sustained hyperhydration with glycerol ingestion
DESCRIPTION
32 to 49 hour studies of hyperhydration in subjects.TRANSCRIPT

Koenigsberg, Peter S., KitrianMarvin L. Riedesel. 1995.
K. Martin, Holly R. Hlava,Sus tained hyperhydration
57 (7): 64s-6s3
andwith glycerol
ingestion. i.ifq Sciences
0024-3205(9t0031.6-9
SUSTAII\ED HYPERHYDRATION WITII GLYCEROL INGESTION
Peter S. Koenigsberg, Kitrian K. Martin, Holly R. Hlava,and Marvin L. Riedesel
Department of BiologyThe University of New Mexico
Albuquerque, New Mexico 87131-1091 USA
(Received in final form May 17, 195)
Strmmr*
Heavy exercise lasting more than three hours tends to result in dehydration, as thefluid intake is less than fluid loss by sweat and urine. Dehydration as small as onepercent ofbody weight has been reported to decrease work capacity. In present andprevious studies insensible water loss and sweat are assummed to be the same in bothcontrol and experimental conditions. Fluid intake less urine volume is utilized as anindicator ofeuhydration, hypohydration, or hyperhydration. Previous studies involv-ing glycerol intake describe hyperhydration for 4.5 to 8 hours. The objective of thisstudy was to keep subjects hyperhydrated (retention of water) for 32 or 49 hours. Theexperimental protocol involved ingestion of a large volume of fluid (39.2 or 51.1mVkg/d) with glycerol Q.9 tD 3.I g/kg/d) and without glycerol. In both Series I (49h) and Series II (32 h) experiments, the intake ofglycerol resulted in smaller urinevolumes. This study demonshates it is possible to keep human subjects hyperhydratedfor extended periods of time and thereby reduce the amount of fluid consumptionnecessary just prior to or during bouts of negative fluid balance situations.
Key Words: water retention, hyperhydration, glycerol-induced hyperhydration, glycerol
Preventing dehydration of athletes, astronauts, and other active people represents a complexproblem. The renal, endocrine, gasfio-intestinal, central nervous and cardiovascular systems interactin maintaining a physiological state of euhydration. This interaction of systems provides a challengeto applied physiologists trying to prevent negative water balance during conditions and activitieswhich result in dehydration. Prior to competition and intense training, athletes tend to avoid drinkingfor fear of gasEo-intestinal discomfort or inconvenience of voiding urine. As a result, dehydration,decreased sweat rate, increased core temperature, and reduced athletic performance may occur (10,7). One approach to preventing hypohydration is to hyperhydrate prior to heavy exercise.Hyperhydration has been demonstrated to provide an advantage for subjects exercising in the heat(6). Ingestion of glycerol (1 g/kg) can induce a state of hyperhydration (4, 5, 9), which increased
Author Responsible for Correspondence:sity of New Mexico, Albuquerque, New03M; E-mail: [email protected].
Marvin L. Riedesel,Mexico 87131-1091
Department of Biology, The Univer-USA; 505/277 -2824; Fax: 505 1277 -
ffi Fluid Intake, Glycerol and Urine Volume Vol.57, No.7, 1995
sweating and decreased the extent of dehydration, in addition to reducing the elevation of heart rate
and body temperature of subjects exercising in a hot environment. These studies involved maintain-
ing glycerol induced hyperhydration (GIH) for 2.5 to 4.5 h.
Multiple variables are involved in extending GIH. Glycerol rapidly moves from one fluid compart-
ment to another as evidenced by serum glycerol values reaching a peak within 15 to 90 min after
a single oral ingestion (8, 12). The catabolism and renal excretion of glycerol varies with serum
concentration (i, tf). The rate of glycerol uptake and retention differs among tissues (4). The
effects of glycerol on volume and osmotic receptors have not been described. These variables make
the timing and amount of glycerol intake needed to obtain fluid retention difficult to predict.
One advantage of using the osmotic action of glycerol to expand total body water is the glycerol
,p"." r.pt"r"its 65% oi totut body mass. Widespread application of GIH is going to require many
differeni research approaches. The present study is an att€mpt to describe timing and volume intakes
of various fluids which can be effective in extending the hyperhydraiton beyond the 4.5 hours
described in previous research (4, 9). Prior studies have involved retention of 500 to 900 ml of
water and the aim of this study was to have fluid intake exceed urine output by similar amounts for
longer periods of time.
Methcxls and Materials
The male subjects were students who were limited to sedentary activities such as attending classes
during all experiements. This limitation accounts for the 32- and 49-hour duration of experiments.
