and androstenedione in healthy controls and chromatin positive patients with Klinefelter’s syndrome. The mean plasma testosterone level in fifteen Kline- felter patients was significantly lower than in ten control subjects, but the mean androstenedione levels were similar. Saliva of the normal men and patients with Klinefelter’s syndrome did not differ significantly in binding potency for testosterone or androstenedione. The mean salivary testosterone level in the Klinefelter patients was significantly lower than in the controls but again salivary androstenedione levels were similar. Although testosterone as well as androstenedione showed a fair correlation between the salivary and plasma concentrations, preliminary data suggested that salivary testosterone levels better characterize the clinical state of androgenicity than do plasma levels. When salivary testosterone and androstenedione were expressed as a percentage of total steroid levels in plasma, the ratios for both steroids were similar in Klinefelter patients and healthy controls and closely approximated to the reported percentages of free steroid levels in plasma. The absolute salivary testosterone concentrations also were almost identical to the reported free plasma hormone levels.
Together the data provide indirect evidence that in Klinefelter patients testosterone and androstenedione binding in plasma and saliva does not differ from that in normal men, and measurement of salivary steroids, by reflecting their free hormone concentration in plasma, may be useful in evaluating endocrine function in both health and disease.
Saliva levels of most biologically active compounds reflect their unbound concentrations in plasma, as only the free fraction can pass easily through the parotid membrane
Correspondence: Dr Th. J. Benraad, Department of Experimental and Chemical Endocrinology, University of Nijmegen, The Netherlands.
0300-0664/83/0100-0051$02.00 0 1983 Blackwell Scientific Publications
51
52 J . J . Wellen et al.
(Dvorchik & Vesell, 1976; Horning et al., 1977; Smith et al., 1979; Walker et al., 1980). Since Shannon et al. (1959) demonstrated that salivary 17-hydroxycorticosteroid concentrations nearly paralleled the serum levels, ample reports have appeared on a variety of steroid hormones stressing the close relationship between salivary hormone levels and their plasma concentrations in both basal and stimulated conditions (Katz & Shannon, 1969; Landman et al., 1976; Walker & Fahmy, 1978; McVie et al., 1979; Turkes et al., 1979, 1980; Gaskell et al., 1980; Riad Fahmy et al., 1980; Luisi et al., 1980, 1981; Baxendaleetal., 1980;Umedaet al., 1981; Wangetal., 1981).Veryrecentlyasimilarclose relationship was not only found between salivary and total plasma testosterone levels, but also between salivary concentrations and the free hormone levels (Baxendale et al., 1980; Wang et al., 1981). Baxendale et al. (1980) showed that salivary testosterone concentra- tions in normal men closely paralleled the free hormone levels in blood and in fact were almost identical. Very recently this finding was extended by Wang et al. (1981) who stressed the similarity of salivary and free testosterone concentrations in plasma in (hyperthyroid) patients with elevated levels of SHBG.
In patients with Klinefelter’s syndrome SHBG levels have been reported to be low or normal (Steeno, 1970; Vermeulen et al., 1971; Wang et al., 1975) or even elevated (Wieland et al., 1980), whereas circulating total testosterone concentrations and also their non-protein bound levels are subnormal (Paulsen et al., 1968; Vermeulen et al., 1971; Weinstein et al., 1971; Stewart-Bently et al., 1973; Serrurier et al., 1976; Smals et al., 1976; Forti el al., 1978; Smalset al., 1978,1981; Wanget af., 1981). The present study compares salivary and total plasma levels of two major steroids of the 6 4 steroidogenic pathway, one with high affinity binding for SHBG and originating mainly from the gonad, i.e. testosterone, and the other with low binding to SHBG and secreted predominantly by the adrenals.
MATERIALS A N D METHODS
Subjects
The subjects studied were normal healthy men and hypergonadotrophic patients with Klinefelter’s syndrome (karyotype 46XXY). All subjects volunteered for this study. Their ages ranged from 27-54 years (mean & SD; 37.5 k 8.4 years, n = 15) for normal men and 20-46 years (33-4k8-6 years, n = 10) for Klinefelter patients. The serum LH and FSH concentration of the Klinefelter patients (33.0& 7-0 and 22.8 f 7.7 iu/l respectively) were significantly (P<O-OOI) higher than in normal men (12.4k3.6 and 3.3k2.1 iu/l respectively).
