spinal gliosarcoma: a light, immunohistochemical and ... · of the literature, the light,...
TRANSCRIPT

ANNALS O F CLINICAL AND LABORATORY SCIEN CE, Vol. 25, No. 3 Copyright © 1995, Institu te for Clinical Science, Inc.
Spinal Gliosarcoma: A Light, Immunohistochemical and Ultrastructural Study*
PER H. B. CARSTENS,G. STEPHAN JOHNSON, M.D., Ph.D.,*
and LAWRENCE F. JELSMA, M.D.§
fDepartm ent o f Pathology, University o f Louisville School o f Medicine,
Louisville, KY 40292 and
Departments o f tPathology and §Neurosurgery Audubon Regional Medical Center,
Louisville, KY 40292
ABSTRACT
Gliosarcomas are mixed tumors of the brain containing both m alignant neuroectoderm al and m esenchym al components. Over 100 cases have been reported w ithin the brain; however, to our knowledge, this is the first reported case located primarily w ithin the spinal cord. Along with a review of the literature, the light, immunohistochemical and ultrastructural findings of a spinal gliosarcoma are reported in a 41-year-old woman with a previously diagnosed oligodendroglioma of the cerebellum 15 years earlier and a concurrent pituitary adenoma. The spinal tumor appears to be morphologically identical to its intracranial counterpart.
Introduction
Extragonadal tum ors w hich contain both m alignant epithelial and m esenchym al e lem en ts are e n co u n te red in fre quently. These tumors are classified as carcinosarcomas or mixed tumors. W ithin the central nervous system, the concept of gliosarcoma (GS) or mixed glioma and sarcoma was accepted after the publication of three such cases by Feigin and Gross in 1955.1 The term gliosarcoma is
* Send reprin t requests to: Per H. B. Carstens, M.D., D epartm ent of Pathology, M edical D ental Research Building #208, University of Louisville, Louisville, KY 40292.
attributed generally to Stroebe, who first used the term in an article in 1895.2 For a tumor to be classified as a GS, it has to be composed of two distinct m alignant cell populations. The glial com ponent shows positive immunoreactivity for glial fibrillary acidic protein (GFAP) and the sarcom atous cells are invested by reticu lin fibers .3 Most commonly, the glial component is a glioblastoma multiforme (GBM), but the sarcomatous elem ents may vary although the histological picture is frequently one of fibrous histiocytoma .4 ,5 ,6 ,7
Gliosarcoma is 2 to 8 percent as frequent as glioblastoma m ultiform e ; 7 ,8 currently, there are well over 1 0 0 cases described in the literature. In a recent study, no sig
2410091-7370/95/0500-0241 $00.90 © Institute for Clinical Science, Inc.
242 CARSTENS, JOHNSON, AND JELSMA
nificant difference was found betw een GS and GBM w ith regard to age, gender, tumor location w ithin the brain, size, and survival. 7 The clinical and morphological features of a spinal GS developing in a 41 year old wom an who had been previously d iagnosed and trea ted (15 years earlier) for an oligodendroglioma of the cerebellum are reported here.
Materials and M ethods
In 1973, at age 26, the p a tien t was treated for an oligodendroglioma of the cerebellum by surgical removal that was followed by radiation therapy and a shunt operation at the National Naval Medical C enter Bethesda, Maryland.
T h ir te e n years la te r in 1986, th e patient underw ent decom pressive laminectomy (T- 6 to L-2) for adhesive arachnoiditis and paraplegia. Shortly thereafter, a one centim eter pituitary adenoma w ithout ev idence of recurrence of the cerebellar tum or was discovered by magnetic resonance imaging. Treatm ent for the pituitary adenom a was determ ined to be unnecessary.
In 1988, at age 41 and 15 years after the removal of the oligodendrogliom a, the p a tie n t u n d e rw en t lam inectom y w ith subtotal resection of a cystic intraspinal sausage-like tum or which filled the spinal canal from T-12 to L-2 and appeared to have arisen from the ventral surface of the spinal cord. The morphological m ateria l for th is rep o rt derives from this operation . T he p a tie n t rece iv ed post operative radiation therapy. Less than a year a fte r th e rem oval o f th e sp inal tumor, the patient had increased pain in the left flank, for which she underw ent open thoracic cordotomy. Com puterized tom ography of th e pe lv is rev ea led a large, in traspinal tum or in the lum bar sacral canal extending beyond the neural canal an terio r to the sacrum into the low er pelvis. Again there was no evidence of recurrence of the cerebellar
tumor. The patient died two months after the cordotomy. An autopsy was not performed. The pa tien t d id not have any family history of m ultiple tumor syndrome.