Subjects had no health problems and had signed consent forms approved by the University of New
Mexico Human Research Review Committee. A two-day pilot study was conducted prior to all
Series I and Series II experiments. This pilot study had two purposes (i) to ensure subjects were
euhydrated prior to control and experimental protocols, and (ii) to familiarize subjects with the
.outine of ingesting specific volumes of fluids at specific times and recording the time and volume
of urine voidi. Ouring ttre pilot studies subjects ingested a minimum of 2500 m1/70 kg body weight
per day. Subjects had meals at a student cafeteria and od libitum fluid intake at all times, but were
required to record all fluid intake. Statistical analyses were paired t test, linear regression or analysis
ofvariance for repeated measures.
Series I
Seven subjects, 75.8 * 8.7 kg, 20 to 26 years, participated in a 49-h control (water and orange
juice) period and a 49-h experimental (water and orange juice with glycerol added) period @able
t;. nui"r and volumes of AuiO ingestion were based on semm glycerol and urine data collected in
previous 4.5 h studies (4). Subjects reported to the laboratory at 0700, 1200, 1600 and 2000 h each
bay for meals, blood draws, and collection of urine voided. The blood draws were conducted after
thi subjects had been seated for 15 min. Three subjects completed the control period first and four
subjecis completed the experimental period first. There was a one-week interval between the
experimental and control protocols.
Blood was analyzed for hematocrit (Hct), hemoglobin (Hgb), plasma osmolality, serum glycerol and
serum creatinine. Urinesamples were pooled at 2000 h and 0800 h (urine voided between 0700 and
2000 h of Day 1 represented one pooled sample, and urine voided between 2000 h of Day 2 and
0700 h of Day 3 represented "noih"t
pooled sample, etc.) for determination of volume, specifrc
Vol.57, No. 7, 1995 Fluid Intake, Glycerol and Urine Volume &7
gravity' glycerol and creatinine. Serum samples for glycerol and osmolality analyses were frozenat -72"c within 15 min of the blood draw, and all analyses were made on the same day.
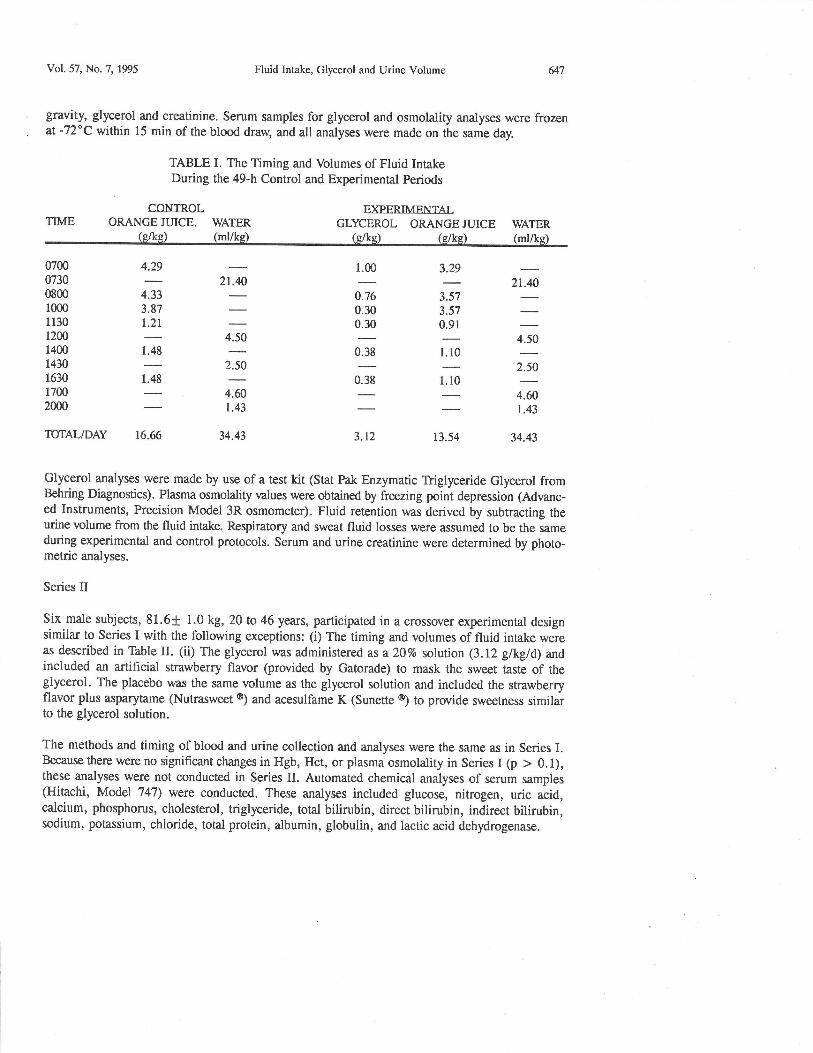
TABLE I. The Timing and Volumes of Fluid IntakeDuring the 49-h Control and Experimental Periods
CONTROI.TIME ORANGEJUICE. WATER
-
(g/ke) (ml/ke)
FXPFRTMENTAIGLYCEROL ORANGEJUICE WATER
(e/ks) (e/ks) (ml/ke)
0700073008001000113012001400
1430
1630
17002000
4.29
4.333.87l.2t
1.48
'j
,t:
*t2.50
a-1.43
34.43
t*0.38
3.12
1.10
1. l0
t3.54
21.40
*t2.50
^^1.43
34.43
1.00 3.29
0.76 3.570.30 3.570.30 0.91
TOTAL/DAY 16.6
Glycerol analyses were made by use of a test kit (Stat Pak Enzymatic Triglyceride Glycerol fromBehring Diagnostics). Plasma osmolality values were obained by freezing point depression (Advanc-ed Instruments, Precision Model 3R osmometer). Fluid retention was derived by subtracting theurine volume from the fluid intake. Respiratory and sweat fluid losses were assumed to be the sameduring experimental and control protocols. Serum and urine creatinine were determined by photo-metric analyses.