Test procedures
Samples Simultaneous mixed saliva and blood samples were collected between 09.00 and 10.00
h. At least 3 ml of mixed saliva was collected 15 min after the mouth had been rinsed with tap water. The saliva samples were centrifuged to remove debris and subsequently stored at -20°C until the time of assay. The blood samples were centrifuged immediately after collection and the plasma was stored at - 20°C until the time of assay.

Klinefelter patients’ salivary steroids 53 Assays
Steroid hormone concentrations in plasma and saliva were measured by radioim- munoassay (RIA) after extraction and chromatographic purification.
Extraction and chromatography. To 2.0 ml of plasma and 3.0 ml of saliva 10 000 d/min of 3H-labelled testosterone [New England Nuclear Enterprises (NEN)] and 3H-labelled androstenedione (NEN) in water-ethylene glycol (100:0.2, v/v) were added as recovery standards. The samples were subsequently extracted with 8-1 1 vol of ether.
The crude extracts were evaporated by air and chromatographed on Whatman paper no. I in a modified Bush A system for 3 h [solvent system petroleum+ther (80: 100)- methanol-water, 9: 7:4, by vol.]. The R,-values in this chromatographic system are: testosterone 0.30 and androstenedione 0.67, whereas the R, values of 5a-dihydrotestoster- one, 17a-hydroxyprogesterone, 1 1-deoxycortisol and cortisol are 0.60, 0.21,0.05 and 0 respectively. The recovery standards were located by radioscanning and the appropriate areas were eluted with 1 4 ml of water-ethylene glycol mixture. Eluates of corresponding areas of simultaneously run blank paper strips served as blanks in the RIA. The recoveries after extraction and paper chromatography were measured in samples of the eluates. The recoveries for testosterone and androstenedione were 52 f 13 and 47 f 7% for plasma and 53 f 12 and 5 1 k 7% for saliva (mean k SD, n = 25). In the calculations of the hormone concentrations the individual recoveries were taken into account, and a correction was also made for the added mass of labelled hormone.
Radioimmunoassay of testosterone. Testosterone concentrations in plasma and saliva were measured by RIA, using an antiserum (kindly provided by Dr Pratt, State University, Groningen) raised in rabbits against testosterone-7a-carboxyethyl thioether conjugated to BSA. This antiserum shows less than 30% cross reaction with 5a-dihydro- testosterone (Pratt et al., 1975). The assay was carried out in 200- and 300-pl samples of the eluates as described previously (Smals et af. , 1976). Briefly the method involved addition of a tracer (6OOO d min )H-testosterone) in 100 pl of 0.02 M phosphate buffer pH 7.4 containing 1% BSA and antiserum (diluted 1 : 1150) in 200 pl of the same buffer. Standard curves (0-1.12 pmol) were set up in duplicate. All incubation mixtures were mixed thoroughly.
After incubation overnight at 4°C the antibody-bound and free fraction were separated according to the method of Poulsen (1969). A suspension of 150 p1 of a dextran-coated charcoal (0.156 g of dextran and 7.8 g of charcoal in 500 ml of phosphate buffer) was pipetted into disposable caps placed on the test tubes. The suspension was mixed with the contents of the tubes by shaking them all simultaneously. After 6 min, at 4°C the tubes were centrifuged at lOOOOg for 10 min. The supernatants were decanted simultaneously into counting vials, using the equipment described by Vecsei (1974) and radioactivity was determined. Starting from 3 ml of saliva, the lower limit of detection of the assay was 0.049 nmol/l. The mean interassay coefficient of variation was 9.3% at a mean testosterone concentration of 8.95
Radioimmunoussay of androstenedione. Plasma and saliva androstenedione concentra- tions were measured by RIA using an antiserum raised against androstenedione- 19-car- boxymethylether, conjugated to BSA (Radioassay Systems Laboratories Inc, California). This antiserum cross reacts with dehydroepiandrosterone (4.2%), androsterone (1.5%), testosterone (0.34%), and 17a-hydroxyprogesterone (0.02%). The assay was performed in 200- and 300-pl samples of the paper eluates. Standard curves (&l. 12 pmol) were set up in duplicate. To standards and unknown samples, 100 pI of tracer solution (I0000 d/min
0.83 nmol/l (n = 32).

