specifying the neuropsychology of affective disorders
TRANSCRIPT

REVIEW
Specifying the Neuropsychology of Affective Disorders:Clinical, Demographic and Neurobiological Factors
Thomas Beblo & Grant Sinnamon & Bernhard T. Baune
Received: 29 November 2010 /Accepted: 24 May 2011# Springer Science+Business Media, LLC 2011
Abstract Neuropsychological research in patients withaffective disorders shows heterogeneous results with regardto the severity and profile of cognitive impairments. In thispaper we hypothesize that the investigation of clinical(subtypes, comorbidity, traumatization, personality, severity,diurnal swings, course, duration, age of onset, biasedprocessing, rumination, motivation, experience of failure,sleep, suicidal tendencies, computer attitudes), demographic(age, education, gender) and neurobiological factors(structural and functional brain changes, glucocorticoids,medication, ECT) that are related to cognitive perfor-mance has specified the understanding of severity andprofile of neuropsychological impairments. We reviewedthe literature pertaining to clinical, demographic andneurobiological factors following Pubmed and PsychInfodatabases using different combinations of general key-termsincluding “Affective Disorder,” “Depression,” “Mania,”“Neuropsychological,” “Neurobiological,” “Moderator,”and “Review” as well as more specific demographic, clinicaland neurobiological search terms. Findings from the literatureshow that the consideration of these factors has improvedknowledge about the severity of neuropsychological impair-
ments in patients with affective disorders whereas theneuropsychological profile is still poorly understood. Despitelimited understanding, however, the existent results providepromising suggestions for the development of treatmentprograms.
Keywords Neurocognition . Depression .Mania .
Neuroimaging . Intervention
Introduction
Affective disorders are highly prevalent with a lifetimeprevalence of 15% for major depression disorder (MDD)within the general population (Wittchen 1994). Apart fromsymptoms of impaired mood, affective disorders arecharacterised by additional emotional, psychological,behavioural, physical, and cognitive symptoms such asneuropsychological dysfunction. According to the Diag-nostics and Statistical Manual of Mental Disorders, FourthEdition (DSM-IV; American Psychiatric Association A. P.1994) and the International Classification of Diseases(ICD-10, WHO 1991), cognitive symptoms of MDD arecharacterised by reduced abilities to concentrate and impaireddecision-making processes, and in the case of mania, flight ofideas, increased distractibility, and continuous change of plansand activities.
For more than 50 years, neuropsychologists haveattempted to understand neuropsychological dysfunctionin depression (Kiloh 1961; Madden et al. 1952). Inparticular, much research has focused on differentiatingdepression from dementia. In addition, neuropsychologicalprofiling of mood disorders also has a close link to basicscience in that patterns of neuropsychological dysfunctionmight closely relate to neurobiological dysfunction which
T. Beblo (*)Department of Research, Evaluation and Documentation,Clinic of Psychiatry and Psychotherapy Bethel,Ev. Hospital Bielefeld, Remterweg 69-71,33617 Bielefeld, Germanye-mail: [email protected]
T. BebloDepartment of Psychology, University of Bielefeld,Bielefeld, Germany
G. Sinnamon : B. T. BauneDepartment of Psychiatry, University of Adelaide,Adelaide, SA 5005, Australia
Neuropsychol RevDOI 10.1007/s11065-011-9171-0

in turn could contribute to an improved understanding ofmood disorders (Keefe 1995). More recently, authorsemphasised that neuropsychological deficits contribute tothe long-term functional outcome of patients with affectivedisorders. In fact, neuropsychological impairment ofdepressed patients has been associated with a reducedlevel of psychosocial and occupational functioning whichremained when statistical analyses controlled for furtherdepressive symptoms. This association has also beenfound among depressed patients in remission withpersistent neuropsychological impairment (Baune et al.2010; Jaeger et al. 2006; Martinez-Aran et al. 2007;Martino et al. 2009; Mur et al. 2009; Wingo et al. 2009).The association between neuropsychological dysfunctionand psychosocial impairment appears to be more promi-nent in patients with mood disorders than in patients withschizophrenia (Brissos et al. 2008). Another clinicalproblem of untreated neuropsychological deficits indepressed patients is that these patients tend to show lesscompliance with antidepressant treatment (Martinez-Aranet al. 2009). Furthermore, patients with cognitive deficitsmay show an increased risk for suicide (Westheide et al.2008). Given the high clinical relevance of neuropsycho-logical deficits, effective neuropsychological treatmentstrategies are needed. The first interventional studies usedtreatment strategies that were originally developed forbrain damaged patients (Elgamal et al. 2007; Naismith etal. 2010; Trebo et al. 2007). The results raised hope thatcognitive deficits in affective disorders are successfullytreatable. However, a better understanding of neuropsy-chological impairment in affective disorders may help todevelop specific and more effective treatment programs.
By now, a huge number of studies have investigatedneuropsychological performance in depressed patients.Studies using large neuropsychological test batteriesdocument neuropsychological impairment in depressedpatients primarily in the areas of attention, executivefunction, and memory (Beblo and Lautenbacher 2006). Inthe domain of attention, impairments of selective attention,divided attention, and vigilance have been reported.However, it is still a matter of debate whether depressedpatients show cognitive slowing. Christensen et al. (1997)conclude from their meta-analysis that depressed patientsshow impaired performance on timed tasks, but it remainsunclear whether this impairment is due to a slowing ofcognitive processing or, alternatively, has to be regardedas a consequence of the increased rumination that isregularly reported among patients with depression. It hasalso been suggested that patients with MDD primarilyshow deficits in “effortful tasks” (Porter et al. 2007). Ascompared to automatic processing effortful processingrequires increased attentional and executive resources(Hasher and Zacks 1979). However, results have been
controversial (Christensen et al. 1997; Degl'Innocenti andBäckman 1999; Den Hartog et al. 2003; Hammar et al.2011).
Reduced executive functioning has been consistentlyreported in depression, with deficits particularly evidentin the domains of cognitive flexibility and verbalfluency. With respect to word fluency, research showsthat category naming (e.g. animals) is more heavilyaffected than letter fluency (e.g. words beginning withthe letter “S”; Henry and Crawford 2005). Reducedcognitive flexibility has also been found to contribute toimpaired decision-making processes (Cella et al. 2009)and to be closely related to impaired empathy (Shamay-Tsoory et al. 2009). In addition to deficits in cognitiveflexibility, several studies have reported deficits incomplex executive functions such as working memory,cognitive planning, problem-solving, and conceptualisa-tion (Beblo and Lautenbacher 2006).
An additional domain of impaired cognitive function indepression is related to explicit memory function. Theseimpairments do not only affect the reproduction of learneditems since a reduced specificity of autobiographicalmemories, known as general autobiographical memories,has also been reported (Hermans et al. 2008). Therehave been several attempts to explain memory deficits asa result of impaired attention or impaired effortfulprocessing; however, the general view is that memorydeficits go beyond attention dysfunction. Furthermore, itremains somewhat unclear in the current research as towhether dysfunction of implicit memory and short-termmemory form part of an impaired neuropsychologicalprofile in depression. In addition to the already reportedreduced abilities in attention, executive function andmemory, studies have shown visuospatial deficits indepression; however, several researchers have suggestedthat these findings are less definite (Austin et al. 1992;Pálsson et al. 2000).
Estimations of the degree of cognitive impairments indepression indicate a statistically moderate magnitude ofcognitive impairment. In a meta-analysis by Christensenet al. (1997), a deficit in cognitive function of, onaverage,−0.63 standard deviations below that of healthycontrols has been reported in patients with depression.This degree of cognitive impairment in depressed patientsis in line with studies from our group (e.g. Beblo et al.1999, 2010; Lahr et al. 2007), in which we found that themost impaired cognitive performance (flexibility) wasmore than one standard deviation lower (z −1) than thehealthy controls’ performance (Beblo et al. 1999).Gualtieri and Morgan (2008) found that patients withmood disorders may, on average, exhibit mild to moderateneuropsychological impairment. However, they reportthat 21% of patients with unipolar depression and 30%
Neuropsychol Rev

of patients with bipolar disorder demonstrate severe andclinically relevant impairment (defined as test perfor-mance at least two standard deviations below normativevalues) in at least two cognitive domains which is onlyfound in 4% of healthy controls.
While a large number of studies have been carried out toinvestigate neuropsychological deficits in depression, rela-tively little neuropsychological research has been con-ducted in mania. Although similar neuropsychologicaldeficits occur in depression and mania (Murphy andSahakian 2001), other researchers such as Gauggel et al.(Gruber et al. 2007; Rathgeber and Gauggel 2006) andGunning-Dixon et al. (2008) demonstrated that patientswith mania may suffer from more prominent neuropsycho-logical deficits, especially in the area of executive function.Overall, the results of neuropsychological comparisons ofmanic and depressed patients are inconsistent since somestudies also showed that performance of certain neuro-psychological functions was worse in depressed patientscompared to manic patients. Murphy et al. (1999)compared manic patients with bipolar type I disorder topatients with MDD and healthy controls. In a go/no-goparadigm, depressed patients showed increased reactionlatencies when flexibility was required, as opposed tomanic patients who showed an overall increase in thenumber of errors (reduced reaction inhibition) andomissions (impaired attention). Furthermore, both patientgroups demonstrated a variety of non-specific neuropsy-chological deficits. Other studies confirmed prominentinhibition deficits among manic patients (Larson et al.2005; McGrath et al. 1997).
In summary, neuropsychological studies with depressedand manic patients present heterogeneous results. Somepatients demonstrated no or only slight impairment inneuropsychological function whereas other patients showedperformances of more than two standard deviations belownormative values in a variety of neuropsychologicaldomains such as attention, executive functions, andmemory. It is, therefore, not surprising that authors ofreviews came to different conclusions. On the basis of ameta-analysis, Veiel (1997) outlined that patients withMDD show diffuse neuropsychological impairments withprominent deficits in cognitive flexibility. Castaneda et al.(2008) came to similar conclusions and suggested primarilyexecutive dysfunctions in depressed patients. By contrast,Zihl and Münzel (2004) suggested that executive dysfunc-tions in general and impairments in cognitive flexibility inparticular were rare in depressed patients. The results ofChristensen’s quantitative review (Christensen et al. 1997)showed dominant impairments of depressed patients in thedomains of perceptual-auditory tasks, memory and atten-tion/tracking. Drevets et al. (2008) and Porter et al. (2007)concluded that studies about the neuropsychology of
affective disorders have produced discrepant results andElderkin-Thompson et al. (2004) reasoned that patientswith MDD do not exhibit specific neuropsychologicalimpairments.
The heterogeneity of results of original research and thediffering conclusions of recent reviews make clear that theattempt to establish a specific neuropsychological charac-terization of patients with affective disorders has failed. Toovercome this failure, different authors (e.g. Beblo andHerrmann 2000; Porter et al. 2007) have suggested a morefocused investigation of the relationship between affectivedisorders and neuropsychology by defining the specificfactors that are found to influence cognitive performance.Some authors summarized evidence for the impact of singlefactors. Balanza-Martinez et al. (2010), for instance,focused on comorbidities and medication of patients withbipolar disorder. They pointed out that their neuropsycho-logical performance is probably worsened by comorbidalcohol dependence, even in the remitted state, and byantipsychotic medication. Schlosser et al. (2011) suggestedthe hypothalamus–pituitary–adrenal (HPA) axis as animportant neurobiological determinant of cognitive impair-ment in depression. Although many inconsistencies werereported, the authors stated that at least 70% of the studiesreviewed indicated an association between excessive baselinesecretion of glucocorticoids or reduced negative feedback andimpairment in visual/verbal memory, working memory andexecutive function in patients with MDD. Only very fewauthors have tried to assemble the most relevant factors thatmay have an impact on cognitive functioning in patients withaffective disorders. Porter et al. (2007) discussed clinicalfeatures (severity and diurnal variations, melancholia, inpa-tient status, psychosis, uni- vs bipolar depression, comorbid-ities, medication), age, and gender. In addition, theydescribed factors with possible causal influence on cognitivefunctioning such as frontostriatal abnormalities, HPA Axisfunctioning and hippocampus structure, as well as psycho-logical factors (catastrophic reactions to failure, effortfulprocessing, mood-related attentional bias). However, theirreview was limited to patients with MDD and some factorsthat are currently regarded as being of great importance weremissing (e.g. rumination).
It is not clear from the research to what extent theconsideration of factors that are related to cognitivedysfunctions have improved our knowledge about theneuropsychology of affective disorders. It is the aim of thispaper to give an up-to-date review about those factors. Wehypothesise that the investigation of these factors hasspecified the knowledge about the profile and severity ofneuropsychological impairments in patients with affectivedisorders. In addition, we aimed at structuring and discus-sing the possible relations between these factors andprovide implications for future research.
Neuropsychol Rev

Methods
Pertinent literature search was identified and retrievedsearching PubMed and PsycINFO databases coveringarticles from 1980 to 2011. The following selectedkeywords were used: “Affective Disorder,” “Depres-sion,” “Mania,” “Neuropsychological,” “Moderator,”“Neurobiology,” “Review” as well as more specificterms such as “subtypes,” “comorbid,” “severity,” “diur-nal variation,” “course,” “duration of illness,” “age,”“onset,” “bias,” “motivation,” “rumination,” “failure,”“MRI,” “PET,” “DTI,” “cortisol,” “default mode net-work,” “structural brain changes,” “functional brainabnormalities,” “connectivity,” “neuronal networks,” “medi-cation,” “ECT.” Additional articles were identified byreviewing reference lists of reviews and research articlesand, where appropriate, included in the review. These articleswere evaluated for inclusion/exclusion according to relevanceof specific moderators (diagnostic subtypes, symptom sever-ity, age, psychological factors, medication and ECT, gender,suicidality, education, neurobiological factors) of neuropsy-chological performance in mood disorders (uni- and bipolardisorders) yielding 208 references finally included in thisreview.
Results
Clinical and Demographic Factors Being Relatedto Neuropsychological Performance
Several clinical and demographic factors are found toinfluence the profile and the severity of neuropsychologicaldeficits of patients with mood disorders. A summary ofsuch factors is presented in Table 1.
