structuralandfunctionaleffectsofadriamycinoncardiaccellsin...
TRANSCRIPT

[CANCER RESEARCH 40, 3901-3909, November 1980]0008-5472/80/0040-OOOOS02.00
Structural and Functional Effects of Adriamycin on Cardiac Cells inVitro1
Theodore J. Lampidis,21. Craig Henderson, Mervyn Israel, and George P. Canellos
Division of Medical Oncology [T. J. L., I. C. H., G. P. C.Jand Pharmacology ¡M.I ], Sidney Farber Cancer Institute. Harvard Medical School, Boston, Massachusetts02115
ABSTRACT
The effects of Adriamycin (ADR) on the heart, seen clinicallyas transient electrocardiographic changes and cardiomy-
opathy, have been simulated in an in vitro cardiac cell system.Structural and functional alterations in cultured heart cells canbe dissociated based upon ADR dose and length of exposure.At high ADR doses (100 to 200 jug/ml), cessation of beatingwas rapid, and structural changes consistent with the in vivocardiomyopathic picture (vacuolization and nucleolar fragmentation) were observed. At low ADR doses (0.1 to 0.5 /ig/ml),arrhythmias were produced in the absence of ultrastructuralchanges (within 48 hr); the incidence and severity of thearrhythmias were demonstrated to be dose dependent. Continued treatment of cultures at low dose levels for sustainedperiods of time (up to 17 days) resulted in a striking loss ofmuscle fiber without concomitant vacuolization and nucleolarfragmentation. An intermediate ADR dose of 10 jug/ml for 1 hrexposure caused vacuolization and cessation of beating, withlysis of cells within 72 hr. The parallel between the effects ofADR on in vitro cardiac cell structure and function with thoseseen in vivo suggests that this simple system may have valuein studies directed towards the mechanism of ADR-induced
cardiac toxicity and in the screening of anthracycline analogsfor their potential effects on the heart.
INTRODUCTION
While ADR3 is of major importance in the management of a
variety of human neoplasms, its use is known to produce anumber of effects on the heart (4, 5, 7, 12, 22, 27, 34).Electrocardiographic changes, which include abnormalities incardiac rhythm, are transient and are not thought to bear uponthe more serious problem of accumulated dose-dependent
cardiomyopathy (12, 27). Cardiomyopathic changes, whichinclude vacuolization, myofibrillar dropout, disorganization ofZ-bands, and swelling of sarcoplasmic reticulum, have been
noted in patients and laboratory animals treated with ADR (1,6, 9, 16, 22, 40). In humans, this pathology can result inirreversible congestive heart failure and therefore is the limitingfactor in the long-term use of ADR. Despite a number ofinvestigations, the mechanism of this cardiac lesion remainsunknown.
Based upon earlier experiences with mammalian heart cells
1This work was supported in part by Research Grants CA 09172, CA 19118,
and CA 24771 from the National Cancer Institute and by funds provided by AdriaLaboratories. Inc., Columbus, Ohio.
2 To whom requests for reprints should be addressed, at Sidney Farber Cancer
Institute. 44 Binney Street, Boston, Mass. 02115.3 The abbreviations used are: ADR, Adriamycin; MEM, Eagle's minimal essen
tial medium.Received May 5, 1980; accepted July 23, 1980.
in vitro (20), it was thought that this system might be useful instudies on anthracycline-induced cardiac toxicity. Mammalian
heart cells grown in culture maintain their structural integrityand their ability to beat autorhythmically and thus could providea simple in vitro model in which to study the effects of ADR onthe structure and function of these cells. The demonstration ofanthracycline-induced specific changes on heart cells in culture which mimic the effects produced in vivo would allow forthe use of an in vitro model for studies on the mechanism ofcardiac toxicity as well as provide a rapid and inexpensivescreening system for the evaluation of potential cardiac effectsof anthracycline analogs. In the present report, the effects oflow and high doses of ADR on both the beating function andstructure of cultured heart cells are described.