Small pieces of tissue for morphological examination w ere available from the 1988 resection o f the thoracic lum bar tumor. These w ere formalin fixed, paraffin em bedded and stained w ith hem atoxylin and eosin and W ilder’s reticulin sta in . T h e sam e paraffin e m b e d d e d blocks w ere used for immunohistochem- istry w ith a n tise ra aga in st v im en tin , glialfibrillary acidic protein (GFAP)* and S-100 p ro te in .! Im m unoreactivity was revealed by the avidin-biotin complex (ABC) m ethod9 with appropriate positive and negative controls. Tissue for electron microscopy was fixed in 3 percent glutar- aldehyde, post fixed in 1 percent osmium tetroxide, and em bedded in plastic. Thin sections were stained w ith uranyl acetate and lead citrate.
Results
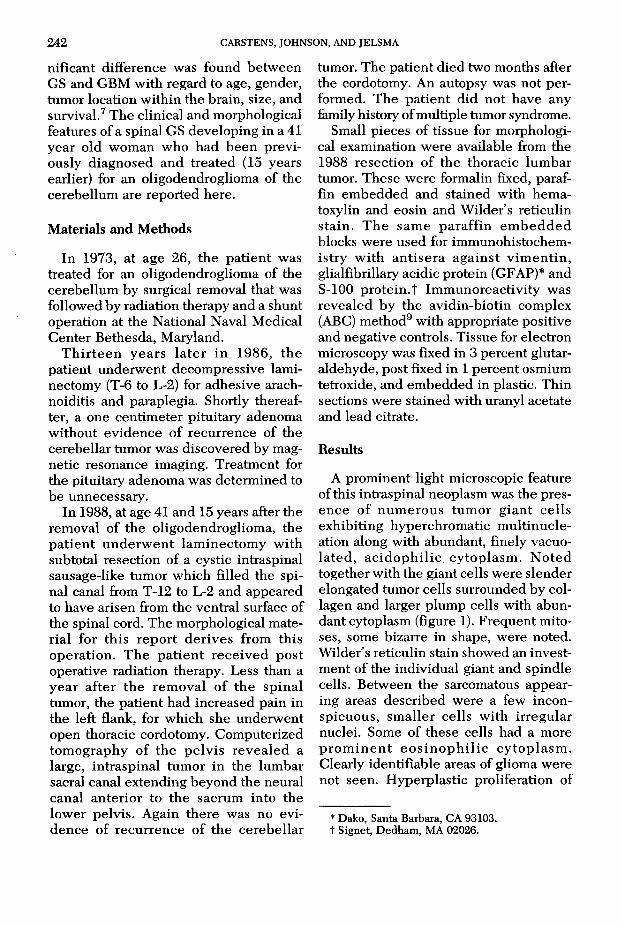
A prom inent light microscopic feature of this intraspinal neoplasm was the presence o f num erous tum or g ian t cells exhibiting hyperchrom atic m ultinucle- ation along with abundant, finely vacuola te d , a c id o p h ilic cy top lasm . N o ted together with the giant cells were slender elongated tum or cells surrounded by collagen and larger plum p cells with abundant cytoplasm (figure 1). F requent mitoses, some bizarre in shape, were noted. W ilder’s reticulin stain showed an investm ent of the individual giant and spindle cells. Between the sarcomatous appearing areas described w ere a few inconspicuous, sm aller cells w ith irregu lar nuclei. Some of these cells had a more p ro m in e n t e o s in o p h il ic cy to p la sm . Clearly identifiable areas of glioma were not seen. H yperplastic proliferation of
* Dako, Santa Barbara, CA 93103. t Signet, Dedham, MA 02026.
SPINAL GLIOSARCOMA 243
ments were noted in addition to large numbers of mitochondria. The nuclei of all the tumor cells were highly irregular w ith p rom inen t he terochrom atin and nucleoli and frequent nuclear bodies. C ellu lar junctions w ere not p resen t. Osteoblastic, chondroblastic, or rhabdo- m yom atous d if fe re n tia tio n was n o t noticed. Degeneration and necrosis with surrounding inflam m atory cells w ere prom inent in the tissue subm itted for electron microscopy.
Discussion
In our report of a spinal GS, the m esenchymal portion of the tumor was characterized by reticulin investment of the individual tumor cells, vimentin immu-
FlG URE 1. Photom icrograph show ing several large and irregular m ultinucleated giant cells. Also noted are elongated and plum p cells with abundant cytoplasm (hematoxylin-eosin, original magnification x300).
endothelial cells of small blood vessels was noted. Areas of degeneration and necrosis were widespread.