Subtypes of Mood Disorders and Co-morbidity
Subtypes The DSM-IV and ICD-10 classification systemsof psychiatric disorders provide a system of diagnostic sub-types in order to capture the various differential presenta-tions of mood disorders. It is not surprising that complexmood disorders tend to be associated with more severeneuropsychological deficits. For example, existing researchdemonstrates that bipolar disorder patients show strongerneuropsychological deficits compared to unipolar depressedpatients (Burt et al. 2000). However, results are somewhatinconsistent among the literature as research has also shownthat neuropsychological deficits are similar between bipolarand unipolar depressed patients or that differences inneuropsychological functioning rather relate to the profileof neuropsychological deficits (Taylor Tavares et al. 2007).Among bipolar patients, patients with bipolar disorder Type
I demonstrated stronger neuropsychological impairmentcompared to patients with bipolar disorder Type II (Hsiaoet al. 2009; Torrent et al. 2006). Along these lines, otherstudies have shown that patients with MDD have moresevere neuropsychological deficits compared to those withdysthymia (e.g. Pálsson et al. 2000). The view that sub-types of depression with additional psychopathologicalsymptoms are associated with poorer neuropsychologicalfunctioning, is also supported by research which demon-strates poorer neuropsychological functioning among MDDpatients with the melancholic or psychotic sub-types of
Table 1 Neuropsychological Relevance of Clinical and DemographicalVariables for the Neuropsychological Performance of Patients withAffective Disorders
Variables Neuropsychological relevance
DSM IV subtypes Deficits:
Bipolar > unipolar
Bipolar I > bipolar II
Major depression > dysthymia
Melancholia > no melancholia
Psychotic symptoms > nopsychotic symptoms
Comorbidity With additional alcohol abuseor anxiety more deficits thanwithout
Borderline personality disorder,cannabis use: possiblyirrelevant, attention-deficithyperactivity disorder:possibly relevant
Severity/diurnal swings More deficits in the morning,rather low associations betweendeficits and severity of a certainsub-type of the disorder
Course Less deficits with remission butprobably no complete recovery
Duration of disorder More deficits with the durationand number of episodes andduration of hospitalization
Age More deficits with increasing age
Onset More deficits with late-onset thanearly-onset
Biased Processing Depression: attentional and memorydeficits with itemsof neutral or positive valence
Mania: possibly deficits withitems of neutral or negativevalence
Rumination Negative impact
Experience of Failure Negative impact
Motivation, Sleep, Education,Gender, Suicidal Tendencies,Attitude toward Computers,Traumatization, Personality
Possibly relevant
Neuropsychol Rev

depression compared to patients with MDD without thesesub-type specifiers (Fleming et al. 2004; Martinez-Aran etal. 2008; Michopoulos et al. 2008; Schatzberg et al. 2000).Withall et al. (2010) found for patients with melancholiccompared to patients with non-melancholic subtypes ofMDD not only poorer performance but also a longer timefor neuropsychological recovery.
Comorbidity This field of research generally indicates thatco-morbid psychiatric disorders which have the ability toimpair neuropsychological performance have an additionalnegative impact on neuropsychological functioning indepressed patients (Baune et al. 2009). Unipolar depressionwith a co-morbid anxiety disorder seems to be associatedwith additional neuropsychological impairment comparedto depression without co-morbidity (Basso et al. 2007;DeLuca et al. 2005). Likewise, patients with bipolardepression and comorbid alcohol abuse or dependencyshow increased neuropsychological impairments (Balanza-Martinez et al. 2010). A study by Levy et al. (2008)indicated that not only bipolar patients with current alcoholdependence were more impaired than bipolar patientswithout alcoholism but also that bipolar patients in fullremission from alcohol dependence displayed increasedcognitive deficits. Sanchez-Moreno et al. (2009) foundpreliminarily inhibition deficits among euthymic bipolarpatients with a history of alcoholism. The significance ofalcoholism for the presentation of neuropsychologicaldeficits even seems to outperform the significance of theaffective disorder. Studies with patients who suffer fromalcoholism with or without comorbid depression showedthat cognitive deficits of patients with alcoholism are notexacerbated by comorbid depression (Rosenbloom et al.2005; Uekermann et al. 2003). Cannabis abuse may alsocontribute to neuropsychological dysfunctions in bipolarpatients (Cahill et al. 2006), however, recent studies(Ringen et al. 2010; Secora et al. 2010) suggested noadditional impairment associated with cannabis use inpatients with bipolar disorder. Ringen et al. found inbipolar patients that cannabis abuse was related even toimproved performance whereas the opposite was found forschizophrenic patients.
In a recent study, we compared patients with MDD withand without comorbid Borderline Personality Disorder(BPD; Beblo et al. 2011), patients with BPD only, andhealthy control subjects. The patient groups showed onlyvery little neuropsychological impairments and impair-ments did not add up in patients with both disorders.Likewise, Fertuck et al. (2006) failed to find additionalneuropsychological impairments in MDD patients withcomorbid BPD indicating that BPD might not be relevantfor neuropsychological deficits in patients with affectivedisorders. Affective Disorders also often co-occur with
attention-deficit hyperactivity disorder (ADHD) in childrenand adolescents. In a study of Rucklidge (2006), adoles-cents with bipolar disorder only, showed no seriousneuropsychological impairments. By contrast, those withcomorbid ADHD were particularly impaired in verbalmemory and inhibition. In a similar sample, Gunther et al.(2011) found depressed patients with comorbid ADHD toperform worse in a few attentional measures as compared topatients with depression only. By contrast, patients withADHD and depression did not perform worse than patientswith ADHD only. However, the authors stated that thedifferences between the clinical groups were relativelysmall.
Taken together, affective disorders that imply additionalsymptoms as compared to affective disorders without theseextra symptoms are associated with more severe neuropsy-chological deficits. Some psychiatric comorbidities such asalcoholism, anxiety disorders, and probably ADHD con-tribute to neuropsychological deficits in affective disorderswhereas others, e.g. Borderline Personality Disorder orcannabis use, may have no or only little additional impacton cognitive functioning.
Severity, Diurnal Swings, Course, and Duration of Illness
While a meta-analysis by McDermott and Ebmeier(2009) concludes that some neuropsychological functionssuch as executive function, cognitive processing speed,and episodic memory are associated with the severity ofthe affective disorder, it generally appears that the severityof a certain sub-type of the disorder does not correlatestrongly with neuropsychological test performance (Bebloand Lautenbacher 2006).
Some types of depression, such as melancholic subtypeof MDD, are characterised by diurnal swings, withsymptoms of depression reportedly worse in the morningcompared to the evening. Research investigating neuropsy-chological function in these patients demonstrates neuro-psychological profiles which reflect this diurnal pattern ofdepressive symptoms with poorer neuropsychological per-formance in the mornings compared to the evenings(Moffoot et al. 1994; Porterfield et al. 1997).
The reversibility of neuropsychological impairmentamong patients has been investigated in patients witheuthymia (e.g. Clark et al. 2005) and prospective studies(e.g. Reppermund et al. 2009). During the course of anacute episode of depression, it has been reported thatcognitive deficits improve with remission of the disorder,most likely among young patients (Savard et al. 1980; forreview see Beblo and Lautenbacher 2006; Douglas andPorter 2009). However, these neuropsychological deficitscommonly do not reverse completely and are, therefore, not
Neuropsychol Rev

only regarded as a state but also as a trait-marker of theaffective disorder. Although a clear profile of neuropsy-chological deficits of residual symptoms have not beenclearly identified, some authors such as Douglas andPorter (2009) regard attention and complex executivefunctions as trait-markers of MDD. Several reasons havebeen discussed for persistent cognitive deficits. On the onehand, it has been suggested that neuropsychologicaldeficits form part of residual symptoms of depression orpart of a sub-threshold depression. On the other hand,some studies indicate that neuropsychological impair-ments may sum up over the course of the disorder.Gorwood et al. (2008) showed in a large sample of 8,229MDD patients that memory performance diminished by 2–3% per previous episode of depression (calculated up tofour episodes). Van Gorp et al. (1998) found in bipolarpatients that lifetime months of mania and depression werenegatively correlated with performance in verbal memoryand several executive functions. Correlations between theduration of hospitalisation and severity of neuropsycho-logical deficits support these findings (Christensen et al.1997). Gorwood et al. (2008) conclude from their findingsthat neurotoxic effects on the hippocampus coming fromstress and depression are responsible for diminishedneuropsychological performance which is exacerbatedwith increasing numbers of depressive episodes. Theirresults and conclusions are also in agreement with the“kindling hypothesis” (Post 1992). This hypothesis sug-gests that depressive episodes become progressivelyindependent of external triggers due to neurobiologicalchanges as a consequence of repeated previous stressorsand repeated previous episodes. However, Gorwood’sfindings could also interpreted in a way that a longerhistory of depression indicates a more severe type ofdepression with more prominent cognitive deficits andmore pronounced neurobiological abnormalities (pleasealso see below “Structural Abnormalities and Cortisol”). Inaddition, Delaloye et al. (2010) found no cognitive deficits ina group of elderly euthymic depressed patients with early-onset. Duration of illness was neither related to brainabnormalities nor to neuropsychological performance. Theauthors speculate that not depression itself but associatedfactors such as comorbid substance abuse may lead toneurotoxic effects and to a progressive decline of neuropsy-chological functioning in the course of the disorder.
To sum up, while the subtype of affective disorder iscorrelated with cognitive deficits, these deficits are,surprisingly, not clearly associated with symptom severityof a certain sub-type of the disorder. However, deficits arerelated to diurnal swings with better performances of thepatients in the evening, and the course of the affectivedisorder. Cognitive impairments improve with remissionbut some impairments may remain.
Age and Onset
Neuropsychological deficits associated with depression areobserved predominantly in elderly patients (Beblo andLautenbacher 2006; Christensen et al. 1997). Althoughthese findings have been reported several times, it is unclearwhich domains of neuropsychological functions are pri-marily impaired. Porter et al. (2007) suggested a strongerimpairment of executive function in elderly patients. Bycontrast, Thomas et al. (2009) reported memory deficitsprimarily in elderly, MDD patients, and Castaneda et al.(2008) reported executive function impairment primarily inyounger MDD patients.
Some studies showed that age of onset might be anadditional factor that influences neuropsychological perfor-mance of elderly, depressed patients. The common point ofview suggests structural brain abnormalities and associatedcognitive deficits in patients with late-onset depression ascompared to those with early-onset depression (Drevets etal. 2008; Laks and Engelhardt 2010). These onset-relateddeficits were found in memory functions (Delaloye et al.2010; Dillon et al. 2009) as well as in executive functionsand attention (Rapp et al. 2005). However, compared topatients with late-onset depression, Rapp et al. foundincreased memory problems in patients with recurringearly-onset MDD.
There are several possible explanations for thesefindings. It has been speculated that late-onset geriatricdepression presents a distinct type of affective disorders.Known risk factors for affective disorders such aspersonality abnormalities, a family history of psychiatricillness and dysfunctional past maternal relationships werefound to be less relevant in late-onset MDD (Brodaty etal. 2001) whereas organic factors such as cerebrovasculardisease and associated structural brain abnormalities aremore prominent (Laks and Engelhardt 2010). However,structural brain abnormalities were also found in patientswith early-onset depression. Hickie et al. (2005) andBallmaier et al. (2008), for instance, reported hippocampaldamage also for patients with early-onset depression—although to a smaller extend than in patients with lateonset.
Alternatively, elderly patients with depression may sufferfrom more prominent cognitive deficits as part of amasked, undetected, early stage of dementia (Gualtieriand Johnson 2008). In fact, the risk of developing a seniledementia of the Alzheimer’s type is increased in patientswith depression. Several factors which may contribute tothis increased risk have been discussed. On the one hand,depressive disorders can be regarded as an early symptomof Alzheimer’s disease but on the other hand, neurobio-logical changes related to depressive disorders mayincrease the risk of Alzheimer’s disease. Neuroendocrino-
Neuropsychol Rev

logical research has shown changes of the hypothalamic-pituitary-adrenal axis (HPA axis) in depressed patients asbeing associated with neurotoxic effects, especially in thehippocampus (Paizanis et al. 2007), predisposing to thedevelopment of Alzheimer’s disease (Sotiropoulos et al.2008). Furthermore, physical and mental activity isprotective against Alzheimer ’s disease, most likelythrough the effect of an enhanced neuronal reserve basedon increased neurogenesis (Elder et al. 2006; Mirochnic etal. 2009). This neuroprotective factor might not take effectin depression due to psychomotor-retardation.
In summary, older patients with affective disorders showmore severe cognitive impairments than younger patients,especially those with late-onset depression. It is a still matterof debate which functions are primarily affected. In addition,possible mechanisms are still controversially discussed.
Psychological Factors: Biased Processing of EmotionalInformation, Motivation, Rumination, Response to Failure
Biased Processing Cognitive models of depression such asthe model of Beck (1967) suggest that depressed patientsshow biased processing of emotional information favouringnegative contents. Except for evidence from cognitive andclinical psychology, these assumptions were also confirmedby neuropsychological research. However, although manystudies found a processing bias in the domains ofperception/attention and memory, there were alsoconflicting results.
In a recent review, Gotlib and Joormann (2010) inferfrom the current literature that an attentional bias fornegative information may primarily be evident in laterstages of attentional processing. That is, depressed patientsshow problems to disengage from negative information butdo not necessarily automatically orient their attentiontoward negative stimuli. Rinck and Becker (2005) showedthat MDD patients were more easily distracted by negativewords but did not detect negative words more easily in avisual search task. However, the authors explain thesefindings with methodological characteristics. Apart fromattentional bias toward negative information, Leppanen(2006) summarized evidence for an attentional bias awayfrom positive emotional stimuli.
Since memory performance depends on attention, it isnot surprising that depressed patients may also exhibit anenhanced memory for emotionally negative material.Indeed, Koster et al. (2010) found that dysphoric subjectsshowed an attention bias for negative words, with theattention bias for negative words predicting free recall ofnegative words. Similar to the findings for attentionalperformance, however, a memory bias for negative infor-mation has not been found consistently in patients withdepression. It has been speculated that the bias is more
evident for explicit as compared to implicit memory(Colombel 2007; Gotlib and Joormann 2010). Moregenerally, Gotlib and Joormann suggest the memory biasto be dependent on the elaboration of the stimuli that haveto be studied, that is, memory bias may only occur withdeeper processing. However, results may also be related toother factors. In a group of severely depressed MDDpatients, Ellwart et al. (2003) found a memory bias forimplicit memory but not for explicit memory performance.The authors speculated that results may depend on theseverity of depression with severely impaired patientsactivating depression related information automaticallywithout effortful processes.
