swiss recommendations 2016 - sgedssed.ch · swiss recommendations 2016 swiss society of...
TRANSCRIPT
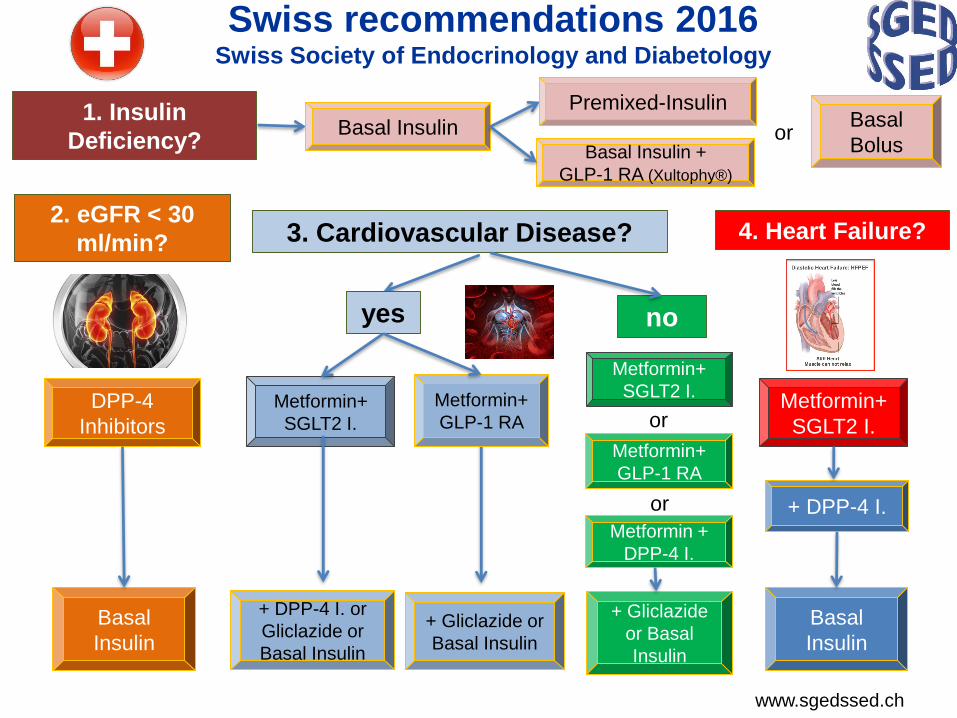
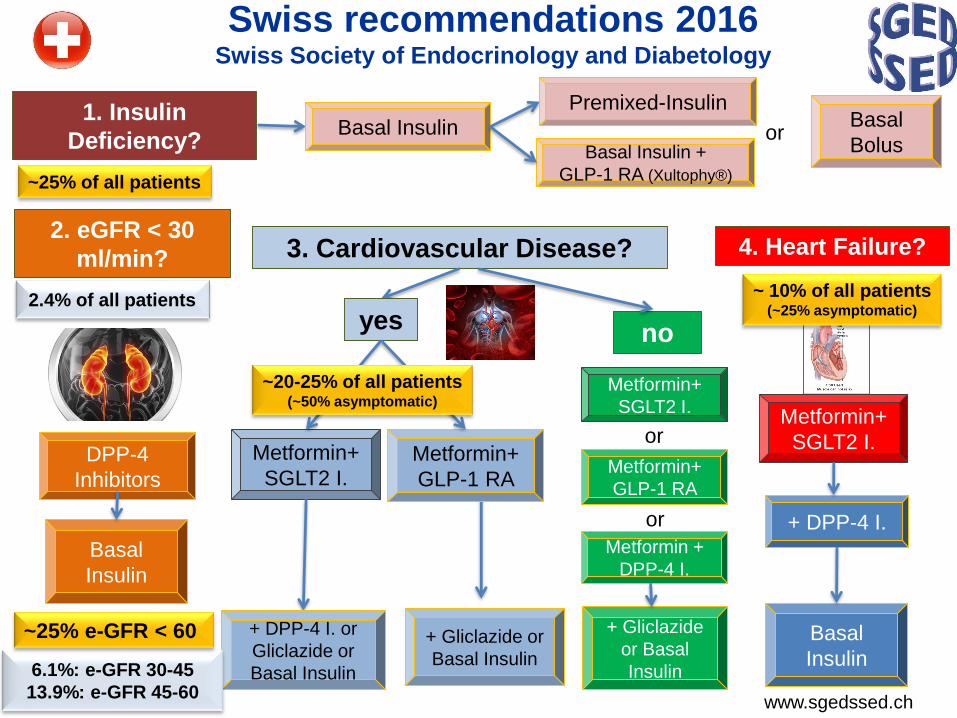
Swiss recommendations 2016Swiss Society of Endocrinology and Diabetology
2. eGFR < 30
ml/min?
DPP-4
Inhibitors
Basal
Insulin
3. Cardiovascular Disease?
yes no
Metformin+
SGLT2 I.
Metformin+
GLP-1 RA
Metformin +
DPP-4 I.
Metformin+
SGLT2 I. Metformin+
GLP-1 RA
+ DPP-4 I. or
Gliclazide or
Basal Insulin
+ Gliclazide or
Basal Insulin
+ Gliclazide
or Basal
Insulin
4. Heart Failure?
Metformin+
SGLT2 I.
+ DPP-4 I.
Basal
Insulin
www.sgedssed.ch
1. Insulin
Deficiency?Basal Insulin
Premixed-InsulinBasal
Bolusor
or
or
Basal Insulin +
GLP-1 RA (Xultophy®)
Guidelines for Type 2 Diabetes:
Keeping the Finger on the Pulse
Lancet Diabetes Endocrinol 2017
Anthony H Barnett, Paul O’Hare, Julian HalcoxPublished Online
April 19, 2017 http://dx.doi.org/10.1016/ S2213-8587(17)30136-5
........Several national guidelines, including those
from Canada and Switzerland, have also
responded quickly to these new data. However, to
our knowledge, NICE in the UK has not yet
responded to this evidence, even though results
from EMPA- REG OUTCOME were published 3
months before the most recent NICE guidance in 2015 (NG28).........
Overview of current T2D treatmentsWhich Priorities?
