symptoms after vestibular neuritis and the high velocity
TRANSCRIPT
1
Chronicsymptomsaftervestibularneuritisandthehigh
velocityvestibulo‐ocularreflex
MiteshPatel1,2,QadeerArshad1,REdwardRoberts1,HenaAhmad1,AdolfoM.Bronstein1*
1DepartmentofNeuro‐otology,DivisionofBrainSciences,ImperialCollegeLondon,Charing
CrossHospitalCampus,FulhamPalaceRoad,LondonW68RF,UK.Tel:+44(0)2033135525,
Fax:+44(0)2033117577
2SchoolofHealth,Sports&Biosciences,UniversityofEastLondon,StratfordCampus,Water
Lane,London.E154LZ.
*Correspondence:[email protected]
Shortrunninghead:ChronicsymptomsandtheVOR
WordCount:1867
ConflictsofInterestandSourcesofFunding
Theauthorsreportnoconflictsofinterest.TheresearchwassupportedbytheUKMedical
ResearchCouncil(MR/J004685/1).
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by UEL Research Repository at University of East London
2
Abstract
Hypothesis:Astheanteriorandposteriorsemicircularcanalsarevitaltotheregulationofgaze
stability,particularlyduringlocomotionorvehiculartravel,wetestedwhetherthehighvelocity
vestibulo‐ocularreflex(VOR)ofthethreeipsilesionalsemicircularcanalselicitedbythe
modifiedHeadImpulseTestwouldcorrelatewithsubjectivedizzinessorvertigoscoresafter
vestibularneuritis(VN).
Background:RecoveryfollowingacuteVNvarieswitharoundhalfreportingpersistent
symptomslongaftertheacuteepisode.However,anunansweredquestioniswhetherchronic
symptomsareassociatedwithimpairmentofthehighvelocityVORoftheanteriororposterior
canals.
Methods:TwentypatientswhohadexperiencedanacuteepisodeofVNatleastthreemonths
earlierwereincludedinthisstudy.Participantswereassessedwiththevideoheadimpulsetest
(vHIT)ofallsixcanals,bithermalcaloricirrigation,theDizzinessHandicapInventory(DHI)and
theVertigoSymptomsScaleshort‐form(VSS).
Results:Ofthese20patients,12feltthattheyhadrecoveredfromtheinitialepisodewhereas8
didnotandreportedelevatedDHIandVSSscores.However,wefoundnocorrelationbetween
DHIorVSSscoresandtheipsilesionalsingleorcombinedvHITgain,vHITgainasymmetryor
caloricparesis.ThehighvelocityVORwasnotdifferentbetweenpatientswhofelttheyhad
recoveredandpatientswhofelttheyhadnot.
Conclusions:OurfindingssuggestthatchronicsymptomsofdizzinessfollowingVNarenot
associatedwiththehighvelocityVORofthesingleorcombinedipsilesionalhorizontal,anterior
orposteriorsemicircularcanals.
Keywords:Vestibular;vestibularneuritis;dizziness;vertigo,head‐impulsetest
3
Introduction
Vestibularneuritis(VN)isanacutedisordercharacterisedbyvertigo,nausea,vomitingand
imbalancefollowingsuddenunilaterallossofperipheralvestibularfunction(1).Recoveryis
throughperipheralandcentralvestibularcompensation(2).Typically,symptomslastdaysor
weeksbutaround50%ofpatientsexperiencechronicdizziness,unsteadinessandspatial
disorientation(3,4).
Ithasbeenpostulatedthatpersistentperipheralvestibularlosscouldaccountforthesechronic
symptoms(5).Thestandardmeasureofperipheralvestibularlossisthegainofthevestibulo‐
ocularreflex(VOR)whichistheratioofthesizeofslowphasecorrectiveeyemovementtothe
sizeofheadmovement(peakslowphaseeyevelocity/peakheadvelocity).TheVORmaintains
gazestabilityandpreservesvisualacuityduringheadmovements.Impairmentcancausevisual
blurringduringheadmotion(6),whichcouldbeinterpretedbythepatientasdizziness,
unsteadinessorspatialdisorientation.Thus,acentralquestionregardingtheprocessof
symptomrecoveryiswhetherthisisrelatedtoadysfunctionalVOR.
