terapia conservativa del carcinoma differenziato della ...chped.it/gico/genova/ca differenziato...
TRANSCRIPT
Terapia conservativa del carcinoma differenziato della tiroide in età pediatrica
Maura Massimino & Paola ColliniSC di Pediatria e
Dip. di Anatomia PatologicaFond. IRCCS Istituto Nazionale Tumori, Milano
Riunione del Gruppo (CSD) Chirurgico Oncologico Venerdì 18-9-2009
Sede del 2° Congresso Nazionale Congiunto Magazzini del Cotone – Porto Antico
GENOVA
Società Italiana di Chirurgia Pediatrica
------- SICP
Associazione Italiana di Emato-Oncologia Pediatrica
------ AIEOP
Optimal treatmentfor
childhood spontaneous tumors…
... is still a controversial topic mainly because…
• these tumors are very rare (1.5% of all pediatric cancers)
• and with a behavior very different from their adult counterpart
Controversial topics
• Amount of thyroid parenchyma excision
• Amount of lymph-nodal dissection• Indications for radio-iodine therapy• Follow-up modalities (suppressive
hormonotherapy, scintigraphic and ultrasound scan, thyroglobulin value)
Natural history
No correlation among:
• initial tumor extension, relapse and mortality
• “radicality” of treatment, relapse and mortality
See also P. Miccoli, et al. Otolaryngology-Head and Neck Surgery 2008; 138: 200-203
Peculiar biology• Gene rearrangements more common than point
mutations• Ret/PTC rearrangements: higher prevalence than in
adults (47-65% vs 3-34%)• Ret/PTC1 type rearrangements is seen in 65% of cases
in older children• PAX8-PPARG fusion present in 50% of adult follicular
carcinoma has not been described in children so far• Ras and BRAF point mutations are uncommon in
children
See also: Yamashita S, et al. Nat Clin Pract Endocrinol metab 2007; 3: 422-429Dianuer CA, et al. Current Opinion in Oncology 2008; 20: 59-65

Surgical guidelines• As of now, and still often, people think that
radical excisions are needed to reach cure (Theodore Kocher, 1890 ca.)
• It is true, however, that...– radical surgery to obtain cure can
compromise quality of life with severe morbidity; neither total thyroidectomy nor complete lymph nodal dissection have to be used routinely or frequently, when treating differentiated thyroid carcinoma
(G. Crile 1953/1971)
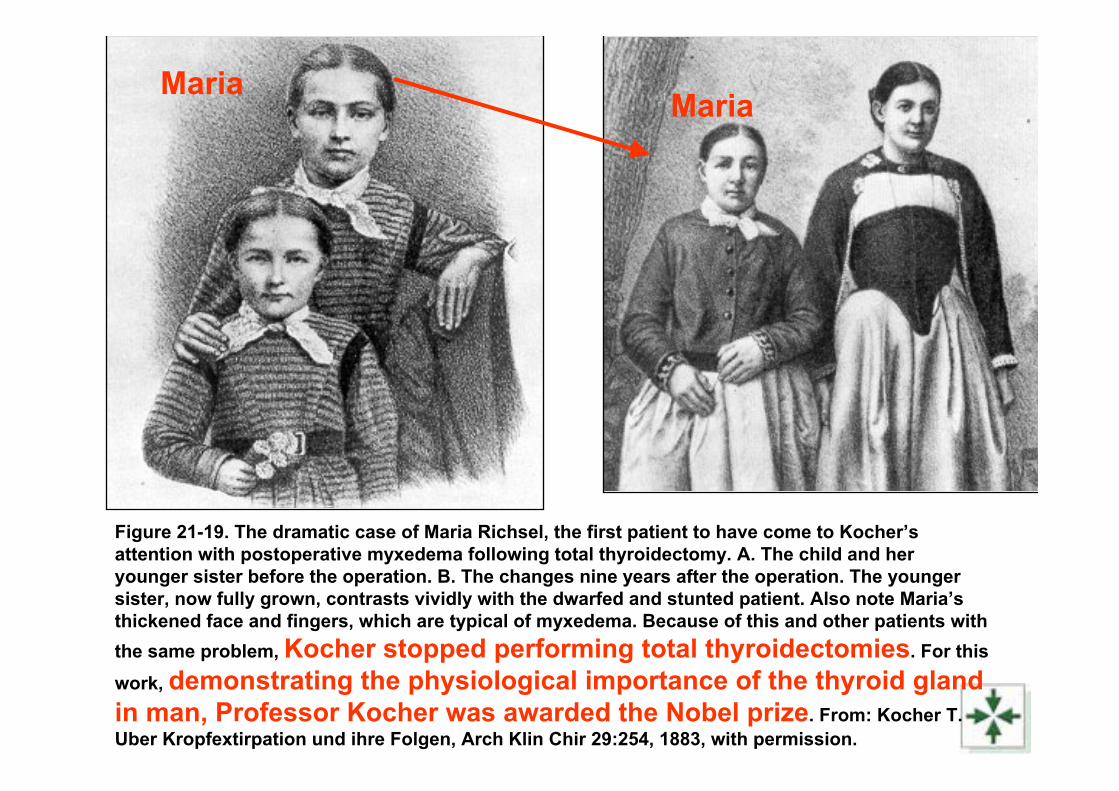
Figure 21-19. The dramatic case of Maria Richsel, the first patient to have come to Kocher’s attention with postoperative myxedema following total thyroidectomy. A. The child and her younger sister before the operation. B. The changes nine years after the operation. The younger sister, now fully grown, contrasts vividly with the dwarfed and stunted patient. Also note Maria’s thickened face and fingers, which are typical of myxedema. Because of this and other patients with the same problem, Kocher stopped performing total thyroidectomies. For this work, demonstrating the physiological importance of the thyroid gland in man, Professor Kocher was awarded the Nobel prize. From: Kocher T. Uber Kropfextirpation und ihre Folgen, Arch Klin Chir 29:254, 1883, with permission.