MATERIALS AND METHODS
Establishment of Primary Cultures. Detailed procedures forthe preparation of cardiac cells in culture have been reported(20). In brief, 15 to 20 neonates (24 to 48 hr old) from Sprague-
Dawley rats (Charles River Laboratories, Wilmington, Mass.)were sacrificed by decapitation, and hearts were excised.Ventricles were separated from auricles and minced to serveas the source of cardiac cells. The pooled tissue was seriallytrypsinized. The fourth to seventh supernatants were combined, filtered through gauze, and centrifuged at 1000 rpm for15 min in chilled conical tubes. Pellets were resuspended inMEM supplemented with 10% fetal calf serum, 100 units ofpenicillin, and streptomycin (100 fig/ml), and the suspensionwas adjusted to a density of 2 x 105 cells/ml. Plastic plates
(35 mm diameter) were seeded with 0.1-ml droplets of the cellsuspension, and incubated at 37°(5% CO2-95% air) for 18 hr,
at which time fresh medium (2 ml) was added to each plate.Medium changes were made every 48 hr thereafter. Drugtreatments were begun 7 days after the cells were seeded, atwhich time cultures beat rhythmically and synchronously (seebelow).
Measurements of Beating Rates and Patterns. The electronic monitoring system used to quantitatively measure andrecord the beating patterns of cardiac cultures is illustrated inChart 1. A specially constructed temperature- and pH-con-
trolled microscopic stage (developed by Dr. Steven Hawley,Harvard School of Public Health, Boston, Mass.) was utilizedto maintain the environmental conditions necessary for culturesto beat rhythmically and consistently. In these experiments, allcultures were maintained and monitored in 5% CO2-95% air at37°.The microscopic image of the cells was transmitted onto
a Sanyo Model VM 4155 television screen by means of an RCAModel TC 1005 video camera. A photodiode, which could bemaneuvered to any point on the screen, detected changes inlight intensity resulting from the pulsations of the cells. Each
NOVEMBER 1980 3901
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

T. J. Lampidis et al.
Microscopewith Heatand pH Controlled Stage
Photodiode
Chart 1. Schematic illustration of the electronic system used for monitoringand recording cardiac culture pulsations.
beat was permanently documented by a Grass InstrumentsModel 7 polygraph recorder connected to the photodiodedevice.
Morphological Evaluation. Heart muscle cells were distinguished from nonmuscle cells under light microscopy according to the following procedure. Cultures were treated withglutaraldehyde, fixed with osmium, and then taken throughascending steps of alcohol dehydration. After Epon embedding, blocks were sectioned 2 /im thick. Toluidine blue, whichwas used to stain the sections, stained muscle cells darkerthan nonmuscle cells. Electron microscopic evaluation wasperformed selectively on the Epon-embedded sections in order
to further characterize ultrastructural effects of drug treatment.Drug Treatment. Cultures grown for 7 days were treated
with ADR (Adria Laboratories, Inc., Columbus, Ohio). ADRstock solutions were prepared by dissolving 10 mg of drug in5 ml of MEM. After appropriate dilution, 0.1 ml of drug solutionwas added to cultures containing 2 ml of medium to obtain thedesired final concentrations. When ADR treatment was continuous, drug was added at each medium change (every 48 hr).When drug exposure was discontinued after 1 hr, cultureswere rinsed with MEM (5x2 ml) and continued in drug-free
medium.
RESULTS
Within 7 days after seeding, primary heart cell culturesbecame confluent through the growth of muscle cells, whichdo not divide but grow large, and nonmuscle cells (epithelialand fibroblasts), which both grow and replicate. At this time,cultures beat rhythmically and synchronously, thus allowingthe monitoring of any area on an individual plate as an indication of the pattern of beating of the entire culture.
High-Dose Effects. The effects of high doses of ADR on thebeating of heart cell cultures are shown in Chart 2. Each pointon the chart represents the beating rate of an individual culture;in each case, the beating rate increased after the addition of
ADR. Cultures exposed continuously to ADR (100 jug/ml) nolonger beat after 250 min. At higher ADR doses (200 /ig/ml),cells stopped beating within 30 min of exposure, but theinhibition could be reversed at that time by rinsing the cultureswith MEM and continuing them in drug-free medium. Cellstreated in this way resumed beating shortly thereafter andcontinued to function for another 48 hr. However, by 72 hr,most of these cells lysed.
With continuous ADR treatment (10 /ig/ml), no effects onbeating rate could be detected in the first 24 hr of treatment.When cultures were incubated with ADR (10 fig/ml) for 1 hrand continued in drug-free medium, the cells began to lyse anddetach from the growing surface 48 to 72 hr after treatment.Cultures exposed to ADR (2 /¿g/ml)for 1 hr, however, continued to beat for as long as the cells were maintained (up to 10months).
The earliest structural effects observed in both cardiac muscle and nonmuscle cells were vacuolization and nucleolarfragmentation (Figs. 1 to 4); both effects were detected within5 hr of continuous exposure to ADR (10 fig/ml). Both effectswere also seen with continuous exposure to ADR (1.0 /ig/ml)for 24 hr.