PreviousstudieshaveshownthatthelowvelocityVORresponsefromthecalorictestdoesnot
predictchronicsymptomsofdizzinessorvertigo(3,7,8).However,recentadvanceshaveledto
thedevelopmentofabedsideclinicalheadthrustorimpulsetest(HIT)measuringthehigh
velocityVORofallsixsemicircularcanals(9).ThehighvelocityVORelicitedbytheHITrecovers
moreslowlyfollowingacuteVNcomparedtothelowvelocityVORelicitedbycaloricirrigation
(10‐12),andmaythusbetterreflectclinicaloutcome.
Interestingly,Pallaandcolleagues(13)haveshownthatthereisnorelationshipbetweenthe
highvelocityhorizontalcanalVORgainandchronicsymptomsfollowingVN.However,asthe
anteriorandposteriorsemicircularcanalsarevitaltotheregulationofgazestability(14),
particularlyduringlocomotionorvehiculartravel,weposedthequestionofwhetherthehigh
velocityVORgainofthethreeipsilesionalsemicircularcanals(elicitedbythemodifiedHIT(9))
4
wouldpredictsubjectivedizzinessorvertigoscoresafterVN.ThelowvelocityVORofthe
horizontalcanal(elicitedbycaloricirrigation)wasmeasuredforcomparison.
MaterialsandMethods
Twentypatients(7male,31‐87years(mean57.3+/‐18)withclinicalhistories,physical
examinationsandfunctionteststypicalofacuteVNwererecruitedi.e,horizontalnystagmus,
clinicallyabnormalhead‐impulsetestandasignificantcanalparesis.Ofourpatients,nonehad
inferiorvestibularneuritis.Theexclusioncriteriawerepatientswithnocurrentindicationsof
overlappingvestibularmigraine.Forthisstudy,allpatientsweretestedinthechronicstageof
VN(3‐36monthsafteracuteVNonset;mean9.8+/‐7.5),includingarepeatcalorictest.
Informedconsentwasobtainedfromallsubjects.
Vestibularassessment
Six‐canalvHIT:EyeandheadmovementsweresimultaneouslyrecordedusingtheICSvideo
HeadImpulsesystem(vHIT,GNOtometrics,Denmark).Thesystemconsistsofapairoflight‐
weightgogglescontaining3‐Dgyroscopestomeasureheadvelocity,andasmallmountedvideo
cameratorecordeyeposition.Thevideocameraismountedwithintherighteye‐frameofthe
goggles,whichweresecuredfirmlytothesubject’sheadwithanadjustableelasticstrap.
Thepatientwasinstructedtofixateonatargetpositionedapproximately1.5metresinfrontof
them.Theexaminer,whileholdingthepatient’sheadfrombehind,thenmadeaseriesofbrisk
headmovements(10–20°amplitude)correspondingtothehorizontal,leftanterior‐right
posterior(LARP)andrightanterior‐leftposterior(RALP)canalplanes(15).Incontrasttoearly
papersmeasuringVORresponsesalongtheLARPandRALPplanes(16),withthevHIT
5
techniquetheheadmustbeturnedinyawbyapproximately40‐45osothattheheadimpulse
deliveredonly(ormostly)elicitsverticalVORmovements.
Eyeandheadvelocitiesweresampledat250Hzandtheratioofeye‐to‐headpeakvelocity(VOR
gain)wascalculatedforeachsemicircularcanalfromanaverageof20headimpulses
performedoverarangeofvelocities(50–300°/s)(17).Asymmetrybetweentheipsilesionaland
contralesionalcanalswasalsocalculatedandexpressedasapercentage(18).
Inadditiontothesinglecanalgainvaluesandasymmetryvaluesgeneratedautomaticallybythe
vHITprogram,wecalculatedatotalgainforeachside:
3⁄ ,andtotal
right/leftasymmetry(%).Aspreviousstudieshavereportednocorrelationbetweenhorizontal
canalvHITgainorasymmetrywithlong‐termrecovery,wealsofocussedontheverticalcanals
andcalculatedaverticalcanalgain 2⁄ ,and
verticalcanalright/leftasymmetry(%).Theseformulaeprovideoverallvaluesforthe
contributionsfromeachcanal.
Calorictest:Bithermalcaloricirrigations(30&44°C)wereperformed(ICSCHARTR,GN
Otometrics,Denmark)andthedegreeofcanalparesiswascalculatedusingJongkeesformula
andexpressedasapercentageaspreviousstudies(18).
Symptomsquestionnaires
Inparallel,symptomsduringthepastmonthwerescoredwiththeDizzinessHandicap
Inventory(DHI)(19)andtheVertigoSymptomsScaleshortform(VSS)(20).Wealsoaskedeach
patientwhethertheyfelttheyhadrecoveredfromtheacuteepisodeornot.