MariaMaria
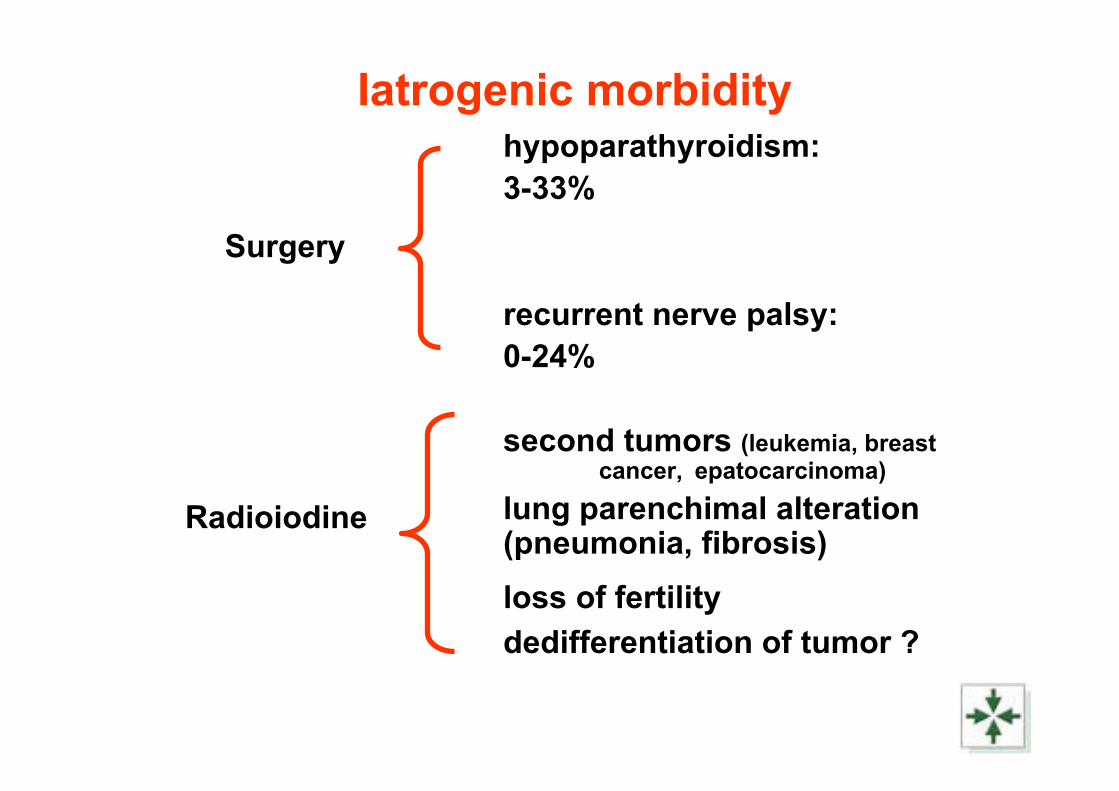
Iatrogenic morbidityhypoparathyroidism: 3-33%
recurrent nerve palsy: 0-24%
second tumors (leukemia, breastcancer, epatocarcinoma)
lung parenchimal alteration(pneumonia, fibrosis)loss of fertilitydedifferentiation of tumor ?