Low-Dose Effects. The effects of continuous exposure to
low doses of ADR (0.1, 0.75, and 0.05 /ig/ml) on the beatingrate of cardiac cells in culture are shown in Chart 3. It can beseen that for the doses used, the average beating rates decreased as the time of exposure to drug increased. Furthermore, compared to controls, the variability in beats/min increased significantly. As a result, the beating rates of thesecultures were not a reliable parameter for study since thebeats/min of individual treated cultures overlapped those ofuntreated cultures.
The more consistent effect on cardiac cell function was adose-dependent arrhythmia which developed upon continuous
exposure of cells to these same drug concentrations. Thepattern of arrhythmias that were produced at several low-doseADR levels at 48 hr is shown in Chart 4. At an ADR dose of0.01 jug/ml, no effects on the rhythmicity of cells, relative tocontrols, were detected. However, at higher concentrationsindividual cultures pulsated with a double beat which wasdependent upon drug concentration. The interval of time between each set of double beats remained constant at the 0.05-/ig/ml ADR dose, whereas at 0.1 /ig/ml the time intervalbetween the double pulsations became irregular. These arrhythmic effects were reversible at 48 hr when cells were
Vocuolization
24 IOO 50 0 50 IOO ISO ZOO 250Hr
MinutesChart 2. Beating rate of 3 individual cultures (x, O, •)pre- and post-ADR
treatment (100 /ig/ml).
3902 CANCER RESEARCH VOL. 40
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Effects of ADR on Cardiac Cells in Vitro
100r
Chart 3. The average beating rate of 10 heart cell cultures per dose levelexposed continuously to ADR, 0.10 (x), 0.75 (O), and 0.05 (A) fig/ml, relativeto untreated controls (•).Drug was added at each media change (every 48 hr).Bars, S.D.
CONTROL
0.05
Chart 4. Polygraph recording (10-mm/sec chart speed) of cultures continuously exposed to ADR for 2 days at several dose levels. The 15-sec tracingsshown here are representative of the beating patterns of cultures that were eachmonitored for 8 min.
DISCUSSION
A serious limitation to the use of ADR is cardiac toxicity (14,23). Two cardiac effects have been reported in patients receiving ADR. The electrocardiographic changes are transient andoccur at all dose levels regardless of schedule. For example,in a study of 1051 ADR-treated patients, it has been reported
that 15.2% exhibited alteration in electrocardiograms. Themost frequently observed abnormalities were of cardiac rhythmand included supraventricular tachyarrhythmias, prematureventricular contractions, and premature supraventricular contractions (27). It is generally accepted that these changes arenonpredictive of eventual cardiomyopathy.
ADR-induced cardiomyopathy is dependent on total cumulative dose and may result in congestive heart failure (2). It hasbeen reported that the probability of anthracycline-induced
cardiomyopathy increases dramatically above a total ADR doseof 550 to 600 mg/sq m (3, 7, 22). A variety of morphologicalchanges, including loss of myofibrils, mitochondrial swelling,vacuolization, and disruption of Z-bands, have been noted
Day
rinsed and reincubated in drug-free medium (Chart 5), and thecells remained morphologically intact for the remainder of theexperiment (see below). When the cells were continuouslyexposed to drug for longer periods of time, the pattern ofarrhythmias became more chaotic and intervals of fibrillation-like beating were seen (Chart 6).
Chart 7 shows the incidence of arrhythmic cultures at 3 ADRdoses. The percentage of rhythmic cultures decreased as theADR concentration increased. Arrhythmias appeared earlier incultures treated with higher ADR doses, but, by Day 9, allcultures, regardless of drug dose, were arrhythmic.
Cultures continuously exposed to ADR (0.1 /ig/ml) for 4days showed no structural alteration, relative to controls, whenexamined by electron microscopy (Fig. 5). However, when cellswere fixed and examined after 17 days of continuous exposureto ADR (0.1 jig/ml), a striking loss of muscle fibers per cellwas observed (Fig. 6). In contrast to high-dose ADR, vacuoli
zation and nucleolar fragmentation were not observed here.The severe loss of muscle fibers seen under electron mi
croscopy was similarly detectable under light microscopy whencultures were fixed, sectioned, and stained with toluidine blue.Fig. 7 illustrates the difference in staining between muscle andnonmuscle cells. Based upon this differential staining, culturesexposed continuously to ADR (0.1 /ig/ml) for 17 days showedthat, of the muscle cells examined (200), greater than 95% hadundergone loss of muscle fiber.