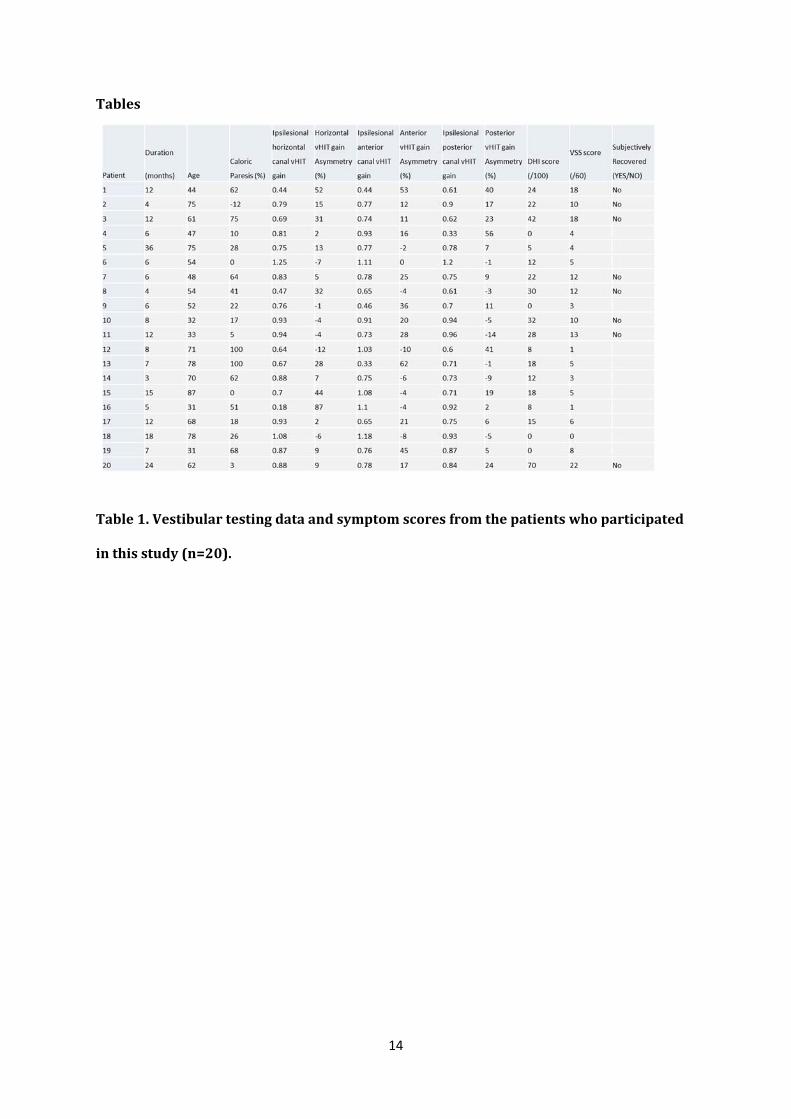
‐Table1abouthere‐
6
PearsonCorrelationCoefficientanalyseswereemployedbetweenallmeasures.Independent
samplest‐testswereusedasconfirmation.LinearregressionwasusedtotestwhethervHIT
gainspredictDHIorVSSscores.P‐valueswerecorrectedformultiplecomparisons.
Results
AsshowninTable1,eightpatientsfeltthattheyhadnotfullyrecoveredfromtheacuteepisode.
ThesepatientsalsohadthehighestDHIandVSSscores(pairedt‐testP<0.002).Therewasa
strongsignificantcorrelationbetweenDHIandVSSacrossthegroupof20VNpatients
(P<0.001,PearsonCorrelationCoefficient=0.857).Therewasnocorrelationbetweencaloric
paresisandDHIscore(Pearsoncorrelationcoefficient=‐0.134,P=0.57)orbetweencaloric
paresisandVSSscore(Pearsoncorrelationcoefficient=‐0.076,P=0.572).Therewasalsono
correlationbetweencaloricparesisandhorizontalcanalvHITgainasymmetry(Pearson
correlationcoefficient=0.176,P=0.458).
Withlinearregression,theadjustedR‐squarewas0.02forDHIscoresand0.084forVSSscores.