While depressed patients process negative informationmore easily, manic patients show a processing bias towardpositive information (Chamberlain and Sahakian 2006). Ina study of Murphy et al. (1999) for instance, depressedpatients had delayed responses for positive stimuli whereasmanic patients had delayed responses for negative stimuli.However, since there are only a few studies with manicpatients, more detailed conclusions about the attentionalbias in manic patients appear to be premature.
Motivation Patients with depression very often reportdiminished drive and motivation which sometimes leadsto the statement in the literature that neuropsychologicaldeficits observed in patients with depression are partly dueto reduced motivation. Contrary to this assumption, it hasbeen observed that patients with depression are wellmotivated during neuropsychological testing. Moreover,patients put themselves under pressure and wish to meetthe expectations of the neuropsychologist during neuropsy-chological testing. Based on these observations, reducedmotivation and decreased neuropsychological functions areinconsistently associated in unipolar depression (Richardsand Ruff 1989; Scheurich et al. 2008). However, motiva-tional deficits seem to be more relevant for cognitivefunction for day-to-day tasks rather than in an artificialneuropsychological testing environment (Lahr et al. 2007).More research is clearly needed to estimate the impact ofmotivation on cognitive performance in depressed patients.
Rumination Rumination is a repetitive pattern of thoughtsfocussing on dysphoric symptoms, their causes andconsequences. Rumination maintains and increases lowmood in non-clinical samples and is related to the onset,severity and chronicity of depression (Donaldson and Lam2004). Apart from its destructive potential for emotionalprocessing, recently it became clearer that rumination alsoaffects further cognitive processing by attracting attention(Donaldson et al. 2007). Indeed, several studies confirmthat rumination has a negative impact on cognitivefunction, particularly on the specificity of the autobio-
Neuropsychol Rev

graphic memory (Crane et al. 2007; Debeer et al. 2009;Raes et al. 2008), inhibition (Philippot and Brutoux 2008),cognitive flexibility (Watkins and Brown 2002), problem-solving (Donaldson and Lam 2004), working memory(Joormann and Gotlib 2008) and attention bias towardsnegative content (Donaldson et al. 2007).
Response to Failure Relative to healthy subjects, MDDpatients are more likely to fail in neuropsychological tasksif they failed in the precedent task. This effect mayprimarily be relevant for response accuracy but not forresponse latency (Elliott et al. 1996). It has been speculatedthat perceived failure trigger “ruminative” thoughts aboutfailure which interfere with task performance or, alternatively,impair motivation (Beats et al. 1996; Elliott et al. 1996).However, in a consequent study Elliott et al. (1997b)demonstrated that depressed patients’ performance did notdecreased following failure but it did not improve. Bycontrast, healthy subjects were able to improve theirperformance after having failed. Results of a recent studyby Douglas et al. (2009) indicated that depressed patientsmay improve their performance after failure as well—but toa lesser extent than healthy participants. Furthermore,depressed patients’ reaction to failure may depend on theaccuracy of feedback: In a study of Murphy et al. (2003)patients with depression showed normal performance whennegative feedback is accurate and informative but animpaired performance when reinforcement contingenciesare misleading or ambiguous.
Taken together, there is evidence for biased informationprocessing in patients with depression and mania. However,for depression an attentional bias for negative stimuli isprimarily detectable for later stages of processing. In addition,depressed patients recall negative information more easilythan neutral or positive information. This bias may increasewith the conscious elaboration of the material. It is still amatter of debate whether motivational deficits account forneuropsychological deficits in depression. By contrast, thereis clear evidence that rumination impairs performance indifferent neuropsychological domains. There are also congru-ent results pertaining to an impaired performance after failingthe preceding task relative to healthy controls. Ruminationand motivational deficits were primarily discussed as possiblemechanisms behind these findings.
Additional Factors
Some studies found an association between suicidality andimpaired executive function in unipolar depressed patients(Dombrovski et al. 2008; Westheide et al. 2008). Thisfinding has implications for the prevention of suicideattempts, although inconsistent results across studies remain
(Roskar et al. 2007). Sleep disturbances often reported bypatients with mood disorders have been suggested toaccount for neuropsychological deficits as reduced sleep isknown to negatively affect cognitive performance (Goder etal. 2007; Naismith et al. 2009). Furthermore, Savitz et al.(2008) found a negative impact of early emotional andsexual trauma on cognitive performance in patients withbipolar disorders. This finding is in line with the study byVythilingam et al. (2002) who reported a reduced hippo-campus volume only in traumatised, MDD patients.
Other factors such as education and gender have alsoshown to be associated with neuropsychological function-ing in patients with mood disorders (Barrett et al. 2008).Depressed patients with lower levels of education tend toperform disproportionately worse in neuropsychologicaltesting compared to education matched control subjects(Avila et al. 2009). It has been speculated that patients withhigher levels of education are in a better position tocompensate for depression-associated neuropsychologicaldysfunction. The relation between gender and neuropsy-chological performance may be moderated by personalitytraits. Van den Heuvel et al. (1996) found in elderly womenthat depression was related to cognitive dysfunctionprimarily in women with a weak internal locus of control.In men, the association between depression and cognitivedysfunction was moderated by neuroticism. The authorsconcluded that low neuroticism or high internal locus ofcontrol act as protective factors against depressive reactionswhen experiencing cognitive dysfunction.
Furthermore, variables related to computer-based taskshave been identified to impact neuropsychological function.Among a sample of depressed patients, Weber et al. (2002)found that a negative attitude towards computers wasrelated to an increased level of nervousness, as well as areduced level of neuropsychological performance whenusing computer-based attention tasks. Such a finding, ifconfirmed, would implicate the (at least additional) use ofpaper-pencil test for assessing depressed patients.
In sum, apart from the above described clinical anddemographic factors, there are more variables that mayinfluence the relation between affective disorders andneuropsychological performance. However, given the smallnumber of related studies, it is too early to draw definiteconclusions. Nevertheless, first results demonstrate thecomplexity of the neuropsychology of affective disorders.
Neurobiological Factors Being Relatedto Neuropsychological Performance
Alterations of Brain Structure and Function
It is undisputed that psychological processes, includingcognitive function, have a neuronal representation. Several
Neuropsychol Rev

structural and functional alterations in patients with mooddisorders have been documented. In some of these studies,structural and functional changes were related to neuropsy-chological impairments. Given the relatively unspecificneuropsychological deficit profile of patients with mooddisorders, it is not surprising that the research findings onneuronal alterations have also been heterogeneous andsomewhat non-specific so far.
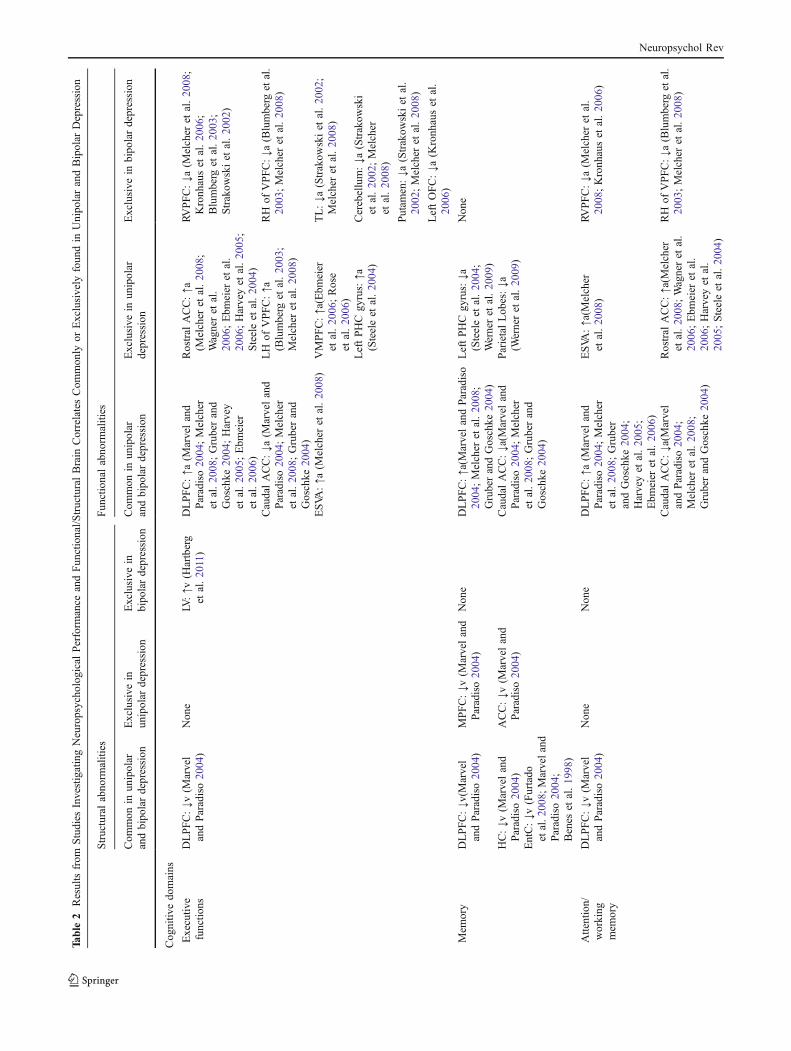
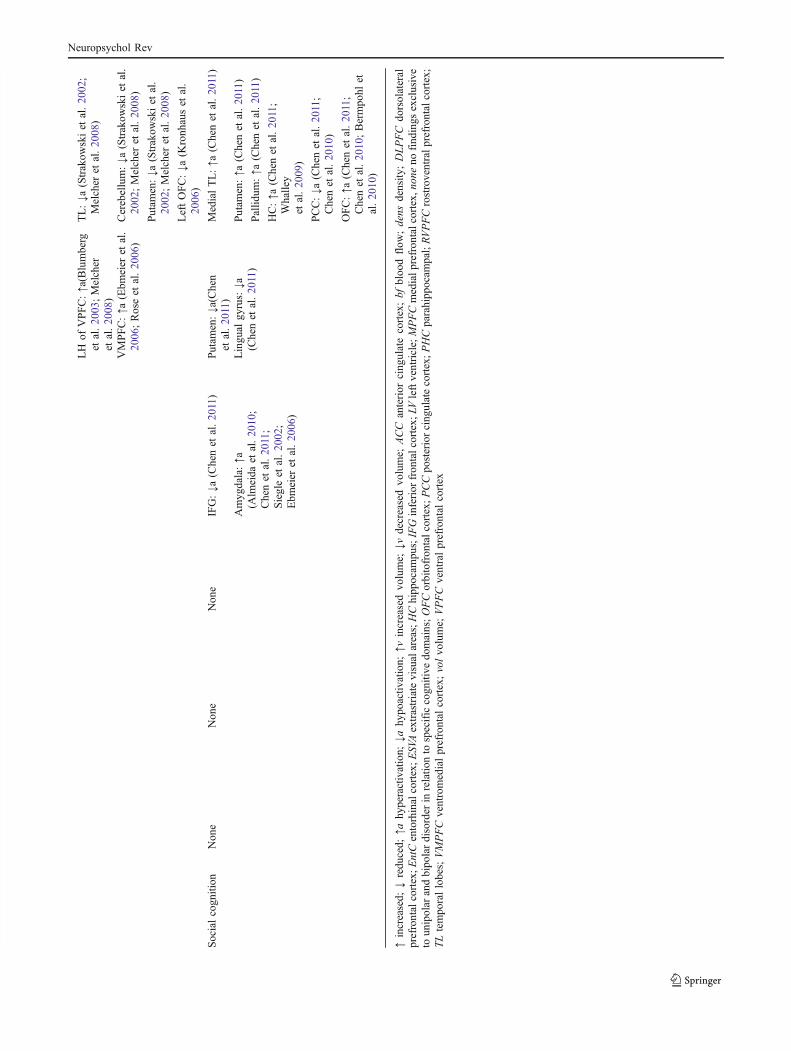
Few studies have reviewed the similarities and variationsbetween unipolar and bipolar mood disorder in relation tocognitive dysfunction and their neurobiological correlates.The literature suggests that mood disorders may sharecommon cognitive impairments in areas such as executivefunction, memory, attention, and social perception as wellas common biological features primarily relating to lackof development or atrophy in the prefrontal cortex(Marvel and Paradiso 2004; Melcher et al. 2008;Strakowski et al. 2002). Further, these PFC abnormalitiesappear to lead to a loss of capacity to modulate the limbicsystem resulting in either emotional cycling (BD) ordepression (UD) depending upon the subcortical abnor-malities uniquely present to each disorder (Strakowski etal. 2002). The neurobiological differences between uni-polar and bipolar depression associated with cognitivefunction are shown in Table 2.
Structural Abnormalities and Cortisol Apart from elderlypatients with a late-onset of depression and patientssuffering from depression with psychotic symptoms (forreview see Drevets et al. 2008; Lorenzetti et al. 2009),global structural abnormalities such as cerebral atrophy arenot typical of mood disorders. Atrophy is reported to bepresent in the prefrontal cortex (PFC), the cingular cortexwith prominent changes in the left subgenual cingularcortex (Drevets et al. 1997), the temporal cortex, and thebasal ganglia. Within the PFC, the orbital, medial, anddorsolateral parts are affected. In addition to grey matterchanges, white matter damage has also been documented(Drevets et al. 2008). Among patients with bipolar disorder,the posterior cingular cortex also shows a reduced volume(Drevets et al. 2008). Several studies which investigated thetemporal cortex with particular focus on the hippocampalvolume, demonstrated atrophy in this brain structure.Investigations into the volume of the amygdala showinconsistent findings; atrophy as well as increased amyg-dala volumes, particularly among patients with bipolardisorder have been reported (Davidson et al. 2002). Inaddition to findings which demonstrate atrophy within thebasal ganglia (Baumann et al. 1999), other research has alsodemonstrated increased volume of the basal ganglia amongpatients with bipolar disorder (Marchand and Yurgelun-Todd 2010). Some of the inconsistencies among thesefindings might also be related to a number of other factors
such as gender, and severity and duration of the mooddisorder (Lorenzetti et al. 2009).
