supplement 2: progress in hypertension control || errors in assessment of blood pressure: patient...
TRANSCRIPT

Errors in Assessment of Blood Pressure: Patient FactorsAuthor(s): Norman R.C. Campbell, Donald. W. McKay, Arun Chockalingam and J George FodorSource: Canadian Journal of Public Health / Revue Canadienne de Sante'e Publique, Vol. 85,SUPPLEMENT 2: Progress in Hypertension Control (SEPTEMBER / OCTOBER 1994), pp. S12-S17Published by: Canadian Public Health AssociationStable URL: http://www.jstor.org/stable/41991194 .
Accessed: 17/06/2014 06:59
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
Canadian Public Health Association is collaborating with JSTOR to digitize, preserve and extend access toCanadian Journal of Public Health / Revue Canadienne de Sante'e Publique.
http://www.jstor.org
This content downloaded from 195.34.79.253 on Tue, 17 Jun 2014 06:59:04 AMAll use subject to JSTOR Terms and Conditions
ABSTRACT
This article reviews patient-related factors affecting blood pressure measurement and provides the scientific rationale underlying current recommendations for the measure- ment of blood pressure in the evaluation of hypertension. Information is included on the magnitude of errors that can occur when the recommendations are not followed. A variety of factors relating to the patient's emotions, activity, bodily function and environment cause blood pressure to fluctuate throughout the day such that peak systolic and diastolic blood pressures are often twice as high as trough levels. Many physicians fail to account for these factors when assessing a patient's blood pressure. Errors in the classi- fication and treatment of a patient's blood pressure and the finding of labile blood pres- sure can occur often when patients are not adequately prepared in advance of the blood pressure measurement.
ABRÉGÉ
Cet article examine les facteurs associés aux patients qui influencent la mesure de la tension artérielle et présente les raisons scien- tifiques à la base des recommandations pour la mesure de la tension artérielle dans l'évalu- ation de l'hypertension. On y trouvera des données sur l'importance des erreurs qui peuvent survenir lorsque les recommanda- tions ne sont pas suivies. Une variété de fac- teurs ayant trait à l'émotivité du patient, à son activité, au fonctionnement de son corps et à son environnement amène des fluctua- tions de la tension artérielle au cours de la journée qui sont telles que les pressions artérielles diastolique et systolique maximales sont souvent deux fois plus élevées que les niveaux minimaux. De nombreux médecins oublient de prendre en compte ces facteurs quand ils évaluent la tension artérielle d'un patient. Des erreurs de classification et de traitement de la tension artérielle d'un patient ainsi que de la tension artérielle labile peuvent survenir lorsque les patients ne sont pas convenablement préparés à l'avance à la mesure de la pression artérielle.
Errors in Assessment of Blood
Pressure: Patient Factors
Norman R.C. Campbell, MD, frcp(C),' Donald. W. McKay, PhD,2 Arun Chockalingam, PhD,3 J George Fodor, MD, FRCP(C), PhD3
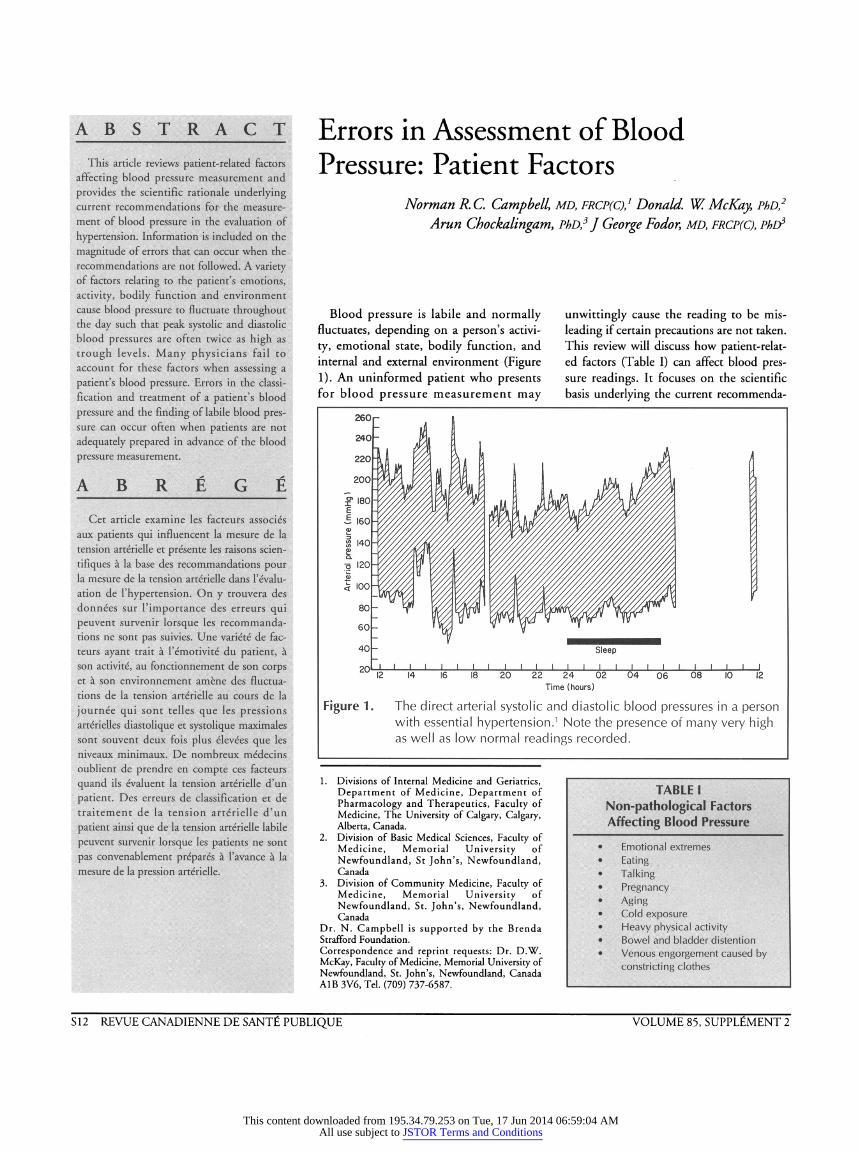
Blood pressure is labile and normally fluctuates, depending on a person's activi- ty, emotional state, bodily function, and internal and external environment (Figure 1). An uninformed patient who presents for blood pressure measurement may
unwittingly cause the reading to be mis- leading if certain precautions are not taken. This review will discuss how patient-relat- ed factors (Table I) can affect blood pres- sure readings. It focuses on the scientific basis underlying the current recommenda-