– Rarely used medications not used in treatment recommendations
(<5% market share = a-glucosidase inhibitors, Pioglitazone, Repaglinide)
– Priority according to treatment strategy
Class
Reduction
cardiovascular
complications
Relative HbA1c
Lowering
(Effectiveness)
Reduced
e-GFR
( <45/<30 mlmin)
Hypo-
glycemia
Risk
Body
WeightApplication Costs
Metformin (long-term) + /- oral $
SGLT-2
Inhibitors - + /- oral $$
GLP-1 R
Agonists () + /- Injection $$$
DPP-4
Inhibitors + /+ oral $$
Insulin
(basal) + /+ Injection
$ -
$$Sulfonyl-
urea -/- oral $
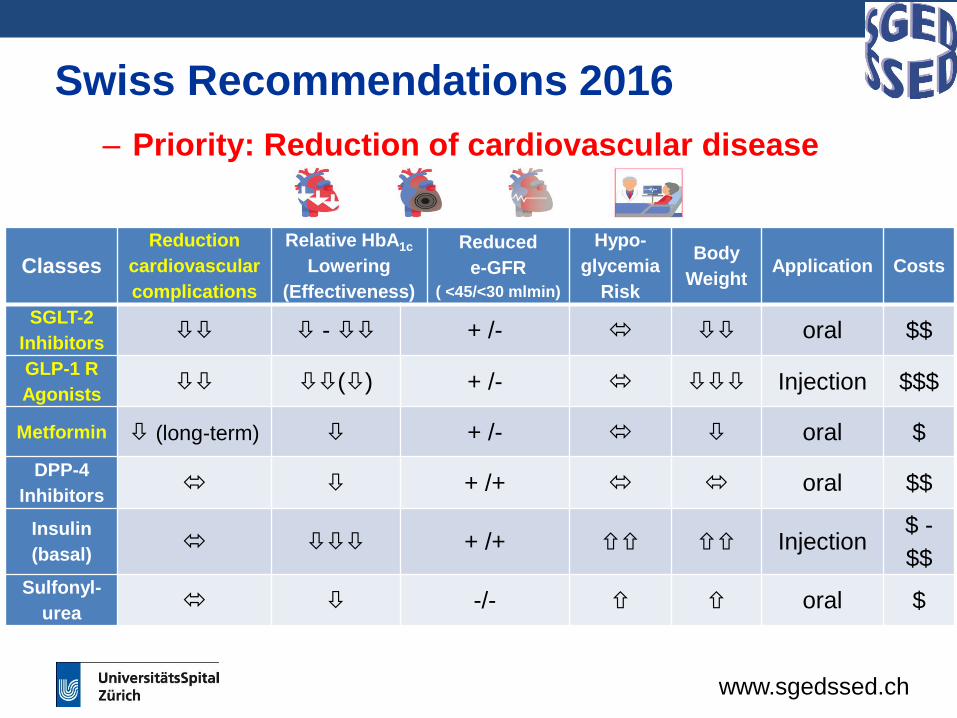
Swiss Recommendations 2016
– Priority: Reduction of cardiovascular disease
www.sgedssed.ch
Classes
Reduction
cardiovascular
complications
Relative HbA1c
Lowering
(Effectiveness)
Reduced
e-GFR
( <45/<30 mlmin)
Hypo-
glycemia
Risk
Body
WeightApplication Costs
SGLT-2
Inhibitors - + /- oral $$
GLP-1 R
Agonists () + /- Injection $$$
Metformin (long-term) + /- oral $
DPP-4
Inhibitors + /+ oral $$
Insulin
(basal) + /+ Injection
$ -
$$Sulfonyl-
urea -/- oral $
