supportive treatment adherence in hiv/aids supportive - onecpd
TRANSCRIPT

Supportive Treatment Adherence in
HIV/AIDS Supportive Housing:
A Guide for Staff
Technical Assistance and
Program Evaluation Bailey House, Inc.
October 2004

Bai
ley
Hou
se, I
nc.
275
Seve
nth
Aven
ue
12th
Flo
or
New
Yor
k, N
ew Y
ork
1000
1

TABLE OF CONTENTS
Bailey House Executive Director’s Note 4
How to Use the Guide 6
HIV/AIDS Treatment Adherence: Background Information
8
Adherence Strategies for Use in HIV/AIDS Supportive Housing 16
Evaluating Adherence Support Activities 41
Conclusion 43
Acknowledgements 44
References 46
Appendices 50
A. Sample outline of adherence training for staff B. Selected bibliography and Internet resources C. Adherence assessment/evaluation tool D. HIV medical adherence--initial visit E. HIV medical adherence – follow-up visit F. Guideline for initial client visit G. Advice from treatment activists H. Medication reminder resources I. About Bailey House & TAPE
3
Bailey House Executive Director’s Note
Stable, permanent housing and support services have always been vital to people living with HIV/AIDS. Even in the so-called “early days” of the epidemic and before the advent of medication treatments ranging from AZT to the newest class-es of antiretrovirals, the ability of a person living with HIV/AIDS to obtain and adhere to available treatment meant the difference between life and death. For homeless persons living with HIV/AIDS, a place to call home has always been a vital, yet often elusive, survival tool.
The founders of Bailey House, Inc. (originally called the AIDS Resource Center) started the agency’s supportive hous-ing programs in 1983 because they believed that housing is a human right. They knew then, as we do today, that homeless persons living with HIV/AIDS must have access to perma-nent housing and support services in order to obtain cutting-edge disease treatment and manage its challenges. Stable, permanent supportive housing has always been the hallmark of Bailey House’s mission.
Over the last 20 years, as the number of HIV cases has grown and treatments have advanced, HIV/AIDS housing and sup-port services have been a crucial element of the HIV/AIDS continuum of care. Thousands of formerly homeless persons living with HIV/AIDS survived into the second decade of the epidemic because they and others, like the Bailey House staff, have relentlessly advocated for the funding and development of a nationwide continuum of permanent housing and support services for persons living with HIV/AIDS.
4

The so-called “difficult to serve”—formerly homeless drugs users and those with mental health problems—readily use available HIV/AIDS services, adhere to complex treatment and seek and obtain resolution to personal and systemic chal-lenges when they have the powerful tools of stable housing and support. We hope this guide will inspire you to advocate for increased funding and development of HIV/AIDS housing so that homeless persons living with HIV/AIDS everywhere have what they need to access and manage treatment and care.
This guide is dedicated to the hundreds of Bailey House resi-dents who have inspired us with their courage, resilience and incredible zest for life. At Bailey House, we say, “The future starts with a place to live” because residents have taught us from the beginning that a place to call home is a powerful tool in the struggle to live with HIV/AIDS.
Gina Quattrochi, Esq. Chief Executive Officer Bailey House, Inc.
5
HOW TO USE THIS GUIDE
How can you, as an HIV/AIDS sup-portive housing staff member, ensure that your agency’s residents have the best opportunity to take advantage of potentially life-saving medication regi-mens? How can you promote HIV/AIDS medication adherence among residents, many of whose lives
encompass chaotic and complex situations, requiring a multi-tude of services on top of HIV medical management?
Supporting Treatment Adherence in HIV/AIDS Supportive Housing: A Guide for Staff addresses these questions with strategies and hands-on tips supported both by research and the day-to-day experiences of front-line workers. While the Guide addresses issues in New York City, it contains lots of information that is applicable to supportive housing programs outside of this geographical region.
Supporting Treatment Adherence in HIV/AIDS Supportive Housing: A Guide for Staff can be used by anyone who works at an HIV/AIDS supportive housing agency such as social workers, case managers, health care coordinators, nurses, property managers, resident coordinators and line staff. It may be used to add adherence-related services to existing pro-grams or to incorporate such services in to the design of new programs. It is not meant to provide content discussion on HIV/AIDS treatment, but ways to enhance treatment adher-ence among residents.
6

We urge you to provide copies of the Guide to staff and vol-unteers and create formal and informal learning opportunities within your agency (and potentially among other local agen-cies) to discuss (1) the barriers to treatment adherence and strategies for overcoming them, and (2) organizational changes that may be required in order to ensure that your agency’s residents receive the highest quality care including the latest medical developments.
Appendix A offers an outline for a 4-hour supporting medica-tion adherence training for use in conjunction with the Guide. The training is intended to convey basic adherence know-ledge, address adherence misconceptions, instill an under-standing of the real barriers that many people living with HIV/AIDS must overcome in order to benefit from treatment, and foster discussions on strategies that will increase access and facilitate treatment adherence for the specific communi-ties an agency serves. The training is for case management teams and clinical staff. Residence managers, maintenance workers, van drivers, cooks and other employees and volun-teers who have regular contact with residents should also be included in the training as their role in the day-to-day lives of residents can be quite significant.
7

HIV TREATMENT ADHERENCE: BACKGROUND INFORMATION
We are not an adherent society.” Claire Wingfield, Program Supervisor, California Statewide Treatment Education Program.
Approximately 800,000-900,000 people in the United States are infected with HIV.1 It is increasingly a disease of people of color and women. In the United States and globally, HIV/AIDS thrives in conditions of poverty, racism and homo-phobia.
Within these circumstances exists a treatment born of intense research and activism—antiretroviral therapy (ART*). Also known as triple combination therapy or the “cocktail”, HIV/AIDS medications have transformed the way people live. ART has significantly improved the health, quality of life and longevity of many people living with the disease. The first widely prescribed antiretroviral treatment, AZT (zidovudine) was introduced in 1987 and it significantly reduced the chance of transmitting HIV from mother to child during pregnancy and birth (referred to as vertical transmis-sion). In 1995 the Federal Drug Administration (FDA) approved the first protease inhibitor and since 1996, the num-ber of deaths among people with AIDS has sharply decreased.2 These decreases are mainly attributed to the use of ART.3
*Preceding the term antiretroviral therapy, this type of medication therapy was called highly active anti-retiroviral therapy (HAART).
8

Treatment guidelines issued by the U.S. Department of Health and Human Services establish the standard of care for the disease and the circumstances under which ART should be initiated. Adherence to ART is a key component of its success and must be taken in to account when discussions on ART ini-tiation begin. Failure to maintain 95% adherence to ART can give the virus just enough room to mutate and become resist-ant to medication.
The reality is that ART is not without challenges to those on it, their health care providers, and their support network (e.g., case managers, counselors, family members, friends). The drugs are expensive, complicated to take, numerous in daily dosage, side-effect rich, and may have long-term side effects that are unknown at this time.
The annual cost of providing ART for one person is approxi-mately $15,000.4 ART is often out of reach for many people unless they are financially secure, they have health insurance or they are eligible for the AIDS drug assistance program (ADAP) or Medicaid.
The demands of ART are formidable even for people with money, strong support networks and stable, uncomplicated lives. In general, 100% adherence to an agreed upon medica-tion regimen is very rare; moderate adherence seems to be the norm, with the majority of patients for all diseases (not just HIV/AIDS) taking 70-99% of the prescribed doses of their medications.5 Many studies have shown that about 50% of patients on ART—regardless of socio-economic background, race/ethnicity or illness—are non-adherent to their prescribed treatment regimens.6
9

In great measure, helping supportive housing residents adhere to ART boils down to helping them manage the jumble of competing needs they have to deal with every day-the first step consisting of the provision of decent housing and sup-portive services.
Sometimes clients’ competing needs are used to judge them ineligible for ART. For example, some health care profes-sionals question if a recovering drug addict with a history of sporadic housing can adhere to ART. In October 2000, Bailey House, Inc. and the Columbia University Joseph Mailman School of Public Health jointly published the findings of a study on HIV/AID housing, health and wellness. The study findings overwhelmingly supported the notion that “margin-alized persons once deemed unlikely to comply with difficult therapies can thrive on them when they have secure housing with supportive services responsive to their complex needs.”7
10

Major Findings of the Bailey House/ Columbia University Study*
Positive medical outcomes depend on appropriate private housing and coordinated non-medical sup-portive services that provide the stability on which access and adherence to treatment depend.
Homeless people with HIV who get any kind of practical housing assistance are almost four t imes more likely to enter into medical care than those who get case management but not housing assis-tance, and they are twice as likely to enter into appropriate, continuing care.
Persons who receive case management are almost 10 times more likely to enter appropriate medical care than those who remain unserved.
Case management, self-help drug treatment (NA,AA), mental health services and direct hous-ing services had the greatest effects on entry into and retention in care.
An integrated service package may result in a rela-tively enduring alleviation of competing needs that previously interfered with medical care.
An on-going, productive relationship with a m e d -ical provider is one of the most important predictors for success with antiretroviral combination thera-pies.
* Columbia University School of Public Health and Bailey House. (2000, October). Housing, Health and Wellness Study.
11
The Bailey House/Columbia University study and other stud-ies have shown that individuals with many competing needs can benefit from ART that includes adequate and individual-ly tailored support.8 The key for health care providers is to recognize and address true adherence barriers and avoid per-ceived barriers based on stereotypes and false assumptions.
Fact-based barriers to ART adherence include:
Homelessness It is estimated that at least 2.3 million and as many as 3.5 million individuals in the United States experience homelessness for at least a short period of time.9 Homelessness fre-quently occurs within the context of mental illness and substance abuse and behaviors related to these conditions can put one at risk for behaviors associated with infectious dis-eases like HIV. In New York City, an esti-mated 11,954 homeless persons are living with HIV.10 This represents a 19% HIV prevalence rate for this population.11
Homelessness for someone with HIV/AIDS likely means a lack of the stability needed to address many of the issues associated with the disease, little access to medical treatment and a lack of resources to purchase and prop-erly store medication.
12