Several biological mechanisms may contribute to thesestructural abnormalities in mood disorders. One area ofinterest relates to the glucocorticoid receptors which arerich in the hippocampus. It is suggested from experimentalresearch in highly stressed animals that cortisol can damagethe hippocampus (Sapolsky 1996). Since pathologicalabnormalities of the hypothalamic-pituitary-adrenal axis(HPA) in conjunction with an increased excretion of cortisolin depression have been described, the abnormalities of theHPA axis following stress may lead, or at least contribute,to the structural changes such as those evident in thehippocampus. In support of these findings are previousstudies which have established an association betweenduration of the mood disorder/numbers of episodes(McKinnon et al. 2009; Sheline et al. 1996) and earlytraumatisation (Vythilingam et al. 2002), respectively, andthe degree of hippocampal damage. In addition, the effectof stress on the hippocampus appears to be modulated bygenetic factors (Frodl et al. 2008). On the other hand, itshould be considered that the structural abnormalitiesrepresent a vulnerability factor for the development ofmood disorders and hypercortisolism (Lorenzetti et al.2009). Another important finding from the past few yearsis the observation that the human hippocampus has theability to generate new neurons over the whole life span(Paizanis et al. 2007) with research suggesting that physicaland mental activity (Mirochnic et al. 2009) and certaindrugs (Wang et al. 2008) may stimulate this process. This isof importance since mood disorders may counteract thislife-long process (Becker et al. 2009).
Associations between neuropsychological performance,cortisol and hippocampus volume are highly complex andadditionally complicated in mood disorders (Schlosser et al.2011). Although the results are not fully conclusive at thisstage, a study by O’Brien et al. (2004) indicates thatcognitive deficits in depressed patients are most likelyassociated with a decreased volume of the hippocampus,rather than with the secretion of cortisol. However, there isa paucity of research that has explored the structuralneurobiology-cognitive impairment relationship. Table 2shows the structure-cognition findings that are robusthowever, this evidence is primarily from earlier studiesand, in light of the existing inconclusive data as well asimproved assessment and imaging technologies, warrantrenewed investigation. The findings indicate that structuralabnormalities that relate to cognitive function are—besidesof the hippocampus—primarily found in the dorsolateralprefrontal cortex (DLPFC). This is consistent with whatcould be expected given the putative functions of theseregions and the impaired cognitive outcomes with whichthey are associated, namely executive function, attention/
Neuropsychol Rev
Table
2Resultsfrom
Studies
InvestigatingNeuropsycho
logicalPerform
ance
andFun
ctional/S
tructuralBrain
CorrelatesCom
mon
lyor
Exclusively
foun
din
Unipo
larandBipolar
Depression
Structuralabno
rmalities
Fun
ctionalabno
rmalities
Com
mon
inun
ipolar
andbipo
lardepression
Exclusive
inun
ipolar
depression
Exclusive
inbipo
lardepression
Com
mon
inun
ipolar
andbipo
lardepression
Exclusive
inun
ipolar
depression
Exclusive
inbipo
lardepression
Cog
nitiv
edo
mains
Executiv
efunctio
nsDLPFC:↓v
(Marvel
andParadiso20
04)
Non
eLV:↑v
(Hartberg
etal.20
11)
DLPFC:↑a
(Marveland
Paradiso20
04;Melcher
etal.20
08;Gruberand
Goschke
2004;Harvey
etal.20
05;Ebm
eier
etal.20
06)
Rostral
ACC:↑a
(Melcher
etal.20
08;
Wagneret
al.
2006
;Ebm
eier
etal.
2006
;Harveyet
al.20
05;
Steeleet
al.20
04)
RVPFC:↓a
(Melcher
etal.20
08;
Kronh
auset
al.20
06;
Blumberg
etal.20
03;
Strakow
skiet
al.20
02)
CaudalACC:↓a
(Marveland
Paradiso20
04;Melcher
etal.20
08;Gruberand
Goschke
2004)
LH
ofVPFC:↑a
(Blumberg
etal.20
03;
Melcher
etal.20
08)
RH
ofVPFC:↓a
(Blumberg
etal.
2003
;Melcher
etal.20
08)
ESVA
:↑a
(Melcher
etal.20
08)
VMPFC:↑a(Ebm
eier
etal.20
06;Rose
etal.20
06)
TL:↓a
(Strakow
skiet
al.20
02;
Melcher
etal.20
08)
LeftPHCgy
rus:↑a
(Steeleet
al.20
04)
Cerebellum:↓a
(Strakow
ski
etal.20
02;Melcher
etal.20
08)
Putam
en:↓a
(Strakow
skiet
al.
2002
;Melcher
etal.20
08)
LeftOFC:↓a
(Kronh
auset
al.
2006
)
Mem
ory
DLPFC:↓v
(Marvel
andParadiso20
04)
MPFC:↓v
(Marveland
Paradiso20
04)
Non
eDLPFC:↑a(M
arvelandParadiso
2004;Melcher
etal.20
08;
GruberandGoschke
2004)
LeftPHCgy
rus:↓a
(Steeleet
al.20
04;
Werneret
al.20
09)
Non
e
HC:↓v
(Marveland
Paradiso20
04)
ACC:↓v
(Marveland
Paradiso20
04)
CaudalACC:↓a(M
arveland
Paradiso20
04;Melcher
etal.20
08;Gruberand
Goschke
2004)
ParietalLob
es:↓a
(Werneret
al.20
09)
EntC:↓v
(Furtado
etal.2
008;
Marveland
Paradiso20
04;
Benes
etal.19
98)
Attention/
working
mem
ory
DLPFC:↓v
(Marvel
andParadiso20
04)
Non
eNon
eDLPFC:↑a
(Marveland
Paradiso20
04;Melcher
etal.20
08;Gruber
andGoschke
2004;
Harveyet
al.20
05;
Ebm
eier
etal.20
06)
ESVA
:↑a(M
elcher
etal.20
08)
RVPFC:↓a
(Melcher
etal.
2008
;Kronh
auset
al.20
06)
CaudalACC:↓a(M
arvel
andParadiso20
04;
Melcher
etal.20
08;
GruberandGoschke
2004)
Rostral
ACC:↑a(M
elcher
etal.20
08;Wagneret
al.
2006
;Ebm
eier
etal.
2006
;Harveyet
al.
2005
;Steeleet
al.20
04)
RH
ofVPFC:↓a
(Blumberg
etal.
2003
;Melcher
etal.20
08)
Neuropsychol Rev
Structuralabno
rmalities
Fun
ctionalabno
rmalities
Com
mon
inun
ipolar
andbipo
lardepression
Exclusive
inun
ipolar
depression
Exclusive
inbipo
lardepression
Com
mon
inun
ipolar
andbipo
lardepression
Exclusive
inun
ipolar
depression
Exclusive
inbipo
lardepression
LH
ofVPFC:↑a(Blumberg
etal.20
03;Melcher
etal.20
08)
TL:↓a
(Strakow
skiet
al.20
02;
Melcher
etal.20
08)
VMPFC:↑a
(Ebm
eier
etal.
2006
;Roseet
al.20
06)
Cerebellum:↓a
(Strakow
skiet
al.
2002
;Melcher
etal.20
08)
Putam
en:↓a
(Strakow
skiet
al.
2002
;Melcher
etal.20
08)
LeftOFC:↓a
(Kronh
auset
al.
2006
)
Socialcogn
ition
Non
eNon
eNon
eIFG:↓a
(Chenet
al.20
11)
Putam
en:↓a(Chen
etal.20
11)
MedialTL:↑a
(Chenet
al.20
11)
Amyg
dala:↑a
(Alm
eida
etal.20
10;
Chenet
al.20
11;
Siegleet
al.20
02;
Ebm
eier
etal.20
06)
Lingu
algy
rus:↓a
(Chenet
al.20
11)
Putam
en:↑a
(Chenet
al.20
11)
Pallid
um:↑a
(Chenet
al.20
11)
HC:↑a
(Chenet
al.20
11;
Whalley
etal.20
09)
PCC:↓a
(Chenet
al.20
11;
Chenet
al.20
10)
OFC:↑a
(Chenet
al.20
11;
Chenet
al.20
10;Bermpo
hlet
al.20
10)
↑increased;
↓redu
ced;
↑ahy
peractivation;
↓ahy
poactiv
ation;
↑vincreasedvo
lume;
↓vdecreasedvo
lume;
ACC
anterior
cing
ulatecortex;bf
bloo
dflow
;dens
density
;DLPFC
dorsolateral
prefrontalcortex;E
ntCentorhinalcortex;E
SVAextrastriatevisualareas;HChipp
ocam
pus;IFGinferior
fron
talcortex;
LVleftventricle;MPFCmedialp
refron
talcortex,
none
nofind
ings
exclusive
toun
ipolar
andbipo
lardisorder
inrelatio
nto
specificcogn
itive
domains;OFCorbitofron
talcortex;P
CCpo
steriorcing
ulatecortex;P
HCparahipp
ocam
pal;RVPFCrostroventralprefrontalcortex;
TLtempo
rallobes;VMPFC
ventromedialprefrontal
cortex;volvo
lume;
VPFCventralprefrontal
cortex
Neuropsychol Rev

working memory, and declarative memory. Furthermore,some correlational studies demonstrated associations betweenneuropsychological deficits and structural abnormalities ofthe orbital frontal cortex (Taylor et al. 2003) left cingulatecortex (Yuan et al. 2008), and the basal ganglia (Naismith etal. 2002) as well as white matter lesions (Hickie et al. 2007)in patients with MDD.
Taken together, relations between neuropsychologicaldeficits and structural brain abnormalities in affectivedisorders are complex and further related to other factorssuch as cortisol. Furthermore, etiological mechanisms arecontroversially discussed. Structural damage was inter-preted as both, consequence and cause of the affectivedisorder.
Functional Abnormalities In several functional studies,researchers assessed the association between neuronalactivation and neuropsychological function. Overall, previ-ous findings are somewhat inconsistent (Rogers et al.2004). In a positron emission tomography (PET) emissionstudy, Elliott et al. (1997a) investigated patients withunipolar depression while performing the Tower of Hanoitask. In comparison to healthy controls, patients withdepression demonstrated reduced planning abilities, as wellas reduced activation of the prefrontal cortex and thestriatum. On the contrary, Bremner et al. (2004) reported areduced activity of the right hippocampus and ACC duringa learning task; however, the MDD patients showed nolearning deficits. Moreover, Videbech et al. (2003) demon-strated reduced cognitive performance in MDD patientscompleting a word fluency task; however, these patientsshowed no abnormalities in brain activation. Finally, Barchet al. (2003) found that patients with MDD had neitherperformance deficits in a working memory task nor anabnormal activation of the PFC.
Several studies indicate that patients with mood disor-ders compared to healthy controls show an increasedactivation while performing cognitive tasks. Fitzgerald etal. (2008) and Harvey et al. (2005) found no cognitivedeficits in a working memory task (“n-back”) in MDDpatients, while they showed a stronger activation of theprefrontal cortex and the ACC compared to healthycontrols. The authors interpret this brain activation as acompensatory mechanism of additional brain regions.Wagner et al. (2008) were able to show in their casecontrol study that healthy subjects demonstrated a deacti-vation of the rostral ACC in the classical colours Stroopparadigm relative to patients with unipolar depression. Theauthors interpreted these findings to suggest that brainactivity which was irrelevant to the neuropsychologicaltask was suppressed. In a functional magnetic resonanceimaging (fMRI) study, Mitterschiffthaler et al. (2008)investigated the activation pattern of the rostral ACC
during the processing of emotionally relevant informationin MDD patients. Using the emotional Stroop test,depressed patients took longer to identify the colour ofnegative items. An increased attentional bias towardsemotionally negative stimuli was associated with a hyper-activation of the rostral ACC. From these findings, theauthors suggest that that a strong activation of the rostralACC might hinder effective task processing of emotion-ally relevant information.
Connectivity analysis using MRI is a research toolwhich has been used more frequently in the past fewyears. Connectivity analysis measures the correlation ofactivation patterns between different brain regions andprovides important information on abnormalities ofneuronal networks in patients with mood disorders.Research using this research tool has demonstratedfindings which support the notion that neuronal networkscorrelate more closely with symptoms of depression thansingle brain structures. The attentional bias has oftenbeen associated with the activation of the amygdala whenpatients were exposed to emotional and anxiety-relatedstimuli in particular (Drevets et al. 2008). Beyond thesefindings, Hamilton and Gotlib (2008) were able to showthat patients with MDD demonstrated a stronger connec-tivity between the amygdala and hippocampus/basalganglia during processes of encoding emotionally negativepictures. Frodl et al. (2010) investigated the attentionalbias in a face-recognition task using connectivity analysis.The authors demonstrated increased as well as decreasedconnectivity between various brain regions and concludedthat the increased connectivity between the DLPFC andthe orbital frontal cortex could serve as a neuronalcorrelate of the attentional bias towards negative stimuliof MDD patients.
In this research context, the concept of default modenetworks (DMN; Raichle et al. 2001) has gained moreimportance in the recent past. The DMN is regarded as anetwork of brain structures that reflects self-referentialprocesses that are deactivated during non self-referentialgoal-oriented tasks (Broyd et al. 2009; Sheline et al. 2009).Sheline et al. investigated the DMN of emotional modula-tion in patients with MDD and healthy subjects. Watchingnegative compared to neutral pictures, depressed patientsshowed reduced deactivation in widespread areas of theDMN such as the anterior cingulate cortex, ventromedialcortex, lateral temporal and lateral parietal cortex. Theauthors also found an increased activation of amygdala,parahippocampus, hippocampus and dorsal medial prefron-tal cortex. Similar patterns were found for reappraising thepictures indicating that changes of DMN activation occurfor automatic and active emotion regulation. The authorsconclude that these DMN changes may reflect ruminativeprocesses in depression. Bluhm et al. (2009) reported
Neuropsychol Rev

abnormalities of the DMN in a resting state in depressedpatients in that there was a reduced connectivity betweenthe precuneus/posterior cingulate cortex and the basalganglia, whereas the connectivity between emotionallyrelevant brain structures in another study reported byGreicius et al. (2007) was increased. These authors foundan increased integration of the subgenual ACC in the DMNactivity and they therefore suggested that the DMN isaltered in MDD.