Surgery
Radioiodine
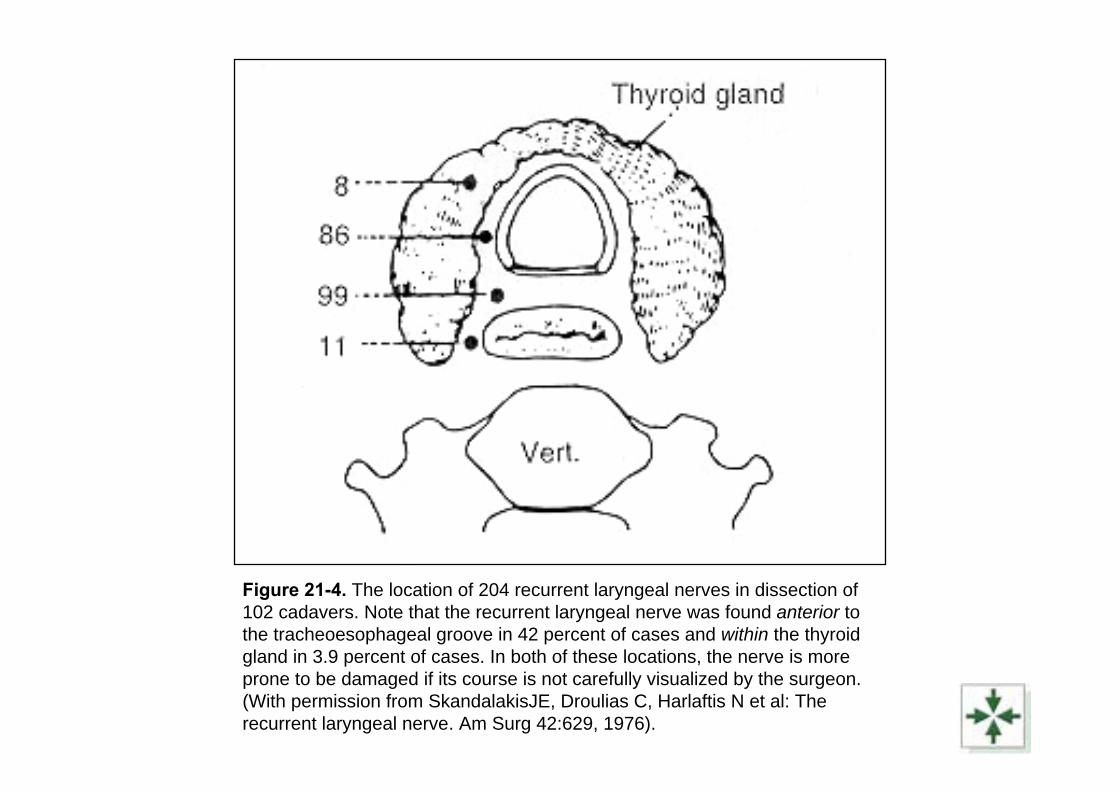
Figure 21-4. The location of 204 recurrent laryngeal nerves in dissection of102 cadavers. Note that the recurrent laryngeal nerve was found anterior to the tracheoesophageal groove in 42 percent of cases and within the thyroid gland in 3.9 percent of cases. In both of these locations, the nerve is more prone to be damaged if its course is not carefully visualized by the surgeon. (With permission from SkandalakisJE, Droulias C, Harlaftis N et al: The recurrent laryngeal nerve. Am Surg 42:629, 1976).

ALL PATIENTS (1968-2002):AGED LESS THAN 18 YEARS
68 PRIMARY TUMORS
• PAPILLARY CARCINOMA 61 (90%)
FOLLICULAR CARCINOMA
minimally invasive 4
• MEDULLARY CARCINOMA 3
42 HISTOLOGICALLY REVISEDPAPILLARY CARCINOMAS : FEATURES AT DIAGNOSIS
• 29 F (69%) median age 14 years (range 4-17)
• 13 M (31%) median age 12 years (range 6-17)
• F/M = 2.2/1• Median age of all series: 14 years • Median age of menarche: 12 years
PATIENTS AND METHODS 1• At the thyroid level, the ‘radical surgical approach’
was defined as a total thyroidectomy, independently of the grossly detectable extent of disease
• At the lymph-node level, the ‘radical surgical approach’ was defined as an elective neck dissection with the preservation of the internal jugular vein, the sternocleidomastoid muscle, the spinal accessory nerve and the greater auricular nerve, unless involved by the tumor, independently of the clinical evidence of nodal metastases.
PATIENTS AND METHODS 2• These patients, treated with the aim of obtaining
the eradication of all clinical and subclinical neoplastic foci, underwent surgery followed by metabolic ablation of thyroid remnants evaluated by routine post-surgical RAI scan
• The subtotal thyroidectomy differed from the total thyroidectomy because a rim of normal thyroid tissue was left, and subsequently metabolic ablated by RAI therapy if showing more than 3% of total activity.
PATIENTS AND METHODS 3• At the thyroid level, the ‘conservative surgical
approach’ was defined as the removal of only the thyroid lobe involved by the clinically detectable disease
• At the lymph-node level, the ‘conservative surgical approach’ consisted of a selective neck dissection of the clinically involved node levels, with preservation of the internal jugular vein, the sternocleidomastoid muscle, the spinal accessory nerve and the greater auricular nerve.
• The selective neck dissection approach had a curative intent. The “berry picking” technique was never applied in our cases
• L-thyroxin at TSH-suppressive doses (2-2.5 μg/Kg/d) was given.