Figure 1. The direct arterial systolic and diastolic blood pressures in a person with essential hypertension.1 Note the presence of many very high as well as low normal readings recorded.
1. Divisions of Internal Medicine and Geriatrics, Department of Medicine, Department of Pharmacology and Therapeutics, Faculty of Medicine, The University of Calgary, Calgary, Alberta, Canada.
2. Division of Basic Medical Sciences, Faculty of Medicine, Memorial University of Newfoundland, St John's, Newfoundland, Canada
3. Division of Community Medicine, Faculty of Medicine, Memorial University of Newfoundland, St. John's, Newfoundland, Canada
Dr. N. Campbell is supported by the Brenda Strafford Foundation. Correspondence and reprint requests: Dr. D.W. McKay, Faculty of Medicine, Memorial University of Newfoundland, St. John's, Newfoundland, Canada A1B 3V6, Tel. (709) 737-6587.
TABLE I Non-pathological Factors Affecting Blood Pressure
• Emotional extremes • Eating • Talking • Pregnancy • Aging • Cold exposure • Heavy physical activity • Bowel and bladder distention • Venous engorgement caused by
constricting clothes
S12 REVUE CANADIENNE DE SANTÉ PUBLIQUE VOLUME 85, SUPPLÉMENT 2
This content downloaded from 195.34.79.253 on Tue, 17 Jun 2014 06:59:04 AMAll use subject to JSTOR Terms and Conditions

ERRORS IN ASSESSMENT OF BLOOD PRESSURE: PATIENT FACTORS
tions for blood pressure measurement2"4 and where appropriate indicates the mag- nitude of error that can arise when patient factors are ignored. Suitable guidelines for patient preparation can be found in a pre- vious publication.5
Daily Living Stresses Even seemingly mundane tasks can
cause blood pressure increases in most individuals.6'9 The degree to which stressors increase blood pressure is not predictable but is in general related to the type and severity of the stimulus.10 Individuals show considerable variability in blood pressure responses to a given stressor. The following are a variety of day-to-day activities provid- ed to indicate typical changes in blood pressure: performance of mental arithmetic produces an average increase of 6 to 12 mm Hg in systolic and diastolic blood pressure both in normotensive and hyper- tensive individuals;11 just speaking on the telephone causes an average increase in blood pressure of 10/7 mm Hg; merely talking results in a 7/7 mm Hg increase;12 and feelings of anger and to a lesser extent happiness are associated with significant increases in blood pressure.13,14 It is recom- mended that patients rest for at least five minutes in a quiet, comfortable room before blood pressure measurement in order to allow time for physical and emo- tional stresses to settle.2,5 Some patients may require a longer rest.5
Many individuals have increased blood pressure while they are at their place of work.15 Work place blood pressures have been found to correlate slightly better than clinic readings with the presence of hyperten- sive target-organ damage. Patients in whom blood pressures are found to be elevated at work but normal at other times need close examination and thorough investigation for target-organ damage. Ambulatory blood pressure monitoring for 24 hours on a work day may help assess the usual blood pressure level. Likewise, in patients who have normal blood pressure in the clinic but who have evi- dence of left ventricular hypertrophy of unknown etiology or hypertensive vascular damage, ambulatory monitoring or measure- ments at their place of work will provide additional information with which to guide antihypertensive therapy.