Swiss Recommendations 2016
www.sgedssed.ch
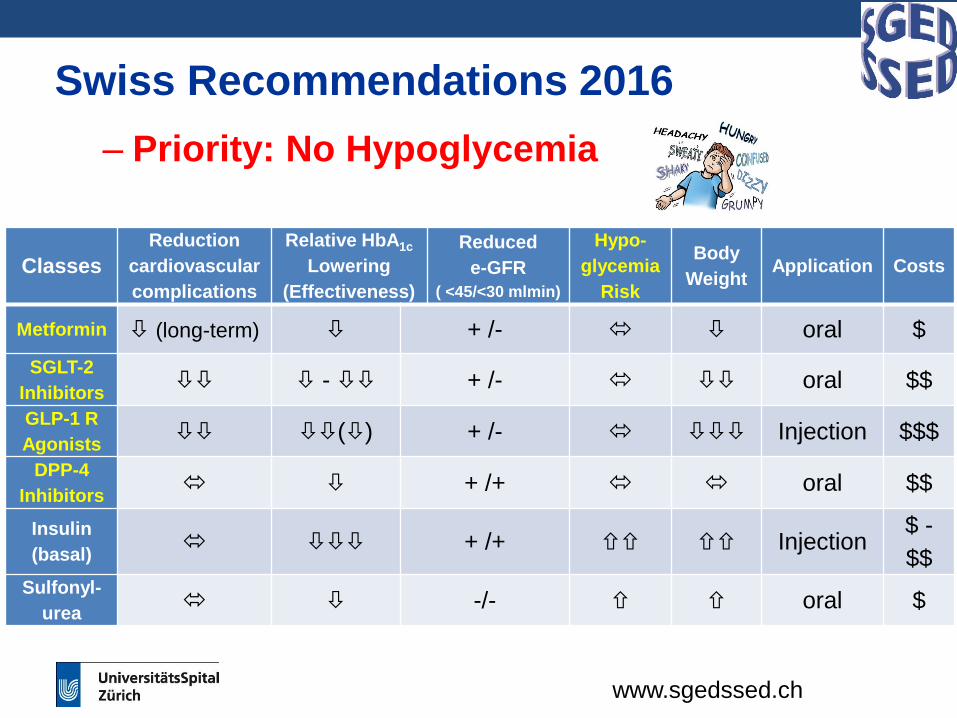
– Priority: No Hypoglycemia
Classes
Reduction
cardiovascular
complications
Relative HbA1c
Lowering
(Effectiveness)
Reduced
e-GFR
( <45/<30 mlmin)
Hypo-
glycemia
Risk
Body
WeightApplication Costs
Metformin (long-term) + /- oral $
SGLT-2
Inhibitors - + /- oral $$
GLP-1 R
Agonists () + /- Injection $$$
DPP-4
Inhibitors + /+ oral $$
Insulin
(basal) + /+ Injection
$ -
$$Sulfonyl-
urea -/- oral $
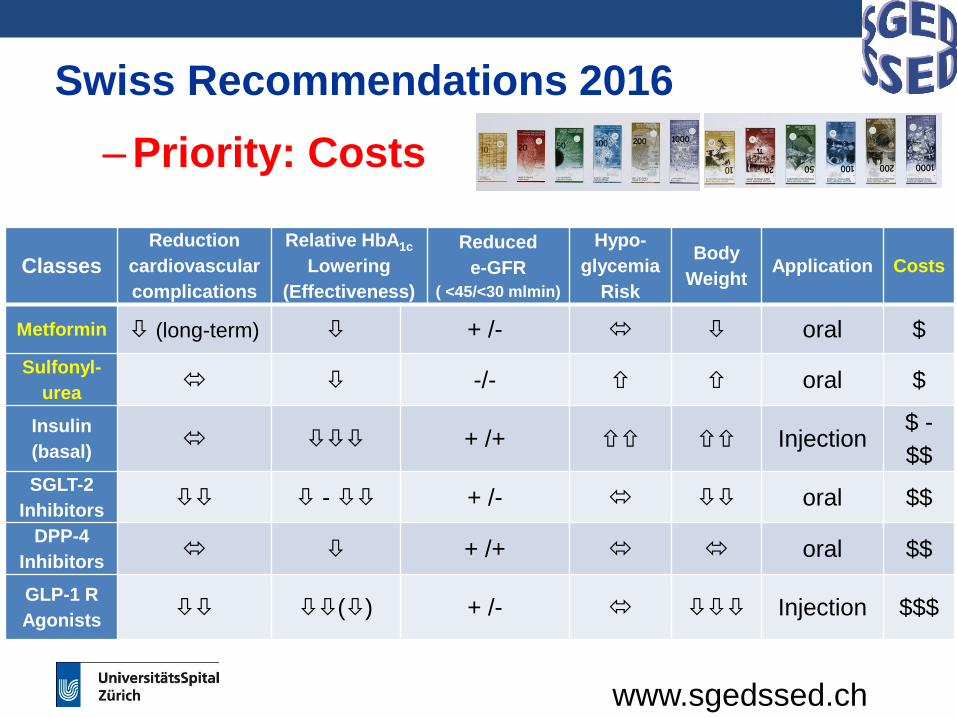
Swiss Recommendations 2016
– Priority: Costs
www.sgedssed.ch
Classes
Reduction
cardiovascular
complications
Relative HbA1c
Lowering
(Effectiveness)
Reduced
e-GFR
( <45/<30 mlmin)
Hypo-
glycemia
Risk
Body
WeightApplication Costs
Metformin (long-term) + /- oral $
Sulfonyl-
urea -/- oral $
Insulin
(basal) + /+ Injection
$ -
$$SGLT-2
Inhibitors - + /- oral $$
DPP-4
Inhibitors + /+ oral $$
GLP-1 R
Agonists () + /- Injection $$$
www.sgedssed.ch
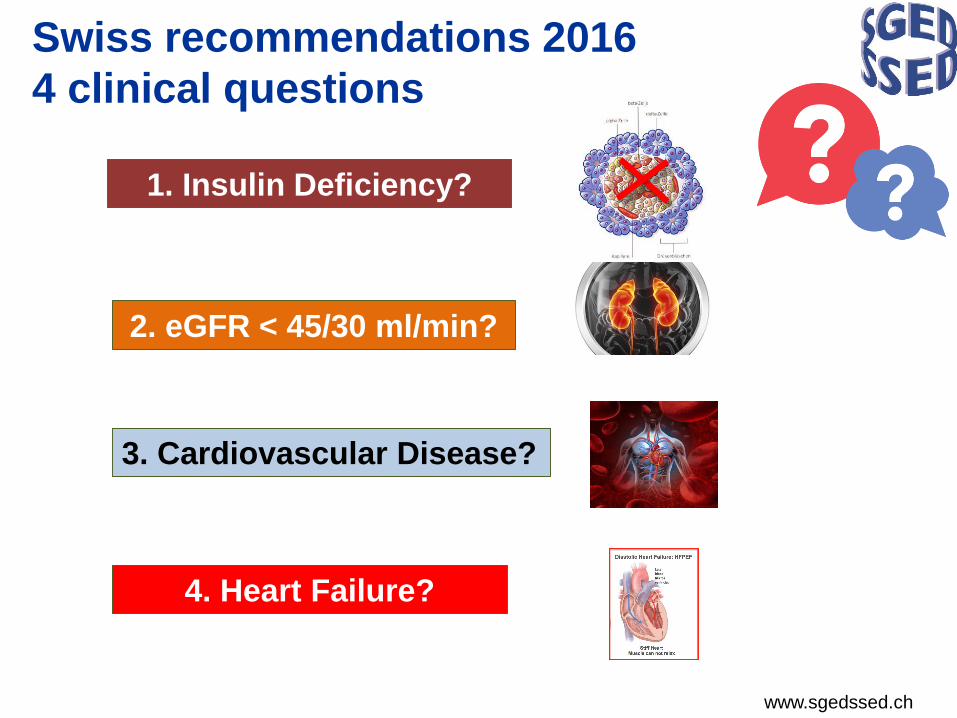
1. Insulin Deficiency?
2. eGFR < 45/30 ml/min?