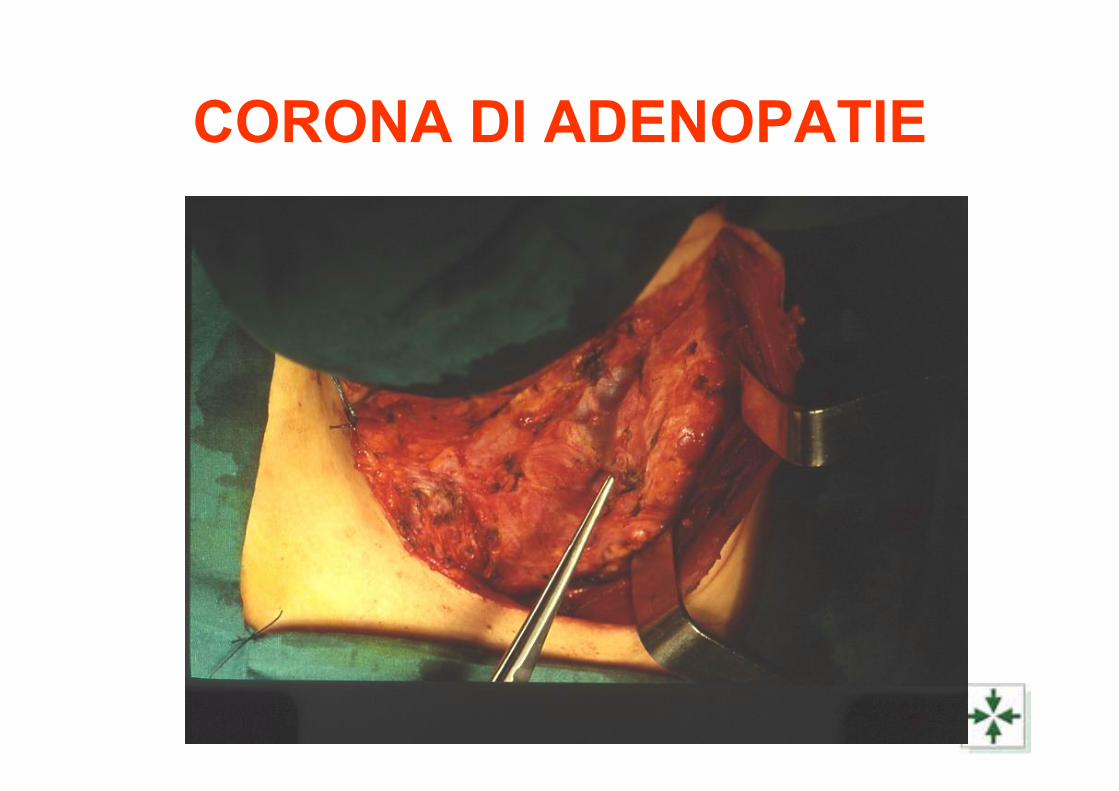
CORONA DI ADENOPATIE

INIZIO SVUOTAMENTO RICORRENZIALE
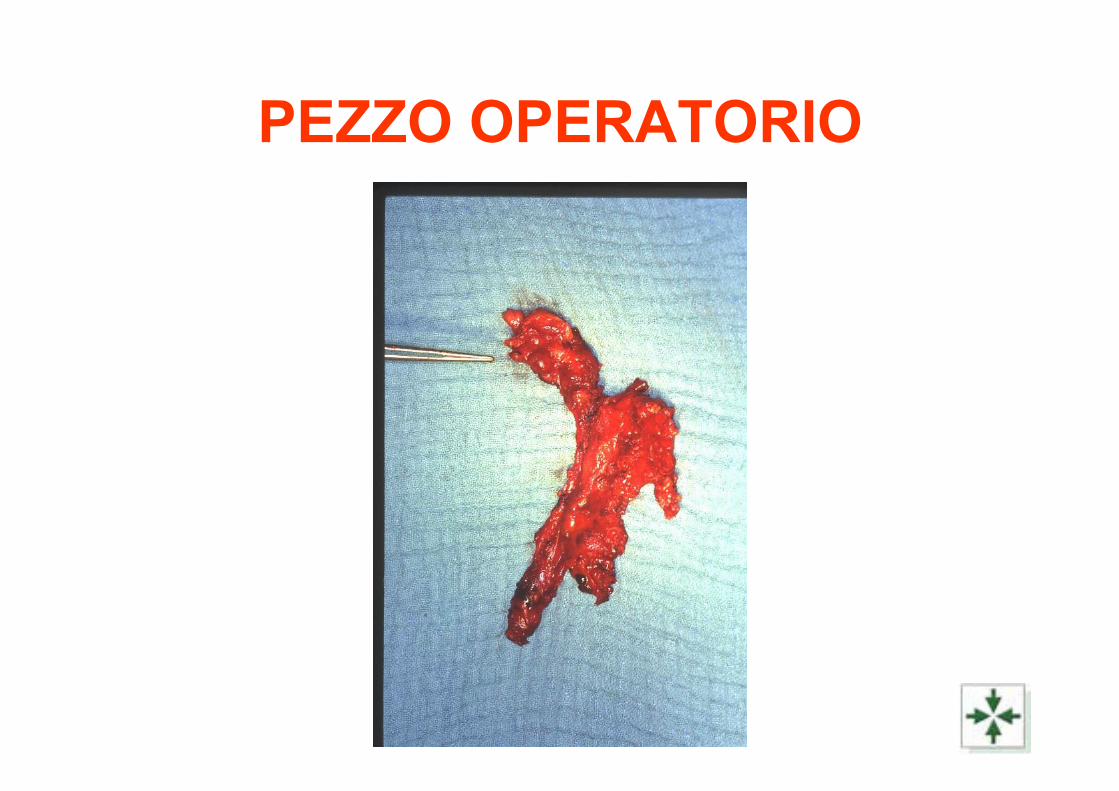
PEZZO OPERATORIO
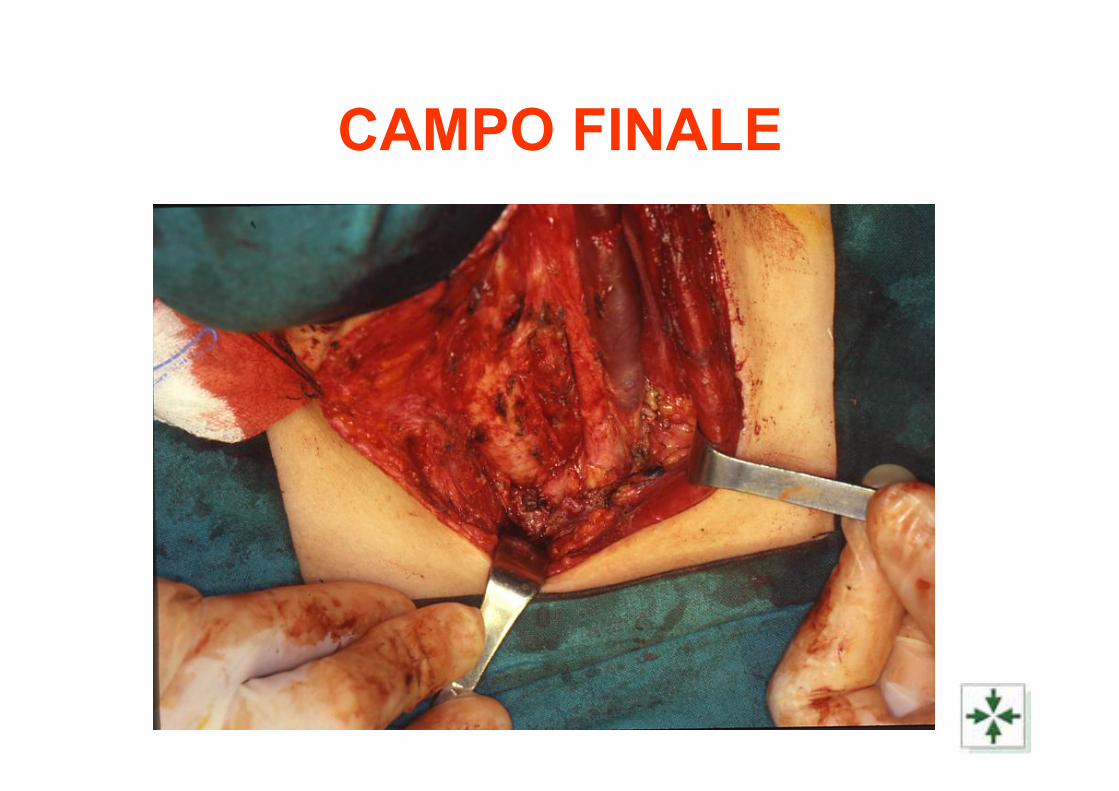
CAMPO FINALE
RESULTS 1• Out 42 cases, the radical surgical approach
at the thyroid level was justified by the presence of a
• bilateral tumor (5 cases), • a tumor involving one lobe and the isthmus
(2 cases) • or large tumors sited in the isthmus (2
cases, 3 and 3.5 cm, respectively), • and in patients with lung metastases
evident at X-rays (2 cases)
RESULTS 2• These 11 cases were excluded from the
study on the impact of the extent of thyroidectomy,
• as well as a case subjected to a subtotal thyroidectomy
• and an inoperable case with also lung metastases subjected only to a biopsy
• To avoid any possible bias, also the case that underwent total thyroidectomy for a tumor in one lobe of the thyroid and had lung metastases visible at RAI scintigraphy was excluded from statistical analyses
RESULTS 3
• Along these lines, 14 cases were excluded from the study on the prognostic significance of the extent of thyroidectomy, that is based on 28 patients with a PTC grossly involving only one lobe (27 cases)
• or with a small tumor in the isthmus (1case, 1.2 cm in diameter, that underwent the resection of the isthmus plus left lobe), without distant metastases at X-rays, that underwent radical (20 cases)