Exercise Physical exertion causes significant
changes in arterial pressure. The increases in blood pressure can be considerable and depend on the individual as well as the level and type of exercise.9,16 After exercise, systolic and diastolic blood pressures drop substantially, by 1 8 to 20 mm Hg and 7 to 9 mm Hg, respectively.17 The post-exercise decrease in blood pressure can persist for much longer than one hour.17 20 During and following exercise the auscultatory method of determining blood pressure is inaccurate, and errors of up to 30 mm Hg have been reported. The changes in blood pressure following exercise are related to both technical error9 and to physiological change9,17 Therefore, the assessment of blood pressure for the presence of hyper- tension during or following heavy physical activity will not accurately assess basal blood pressure levels.
Bowel and Bladder Distension The effect of bowel and bladder distention
in otherwise well hypertensive patients has not been completely investigated. Although bladder distension has been shown to increase blood pressure using certain animal models,21 little change in blood pressure has been noted when patients micturate freely.21 If the bladder is uncomfortably distended, increases in blood pressure up to 50/40 mm Hg can occur.21 Pathological distension of the bladder due to prostatic hypertrophy in elderly men is a common cause of reversible and severe hypertension.22 Bowel and blad- der distension can also cause severe and inju- rious elevation of blood pressure in patients with uninhibited spinal sympathetic reflexes.23,24 The aforementioned factors have led to the recommendation that the bowel and bladder be emptied prior to determina- tion of basal blood pressure.
Meals Reductions in systolic and diastolic
blood pressure follow the ingestion of meals.25 28 The decreases are modest in younger patients,26 but in the elderly can exceed 20 mm Hg and be maintained for longer than one hour.26"28 Blood pressure measurement is not recommended within half an hour of eating,2,5 and a longer wait in elderly patients is prudent.
TABLE II Nonprescribed
Medications/Substances Causing Acute or Chronic Increases in Blood
Pressure • Nicotine • Licorice • Phenylpropanolamine and other
over-the-counter sympathomimet- ics
• Amphetamines • Cocaine • Alcohol • Nonsteroidal anti-inflammatory
agents • Caffeine • Tyramine-containing foods in
patients who are taking monoamine oxidase inhibitors
Over-The-Counter Vasopressors A variety of substances (Table II) have
been reported to cause blood pressure ele- vation. The increases in blood pressure may be substantial in some patients, whereas little blood pressure change is seen in other patients.29 Some substances (e.g., sympathomimetics as found in many nasal decongestants) elevate blood pressure acutely and have no chronic effects29 while other substances (e.g., licorice) can cause sustained elevations in blood pressure that persist after the substance is ingested. Physicians are often not aware that patients are using over-the-counter pressor agents, and this lack of information can result in the false impression that the patient has primary hypertension.
Alcohol Alcohol has a complex effect on blood