TheregressionwasnotsignificantforeitherDHIscores(F[0.47],P=0.82)orVSSscores
(F[1.29],P=0.327).Similarly,stepwiselinearregressionidentifiednopredictingindependent
variablesintheanalysis(novariableswereenteredintotheanalysisforeitherDHIorVSS).
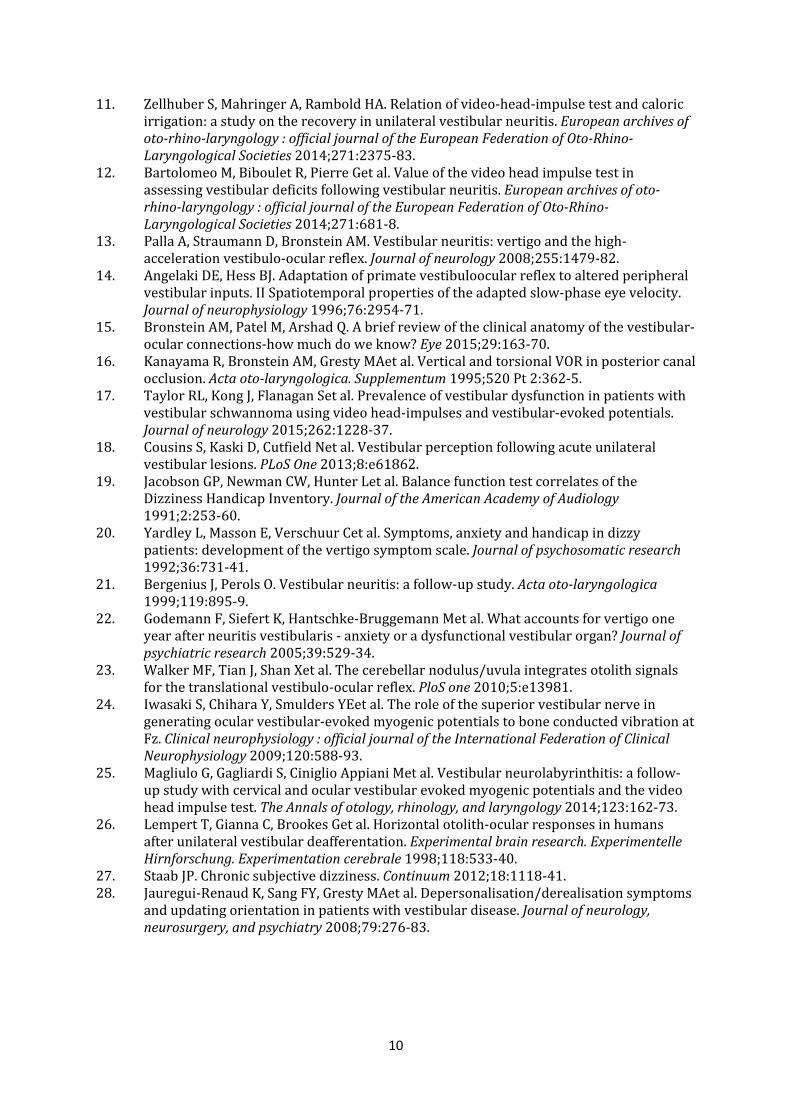
AsshowninFigure1A‐F,therewasnocorrelationbetweentheipsilesionalvHITgainsforthe
horizontal,anteriorandposteriorcanalsandvHITgainasymmetryforthehorizontal,anterior
andposteriorcanalsversusDHIscore.