54 J . J . Wellen et al.
3H-androstenedione) and 200 p1 of antiserum (diluted 1 : 22 500) were added. The tracer and antiserum were dissolved in 0.05 M borate buffer pH 8.0 containing 0.1% Beriglobine (Bering Institute). The mixture was incubated overnight at 4°C and afterwards the antibody-bound and free fraction were separated by shaking for 3 min with 150 p1 of dextran-coated charcoal in borate buffer (0.156 g of dextran and 7.8 g of charcoal in 500 ml of borate buffer) as described for testosterone.
Starting from 3.0 ml of saliva, the lower limit of detection of the assay was 0.098 nmol/l. The mean interassay coefficient of variation was 8.6% at a mean androstenedione concentration of 9.08 f 0.78 pmol/l (n = 3 1).
Equilibrium dialysis of saliva. To examine whether saliva contains components which bind testosterone and androstenedione, saliva was dialysed overnight at 37°C against 0.15 M protein free phosphate buffer pH 7.4. These experiments were carried out in a Dianorm apparatus (Diachema AG, Riischlikon, Switzerland) using microcells (250 pl volume) and membranes which were cut from Visking dialysis tubing (molecular weight cut-off about 20 OOO). Samples of saliva (1 90 pl) were dialysed against 190 pl of buffer to which a tracer amount of 3H-testosterone or 3H-androstenedione was added. Before and after equilibrium the radioactivity was measured in duplicate in 50-pi samples of both buffer and saliva. The counts were corrected for quenching and the distribution of the labelled hormones between saliva and buffer was calculated.
Statistical methods
The data were analysed using Wilcoxon’s signed rank test (*P) , Wilcoxon’s two sample test (P), and Spearman’s rank correlation test ( * * P ) mean values f 1 SD are given.
RESULTS
Plasma steroid levels The mean morning plasma testosterone levels in the Klinefelter patients (9.5 & 4.3
nmol/l, range 4.0-19.4 nmol/l) were significantly lower (P < 0.001) than in the control subjects (19.7 f 4.0 nmolfl). In two of the patients levels were above the lower limit of the normal range (10-9 nmol/l). In contrast to testosterone, the mean plasma androstene- dione levels were almost identical (4.6 f 2.0 v. 4.5 & 1.8 nmol/l) in the patients and healthy controls (Table 1).
Salivary steroid levels Saliva samples of normal men and Klinefelter patients did not differ significantly in
binding for either of the two steroids tested (Table 2). Remarkably, both steroids showed a small, though significant difference in the distribution of the tracer between buffer and saliva.
Salivary testosterone levels in the Klinefelter patients (mean 0.14 f 0.08 nmol/l, range 0.04-0.28 nmol/l) were significantly lower (P < 0-002) than in the eugonadal men (0.25 f 0.08 nmol/l, range 0.12-0.39 nmol/l). The mean salivary androstenedione levels in the Klinefelter patients and eugonadal controls were virtually the same (0.44 f 0.23 v. 0.35 f 0.12 nmol/l, P > 0-10).
