stent performance: never too late to sort it out
TRANSCRIPT
Comment
www.thelancet.com Published online March 14, 2014 http://dx.doi.org/10.1016/S0140-6736(14)60461-X 1
Stent performance: never too late to sort it outDrug-eluting stents have greatly improved the clinical outcomes of patients undergoing percutaneous coronary intervention by mitigating the risk of restenosis inherent to bare-metal stents, and are now the standard of care.1 However, the antirestenotic eff ectiveness achieved with early-generation drug-eluting stents during the fi rst year after implantation came at the cost of delayed arterial healing of the treated coronary artery segment,2 which was associated with a small increase in the risk of stent thrombosis that emerged only during very late follow-up after cessation of dual antiplatelet therapy.3 New-generation drug-eluting stents have been developed to overcome this limitation through the use of new platform materials, thinner stent struts, more biocompatible durable or biodegradable surface polymer coatings, and novel antiproliferative agents. The Endeavor zotarolimus-eluting stent was developed based on the hypothesis that reduced antiproliferative potency could improve healing of the treated coronary artery segment.
In The Lancet, Michael Maeng and colleagues4 report the fi nal 5-year follow-up of the SORT OUT III trial, a randomised comparison of the zotarolimus-eluting stent (n=1162 patients) with the Cypher sirolimus-eluting stent (n=1170 patients)—the gold standard in terms of restenosis prevention among early-generation drug-eluting stents. At 9 months’ follow-up, the study had shown that the zotarolimus-eluting stent had lower effi cacy than the sirolimus-eluting stent for the primary endpoint of major adverse cardiac events (a composite of cardiac death, myocardial infarction, and target vessel revascularisation).5 However, at 5 years’ follow-up, the two types of stent no longer diff ered signifi cantly in terms of the primary endpoint (odds ratio [OR] 1·10, 95% CI 0·88–1·37), its individual components, or defi nite stent thrombosis.4 This outcome was the consequence of time-dependent changes in the relative treatment eff ects of the two devices, with the zotarolimus-eluting stent having an inferior outcome to the sirolimus-eluting stent in terms of major adverse cardiac events during the fi rst year of follow-up (OR 2·13, 95% CI 1·48–3·07), which was subsequently compensated for between 1 and 5 years’ follow-up by a reduced risk of target lesion revascularisation (0·49, 0·30–0·79) and very late stent thrombosis (0·05, 0·01–0·36) in the zotarolimus-eluting stent treatment group.4 Notably, a similar off setting
phenomenon between early and late events after drug-eluting stent implantation was recorded at 3 years in the larger PROTECT trial6 that compared the same devices as those in SORT OUT III, and at 5 years in the SIRTAX trial7 that compared sirolimus-eluting stents with paclitaxel-eluting stents. Similarly, the safety advantage of new-generation drug-eluting stents—such as everolimus-eluting stents and biolimus-eluting stents—as compared with early-generation drug-eluting stents emerged only during long-term follow-up.8,9