Chart 5. Polygraph recordings (10 mm/sec, 15-sec samplings) of the beatingpattern of a culture continuously exposed for 2 days to ADR (10 fig/ml) and thenrinsed and reincubated in drug-free medium. Note the return to rhythmicity within24 hr after drug was removed and the continued rhythmic beating for theremainder of the experiment.
NOVEMBER 1980 3903
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

T. J. Lampidis et al.
Day
2
w A/yy /yvy A/v ""^
/wwvvvmvvvvvvvvvvvvvvvvvvvv^^
11
14
TT** *«*»«»"»<*>«'">'«'~*-«»-«
—Chart 6. Polygraph recordings (10-mm / sec chart speed. 15-sec sampling) of
the beating patterns of a culture continuously exposed to ADR (10 /ig/ml). Notethe fibrillating-like patterns at Days 4 and 11 and the general decrease in theamplitude of contraction with increased treatment time.
upon autopsy in hearts from patients who have succumbed toADR-induced congestive heart failure; similar changes have
been produced in a number of different animal species (1, 8,9, 16, 24, 30, 40). An endomyocardial biopsy procedure hasbeen developed (6) to ascertain the amount of damage incurred, relative to dose, in patients being treated with ADR. Tograde the amount of ADR-induced cardiomyopathy, Billingham
et al. (2, 6) use a histological scoring system which is basedupon the extent of vacuolization and loss of muscle fiber in themyocardium.
Cardiac muscle cells in culture are unique in that they maintain their ability to beat autorhythmically for prolonged periodsof time (20). Thus, they present an in vitro system in which thestructural and functional effects of various agents on cells,which retain their in vivo properties, may be assessed. Anumber of previous investigators have attempted to use heartcell cultures to evaluate anthracycline-induced toxicity, and
effects on beating rate and rhythmicity have been described(28, 29, 31, 35, 36). These studies have generally been non-
systematic, were performed at selected dose levels, and havenot equated functional alterations with morphological changes.In addition, a number of these studies used cultures which had
been established for only a few hr or days. However, it hasbeen reported that cardiac cells from various species areseverely damaged by trypsinization (11,17, 25), which causesmarked disorganization of myofilaments and complete loss ofZ-line material (25). Cardiac cells require nearly 7 days inculture to regain a morphology comparable to undissociatedtissue (25). Furthermore, it has been demonstrated that trypsinpersists on the cell surface for 24 hr after application (32) andintracellular enzyme activity has been noted for up to 48 hr(15). Thus, it is difficult to interpret the effects of drugs onrecently trypsinized cardiac cells. In the work described here,cells were allowed to grow in culture for at least 7 days beforetreatment, at which time cardiac cultures maintain stablerhythmic contractions (Chart 6) and are morphologically intact.
We find that high dose levels of ADR (100 to 200 /ig/ml)cause rapid alterations in beating and extensive morphologicalchanges (vacuolization and nucleolar fragmentation) in heartcell cultures. The effects on beating at 30 min can be reversedby rinsing the cultures and reincubating them in drug-freemedium, but such cultures lyse within 3 days. Thus, the short-term exposure of heart cells to high-dose ADR is lethal despite
the apparent recovery of beating. While it is known that ADRlocalizes in the nuclei of live cells (10, 18), the effects onbeating of the high dose of ADR used here indicate either thatnuclear ADR causes secondary effects in the cytoplasm or,more likely, that ADR is present in the cytoplasm and producesa direct effect on beating. Fluorescence studies are presentlyunder way to investigate this possibility.
At low doses of ADR (up to 0.1 /ig/ml), effects on beatingare seen earlier than are those on morphology. Furthermore,these effects are qualitatively different than those seen at highdoses. While high doses result in cessation of beating within 4hr, low doses produce arrhythmias that continue for prolongedperiods (more than 10 days). The incidence and severity of
ICO80604020
UntreatedIO/IO IO/IO IO/IO IO/IO IO/IOimi
lOO80'60-
13579
,„,Treatment
E/II
B
0100/i.g/ml
O/M o/ii O/M
IOO8060'4°20
I 3 5 7IO/IOIO/IOil0.075/xg/ml
o/io o/io o/io
IOO80604020
0.050/u.g/mlI'foot*
I 4/IO•i- O/IO
I 3579
DaysChart 7. Incidence of arrhythmic cultures at 3 different ADR doses. Numbers
above bars, number of rhythmic cultures per number of cultures treated. Arrhythmias were counted as any deviation from the normal interval of time betweensingle beats observed in 10 of 10 control cultures throughout the 9-day experimental period.