• or conservative (8 cases) thyroid surgery depending on the surgeon philosophy
• This philosophy was independent from the pediatric oncologist advice prior to 1990’s and followed prevalently the radical approach adopted for adult patients
• These subgroups of patients were homogeneously matched concerning extent of disease at diagnosis
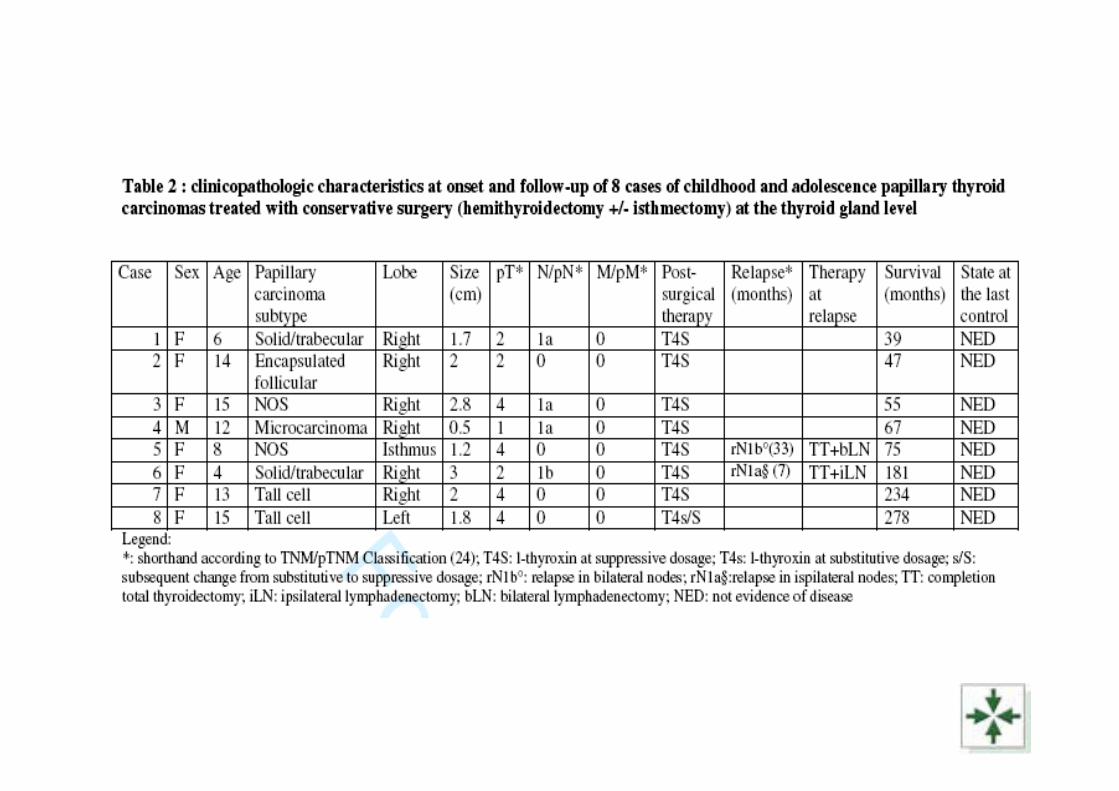
Clinicopathologic characteristics at onset and during follow-up of the 8 cases conservatively
treated at the thyroid level 1
• Hemithyroidectomy +/- isthmectomy was applied in 3 cases before and in 5 cases after 1990
• The tumor clinically involved the right lobe in 6 cases, the left lobe in 1 case, and the isthmus in 1 case
• The median diameter of the neoplastic mass was 1.9 cm (range 0.5-3 cm)
• Four cases were pT4, 3 were pT2, and 1 case was pT1
• Vascular invasion occurred in 5 cases (60%)• Nodal metastases were present in 4 cases
(ipsilateral in 3 cases, bilateral in 1 case)
Clinicopathologic characteristics at onset and during follow-up of the 8 cases conservatively
treated at the thyroid level 2
• Two patients, previously submitted to conservative nodal surgery, relapsed at nodal level after 7 and 33 months from primary surgery, respectively
• One patient had undergone selective neck dissection and the other did not undergo any nodal surgery at diagnosis in absence of clinically evident metastases