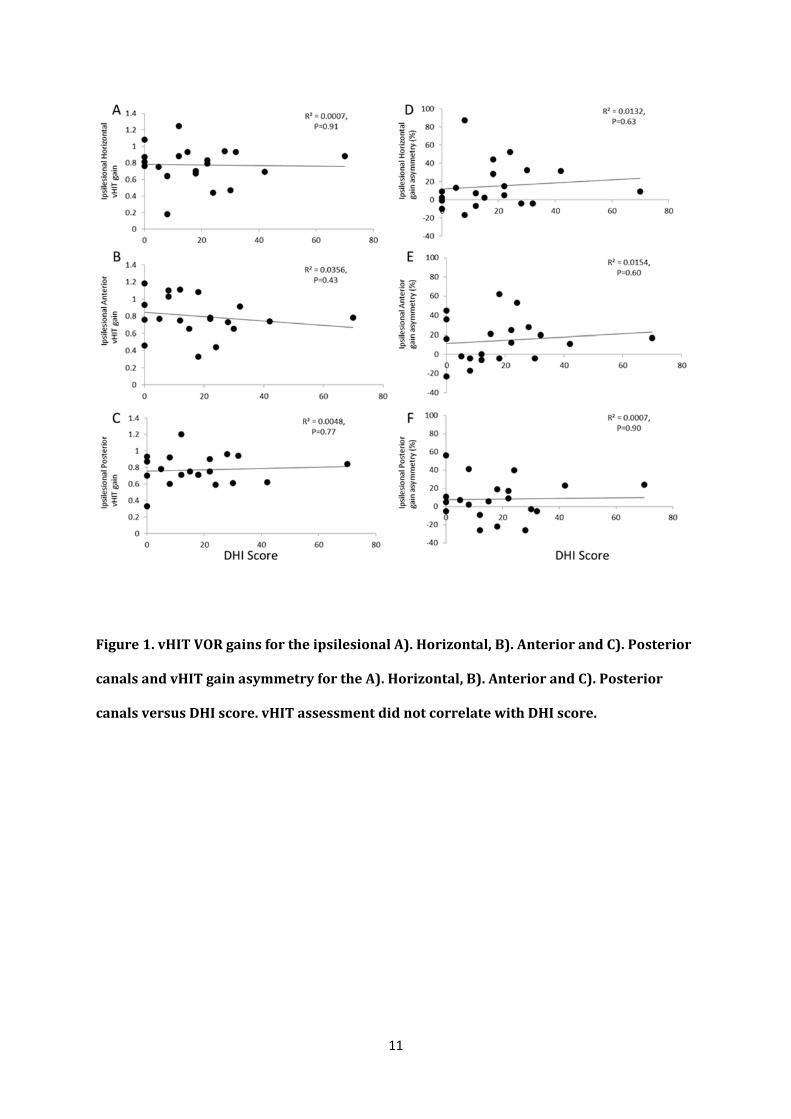
AsshowninFigure2A‐F,therewasalsonocorrelationbetweentheipsilesionalvHITgainsfor
thehorizontal,anteriorandposteriorcanalsandvHITgainasymmetryforthehorizontal,
anteriorandposteriorcanalsversusVSSscore.
7
WealsocomparedvHITgainsandvHITgainasymmetriesforthehorizontal,anteriorand
posteriorcanalsbetweenthe8patientswhofelttheyhadnotrecoveredandthe12patients
whofelttheyhadrecovered.Independentsamplest‐testsshowednodifferencebetweenthese
groups(P=0.26‐0.92).
‐Figure1abouthere‐
‐Figure2abouthere‐
WealsoinvestigatedtherelationshipbetweenvHITresponseandrecoverybygroupingthe
vHITsinglecanalgainsintothemeansumofthecanalvectorstogiveasinglegainvalueforthe
ipsilesionalandcontralesionalsides.Wealsogroupedtheipsilesionalsemicircularcanalsintoa
singlevaluefortheanteriorandposterior(vertical)canalsgainandasymmetry,asdescribedin
Methods.
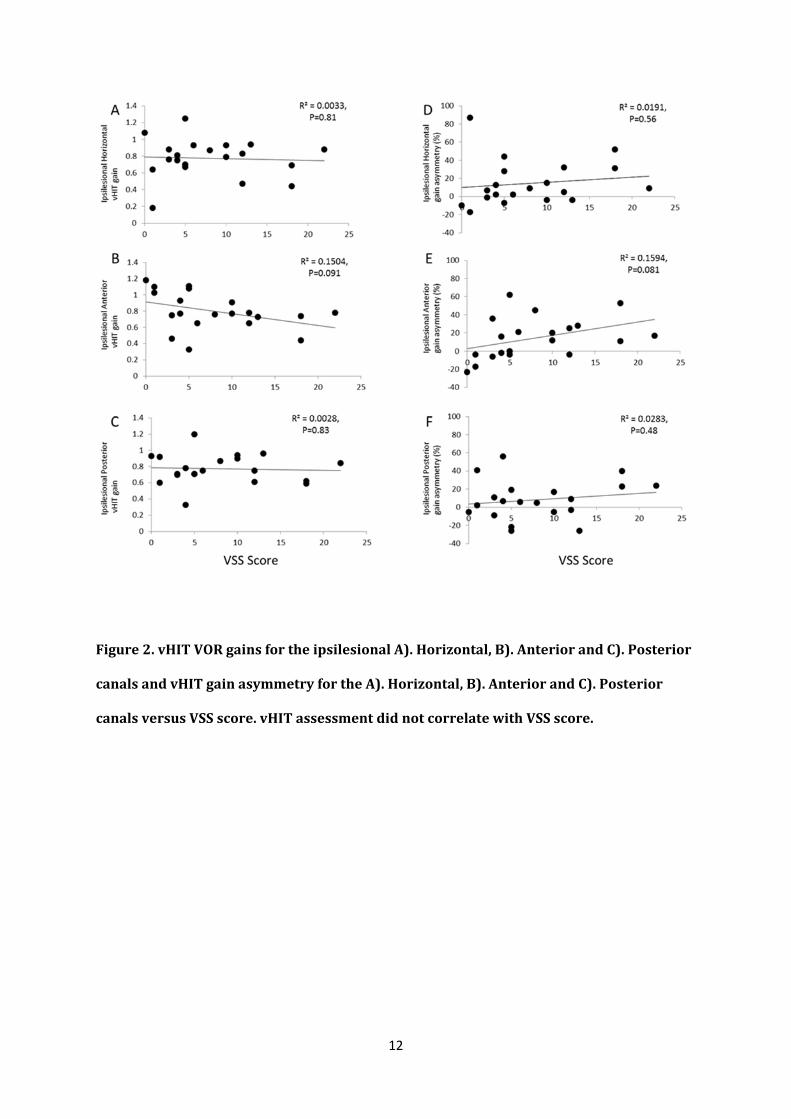
Wefoundnosignificantcorrelationbetweenthevectorsumofthethreeipsilesionalcanalgains
(horizontal+anterior+posterior)andDHIscores(Pearsoncorrelationcoefficient=‐0.124,
P=0.60)orVSSscores(Pearsoncorrelationcoefficient=‐0.302,P=0.196).Asymmetrydidnot
correlatetoDHI(P=0.55)orVSSscores(P=0.13)asshowninFigures3Aand3B.
Inaddition,therewasnosignificantcorrelationbetweenthevectorsumoftheverticalcanals
(anterior+posterior)andDHIscores(Pearsoncorrelationcoefficient=‐0.125,P=0.60)orVSS
scores(Pearsoncorrelationcoefficient=‐0.152,P=0.15).AsymmetrydidnotcorrelatewithDHI
(P=0.77)orVSSscores(P=0.10)asshowninFigures3Cand3D.
NeithertotalnorverticalcanalgainandasymmetryvaluesweresignificantpredictorsofDHIor