Active substance use and/or mental illness People in HIV/AIDS supportive housing often have mental illness and/or histories of substance use. The rigorous demands of ART require the establishment of a routine of which a reliable and stable daily life makes adherence easier. Multi-diagnosed individu-als face the challenges inherent in chaotic drug use and/or untreated mental illness.
ART regimens can be complicated and often require many pills
For an individual with HIV/AIDS, there are many elements that can have a dramatic effect on their ability to adhere to medica-tion: understanding the disease, disease treat-ment and treatment commitment; the conse-quences of non-adherence; and interactions with medical professionals.12
Fundamentally, the complexity of ART and the often medical school-like information given to patients can make them unlikely to feel like partners in, much less directors of their own treatment. Despite the pharmaceu-tical industry’s move toward simplifying and combining medication dosages, most people on ART take many pills every day (including some pills to address ART side effects and others to guard against opportunistic infec-tions).
13
Medications often have specific instructions for the number of doses needed a day, inges-tion of medication (i.e., taking the medica-tion a certain number of hours before or after eating), taking medication with food, and avoiding interactions with other medications.
Many HIV/AIDS medications have side effects that affect day-to-day living
ART can be highly effective and it can have many side effects. Side effects and adverse events include anemia, diarrhea, fatigue, rashes, elevated triglycerides (cholesterol), bone marrow suppression and metabolic dis-orders such as lipodystrophy (a redistribution of fat cells).13 Add to that the reality that peo-ple with HIV/AIDS are more likely to expe-rience adverse effects from non-HIV medica-tions than the general public.14
ART regimens are expensive and many peopleare uninsured or underinsured
ART is not cheap; it is estimated that the annual cost of providing medication for one person is $15,000.15 In many states, ADAPs have had to restrict access to medications because funding has not kept up with demand.16 While New York currently has the largest ADAP drug formulary in the United States,17 in any state the ADAP funding amounts can change from year to year.
14

Distrust of the medical field and pharmaceuticalcompanies
Overcoming some residents’ skepticism of the government, the medical field and the pharmaceutical industry can be a formidable challenge, particularly in communities of color, which have been exploited by some of these same industries under the guise of med-ical research. The Tuskegee Syphilis Study of 1932-1972 remains, for many people, a reference point for the medical community and the government’s intentions. The Tuskegee Syphilis Study involved African-American men with and without syphilis who were enrolled, without informed con-sent, in the study. Those study participants with syphilis were not offered standard-of-care disease treatment and severely suffered (in some cases, died) due to this (lack of) action.18
15

“People living with HIV/AIDS can initiate and maintain dif-ficult regimens despite histories of homelessness, problem drug use and mental illness if appropriate information and support is provided.
Adherence Strategies for Use in HIV/AIDS Supportive Housing
#1. Provide residents and staff access to accurate and current HIV/AIDS treatment informa-tion and provide staff with on-going HIV/AIDS treatment and adherence training
#2. Develop an honest, supportive case management relation-ship with residents that will help them manage their lives
#3. Develop resident-centered adherence strategies based on the resident’s life
#4. Facilitate the availability of accessible and coordi-nated HIV/AIDS medical services for residents
#5 Help residents develop effective relationships with medical personnel and self-advocacy skills
#6 Understand the importance of non-clinical staff in adherence support activities
16
#7 Use cues to help residents remember to take their medication
#8 Provide access to nutritional food and information on proper nutrition.
Strategy #1: Provide residents and staff access to accurate and current
treatment information and provide staff with on-going HIV/AIDS treatment and adherence training
“Residents are often afraid to report the side effects, thinking something is wrong with them or that this is par for the course for the virus, instead of an effect of the meds,” Nadia Elliot-Hernandez, RN, Program Director, Heath Services Coordination, Bailey House, Inc.
Information on HIV/AIDS disease is constantly updated with new findings on prevention and treatment. Just staying on top of these developments can be a full-time job. This abundance of information can be overwhelming, yet it is incredibly important for people to stay well informed—whether it be a resident trying to chose a course of treatment or a case man-ager working with a recently diagnosed individual.
People taking medications need to know what they are putting into their bodies and why the medications are considered ben-eficial. Before residents even make the decision to begin a treatment regimen as complex as ART, they need to under-stand and seriously consider all aspects of the decision: What will it take to enter treatment? What will the side effects be?
17

What kind of support is available? What are the consequences of non-adherence or less-than-optimal adherence? Sound decisions are predicated on accurate information.
For staff to be conduits of current, accurate and complete information, they must be knowledgeable and up-to-date on treatment information. For example, Nadia Elliot-Hernandez, RN, Program Director, Health Services Coordination, Bailey House, Inc., said that when Sustiva was introduced, many res-idents weren’t told that hallucinations and vivid nightmares were potential side effects. She recounted the story of a resi-dent with mental illness who suddenly started hallucinating again, but this time as the result of a medication. Since he wasn’t aware that it was related to his medications, he didn’t report it to the health care coordinator. Elliot-Hernandez works with residents to help them become proactive and insists that their medical provider review all potential side effects of medications before prescribing.
Research on HIV/AIDS and its treatment is constantly evolv-ing so it is important to find sources of information that keep up with these changes and are accurate and credible. See Appendix B for a selected bibliography and Internet resources.
18
Tips for Increasing Residents’ Access to & Understanding of HIV/AIDS Treatment Information
Every encounter with resident is an opportunity to discuss medication adherence (e.g., case managers can discuss treatment issues and medication adher-ence at every appointment with a resident).
Ensure that residents have access to the Internet where they can download information on medica-tions. Provide links to websites that have gained acceptance and respect in the field for accurate and up-to-date information (see Appendix B for specif-ic sites).
Offer HIV treatment education meetings for r e s i -dents.
Create resident information-sharing groups that give residents a forum to talk to each other openly about their treatment experiences and share adher-ence tips.
Contact pharmaceutical companies—find out who are your community’s pharmaceutical company representatives for ART medications and ask them for free publications in plain language, free train-ings, visuals, and other useful tool they can offer.
19
Tips for Increasing Staffs’ Access to & Understanding of HIV/AIDS Treatment Information
Ensure that staff has access to the Internet where they can download information on medications. Provide links to websites that have gained accep-ance and respect in the field for accurate and up-to-date information (see Appendix B for specific sites).
Make sure meetings involving the agency’s entire staff include discussions on HIV/AIDS treatment and adherence. Staff needs a forum for sharing tips and advice on the challenge of helping resi-dents adhere to complicated treatment regimens. Have staff members take turns researching and presenting grand rounds training to the rest of the staff. Grand rounds are case presentations to multi-disciplinary teams.
Make sure training resources are accessible and affordable to staff and well advertised within the agency. Sometimes such resources (e.g., train-ings, conferences, journals) can be written in to contracts under the category of “professional development” or “staff training.”
Require a specific number of annual ART and treatment adherence training hours for staff as part of the agency’s overall training program.
20
Create linkages with other local community based organ-izations that offer treatment adherence information and services. Hire a health services coordinator (usually a nurse) or training coordinator to develop and conduct in-house trainings as needed and to provide up-to-date med-ical information for staff and residents.
Strategy #2 Develop an honest, supportive case management relation-ship with residents that will help them manage their lives
The Bailey House/Columbia University study stated that case management makes an individual 10 times more likely to enter appropriate medical care.19 At the heart of providing services to people with multiple needs is the need to establish non-judgmental and honest relationships. Residents will dis-close information if they feel that there will not be negative repercussions (e.g., discontinuation of service, judgmental comments, cold shoulder response). Residents may have many difficult situations in their lives that they need to man-age—violent relationships, children in foster care, drug use, mental illness, sex work. Passing judgment on residents can get in the way of identifying treatment obstacles and creating effectives plans to address these obstacles.
As with most HIV-related services, it is imperative that resi-dents are certain that what they discuss with case managers will be kept confidential. Case managers can alleviate con-cern by discussing their agency’s case management confiden-tiality guidelines with residents and making sure they under-stand them.
21

Tips for Creating a Supportive Case Management Relationship with Residents
When meeting with residents, use body language that is open and sensitive. For example, make eye contact, show personal interest in what the resident is saying, and provide positive reinforce-ment.* Let residents know that they are free to discuss reservations and fears that they have about ART and that they always have the option of not start-ing ART. Ask residents questions about their adherence that will not only involve affirmative response, but also prompt discussion. By being able to answer “yes”, the client may be better able to pro-vide an honest assessment of his/her practices. For example, “Do you ever forget to t a k e y o u r medicines and if so, when does that h a p p e n ? ” and “When you feel better do you sometimes stop taking your medication and if so, what can I do to help you change that?**
Do not discuss residents’ personal information in public areas. Even if you do not mention a peson’s name, people around you may be able to determine whom you are discussing. Review your agency’s confidentiality policy with residents.
22