Regarding the distinction between uni- and bipolardepression some particularities have to be mentioned (fordetails see Table 2). While unipolar depression is charac-terised by more diffuse hypofrontal activation and localisedlimbic hyperactivation (Almeida et al. 2010; Furtado et al.2008; Marvel and Paradiso 2004; Melcher et al. 2008;Siegle et al. 2002; Wagner et al. 2006) neurobiology inbipolar depression appears to be associated with cogni-tive impairment that can be surmised functionally asinvolving localised hypoactivation of frontal regions anda more widely distributed hyperactivation of the limbicstructures (Chen et al. 2011). This supports the existingmodels of bipolar disorder which suggests that emotiondysregulation and executive functions are associated withimpulse control and performance monitoring features(Green et al. 2007; Phillips et al. 2008). The cognitiveoutcomes converge in the limbic-cortical dysregulationcreated in both neurobiological profiles. This dysregula-tion results in the simultaneous activation or deactivationof otherwise synchronised regions resulting in reducedcapacity for information processing and behaviour forma-tion through functional deficits in regions responsible forthe cognitive and affective interactions between evalua-tion, regulation, and inhibition.
There is increasing evidence that elements of thefunctional neurobiology of both conditions is trait-basedand therefore independent of mood-state (Blumberg et al.2003; Chen et al. 2011; Kronhaus et al. 2006; Melcher et al.2008; Wagner et al. 2006). However, the cognitive deficitsin both conditions have been largely correlated withsymptom severity and therefore might be state-dependentas well (Chen et al. 2011; Marvel and Paradiso 2004;Melcher et al. 2008). There is a paucity of research that hassufficiently controlled for symptomatic state-specific per-formance and further investigation is required to identifystate-independent cognition-biology correlations in order toidentify those factors that may be more closely related topathophysiology rather than mood-state.
In sum, patients with affective disorders show both,increases and decreases of neuronal activation whileperforming neuropsychological tasks. Bipolar patients ascompared to patients with unipolar depression may showmore widely distributed hyperactivation of limbic struc-tures. Hypoactivation is regarded as insufficient recruitment
of neuronal networks. By contrast, hyperactivation isinterpreted as compensatory mechanism or, alternatively,as reduced deactivation of DMN structures. Connectivityanalyses further support the notion that neuropsychologicalabnormalities are more closely related to neuronal networksthan single brain structures.
Neuropsychological Dysfunction and NeurobiologicalModels of Depression
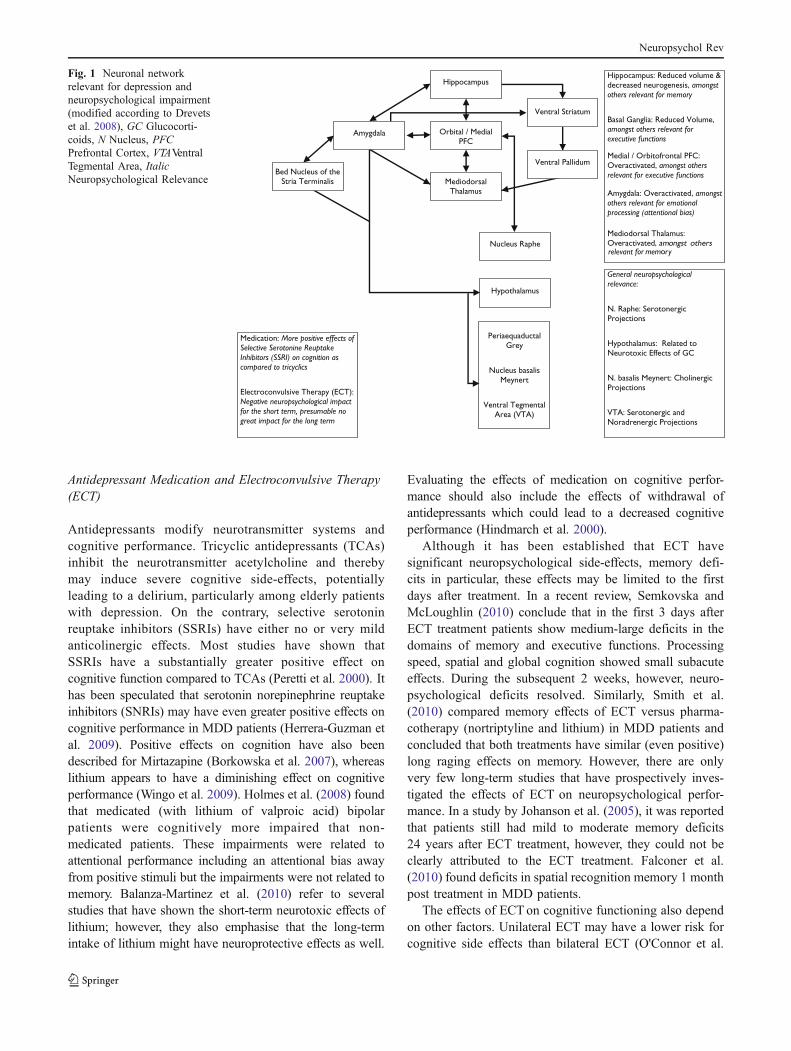
The aforementioned structural and functional alterationsrelevant to neuropsychological function in depressionshould be interpreted in the context of neurobiologicalmodels of depression which suggest the involvement ofabnormal neuronal networks. Over the past few years,several empirically supported neurobiological models ofmood disorders have been developed. According toMayberg’s Model (Mayberg 1997) primarily developedon findings with MDD patients, alterations of the rostralACC play an important role in the mediation between theventral and dorsal brain structures. A reduced activationof dorsal brain areas (DLPFC, dorsal ACC, posteriorcingular cortex, inferior parietal cortex) possibly under-lies neuropsychological dysfunction in depression and anactivation of ventral areas (ventral PFC, subgenual ACC,anterior-insular, hypothalamus) probably forms the neu-ronal basis of vegetative and somatic symptoms ofdepression. On the basis of previously reported fronto-striatal models of depression (Drevets and Raichle 1992;Swerdlow and Koob 1987) and newer empirical findings,a dysfunctional neuronal network, including a hyper-activated positive feedback loop between the amygdala,medial dorsal thalamus and the medial PFC is postulated(see Fig. 1; Drevets et al. 2008). These authors suggest areduced inhibiting input of this hyperactivated positivefeedback loop in depression through other feedback loopswhich involve the basal ganglia. As a result, activationpatterns of further subcortical structures such as the bednucleus of the stria terminalis, hypothalamus and theperi-aqueductal grey change, too. Drevets et al. (2008)suggested abnormalities in the Nucleus Basalis ofMeynert, with it cholinergic projections, in particular, tobe an important basis of neuropsychological deficits indepressed patients
Collectively, a variety of structural and functionalalterations have been associated with neuropsychologicalimpairments of mood disorders and depression in particular.Etiological models of depression involving abnormal brainnetwork functions such as fronto-striatal models of depres-sion (Drevets et al. 2008) integrate those findings andsuggest associations with neuropsychological dysfunctionin depression.
Neuropsychol Rev
Antidepressant Medication and Electroconvulsive Therapy(ECT)
Antidepressants modify neurotransmitter systems andcognitive performance. Tricyclic antidepressants (TCAs)inhibit the neurotransmitter acetylcholine and therebymay induce severe cognitive side-effects, potentiallyleading to a delirium, particularly among elderly patientswith depression. On the contrary, selective serotoninreuptake inhibitors (SSRIs) have either no or very mildanticolinergic effects. Most studies have shown thatSSRIs have a substantially greater positive effect oncognitive function compared to TCAs (Peretti et al. 2000). Ithas been speculated that serotonin norepinephrine reuptakeinhibitors (SNRIs) may have even greater positive effects oncognitive performance in MDD patients (Herrera-Guzman etal. 2009). Positive effects on cognition have also beendescribed for Mirtazapine (Borkowska et al. 2007), whereaslithium appears to have a diminishing effect on cognitiveperformance (Wingo et al. 2009). Holmes et al. (2008) foundthat medicated (with lithium of valproic acid) bipolarpatients were cognitively more impaired that non-medicated patients. These impairments were related toattentional performance including an attentional bias awayfrom positive stimuli but the impairments were not related tomemory. Balanza-Martinez et al. (2010) refer to severalstudies that have shown the short-term neurotoxic effects oflithium; however, they also emphasise that the long-termintake of lithium might have neuroprotective effects as well.
Evaluating the effects of medication on cognitive perfor-mance should also include the effects of withdrawal ofantidepressants which could lead to a decreased cognitiveperformance (Hindmarch et al. 2000).
Although it has been established that ECT havesignificant neuropsychological side-effects, memory defi-cits in particular, these effects may be limited to the firstdays after treatment. In a recent review, Semkovska andMcLoughlin (2010) conclude that in the first 3 days afterECT treatment patients show medium-large deficits in thedomains of memory and executive functions. Processingspeed, spatial and global cognition showed small subacuteeffects. During the subsequent 2 weeks, however, neuro-psychological deficits resolved. Similarly, Smith et al.(2010) compared memory effects of ECT versus pharma-cotherapy (nortriptyline and lithium) in MDD patients andconcluded that both treatments have similar (even positive)long raging effects on memory. However, there are onlyvery few long-term studies that have prospectively inves-tigated the effects of ECT on neuropsychological perfor-mance. In a study by Johanson et al. (2005), it was reportedthat patients still had mild to moderate memory deficits24 years after ECT treatment, however, they could not beclearly attributed to the ECT treatment. Falconer et al.(2010) found deficits in spatial recognition memory 1 monthpost treatment in MDD patients.
The effects of ECTon cognitive functioning also dependon other factors. Unilateral ECT may have a lower risk forcognitive side effects than bilateral ECT (O'Connor et al.
Fig. 1 Neuronal networkrelevant for depression andneuropsychological impairment(modified according to Drevetset al. 2008), GC Glucocorti-coids, N Nucleus, PFCPrefrontal Cortex, VTAVentralTegmental Area, ItalicNeuropsychological Relevance
Neuropsychol Rev
2010). In addition, greater cognitive reserves may protectagainst adverse effects of ECTon cognition (Legendre et al.2003). Effects of ECT may also depend on stress hormonelevels. In a study of Neylan et al. (2001) elevated basalcortisol levels were associated with a greater decrease ofcognitive functioning after ECT in MDD patients.
Taken together, psychotropic medication and ECTinfluence the neuropsychological performance of patientswith affective disorder. Positive and negative effects havebeen described depending on additional factors such as thespecific type of antidepressants, type of ECT, cognitivereserves and cortisol levels. Furthermore, short-term effectshave to be separated from long-term effects.
Discussion
In agreement with our expectations, we found clinical,demographic and neurobiological factors to be associatedwith the severity of neuropsychological impairments inpatients with affective disorders. In particular, patients withmore severe diagnoses, some comorbid mental disorderssuch as alcohol abuse, anxiety disorders, and possiblyADHD, higher age, and late onset, psychological processessuch as rumination and processing bias, and potentially,sleep disturbances, lower eduction, suicidal tendencies,traumatization, and negative attitude toward computers(only computer tasks) are more severely impaired. Somefactors such as gender and personality may interact withthese factors. In addition, changes of brain structure and
function, neuroendocrinological and neurochemical devia-tions are associated with neuropsychological impairmentsin affective disorders. Antidepressant anticholinergicmedication and ECT treatment (rather short-lastingeffects) are relevant external neurobiological factors withpotentially destructive effects on cognition. Most studiesincluded depressed patients. For patients in the manicstate too few studies have been conducted for definiteconclusions about relevant factors that influence theneuropsychological outcome.
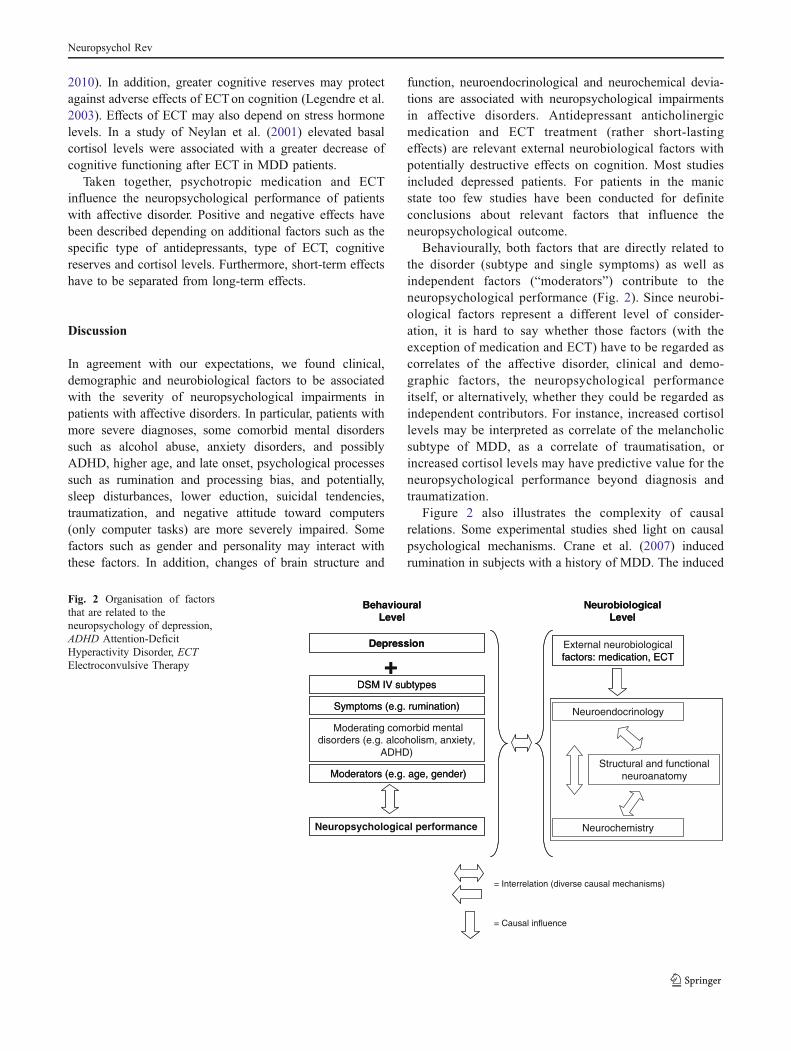
Behaviourally, both factors that are directly related tothe disorder (subtype and single symptoms) as well asindependent factors (“moderators”) contribute to theneuropsychological performance (Fig. 2). Since neurobi-ological factors represent a different level of consider-ation, it is hard to say whether those factors (with theexception of medication and ECT) have to be regarded ascorrelates of the affective disorder, clinical and demo-graphic factors, the neuropsychological performanceitself, or alternatively, whether they could be regarded asindependent contributors. For instance, increased cortisollevels may be interpreted as correlate of the melancholicsubtype of MDD, as a correlate of traumatisation, orincreased cortisol levels may have predictive value for theneuropsychological performance beyond diagnosis andtraumatization.