• Relapsed cases were subjected to surgery and hormonal therapy, which were effective in the cure of the relapse in every instance
RESULTS 4• At the neck node level, out of 42 patients, 28
patients underwent a selective node dissection and
• 10 patients underwent an elective neck dissection
• Four patients without node metastases at diagnosis were treated conservatively, and did not undergo any node surgery
• In sum, 32 patients were treated conservatively and 10 radically
• These subgroups of patients were homogeneously matched concerning extent of disease at diagnosis.
Clinicopathologic characteristics at onset and during follow-up of the 20 cases radically
treated at the thyroid level
• Total thyroidectomy was applied in 14 cases before and in 6 cases after 1990
• The median diameter of the tumor was 3 cm (range 0.4-9 cm)
• Ten cases were pT4, 3 were pT2, and 6 cases were pT1. One case was pTX
• Vascular invasion occurred in 5 cases (25%)
• Nodal metastases were present in all cases (ipsilateral in 11 cases, bilateral in 9 cases)
Clinicopathologic characteristics at onset and during follow-up of the 20 cases radically
treated at the thyroid level
• Five patients relapsed• 3 at lungs (7, 12, and 20 months from primary
surgery, respectively; 2 visible only on scintigraphic scan and one visible on X-rays)
• and 2 at nodal level (previously submitted to conservative nodal excision, after 13 and 19 months from primary surgery, respectively).
• Lung metastases were treated by RAI therapy and l-thyroxin at suppressive dosages
• Nodal relapsed cases were subjected to surgery and hormonal therapy, which were effective in the cure of the relapse in every instance
0
,2
,4
,6
,8
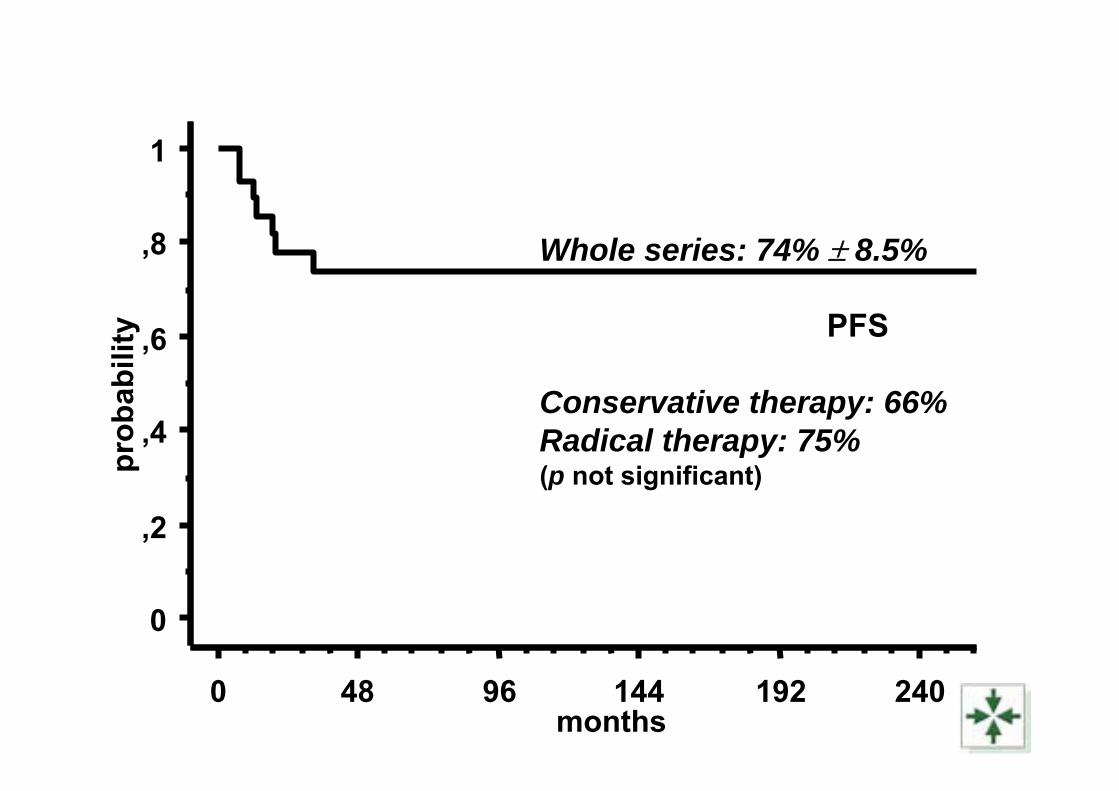
1pr
obab
ility
0 48 96 144 192 240months
Whole series: 74% ± 8.5%
PFS
Conservative therapy: 66%Radical therapy: 75%(p not significant)
Post-operative complications• Post-operative complications of thyroid surgery
occurred in 11/28 cases (39%)• Significantly, they occurred only in patients that
had undergone total thyroidectomy (in 8 out of 20 total thyroidectomies performed in this series, 40%)
• as permanent (> 6 months) hypoparathyroidismin 6 cases (21% of the whole series, and 30% of totally thyroidectomized cases)
• and recurrent laryngeal nerve deficit in 2 cases (7% of the whole series, and 10% of totally thyroidectomized cases)
• Hypoparathyroidism required life-long medication. Parathyroid transplantation was never applied
• Post-operative complications of neck node surgery occurred in 4/38 cases (10.5%), as spinal accessory nerve deficit in 2 cases and perioperatory pneumothorax in 2 cases
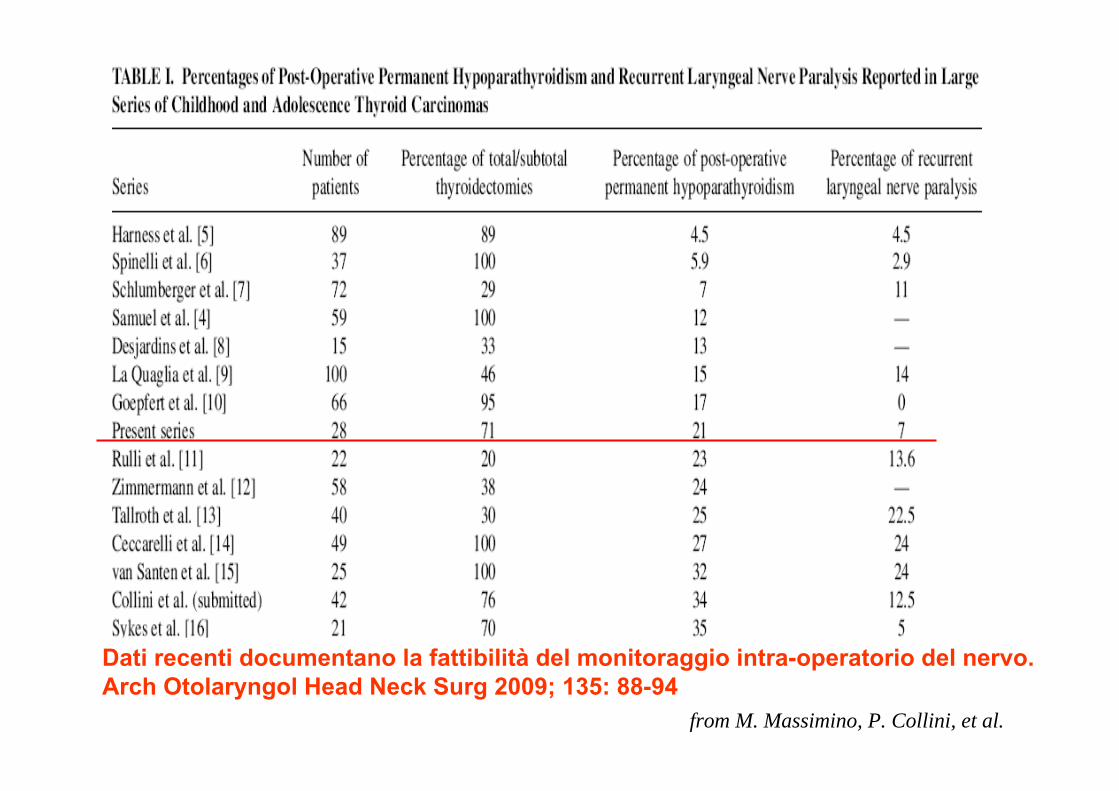
from M. Massimino, P. Collini, et al.