Series II
Six male subjects, 81.6+ 1.0 kg, 20 to 46 years, participated in a crossover experimental designsimilar to Series I with the following exceptions: (i) The timing and volumes of fluid intake wereas described in Tbble II. (ii) The glycerol was administered as a 20% solution (3.12 g/kg/d) ndincluded an artificial strawberry flavor (provided by Gatorade) to mask the sweet taste of theglycerol. The placebo was the same volume as the glycerol solution and included the strawberryflavor plus asparytame (Nutrasweet o) and acesulfame K (Sunette @) to provide sweetness similarto the glycerol solution.
The methods and timing of blood and urine collection and analyses were the same as in Series I.Because there were no significant changes in Hgb, Hct, or plasma osmolality in Series I (p > 0. 1),these analyses were not conducted in Series II. Automated chemical analyses of serum samples(Hitachi, Model 747) were conducted. These analyses included glucose, nitrogen, uric acid,calcium, phosphorus, cholesterol, triglyceride, total bilirubin, direct bilirubin, indirect bilirubin,sodium, potassium, chloride, total protein, albumin, globulin, and lactic acid dehydrogenase.
6rA
Day 2:
0730080008301030
1100
1130
1400
14301630
1700
20002030
TUIAL
0730080008301030
I 1001130
TOTAL
5.0
0.51.51.5
2.0
;
2.0
14.5
,y
*
2.5
*
4.6
37.6
21.4
*
25.9
Fluid Intake, Glycerol and Urine Volume
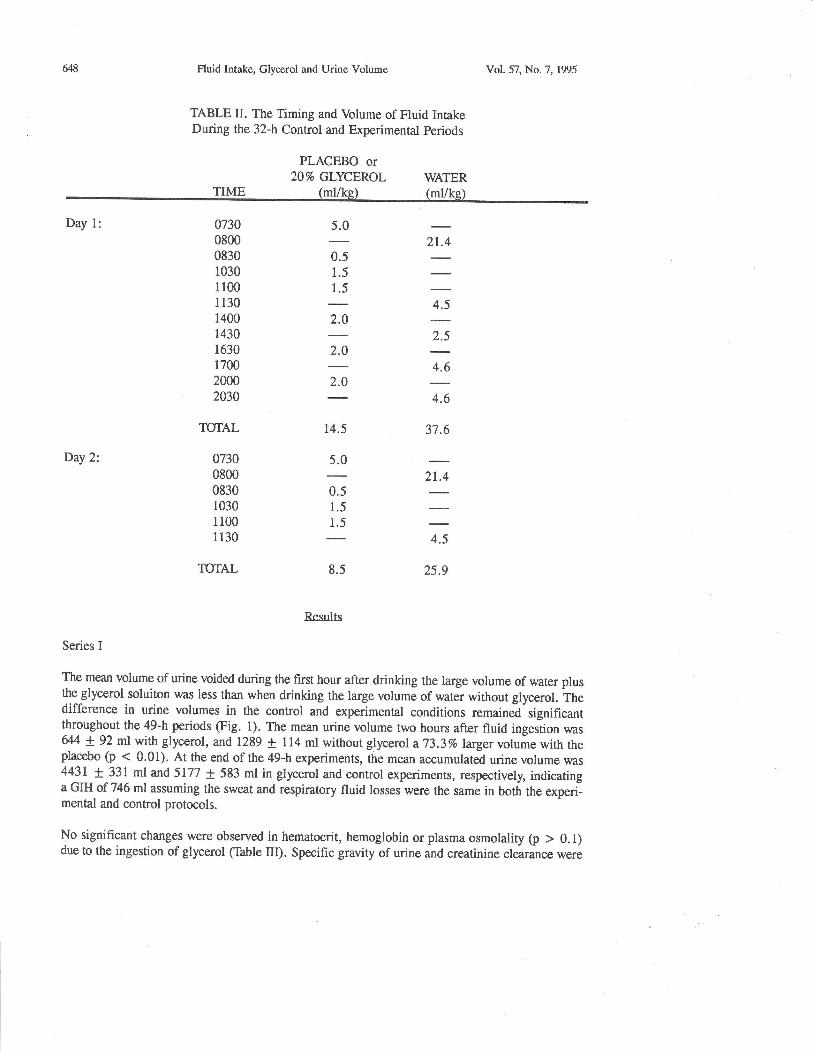
TABLE II. The Timing and Volume of Fluid IntakeDuring the 32-h Control and Experimental periods
PLACEBO or20% GLYCEROL
Vol.57, No.7, 1995
WATER(ml/ke)
5.0
0.51.51.5
8.5
Resrrlts
Series I
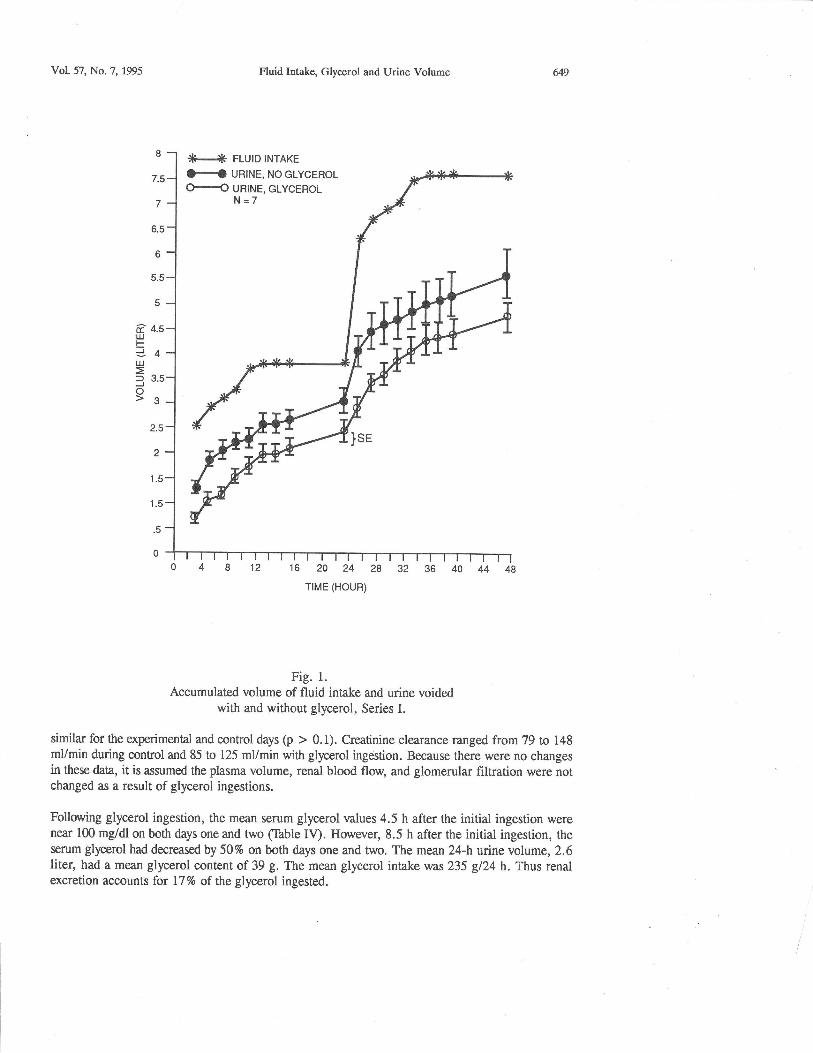
The mean volume of urine voided during the first hour after drinking the large volume of water plusthe glycerol soluiton was less than when drinking the large volume of water without glycerol. hhedifference in urine volumes in the control and experimental conditions remaini'significantthroughout the 49-h periods (Fig. 1). The mean urine volume two hours after fluid inges=tion was&4 ! gZ ml with glycerol, and 1289 t 1 14 ml without glycerol a 73.3% larger voluire with theplacebo (p < 0'01). At the end of the 49-h experiments, the mean accumulated urine volume was4431 + 331 ml and 5177 + 583 ml in glycerol and control experiments, respectively, indicatinga GIH of 746 ml assuming the sweat and respiratory fluid losses were the same in both the experi-mental and control protocols.