Klinefelter patients' salivary steroids 55
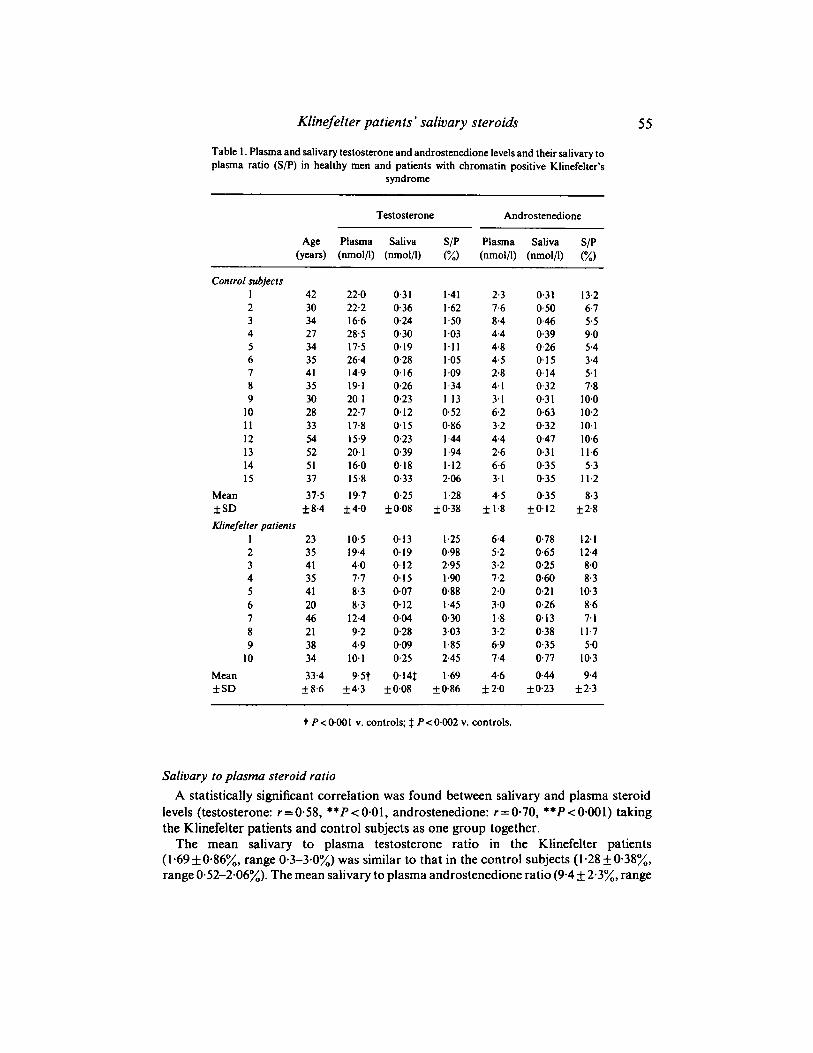
Table 1. Plasma and salivary testosterone and androstenedione levels and their salivary to plasma ratio (S/P) in healthy men and patients with chromatin positive Klinefelter's
syndrome
Testosterone Androstenedione
Age Plasma Saliva S/P Plasma Saliva S/P (years) (nmol/l) (nmol/l) (%I (nmol/l) (nmol/l) (%I
Control subjects 1 42 2 30 3 34 4 27 5 34 6 35 7 41 8 35 9 30
10 28 11 33 12 54 13 52 14 51 15 37
Mean 37.5 f SD f 8.4 Klinefelter patients
1 23 2 35 3 41 4 35 5 41 6 20 7 46 8 21 9 38
10 34 Mean 33.4 f SD f 8.6
22.0 0.31 22.2 0.36 16.6 0.24 28.5 0.30 17.5 0.19 26.4 0.28 14.9 0.16 19.1 0.26 20.1 0.23 22.7 0.12 17.8 0.15 15.9 0.23 20.1 0.39 16.0 0.18 15.8 0.33 19.7 0.25
k4.0 f0.08
10.5 0.13 19.4 0.19 4.0 0-12 7.7 0.15 8.3 0.07 8.3 0.12
12.4 0.04 9.2 0.28 4.9 0.09
10.1 0.25 9.5t 0.14t
k4.3 f0.08
1.41 1.62 1.50 1.03 1.11 1.05 1.09 1.34 1.13 0.52 0.86 1 44 1.94 1.12 246 1.28
f 0.38
1.25 0.98 2.95 1.90 0.88 1.45 0.30 3.03 1.85 2.45 1.69
k 086
2.3 7.6 8.4 4.4 4.8 4.5 2.8 4.1 3.1 6.2 3.2 4.4 2.6 6.6 3. I 4.5
f 1.8
6.4 5.2 3.2 7.2 2.0 3.0 1.8 3.2 6.9 7.4 4.6 f 2.0
0.3 1 0.50 0.46 0.39 0.26 0.15 0.14 0.32 0.3 1 0.63 0.32 0.47 0.3 1 0.35 0.35 0.35
f0.12
0.78 0.65 0.25 0.60 0.21 0.26 0.13 0.38 0.35 0.77 0.44
f0.23
13.2 6.7 5.5 9.0 5.4 3.4 5.1 7.8
10.0 10.2 10.1 10.6 11.6 5.3
11.2 8.3
f 2.8
12.1 12.4 8.0 8.3
10.3 8.6 7.1
11.7 5.0
10.3 9.4
t 2.3
t P < 0.00 I v. controls; # P < 0.002 v. controls.