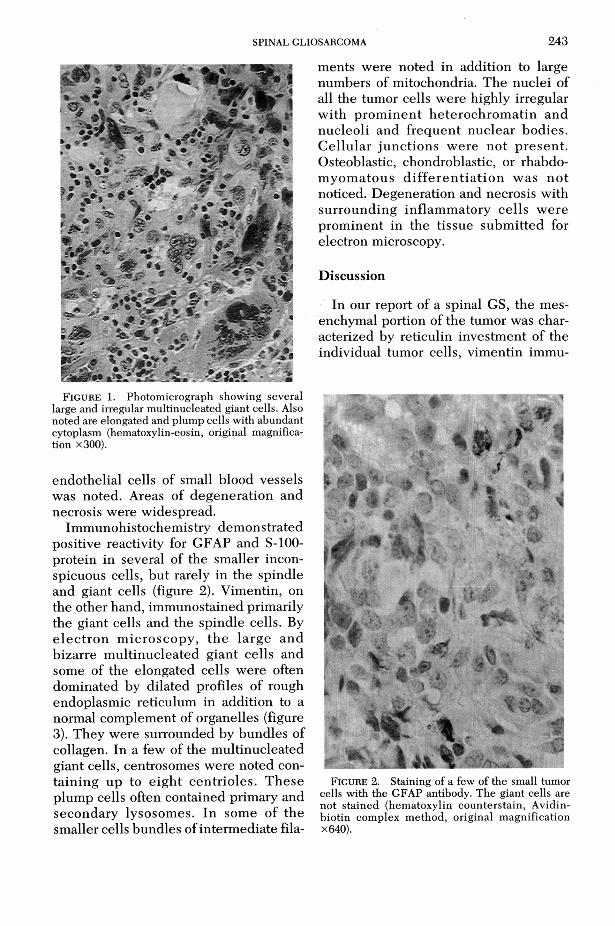
Im m unohistochem istry dem onstrated positive reactivity for GFAP and S-100- protein in several of the smaller inconspicuous cells, but rarely in the spindle and giant cells (figure 2). Vimentin, on the other hand, immunostained primarily the giant cells and the spindle cells. By e le c tro n m icroscopy , th e large and bizarre m ultinucleated giant cells and some of the elongated cells were often dom inated by dilated profiles of rough endoplasmic reticulum in addition to a normal complement of organelles (figure 3). They were surrounded by bundles of collagen. In a few of the m ultinucleated giant cells, centrosomes were noted contain ing up to e igh t cen trio les. These plum p cells often contained primary and secondary lysosom es. In some of the smaller cells bundles of interm ediate fila
FlGURE 2. Staining of a few of the small tumor cells with the GFAP antibody. The giant cells are no t sta ined (hem atoxylin countersta in , Avidin- b io tin com plex m ethod, original m agnification X640).

244 CARSTENS, JOHNSON, AND JELSMA
FIGURE 3 . E le c tr o n m icro g ra p h s h o w in g b in u c le a te d g ia n t c e l l w ith d i la te d p r o f ile s o f ro u g h e n d o p la s m ic r e t ic u lu m a n d a n u c le a r b o d y (o r ig in a l m a g n ific a tio n x4,500).
nopositive and GFAP immunonegative features of the giant cells and the ultra- struc tu ra l find ings. This portion had some sim ilarity to a m alignant fibrous histiocytoma. The isolated small cells, which were positive for GFAP and possessed interm ediate filaments, indicated that a small portion of this tumor was a glioma, most likely a glioblastoma multiforme (GBM).
The presence of a mixture of GBM and sarcoma in a nervous system tumor could represent either a tumor arising from a high grade GBM with malignant transformation of the mesenchymal component into a sarcoma,10 or it could indicate the invasion of a primary meningeal sarcoma or malignant meningioma into the brain, which initially incites a hyperplastic neuroglial reaction that eventually undergoes a m alignant transformation into a GBM.11,12 In the first and most common situation, the mixed tum or is called a gliosarcoma (GS); in the latter, it is called
a sarcoglioma which morphologically is characterized by an inner core of sarcoma su rro u n d e d by a p e r ip h e ra l rim of glioma. The tumor described by us did not have this appearance, but consisted of a haphazard mixture of glioma and sarcoma; therefore, it belongs to the GS category. Gliosarcoma can be separated from g ian t ce ll g liob lastom a by the re ticu lin enclosure of the ind iv idual malignant mesenchymal cells just as the presence of GFAP and interm ediate filaments in GS indicate that the tumor is more than a primary or secondary sarcoma of the brain.