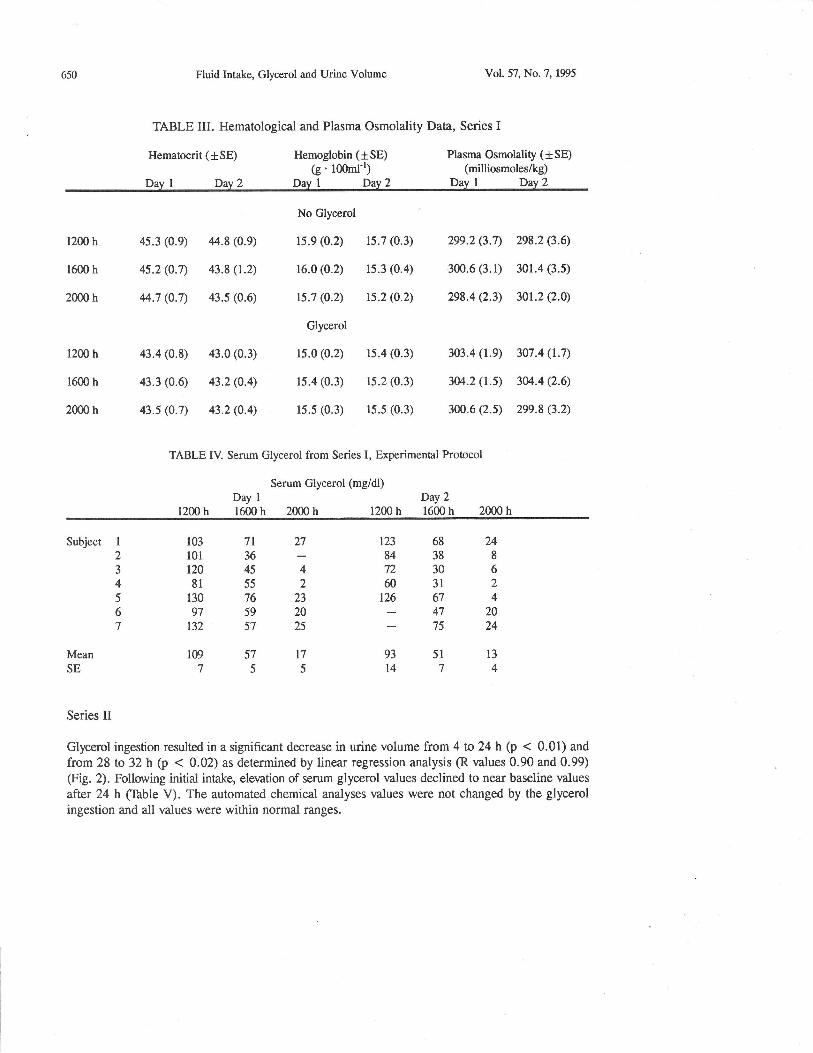
No significant changes were observed in hematocrit, hemoglobin or plasma osmolality (p > 0. 1)due to the ingestion of glycerol (Table III). Specific gravity of urine and creatinine clearance were
Vol.57, No.7, 195 Fluid Intake, Glycerol and Urine Volume &9
Fig. 1.
Accumulated volume of fluid intake and urine voidedwith and without glycerol, Series I.
similar for ttre experimental and control days (p > 0.1). Creatinine clearance ranged from 79 to 148mVmin during connol and 85 to 125 mVmin with glycerol ingestion. Because there were no changesin these data, it is assumed the plasma volume, renal blood floq and glomerular filtration were notchanged as a result of glycerol ingestions.
Following glycerol ingestion, the mean serum glycerol values 4.5 h after the initial ingestion werenear 100 mg/dl on both days one and two (Ihble IV). However, 8.5 h after the initial ingestion, theserum glycerol had decreased by 507o on both days one and two. The mean 24-h urine volume, 2.6liter, had a mean glycerol content of 39 g. The mean glycerol intake was 235 gl24 h. Thus renalexcretion accounts for 17% of the glycerol ingested.