3. Cardiovascular Disease?
4. Heart Failure?
Swiss recommendations 2016
4 clinical questions
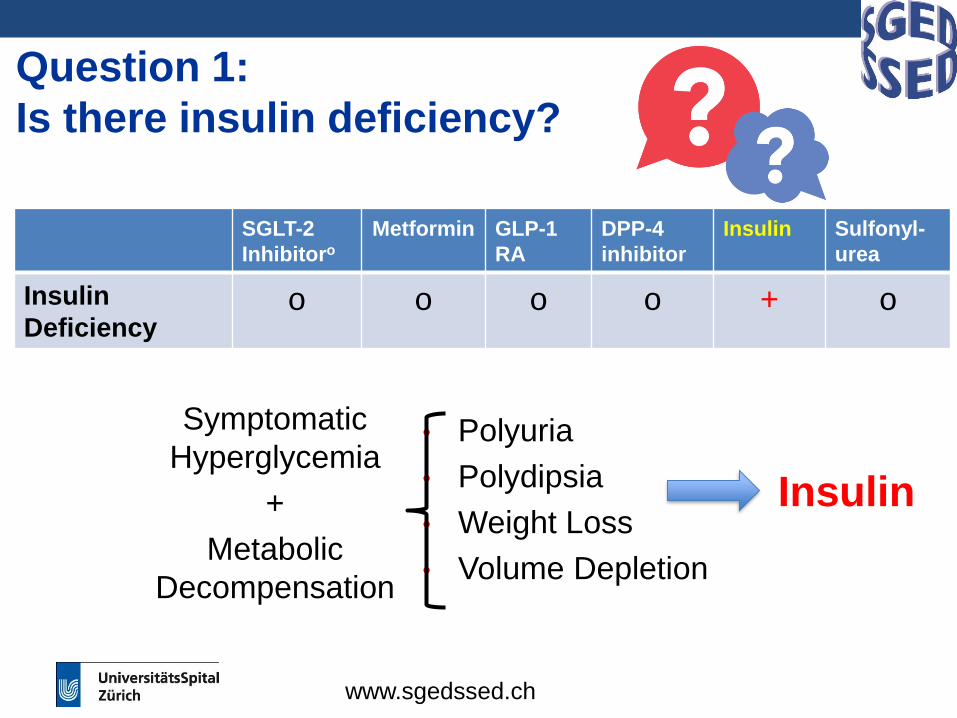
Question 1:
Is there insulin deficiency?
SGLT-2
Inhibitoro
Metformin GLP-1
RA
DPP-4
inhibitor
Insulin Sulfonyl-
urea
Insulin
Deficiencyo o o o + o
Symptomatic
Hyperglycemia
+
Metabolic
Decompensation
• Polyuria
• Polydipsia
• Weight Loss
• Volume Depletion
Insulin
1. SSED/SGED guidelines. 2016 update.
www.sgedssed.ch
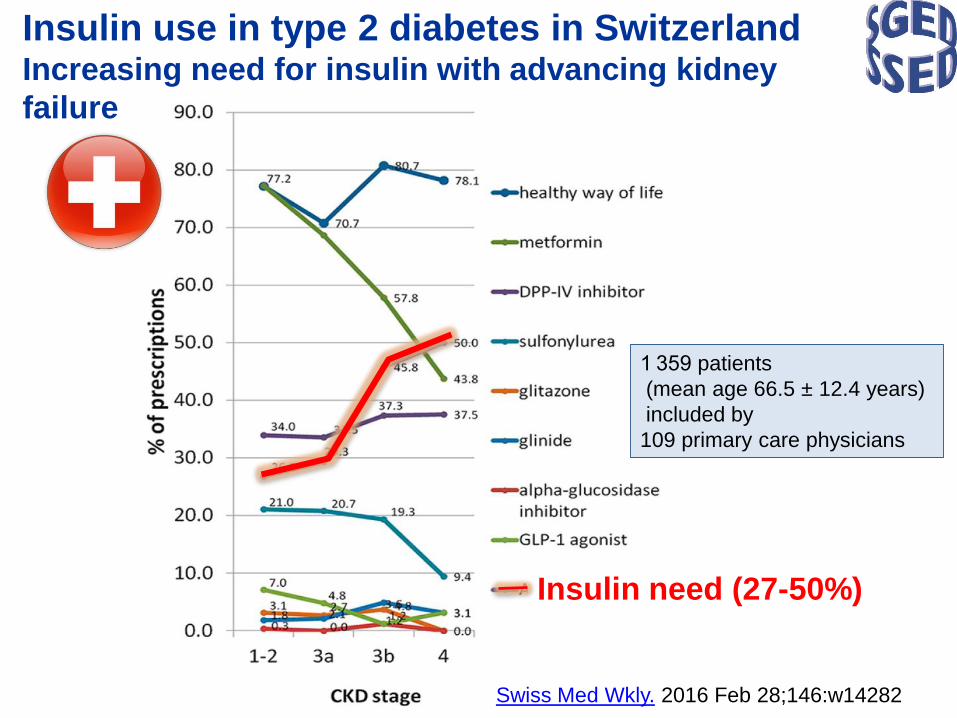
Insulin use in type 2 diabetes in SwitzerlandIncreasing need for insulin with advancing kidney
failure
Insulin need (27-50%)
1 359 patients
(mean age 66.5 ± 12.4 years)
included by
109 primary care physicians
Swiss Med Wkly. 2016 Feb 28;146:w14282
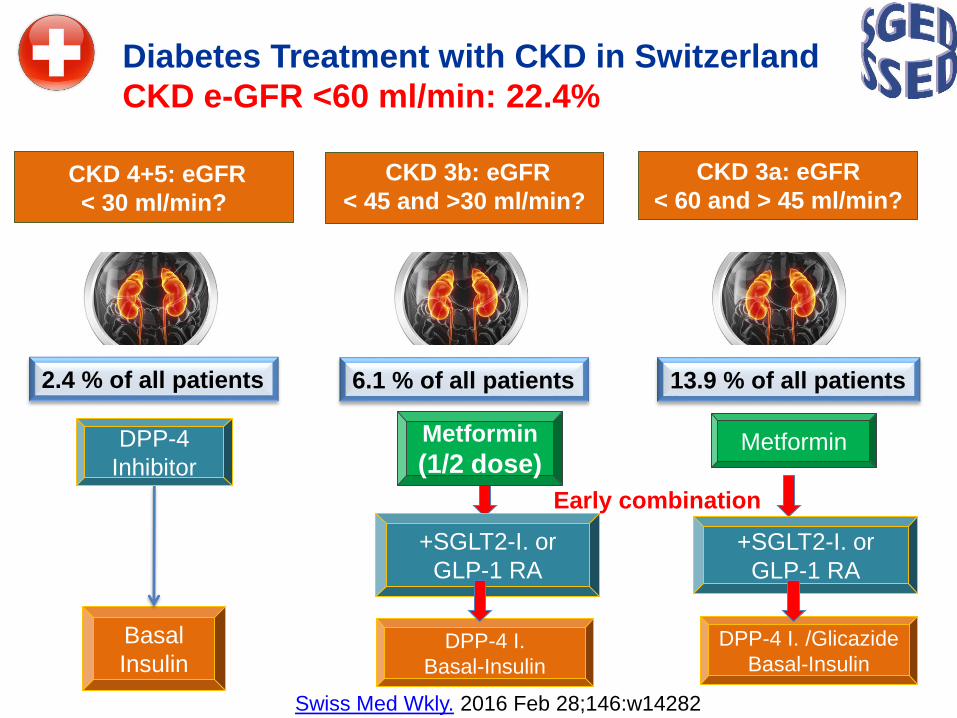
Diabetes Treatment with CKD in Switzerland
CKD e-GFR <60 ml/min: 22.4%
CKD 4+5: eGFR
< 30 ml/min?