Salivary to plasma steroid ratio A statistically significant correlation was found between salivary and plasma steroid
levels (testosterone: r = 0.58, **P < 0.01, androstenedione: r =0.70, **P < 0.001) taking the Klinefelter patients and control subjects as one group together.
The mean salivary to plasma testosterone ratio in the Klinefelter patients (1.69 i- 0.86%, range 0.3-3.0%) was similar to that in the control subjects (1.28 f 0-38%, range 0.52-2.06%). The mean salivary to plasma androstenedione ratio (9.4 _+ 2.3%, range

56 J . J . Wellen et al.
Table 2. Distribution of tracer between buffer and saliva after equilibrium dialysis in Klinefelter patients and healthy male controls
Klinefelter patients Healthy controls All subjects (n = 6) (n = 4) (n= 10)
Tracer (3H) Buffer Saliva Buffer Saliva Buffer Saliva
Testosterone 46.6f 2.3% 53.4* 2.3% 46.2 f 2.9% 53.8 & 2.9% 46.4 f 2,4% 53.6 f 2.4%t Androstenedione 47.7+2.0% 52.3f2.0% 48.4+2.5% 51.6f2.5% 48.0*2.1% 52.0+2.1%$
Buffer v. saliva: t * P < 0.01 ; $ ' P < 0.02.
54-12.4%) in the patients also did not differ significantly from the value in normal controls (8-3 +2.8%, range 5.1-13.273.
DISCUSSION The present study illustrates that steroid measurement in saliva is of value in evaluating testicular and also adrenocortical function in normal men and patients with hypo- gonadism, the salivary steroid levels showing a fair correlation with their plasma steroid levels. In the patients with Klinefelter's syndrome, in the present study, both plasma and salivary testosterone levels were significantly lowered, whereas the levels of the predominantly adrenal androgen androstenedione (Wieland et d., 1965; Gandy et d., 1968) were almost identical in the Klinefelter patients and control subjects.
Expressing salivary testosterone as a percentage of total plasma testosterone, the salivary to plasma testosterone ratio in the Klinefelter patients agreed closely with the value found in the healthy controls in the present study and with the values recently reported in normal men by Turkes et d. (1979) (1 - 1 873, Riad-Fahmy et ~ l . (1980) (1%) and Wang et d. (1 98 1) (1.38 f. 0.44%). These values also closely agree with the percentage free testosterone in plasma reported by Vermeulen et QI. (1971) (2.08 f 0.60), Wang et d. (1981) (1.66+0.73%), Baxendaleet QI. (1980) (1.3-2.6%) and Dunn el al. (1981)(2.2%)in plasma of normal men. In three Klinefelter patients Vermeulen et QI. (1971) reported free testosterone fractions ranging from 0.99 to 1.25%. The absolute salivary testosterone levels (0.25 f 0.08 nmol/l) in the control subjects from the present study were almost identical to those reported by Turkes et al. (1979) (0.1 14-31 nmol/l), Baxendale et d. (1980) (0.27 + 0.07 nmol/l) and Wang et QI. ( I 98 I ) (0.29 + O - 12 nmol/l) in normal human saliva. Our values are slightly lower than those reported by Walker et d. (1980) (0.36k0.17 nmol/l) but it has to be realized that the age in our control subjects (27-54 years) was higher than in Walker's control group (1 8-36 years). This point is of some pertinence as it has clearly been shown that salivary testosterone concentrations fall with advancing age (Read et al., 1981). It has to be noted that the salivary testosterone values were almost identical to the non-protein bound, free plasma testosterone levels reported by Baxendale et QI. ( I 980) and Wang et al. (1 98 1) (0.26 f 0.05 and 0.4 1 + 0.17 nmol/l respectively) in normal men.
In the Klinefelter patients the low salivary testosterone levels (0- 14 f 0-08 nmol/l) which paralleled their low plasma testosterone values, were in line with the low free plasma testosterone levels (0.10 kO.06 nmol/l) in eleven patients with the syndrome reported by Wang et al. (1981).