* National Institutes of Health, Office of AIDS Research. (1997, November, 20-21). Adherence to new HIV therapies: A research conference. Held in Washington, DC. ** Morisky, D. E., Green, L. W., & Levine, D. M. (1986). Concurrent and predic-tive validity of a self-reported measure of medication adherence. Medical Care, 24(1), 67-74.
Strategy #3 Develop resident-centered adherence strategies based on
the resident’s life
Adherence activities should take into account that residents’ move along a care and treatment continuum and that they should have access to adherence support services at every point along this continuum.
Helping residents decide if ART is the right option for them is one of the first steps in supporting an appropriate adherence plan based on the realities of residents’ lives.
If residents are interested in beginning ART, they should be involved in the creation of resident-specific treatment adher-ence support plans, based on current knowledge and under-standing about adherence.20
“[As an agency staff member] the key is knowing what ART [antiretroviral therapy] exists, when they [medication] are supposed to be taken and how, along with the common side effects. Fact sheets for most ART [medications] are available and would be a good resource for case managers or other pro-gram staff working with residents who are not clinicians,” according to Mark Waters, Director of Treatment Adherence and Clinical Education Initiatives, AIDS Institute, New York State Department of Health.
23

“Ask them [residents] what [treatment adherence] support they want. Give them a menu,” suggests David Evans, Assistant Director of Treatment Education, Gay Men’s Health Crisis, New York City. By asking residents what type of ART support they would like, you can reverse the usual doctor (or provider)-to-client relationship, reinstating residents as the ultimate authorities on their health and well-being. In this scenario, staff help residents achieve their own goals by guid-ing them with accurate information and offering multiple sup-port activities the residents can choose from. For instance, the staff could offer a range of specific support options from weekly check-ins to daily observed medication taking.
Waters recommends addressing adherence at every client encounter, “There is too much at stake to wait until some defined point in time for an assessment. If the client becomes resistant to his/her current regimen, the options for other reg-imens may be greatly limited.” Formal treatment adherence assessments can identify specific areas where a resident has adherence barriers. An assessment should be used whenever a new treatment plan is necessary, particularly upon discovery that an old treatment plan is no longer working. The treat-ment plan is written by the resident with support from the case manager and it lays out what steps they will take to address any identified issues. Regular health assessments should include medication adherence questions. (See Appendix C for a sample adherence assessment tool.)
24

Tips for Developing a Resident-centered Approach to ART Adherence
Residents thinking about starting ART...
Talk to residents about ART and whether or not it is a potential treatment option for them. Use adher-ence assessment tool (see Appendix C) to aid in these discussions. Ultimately, the resident will make the decision as to whether or not to pursue ART.
Help residents prepare for treatment adherence by having them mimmick a medication schedule, make their own doctors appointments, engage in support groups, name adherence barriers and devel-op adherence plans to address barriers. Claire Wingfield of California’s Statewide Treatment Education Program (CSTEP), a collaboration between Asian & Pacific Islander Wellness Center and Project Inform, uses jelly beans as an adher-ence practice tool. “I have clients test their ability to adhere and to explore what their limitations are by using jelly beans. Have them adhere to a regi-men of jelly beans for two weeks. It can give someone confidence or make them realize how they will have to adjust,” said Wingfield.
Share medication fact sheets with residents ( f a c t sheet source: http://www.nlm.nih.gov/medline-plus/druginformation.html)
25

Once the resident has started ART…
At every encounter (e.g., case mangement, nutri-tion counseling, regular health assessments/reass-essments), discuss adherence issues with residents.
In discussing adherence with residents, include open-ended questions that will foster discussion, like, “How can I help you to adhere to your treat-ment?” Simply asking yes or no questions like, “Have you been adhering to your medications this week?” can have a stifling effect on the discus-sion.
Help clients plan for anticipated and unanticipat-ed (to the degree possible) breaks in their adher-ence routine. Have backup plans in place.
Enlist the help of peer educators and volunteers who can help residents get to their appointments by accompanying them or providing buddy sup-port.
Provide incentives for clients who engage in adherence activities. Incentives don’t have to be cash; get creative and use subway tokens, goodie bags with shampoos samples and tooth brushes, movie passes, etc.
Ensure that medical and social services are acces-sible by offering home visits or convenient hours and service locations.
Share medication fact sheets with residents.
26

Strategy #4 Facilitate the availability of accessible and coordinated
HIV/AIDS medical services for residents
If a resident grants you (as a case manager) permission to speak to his/her doctor, the housing staff should regard the doctor as an important member of the resident’s team.
Access to and coordination of HIV/AIDS medical services for residents involves residents finding appropriate care, being able to get medical appointments, establishing relationships with medical staff, and being treated well by medical staff. It also includes appropriate staff establishing a relationship with residents’ primary care providers and helping residents get to medical appointments, and avoiding duplication of services. Coordinated medical services need to be the effort of multiple providers—providing comprehensive HIV/AIDS disease services is too complex a task for any one provider.21
Action Point, a treatment adherence case management pro-gram in San Francisco, facilitates medical services access by having a conveniently located storefront operation and a flex-ible appointment schedule. Action Point also provides trans-portation to the clinic and pharmacy as needed. Day treat-ment programs that provide one-stop shopping for a range of service needs are more often providing their own primary care programs and expanding their ability to provide array of services at one location.
27

Bailey-Holt House, a congregate residence, supports medical sevices access by having an on-site nurse provide health edu-cation and assistance to residents as needed. The agency also provides cluster care homecare assistance, where eligible res-idents share a home health aid’s time during the day, enabling the aid to attend to the resident’s needs more organically throughout the day rather than within a 2-hour time period.
Case managers need to be familiar with and current on med-ical management models and important developments in HIV/AIDS medication treatment therapies. This will help them understand the type of medical services residents need and the ways in which to coordinate such services.
Tips for Creating Accessible & Coordinated Medical Services for Residents
Make your agency/services easily accessible to clients (i.e., on bus and/or subway route). Transportation barriers are often easily resolved with a small amount of money. In New York City, Access-A-Ride offers paratransit trans-portation for people with disabilities for the price of regular public transportation ($2). Medicaid covers the price of other ambulette services when needed.
28

Have on-site nurses provide health education and assistance. In congregate housing settings, have eligible residents share the services of a home health aid and involve the aid in adherence strate-gies
Should a resident grant you permission, make his/her medical provider an integral member of the service team. Keep track of residents’ med-ical appointments and ask if they need a reminder phone call. Set up transportation a day in advance if needed.
Accompany residents to their doctor’s appoint-ments. Have case managers visit their residents’ doctor offices to build a care team and coordinate treatment information (with resident’s consent). Keep adherence high on the list of team meeting topics.
Share adherence tools with residents’ medical providers (see Appendix D, E & F).
Locate pharmacies that provide services such as medication delivery, simplified billing, reminders for refills, and medication adherence devices.
Provide an escort to the pharmacy to pick up medication.
29
Strategy #5 Help residents develop effective relationships with medical
personnel and self-advocacy skills
“In order for ART to be effective, the client needs to be able to be open and honest with the primary care physician (PCP). Charles King, Co-CEO, Housing Works, Inc.
In an examination of 1997-1999 ART research, the variable most predictive of better adherence was “…a strong relation-ship (support, trust and a feeling of being well cared for) between the patient and the clinician/health care provider and/or system.”22
In addition, “An on-going relationship with a medical provider is one of the most important predictors for success with anti-retroviral combination therapies.”23
An important aspect of this strategy involves finding a pri-mary care provider (PCP) who has experience treating patients with HIV/AIDS and who won’t make negative judg-ments that are adverse to the patient’s interests. “That may mean using a nurse practitioner as a PCP. It may mean circu-lating till you find the right PCP. Or it may involve residents talking to other residents and staff about identifying a PCP who has a reputation for being non-judgmental,” said Charles King, Co-CEO of Housing Works, Inc., New York City.
Keith Cylar, the other half of the Housing Works, Inc. co-CEO team added that seeking out such a PCP may be tricky. “This is not a black and white issue. [For instance] Once you
30

[a resident] tell your healthcare provider that you use drugs, your care becomes tainted. Everything you do is viewed through that lens and you can bet it has a major impact on your relationship. Before you go through that door, it is help-ful and wise to get a sense of the impact of your drug use on your health and medications first from someone besides your PCP. Weigh the benefit and risk and then make a decision.” Practicing these discussions with a non-judgmental case man-ager, health educator or nurse can prepare residents and trans-forms their expectations of medical care.
New York City’s Housing Works community case manage-ment program makes an effort to accompany all residents to their doctors’ appointments. The presence of the case man-ager (or community follow-up worker or case management technician) helps empower residents to ask more questions of their doctor. Housing Works case managers hit the road to coordinate case management and medical services (with the client’s consent).
With the consent of the resident, regular interaction between the doctor and the appropriate staff can take place through telephone calls, emails and faxes. When using these types of technology for communication, it is important to address con-fidentiality issues including the Health Insurance Portability and Accountability Act of 1996 (HIPAA).
Case managers can also discuss aspects of disease treatment with residents that address standards of care and service coor-dination. Some questions a case manager may want to ask residents include:
1. What do you think about the care you’re getting from your medical provider?
31

2. Can you do the things your doc-tor tells you to do?
3. Can you take your medication the way the doctor told you to take it?
4. Have you ever had a resistance test?
5. How can I help you get the ser- vices you need?
6. When is your next appointment?
7. Can I come with you to your doc-doctor appointment?
Tips for Helping Residents Develop Effective Relationships with Medical Personnel & Self-advocacy Skills
As a case manager, foster an open and honest rela-tionship with residents and help empower them to demand the same from their PCPs. Create a referral list of PCPs who are available to residents and provide effective, nonjudgmental care.
Help residents build assertiveness by roleplaying a discussion with doctor.
Have residents plan questions for the doctor using 3x5 cards. Reviewing potential answers can help residents understand the reason for the question along with the relevance and implications of the answers.
Encourage residents to get copies of their lab work from their medical providers and keep the informa-tion at their service provider’s office.
32