3904 CANCER RESEARCH VOL. 40
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Effects of ADR on Cardiac Cells in Vitro
arrhythmias are clearly dose dependent (Charts 4 and 7): asthe exposure time increased, there was a general tendencytoward more irregular and chaotic beating. Recently, Villani etal. (37) have reported that in isolated guinea pig atria ADRcauses a shift of calcium from the rapidly to the slowly exchanging pool. Since spontaneous contractions of cardiac cells invitro have been shown to be sensitive to small calcium shifts(13), ADR-induced arrhythmias may be a reflection of this shift.
Although ADR produced arrhythmias as early as 24 hr at 0.1/ig/ml, ultrastructural changes were not detected until muchlater (17 days). Furthermore, when cultures were washed afterbeing exposed to ADR (0.1 jug/ml) and continued in drug-free
medium, the arrhythmias were reversible (Chart 5), and thecells appeared morphologically intact for as long as they weremaintained (17 days). However, when cells were exposed tolow ADR doses for up to 17 days, a striking loss of musclefiber per muscle cell was observed, while nuclear effects andvacuolization were not seen.
When other anticancer agents were compared with ADR inthis system at doses which were not immediately lethal, loss ofmuscle fiber was seen only with ADR and, to a lesser extent,with actinomycin D, while arrhythmias were produced by several agents, including ADR (19). ADR is known to inhibit RNAsynthesis (26). Thus, it is possible that the striking loss ofmuscle fibers in cells continuously exposed to low doses ofADR may be reflecting this inhibition of RNA synthesis. Alternatively, ADR may have a direct effect on muscle fiber leadingto its destruction.
We have found that electrocardiographic and histopatholog-
ical effects of ADR similar to those seen in animals and patientscan be produced in vitro. Furthermore, we have found thatcertain pathological effects, such as vacuolization and myofi-
brillar dropout, which have been reported in a variety of in vivosystems after a number of different dose treatments, occur atdistinct doses in vitro. We recognize, however, that in order toproduce these effects higher ADR levels were used here thanare achieved in heart tissue in vivo following a bolus administration. Notwithstanding, recent reports by Weiss and Manthei(39) and others (21, 33, 38) have indicated a reduction incardiomyopathy in patients treated with fractionated doses ofADR. Since vacuolization and lysis of myocardial cells do notoccur in vitro at low doses, it is conceivable that the reducedcardiac toxicity reported with fractionated ADR doses clinicallymay be the result of the failure to induce the high-dose pathol
ogy.
ACKNOWLEDGMENTS
We are grateful to Howard Fixier and Barry S. Saperia for skillful technicalassistance and to Martha Mann for providing a continuing supply of rat neonates.The assistance of Janet Gibeau in preparing the manuscript is greatly appreciated.
REFERENCES
1. Bertazolli, C., Bellini, O., Magrini, U , and Tosana, M. G. Quantität'""
experimental evaluation of Adriamycin cardiotoxicity in the mouse. CancerTreat. Rep.. 63. 1877-1883. 1979.
2. Billingham, M.. Bristow, M. E., Mason, J. W , and Daniels. J. R. Anthracyclinecardiomyopathy monitored by morphologic changes. Cancer Treat. Rep.,62. 857-864, 1978.
3. Bonadonna, G., Beretta, G., Tancici, G., Brambilla, C., Bajetta, E., De Palo,Q. M., Del Lena, M., Fossati Bellani, F., Gasparini, M., Valagussa, P., andVeronesi, U. Adriamycin studies at the Instituto Nazionale Tumori, Milan.Cancer Chemother. Rep., 6. 231-245, 1975.
4. Bonadonna, G., De Lena, M., and Beretta, G. Preliminary clinical screeningwith Adriamycin in lung cancer. Eur. J. Cancer, 7. 365-367, 1971.
5. Bonadonna, G., and Monfardini, S. Cardiac toxicity of daunorubicin. Lancet.Õ.-837. 1969.
6. Bristow, M. R.. Mason, J. W., Billingham, M. E., and Daniels, J. R. Doxorub-¡cincardiomyopathy: evaluation by phonocardiography, endomyocardialbiopsy, and cardiac catheterization. Ann. Intern. Med . 88 168-175, 1978.