Klinefelter patients’ salivary steroids 57 Together these data illustrate that salivary testosterone levels closely parallel the
reported free testosterone levels in plasma in both normal men and patients with Klinefelter’s syndrome. Wang et al. (198 1) came to the same conclusion in hyperthyroid patients even with elevated plasma levels of SHBG. Our finding of a normal salivary to plasma testosterone ratio in patients with Klinefelter’s syndrome, albeit at a lower total plasma testosterone level, reinforces this conclusion and thereby provides indirect evidence that in Klinefelter patients testosterone binding to plasma proteins does not differ from that in normal men. This agrees with the data of most (Steeno, 1970; Vermeulen et al., 1971; Wanget al., 1975) but not all investigators (Wieland et al., 1980).
Also in another respect, patients with Klinefelter’s syndrome do not differ from healthy controls. In vitro studies demonstrated that salivary binding of testosterone and androstenedione was virtually identical in both groups.*
To our knowledge no data on salivary androstenedione levels in health and disease have been reported so far. Paulsen el al. (1 968), Weinstein et al. (197 1) and Forti et al. (1 978) reported normal plasma androstenedione levels in patients with Klinefelter’s syndrome, whereas only Serrurier et al. (1976) found slightly elevated values. In the present study both salivary and plasma androstenedione levels in Klinefelter patients were similar to those in normal men, which is not surprising in view of the predominantly adrenal origin of this steroid in men (Wieland el al., 1965; Gandy et al., 1968).
Salivary androstenedione levels expressed as the percentage of total androstenedione in plasma in both normal men and Klinefelter patients (8.3k2.8 v. 9.4+2.3%) closely approximated the unbound androstenedione fraction of 7.9% calculated by Dunn et al. (1981) for plasma of normal men. It has to be noted that in normal plasma, androstenedione is only bound to a minor extent to SHBG (2.8%) in contrast to testosterone (49.9%) whereas the binding to albumin is 88 and 44% respectively.
In this relatively small series of observations in men with normal gonadal function and patients with hypogonadism, a meaningful evaluation of the relationship between the salivary levels of testosterone and the state of androgenicity could not be given (Smals et al., 1974). Nevertheless in two of the three Klinefelter patients with clinical signs of defective androgenicity (patients 5 and 7, Table 1 ), salivary testosterone levels were low, whereas at least six of the seven patients with normal salivary testosterone concentrations showed normal virilization.
Together, the data illustrate that measurement of salivary steroids by reflecting the free hormone fraction in blood may be useful in evaluating endocrine function in both health and disease.
REFERENCES
BAXENDALE, P.M., REED, M.J. &JAMES, V.H.T. (1980)Testosterone in saliva of normal men and its relationship with unbound and total testosterone levels in plasma. Journof of Endocrinology, 87.46P-47P.
* We have no explanation for the slightly but significantly higher tracer binding in saliva as compared to buffer for both steroids tested. The difference cannot be attributed to SHBG which is not present in saliva p a n g et ol., 1981). As the difference was found not only for testosterone and androstenedione but also for 17a-OH progesterone and cortisol (unpublished observation), each with different specific binding globulins, the possibility of non-specific binding to proteins (present in saliva but not in the buffer) or an artefact induced by dialysis has to be considered. It remains unclear, however, whether this phenomenon plays a role in the secretion of hormones in saliva.
58 J . J . Wellen el al.
Durn, J.F., NISULA, B.C. & RODBARD, D. (1981) Transport of steroid hormones: binding of 21 endogenous steroids to both testosterone-binding globulin and corticosteroid-binding globulin in human plasma. Journal of Clinical Endocrinology and Metabolism, 53.5868.
DVORCHIK, B.H. & VESELL, E.S. (1976) Pharmacokinetic interpretation of data gathered during therapeutic drug monitoring. Clinical Chemistry, 22,868-878.
GuNorn, P., FUSI, S. & SEFUO, M. (1978) Klinefelter’s syndrome: a study of its hormonal pattern. Journal of Endocrinological Investigation, 2, 149-154.
CANDY, H.M. & F’EIERWN, R.E. (1968) Measurement of testosterone and 17-ketosteroids in plasma by double isotope. dilution derivative technique. Journal of Clinical Endocrinology and Metabolism, 28,949-977.