pressure. An acute reduction in blood pres- sure lasting up to eight hours was found following alcohol ingestion by habitual Japanese drinkers30 while 'sustained' blood pressure elevation is seen when alcohol is habitually ingested in quantities in excess of one ounce of alcohol per day.31 Unfortunately, the 24-hour blood pressure response to alcohol ingestion has not been documented in many studies, and an acute vasodepressor effect of alcohol cannot be ruled out in chronic drinkers.
Caffeine Chronic ingestion of caffeine results in
little change in blood pressure.32 However, in many patients who are not accustomed to caffeine or who have
SEPTEMBER - OCTOBER 1994 CANADIAN JOURNAL OF PUBLIC HEALTH - SUPPLEMENT 2 S13
This content downloaded from 195.34.79.253 on Tue, 17 Jun 2014 06:59:04 AMAll use subject to JSTOR Terms and Conditions
ERRORS IN ASSESSMENT OF BLOOD PRESSURE: PATIENT FACTORS
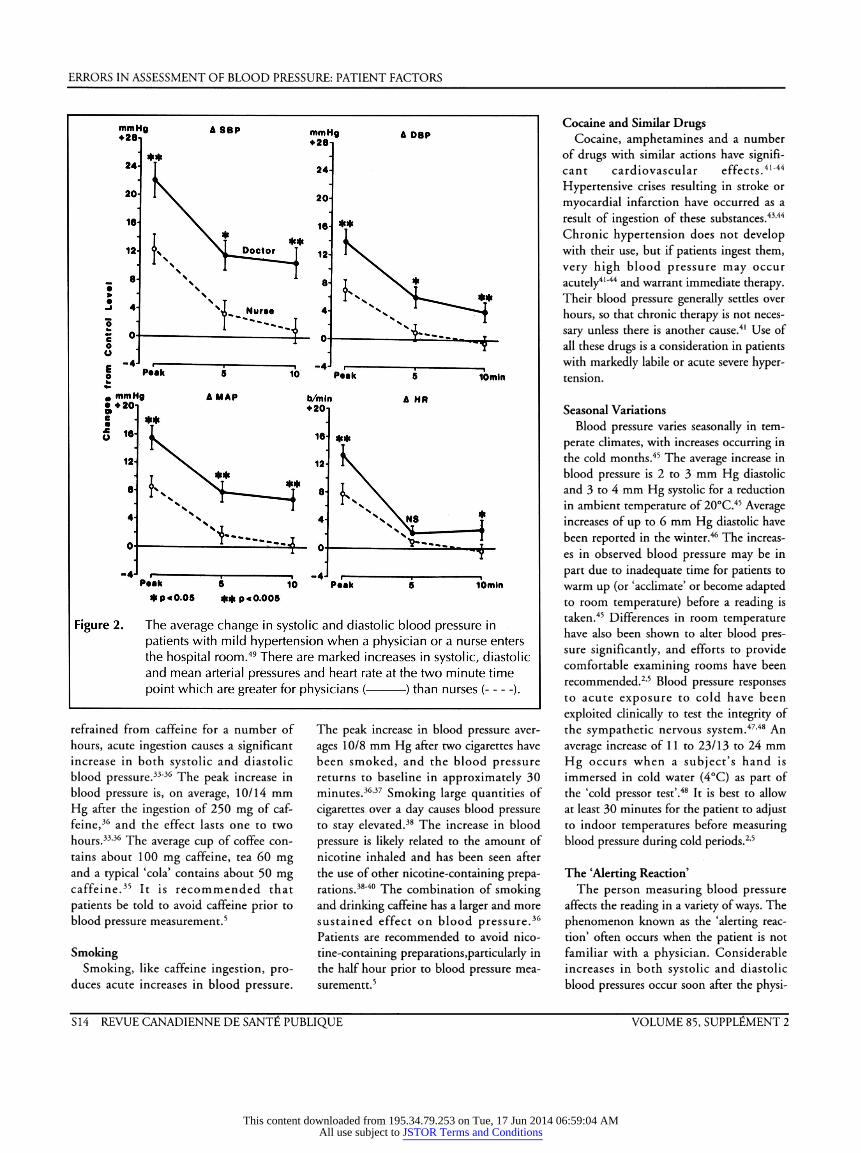
Figure 2. The average change in systolic and diastolic blood pressure in patients with mild hypertension when a physician or a nurse enters the hospital room.49 There are marked increases in systolic, diastolic and mean arterial pressures and heart rate at the two minute time point which are greater for physicians ( ) than nurses ( ).
refrained from caffeine for a number of hours, acute ingestion causes a significant increase in both systolic and diastolic blood pressure.33'36 The peak increase in blood pressure is, on average, 10/14 mm Hg after the ingestion of 250 mg of caf- feine,36 and the effect lasts one to two hours.33'36 The average cup of coffee con- tains about 100 mg caffeine, tea 60 mg and a typical 'cola' contains about 50 mg caffeine.35 It is recommended that patients be told to avoid caffeine prior to blood pressure measurement.5
Smoking Smoking, like caffeine ingestion, pro-
duces acute increases in blood pressure.
The peak increase in blood pressure aver- ages 10/8 mm Hg after two cigarettes have been smoked, and the blood pressure returns to baseline in approximately 30 minutes.36,37 Smoking large quantities of cigarettes over a day causes blood pressure to stay elevated.38 The increase in blood pressure is likely related to the amount of nicotine inhaled and has been seen after the use of other nicotine-containing prepa- rations.38"40 The combination of smoking and drinking caffeine has a larger and more sustained effect on blood pressure.36 Patients are recommended to avoid nico- tine-containing preparations, particularly in the half hour prior to blood pressure mea- surementt.5
Cocaine and Similar Drugs Cocaine, amphetamines and a number
of drugs with similar actions have signifi- cant cardiovascular effects.41"44 Hypertensive crises resulting in stroke or myocardial infarction have occurred as a result of ingestion of these substances.43,44 Chronic hypertension does not develop with their use, but if patients ingest them, very high blood pressure may occur acutely41"44 and warrant immediate therapy. Their blood pressure generally settles over hours, so that chronic therapy is not neces- sary unless there is another cause.41 Use of all these drugs is a consideration in patients with markedly labile or acute severe hyper- tension.