7. Cortes. E. P., Lutman, G., Wanka. J.. Wang, J. J.. Pickren, J.. Wallace, J.,and Holland, J. F. Adriamycin cardiotoxicity: a clinicopathologic correlation.Cancer Chemother. Rep., 6. 215-225, 1975.
8. Dantchev, D., Sliuossartchouk, V.. Paintrand, M., Hayat, M., Bourut, C., andMathé,G. Electron microscopic studies of the heart and light microscopicstudies of the skin after treatment of golden hamsters with Adriamycin,détorubicin, AD-32, and aclacinomycin. Cancer Treat. Rep., 63. 875-888.
1979.9. Denine, E. P., and Schmidt, L. H. Adriamycin-induced myopathies in the
rhesus monkey with emphasis on cardiomyopathy. Toxicol. Appi. Pharma-
COl., 33. 162, 1975.10. Egorin, M. J., Hildebrand, R. C., Cimino, E. F.. and Bachur. N. R. Cyioflu-
orescence localization of Adriamycin and daunorubicin. Cancer Res.. 34:2243-2245, 1974.
11. Fischman, D. A., and Moscona, A. A. Reconstitution of heart tissue fromsuspensions of embryonic myocardial cells: ultrastructural studies on dispersed and reaggregated cells. In: N. R. Alpert (ed.). Cardiac Hypertrophy,pp. 125-139. New York: Academic Press, Inc., 1971.
12. Gilladoga, A. C.. Manuel, C., Tan, C., Wollner. N., and Murphy, L. M.Cardiotoxicity of Adriamycin in children. Cancer Chemother. Rep., 6. 209-
214, 1975.13. Harary, J., Renaud, J. F., Sato, E., and Wallace. G. A. Calcium ions regulate
cyclic AMP and beating in cultured heart cells. Nature (Lond.), 261 60-61,1976.
14. Henderson, I. C., and Frei. E.. III. Adriamycin cardiotoxicity. Am. Heart J.,99. 671-674, 1980.
15. Hodges, G. N., Livingston, D. C., and Franks, L. M. The localization oftrypsin in cultured mammalian cells. J. Cell Sci., 12: 887-902, 1973.
16. Jaenke, R. S. An anthracycline antibiotic-induced cardiomyopathy in rabbits.Lab. Invest., 30. 292-304. 1974.
17. Kasten, F. H. Electron microscope studies of the combined effects oftrypsinization and centrifugation of rat heart cells, with observations of earlycultures. J. Cell. Biol., 31: 131 A, 1966.
18. Krishan, A.. Israel, M.. Modest. E. J., and Frei, E., III. Differences in cellularuptake and cytofluorescence of Adriamycin and fV-trifluoroacetyl-adriamy-cin-14-valerate. Cancer Res., 36. 2114-2116, 1976.
19. Lampidis, T. J., Henderson, I. C., Israel, M.. Canellos, G. P., and Frei, E., III.Evaluation of Adriamycin (ADR) cardiotoxicity (CT) using an in vitro rat heartcell system. Proc. Am. Soc. Cancer Res., 20. 216. 1979.
20. Lampidis, T. J., Weichselbaum, R. R., and Little, J. B. Gamma-irradiation ofmammalian beating heart cells in vitro: effects of cellular function. Int. J.Radiât.Biol.. 28. 99-102, 1975.
21. Lazarus, A. J., and Manthei, R. W. Experience with the use of Adriamycin incombination with other anti-cancer agents using a weekly schedule, withparticular reference to lack of cardiac toxicity. Cancer (Phila.), 40 2046-
2052, 1977.22. Lefrak, E. A., Pitha, J., Rosenheim, S., and Gottleib, J. A. A clinicopathologic
correlation. Cancer (Phila.), 32. 302-314, 1973.23. Lenaz, L., and Page, J. A. Cardiotoxicity of Adriamycin and related anthra-
cyclines. Cancer Treat. Rev., 3. 111-120, 1976.24. Lenaz, L, Sternberg, S. S., DeHarven, E., Vidal, R. M., and Philips, F. S.
Cardiac lesions in Adriamycin (ADM) treated mice. Proc. Am. Soc. CancerRes.. »9:213, 1978.
25. Masson-Pevet. M., Jongsma, H. J., and De Bruijne, J. Collagenase- andtrypsin-dissociated heart cells: a comparative ultrastructural study. J. Mol.Cell Cardici., 8. 747-757, 1976.
26. Meriwether, W. D., and Bachur, N. R. Inhibition of DNA and RNA metabolismby daunorubicin and Adriamycin in L1210 mouse leukemia. Cancer Res.,32. 1137-1142, 1972.