The possible origin of the sarcomatous com ponen t has caused c o n sid e rab le speculation. With the prom inent vascular proliferation present in GBM, it is not su rp rising that an en d o th e lia l orig in should be considered.1,10 Feigin e t al visualized a spectrum of changes ranging from slight vascular endothelial hyperplasia to infiltrating sarcoma extending from the hyperplastic blood vessels. In an immunohistochemistry study,13 Factor VIII related antigen was positive not only in all endothelial cells bu t also in a few scattered cells, including giant cells in the sarcomatous areas. Another study14 demonstrated intense cytoplasmic staining for U lex E u ropeus a g g lu tin in 1 (UEA-1) in a num ber of sarcom atous cells, and W eibel-Palade-like bodies were noted in both vascular endothelial and adjacent sarcoma cells. O ther more recent studies, however, failed to identify the p resence of Factor V III and U E A -1 o u t s i d e th e e n d o t h e l i a l cells4,5,15,16,17,18 or the presence of Wei- bel-Palade bodies in the sarcoma cells outside the blood vessels.6 The endothelial cell has, therefore, been abandoned as the cell of origin for the sarcomatous com ponent. M ore recen t specu la tion about the histogenesis of the sarcomatous component has centered on undifferentiated mesenchymal cells.4 It may be of interest at this point to note that it is often

SPINAL GLIOSARCOMA 245
more useful to classify neoplasms on the basis of appropriate phenotypic differen tia tion m arkers, ra ther than on the basis of questionable assumptions about their origins . 19
The admixture of neoplastic epithelial and mesenchymal cells, w hich have been no ted in carcinosarcom a and gliosar- coma, have been explained as occurring by three different m echanism s .20 First of all, the epithelial neoplasm m ight induce a benign (pseudosarcomatous) reaction in the connective tissue. Secondly, two spatially distinct neoplasm s representing a carcinoma and a sarcoma m ight eventually grow close enough to m ingle and form a collision tumor. Finally, a single m alignant clone can have the sim ultaneous capacity for both epithelial and m esenchym al d ifferen tia tion and thus form a composite tumor. It is difficult to accept the “pseudosarcomatous reaction” as being benign w hen both the glioma- tous as well as sarcomatous portions are represented in the m etastases . 11 Collision tum ors do occur, b u t very infreq u en tly . 21 T his leaves th e com posite tumor explanation as the most likely for the majority of GS.
The proportion of the gliomatous versus sarcom atous com ponents can vary considerably in GS from those cases in which the first biopsy revealed GBM and only tissue from later stages of the tumor showed additional sarcoma8 ,1 4 to those cases, such as ours, in which the gliomatous portion could be recognized only by im m unohistochem istry .5 In the former in stance , th e a d d itio n a l sarcom atous tissue was mostly ( 8 of 1 2 patients) discovered fo llow ing surgery , rad ia tion therapy, and/or chemotherapy. Our patient underwent decompressive laminectomy in the same region of the spinal cord two years before the GS was diagnosed.
O ur patient appeared to have a propensity for developing tumors of the nervous system. I t is highly unlikely that the GS is a m etastasis from the cerebellar oligo
dendroglioma which was diagnosed and treated 15 years previously. No area of the spinal GS had morphologic similarity to an oligodendroglioma. There is, however, a report of a GS where the gliomatous portion was an oligodendroglioma of the temporal lobe with an angiosarcoma- tous com ponent; four months later, an intramedullary and subdural GS was discovered .2 2 To our knowledge, our case is the first GS occurring prim arily in the spinal cord.
Finally, it is of in terest to note that m ultiple intracranial tumors of different histologic types have been described . M anuelidis and Solitare23 review ed intracranial tumors associated w ith GBM. T hey found th a t a fte r m en ing iom as, p i tu i ta ry ad en o m as w ere m o st f re quently noted in association w ith GBM and that m u ltip le tum ors overw helm ingly occurred concurrently. Our patient had a small pituitary adenoma discovered one and one half years before the GS was diagnosed.
Acknowledgem ent
Thanks are extended to Dr. Rose Dagirmanjian for reviewing the manuscript and to Mrs. Lucille O. Chann for excellent secretarial assistance.