Figure 2 also illustrates the complexity of causalrelations. Some experimental studies shed light on causalpsychological mechanisms. Crane et al. (2007) inducedrumination in subjects with a history of MDD. The induced
Moderators (e.g. age, gender)
Symptoms (e.g. rumination)
DSM IV subtypes
Depression
+
BehaviouralLevel
NeurobiologicalLevel
Structuraland functionalneuroanatomy
Neuroendocrinology
Neurochemistry
factors: medication, ECT
Neuropsychological performance
Moderators (e.g. age, gender)
Symptoms (e.g. rumination)
DSM IV subtypes
Depression
+
BehaviouralLevel
NeurobiologicalLevel
Structural and functionalneuroanatomy
Neuroendocrinology
Neurochemistry
External neurobiologicalfactors: medication, ECT
Moderating comorbid mental disorders (e.g. alcoholism, anxiety,
ADHD)
= Interrelation (diverse causal mechanisms)
= Causal influence
Fig. 2 Organisation of factorsthat are related to theneuropsychology of depression,ADHD Attention-DeficitHyperactivity Disorder, ECTElectroconvulsive Therapy
Neuropsychol Rev

rumination resulted in reduced autobiographical memoryspecificity in the patient group. Likewise, Murphy et al.(2003) investigated the influence of negative feedback ontask performance in MDD. Compared to healthy controlsubjects, depressed patients performed worse in maintain-ing response sets when confronted with misleadingnegative feedback. By contrast, like healthy controlsubjects they were able to increase task performance afternegative but correct feedback. However, with regard toseveral factors causal mechanisms are yet not fullyunderstood. As reported above, for instance, it has beenfound that the duration of MDD is associated withhippocampus shrinkage (Sheline et al. 1996). In accor-dance with these findings, Gorwood et al. (2008) showedthat memory performance diminished by 2–3% perprevious episode of MDD (calculated up to four episodes).They conclude from their findings that stress and depres-sion related neurotoxic effects on the hippocampus areresponsible for reduced memory performance. However, itcan also be postulated that a longer history of depressionor mania indicates a more severe type of affective disorderwith more prominent cognitive deficits and a reducedhippocampus volume. Some studies indeed suggest aconverse causality with a reduced hippocampal volumebeing the cause or correlate of mental disorders instead ofbeing the consequence (e.g. Lyons et al. 2001). Gilbertsonand coworkers (2002) investigated monozygote twins.More severe symptoms in patients with PTSD wereassociated with smaller hippocampi of both the patientsand the patients' trauma-unexposed identical co-twin. Inaddition, twin pairs with one twin showing a severe PTSDhad smaller hippocampi than non-PTSD pairs.
While the factors discussed in this paper are related tothe severity of neuropsychological impairment in patientswith affective disorders, no clear conclusions could bedrawn with respect to the neuropsychological profile. Forinstance, patients in a euthymic state of their disorder,younger patients, or patients with a milder affectivedisorder, tend to perform relatively better, but study resultsdo not clearly show which functions are primarily affected.Several reasons may account for this ambiguity. Firstly,some studies indicate that the factors here discussed arecomplexly interrelated. Van den Heuvel et al. (1996) foundthat depressive symptoms were related to cognitive dys-function in female elderlies who exhibit a weak internallocus of control. In men, by contrast, the associationbetween depression and cognitive dysfunction was moder-ated by neuroticism. Thus, the relation between depression,gender, and neuropsychological performance was furthermoderated by personality traits. Investigating the memorybias for emotionally relevant stimuli in MDD, Ellwart et al.(2003) found a memory bias for implicit memory but notfor explicit memory performance. This finding contrasts
with other findings where memory bias was evident inexplicit memory performance. The authors speculated thatthe factor “biased information processing” may not generallybe related to memory performance in depressed patients butdepend additionally on the symptom severity. Unfortunately,possible interactions are clearly unmanageable given the highnumber of factors that are known to influence neuropsycho-logical performance in patients with affective disorders.However, guided by clear hypothesis, future studies shouldinclude different factors.
Secondly, the expectation to find specific neuropsycho-logical deficits in patients with affective disorders comesfrom studies with neurological patients with distinct braindysfunctions. By contrast, Hasler and colleagues (2004,2006) regard mood disorders as an aggregation of variouspsychopathological and biological clusters. These clusters(“endophenotypes”) are genetically and phenomenologicallymore homogenous and might act as a promising basis for theformulation of etiologically-based sub-types of mood disor-ders. However, it seems possible that not only affectivedisorders are too broadly conceptualised to be related todistinct brain regions and distinct neuropsychologicaldomains but that the clinical and demographical factorsdiscussed here do not have a distinct neural and neuropsy-chological correlate either. Rumination, for instance, unfoldsits destructive effects on cognitive performance by occupyingand biasing processing capacities. Thus, rumination mayaffect all neuropsychological domains that depend on thesecapacities. Furthermore, rumination is related to broad brainnetworks. Cooney et al. (2010) suggested that rumination inMDD patients is associated with enhanced recruitment oflimbic and medial and dorsolateral prefrontal regions. Asalready mentioned above, Sheline et al. (2009) relatedrumination to a changed regulation of default mode networkstructures during cognitive tasks. Subjects had to look atnegative pictures and reappraising them. In particular,depressed patients exhibited a failure to reduce activityin the ventromedial prefrontal cortex prefrontal cortex(BA 10), anterior cingulate (BA 24/32), lateral parietalcortex (BA 39), and lateral temporal cortex (BA 21) andan accelerated activity in amygdala, parahippocampus,hippocampus, and dorsal medial prefrontal cortex.
Apart from theoretical aspects, some of the factorsdiscussed here have important clinical impact and maystimulate the development of effective neuropsychologicaltreatment strategies. If, for instance, cortisol is a majordestructive agent of cognitive performance, both psycho-therapeutic and psychopharmacological treatment strategiesthat are known to regulate HPA axis functioning may befurther developed and applied. If sleep disturbancescontribute to cognitive impairments, treatment strategies,from the neuropsychological point of view, should alsofocus on sleep. With regard to rumination, mindfulness
Neuropsychol Rev

based intervention is a promising treatment strategy. Amindful mindset brings rumination into consciousness andenables the person concerned to orientate attention back towhat is relevant in the present moment. Indeed, Deyo et al.(2009) showed that mindfulness based stress reduction(MBSR; Kabat-Zinn 1990) increased wellbeing and reducedrumination in a sample of individuals seeking support fromMBSR for various medical and psychological problems. Inaddition, symptoms of depression improved. In a sample ofpatients with life time mood disorders, Ramel et al. (2004)showed that MBSR reduced rumination even after control-ling for reductions in affective symptoms and dysfunctionalbeliefs. Furthermore, training intensity was correlated withdecreased rumination. With a comparable program,Zylowska et al. (2008) found pre-post improvements intest performance on tasks measuring attention andcognitive inhibition in ADHD patients. They alsoreported a decrease of ADHD related symptoms, anxiety,and depression. However, “classical neuropsychologicaltherapy” has also been proved to be successful in affectivedisorders disorders (Elgamal et al. 2007; Naismith et al. 2010;Trebo et al. 2007) but these treatment strategies could verylikely be further optimised by considering the here discussedfactors.
In conclusion, patients with mood disorders may exhibitimpairments in various cognitive domains including attention,executive function and memory. A promising approach tofurther specify theses impairments is the additional consider-ation of clinical (subtypes, comorbidity, traumatization,personality, severity, diurnal swings, course, duration, age ofonset, biased processing, rumination, motivation, experienceof failure, sleep, suicidal tendencies, computer attitudes),demographic (age, education, gender) and neurobiologicalfactors (structural and functional brain changes, glucocorti-coids, medication, ECT) that are known to be related tocognitive performance. Studies have demonstrated that thesefactors have an impact on the severity of cognitive impairmentbut findings regarding the neuropsychological profile remainheterogeneous. Nevertheless, some of the factors discussedhere have an important clinical impact and the knowledgeabout those factors may help to further improve effectiveneuropsychological treatment strategies for patients withaffective disorders. This is a very relevant goal sinceneuropsychological deficits contribute to long-term functionaloutcome, and patients concerned with deficits may show lesscompliance and an increased risk for suicide. In connectionwith the development of effective neuropsychological treat-ment strategies for patients with affective disorders, futureresearch should imply manic patients, too. In addition, apromising approach to further specify neuropsychologicalimpairments is the coincidental consideration of differentfactors that are known to influence cognitive performance.Experimental studies and prospective studies are needed to
better understand etiological mechanisms. Such studies maythen allow identifying etiologically-defined clusters con-sisting of psychopathological, neuropsychological andbiological characteristics.
References
Almeida, J. R., Versace, A., Hassel, S., Kupfer, D. J., & Phillips, M. L.(2010). Elevated amygdala activity to sad facial expressions: astate marker of bipolar but not unipolar depression. BiologicalPsychiatry, 67, 414–421.
American Psychiatric Association, A. P. (1994). DSM IV Diagnosticand statistical manual of mental disorders (4th ed.). Washington:American Psychiatric Association.
Austin, M. P., Ross, M., Murray, C., O’Carroll, R. E., Ebmeier, K. P.,& Goodwin, G. M. (1992). Cognitive function in majordepression. Journal of Affective Disorders, 25, 21–29.
Avila, R., Moscoso, M. A., Ribeiz, S., Arrais, J., Jaluul, O., & Bottino, C.M. (2009). Influence of education and depressive symptoms oncognitive function in the elderly. International Psychogeriatrics, 21(3), 560–567.
Balanza-Martinez, V., Selva, G., Martinez-Aran, A., Prickaerts, J.,Salazar, J., Gonzalez-Pinto, A., et al. (2010). Neurocognition inbipolar disorders—a closer look at comorbidities and medications.European Journal of Pharmacology, 626(1), 87–96.
Ballmaier, M., Narr, K. L., Toga, A. W., Elderkin-Thompson, V.,Thompson, P. M., Hamilton, L., et al. (2008). Hippocampalmorphology and distinguishing late-onset from early-onset elderlydepression. The American Journal of Psychiatry, 165(2), 229–237.
Barch, D. M., Sheline, Y. I., Csernansky, J. G., & Snyder, A. Z. (2003).Working memory and prefrontal cortex dysfunction: specificity toschizophrenia compared with major depression. BiologicalPsychiatry, 53(5), 376–384.
Barrett, S. L., Kelly, C., Bell, R., & King, D. J. (2008). Genderinfluences the detection of spatial working memory deficits inbipolar disorder. Bipolar Disorders, 10(5), 647–654.
Basso, M. R., Lowery, N., Ghormley, C., Combs, D., Purdie, R., Neel,J., et al. (2007). Comorbid anxiety corresponds with neuropsy-chological dysfunction in unipolar depression. Cognitive Neuro-psychiatry, 12(5), 437–456.
Baumann, B., Danos, P., Krell, D., Diekmann, S., Leschinger, A.,Stauch, R., et al. (1999). Reduced volume of limbic system-affiliated basal ganglia in mood disorders: preliminary data froma postmortem study. The Journal of Neuropsychiatry and ClinicalNeurosciences, 11(1), 71–78.
Baune, B. T., McAfoose, J., Leach, G., Quirk, F., & Mitchell, D.(2009). Impact of psychiatric and medical comorbidity oncognitive function in depression. Psychiatry and Clinical Neuro-sciences, 63(3), 392–400.
Baune, B. T., Miller, R., McAfoose, J., Johnson, M., Quirk, F., &Mitchell, D. (2010). The role of cognitive impairment in generalfunctioning in major depression. Psychiatry Research, 176(2–3),183–189.
Beats, B. C., Sahakian, B. J., & Levy, R. (1996). Cognitiveperformance in tests sensitive to frontal lobe dysfunction in theelderly depressed. Psychological Medicine, 26, 591–603.
Beblo, T., & Herrmann, M. (2000). Neuropsychologische Defizite beiDepression. Fortschritte der Neurologie-Psychiatrie, 68, 1–11.
Beblo, T., & Lautenbacher, S. (2006). Neuropsychologie der Depression.Göttingen: Hogrefe.
Beblo, T., Baumann, B., Bogerts, B., Wallesch, C.-W., & Herrmann,M. (1999). Neuropsychological correlates of major depression: Ashort term follow-up. Cognitive Neuropsychiatry, 4, 333–341.
Neuropsychol Rev
Beblo, T., Mensebach, C., Wingenfeld, K., Schlosser, N., Rullkoetter,N., Schaffrath, C., et al. (2010). The impact of neutral andemotionally negative distraction on memory performance and itsrelation to memory complaints in major depression. PsychiatryResearch, 178, 106–111.
Beblo, T., Mensebach, C., Wingenfeld, K., Rullkoetter, N., Schlosser,N., & Driessen, M. (2011). Patients with borderline personalitydisorder and major depression are not distinguishable by theirneuropsychological performance: a case-control study. ThePrimary Care Companion for CNS Disorders, 13(1), 1–9.
Beck, A. T. (1967). Depression: Clinical, experimental and theoreticalaspects. New York: Harper and Row.
Becker, S., Macqueen, G., & Wojtowicz, J. M. (2009). Computationalmodeling and empirical studies of hippocampal neurogenesis-dependent memory: effects of interference, stress and depression.Brain Research, 1299, 45–54.
Benes, F. M., Kwok, E.W., Vincent, S. L., & Todtenkopf, M. S. (1998). Areduction of nonpyramidal cells in sector CA2 of schizophrenicsand manic depressives. Biological Psychiatry, 44, 88–97.
Bermpohl, F., Kahnt, T., Dalanay, U., Hagele, C., Sajonz, B.,Wegner, T., et al. (2010). Altered representation of expectedvalue in the orbitofrontal cortex in mania. Human BrainMapping, 31, 958–969.
Bluhm, R., Williamson, P., Lanius, R., Theberge, J., Densmore, M.,Bartha, R., et al. (2009). Resting state default-mode networkconnectivity in early depression using a seed region-of-interestanalysis: decreased connectivity with caudate nucleus. Psychiatryand Clinical Neuroscience, 63(6), 754–761.
