stress testing
DESCRIPTION
Stress testing. Physiology: Sympathetic system activation increases: Heart rate Stroke volume Cardiac output Ventricular contractility Afterload (Vasoconstriction) Muscular & Coronary flow (Vasodilatation). Demand vs. Supply. Oxygen consumption (VO 2 ). Coronary flow. - PowerPoint PPT PresentationTRANSCRIPT

Stress testingStress testing
Physiology:Physiology:
Sympathetic system activation increases: Sympathetic system activation increases: Heart rateHeart rateStroke volumeStroke volumeCardiac outputCardiac outputVentricular contractilityVentricular contractilityAfterload (Vasoconstriction)Afterload (Vasoconstriction)Muscular & Coronary flow (Vasodilatation)Muscular & Coronary flow (Vasodilatation)

Demand vs. Supply Demand vs. Supply
Coronary flowOxygen consumption
(VO2)
Resting VO2 = 1 Mets = 3,5 ml O2 / min / kg.

Exercise testsExercise tests
Master testMaster test
Bicycle Bicycle
TreadmillTreadmill
ECG - 3 leads (V5), 12 ECG - 3 leads (V5), 12 leadsleads
Computerized ST Computerized ST analysisanalysis
Treadmill stress testTreadmill stress test

Positive stress testPositive stress test
Anginal pain or dyspneaAnginal pain or dyspnea
ST↓ horizontal ST↓ horizontal >>1 mm 0.08” after J point1 mm 0.08” after J point
ST↓ downsloping ST↓ downsloping >> 0.5 mm 0.5 mm
ST↓ upsloping ST↓ upsloping >> 1.5 mm 1.5 mm
ST↑ elevationST↑ elevation
QRS wideningQRS widening

Exercise test accuracyExercise test accuracy
SensitivitySensitivity =% of pts. w. CAD & ETT(+) ~ 66 % =% of pts. w. CAD & ETT(+) ~ 66 %
SpecificitySpecificity = % of normals with ETT(-) ~77 % = % of normals with ETT(-) ~77 %
False negative: borderline lesions, collateralsFalse negative: borderline lesions, collaterals
False positive: LVH, MVP, digitalis, LBBBFalse positive: LVH, MVP, digitalis, LBBB

Indications for ETTIndications for ETT
I. I. DiagnosticDiagnostic – probability of CAD – probability of CAD Evaluation of symptoms: chest pain, Evaluation of symptoms: chest pain,
dyspnea, fatiguedyspnea, fatigue Asymptomatic – Multiple CAD risk factorAsymptomatic – Multiple CAD risk factor ScreeningScreening Functional CapacityFunctional Capacity Detection of Arrthymia and response to RxDetection of Arrthymia and response to Rx Hypertensive responseHypertensive response

II. II. PrognosticPrognostic::
Known CAD – risk stratificationKnown CAD – risk stratification
Stable AP, or worsening AP, DOE, FCStable AP, or worsening AP, DOE, FC
Before and after revascularization Before and after revascularization (PTCA, CABG)(PTCA, CABG)
Pre operative risk evaluationPre operative risk evaluation
Indications for ETTIndications for ETT

III. III. Post Acute Coronary SyndromePost Acute Coronary Syndrome
Need for revascularization Need for revascularization Medical treatment adjustment Medical treatment adjustment
(AP, BP, HR, Arrhythmias)(AP, BP, HR, Arrhythmias)Guide for cardiac rehabilitation, Guide for cardiac rehabilitation, Self-confidenceSelf-confidenceTiming of return to work and its intensityTiming of return to work and its intensity
Indications for ETTIndications for ETT
High risk ETT High risk ETT > 4 % Mortality risk> 4 % Mortality risk
Low F.C. < 6 min exerciseLow F.C. < 6 min exercise
ST depression at low HR or stressST depression at low HR or stress
ST depression > 2 mmST depression > 2 mm
ST elevation or QRS wideningST elevation or QRS widening
Severe AP or dyspneaSevere AP or dyspnea
Arrhythmias (VT, PAF)Arrhythmias (VT, PAF)
Systolic BP dropSystolic BP drop