2.4 % of all patients
Swiss Med Wkly. 2016 Feb 28;146:w14282
CKD 3b: eGFR
< 45 and >30 ml/min?
6.1 % of all patients
CKD 3a: eGFR
< 60 and > 45 ml/min?
13.9 % of all patients
DPP-4
Inhibitor
Basal
Insulin
Metformin
(1/2 dose)
+SGLT2-I. or
GLP-1 RA
DPP-4 I.
Basal-Insulin
Metformin
+SGLT2-I. or
GLP-1 RA
DPP-4 I. /Glicazide
Basal-Insulin
Early combination
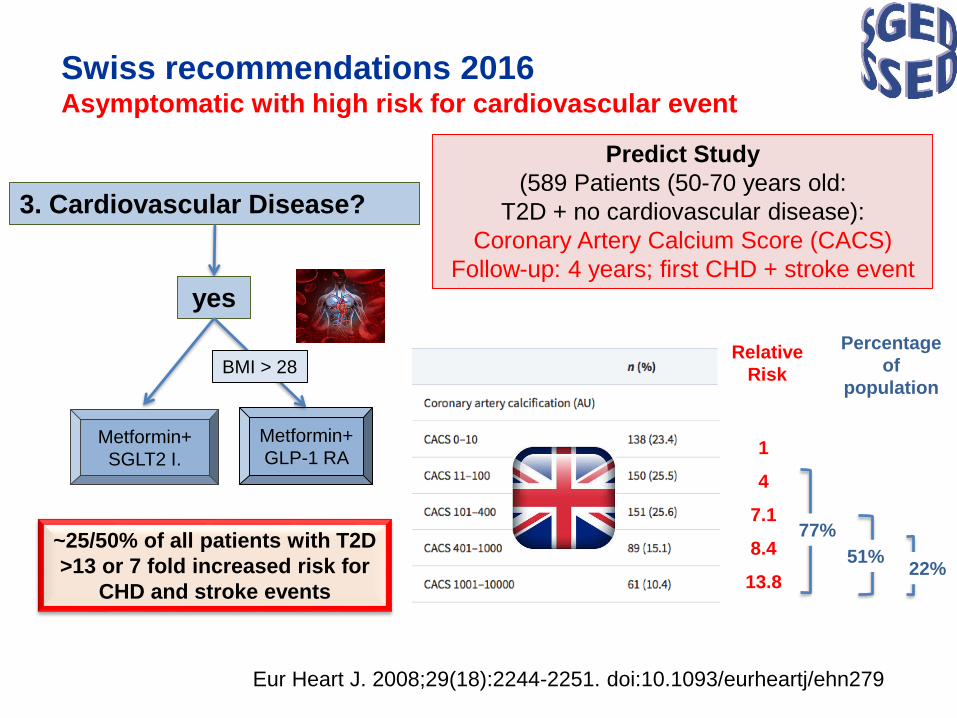
Swiss recommendations 2016Asymptomatic with high risk for cardiovascular event
3. Cardiovascular Disease?
yes
Metformin+
SGLT2 I.
Metformin+
GLP-1 RA
BMI > 28
~25/50% of all patients with T2D
>13 or 7 fold increased risk for
CHD and stroke events
Eur Heart J. 2008;29(18):2244-2251. doi:10.1093/eurheartj/ehn279
Predict Study
(589 Patients (50-70 years old:
T2D + no cardiovascular disease):
Coronary Artery Calcium Score (CACS)
Follow-up: 4 years; first CHD + stroke event
Relative
Risk
Percentage
of
population
1
4
7.1
8.4
13.8
51%
77%
22%
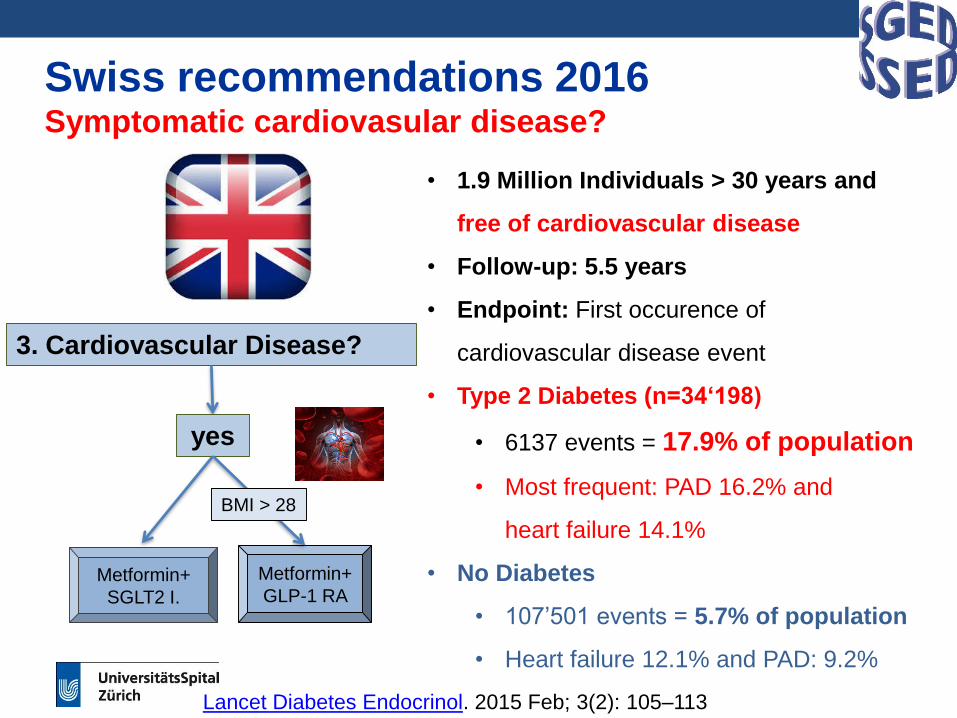
Swiss recommendations 2016Symptomatic cardiovasular disease?