Encourage residents to keep a notebook of what is going on with them between doctor office visits. This activity may make it easier to remember questions. Case managers can help fill in the notebook, especially if the resident has difficulty reading and writing.
Have residents accompany each other to the doctor for support.
Create empowerment groups (e.g., weekly sup-port group) to help residents feel comfortable questioning and challenging their doctors.
Give residents information on treatment advo-cacy (see Appendix G).
Strategy #6 Understand the importance of non-clinical staff in
supporting adherence activities
“Food service staff are like hair dressers for the residents— residents tell them their whole life story,” Chris McCloud, former Director of Housing Management, Bailey House, Inc.
In some instances, residents will have more contact with front-line maintenance staff than their case managers. Maintenance staff may be privy to details about a resident’s living conditions that case managers may not see or take into account when developing adherence schedules.
33

Assuming that all competing needs are potential barriers to treatment adherence, the maintenance person’s knowledge can be key to helping a client identify and address barriers. Treatment adherence issues should be discussed at all staff meetings and when appropriate, non-clinical staff should report adherence related issues to case managers. It is impor-tant to have the appropriate staff sign confidentiality state-ments.
Tips for Enhancing ART Adherence Through Non-medical Staff Relationships
Medical and social service staff should recognize that resident managers are usually the first staff to see returning or existing chaos in a resident’s life. Provide non-clinical staff with trainings that help them understand clinical issues such as adher-ence.
Include non-clinical staff (e.g., housing manage-ment staff, food service staff) in team meetings.
Let non-clinical staff know about adherence issues that may affect their interactions with res-idents (e.g., residents requesting access to certain foods in order to take their HIV/AIDS medica-tions in the proper manner).
Address resident confidentiality issues with non-medical staff and discuss who it is appropriate to pass resident information to (e.g., case man-agers).
34

To enhance the development of resident and staff rela-tionships, create open office space and common areas.*
* Joan Byron, Pratt Institute Center for Community and Environmental Development.
Strategy #7 Use cues to help residents remember to take their
medication
The most frequently cited reason for not taking medications according to schedule is forgetfulness.24 Many cueing servic-es and gadgets are now available free or at low-cost to people with limited incomes. When talking to residents about the types of adherence support they would like, determine if the below-mentioned cues are available and if they would be helpful to them.
Tools & Strategies That May Help Residents Adhere to Their Medication
Pill charts and pillboxes Pill charts are visual charts that graphically dis-play which pills need to be taken and when. Pillboxes come in daily, weekly and monthly sizes. They help residents organize in advance the pills they have to take so as to minimize both hassle and room for error. Pill charts and boxes are available free of charge from many pharma-ceutical companies. Some HIV/AIDS support-ive housing agencies include pillboxes in their orientation package for new residents.
Directly Observed Therapy DOT was initially mandated for certain people who had tuberculosis. DOT is when a person
35

helps you remember to take your medication by actually watching your take it. With ART adher-ence, DOT is voluntary and many clients appre-ciate having someone remind them when to take their pills and administering the medication. Most programs using DOT consider it a good way to assist people in developing the skills to take their medicine independently.
Medication monitoring bottle caps This tool is sometimes called MEMS. It is an electronic beeping device in a pill bottle’s cap that tracks the opening of the bottle, providing feedback on how the individual is taking medica-tions.
Human help There are a multitude of verbal cues and prompts that can help residents with medication adher-ence:
1. Residents can request that their medication be stored at the nurs-es’ office and distributed to them daily.
2. Residents can request phone calls from the front desk to remind them to take their med-ication.
3. Staff can prompt residents about medication adherence by linking pill taking to daily activities (e.g., “Take your second dose when Oprah comes on.”).
36

4. Residents can share their own experiences and remind each other to take their medications.
The pharmaceutical industry Pharmaceutical companies offer all kinds of gadgets to help their customers adhere to med-ication. They and pharmacists are a valuable resource for information on drug interactions. Contact pharmaceutical companies’ community representatives in your neighborhood and local pharmacists to find out about support aids that they offer to customers. In addition, some phar-macists give out beepers and program them according to the resident’s medication schedule.
See Appendix H for a list of medication reminder tool resources.
37

Pros and Cons of Adherence Reminders
Tools Pros Cons
Directly observed therapy
The most effective way toensure that the dose is actually taken
Labor intensive (seven days a week, 365 days a year, multiple daily doses
(DOT) Can be combined with other treatments (e.g.,DOT for TB, methadone dosing)
require multiple daily encounters)
Medication Allows for privacy Expensive
montioring Offers residents a record Adherence measured bottle caps of their pill taking times when bottle is opened,
(MEMS) which may not be pro-ceeded by the individual actually taking their med-ication
Don’t work well with pill boxes
Pagers Allow for privacy
Can travel with resident Need to be programmed
Personal reminders
Can develop relationship between staff and resi-dents
Can be disrupted by changing schedules
May be seen as another
Can help residents devel-op their own cues
task for often overbur-dened staff
Can create a power dynamic between staff and residents
Pill boxes Relatively inexpensive Individual must be able to (sometimes available pre-pour pill boxes forfrom phramaceutical rep- themselves resentatives for free)
May require weekly clini-cal supervision or super-vision by a nurse (some
38

Tools Pros
Can travel with resident
Some pill boxes provide cues indicating the time of day the medication should be taken
Cons
jurisdictions may restrict who can supervise pill box prepouring)
Some individuals may want to pre-pour pill boxes (issues of con-fidentiality)
Refrigerated medications can’t be combined with other medications (consider using more than one pill box)
Pill boxes may not fit in to an individual’s pocket if they are away from home
Pill Charts Useful for organizing and displaying complex, multi-dose regimens
Colorful pill charts and pill pictures (stickers) are available (often at no charge) from pharmaceu-tical representatives
Pills charts should be developed only by licensed health care providers-some jursidictions may restrict who may develop pills charts
Pill pictures are usually available for HIV/AIDS not other medica-tions
Using a black and white printer for printing out pill charts can have less impact than using a color printer
Timers Travel with resident
Relatively inexpensive
Have to be set
Can draw attention to the resident
Watches Travel with resident
Relatively inexpensive
Have to be set
Can draw attention to the resident
39

Strategy #8 Provide access to nutritional food and
information on proper nutrition
Food can become a tricky issue for a person on ART. Some HIV/AIDS medications come with very specific directions for ingestion—some must be taken on an empty stomach, oth-ers on a full stomach or after the person has had a specific snack. Dairy or a high fat meal may be required to aid absorption.
Easy access to food at specific times—not just at mealtimes— becomes essential to adherence. Small individual refrigera-tors are an inexpensive but critical tool to give residents a place to store their medication (some require storage in a cool place) and a place to keep whatever nutritional requirements are necessary. In some congregate settings specific foods such as sandwiches, orange juice, vegetable juice, yogurt, milk, pudding, Gatorade and fresh fruit are always made available. New York City’s God’s Love We Deliver offers free nutritional assessments and counseling along with the delivery of two homemade meals (lunch and dinner) every day. These meals may be individually tailored to the person’s dietary restrictions. There are enough available treatments that doctors have some ability to prescribe medications taking a person’s life, schedule and dietary limitations into account.25
40

Tips for Supporting Residents’ Nutritional Health
When appropriate, labels foods that are good for taking with certain medications.
Talk to residents about the foods they like to eat and help them get those foods.
In congregate housing settings, have small refrig-erators in residents’ rooms.
Encourage residents to talking with their PCP about the nutritional specifics of the HIV/AIDS medications they take.
Have “cheat sheets” on medications and food to review and share with residents.
EVALUATING ADHERENCE SUPPORT ACTIVITIES
How can you tell if the adherence activities are working? What will “success” look like? Ideally, any agency that wants to measure the effects of its adherence activities would determine what success look likes before the start of the activities so they could look back to see if the “success” was achieved.
41

Some markers of program success may include:
Are residents self reporting that their adherence has increased since the start of adherence activities?
If the adherence activity involves having case man-agers help residents develop “back-up plans” for use when they have an anticipated or unanticipated break in their adherence routine, have these back-up plans been developed and have residents actually used the plan when needed?
If the adherence activity involves working with res-idents to help them have more positive communica-tions with their healthcare professionals, are the res-idents reporting such communications?
If the adherence activity involves increasing the number of scheduled discussions case managers regularly hold with residents’ health care providers, has this happened and what were the results of such discussions? If a staff member is using adherence assessment tools with residents at regular intervals, do the tools show that the resident has increased his/her adher-ence and/or activities that may lead to increased adherence?
These are some of the ways your agency can assess its adher-ence activities and then this practical knowledge can be used to made program modification when warranted. In addition, this information can be used when training current and future staff and it can also be used as part of program reporting and when applying for grants/funding. Always look out for the latest information on adherence research and adherence assessments tools and resources that your agency can use.
42

CONCLUSION
The battle for 95% or higher adherence among a population that daily faces many complex competing needs is daunting. It requires a fundamental shift in the standard model of hous-ing and services. This shift requires that all staff (clinical and non-clinical) be committed to learning about HIV/AIDS treatment and adherence issues and supporting residents who go on ART.
While people in HIV/AIDS supportive housing often face competing needs, adherence activities can drastically improve an individual’s ability to adhere to complex medication treat-ments and live longer, more healthful lives.
43
Acknowledgements
Supporting Treatment Adherence in HIV/AIDS Supportive Housing: A Guide for Staff was made possible by generous grants from The Jacob and Valeria Langeloth Foundation and the New York Community Trust. This guide was written and edited by Leah Stockett under the supervision of Christine Campbell, Nina Herzog and Jeanne Bergman. Any document errors are the responsibility of Bailey House, Inc.
Thanks are due to the following people for the generous contribu-tion of their time and expertise:
Joshua Bamberger, Medical Director for Housing and Urban Health, San Francisco Department of Health, and Director, Action Point
Daniel Bao, Associate Director, Research and Technical Assistance, Asian/Pacific Islander Wellness Center
Joan Byron, Architectural Director, Pratt Institute Center for Community and Environmental Development
Sheryl L. Catz, PhD, Assistant Professor of Psychiatry and Behavioral Medicine, Center for HIV/AIDS Intervention Research (CAIR), Medical College of Wisconsin
Andrew Coamey, Manager of Consulting Services, Hudson Planning Group
Connie Cunningham, Chief Program Officer, Bailey House, Inc.
Keith Cylar, Co-CEO, Housing Works, Inc.
David Evans, Assistant Director of Treatment Education, Gay Men’s Health Crisis
44