Contraindications for ETTContraindications for ETT
Risk < 0.01 %, Post MI 0.03%Risk < 0.01 %, Post MI 0.03%
Unstable AnginaUnstable AnginaAcute Heart FailureAcute Heart FailureArrhythmiasArrhythmiasMyo- or Peri-carditisMyo- or Peri-carditisSevere Aortic StenosisSevere Aortic StenosisHypertrophic obstructive cardiomyopathyHypertrophic obstructive cardiomyopathySevere Hypertension (>220/110 mmHg)Severe Hypertension (>220/110 mmHg)

Exercise testingExercise testing
Fasting, off Fasting, off ββ-blockers-blockers
Symptom limited: Symptom limited:
AP, dyspnea, dizziness, fatigue, leg painAP, dyspnea, dizziness, fatigue, leg pain
Max. heart rate = 220 – ageMax. heart rate = 220 – age
Target heart rate: 85 % of max. HRTarget heart rate: 85 % of max. HR
If not achieved – non diagnostic testIf not achieved – non diagnostic test
Stop ifStop if: ST↓ : ST↓ >> 3 mm, ST↑, SBP↓ > 10mmHg, 3 mm, ST↑, SBP↓ > 10mmHg,
technical problems with ECG monitoringtechnical problems with ECG monitoring


Nuclear CardiologyNuclear Cardiology
Myocardial perfusionMyocardial perfusion
Thallium – 201Thallium – 201
Cyclotron product: dose - 2 mCurieCyclotron product: dose - 2 mCurie
Long half life – 72 hoursLong half life – 72 hours
85% - first pass myocardial uptake85% - first pass myocardial uptake
Na-K-ATPase pumpNa-K-ATPase pump
Redistribution: 4 or 24 hr.= viabilityRedistribution: 4 or 24 hr.= viability

LAO view of the heart
(pathology)
SRV
PW
A
LV

Thallium image during anginaThallium image during angina

Thallium - planar views of the heartThallium - planar views of the heart



ThalliumThalliumTreadmill Treadmill
stress stress testtest
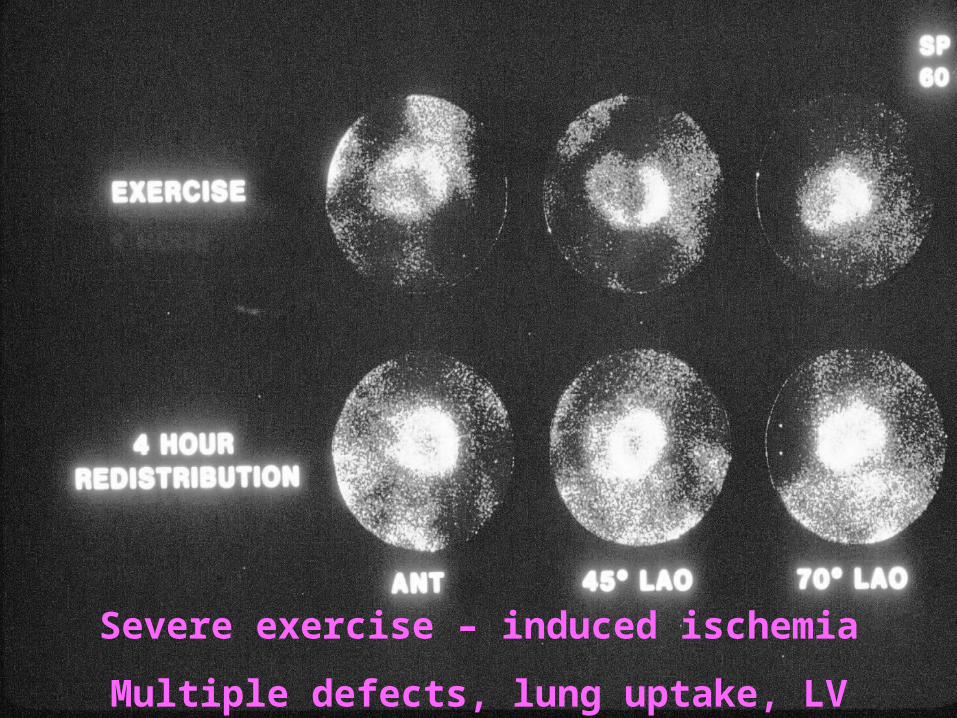
Severe exercise – induced ischemia
Multiple defects, lung uptake, LV dilatation