References
1. Feigin IH , Gross SW. Sarcoma arising in glioblastoma of the brain. Am J Pathol 1955;31: 633-53.
2. Stroebe H. U eber E ntstehung und bau der gehirngliom e. Beitr Pathol Anat Allg Pathol 1895;18:405-86.
3. Meis JM, Ho KL, Nelson JS. Gliosarcoma: A histologic and im munohistochemical reaffirmation. Mod Pathol 1990;3:19-24.
4. Grant JW, Steart PV, Aguzzi A, Jones DB, Gallagher PJ. Gliosarcoma: an im m unohistochem ical study. Acta Neuropathol 1989;79:305-9.
5. Ng HK, Poon WS. Gliosarcoma of the posterior fossa w ith features of a m alignant fibrous histiocytoma. Cancer 1990;65:1161-6.
6. Ho KL. H istogenesis of sarcomatous compon en t o f th e gliosarcom a: an u ltrastructu ra l study. Acta Neuropathol 1990;81:178-88.
7. Meis JM, Martz KL, Nelson JS. Mixed glioblastoma multiforme and sarcoma. A clinicopatho-
246 CARSTENS, JOHNSON, AND JELSM A
logic study of 26 radiation therapy oncology group cases. Cancer 1991;67:2342-9.
8. Morantz RA, Feigin I, Ransohoff J. Clinical and pathological study of 24 cases of gliosarcoma J. Neurosurg 1976;45:398-408.
9. Hsu SM, Raine L, Fänger H. Use of avidin- biotin-peroxidase complex (ABC) in immuno- peroxidase techniques: A comparison betw een ABC and u n lab e led an tibody (PAP) p rocedures. J H istochem Cytochem 1981;29;577-80.
10. Feigin I, Allen LB, L ipkin L, Gross SW. The endothelial hyperplasia of the cerebral blood vessels w ith brain tum ors, and its sarcomatous transformation. C ancer 1958;11:264-77.
11. Smith DR, Hardm an JM, Earle KM. Contiguous glioblastoma m ultiform e and fibrosarcoma with extracranial metastasis. Cancer 1969;24:270-6.
12. Lalitha VS, R ubinstein LJ. Reactive glioma in intracranial sarcoma: A form of mixed sarcoma and glioma (“ sarcogliom a” ). Report of eigh t cases. Cancer 1979;43:246-57.
13. Schiffer D, G iordana MT, Mauro A, Migheli A. GFAP, FVIII/RAg, Laminin, and Fibronectin in gliosarcom as: An im m unoh istochem ica l study. Acta Neuropathol 1984;63:108-16.
14. Slowik F , Je llinger K, Gas zo L, F ischer J. G liosarcom as: h is to lo g ica l, im m u n o h is to chem ical, u ltrastructural, and tissue culture studies. Acta Neuropathol 1985;67:201-10.
15. McComb RD, Jones TR, Pizzo SV, Bigner DD. Im munohistochem ical detection of factor V III/ von W illibrand factor in hyperplastic endothelial cells in glioblastoma multiforme and mixed gliosarcoma. J Neurological Exp Neurol 1982; 41:479-89.
16. Kishikawa M, Tsuda N, Fujii H, Nishimori I, Yokoyama H , Kihara M. Glioblastoma w ith sar
comatous com ponent associated w ith myxoid change. A histochem ical, im munohistochemical and electron microscopic study. Acta N europathol 1986;70:44-52.
17. Kochi N, Budka H. Contribution of histiocytic cells to sarcomatous developm ent of the gliosarcoma. An immunohistochemical study. Acta N europathol 1987;73:124—30.
18. Banerjee AK, Sharma BS, Kak VK, Ghatak NR. Gliosarcoma w ith cartilage formation. Cancer 1989;63:518-23.
19. G ould VE. H istogenesis and differentiation: A re-evaluation of these concepts as criteria for the classification of tumors. Hum Pathol 1986; 17:212-5.
20. Goldman RL, W eidner N. Pure squamous cell carcinom a of the larynx w ith cervical nodal metastasis showing rhabdomyosarcomatous differentiation. Clinical, pathologic, and im munohistochem ical study of a unique example of d ivergen t differentiation. Am J Surg Pathol 1993;17:415-21.
21. Mayo CM, Barron KD. C oncurrent glioma and primary intracranial sarcoma. A report of two cases and a review of the literature. N eurol 1966;16:662-72.
22. Pasquier B, Couderc P, Pasquier D, Panh MH, N ’G olet A. Sarcoma arising in o ligodendroglioma of the brain. A case with intram edullary and subarachnoid spinal m etastases. C ancer 1978;42:2753-8.
23. M anuelidis E E , Solitare GB. Glioblastoma m ultiforme. In: M inckler J, editor. Pathology of the nervous system. New York: McGraw-Hill Book Company, 1971:2050-1.