VSSscoreswithmultipleregressionanalysis,i.e.,novalueswereenteredintotheanalysis
duringstepwiseregression.
‐Figure3abouthere‐

8
Discussion
Here,wefindnoevidencetosupportthehypothesisthatchronicsymptomsofdizzinessor
vertigofollowingacuteVNareassociatedwiththehighvelocityVORofthethreeipsilesional
semicircularcanals.TherewasnocorrelationbetweenipsilesionalhighvelocityVORgainor
gainasymmetryofthesingleorcombinedhorizontal,anteriorandposteriorcanalsmeasured
withthevHITandDHIorVSSscores.Patient4isarepresentativeexample:thisindividualwas
asymptomatic(DHI=0)buthadanipsilesionalposteriorcanalgainof0.33.Incontrast,patient
20whowasthemostsymptomaticindividual(DHI=70)hadnormalvHITgainsforeachofthe
canals(above0.78).
Also,asinpreviousstudies,therewasnocorrelationbetweencaloricparesisandchronic
symptomsafterVN(21,22)orbetweencaloricparesisandhorizontalcanalHITasymmetry(11)
probablyreflectingthedifferentfrequencyrangesofthesetests.
ThereislittledoubtthatacuteVNtriggeredthepatients’chronicsymptoms,howeverresidual
semicircularcanaldeficitsmightnotbeacrucialfactor.Astheotolithsareinvolvedinthe
translationalVOR(tVOR)(23),itispossiblethatimpairedotolithfunctioncouldexplainchronic
symptomsinsomepatients.UtricularfunctionistypicallyaffectedinVNasmeasuredwith
ocularVEMP(oVEMP)(24).Inaone‐yearfollow‐upstudyinVNpatients,Magliuloand
colleagues(25)foundthatfouroutoffivepatientswithchronicsymptoms,hadabsent
ipsilesionaloVEMPresponses.Saccularfunctionisimpairedwhentheinferiorbranchofthe
vestibularnerveisaffected.However,itisunlikelythatotolithdamagewouldbethecritical
variablepredictinglongtermoutcomeinVNgiventhatevenpatientswithvestibular
neurectomyrecoverwell(26).