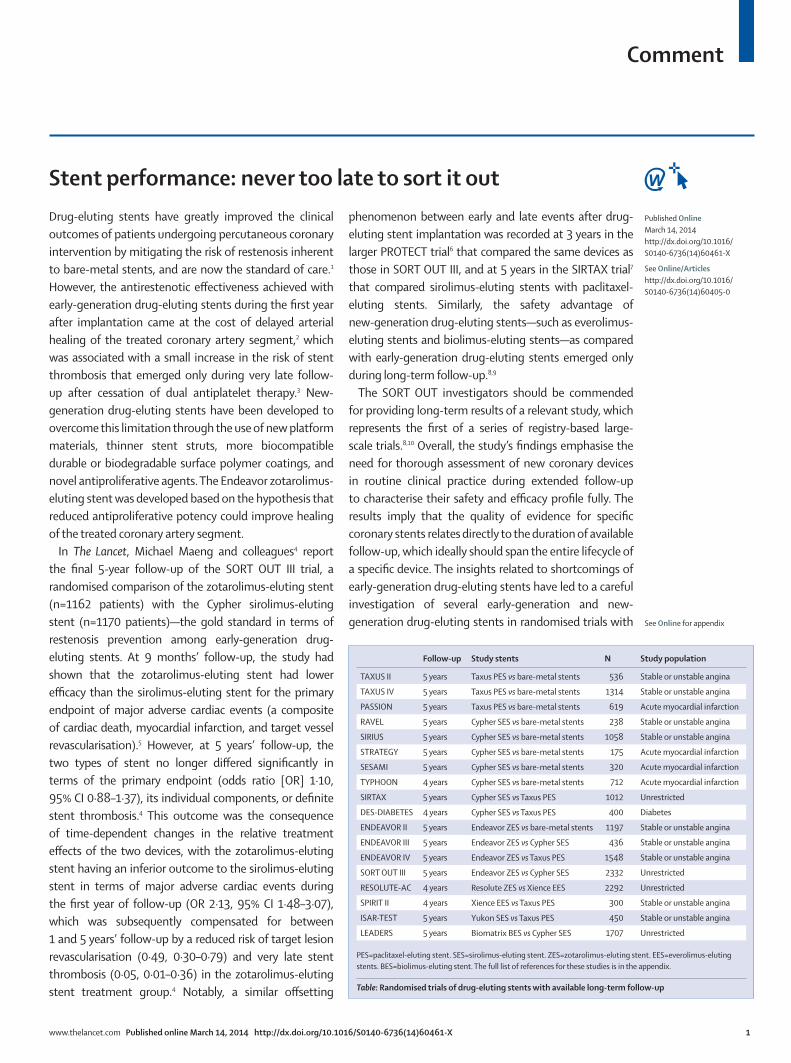
The SORT OUT investigators should be commended for providing long-term results of a relevant study, which represents the fi rst of a series of registry-based large-scale trials.8,10 Overall, the study’s fi ndings emphasise the need for thorough assessment of new coronary devices in routine clinical practice during extended follow-up to characterise their safety and effi cacy profi le fully. The results imply that the quality of evidence for specifi c coronary stents relates directly to the duration of available follow-up, which ideally should span the entire lifecycle of a specifi c device. The insights related to shortcomings of early-generation drug-eluting stents have led to a careful investigation of several early-generation and new-generation drug-eluting stents in randomised trials with
Follow-up Study stents N Study population
TAXUS II 5 years Taxus PES vs bare-metal stents 536 Stable or unstable angina
TAXUS IV 5 years Taxus PES vs bare-metal stents 1314 Stable or unstable angina
PASSION 5 years Taxus PES vs bare-metal stents 619 Acute myocardial infarction
RAVEL 5 years Cypher SES vs bare-metal stents 238 Stable or unstable angina
SIRIUS 5 years Cypher SES vs bare-metal stents 1058 Stable or unstable angina
STRATEGY 5 years Cypher SES vs bare-metal stents 175 Acute myocardial infarction
SESAMI 5 years Cypher SES vs bare-metal stents 320 Acute myocardial infarction
TYPHOON 4 years Cypher SES vs bare-metal stents 712 Acute myocardial infarction
SIRTAX 5 years Cypher SES vs Taxus PES 1012 Unrestricted
DES-DIABETES 4 years Cypher SES vs Taxus PES 400 Diabetes
ENDEAVOR II 5 years Endeavor ZES vs bare-metal stents 1197 Stable or unstable angina
ENDEAVOR III 5 years Endeavor ZES vs Cypher SES 436 Stable or unstable angina
ENDEAVOR IV 5 years Endeavor ZES vs Taxus PES 1548 Stable or unstable angina
SORT OUT III 5 years Endeavor ZES vs Cypher SES 2332 Unrestricted
RESOLUTE-AC 4 years Resolute ZES vs Xience EES 2292 Unrestricted
SPIRIT II 4 years Xience EES vs Taxus PES 300 Stable or unstable angina
ISAR-TEST 5 years Yukon SES vs Taxus PES 450 Stable or unstable angina
LEADERS 5 years Biomatrix BES vs Cypher SES 1707 Unrestricted
PES=paclitaxel-eluting stent. SES=sirolimus-eluting stent. ZES=zotarolimus-eluting stent. EES=everolimus-eluting stents. BES=biolimus-eluting stent. The full list of references for these studies is in the appendix.
Table: Randomised trials of drug-eluting stents with available long-term follow-up
See Online for appendix
Published OnlineMarch 14, 2014http://dx.doi.org/10.1016/S0140-6736(14)60461-X
See Online/Articleshttp://dx.doi.org/10.1016/S0140-6736(14)60405-0

Comment
2 www.thelancet.com Published online March 14, 2014 http://dx.doi.org/10.1016/S0140-6736(14)60461-X
extended follow-up (table). However, long-term studies are not available for many other drug-eluting stents that are approved for clinical use.