3. Cardiovascular Disease?
yes
Metformin+
SGLT2 I.
Metformin+
GLP-1 RA
BMI > 28
• 1.9 Million Individuals > 30 years and
free of cardiovascular disease
• Follow-up: 5.5 years
• Endpoint: First occurence of
cardiovascular disease event
• Type 2 Diabetes (n=34‘198)
• 6137 events = 17.9% of population
• Most frequent: PAD 16.2% and
heart failure 14.1%
• No Diabetes
• 107’501 events = 5.7% of population
• Heart failure 12.1% and PAD: 9.2%
Lancet Diabetes Endocrinol. 2015 Feb; 3(2): 105–113
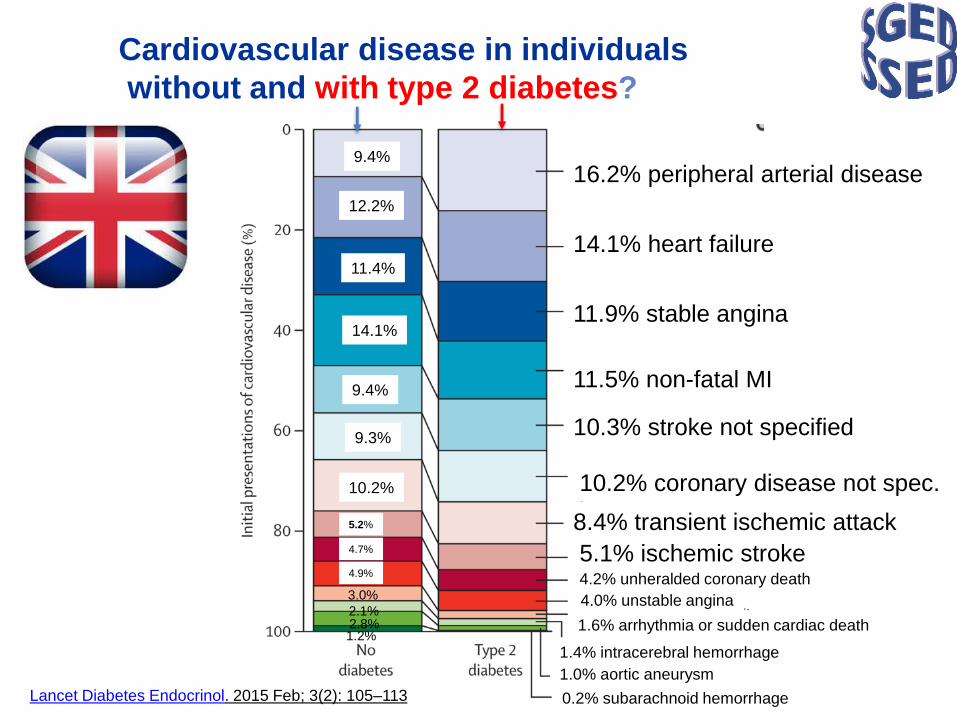
Cardiovascular disease in individuals
without and with type 2 diabetes?
Lancet Diabetes Endocrinol. 2015 Feb; 3(2): 105–113
16.2% peripheral arterial disease
14.1% heart failure
11.9% stable angina
11.5% non-fatal MI
10.3% stroke not specified
10.2% coronary disease not spec.
8.4% transient ischemic attack
5.1% ischemic stroke
1.0% aortic aneurysm
4.2% unheralded coronary death
4.0% unstable angina
1.6% arrhythmia or sudden cardiac death
1.4% intracerebral hemorrhage
1.0% aortic aneurysm
0.2% subarachnoid hemorrhage
9.4%
12.2%
9.3%
9.4%
14.1%
11.4%
4.9%
4.7%
5.2%
10.2%
3.0%
2.1%2.8%1.2%
Swiss recommendations 2016Symptomatic cardiovasular disease?
Rawshani A. et al, NEJM 2017, 376: 1407-18
• Swedish National Diabetes Register
• 457’473 individuals with type 2 diabetes
• Age: 65 years
• Coronary Heart Disease: 17.3%
• Acute Myocardial Infarction: 9.1
• Stroke: 6.6%
• Amputation: 0.4%
• Atrial fibrillation 7.6%
• Heart failure: 6.6%
24.3%
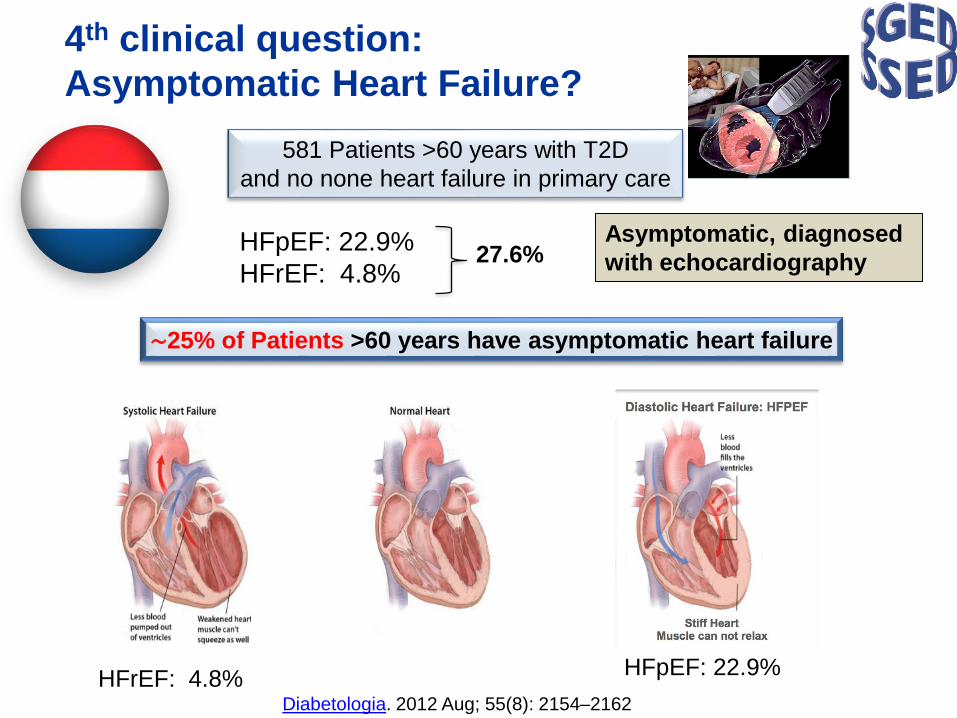
4th clinical question:
Asymptomatic Heart Failure?