Seasonal Variations Blood pressure varies seasonally in tem-
perate climates, with increases occurring in the cold months.45 The average increase in blood pressure is 2 to 3 mm Hg diastolic and 3 to 4 mm Hg systolic for a reduction in ambient temperature of 20°C.45 Average increases of up to 6 mm Hg diastolic have been reported in the winter.46 The increas- es in observed blood pressure may be in part due to inadequate time for patients to warm up (or 'acclimate' or become adapted to room temperature) before a reading is taken.45 Differences in room temperature have also been shown to alter blood pres- sure significantly, and efforts to provide comfortable examining rooms have been recommended.2,5 Blood pressure responses to acute exposure to cold have been exploited clinically to test the integrity of the sympathetic nervous system.47'48 An average increase of 1 1 to 23/ 1 3 to 24 mm Hg occurs when a subject's hand is immersed in cold water (4°C) as part of the 'cold pressor test'.48 It is best to allow at least 30 minutes for the patient to adjust to indoor temperatures before measuring blood pressure during cold periods.2'5
The 'Alerting Reaction' The person measuring blood pressure
affects the reading in a variety of ways. The phenomenon known as the 'alerting reac- tion' often occurs when the patient is not familiar with a physician. Considerable increases in both systolic and diastolic blood pressures occur soon after the physi-
S 14 REVUE CANADIENNE DE SANTÉ PUBLIQUE VOLUME 85, SUPPLÉMENT 2
This content downloaded from 195.34.79.253 on Tue, 17 Jun 2014 06:59:04 AMAll use subject to JSTOR Terms and Conditions

ERRORS IN ASSESSMENT OF BLOOD PRESSURE: PATIENT FACTORS
cian enters the room. Physician-provoked peak increases average 30/18 mm Hg, and nurses have a less pronounced effect.49 The blood pressure increase is partially attenu- ated after five minutes (average increase of 8/3 mm Hg), but further blood pressure reductions may not occur by waiting as long as 10 minutes between measurements (Figure 2). The increases in blood pressure ascribed to the alerting reaction can occur during repeated visits over a short period,49 but they subside when the patient sees the physician on a regular basis.50'51 Several studies have shown large reductions in blood pressure over three to six months during observation or placebo treatment; this is likely due to attenuation of the alert- ing reaction as patients become accus- tomed to the study and its personnel. The diagnosis of hypertension requires several visits over a period of three to six months in patients who have mildly elevated blood pressures. Because of the attenuated alert- ing reaction some experts have suggested that nurses rather than physicians should measure blood pressure.52 The results of recent studies also suggest that sex differ- ences between the patient and measurer may affect blood pressure.53
'White Coat Hypertension' The recently popularized 'white coat
phenomenon' has been known for a num- ber of decades.54 Although some people do not distinguish between the alerting reac- tion and the white coat phenomenon, the former wanes after several visits whereas the latter is provoked by the physician and is persistent over time.3,55 Approximately 20% of patients with diastolic blood pressure of 90 to 104 and approximately 5% of patients with diastolic blood pressure greater than 104 mm Hg when assessed by a physician will have 24-hour ambulatory diastolic blood pressure below 85 mm Hg.56 The increases in blood pressure can be greater in some individuals with white coat hypertension. Many investigators fail to distinguish the alerting reaction from white coat hypertension in their studies, and this has likely inflated current estimates of the incidence of white coat hypertension. The presence of white coat hypertension can be suspected in patients who have no hypertensive damage, who have hypoten-
sive symptoms with therapy despite repeat- edly normal or high clinic readings, and in whom blood pressure readings at home are substantially lower than the clinic readings. White coat hypertension occurs when the degree of hypertension cannot be con- firmed by home blood pressure readings or ambulatory monitoring. Of note, some patients will have higher home, office or ambulatory blood pressure readings than those recorded in a physician's office. These patients may be at greater risk for hyperten- sive target-organ damage than indicated by blood pressures obtained in a physician's office.57
Self Measurement Patient self-measured blood pressure
readings are on average lower than those obtained in the office by a physician.54,58 Some investigators have suggested that these home measurements correlate better with 24-hour ambulatory measurements and also with the presence of hypertensive end-organ damage (e.g., left ventricular hypertrophy59"64). However, not all home measurements are reliable or accurate, and some patients selectively report only lower blood pressure readings.65"67 Ambulatory blood pressure monitoring can be per- formed if the reliability of the patient is questionable and there are significant dis- crepancies between clinic and home read- ings. Patients measuring blood pressure at home require supervised training and peri- odic assessment of technique. In motivat- ed, well-trained patients the assessment of home blood pressure readings provides invaluable information in the diagnosis and management of hypertension.
Pregnancy and Menstruation The physiological status of the patient
demands modification of the blood pres- sure measurement in certain circum- stances. Phase IV Korotkoff sounds persist in about 10% of pregnant patients. When this occurs, the point of abrupt muffling of Korotkoff sounds (i.e., phase IV) should be used to estimate diastolic blood pressure, and phase V should be recorded as zero.68 The supine position for blood pressure measurement in pregnant patients is to be avoided, as the gravid uterus can compro- mise venous return to the heart and signifi-
cantly reduce blood pressure readings. Blood pressure measured when the preg- nant woman is in the seated position or lying tilted slightly (15-30°) to her left side avoids this problem.68 Changes in blood pressure have been noted during the men- strual cycle, with slightly higher blood pressures at the start of menstruation and slightly higher blood pressures during the follicular phase compared with the luteal phase.69 These are small changes of ques- tionable clinical significance.
Children The measurement of blood pressure in
the paediatric population also requires some modification.70 In patients aged 13 or older, blood pressure measurement is essen- tially the same as for adults. The disappear- ance of Korotkoff sounds is not as reliable an indicator of diastolic blood pressure as it is in adults, and in many children, Korotkoff sounds can be heard even when no cuff pressure is applied. For this reason it is recommended that the onset of phase IV Korotkoff sounds (i.e., muffling) be used to estimate diastolic blood pressure. In children under the age of three, accurate measurement of blood pressure commonly requires the use of doppler or oscillometric devices rather than auscultatory technique. Even using these devices, diastolic blood pressure measurement can be inaccurate.70 If the measurement of blood pressure by auscultation suggests hypertension or if the child is at risk of hypertension, referral for blood pressure measurement to centres with doppler or oscillometric equipment is advised.70 When measuring the blood pres- sure of a child, it is particularly important that the child be relaxed and rested and that an appropriately sized blood pressure cuff is used.70
Arrhythmias In patients with ongoing arrhythmias
there are problems estimating blood pres- sure because of variation in the blood pres- sure from beat to beat. Changes in phase I and V Korotkoff sounds due to isolated ectopic beats should be ignored.2 In patients with irregular rhythms, several blood pressure measurements need to be taken and averaged to obtain a more accu- rate estimate of blood pressure.