Anotherexplanationisthattherelativeweightingsofvestibular,visualandsomatosensory
signalschangefollowingunilateralvestibularloss.Indeed,wehavefoundthatchronic
symptomsafterVNmayrelatetoincreasedvisualdependence(3).Psychological(22,27)and
spatialorientationfactors(28),alsohaveastronginfluenceonlongtermoutcome.
9
Thesamplesizeusedinthisstudy(n=20)isalsoapotentiallimitation,butifthiswerethecase
itwouldimplythattherelationshipbetweenclinicaloutcomeandvHITgainsisveryweakand
thereforeunlikelytobesensitiveenoughtobeofpracticaluseinaclinicalenvironment.Using
meanandstandarddeviationdatafromourstrongestcorrelationcoefficient(Figure2E,
anteriorcanalgainvsVSS)wecalculatedthatsubjectsrecruitedwouldneedtoequaln=58to
achieveP<0.05(Power=0.8)beforecorrectionformultiplecomparisons.
Toconclude,chronicsymptomsofdizzinessorvertigofollowingacuteVNwerenotrelatedto
thehighvelocityVORofthehorizontal,anteriororposteriorsemicircularcanals.Itislikelythat
clinicalrecoveryandoutcomedependsmostlyoncentralcompensation,includinghigherlevel
processinginthebrain.
References
1. DixMR,HallpikeCS.Thepathology,symptomatologyanddiagnosisofcertaincommondisordersofthevestibularsystem.TheAnnalsofotology,rhinology,andlaryngology1952;61:987‐1016.
2. JeongSH,KimHJ,KimJS.Vestibularneuritis.Seminarsinneurology2013;33:185‐94.3. CousinsS,CutfieldNJ,KaskiDetal.Visualdependencyanddizzinessaftervestibular
neuritis.PLoSOne2014;9:e105426.4. KammerlindAS,LedinTE,SkargrenEIetal.Long‐termfollow‐upafteracuteunilateral
vestibularlossandcomparisonbetweensubjectswithandwithoutremainingsymptoms.Actaoto‐laryngologica2005;125:946‐53.
5. CurthoysIS,HalmagyiGM.Vestibularcompensation:areviewoftheoculomotor,neural,andclinicalconsequencesofunilateralvestibularloss.Journalofvestibularresearch:equilibrium&orientation1995;5:67‐107.
6. MacdougallHG,CurthoysIS.PlasticityduringVestibularCompensation:TheRoleofSaccades.Frontiersinneurology2012;3:21.
7. ShupakA,IssaA,GolzAetal.Prednisonetreatmentforvestibularneuritis.Otology&neurotology:officialpublicationoftheAmericanOtologicalSociety,AmericanNeurotologySociety[and]EuropeanAcademyofOtologyandNeurotology2008;29:368‐74.
8. OkinakaY,SekitaniT,OkazakiHetal.Progressofcaloricresponseofvestibularneuronitis.Actaoto‐laryngologica.Supplementum1993;503:18‐22.
9. MigliaccioAA,CremerPD.The2Dmodifiedheadimpulsetest:a2Dtechniqueformeasuringfunctioninallsixsemi‐circularcanals.Journalofvestibularresearch:equilibrium&orientation2011;21:227‐34.
10. Schmid‐PriscoveanuA,BohmerA,ObzinaHetal.Caloricandsearch‐coilhead‐impulsetestinginpatientsaftervestibularneuritis.JournaloftheAssociationforResearchinOtolaryngology:JARO2001;2:72‐8.
10
11. ZellhuberS,MahringerA,RamboldHA.Relationofvideo‐head‐impulsetestandcaloricirrigation:astudyontherecoveryinunilateralvestibularneuritis.Europeanarchivesofoto‐rhino‐laryngology:officialjournaloftheEuropeanFederationofOto‐Rhino‐LaryngologicalSocieties2014;271:2375‐83.
12. BartolomeoM,BibouletR,PierreGetal.Valueofthevideoheadimpulsetestinassessingvestibulardeficitsfollowingvestibularneuritis.Europeanarchivesofoto‐rhino‐laryngology:officialjournaloftheEuropeanFederationofOto‐Rhino‐LaryngologicalSocieties2014;271:681‐8.
13. PallaA,StraumannD,BronsteinAM.Vestibularneuritis:vertigoandthehigh‐accelerationvestibulo‐ocularreflex.Journalofneurology2008;255:1479‐82.