1. SSED/SGED guidelines. 2016 update.
581 Patients >60 years with T2D
and no none heart failure in primary care
Diabetologia. 2012 Aug; 55(8): 2154–2162
HFpEF: 22.9%
HFrEF: 4.8%27.6%
Asymptomatic, diagnosed
with echocardiography
HFpEF: 22.9%HFrEF: 4.8%
∼25% of Patients >60 years have asymptomatic heart failure
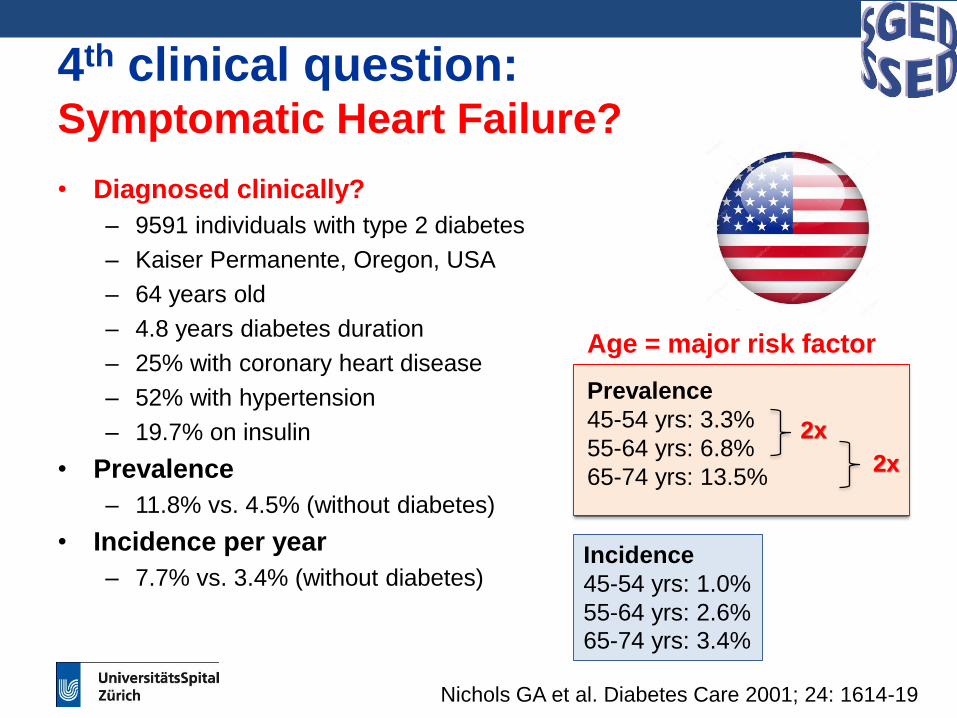
4th clinical question: Symptomatic Heart Failure?
• Diagnosed clinically?
– 9591 individuals with type 2 diabetes
– Kaiser Permanente, Oregon, USA
– 64 years old
– 4.8 years diabetes duration
– 25% with coronary heart disease
– 52% with hypertension
– 19.7% on insulin
• Prevalence
– 11.8% vs. 4.5% (without diabetes)
• Incidence per year
– 7.7% vs. 3.4% (without diabetes)
Age = major risk factor
Prevalence
45-54 yrs: 3.3%
55-64 yrs: 6.8%
65-74 yrs: 13.5%
2x
2x
Incidence
45-54 yrs: 1.0%
55-64 yrs: 2.6%
65-74 yrs: 3.4%
Nichols GA et al. Diabetes Care 2001; 24: 1614-19
1st step: individual HbA1c-Target
2nd step: best individual therapy for patients:
Setting which priorities?
3rd step: Think in drug classes: choose the
substance with the best evidence
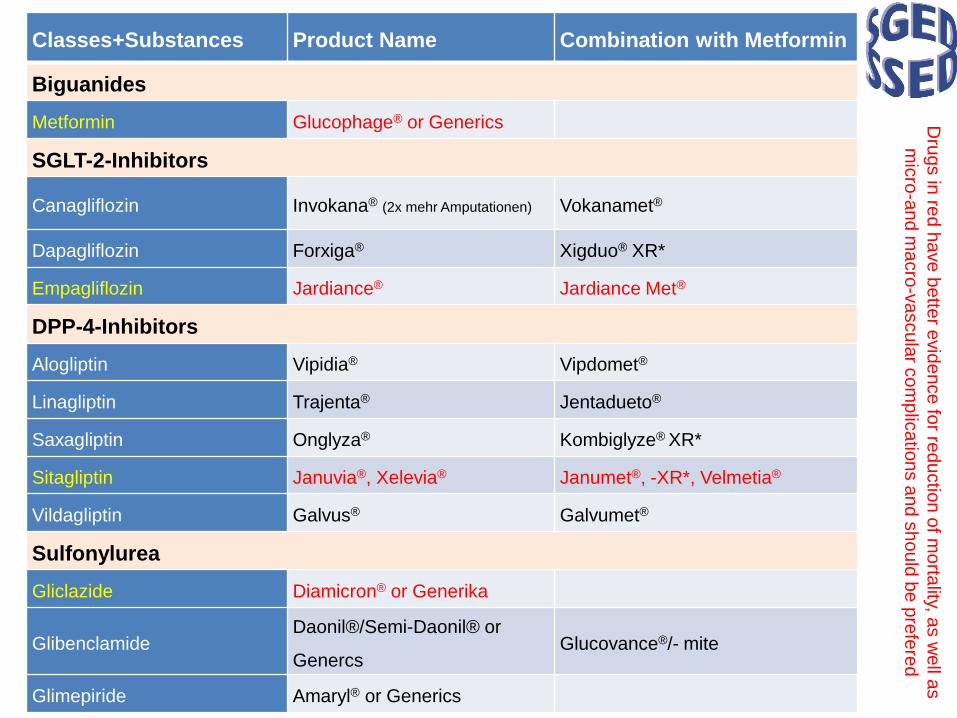
Classes+Substances Product Name Combination with Metformin
Biguanides
Metformin Glucophage® or Generics
SGLT-2-Inhibitors
Canagliflozin Invokana® (2x mehr Amputationen) Vokanamet®
Dapagliflozin Forxiga® Xigduo® XR*
Empagliflozin Jardiance® Jardiance Met®
DPP-4-Inhibitors
Alogliptin Vipidia® Vipdomet®
Linagliptin Trajenta® Jentadueto®
Saxagliptin Onglyza® Kombiglyze® XR*
Sitagliptin Januvia®, Xelevia® Janumet®, -XR*, Velmetia®
Vildagliptin Galvus® Galvumet®
Sulfonylurea
Gliclazide Diamicron® or Generika
GlibenclamideDaonil®/Semi-Daonil® or
GenercsGlucovance®/- mite
Glimepiride Amaryl® or Generics
Dru
gs in
red
ha
ve
be
tter
evid
en
ce
for
red
uctio
nofm
orta
lity, as
we
lla
s
mic