SEPTEMBER - OCTOBER 1 994 CANADIAN JOURNAL OF PUBLIC HEALTH - SUPPLEMENT 2 S 1 5
This content downloaded from 195.34.79.253 on Tue, 17 Jun 2014 06:59:04 AMAll use subject to JSTOR Terms and Conditions

ERRORS IN ASSESSMENT OF BLOOD PRESSURE: PATIENT FACTORS
CONCLUSIONS
Many factors cause marked variation in blood pressure within an individual. A number of situations evoke apprehension in patients, including the presence of an unfamiliar physician, and can cause tem- porary elevations in blood pressure. The responses to these nonspecific stimuli could all be considered 'alerting reactions'. 'Casual' blood pressure measurements fail to account for alerting reactions or other environmental and internal factors that can contribute to fluctuation of blood pressure. Current recommendations to measure blood pressure2"4 attempt to control factors influencing blood pressure and result in a better estimate of basal blood pressure. Education and preparation of patients in advance of their next office blood pressure measurement is essential to obtain mean- ingful readings.
ACKNOWLEDGEMENTS
We thank Dr. P. Magner for reviewing this manuscript and Ms. H. Arcari for her expert secretarial assistance.
REFERENCES: 1. Bevan AT, Honour AJ, Stott FH. Direct arterial
pressure recording in unrestricted man. Clin Sci 1969;36:329-344.
2. Perloff D, Grim C, Flack J, et al. Human blood pressure determination by sphygmomanometry. Circulation 1993; 88:2460-2470.
3. Petrie JC, O'Brien ET, Littler WA, De Swiet M. Recommendations on blood pressure measure- ment. BMJ 1986;293:611-615.
4. American Society of Hypertension. Recommendations for routine blood pressure measurement by indirect cuff syphygmomanome- try. Am J Hypertens 1992;5207-209.
5. Campbell NRC, Chockalingam A, Fodor JG, McKay DW. Accurate, reproducible measure- ment of blood pressure. Can Med Assoc J 1990;143:19-24.
6. Pickering TG. Short term variability of blood pressure, and the effects of physical and mental activity. In: Pickering TG, ed. Ambulatory Monitoring and Blood Pressure Variability. London UK: Science Press; 1991:12.1-12.12.
7. Watson RDS, Stallard TJ, Flinn RM, Littler WA. Factors determining direct arterial pressure and its variability in hypertensive man. Hypertension. 1980;2:333-341.
8. Henschel A, De La Vega F, Taylor HL. Simultaneous direct and indirect blood pressure measurement in man at rest and work. J Appi Physiol 1954;5:506-507.
9. Gould BA, Hornung RS, Altman DG, et al. Indirect measurement of blood pressure during exercise testing can be misleading. Br Heart J 1985;53:611-615.
10. Schmieder R, Ruddel H, Langewitz W, et al. The influ- ence of monotherapy with oxeprenolol and nitrendip- ine on ambulatory blood pressure in hypertensives. Clin ExpHypertens Part A Theory Pract 1985;7:445-454.
11. Nyberg G. Blood pressure and heart rate response to isometric exercise and mental arithmetic in normo tensive and hypertensive subjects. Clin Sci Mol Med 1 976;5 1:681 s-685s.
12. Pickering TG. The influence of daily activity on ambulatory blood pressure. Am Heart J 1988;116:1141-1145.
13. James GD, Yee LS, Harshfield GA, et al. The influence of happiness, anger and anxiety on the blood pressure of borderline hypertensives. Psychosom Med 1986;48:502-508.
14. Schneider RH, Egan BM, Johnson EH, et al. Anger and anxiety in borderline hypertension. Psychosom Med 1986;48:242-248.
15. Schnall PL, Pieper C, Schwartz JE, et al. The relationship between cjob strain', workplace dias- tolic blood pressure, and left ventricular mass index. Results of a case control study. JAMA 1990;263:1929-1935.
16. Henschel A, De La Vega F, Taylor HL. Simultaneous direct and indirect blood pressure measurement in man at rest and work. J Appi Physiol 1954;5:506-507.
17. Kenney MJ, Seals DR. Postexercise hypotension. Key features, mechanisms, and clinical signifi- cance. Hypertension 1993;22:653-664.
18. Somers VK, Conway J, Coats A, et al. Postexercise hypotension is not sustained in nor- mal and hypertensive humans. Hypertension. 1991;18:211-215.