Thalium 201Thalium 201
DiagnosisDiagnosis
Infarct: Perfusion defect at stress and restInfarct: Perfusion defect at stress and rest
Ischemia: Defect at stress that normalizes after Ischemia: Defect at stress that normalizes after 4 or 24 hours.4 or 24 hours.
Sensitivity ~ 90 %Sensitivity ~ 90 %
Specificity ~ 80 %Specificity ~ 80 %
Localization of ischemia / infarctLocalization of ischemia / infarct
Extend and severity of CADExtend and severity of CAD
Functional vs. anatomic assessment (angio)Functional vs. anatomic assessment (angio)
Planar vs. spect (tomographic) imagingPlanar vs. spect (tomographic) imaging


Normal Myocardial Perfusion

Myocardial Ischemia

Myocardial Infarction

Technetium SestamibiTechnetium Sestamibi
Higher dose (30 mCurie), improved image Higher dose (30 mCurie), improved image qualityquality
Shorter half life (6 hours)Shorter half life (6 hours)
No redistribution, therefore 2 separate No redistribution, therefore 2 separate injections for rest and stressinjections for rest and stress
ECG gating for wall motion, EFECG gating for wall motion, EF
First pass imagingFirst pass imaging

Pharmacologic vs. stress imagingPharmacologic vs. stress imaging
Indicated for pts. unable to complete full stress Indicated for pts. unable to complete full stress test due to low HR, PVD, COPD, CHF, test due to low HR, PVD, COPD, CHF, orthopedic disabilityorthopedic disability
Adenosin or dypiridamole drip: vasodilatation Adenosin or dypiridamole drip: vasodilatation
of normal vs. narrowed coronariesof normal vs. narrowed coronaries
Thallium or Tech. sestamibi injectionThallium or Tech. sestamibi injection
Perfusion abnormality similar to stressPerfusion abnormality similar to stress

Contrast left Contrast left ventricular ventricular
angiography: angiography: Antero – apical Antero – apical
aneurysmaneurysmRAO viewRAO view
Diastole
Systole

Technetium 99 labeled RBCTechnetium 99 labeled RBC
First pass image or at equilibriumFirst pass image or at equilibriumMultigated acquisition (MUGA)Multigated acquisition (MUGA)Regional wall motion at rest and / or stressRegional wall motion at rest and / or stress
Ejection Fraction (%)= X 100Ejection Fraction (%)= X 100
Assessment of ischemia Assessment of ischemia Viability: Dobutamine effectViability: Dobutamine effect
m
EDC - ESC
EDC



ECG – gated acquisition

MUGA – RAO viewMUGA – RAO view

MUGA – LAO viewMUGA – LAO view
RVLV
Diastole Systole
RV LV

MUGA – bicycle exerciseMUGA – bicycle exercise



Gated Cardiac Results

Indications for nuclear testingIndications for nuclear testing
I.I. DiagnosticDiagnostic
CAD assessment – best for intermediate CAD assessment – best for intermediate likelihood of CADlikelihood of CAD
Extent and severity of CADExtent and severity of CAD Extent of ischemic vs. infarcted areasExtent of ischemic vs. infarcted areas Need for revascularization Need for revascularization

II. II. PrognosticPrognostic: :
Risk stratification - MI / Death:Risk stratification - MI / Death:
0.5 – 50 % for normal vs. high risk scan0.5 – 50 % for normal vs. high risk scan
Pre-operative assessmentPre-operative assessment
Post ACS / MIPost ACS / MI
Change in symptoms / ETT resultsChange in symptoms / ETT results
Indications for nuclear testingIndications for nuclear testing
High risk nuclear testHigh risk nuclear test
Multiple and / or severe perfusion defectsMultiple and / or severe perfusion defects
Increased lung uptakeIncreased lung uptake
Stress induced LV dilatation Stress induced LV dilatation

III. III. Viability studyViability study (hybernating vs. scar tissue) (hybernating vs. scar tissue)
Thallium late redistributionThallium late redistribution
MUGA with dobutamine dripMUGA with dobutamine drip
Positron emission tomography (PET)Positron emission tomography (PET)
Mismatch between reduced perfusion Mismatch between reduced perfusion (ammonia or rubidium) and preserved (ammonia or rubidium) and preserved metabolism (glucose)metabolism (glucose)
Improved function following revascularizationImproved function following revascularization
Indications for nuclear testingIndications for nuclear testing

PET Scan: Viability studyPET Scan: Viability study