27. Minow, R. A., Benjamin, R. S., and Gottlieb. J. A. Adriamycin cardiomy-opathy-an overview with determination of risk factors. Cancer Chemother.Rep.. 6. 195-201. 1975.
28. Neceo. A.. Dasdia. T., Cozzi. S.. and Ferraguti. M. Ultrastructural changesproduced in cultured. Adriamycin-treated myocardial cells. Tumori, 62.537-544, 1976.
29. Neceo, A., Dasdia. T.. Di Fransesco, D.. and Ferroni, A. Action of ouabain,oligomycin, and glucagon on cultured heart cells treated with Adriamycin.Pharmacol. Res. Commun.. 8. 105-109, 1976.
30. Olson, H. M., Young. D. M., Prieur, D. J., Leroy, A. F.. and Reagan, R. L.Electrolyte and morphologic alterations of myocardium in Adriamycin-treated rabbits. Am. J. Pathol., 77. 439-450, 1974.
31. Petrovic, D.. Brown, S. M., and Yatvin. M. B. Effects of Adriamycin andirradiation on beating of rat heart muscle cells in culture. Int. J. Rad. Oncol.Biol. Phys., 2. 505-513, 1977.
32. Poste, G. Tissue dissociation with proteolytic enzymes. Adsorption andactivity of enzymes at the cell surface. Exp. Cell. Res.. 65. 359-367. 1971.
NOVEMBER 1980 3905
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
T. \J. Lampidis et al.
33. Praga, C., Beretta, G., Vigo, P. L. Lenaz. G. R., Polloni, C.. Bonadonna, G., J. Mol. Cell Cardiol., 9. 375-382, 1977.Caretta, R., Castellani, R., Villa, E., Gallagher, C. G., von Melchner. H., 37. Villani, F., Piccinini, F., Merelli. P., and Faualli, L Influence of Adriamycin onHayat, M.. Ribaud, P., De Wasch, G., Mattsson, W., Heinz, R., Waldner, R., calcium exchangeability in cardiac muscle and its modification by ouabain.Kolaric, K., Beuhner. R., Ten Bokkel-Huyninck, W., Perevodchikova, N. I., Biochem. Pharmacol.. 27. 985-987, 1978.Manzuik, L. A., Senn, H. J., and Mayr, A. C. Adriamycin cardiotoxicity: a 38. Von Hoff, D. D., Layand, M., Basa, P., Davis, H. L., Jr., Von Hoff. A. L.,survey of 1273 patients. Cancer Treat. Rep.. 63 827-834, 1979. Rozenweig, M., and Muggia, F. M. Risk factors for doxorubicin-induced
34 Rinehart, J. J.. Lewis, R. P., and Balcerzak, S. P. Adriamycin cardiotoxicity congestive heart failure. Ann. Intern. Med., 97. 710-717, 1979.in man. Ann. Intern. Med., 81: 475-478. 1974. 39. Weiss, A. J., and Manthei, R. W. Experience with the use of Adriamycin in
35. Seraydarian, M. W., and Artaza, L. Modification by adenosine of the effect combination with other anti-cancer agents using a weekly schedule, withof Adriamycin on myocardial cells in culture. Cancer Res.. 39: 2940-2944, particular reference to lack of cardiac toxicity. Cancer (Phila.), 40 2046-1979. 2052,1977.
36. Seraydarian, M. W., Artaza, L., and Goodman, M. F. Adriamycin: effect on 40. Young, D. M. Pathological effects of Adriamycin in experimental systems,mammalian cardiac cells in culture I. Cell population and energy metabolism. Cancer Chemother. Rep., 6. 159-175, 1975.
Fig. 1. Phase-contrast micrograph of cardiac muscle (M) cell and nonmuscle (A/M) cell. Note rounded shape of nucleus, large distinct mitochondria, and 1nucleolus/nucleus in muscle cell; whereas nonmuscle cell has a larger, oval nucleus containing 2 nucleoli, and less distinct mitochondria, x 600.
Fig. 2. Phase-contrast micrograph of cardiac cells containing vacuoles (V) after 5 hr of continuous exposure to ADR (10 /ig/ml), x 300.
Fig. 3. Phase-contrast micrograph of cardiac nonmuscle cells containing vacuoles (V) and nucleolar fragmentation (NF) after 5 hr of continuous exposure to ADR(10/ig/ml). x 1000.