19. Bennett T, Wilcoxon RG, MacDonald IA. Post exercise reduction of blood pressure is not due to impairment of baroreceptor function. Clin Sci 1984;67:97-103.
20. Floras JS, Sinkey CA, Aylward PE, et al. Postexercise hypotension and sympathoinhibition in borderline hypertensive man. Hypertension 1989;14:28-35.
21. Szasz JJG, Whyte HM. Effect of distension of the bladder and of contraction of sphincters on blood pressure. BMJ 1967;2:208-210.
22. Jones DA, O'Reilly PH, George NJR, Barnard RJ. Reversible hypertension associated with unrecognized high pressure chronic retention of urine. Lancet 1987;1:1052-1054.
23. Wurster RD, Randall WC. Cardiovascular respons- es to bladder distension in patients with spinal tran- section. Am J Physiol 1975;228:1288-1292.
24. Naftchi NE, Demeny M, Lowman EW, Tuckman J. Hypertensive crises in quadriplegic patients. Circulation 1978;57:336-341.
25. Ťsuchihashi T, Abe I, Tsukashima A, et al. Effects of meals and physical activity on blood pressure variability in elderly patients. A pre- liminary study. Am J Hypertens 1990;3:943- 946.
26. Jansen RWMM, Penterman BJM, Van Lier HJJ, Hoefnagels WHL. Blood pressure reduction after oral glucose loading its relation to age, blood pressure and insulin. Am J Cardiol 1987;60:1087-1091.
27. Lipsitz LA, Nyquist RP, Wei JY, Rowe JW. Postprandial reduction in blood pressure in the elderly. N Engl J Med 1983-309:81-80.
28. Fagan TC, Conrad KA, Mar JH, Nelson L. Effects of meals on hemodynamics: Implications for antihypertensive drug studies. Clin Pharmacol Ther 1986;39:255-260.
29. Bravo EL. Phenylpropanolamine and other over- the-counter vasoactive compounds. Hypertension (Suppl. II) 1988;1 1:11-7-11-10.
30. Kawano Y, Abe H, Kojima S, et al. Acute depressor effect of alcohol in patients with
essential hypertension. Hypertension 1992;20:219-226.
31. Cooke KM, Frost GW, Stokes GS. Blood pres- sure and its relationship to low levels of alcohol consumption. Clin Exp Pharmacol Physiol 1983;10:229-233.
32. Bertand CA, Pomper I, Hillman G, et al. No relation between coffee and blood pressure. N Engl J Med 1 978;200:3 1 5-3 1 6.
33. Robertson D, Frolich JC, Carr RK. et al. Effects of caffeine on plasma renin activity, cate- cholamines and blood pressure. N Engl J Med 1978;298:181-186.
34. Lane JD. Caffeine and cardiovascular responses to stress. Psychosom Med 1983;45:447-451.
35. Izzo JL, Ghosal A, Kwong T, et al. Age and prior caffeine alter the cardiovascular and adrenomedullary responses to oral caffeine. Am J Cardiol 1983;52:769-773.
36. Freestone S, Ramsay LE. Effect of coffee and cig- arette smoking on the blood pressure of untreat- ed and diuretic-treated hypertensive patients. Am J Med 1982;73:348-353.
37. Cryer PE, Haymond MW, Santiago JV, Shah SD. Norepinephrine and epinephrine release and adrenergic mediation of smoking - associated hemodynamic and metabolic events. N Engl J Med 1976;295:573-577.
38. Groppelli A, Giorgi DMA, Omboni S, et al. Persistent blood pressure increase induced by heavy smoking. J Hypertens 1992;10:495-499.
39. Wells DG, Řustick JM. Hypertension from smokeless tobacco. (Abstract). Anesthesiology 1986;65:339.
40. Morris DJ, Davis E, Latif SA. Licorice, tobacco chewing and hypertension. (Letter) N Engl J Med 1990;332:849.
41. Gay GR, Loper KA. Control of cocaine induced hypertension with labetalol (letter). Anesth Analg 1988;67:92.
42. Fischman MW, Schuster CR. Cocaine self- administration in humans. Fed Proc 1982;41:241-246.
43. Resnick RB, Kestenbaum RS, Schwartz LK. Acute systemic effects of cocaine in man: a con- trolled study by intranasal and intravenous routes. Science 1977;195:696-698.
44. Hoffman BB, Lefkowitz RJ. Catecholamines and sympathomimetic drugs. In: Gilman AG, Rail TW, Nies AS, Taylor P eds. Goodman and Gilman's The Pharmacological Basis of Therapeutics. 8th Ed. New York: Pergamon Press; 1990; 187-220.
45. Brennan PJ, Greenberg G, Miall WE, Thompson SG. Seasonal variation in arterial blood pressure. BMJ 1982;285:919-923.
46. Giaconi S, Palombo C, Genovesi-Ebert A, et al. Long-term reproducibility and evaluation of sea- sonal influences on blood pressure monitoring. J Hypertens 1988;6:64s-66s.
47. Scriven AJI, Brown MJ, Murphy MB, Dollery CT. Changes in blood pressure and plasma cate- cholamines caused by tyramine and cold expo- sure. J Cardiovasc Pharmacol 1984;6:954-960.