Alison Fogge, Program Manager, SHAP, Bailey House, Inc.
Marc Gourevitch, MD, Director of Addiction Medicine, Montefiore Medical Center and Albert Einstein College of Medicine
Sheila Harrington, Substance Abuse/Mental Health Specialist, Bailey-Holt House
Patricia Haversham-Brown, Director, SHAP, Bailey House, Inc.
45

References
1. Centers for Disease Control and Prevention. (1999). CDC guidelines for national human immunodeficiency virus case surveillance, including monitoring for human immunodeficiency virus infection and acquired immunodefi-ciency syndrome, RR-13(48), p. 1-27.
2. Centers for Disease Control and Prevention. (2002). HIV/AIDS surveillance report, 13(2), p. 6.
3. Centers for Disease Control and Prevention. (1999). CDC guidelines for national human immunodeficiency virus case surveillance, including monitoring for human immun-odeficiency virus infection and acquired immunodeficiency syndrome, RR-13(48), p. 1-27.
4. Lurie, P., DeCarlo, P., & Miller, S. (1997, May). Do new HIV drugs affect HIV prevention? [Fact sheet, #27E]. San Francisco, CA. University of California, San Francisco, Center for AIDS Prevention Studies. Retrieved April 19, 2002, from http://www.caps.ucsf.edu/FSindex.html
5. Flexner, C. (1998). Practical treatment issues and adher-ence: challenges from the clinic. HIV/AIDS Treatment Updates.
6. Levine, A. (1998). Antiretroviral therapy: Adherence. Medscape HIV/AIDS eJournal, 4(2). Retrieved April 19, 2002, from http://www.medscape.com/viewarticle/408212
46

7. Bailey House, Inc. and Columbia University Joseph Mail School of Public Health. (2000, October). Housing, health and wellness study: Final report. New York, NY: Author.
8. Shelton, D. L. (2000, Sept. 18). Complications of AIDS. American Medical News, 43(35). Retrieved April 19, 2002, http://www.amaassn.org/scipubs/amnews/pick_00/hlsa0918. htm
9. Urban Institute. (2000, February). A New Look at Homelessness in America.
10. McClain and Associates, Inc. (2002, March). Initial needs assessment for New York City, 2002, p. 59.
11. McClain and Associates, Inc. (2002, March). Initial needs assessment for New York City, 2002, p. 59.
12. Ibid.
13. Department of Health and Human Services & the Henry J. Kaiser Family Foundation. (2002, February 4). Guideliness for the use of antiretroviral agents in HIV-infected adults and adolescents.
14. Piscitelli, S. C., & Flexner, C. (2001, July 27). Scheduling medications in HIV disease [Presentation]. Retrieved on April 19, 2002, from http://www.medscape.com/viewprogram/673
15. Lurie, P., DeCarlo, P., & Miller, S. (1997, May). Do new HIV drugs affect HIV prevention? [Fact sheet, #27E]. San Francisco, CA. University of California, San Francisco, Center for AIDS Prevention Studies. Retrieved April 19, 2002, from http://www.caps.ucsf.edu/FSindex.html
47
16. AIDS Policy & Law. (2002). Access to HIV drug pro-grams loses pace as need grows, 17(12), 3.
17. AIDS Policy & Law. (2002). Access to HIV drug pro-grams loses pace as need grows, 17(12), 3.
18. Centers for Disease Control and Prevention. The Tuskegee Syphilis Study: A hard lesson learned. Retrieved August 21, 2002 from http://www.cdc.gov/nchstp/od/tuskegee/time.htm
19. Bailey House, Inc. and Columbia University Joseph Mail School of Public Health. (2000, October). Housing, health and wellness study: Final report. New York, NY: Author.
20. Indky, D. (n.d.). Providing adherence support to special populations: Reaching, engaging, and retaining elusive indi-viduals in consistent care [Presentation]. New York, NY. New York State Department of Health, AIDS Institute. Retrieved April 19, 2002, from http://www.hivguidelines.org/public_html/center/clinical-education/education-slide-presentations/educ_slide_pres.htm
21. Gray, L., Edmondson, E., & Lemke, A. L. (1998, October). HIV treatment adherence: A guide for program development. Seattle, Washington: University of Washington, School of Social Work, HIV/AIDS Project Development and Evaluation Unit.
48

22. Webster, R. D., & Barr, D. (1999, November). Adherence to highly active antiretroviral therapy (HAART) among individuals with HIV/AIDS: A compendium of HAART adherence research, November 1997 – November 1999. Washington, DC: The George Washington University Medical Center, Center for Health Policy Research.
23. Bailey House, Inc. and Columbia University Joseph Mail School of Public Health. (2000, October). Housing, health and wellness study: Final report. New York, NY: Author.
24. Chesney, M. (1998, June). 12th World AIDS Conference, Geneva, Switzerland (Presentation).
25. Piscitelli, S. C., & Flexner, C. (2001, July 27). Scheduling medications in HIV disease [Presentation]. Retrieved on April 19, 2002, from http://www.medscape.com/viewprogram/673
49

APPE
ND
IX A
Supporting Medication Adherence Staff Training
Below is an outline for a sample 2-day, 4.5 hour train-ing intended to create a forum for discussing some of the notions and best practices presented within the manual. The training below outlines such a forum while highlighting the main points of the manual. Its audience is broad: case management team members to food service providers to development directors. This training is intended as an overview and introduc-tion to the topics discussed in the manual and can be helpful to all levels and roles in HIV/AIDS sup-portive housing organizations. It is intended to empower staff (and potentially clients) to consider ways that they can integrate health management into their jobs and ways the organization itself can respond to this new challenge. Participants are asked to come up with new ideas for working.
We recommend that when possible, this training should be given by a health educator or nurse.
DAY ONE: 2 hr., 15 min. A. New Model for Services: Housing + Services +
Primary Care (1 hour, 10 minutes)
a. Defining terms (35 minutes)
i. Adherence (10 minutes)
1. Taking your meds when and as pre-scribed
50
2. Consider all the ways someone could be non-compliant in taking their ART other than simply missing a dose.
3. Taking it at the wrong time. 4. Under the wrong conditions: empty stomach,
full stomach, etc.
ii. Antiretroviral therapy (10 minutes)
1. Ask participants, Name some of the antiretro-viral drugs.
2. Define antiretroviral therapy, its purpose, and how it works.
iii. Human immunodeficiency virus (15 minutes)
1. Quick review of HIV’s effect on the body 2. Quick review of what antiretrovirals do to
HIV. 3. Encourage lots of questions.
b. Expanding the traditional model of supportive housing from housing plus services to housing + services + healthcare. (35 minutes)
i. What is supportive housing? (15 minutes)
1. What services make up the “housing plus services” model?
2. What kinds of supportive housing are there?
3. How has medical care been included in supportive housing?
51
ii. Explain what lead to the shift in focus on medical care (more medical hope translatininto a greater focus on medical care) (5 minutes)
iii. Hand out 3 x 5 cards. Ask each person to write their job title on a card and then write down 2 tasks they could do in the course of their work to help clients’ healthcare. Then pass the card to your right and add one task to the card that you receive (maybe you get the development director’s or the driver’s). Repeat as time allows. Return the cards to their original own ers and discuss the results.
II. Barriers to Adherence (1 hour, 15 minutes)
(This section is intended to be primarily a group discus-sion. Case managers and participants are encouraged to draw upon real life situations and share cases with the group. This is an information sharing session.)
a. Non-adherence is a fact of life. (5 minutes)
i. Don’t get all high and mighty. The chances are that if you were on long-term complicated treatment, you would be less than perfectly adherent, too.
ii. Ask, how many people here have at one time or another not completed a dose of antibiotics? Or not fully refrained from drinking alcohol during the treatment?
52

b. People with HIV are prone to more severe sideffects. (15 minutes)
i. HIV itself can exacerbate otherwise nasty side effects.
ii. Mental illness (latent or not) can exacerbate psy-chological side effects
iii. Ask participants to name some of the side effects they or their clients have experienced.
iv. Trade tips on dealing with side effects. Form small groups and writedown some tricks of the trade.
c. People are still dying. (15 minutes)
i. Why do people remain skeptical of the medical-pharmaceutical industrial complex? Explore valid history of racism, exploitation, profiteering, etc.)
ii. Do you believe in a antiretrovirals? If so, why? If not, why not?
iii. How can a service provider help a client to over come skepticism standing in the way of helpful treatment? Discuss strategies.
d. Adherence to ART is difficult and complicated. (10 minutes) i. Have case managers share some of their clients’
treatment regimens. Share some true cases (with out names).
1. Include the client’s ART 2. Include the client’s opportunistic infection
prevention medications.
53