Dati recenti documentano la fattibilità del monitoraggio intra-operatorio del nervo.Arch Otolaryngol Head Neck Surg 2009; 135: 88-94
CONCLUSIONS 1• The application of a conservative surgery
at thyroid level did not influence either PFS or OS
• Actually, both PFS and OS proved to be independent of the type of surgery (conservative vs radical) at the thyroid level in two groups of patients homogeneously matched concerning the extent of disease at onset, in agreement with the results of others
CONCLUSIONS 2• Actually, the presence of microscopic foci is quite
common in PTCs• We found up to 70% of ipsilateral and 20% of
contralateral neoplastic microfoci in the thyroid glands, and 70% of subclinical nodal metastases. No clinical local relapse occurred
• Nodal relapses occurred in 4 out of 32 patients (12.5%) that had undergone a conservative nodal approach at diagnosis. These patients had their disease controlled by further surgery and hormonal manipulation
• Notably, only one of the 4 patients that did not undergo nodal surgery at diagnosis in absence of clinical nodal metastases relapsed.
…
• All these results highlight the extremelyhigh sensitivity to hormonal manipulation, that can control the subclinical diseaseand prevent the occurrence of clinicalrelapse
• This sensitivity to hormonal manipulationseems to represent an importantbiological difference with respect to adultPTC s
…• The percentage of permanent post-operative
complications in the cases in our series thatunderwent total thyroidectomy was distressinglyhigh (40%, being 39% in the whole case series)
• we registered the occurrence of permanent hypoparathyroidism in the 21% of the whole case series and in 30% of totally thyroidectomizedcases,
• and recurrent laryngeal nerve deficit in 7% of the whole series and in 10% of totally thyroidectomized cases.
• We registered also quite high percentages of complications subsequent to neck dissection, represented by spinal accessory nerve deficit and perioperatory pneumothorax, even if a functional neck dissection was always adopted
HOW DIFFICULT IS HYPOPARATHYROIDISM CARE?• Case report. VDF, 8 yrs: 1-year history of neck mass, ultrasound isthmic
nodule of 1.5 cm, FNA pos. for papillary ca.
• 12/2/98 isthmectomy+left emithyroidectomy
– Papillary ca nos 1.2 cm infiltrating surrounding soft tissue (pT4)
• 10/00 progression with left recurrential node enlargement and localsuspicious relapse
• 8/11/00 left recurrent lymphadenectomy and biopsy of right recurrentnodes suspicious at operatory inspection
• 24/1/01 right emithyroidectomy and right recurrent lymphadenectomy(level 2,3,4,5)
– Papillary ca at nodes, not at right thyroid but surrounding tissue
– Hypoparathyroidism check every week for 6 mos, every month for 6 mos, each other monthfor 2 yrs, every 6 mos so far
• 3/02 menarch
• CCR
And how much is the cost for Italian Public Health System ?
Blood exam for Calcium, Phosphorus, and clinical survey = 23.11 €
If also PTH is evaluated = 48.28 €
• PFS/OS were independent of the type of surgery (prophylactic vs conservative)
• Childhood PTC showed sensitivity to hormonal manipulation both at diagnosis and at relapse
CONCLUSIONS 3
• Thyroid carcinomas in children and adults are different diseases and notmerely different stages of a samedisease……with specific prognosis and therapy needs(Cady B. Cancer 1998; 83: 844-47Surgery 1998; 124: 947-57)
CONCLUSIONS 4
→ presence of neoplastic microfoci, vascular invasion and nodal metastases are very common and not related to final outcome
CONCLUSIONS 5
OUR APPROACHTherapy of choice in cases with tumor limited to one
lobe and without clinical evidence of distant
metastases → REMOVAL OF ALL MACROSCOPIC
DISEASE AT THYROID AND NODAL LEVEL +
SUPPRESSIVE HORMONOTHERAPY
and life-long follow-up to adjust therapy over time
MORE AGGRESSIVE THERAPEUTICAL APPROACHES
HAVE TO BE APPLIED ONLY TO SELECTED CASES

CARCINOMA DI DERIVAZIONECARCINOMA DI DERIVAZIONEDALL’EPITELIO FOLLICOLARE DELLADALL’EPITELIO FOLLICOLARE DELLA
TIROIDE IN TIROIDE IN ETA’ ETA’ PEDIATRICAPEDIATRICA
PROF. C. SPINELLIPROF. C. SPINELLI DOTT. A. INSERRADOTT. A. INSERRA DOTT. DOTT.ssa ssa M. MASSIMINOM. MASSIMINO DOTT.DOTT.ssa ssa P. COLLINIP. COLLINI DOTT. F. MATTAVELLI DOTT. F. MATTAVELLI DOTT. A. GROSSIDOTT. A. GROSSI DOTT. DOTT.ssa ssa M. C. GARGANESEM. C. GARGANESE DOTT. E. SEREGNIDOTT. E. SEREGNI
Clinica Chirurgica Pediatrica, Università di Pisa,Clinica Chirurgica Pediatrica, Università di Pisa,Chirurgia Pediatrica ed Endocrinologia, Ospedale Bambino Gesù, RomaChirurgia Pediatrica ed Endocrinologia, Ospedale Bambino Gesù, RomaOncologia Pediatrica, Anatomia Patologica, Otorinolaringoiatria eOncologia Pediatrica, Anatomia Patologica, Otorinolaringoiatria eMedicina Nucleare, INT , MilanoMedicina Nucleare, INT , Milano
PROPOSTA DI LINEE GUIDA PEDIATRICHEPROPOSTA DI LINEE GUIDA PEDIATRICHEA CURA DIA CURA DI