Fig. 4. Electron micrograph of cardiac muscle cell treated with ADR (10 fig/ml) for 24 hr. Note segregated nucleolus (SN) and vacuoles (V). Muscle fibers (MF)were still intact, and the cell was still beating rhythmically at the time of fixation, x 5200.
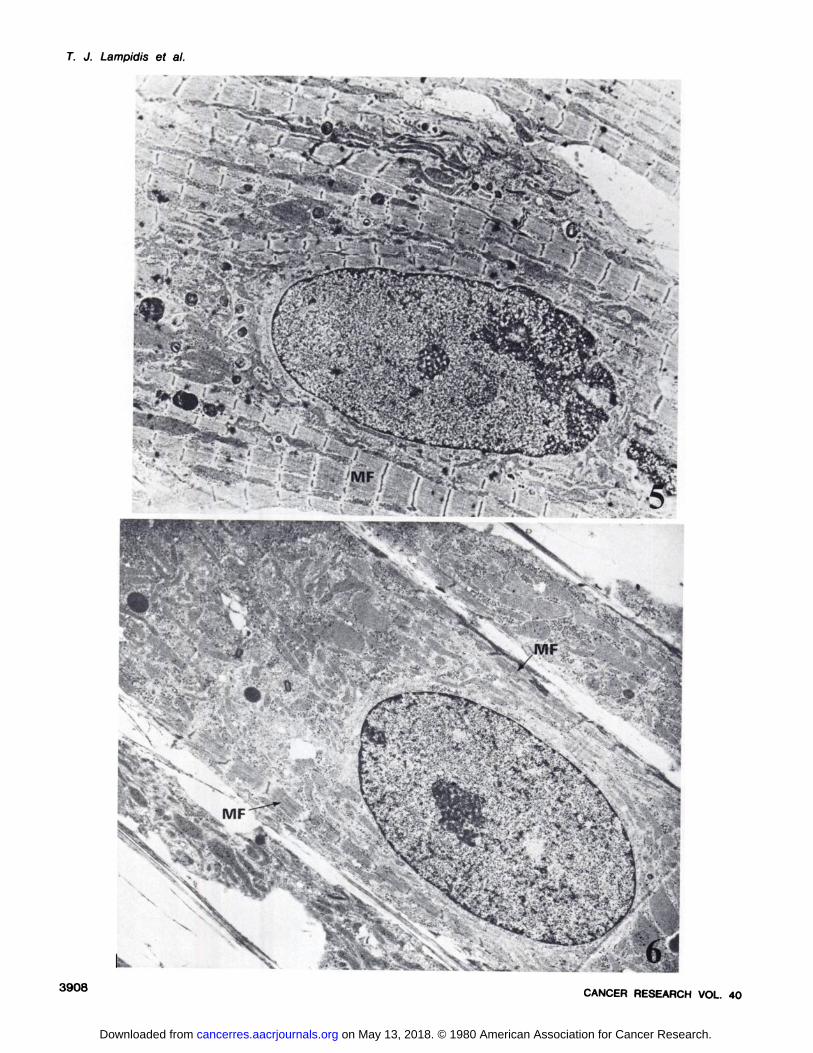
Fig. 5. Electron micrograph of cardiac muscle cell in culture for 24 days with intact muscle fibers (MF), x 5200.
Fig. 6. Electron micrograph of cardiac muscle cell in culture for 7 days and subsequently treated for 17 days, with ADR (0.1 fig/ml). Note the striking loss ofmuscle fibers (MF) (few remain) and the absence of vacuolization and nuclear effects, x 5200.
Fig. 7. Light micrograph of toluidine blue-stained section of cardiac cells grown in culture for 17 days. Note the light-staining nonmuscle cells (N/vf), as comparedto the dark-staining muscle cells, x 400.
3906 CANCER RESEARCH VOL. 40
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Effects of ADR on Cardiac Cells in Vitro
IMM
1
V ..
•
MF
MF
NOVEMBER 1980 3907
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
^-êiil; /%/* '-
-
sS^K$$ÿ&m Ãr- •:^ÉlÉáAl¿M
3908 CANCER RESEARCH VOL. 40
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Effects of ADR on Cardiac Cells in Vitro
NOVEMBER 1980 3909
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1980;40:3901-3909. Cancer Res Theodore J. Lampidis, I. Craig Henderson, Mervyn Israel, et al.
in VitroCells Structural and Functional Effects of Adriamycin on Cardiac
Updated version
http://cancerres.aacrjournals.org/content/40/11/3901
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/40/11/3901To request permission to re-use all or part of this article, use this link
on May 13, 2018. © 1980 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from