3. Include medication to treat side effect 4. Include other medications: for high blood
pressure, vitamins, etc.
e. Drug use and psychological disabilities pose additional challenges. (10 minutes)
i. Give some examples of how clients’ mental health has an impact on their health care and/or adher-ence.
ii. Give some examples of how clients’ drug use has an impact.
f. The medical-pharmaceutical industrial complex speaks a foreign language. (5 minutes)
i. How large are the warning labels on medications? ii. Can you understand the 11 x 14 insert that comes
stuffed inside the medication, written in a four-point font?
iii. Can you read your doctor’s handwriting? iv. Can you understand your doctor at all? v. Do you think s/he tries to understand you? vi. What language do they speak?
g. Confidentiality is key. (5 minutes)
i. How can confidentiality play a role? ii. Briefly review the importance of the confidential-
ity form and how it’s used. (The confidentiality law can always stand repeating.)
54

h. Social support is important for success. (10 minutes)
i What do we mean by social support?
ii. Give some examples of how providers lend social support?
iii. What can providers do to encourage support from others?
1. Peer groups 2. Buddy systems 3. Family work 4. Support groups 5. Peer education work 6. More
55

III. DAY TWO: 2 hrs., 10 min. Supporting Adherence (2 hours, 10 minutes)
a. Client-centered approach (25 minutes)
i Review the goals of a client-centered approach (5 minutes)
1. Bringing individuals into care 2. Keeping clients in care 3. Reducing additional risk 4. Linking prevention and care\
ii. Review the principles (5 minutes)
1. Clients are self-directing adults whose choices should be respected.
2. Service providers play an important supporting role by facilitating access to the best informa-tion on which to base decisions and helping clients to clarify choices.
3. Every client can and must be engaged at some point along the health and wellness continuum.
4. Help clients identify the next small step they are willing to take to manage their health and make a plan to achieve it. (The client sets the goal. Ask the client how you can help him/her achieve the goal.)
iii. All unmet needs are potential obstacles. (5 minutes)
1. Name some needs that can get in the way of health management and treatment adherence.
56

2. Clients need accessible supportive services in order to achieve their goals. Name some acces-sible support services that can meet some of the needs mentioned in the previous point.
3. Treatment regimens need to be designed to fit the consumer’s life.
b. Current, accurate and complete information (15 minutes)
i. Consumers must have access to all the available information. 1. In what ways can an organization facilitate
clients’ access to information? (5 minutes) 2. Staff members need on-going training (like this
one) and access to information themselves. 3. Ask participants to discuss what kind of train-
ing they would benefit from. If they could cre-ate an annual calendar of trainings, what would it entail. Also, what additional resources does
the organization need in order for its staff mem- bers to have access to current information. Participants should divide into job-related groups. (10 minutes)
c. While in these same groups, ask participants to turn to the Tips section of their manuals. Review the tips for “A Client-Centered Approach” and “Current, Accurate and Complete Information.” Discuss which ones are applica-ble and which are not. Change them and add to them as a group, using the Notes section in the margins. (10 minutes)
57
d. Open and honest communication (30 minutes) i. Service providers can model non-judgmental
relationships (10 minutes)
1. What is a non-judgmental relationship? What are its benefits?
2. How does this translate to a client’s rela-tionship with his/her doctor?
3. What are the dynamics between a doctor and patient?
4. Should a client discuss street drug use with a doctor?
ii. Service providers can teach assertiveness and empowerment skills. (10 minutes)
1. How can providers help empower their clients in their relationships with their doctors? a. How can case managers do this? b. How can non-clinical staff do this?
iii. What effects can environment have on client’s health? (5 minutes)
1. Ask housing management and maintenance staff, in particular.
iv. Treatment adherence discussions require hon-esty. (5 minutes)
1. What do you need in order to be honest? 2. What can impede honesty? 3. Why is honesty so important?
58

e. Reducing basic competing needs (15 minutes)
i. Assessments and reassessments are tools for determining changing needs.
1. Hand out organization’s assessment and reassessment tools. Ask participants to review them. Do they address adherence? Do they address health management?
ii. Nutritional assessments and counseling are essential.
iii. Untreated mental illness can become an impediment to adherence.
iv. Substance users have special needs.
v. What steps can staff members take to strengthen access to nutritional, mental health and substance use? Is access adequate at this point? What other services are essential to reduce basic competing needs.
f. Ask participants to turn to the Tips section of their manuals. Review the tips for “Open and Honest Communication” and “Reducing Basic Competing Needs.” Discuss which ones are applicable and which are not. Change them and add to them as a group, using the Notes section in the margins. (10 minutes)
59

g. Coordination of services (10 minutes)
i. Coordinate medical and case management services
ii. Plan regular team meetings and case confer-ences around adherence.
iii. Maintain regular contact with medical providers as part of the service provision team.
iv. Ask participants to review the tips section. Which of these tips are possible and which are not? What are some alternatives better suited to your agency and clients?
h. Using cues (10 minutes)
i. Most frequently cited reason for missing doses: forgetfulness.
ii. What techniques and devices are available?
1. Directly Observed Therapy, Memscaps, pillboxes and pill charts, human help, ask the pharmaceutical companies for tools/devices.
2. What have participants’ experiences been with cuing devices? What works, what doesn’t?
60

i. Ensuring quality services (5 minutes)
i. Quality improvement indicators should include medical markers.
1. Does the organization’s quality improvement program capture health management? If so, how? And if not, what are some suggestions for change?
2. Client satisfaction surveys can be helpful.
61

APPE
ND
IX B
Selected Bibliography & Internet Resources
AIDS Info (HIV/AIDS drug and treatment information) http://www.aidsinfo.nih.gov/drugs/
American Foundation for HIV/AIDS Research. (n.d.) The amfAR treatment insider. Retrieved June 30, 2003 from http://www.amfar.org/cgi-bin/iowa/td/index.html
Bailey House, Inc. and Columbia University Joseph Mail School of Public Health. (2000, October). Housing, health and wellness study: Final report. New York, NY: Author.
Bangsberg, D., Tulsky, J. P., Hecht, F. M., & Moss, A. R. (1997). Protease inhibitors in the homeless. Journal of the American Medication Association, 278(1), 63-65.
Catz, S. L., Kelly, J. A., Bogart, L. M., Benotsch, E. G., & McAuliffe, T. L. (2002). Patterns, correlates, and barriers to medication adherence among persons prescribed new treatments for HIV disease. Health Psychology, 19(2), 124-133.
Center for AIDS Prevention Studies (CAPS) Self-reported adherence to medications instruments. Retrieved June 30, 2003 from http://www.caps.ucsf.edu/projects/instrumentindex.ht ml
62

Center for HIV Identification, Prevention, and Treatment Services (adherence assessment tools). Retrieved July 2, 2003 from http://chipts.ucla.edu/index.html
Gay Men’s Health Crisis. (n.d.). Treatment Issues [Newsletter]. Retrieved June 30, 2003 from http://www.gmhc.org/living/treatment/ti.html
Gilden, Dave. (2001, April). The conference of our discon-tent. The amfAR Treatment Insider, 2(2), 1-4. Retrieved June 30, 2003 from http://199.105.91.6/TREATMENT/HIV+/March01.P DF
Gray, L., Edmondson, E., & Lemke, A. L. (1998, October). HIV treatment adherence: A guide for program development. Seattle, Washington: University of Washington, School of Social Work, HIV/AIDS Project Development and Evaluation Unit.
HIV/AIDS at 20: Special Report. (2001, June 11). Newsweek [Magazine].
HIV/AIDS Treatment Information Service. Guidelines for the Use of Antiretroviral Agents in HIV-Infected Adults and Adolescents. Retrieved June 30, 2003 http://www.aidsinfo.nih.gov/
Kalichman, S., C., Ramachandran, B., & Catz, S. (1999). Adherence to combination antiretroviral therapies in HIV patients of low health literacy. Journal of General Internal Medicine, 14(5), 267-273.
LPI Publications. (n.d.). HIV Plus: Research + Treatment + Life [Magazine]. Los Angeles, CA. Retrieved June 30, 2003 from www.hivplusmag.com
63

National Library of Medicine Drug Information (medication information). Retrieved June 30, 2003 from http://www.nlm.nih.gov/medlineplus/druginforma-tion.html
New York State Department of Health AIDS Institute. Educational slide presentations. Retrieved June 30, 2003 from http://www.hivguidelines.org/public_html/center/clini cal-education/education-slide-presentations/educ_slide_pres.htm
New York State Department of Health AIDS Institute. (2000). Promoting GYN CARE for HIV-infected women: Best practices from New York State. Retrieved June 30, 2003 from http://www.hivguide-lines.org/public_html/center/best-practices/best-prac-tices.shtml
New York State Department of Health AIDS Institute. (2001, June.) Promoting adherence to HIV antiretro-viral therapy. Retrieved June 30, 2003 from http://www.hivguidelines.org/public_html/center/best -practices/best-practices.shtml
Paterson, D. L., Swindells, S., Mohr, J., Brester, M., Vergis, E. N., Squier, C., et al. (2001). Adherence to pro-tease inhibitor therapy and outcomes in patients with HIV infection. Annals of Internal Medicine, 134(7), 625.
64

Treatment Action Group (TAG) http://www.aidsinfonyc.org/tag/
U. S. Department of Health and Human Services. (2001). A guide to the clinical care of women with HIV. Retrieved June 30, 2003 from http://www.hab.hrsa.gov/publications/womencare. htm
U.S. Food & Drug Administration/Center for Drug Evaluation and Research Consumer Drug Information (drug information). Retrieved June 30, 2003 from http://www.fda.gov/cder/consumerinfo/default.htm
Waters, M., Hoos, D., Agins, B. D., Savicki, K. S., Glaros, R., Devore, B. S., et al. (1998). Service delivery models for treatment adherence to combination anti-retroviral therapy. Abstract presented at the International Conference on HIV/AIDS. Retrieved June 30, 2003 from http://www.aegis.org/pubs/HIV/AIDSline/1998/dec/ m98c3517.html
Weidle, P. J., Ganera, C. E., Irwin, K. L, McGowan, J. P., Olivo, N., et al. (1999). Adherence to antiretroviral medications in an inner-city population. Journal of Acquired Immune Deficiency Syndromes, 22(5), 498-502.
65
APPE
ND
IX C
Adherence Assessment/Evaluation Tool*
Date:___________(DD/MM/YY)
MR#:_____________
This tool is to help in the assessment process dur-ing the adherence counseling session, as well as to collect data to evaluate the HIV medication adherence program and gain insight into adher-ence rates and reasons for poor adherence.
PART I.
I’d next like to ask you some questions to help us under stand your experience with the HIV medications you are taking.
Most people with HIV have many pills to take at different times during the day. Many people find it hard to always remember their pills.
We need to understand how people with HIV are really tak-ing their pills. Please tell us what you are actually doing. Do not worry about telling us that you do not take all of your pills. We need to know what is really happening, not what you think we “want to hear.”
66