Blumberg, H. P., Leung, H. C., Skudlarski, P., Lacadie, C. M.,Fredericks, C. A., Harris, B. C., et al. (2003). A functionalmagnetic resonance imaging study of bipolar disorder: state- andtrait-related dysfunction in ventral prefrontal cortices. Archives ofGeneral Psychiatry, 60, 601–609.
Borkowska, A., Drozdz, W., Ziolkowska-Kochan, M., & Rybakowski, J.(2007). Enhancing effect of mirtazapine on cognitive functionsassociated with prefrontal cortex in patients with recurrent depres-sion. Neuropsychopharmacologia Hungarica, 9(3), 131–136.
Bremner, J. D., Vythilingam, M., Vermetten, E., Vaccarino, V., &Charney, D. S. (2004). Deficits in hippocampal and anteriorcingulate functioning during verbal declarative memory encodingin midlife major depression. The American Journal of Psychiatry,161(4), 637–645.
Brissos, S., Dias, V. V., Carita, A. I., & Martinez-Aran, A. (2008).Quality of life in bipolar type I disorder and schizophrenia inremission: clinical and neurocognitive correlates. PsychiatryResearch, 160(1), 55–62.
Brodaty, H., Luscombe, G., Parker, G., Wilhelm, K., Hickie, I. B.,Austin, M. P., et al. (2001). Early and late onset depression in oldage: different aetiologies, same phenomenology. Journal ofAffective Disorders, 66(2–3), 225–236.
Broyd, S. J., Demanuele, C., Debener, S., Helps, S. K., James, C. J., &Sonuga-Barke, E. J. (2009). Default-mode brain dysfunction inmental disorders: a systematic review. Neuroscience andBiobehavioural Reviews, 33(3), 279–296.
Burt, T., Prudic, J., Peyser, S., Clark, J., & Sackeim, H. A. (2000). Learningand memory in bipolar and unipolar major depression: effects ofaging. Neuropsychiatry, Neuropsychology, and Behavioral Neurolo-gy, 13(4), 246–253.
Cahill, C. M., Malhi, G. S., Ivanovski, B., Lagopoulos, J., & Cohen,M. (2006). Cognitive compromise in bipolar disorder withchronic cannabis use: cause or consequence? Expert Review ofNeurotherapeutics, 6(4), 591–598.
Castaneda, A. E., Tuulio-Henriksson, A., Marttunen, M., Suvisaari, J.,& Lonnqvist, J. (2008). A review on cognitive impairments indepressive and anxiety disorders with a focus on young adults.Journal of Affective Disorders, 106(1–2), 1–27.
Cella, M., Dymond, S., & Cooper, A. (2009). Impaired flexibledecision-making in major depressive disorder. Journal of Affec-tive Disorders, 124(1–2), 207–210.
Chamberlain, S. R., & Sahakian, B. J. (2006). The neuropsychologyof mood disorders. Current Psychiatry Reports, 8(6), 458–463.
Chen, C. H., Suckling, J., Ooi, C., Jacob, R., Lupson, V., Bullmore,E. T., et al. (2010). A longitudinal fMRI study of the manicand euthymic states of bipolar disorder. Bipolar Disorders, 12,344–347.
Chen, C. H., Suckling, J., Lennox, B. R., Ooi, C., & Bullmore, E. T.(2011). A quantitative meta-analysis of fMRI studies in bipolardisorder. Bipolar Disorders, 13, 1–15.
Christensen, H., Griffiths, K., Mackinnon, A., & Jacomb, P. (1997). Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia. Journal of the International Neuro-psychological Society, 3(6), 631–651.
Clark, L., Sarna, A., & Goodwin, G. M. (2005). Impairment ofexecutive function but not memory in first-degree relatives ofpatients with bipolar I disorder and in euthymic patients withunipolar depression. The American Journal of Psychiatry, 162(10), 1980–1982.
Colombel, F. (2007). Memory bias and depression: a criticalcommentary. Encephale, 33(3 Pt 1), 242–248.
Cooney, R. E., Joormann, J., Eugene, F., Dennis, E. L., & Gotlib, I. H.(2010). Neural correlates of rumination in depression. Cognitive,Affective & Behavioural Neuroscience, 10(4), 470–478.
Crane, C., Barnhofer, T., Visser, C., Nightingale, H., & Williams, J. M.(2007). The effects of analytical and experiential rumination onautobiographical memory specificity in individuals with a historyof major depression. Behaviour Research and Therapy, 45(12),3077–3087.
Davidson, R. J., Pizzagalli, D., Nitschke, J. B., & Putnam, K. (2002).Depression: perspectives from affective neuroscience. AnnualReview of Psychology, 53, 545–574.
Debeer, E., Hermans, D., & Raes, F. (2009). Associations betweencomponents of rumination and autobiographical memory speci-ficity as measured by a Minimal Instructions AutobiographicalMemory Test. Memory, 17(8), 892–903.
Degl'Innocenti, A., & Bäckman, L. (1999). Source memory in majordepression. Journal of Affective Disorders, 54(1–2), 205–209.
Delaloye, C., Moy, G., de Bilbao, F., Baudois, S., Weber, K., Hofer,F., et al. (2010). Neuroanatomical and neuropsychologicalfeatures of elderly euthymic depressed patients with early- andlate-onset. Journal of the Neurological Sciences, 299(1–2), 19–23.
DeLuca, A. K., Lenze, E. J., Mulsant, B. H., Butters, M. A., Karp, J.F., Dew, M. A., et al. (2005). Comorbid anxiety disorder in latelife depression: association with memory decline over four years.International Journal of Geriatric Psychiatry, 20(9), 848–854.
Den Hartog, H. M., Derix, M. M., Van Bemmel, A. L., Kremer, B., &Jolles, J. (2003). Cognitive functioning in young and middle-aged unmedicated out-patients with major depression: testing theeffort and cognitive speed hypotheses. Psychological Medicine,33(8), 1443–1451.
Deyo, M., Wilson, K. A., Ong, J., & Koopman, C. (2009).Mindfulness and rumination: does mindfulness training lead toreductions in the ruminative thinking associated with depression?Explore (NY), 5(5), 265–271.
Dillon, C., Allegri, R. F., Serrano, C. M., Iturry, M., Salgado, P.,Glaser, F. B., et al. (2009). Late- versus early-onset geriatricdepression in a memory research center. Journal of Neuropsychi-atric Disease and Treatment, 5, 517–526.
Dombrovski, A. Y., Butters, M. A., Reynolds, C. F., 3rd, Houck, P. R.,Clark, L., Mazumdar, S., et al. (2008). Cognitive performance insuicidal depressed elderly: preliminary report. The AmericanJournal of Geriatric Psychiatry, 16(2), 109–115.
Neuropsychol Rev
Donaldson, C., & Lam, D. (2004). Rumination, mood and socialproblem-solving in major depression. Psychological Medicine,34(7), 1309–1318.
Donaldson, C., Lam, D., & Mathews, A. (2007). Rumination andattention in major depression. Behaviour Research and Therapy,45(11), 2664–2678.
Douglas, K. M., & Porter, R. J. (2009). Longitudinal assessment ofneuropsychological function in major depression. The Australianand New Zealand Journal of Psychiatry, 43(12), 1105–1117.
Douglas, K. M., Porter, R. J., Frampton, C. M., Gallagher, P., &Young, A. H. (2009). Abnormal response to failure inunmedicated major depression. Journal of Affective Disorders,119(1–3), 92–99.
Drevets, W. C., & Raichle, M. E. (1992). Neuroanatomical circuits indepression: implications for treatment mechanisms. Psychophar-macological Bulletin, 28, 261–273.
Drevets, W. C., Price, J. L., Simpson, J. R., Todd, R. D., Reich, T.,Vannier, M., et al. (1997). Subgenual prefrontal cortex abnormal-ities in mood disorders. Nature, 386, 824–827.
Drevets, W. C., Price, J. L., & Furey, M. L. (2008). Brain structuraland functional abnormalities in mood disorders: implications forneurocircuitry models of depression. Brain Structure & Function,213(1–2), 93–118.
Ebmeier, K., Rose, E., & Steele, D. (2006). Cognitive impairment andfMRI in major depression. Neurotoxicity Research, 10, 87–92.
Elder, G. A., De Gasperi, R., & Gama Sosa, M. A. (2006). Researchupdate: neurogenesis in adult brain and neuropsychiatric disor-ders. The Mount Sinai Journal of Medicine, 73(7), 931–940.
Elderkin-Thompson, V., Boone, K. B., Hwang, S., & Kumar, A.(2004). Neurocognitive profiles in elderly patients with fronto-temporal degeneration or major depressive disorder. Journal ofthe International Neuropsychological Society, 10(5), 753–771.
Elgamal, S., McKinnon, M. C., Ramakrishnan, K., Joffe, R. T., &MacQueen, G. (2007). Successful computer-assisted cognitiveremediation therapy in patients with unipolar depression: a proofof principle study. Psychological Medicine, 37(9), 1229–1238.
Elliott, R., Sahakian, B. J., McKay, A. P., Herrod, J. J., Robbins, T. W.,& Paykel, E. S. (1996). Neuropsychological impairments inunipolar depression: the influence of perceived failure onsubsequent performance. Psychological Medicine, 26, 975–989.
Elliott, R., Baker, S. C., Rogers, R. D., O'Leary, D. A., Paykel, E.S., Frith, C. D., et al. (1997a). Prefrontal dysfunction indepressed patients performing a complex planning task: a studyusing positron emission tomography. Psychological Medicine,27, 931–942.
Elliott, R., Sahakian, B. J., Herrod, J. J., Robbins, T. W., & Paykel, E.S. (1997b). Abnormal response to negative feedback in unipolardepression: evidence for a diagnosis specific impairment. Journalof Neurology, Neurosurgery, and Psychiatry, 63(1), 74–82.
Ellwart, T., Rinck, M., & Becker, E. S. (2003). Selective memory andmemory deficits in depressed inpatients. Depression and Anxiety,17(4), 197–206.
Falconer, D. W., Cleland, J., Fielding, S., & Reid, I. C. (2010). Usingthe Cambridge Neuropsychological Test Automated Battery(CANTAB) to assess the cognitive impact of electroconvulsivetherapy on visual and visuospatial memory. PsychologicalMedicine, 40(6), 1017–1025.
Fertuck, E. A., Marsano-Jozefowicz, S., Stanley, B., Tryon, W. W.,Oquendo, M., Mann, J. J., et al. (2006). The impact of borderlinepersonality disorder and anxiety on neuropsychological perfor-mance in major depression. Journal of Personality Disorders, 20(1), 55–70.
Fitzgerald, P. B., Srithiran, A., Benitez, J., Daskalakis, Z. Z., Oxley, T.J., Kulkarni, J., et al. (2008). An fMRI study of prefrontal brainactivation during multiple tasks in patients with major depressivedisorder. Human Brain Mapping, 29(4), 490–501.
Fleming, S. K., Blasey, C., & Schatzberg, A. F. (2004). Neuropsy-chological correlates of psychotic features in major depressivedisorders: a review and meta-analysis. Journal of PsychiatricResearch, 38(1), 27–35.
Frodl, T., Moller, H. J., & Meisenzahl, E. (2008). Neuroimaginggenetics: new perspectives in research on major depression? ActaPsychiatrica Scandinavica, 118(5), 363–372.
Frodl, T., Bokde, A. L., Scheuerecker, J., Lisiecka, D., Schoepf, V.,Hampel, H., et al. (2010). Functional connectivity bias of theorbitofrontal cortex in drug-free patients with major depression.Biological Psychiatry, 67(2), 161–167.
Furtado, C. P., Maller, J. J., & Fitzgerald, P. B. (2008). A magneticresonance imaging study of the entorhinal cortex in treatment-resistant depression. Psychiatry Research, 163, 133–142.
Gilbertson, M. W., Shenton, M. E., Ciszewski, A., Kasai, K., Lasko,N. B., Orr, S. P., et al. (2002). Smaller hippocampal volumepredicts pathologic vulnerability to psychological trauma. NatureNeuroscience, 5(11), 1242–1247.
Goder, R., Fritzer, G., Hinze-Selch, D., Huchzermeier, C., Koch, J. M.,Seeck-Hirschner, M., et al. (2007). Sleep in major depression:relation to memory performance and outcome after interpersonalpsychotherapy. Neuropsychobiology, 55(1), 36–42.
Gorwood, P., Corruble, E., Falissard, B., & Goodwin, G. M. (2008).Toxic effects of depression on brain function: impairment ofdelayed recall and the cumulative length of depressive disorder ina large sample of depressed outpatients. The American Journal ofPsychiatry, 165(6), 731–739.
Gotlib, I. H., & Joormann, J. (2010). Cognition and depression:current status and future directions. Annual Review of ClinicalPsychology, 6, 285–312.
Green, M. J., Cahill, C. M., & Malhi, G. S. (2007). The cognitive andneurophysiological basis of emotion dysregulation in bipolardisorder. Journal of Affective Disorders, 103, 29–42.
Greicius, M. D., Flores, B. H., Menon, V., Glover, G. H., Solvason, H.B., Kenna, H., et al. (2007). Resting-state functional connectivityin major depression: abnormally increased contributions fromsubgenual cingulate cortex and thalamus. Biological Psychiatry,62(5), 429–437.
Gruber, O., & Goschke, T. (2004). Executive control emerging fromdynamic interactions between brain systems mediating language,working memory and attentional processes. Acta Psychologica,115, 105–121.
Gruber, S., Rathgeber, K., Braunig, P., & Gauggel, S. (2007). Stabilityand course of neuropsychological deficits in manic and depressedbipolar patients compared to patients with Major Depression.Journal of Affective Disorders, 104(1–3), 61–71.
Gualtieri, C. T., & Johnson, L. G. (2008). Age-related cognitivedecline in patients with mood disorders. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 32(4), 962–967.
Gualtieri, C. T., & Morgan, D. W. (2008). The frequency of cognitiveimpairment in patients with anxiety, depression, and bipolardisorder: an unaccounted source of variance in clinical trials. TheJournal of Clinical Psychiatry, 69(7), 1122–1130.
Gunning-Dixon, F. M., Murphy, F. C., Alexopoulos, G. S., Majcher-Tascio, M., & Young, R. C. (2008). Executive dysfunction inelderly bipolar manic patients. The American Journal ofGeriatric Psychiatry, 16(6), 506–512.