GASKELL, S.J., PIKE, A.W. & G m m , K. (1980) Analysis of testosterone and dehydroepiandrosterone in saliva by gas chromatography-mass spectrometry. Steroids, 36,219-228.
HORNING, M.G., BROWN, L., NOWLIN, J., LERTUTANANGKOON, K., KELLAWAY, P. &ZION, T.E. (1977) Use of saliva in therapeutic drug monitoring. Clinical Chemistry, 23, 157-164.
KATZ, F.H. & SHANNON, I.L. (1969) Parotid fluid cortisol and cortisone. Journal of Clinical Investigation, 48, 848-855.
LANDMAN, A.D., SANFORD, L.M., HOWLAND, B.E., DAWFS, C. & PRITCHARD, E.T. (1976) Testosterone in human saliva. Experienta, 32, 940-941.
LUISI. M.. BEFWNI, G.P., DFLGGENOWXE, A., BIRINDELLI, R., BARLEITA, D., GASPERI, M. & FRANCHI, F. (1980) Radioimmunoassay of ‘free’ testosterone in human saliva. Journal of Steroid Biochemistry, 12, 513-51 6.
LULSI, M., FRANCHI, F., KICCJVIC, P.M., SILVESTRI, D., CQSSU, G., CATARSI, A.L., BAREITA, D. &GASPER], M. (1981) Radioimmunoassay for progesterone in human saliva during the menstrual cycle. Journal ofsteroid Biochemistry, 14, 1069-1073.
MCVIE, R., LEVINE, L.S. & NEW, M.I. (1979)The biologicsignificanceofthealdosteronecuncentrationin saliva. Pediatric Research, 13, 755-759.
PAULSEN, C.A., GORDON, D.L., CARPENTER, R.W., GANDY, H.M. & DRUCKER, W.D. (1968) Klinefelter’s syndrome and its variants: a hormonal and chromosomal study. Recent Progress in Hormone Research, 24,
POULSEN, K. (1969) Radioimmunoassay for angiotensine I1 to be used in direct conjunction with renin assay. Scandinavian Journal of Loboratory Investigation, 24,285-290.
PRATT, J.J., WIEGMAN, T.T., LAPP~HN, R.E. & WOLDRING M.G. (1975) Estimation of plasma testosterone without extraction and chromatography. Clinica Chimica Acta, 59, 337-346.
READ, G.F., HARPER, M.E., &LING, W.B. & GRIFFITH, K. (1981) Changes in male salivary testosterone concentrations with age. International Journal of Andrology, 4, 623-627.
RIADFAHMY, D., RVID, G.F. &WALKER, R.F. (1980) Salivary steroid assays for screening endocrine function. Postgraduate Medical Journal, 56, (Suppl. 1) 75-78.
SERRURIER, B., PFSQUm, P., MERINO, D., GUIGNARD, M., GAUTIER, D. & FROMANTTN, M. (1976) Etude des androgenes plasmatiques dans le syndrome de Klinefelter a propos de 25 a s . Annales d’Endocrinologie (Paris), 31, 501-502.
SHANNON, I.L., PROGMORE, J.R., BROOKS, R.A. &FELLER, R.P. (1959)The 17-hydroxycorticosteroidsof parotid fluid, serum and urine following intramuscular administration of repository corticotropin. Journal of Clinical Endocrinology and Metabolism, 19, 1477.
SMALS, A.G.H., KLOPPENBORC, P.W.C. & BENIUAD T.J. (1974) Body proportions and androgenicity in relation to plasma testosterone in Klinefelter’s syndrome. Acta Endocrinologica (Kbh), 77, 387-400.
SMALS, A.G.H., KLOPPENBORG, P.W.C., LEQUIN, R.M. & BENRAAD, TH.J. (1976) The effect of gonadotrophin releasing hormone on pituitary-gonadal function in Klinefelter’s syndrome. Acta Endocrinologica (Kbh), 83,829-838.
SMALS, A.G.H., KLOPPENBORG, P.W.C., PLETERS, G.F.F.M., LOSEKOOT, D.C. & BENRAAD, TH.J. ( 1 978) Basal and human chorionic gonadotropin stimulated 1701 hydroxyprogesterone and testosterone levels in Klinefelter’s syndrome. Journal of Clinical Endocrinology and Metabolism, 41, 1144-1 148.