Name of # of # of antiretrovi- pills times ral drugs taken per day
each
How many doses did you miss...
(doses Day before 3 daysYesterday time per day) yesterday ago(pills
each dose)
67

Ask the following questions only if there were no missed doses from the above table. Otherwise, skip to next ques-tion.
How many times did you miss a dose in the last.....
Week? _____
Month? _____
3 months? _____
The last missed does was more than three months ago
Never skipped medication
PART II.
Reasons for missing doses:
Please tell me how often you missed taking your medications because of each of the following reasons. This is not just in the last 3 days, but generally speaking. (Check one response for each question)
Never Sometimes Often Taking pills didn’t fit into your daily routine?
Simply forgot Too hard to take so many pills according to a schedule?
Wanted to avoid side effects?
68
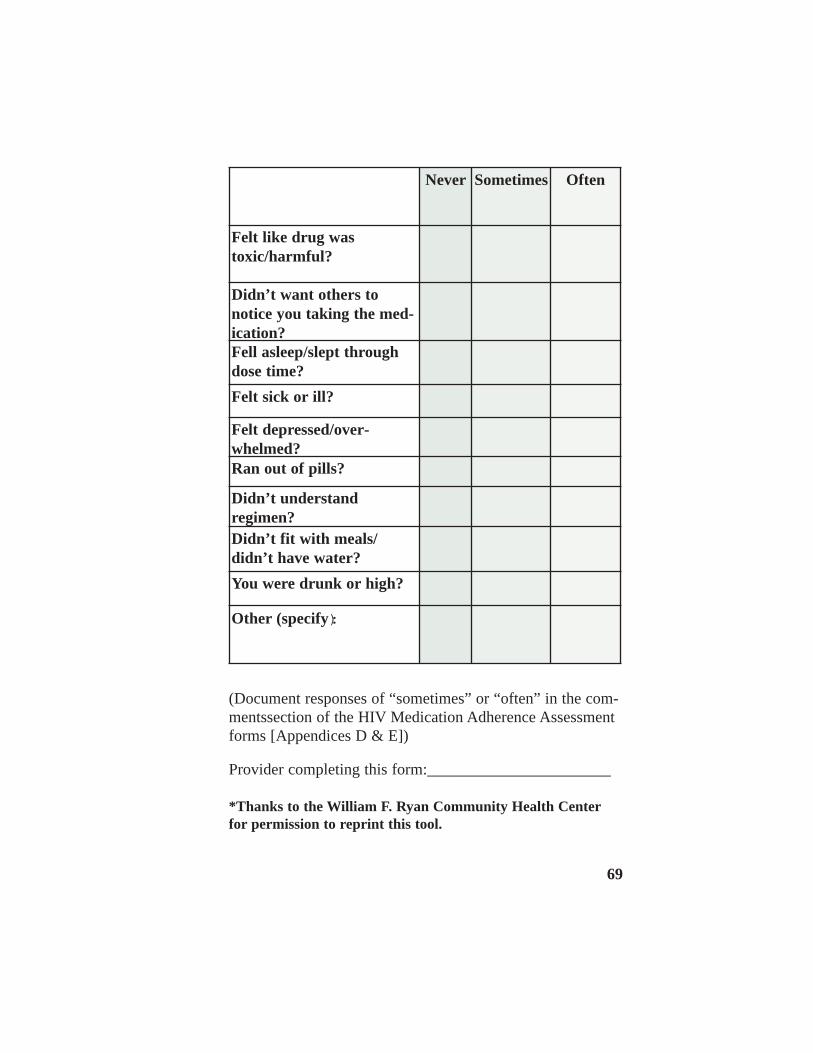
Never Sometimes Often
Felt like drug was toxic/harmful?
Didn’t want others to notice you taking the med-ication? Fell asleep/slept through dose time? Felt sick or ill?
Felt depressed/over-whelmed? Ran out of pills?
Didn’t understand regimen? Didn’t fit with meals/ didn’t have water? You were drunk or high?
Other (specify):
(Document responses of “sometimes” or “often” in the com-mentssection of the HIV Medication Adherence Assessment forms [Appendices D & E])
Provider completing this form:_______________________
*Thanks to the William F. Ryan Community Health Center for permission to reprint this tool.
69

APPE
ND
IX D
HIV Medical Adherence Assessment Initial Visit*
Date:
CLINICAL HISTORY (from review of patient’s medical record & interview)
Date of HIV diagnosis:__________(DD/MM/YY)
Current Antiretroviral Medications (check all that apply)
Date regiment started_______(DD/MM/YY) initial regimen______ salvage regimen________
NRTI PI ___ Abacavir ___ Adefvoir ___ Combivir ___ 3TC ___ Trizivir
__ddC __ddl __d4T __AZT
___Amprena ___Fortovase ___Indinavir ___Invirase
___Nelfinavir ___Ritonavir ___Kaletra
NNRTI
___ Delavirdine ___ Efaviren ___ Nevirapine
Other
___Hydroxyurea
70

Other medications (including OTC)
Prior ART
Dates Reason for D/C
(code)
Key for medication D/C code:
R= Resistance S= Side Effects T= Toxicities O= Other
Demographics
Age_______ Gender M F T
Education Level___________
Housing_________________________________________
Substance Abuse: Active____Non active______
Ethnicity_______________ Occupation/status__________
Risk: ___MSM ___MSF ___FSM ___h/o IVDU
____Other
71

___________________________________________ ___________________________________________ ___________________________________________
___________________________________________ ___________________________________________ ___________________________________________
___________________________________________ ___________________________________________ ___________________________________________
___________________________________________ ___________________________________________ ___________________________________________
___________________________________________ ___________________________________________ ___________________________________________
___________________________________________ ___________________________________________ ___________________________________________
FACTORS THAT MAY IMPACT ADHERENCE (check all completed items)
Assessed the following questions:
“What things in your life are most important to you?”
“What things in your life stress you out the most?”
“Who do you go to when you have problems?”
“What do you think is good/bad about the HIV pills?”
“What have you heard about the HIV pills?”
Other comments:
72

___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________
Adherence assessment/evaluation tool completed (Part I & II if doses missed)
Knowledge of medications (check all items completed):
Reviewed patient’s understanding of goals of therapy and drug resistance and its implications
Reviewed patient’s familiarity with medications, their dose and frequency, food and storage require-ments
Reviewed patient’s knowledge of potential side effects and how to manage the most common of these
Reviewed patient’s knowledge of possible drug inter-actions (including OTC, recreational)
Reviewed procedure for obtaining medication refills and medical care
Comments:
73

___________________________________________ ___________________________________________ ___________________________________________
Adherence treatment plan (check all that apply):
Given written information regarding each medication
Given assistive device(s) [e.g., pocket medication charts, pill boxes, alarms, etc.]
Referral (e.g., case management, mental health, harm reduction)
Follow-up appointment (2,6, 12 weeks & then every 3-4 months or as needed):
Other:
Provider:________________________________________
*Thanks to the William F. Ryan Community Health Center for permission to reprint this tool.
74

HIV Medical Adherence Assessment Follow-up Visit*
Date:______________
Date started regimen:_____________(DD/MM/YY)
Current antiretroviral medications (check all that apply):
APPE
ND
IX E
NRTI PI
___ Abacavir ___ Adefvoir ___ Combivir ___ 3TC ___ Trizivir
__ddC __ddl __d4T __AZT
___Amprena ___Fortovase ___Indinavir ___Invirase ___Nelfinavir ___Ritonavir ___Kaletra
NNRTI
___ Delavirdine ___ Efaviren ___ Nevirapine
Other
___Hydroxyurea
75

___________________________________________
___________________________________________
___________________________________________
CD4 count:______________
Date of test______________ (DD/MM/YY)
Viral load:_______________
Date of test______________ (DD/MM/YY)
Does this represent a change in the antiretroviral medication regimen since the last visit?
No
Yes
Indicate the reason(s) for the change in the medication regi-men:
__ side effects __ non-adherence __ treatment failure
Other____________________________________________
Barriers to Adherence
Comments (from Adherence Assessment Tool)
76

___________________________________________
___________________________________________
___________________________________________
___________________________________________ ___________________________________________ ___________________________________________
Adherence assessment/evaluation tool completed (Part I & II if doses missed)
Knowledge of medications
Comments (from Adherence Assessment Tool)
Adherence treatment plan (check all that apply):
Reviewed information regarding each medication
Given assistive device(s) [e.g., pocket medication charts, pill boxes, alarms, etc.)
Referral (e.g., case management, mental health, harm reduction)
Follow-up appointment (2, 6, 18 weeks & then every 3-4 months or as needed):_________
Other:
Provider:_________________________________________
77
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
_____________________________________________________
PROGRESS NOTES Chart No:
_______________________ Name:
_______________________
_______________________ Address:
_______________________
_______________________ B.D.
*Thanks to the William F. Ryan Community Health Center for permission to reprint this tool.
78