ro-a
nd
ma
cro
-va
scu
lar
co
mp
lica
tion
sand
sh
ou
ldbe
pre
fere
d
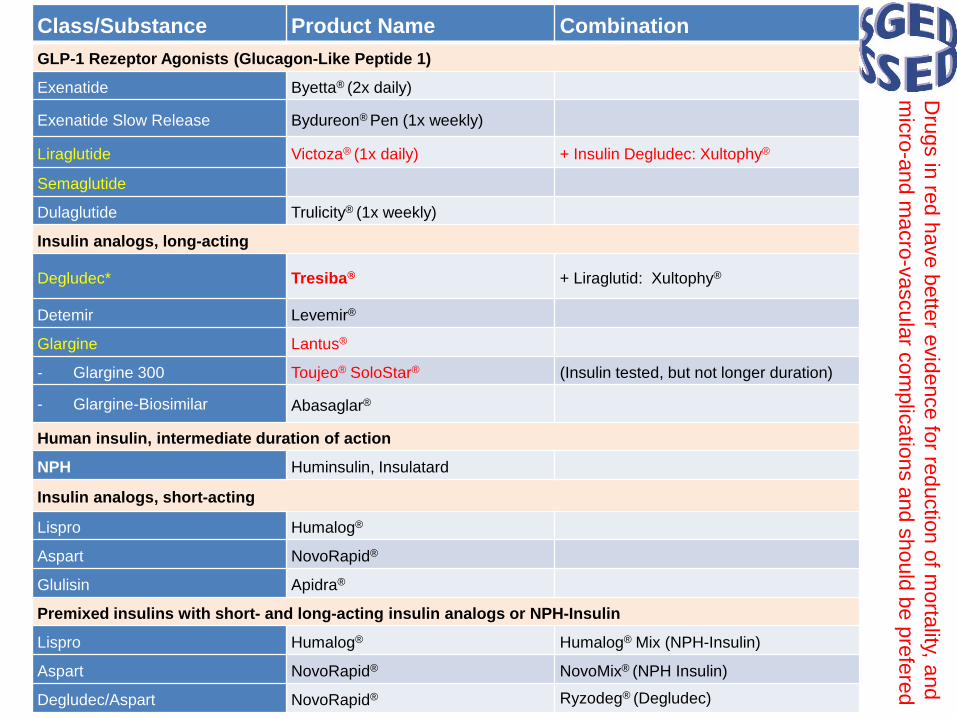
Class/Substance Product Name Combination
GLP-1 Rezeptor Agonists (Glucagon-Like Peptide 1)
Exenatide Byetta® (2x daily)
Exenatide Slow Release Bydureon® Pen (1x weekly)
Liraglutide Victoza® (1x daily) + Insulin Degludec: Xultophy®
Semaglutide
Dulaglutide Trulicity® (1x weekly)
Insulin analogs, long-acting
Degludec* Tresiba® + Liraglutid: Xultophy®
Detemir Levemir®
Glargine Lantus®
- Glargine 300 Toujeo® SoloStar® (Insulin tested, but not longer duration)
- Glargine-Biosimilar Abasaglar®
Human insulin, intermediate duration of action
NPH Huminsulin, Insulatard
Insulin analogs, short-acting
Lispro Humalog®
Aspart NovoRapid®
Glulisin Apidra®
Premixed insulins with short- and long-acting insulin analogs or NPH-Insulin
Lispro Humalog® Humalog® Mix (NPH-Insulin)
Aspart NovoRapid® NovoMix® (NPH Insulin)
Degludec/Aspart NovoRapid® Ryzodeg® (Degludec)
Dru
gs in
red
ha
ve
bette
re
vid
en
ce
for
red
uctio
nof
mo
rtality, a
nd
mic
ro-a
nd
macro
-vascula
rcom
plic
atio
ns
an
dshould
be
pre
fere
d
Swiss recommendations 2016Swiss Society of Endocrinology and Diabetology
2. eGFR < 30
ml/min?
DPP-4
Inhibitors
Basal
Insulin
3. Cardiovascular Disease?
yesno
Metformin+
SGLT2 I. Metformin+
GLP-1 RA
Metformin +
DPP-4 I.
Metformin+
SGLT2 I.
Metformin+
GLP-1 RA
+ DPP-4 I. or
Gliclazide or
Basal Insulin
+ Gliclazide or
Basal Insulin
+ Gliclazide
or Basal
Insulin
4. Heart Failure?
Metformin+
SGLT2 I.
+ DPP-4 I.
Basal
Insulin
1. Insulin
Deficiency?Basal Insulin
Premixed-InsulinBasal
Bolusor
or
or
Basal Insulin +
GLP-1 RA (Xultophy®)
~20-25% of all patients(~50% asymptomatic)
~ 10% of all patients(~25% asymptomatic)
2.4% of all patients
~25% of all patients
6.1%: e-GFR 30-45
13.9%: e-GFR 45-60
~25% e-GFR < 60
www.sgedssed.ch