SMALS, A.G.H.. PLFIERS, G.F. & KLOPPENBORG, P.W.C. (1981) Indirect evidence of chronic Leydig cell desensitization in Klinefelter’s syndrome. Acta Endocrinologica (Kbh), 96, 552-558.
SMITH, R.G., BESCH, P.K., DILL, B. & BUTTRAM, JR V.C. (1979) Saliva as a matrix for measuring free. androgens: comparison with serum androgens in polycystic ovarian disease. Fertility and Sterility, 31, 513-517.
STEENO, 0. (1970) Testosterone binding in human plasma. Thesis, Leuven. STEWART-BEK~LEY, M. & HORTON, R. (1973) Leydig cell function in Klinefelter’s syndrome’. Metabolirm, 22,
FORTI, G., G ~ u ~ T I , G., BORGHI, A., PAZZAGLI, M., FIORELLI, G., CABRBI, E., MANELLI, M., B-I, F.,
321-363.
875-884.

Klinefelter patients’ salivary steroidr 59 TURKES, A., TURKES, A.O., JOYCE, B.G., READ, G.F. & RIAD-FAHMY, D. (1979) Sensitive solid phase. enzyme
immunoassay for testosterone in plasma and saliva. Sferoidc, 33, 347-359. TURKES, A.O., TURKES, A., JOYCE, B.G. & RIAD-FAHMY, D. (1980) A sensitive enzyme immunoassay with a
fluonmetric end point for the determination of testosterone in female plasma and saliva. Steroidc, 35,
U-A, T., HIRAMATSU, R., IWAOKA, T., SHIMADA, T., MIURA, F. & SATO, I . (1981) Use of saliva for monitoring unbound free cortisol levels in serum. Clinic0 Chimica Acro, 110, 245-254.
VECS~, P. (1974) Glucocorticoids: cortisol, corticosterone and compound S . In Merhodc of Hormone Rodioimmunoossoy (eds B. M. Jaffe & H. R. khrmann), pp. 393-417. Academic Press, New York.
VERMEUL~, A., S~OICA., T. & VERDONCK, L. (1971) The apparent free testosterone concentration as an index of androgenicity. Journol of Clinical Endocrinology ond Metabolism, 33, 159-767.
WALKER, R.F. & FAHMY, D.R. (1978) Radioimmunoassay of 17a hydroxyprogesterone in whole saliva and parotid fluid of children with congenital adrenal hyperplasia. Journal of Endocrinology, 79, 64P-65P.
WALKER, R.F., WILSON, D.W., READ, G.F. & RIAD-FAHMY, D. (1980) Assessment of testicular function by the radioimmunoassay of testosterone in saliva. Infernofionof Journal of Andrology, 3, 1 O S I 20.
WANG, C., BAKER, H.W.G., BURGER, H.G., DE KRFSIER, D.M. & HUDSON, B. (1975) Hormonal studies in Klinefelter’s syndrome. Clinical Endocrinology, 4, 39941 I .
WANG, C., PLYMATE, S., NIFSCHLAG, E. & PAULSEN, C.A. (I98 I ) Salivary testosterone in men: further evidence of a direct correlation with free serum testosterone. Jourml of Clinical Endocrinology and Merobolism, 53,
WEINSTEIN, R.L., KAPLAN, S.L. & GRUMBACH, M.M. (1971) Gonadal and pituitary insensitivity to HCG and clomiphene stimulation in Klinefelter’s syndrome. Program of53rd Meeting ofthe Endocrine Sociefy. Son Francisco, Abstract 119.
WIELAND, R.G., DE COURCY, C. & LEVY, R.P. (1964) C19O2 steroids and some of their precursors in blood from normal human adrenals. Journal of Clinicol Inwsfigafion, 44, 159-168.
WIELAND, R.G., ZQRN, E.M. &JOHNSON, M.W. (1980) Elevated testosterone-binding globulin in Klinefelter’s syndrome. Journal of Clinical Endocrinology ond Metobolism, 51, 1199-1200.
89-101.
1021-1 024.