APPE
ND
IX F
Guideline for Initial Client Visit*
Establish trust (on going process) by pro-viding clear communications, rapport, mutual respect, assurance of confidentiality
Introduce adherence program
Identify potential barriers to adherence:
belief’s system stage of treatment readiness physical health emotional health skills prior adherence experience
Assess current situation
Determine treatment category:
-preparing to start medication -starting medication -changing treatment regimens -having difficulty adhering to regimen
Review treatment history:
-general health -substance use -mental health -current medications -known allergies -drug side effects -other treatments used
79

Discuss current health status:
-overall health -current health and social problems -CD4 and viral load results -patient goals for his/her health
Establish a treatment plan
Describe and discuss proposed new regimen Document treatment plan Discuss potential side effects and a plan for Response including prescription Give written information on drugs, includingnames, dosing, frequency, food, and storage requirements
Support and maintenance
Follow-up plan, including whom the clientcan contact with questions
Determine how to stay in contact with theclient until the next appointment Schedule the next appointment
*Reprinted with permission from the NYS Department of Health HIV/AIDS Institute’s Promoting Adherence To HIV Antiretroviral Therapy and from the author agency, Village Center for Care.
80

APPE
ND
IX G
On an ADAP Waiting List? Advice from Treatment Activists
by Kate Krauss
AIDS treatment activists submitted these suggestions during the writing of the story on the current ADAP funding crisis ("Thousands Face Loss of Treatment in ADAP Money Crisis," AIDS Treatment News (June 2002).
1. Sign up for the ADAP waiting list, don't just walk away. Make sure that you keep in touch with your case manager so that he or she can find you when it's your turn.
2. No matter how upset and frus-trated you feel, do not drop out of care.
3. Remember that people who are newly diagnosed with HIV are not supposed to start multi-drug ther-apy until they have fewer than 350 CD4 cells you may not need to start your treatment regimen yet.
81
4. Push your physician or case manager to enroll you in patient assistance programs. These are drug company programs that pro-vide medications for low-income people who cannot obtain drugs through another source. A savvy doctor's office manager or case manager should fill out the paperwork. If you need advice on this, call Project Inform's treatment hotline: 800-822-7422 (toll-free in the United States) or 415-558-9051 (in the San Francisco Bay Area or internationally). Hotline hours are Monday-Friday, 9am-5pm and Saturday, 10am-4pm (Pacific Time). For a directory of patient assistance programs, see http://phrma.og/searchcures/dpdpap/ or call (800) 762-4636 for a copy. The directory is organized by drug company name.
5. Some clinics keep stashes of AIDS medications for people like you; some PWAs may operate a commu nity "medicine chest" of free, unused medications. Ask around in support groups. Visit AIDS clinics and explain your situation -- discreetly. Get out the word that you are stuck and you need help. Remember, though, that interrupting antiviral therapy maybe worse than waiting to begin.
6. Find out if your community has an emergency med-ication fund.
7. Check to see if you qualify for Medicaid.
82
8. Document your situation and distribute the information to AIDS law organizations and other advocates. It will give them ammuni-tion to fight for funding. Offer to tell your story to legislators or other officials.
9. Join an advocacy group (see the list in the associated article). Learn how to lobby and write letters to the editor. Then do it. There is power in numbers.
Plan carefully before you move to another state -- ADAP for-mularies vary widely from state to state, and some don't even cover antiviral drugs. Some states require a six-month wait before you can access benefits. Some ADAPS may have a waiting list. Call local AIDS organizations and people with AIDS to get current information -- before you move.
83

APPE
ND
IX H
Medication Reminder Resources
ALRT offers a multitude of medication reminder tools. Visit http://www.alrt.com, [email protected], 336.722.2254.
Clock and Watch Reminders:
The Invisible Clock, http://www.invisible clock.com, 1.888-602-2588 (toll free) Cadex (watch), http://www.cadexproducts .com, 1.888.726.8805 (toll free)
e-pill offers a multitude of medication reminder tools. Visit http://www.empill.com, 1.800.549.0095 (toll free)
MedReminder is a pager system. For information, contact http://www.medreminder.com, 1.887.236.3901 (toll free).
Medication Monitoring Bottle Caps medication bottles that record the time and date the bottle is opened. To get more information on this tool, visit http://www.aardex.ch or call 1.877.227.3391 or 1.510.476.1940.
On-Time Rx is medication reminder for people that have a Palm OS. For more information, go to http://www.ontimerx.com or call 1.888-383-8688 (toll free).
PageMinder is a pager system that reminds individuals when and how to take their medication schedule. To get more information, go to http://www.pageminderinc.com or call 1.888.882.7787 (toll free).
84

APPE
ND
IX I
About Bailey House & TAPE
Bailey House, Inc., was founded in 1983 by clergy, gay and lesbian community activists and business people in the West Village, the New York City neigh-borhood then most devastated by AIDS. In the early years, when we were known as the AIDS Resource Center, our mission was simple: to give people with AIDS a place to live and die with dignity. That mis-sion has evolved to keep pace with the epidemic and the changing needs of people infected with and affect-ed by HIV. Bailey House’s commitment now is to empower people living with HIV/AIDS, their loved ones and the communities and agencies that serve them to operate at their fullest potential through the development and provision of housing and supportive services.
As the country’s first provider of scattered site housing to people with HIV/AIDS, we have expertise in supportive housing that we now share with HIV/AIDS service providers through our Technical Assistance and Program Evaluation (TAPE) Department. TAPE was initiated in 1993 and since then it has grown into a 16-person department. TAPE’s mis-sion is to support the development and expression of the high-est quality supportive housing and services for people living with HIV/AIDS in the most affected community in New York City and nationally. TAPE is dedicated to transferring resources, knowledge and power to organizations led by and serving communities of color hardest hit by the HIV/AIDS epidemic.
85

TAPE offers HIV/AIDS housing and housing support service providers a wide range of integrated capacity building techni-cal assistance that includes trainings and direct technical assistance.
TAPE assists agencies with developing AIDS supportive housing programs, including identifying potential funding sources, connecting with the federal Continuum of Care and Consolidated Planning process, construction of appropriate service models, organizational development and establishing collaborative arrangements.
TAPE has six program areas:
AIDS Service Organization Management Institute (ASOMI) ASOMI provides an integrated curriculum of training and direct technical assistance to the leaders of organizations that provide HIV/AIDS services and are run by and for people of color. ASOMI helps organizations build capacity in core management areas including human resources, board devel-opment, fundraising, marketing, and program design and pro-gram evaluations. The ASOMI core program includes a 3 1/2 month-long semester of seminars, one-to-one technical assis-tance appropriate to each organizations stage of growth, spe-cialized work plan development, customized information and referral, and organizational stipends for specific capacity building needs.
Fiscal Infrastructure Services Fiscal Infrastructure Services provides technical assistance to HIV/AIDS housing and services provider organizations in designing, developing and implementing high quality fiscal infrastructure systems.
86

Fiscal Infrastructure Services specializes in reviews of inter-nal controls, fiscal policies and procedures, budgeting, con-tract management, cash flow processes, payroll and prepara-tion for annual financial audits.
Housing Services and Operations Programs Housing Services and Operation help agencies develop and expand HIV/AIDS housing programs and strengthen and improve their property management, operations and support-ive services delivery systems. Services include direct techni-cal assistance to programs; the publishing of manuals, direc-tories and other resources that provide guidance and informa-tion to agencies; and workshops targeting clinical services, independent living skills and operations. Housing Services and Operation is comprised of four areas: the Clinical Staff Training Institute, the Operations Resource Center, the ILS Training Program and resource development.
Human Resources Technical Assistance Program (HR TA) Human Resources Technical Assistance provides TA training and one-to-one assistance in human resource management. Additionally, the HR TA Program offer conflict resolution services.
Permanent Housing and Special Efforts for Subpopulation Technical Assistance Program (PHASES-TA) Permanent Housing and Special Efforts for Subpopulation Technical Assistance helps to improve and expand the hous-ing and services for homeless people by increasing the capac-ity of grass-roots faith- and community based organizations; supporting them through free hands-on technical assistance, regional group trainings and resource dissemination.
87

Program Evaluation Services (PES) Program Evaluation Services provides capacity building tech-nical assistance to HIV/AIDS organizations to design and implement appropriate outcome-based program evaluation. Services include identification of outcome measures, design and modification of data collection systems, analysis and interpretation of outcome data and support to program staff in maintaining evaluations systems through hands-on support and group training.
Technical Assistance Clearinghouse (TAC) TAC (www.taclearinghouse.org) is a free website that pro-vides relevant, comprehensive and useful information and access to resources to local organizations doing HIV/AIDS work. It offers a searchable database of New York-area con-sultants and technical assistance providers and information on trainings, websites and publications that address organiza-tional and program development. A TAC section for people living with HIV/AIDS gives up-to-date information on opportunities for training and community involvement plus access to the internet’s many sources of information.
TAPE Publications Available in hard-copy or on www.baileyhouse.org or through www.taclearinghouse.org
New York City HIV/AIDS Housing Resource Book (2002)
New York City HIV/AIDS housing resource database (www.hivhousingnyc.org)
New York State HIV/AIDS Housing Resource Book (2003)
88

New York State HIV/AIDS housing resource database (www.hivhousingnys.org)
Successfully Creating Community Advisory Boards: A Manual for HIV/AIDS Housing and Service Programs (2002)
The Operations Manager’s Workbook (2003)
Getting the Help your Organization Needs: A Guide to Technical Assistance for New York AIDS Service Providers (2003)
Fighting Mold: A Guide for Staff of HIV/AIDS Supportive Housing (2004)
89