H URINE, NOGLYCEROLH URINE. GLYCEROL
650 Ftuid Intake, Glycerol and Urine Volume
TABLE III. Hematological and Plasma Osmolality Data, Series I
Hematocrit (tSE) Ilemoglobin (tSE)(g' 100m1-1)
Dav 1 Dav 2 Dav I Dav 2
Vol. 57, No.7, 195
Plasma Osmolality (t SE)(milliosmoles/kg)
Dav I Day 2
1200 h
1600 h
2000 h
1200 h
1600 h
2m0 h
45.3 (0.e)
4s.2 (0.7)
44.7 (0.7)
43.4 (0.8)
43.3 (0.6)
43.5 (0.7)
No Glycerol
15.9 (0.2)
16.0 (0.2)
r5.7 (0.2)
Glycerol
ls.0 (0.2)
15.4 (0.3)
15.5 (0.3)
15.7 (0.3)
rs.3 (0.4)
ts.2 (0.2)
15.4 (0.3)
15.2 (0.3)
15.5 (0.3)
299.2 (3.7)
300.6 (3.1)
298.4 Q.3)
303.4 (1.9)
3M.2 (t.s)
3m.6 (2.s)
298.2 (3.6)
301.4 (3.5)
301.2 Q.0)
307.4 (1.7)
30/..4 (2.6)
2e9.8 (3.2)
,14.8 (0.9)
43.8 (1.2)
43.5 (0.6)
43.0 (0.3)
43.2 (O.4)
43.2 (0.4)
Day 1
1200 h 1600 h 2000 hDay 2
1200 h 1600 h 2000 h
TABLE IV. Serum Glycerol from Series I, Experimental Protocol
Serum Glycerol (mg/dl)
Subject 1
23
4
567
MeanSE
r23 68 24843887230660312126 67 4
47 2075 24
93 51 13
1474
103 7r 27101 36t20 45 481552130 76 2397 59 20132 57 25
109 57 l7755
Series II
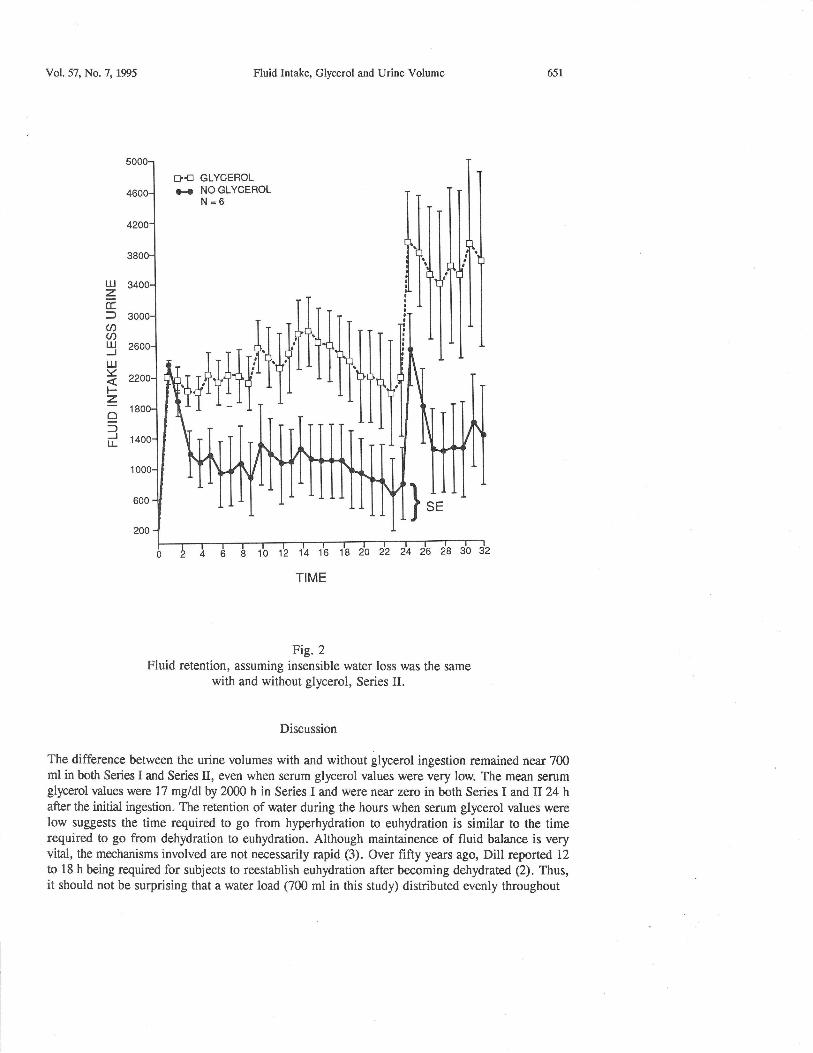
Glycerol ingestion resulted in a significant decrease in urine volume from 4 to 24 h (p < 0.01) and
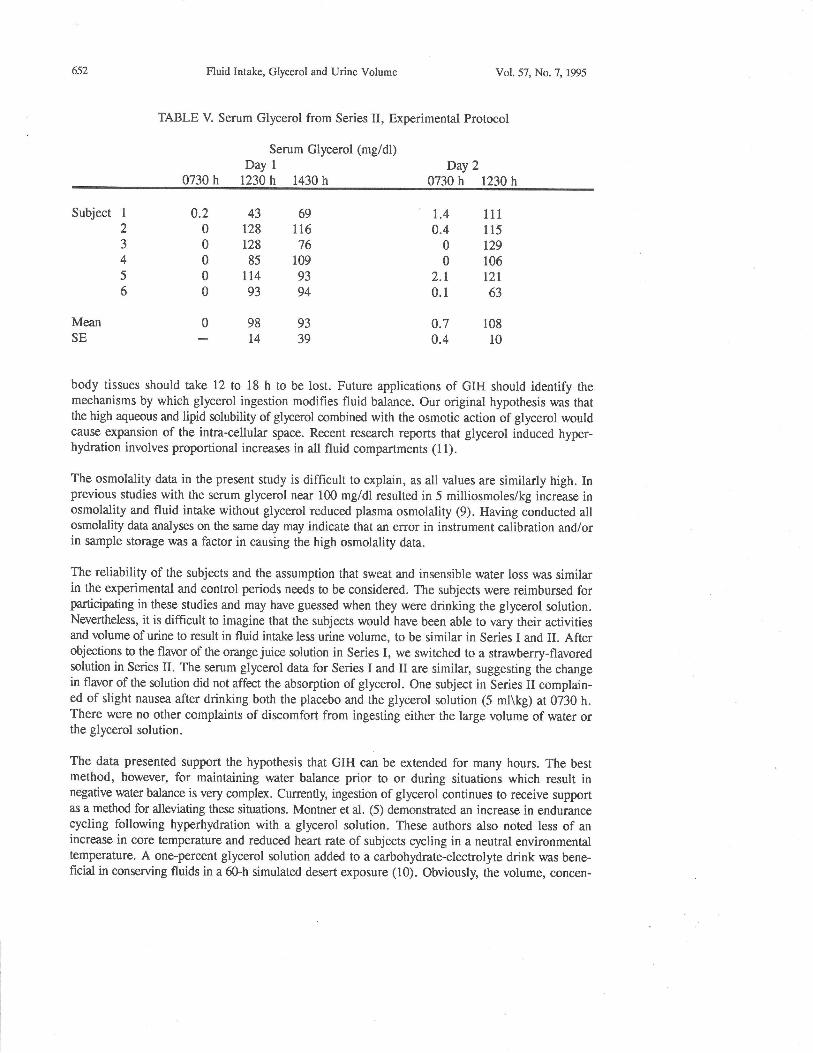
from 28 to 32 h (p < 0.02) as determined by linear regression analysis (R values 0.90 and 0.99)(Fig. 2). Folluving initial intake, elevation of serum glycerol values declined to near baseline values
after 24 h (Ihble V). The automated chemical analyses values were not changed by the glycerolingestion and all values were within normal ranges.
Vol.57, No.7, 1995 Fluid Intake, Glycerol and Urine Volume
GLYCEROLNO GLYCEROLN=6
Fig.2Fluid retention, assuming insensible water loss was the same