48. Wood DL, Shepps SG, Elvebach LR, Schirger A. Cold pressor tests as a predictor of hypertension. Hypertension 1984;6:301-306.
49. Mancia G, Parati G, Pomidossi G, et al. Alerting reaction and rise in blood pressure during mea- surement by physician and nurse. Hypertension 1987;9:209-215.
50. Medical Technology and Practice Patterns Institute. Hypertension: Questions of prevalence, diagnosis and management. J Clin Hypertens 1978;3:757-767.
51. Pearce KA, Grimm RH, Rao S, et al. Population- derived comparisons of ambulatory and office
S 16 REVUE CANADIENNE DE SANTÉ PUBLIQUE VOLUME 85, SUPPLÉMENT 2
This content downloaded from 195.34.79.253 on Tue, 17 Jun 2014 06:59:04 AMAll use subject to JSTOR Terms and Conditions
ERRORS IN ASSESSMENT OF BLOOD PRESSURE: PATIENT FACTORS
blood pressures. Implications for the determina- tion of usual blood pressure and the concept of white coat hypertension. Arch Intern Med 1992;152:750-756.
52. de Blok K, Veerman DP, Hoek F, et al. Relationship between blood pressure, as mea- sured by a nurse, by a doctor and under basal conditions, and microalbuminuria and left ven- tricular ma ss. J Hypertens 1 99 1;9: 106s- 107s.
53. McCubbin JA, Wilson JF, Bruehl S, et al. Gender effects on blood pressure obtained during an on-campus screening. Psychosom Med 1991;53:90-100.
54. Ayman D, Goldshine AD. Blood pressure deter- minations by patients with essential hyperten- sion. I. The difference between clinic and home readings before treatment. Am J Med Sci 1940;200:465-474.
55. Pickering TG. Clinic measurement of blood pres- sure and white coat hypertension. In: Pickering T.G., ed. Ambulatory Monitoring and Blood Pressure Variability. London UK: Science Press; 1991;7.1-7.14.
56. Pickering TG, James GD, Boddie C, et al. How common is whitecoat hypertension? JAMA 1988;259:225-228.
57. Hoegholm A, Kristensen KS, Madsen NH, Svendsen TL. White coat hypertension diagnosed
by 24-h ambulatory monitoring. Examination of 159 newly diagnosed hypertensive patients. Am J Hypertens 1992;5:64-70.
58. Beckman M, Panfilov V, Silvertsson R, et al. Blood pressure and heart rate recordings at home and at the clinic. Acta MedScandWl;2l0:97-l02.
59. Pickering TG. Which measures of blood pressure give the best prediction of target organ damage and prognosis? In: Pickering T.G., ed. Ambulatory Monitoring and Blood Pressure Variability. London UK: Science Press; 1991;13.1-13.15.
60. Ibrahim MM, Tarazi RC, Dustin HP, Gifford RW. Electrocardiogram in the evaluation of resis- tance to antihypertensive therapy. Arch Int Med 1977;137:1125-1129.
61. Sokolow M, Werdegar G, Kain HK, et al Relationship between level of blood pressure measured casually and by portable recorders and severity of complications in essential hyperten- sion. Circulation 1966;34:279-298.
62. Perloff D, Sokolow M, Cowan R The prognostic value of ambulatory blood pressures. JAMA 1983;249:2792-2798.
63. Rowlands DB, Ireland MA, Glover DR, et al. The relationship between ambulatory blood pressure and echocardiographically assessed left ventricular hypertrophy. Clin Sci 1981;6l:101s-103s.
64. Drayer JIM, Weber MA, De Young JL. BP a determinate of cardiac left ventricular muscle mass. Arch Int Med 1983;143:90-92.
65. Vidt DG, Bolen K, Gifford RW, Medendorp SV. The Telelab personal blood pressure transmitter: Accurate and reliable home monitoring for hypertensive patients. Cleve Clin J Med 1991;58:28-32.
66. Bruce NG, Shaper AG, Walker M, Wannamethee G. Observer bias in blood pres- sure studies. J Hypertens 1988;6:375-380.
67. Sheps SG. Finding the right role for home blood pressures. Cleve Clin J Med 1991;58:61-63.
68. Working Group Report. High blood pressure in pregnancy. National High Blood Pressure Education Program (NHBPEP). U.S. Department of Health and Human Services. NIH Publication No. 90-3029. 1990.
69. Dunne FP, Barry DG, Ferriss JB, et al. Changes in blood pressure during the menstrual cycle. Clin Sci 1991;81:515-518.
70. Task Force on Blood Pressure Control in Children. Report of the second Task Force on Blood Pressure Control in Children - 1987. Pediatrics 1987;79:1-25.
SEPTEMBER - OCTOBER 1994 CANADIAN JOURNAL OF PUBLIC HEALTH - SUPPLEMENT 2 S17
This content downloaded from 195.34.79.253 on Tue, 17 Jun 2014 06:59:04 AMAll use subject to JSTOR Terms and Conditions