Although the SORT OUT III study design is pragmatic, cost eff ective, and important to inform clinical practice, it does have some limitations. Specifi cally, patient-triggered event rates are typically lower than are those obtained with active clinical follow-up, at least partly because of intrinsic inaccuracies of discharge coding that could represent a source of detection bias. Additionally, the direct relevance for present clinical practice of the long-term results of SORT OUT III is limited by the fact that the investigated devices are outdated, which is often the case when very long-term follow-up results of coronary stent trials are reported.6,7 Finally, the absence of data for compliance with dual antiplatelet therapy throughout the study period precludes any conclusions about the eff ect of antiplatelet therapy cessation on thrombotic events.
Overall, the long-term follow-up results of SORT OUT III have important implications for the design of future studies investigating novel coronary devices. Close collaboration between physicians, regulatory authorities, and device manufacturers is needed for meaningful post-marketing device assessment, and approval of novel coronary devices should be based on the commitment to undertake appropriately designed long-term follow-up studies. However, innovation is the driving force to resolve the shortcomings of existing technology and needs to be preserved to safeguard further advances in the specialty. Since long-term data might only become available when devices with a short lifecycle have been replaced by more innovative technologies, sometimes it could be too late to “sort it out”.
*Giulio G Stefanini, Stephan WindeckerDepartment of Cardiology, Bern University Hospital, 3010 Bern, [email protected]
SW has received research grants to his institution from Abbott, Biotronik, Edwards, Medtronic, and St Jude. GGS declares that he has no competing interests.
1 Stefanini GG, Holmes DR Jr. Drug-eluting coronary-artery stents. N Engl J Med 2013; 368: 254–65.
2 Raber L, Baumgartner S, Garcia-Garcia HM, et al. Long-term vascular healing in response to sirolimus- and paclitaxel-eluting stents: an optical coherence tomography study. JACC Cardiovasc Interv 2012; 5: 946–57.
3 Daemen J, Wenaweser P, Tsuchida K, et al. Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort study. Lancet 2007; 369: 667–78.
4 Maeng M, Tilsted HH, Jensen LO, et al. Diff erential clinical outcomes after 1 year versus 5 years in a randomised comparison of zotarolimus-eluting and sirolimus-eluting coronary stents (the SORT OUT III study): a multicentre, open-label, randomised superiority trial. Lancet 2014; published online March 14. http://dx.doi.org/10.1016/S0140-6736(14)60405-0.
5 Rasmussen K, Maeng M, Kaltoft A, et al. Effi cacy and safety of zotarolimus-eluting and sirolimus-eluting coronary stents in routine clinical care (SORT OUT III): a randomised controlled superiority trial. Lancet 2010; 375: 1090–99.
6 Camenzind E, Wijns W, Mauri L, et al. Stent thrombosis and major clinical events at 3 years after zotarolimus-eluting or sirolimus-eluting coronary stent implantation: a randomised, multicentre, open-label, controlled trial. Lancet 2012; 380: 1396–405.
7 Raber L, Wohlwend L, Wigger M, et al. Five-year clinical and angiographic outcomes of a randomized comparison of sirolimus-eluting and paclitaxel-eluting stents: results of the Sirolimus-Eluting Versus Paclitaxel-Eluting Stents for Coronary Revascularization LATE trial. Circulation 2011; 123: 2819–28.
8 Jensen LO, Thayssen P, Christiansen EH, et al. 2-year patient-related versus stent-related outcomes: the SORT OUT IV (Scandinavian Organization for Randomized Trials With Clinical Outcome IV) Trial. J Am Coll Cardiol 2012; 60: 1140–47.
9 Stefanini GG, Kalesan B, Serruys PW, et al. Long-term clinical outcomes of biodegradable polymer biolimus-eluting stents versus durable polymer sirolimus-eluting stents in patients with coronary artery disease (LEADERS): 4 year follow-up of a randomised non-inferiority trial. Lancet 2011; 378: 1940–48.
10 Christiansen EH, Jensen LO, Thayssen P, et al. Biolimus-eluting biodegradable polymer-coated stent versus durable polymer-coated sirolimus-eluting stent in unselected patients receiving percutaneous coronary intervention (SORT OUT V): a randomised non-inferiority trial. Lancet 2013; 381: 661–69.