with and without glycerol, Series II.
Discussion
The difference between the urine volumes with and without glycerol ingestion remained near 700ml in both Series I and Series II, even when serum glycerol values were very low. The mean serumglycerol values were 17 mgldlby 2000 h in Series I and were near zero in both Series I and II 24 hafter the initial ingestion. The retention of water during the hours when serum glycerol values werelow suggests the time required to go from hyperhydration to euhydration is similar to the timerequired to go from dehydration to euhydration. Although maintainence of fluid balance is veryvital, the mechanisms involved are not necessarily rapid (3). Over fifty years ago, Dill reported 12
to 18 h being required for subjects to reestablish euhydration after becoming dehydrated (2). Thus,it should not be surprising that a water load (700 ml in this study) distributed evenly throughout
651
Dfla{
1
1
L!zccf@U)IUJuJYFzo:)JtL
652 Fluid Intale, Glycerol and Urine Volume
TABLE V. Serum Glycerol from Series II, Experimental Protocol
Vol.57, No.7, 195
0730 h
Serum Glycerol (mg/dl)Day 1
1230 h 1430 hDay 2
0730 h t230 h
Subject
MeanSE
108
10
43 69128 116r28 7685 109
lr4 9393 94
98 93t4 39
0.200000
0
1
2345
6
r.40.4
00
2.r0.1
0.70.4
111
115
t29106
t2r63
body tissues should t*e 12 to 18 h to be lost. Future applications of GIH should identify themechanisms by which glycerol ingestion modihes fluid balance. Our original hypothesis was thatthe high aqueous and lipid solubility of glycerol combined with the osmotic action of glycerol wouldcause expansion of the intra-cellular space. Recent research reports that glycerol induced hyper-hydration involves proportional increases in all fluid compartments (11).