14. AngelakiDE,HessBJ.Adaptationofprimatevestibuloocularreflextoalteredperipheralvestibularinputs.IISpatiotemporalpropertiesoftheadaptedslow‐phaseeyevelocity.Journalofneurophysiology1996;76:2954‐71.
15. BronsteinAM,PatelM,ArshadQ.Abriefreviewoftheclinicalanatomyofthevestibular‐ocularconnections‐howmuchdoweknow?Eye2015;29:163‐70.
16. KanayamaR,BronsteinAM,GrestyMAetal.VerticalandtorsionalVORinposteriorcanalocclusion.Actaoto‐laryngologica.Supplementum1995;520Pt2:362‐5.
17. TaylorRL,KongJ,FlanaganSetal.Prevalenceofvestibulardysfunctioninpatientswithvestibularschwannomausingvideohead‐impulsesandvestibular‐evokedpotentials.Journalofneurology2015;262:1228‐37.
18. CousinsS,KaskiD,CutfieldNetal.Vestibularperceptionfollowingacuteunilateralvestibularlesions.PLoSOne2013;8:e61862.
19. JacobsonGP,NewmanCW,HunterLetal.BalancefunctiontestcorrelatesoftheDizzinessHandicapInventory.JournaloftheAmericanAcademyofAudiology1991;2:253‐60.
20. YardleyL,MassonE,VerschuurCetal.Symptoms,anxietyandhandicapindizzypatients:developmentofthevertigosymptomscale.Journalofpsychosomaticresearch1992;36:731‐41.
21. BergeniusJ,PerolsO.Vestibularneuritis:afollow‐upstudy.Actaoto‐laryngologica1999;119:895‐9.
22. GodemannF,SiefertK,Hantschke‐BruggemannMetal.Whataccountsforvertigooneyearafterneuritisvestibularis‐anxietyoradysfunctionalvestibularorgan?Journalofpsychiatricresearch2005;39:529‐34.
23. WalkerMF,TianJ,ShanXetal.Thecerebellarnodulus/uvulaintegratesotolithsignalsforthetranslationalvestibulo‐ocularreflex.PloSone2010;5:e13981.
24. IwasakiS,ChiharaY,SmuldersYEetal.Theroleofthesuperiorvestibularnerveingeneratingocularvestibular‐evokedmyogenicpotentialstoboneconductedvibrationatFz.Clinicalneurophysiology:officialjournaloftheInternationalFederationofClinicalNeurophysiology2009;120:588‐93.
25. MagliuloG,GagliardiS,CiniglioAppianiMetal.Vestibularneurolabyrinthitis:afollow‐upstudywithcervicalandocularvestibularevokedmyogenicpotentialsandthevideoheadimpulsetest.TheAnnalsofotology,rhinology,andlaryngology2014;123:162‐73.
26. LempertT,GiannaC,BrookesGetal.Horizontalotolith‐ocularresponsesinhumansafterunilateralvestibulardeafferentation.Experimentalbrainresearch.ExperimentelleHirnforschung.Experimentationcerebrale1998;118:533‐40.
27. StaabJP.Chronicsubjectivedizziness.Continuum2012;18:1118‐41.28. Jauregui‐RenaudK,SangFY,GrestyMAetal.Depersonalisation/derealisationsymptoms
andupdatingorientationinpatientswithvestibulardisease.Journalofneurology,neurosurgery,andpsychiatry2008;79:276‐83.
11
Figure1.vHITVORgainsfortheipsilesionalA).Horizontal,B).AnteriorandC).Posterior
canalsandvHITgainasymmetryfortheA).Horizontal,B).AnteriorandC).Posterior
canalsversusDHIscore.vHITassessmentdidnotcorrelatewithDHIscore.
12
Figure2.vHITVORgainsfortheipsilesionalA).Horizontal,B).AnteriorandC).Posterior
canalsandvHITgainasymmetryfortheA).Horizontal,B).AnteriorandC).Posterior
canalsversusVSSscore.vHITassessmentdidnotcorrelatewithVSSscore.
13
Figure3:vHITVORgainforthetotalresponseversusDHIscore(A)andVSSscore(B)&
vHITVORgainfortheverticalcanal(anterior+posteriorcanals)responseversusDHI
score(C)andVSSscore(D).
14
Tables
Table1.Vestibulartestingdataandsymptomscoresfromthepatientswhoparticipated
inthisstudy(n=20).