The osmolality data in the present study is difficult to explain, as all values are similarly high. Inprevious studies with the serum glycerol near 100 mg/dl resulted in 5 milliosmoles/kg increase inosmolality and fluid intake without glycerol reduced plasma osmolality (9). Having conducted allosmolality data analyses on the same day may indicate that an error in instrument calibration and/orin sample storage was a factor in causing the high osmolality data.
The reliability of the subjects and the assumption that sweat and insensible water loss was similarin the experimental and control periods needs to be considered. The subjects were reimbursed forparticipating in these studies and may have guessed when they were drinking the glycerol solution.Nevertheless, it is difhcult to imagine that the subjects would have been able to vary their activitiesand volume of urine to result in fluid intake less urine volume, to be similar in Series I and II. Afterobjections to the flavor of the orange juice solution in Series I, we switched to a strawberry-flavoredsolution in Series II. The serum glycerol data for Series I and II are similar, suggesting the changein flavor of the solution did not affect the absorption of glycerol. One subject in Series II complain-ed of slight nausea after drinking both the placebo and the glycerol solution (5 ml\kg) at 0730 h.There were no other complaints of discomfort from ingesting either the large volume of water orthe glycerol solution.
The data presented support the hypothesis that GIH can be extended for many hours. The bestmethod, however, for maintaining water balance prior to or during situations which result innegative water balance is very complex. Cunently, ingestion of glycerol continues to receive supportas a method for alleviating these situations. Montner et al. (5) demonstrated an increase in endurancecycling following hyperhydration with a glycerol solution. These authors also noted less of anincrease in core temperature and reduced heart rate of subjects cycling in a neutral environmentaltemperature. A one-percent glycerol solution added to a carbohydrate-electrolyte drink was bene-ficial in conserving fluids in a 6Gh simulated desert exposure (10). Obviously, the volume, concen-
Vol.57, No.7, 195 Fluid Intake, Glycerol and Urine Volume 653
tration, and timing of glycerol and other fluid intake requires additional exploration and modificationto meet the requirements of specific situations. Pre-loading with fluid could be particulady importantfor situations in which subjects must perform heavy work or be in a hot environment. For example,astronauts during exhavehicular activities, workers in chemical warfare suits, firemen in protectivegear, and athletes participating in 2- to 3-h events without breaks and with limi0ed access to fluidscould have reduced work capacities if they are unable to pre{oad with glycerol solutions.
Acknowledgements
This study was supported in part by NASA grants NAG 9-453/Basic, NAG 9-401 and NIH grant5M01-RR00997.
References
1. w.M. BoRTz,P.PAIJL, A.c. HAF4 and w.L. HOLMS, J. clin. Invest. 5rt537-1546(1982).
2. D.B. DILL, Iife, He:f, and Alrirrrde- 211p, Harvard Univ. press, cambridge, Mass.(1938).
3. J.E. GREENLEAR Med. Sci. Sporrs pas1s. )4((\) &5-656 (Igg2).4. T.P. LYoNs, M.L. RIEDESEL,L.E. MEULI and T.w. cHIcK, Med. Sci. Sporrs Exerc.
22 477-483 (1990).5' P. MONTNER, T. cHIcK, M.L. RIEDESEL, M. TIMMS and D. srARK, Med. Sci.
Sports Exerc. ?4(.s5) S152 (1992).S.V. MOROFR D.E. BASS, J. Appl. physiot.2n267-270 (1965).H.M. NEISLER, WG. LOIZ, K.D. JOHNSON, L.G. MEYER and D.J. HORRIGAN,J. FASEB 6(4) A1198 (1992).R. PELKONEN, E.Z. NIKKILA, and M. KEKKI, Diabetologia, 3 1_g (1967).M.L. RIEDESEL, D.Y. ALLEN, c.T. PEAKE and K. AL-eATTAN, J. Appl. physiol.632262-2268 (1987).
10. M.N. SAIVKA, Med. Sci. Sports Exerc.24 657-670 (1992).11. M.N. SAWKA, Md. Sci. Sports Exerc. 25S S35 (1993).12, S.L. WALD and R.L. MCLAURIN, J. Neur. Surg. 56 323-331(19g2).13. B. WTNKLER, R. srEELE, and N. ALTSZULER, Am. J. physiol. )16 tgt-tg6 (1969).
6.7.
8.
9.