Gunther, T., Konrad, K., De Brito, S. A., Herpertz-Dahlmann, B., &Vloet, T. D. (2011). Attentional functions in children andadolescents with ADHD, depressive disorders, and the comorbidcondition. Journal of Child Psychology and Psychiatry, 52(3),324–331.
Hamilton, J. P., & Gotlib, I. H. (2008). Neural substrates of increasedmemory sensitivity for negative stimuli in major depression.Biological Psychiatry, 63(12), 1155–1162.
Neuropsychol Rev
Hammar, A., Strand, M., Ardal, G., Schmid, M., Lund, A., & Elliott,R. (2011). Testing the cognitive effort hypothesis of cognitiveimpairment in major depression. Nordic Journal of Psychiatry, 65(1), 74–80.
Hartberg, C. B., Sundet, K., Rimol, L. M., Haukvik, U. K., Lange, E.H., Nesvag, R., et al. (2011). Subcortical brain volumes relate toneurocognition in schizophrenia and bipolar disorder and healthycontrols. Progress in Neuropsychopharmacology and BiologicalPsychiatry, 35(6), 1122–1130.
Harvey, P. O., Fossati, P., Pochon, J. B., Levy, R., Lebastard, G.,Lehericy, S., et al. (2005). Cognitive control and brain resourcesin major depression: an fMRI study using the n-back task.NeuroImage, 26(3), 860–869.
Hasher, L., & Zacks, R. T. (1979). Automatic and effortful processingin memory. Journal of Experimental Psychology. General, 108,356–388.
Hasler, G., Drevets, W. C., Manji, H. K., & Charney, D. S. (2004).Discovering endophenotypes for major depression. Neuropsycho-pharmacology, 29(10), 1765–1781.
Hasler, G., Drevets, W. C., Gould, T. D., Gottesman, I. I., & Manji, H.K. (2006). Toward constructing an endophenotype strategy forbipolar disorders. Biological Psychiatry, 60(2), 93–105.
Henry, J., & Crawford, J. R. (2005). A meta-analytic review of verbalfluency deficits in depression. Journal of Clinical and Experi-mental Neuropsychology, 27(1), 78–101.
Hermans, D., Vandromme, H., Debeer, E., Raes, F., Demyttenaere, K.,Brunfaut, E., et al. (2008). Overgeneral autobiographical memorypredicts diagnostic status in depression. Behaviour Research andTherapy, 46(5), 668–677.
Herrera-Guzman, I., Gudayol-Ferre, E., Herrera-Guzman, D., Guardia-Olmos, J., Hinojosa-Calvo, E., & Herrera-Abarca, J. E. (2009).Effects of selective serotonin reuptake and dual serotonergic-noradrenergic reuptake treatments on memory and mentalprocessing speed in patients with major depressive disorder.Journal of Psychiatric Research, 43(9), 855–863.
Hickie, I. B., Naismith, S., Ward, P. B., Turner, K., Scott, E., Mitchell,P., et al. (2005). Reduced hippocampal volumes and memory lossin patients with early- and late-onset depression. The BritishJournal of Psychiatry, 186, 197–202.
Hickie, I. B., Naismith, S. L., Ward, P. B., Little, C. L., Pearson, M.,Scott, E. M., et al. (2007). Psychomotor slowing in older patientswith major depression: Relationships with blood flow in thecaudate nucleus and white matter lesions. Psychiatry Research,155(3), 211–220.
Hindmarch, I., Kimber, S., & Cockle, S. M. (2000). Abrupt and briefdiscontinuation of antidepressant treatment: effects on cognitivefunction and psychomotor performance. International ClinicalPsychopharmacology, 15(6), 305–318.
Holmes, M. K., Erickson, K., Luckenbaugh, D. A., Drevets, W. C.,Bain, E. E., Cannon, D. M., et al. (2008). A comparison ofcognitive functioning in medicated and unmedicated subjectswith bipolar depression. Bipolar Disorders, 10(7), 806–815.
Hsiao, Y. L., Wu, Y. S., Wu, J. Y., Hsu, M. H., Chen, H. C., Lee, S. Y., et al.(2009). Neuropsychological functions in patients with bipolar I andbipolar II disorder. Bipolar Disorders, 11(5), 547–554.
Jaeger, J., Berns, S., Uzelac, S., & Davis-Conway, S. (2006).Neurocognitive deficits and disability in major depressivedisorder. Psychiatry Research, 145(1), 39–48.
Johanson, A., Gustafson, L., Risberg, J., Rosen, I., Sjobeck, M., &Silfverskiold, P. (2005). Long-term follow-up in depressedpatients treated with electroconvulsive therapy. The Journal ofECT, 21(4), 214–220.
Joormann, J., & Gotlib, I. H. (2008). Updating the contents ofworking memory in depression: interference from irrelevantnegative material. Journal of Abnormal Psychology, 117(1),182–192.
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom ofyour body and mind to face stress, pain, and illness. New York:Delta Trade Paperbacks.
Keefe, R. S. (1995). The contribution of neuropsychology topsychiatry. The American Journal of Psychiatry, 152(1), 6–15.
Kiloh, L. G. (1961). Pseudo-dementia. Acta Psychiatrica Scandinavica,37, 336–351.
Koster, E. H., De Raedt, R., Leyman, L., & De Lissnyder, E. (2010).Mood-congruent attention and memory bias in dysphoria:exploring the coherence among information-processing biases.Behaviour Research and Therapy, 48(3), 219–225.
Kronhaus, D. M., Lawrence, N. S., Williams, A. M., Frangou, S.,Brammer, M. J., Williams, S. C., et al. (2006). Stroopperformance in bipolar disorder: further evidence for abnormalitiesin the ventral prefrontal cortex. Bipolar Disorders, 8, 28–39.
Lahr, D., Beblo, T., & Hartje, W. (2007). Cognitive performance andsubjective complaints before and after remission of majordepression. Cognitive Neuropsychiatry, 12(1), 25–45.
Laks, J., & Engelhardt, E. (2010). Peculiarities of geriatric psychiatry:a focus on aging and depression. CNS Neuroscience &Therapeutics, 16(6), 374–379.
Larson, E. R., Shear, P. K., Krikorian, R., Welge, J., & Strakowski, S.M. (2005). Working memory and inhibitory control among manicand euthymic patients with bipolar disorder. Journal of theInternational Neuropsychological Society, 11(2), 163–172.
Legendre, S. A., Stern, R. A., Solomon, D. A., Furman, M. J., &Smith, K. E. (2003). The influence of cognitive reserve onmemory following electroconvulsive therapy. The Journal ofNeuropsychiatry and Clinical Neurosciences, 15(3), 333–339.
Leppanen, J. M. (2006). Emotional information processing in mooddisorders: a review of behavioral and neuroimaging findings.Current Opinion in Psychiatry, 19(1), 34–39.
Levy, B., Monzani, B. A., Stephansky, M. R., & Weiss, R. D. (2008).Neurocognitive impairment in patients with co-occurring bipolardisorder and alcohol dependence upon discharge from inpatientcare. Psychiatry Research, 161(1), 28–35.
Lorenzetti, V., Allen, N. B., Fornito, A., & Yucel, M. (2009). Structuralbrain abnormalities in major depressive disorder: a selectivereview of recent MRI studies. Journal of Affective Disorders, 117(1–2), 1–17.
Lyons, D. M., Yang, C., Sawyer-Glover, A. M., Moseley, M. E., &Schatzberg, A. F. (2001). Early life stress and inherited variation inmonkey hippocampal volumes. Archives of General Psychiatry, 58(12), 1145–1151.
Madden, J. J., Luhan, J. A., Kaplan, L. A., & Manfredi, H. M. (1952).Nondementing psychoses in older persons. Journal of theAmerican Medical Association, 150, 1567–1572.
Marchand, W. R., & Yurgelun-Todd, D. (2010). Striatal structure andfunction in mood disorders: a comprehensive review. BipolarDisorders, 12, 764–785.
Martinez-Aran, A., Vieta, E., Torrent, C., Sanchez-Moreno, J.,Goikolea, J. M., Salamero, M., et al. (2007). Functional outcomein bipolar disorder: the role of clinical and cognitive factors.Bipolar Disorders, 9(1–2), 103–113.
Martinez-Aran, A., Torrent, C., Tabares-Seisdedos, R., Salamero, M.,Daban, C., Balanza-Martinez, V., et al. (2008). Neurocognitiveimpairment in bipolar patients with and without history ofpsychosis. The Journal of Clinical Psychiatry, 69(2), 233–239.
Martinez-Aran, A., Scott, J., Colom, F., Torrent, C., Tabares-Seisdedos, R., Daban, C., et al. (2009). Treatment nonadherenceand neurocognitive impairment in bipolar disorder. The Journalof Clinical Psychiatry, 70(7), 1017–1023.
Martino, D. J., Marengo, E., Igoa, A., Scapola, M., Ais, E. D., Perinot,L., et al. (2009). Neurocognitive and symptomatic predictors offunctional outcome in bipolar disorders: a prospective 1 yearfollow-up study. Journal of Affective Disorders, 116(1–2), 37–42.
Neuropsychol Rev
Marvel, C. L., & Paradiso, S. (2004). Cognitive and neurologicalimpairment in mood disorders. Psychiatric Clinics of NorthAmerica, 27(19–36), vii–viii.
Mayberg, H. S. (1997). Limbic-cortical dysregulation: a proposedmodel of depression. The Journal of Neuropsychiatry andClinical Neurosciences, 9(3), 471–481.
McDermott, L. M., & Ebmeier, K. P. (2009). A meta-analysis ofdepression severity and cognitive function. Journal of AffectiveDisorders, 119(1–3), 1–8.
McGrath, J., Scheldt, S., Welham, J., & Clair, A. (1997). Performanceon tests sensitive to impaired executive ability in schizophrenia,mania and well controls: acute and subacute phases. SchizophreniaResearch, 26(2–3), 127–137.
McKinnon, M. C., Yucel, K., Nazarov, A., & MacQueen, G. M.(2009). A meta-analysis examining clinical predictors of hippo-campal volume in patients with major depressive disorder.Journal of Psychiatry & Neuroscience, 34(1), 41–54.
Melcher, T., Falkai, P., & Gruber, O. (2008). Functional brainabnormalities in psychiatric disorders: neural mechanisms todetect and resolve cognitive conflict and interference. BrainResearch Reviews, 59, 96–124.
Michopoulos, I., Zervas, I. M., Pantelis, C., Tsaltas, E., Papakosta, V.M., Boufidou, F., et al. (2008). Neuropsychological andhypothalamic-pituitary-axis function in female patients withmelancholic and non-melancholic depression. European Archivesof Psychiatry and Clinical Neuroscience, 258(4), 217–225.
Mirochnic, S., Wolf, S., Staufenbiel, M., & Kempermann, G. (2009).Age effects on the regulation of adult hippocampal neurogenesis byphysical activity and environmental enrichment in the APP23 mousemodel of Alzheimer disease. Hippocampus, 19(10), 1008–1018.
Mitterschiffthaler, M. T., Williams, S. C., Walsh, N. D., Cleare, A. J.,Donaldson, C., Scott, J., et al. (2008). Neural basis of theemotional Stroop interference effect in major depression.Psychological Medicine, 38(2), 247–256.
Moffoot, A. P., O'Carroll, R. E., Bennie, J., Carroll, S., Dick, H.,Ebmeier, K. P., et al. (1994). Diurnal variation of mood andneuropsychological function in major depression with melancho-lia. Journal of Affective Disorders, 32(4), 257–269.
Mur, M., Portella, M. J., Martinez-Aran, A., Pifarre, J., & Vieta, E.(2009). Influence of clinical and neuropsychological variables onthe psychosocial and occupational outcome of remitted bipolarpatients. Psychopathology, 42(3), 148–156.
Murphy, F. C., & Sahakian, B. J. (2001). Neuropsychology of bipolardisorder. The British Journal of Psychiatry. Supplement, 41,s120–s127.
Murphy, F. C., Sahakian, B. J., Rubinsztein, J. S., Michael, A., Rogers,R. D., Robbins, T. W., et al. (1999). Emotional bias and inhibitorycontrol processes in mania and depression. PsychologicalMedicine, 29(6), 1307–1321.
Murphy, F. C., Michael, A., Robbins, T. W., & Sahakian, B. J. (2003).Neuropsychological impairment in patients with major depres-sive disorder: the effects of feedback on task performance.Psychological Medicine, 33(3), 455–467.
Naismith, S. L., Hickie, I. B., Ward, P. B., Turner, K., Scott, E., Little,C., et al. (2002). Caudate nucleus volumes and geneticdeterminants of homocysteine metabolism in the prediction ofpsychomotor speed in older persons with depression. TheAmerican Journal of Psychiatry, 159(12), 2096–2098.
Naismith, S. L., Norrie, L., Lewis, S. J., Rogers, N. L., Scott, E. M., &Hickie, I. B. (2009). Does sleep disturbance mediate neuropsy-chological functioning in older people with depression? Journalof Affective Disorders, 116(1–2), 139–143.
Naismith, S. L., Redoblado-Hodge, M. A., Lewis, S. J., Scott, E. M.,& Hickie, I. B. (2010). Cognitive training in affective disordersimproves memory: a preliminary study using the NEARapproach. Journal of Affective Disorders, 121(3), 258–262.
Neylan, T. C., Canick, J. D., Hall, S. E., Reus, V. I., Sapolsky, R. M.,& Wolkowitz, O. M. (2001). Cortisol levels predict cognitiveimpairment induced by electroconvulsive therapy. BiologicalPsychiatry, 50(5), 331–336.
O'Brien, J. T., Lloyd, A., McKeith, I., Gholkar, A., & Ferrier, N.(2004). A longitudinal study of hippocampal volume, cortisollevels, and cognition in older depressed subjects. The AmericanJournal of Psychiatry, 161(11), 2081–2090.
O'Connor, D. W., Gardner, B., Eppingstall, B., & Tofler, D. (2010).Cognition in elderly patients receiving unilateral and bilateralelectroconvulsive therapy: a prospective, naturalistic comparison.Journal of Affective Disorders, 124(3), 235–240.
Paizanis, E., Hamon, M., & Lanfumey, L. (2007). Hippocampalneurogenesis, depressive disorders, and antidepressant therapy.Neural Plasticity, 2007, 73754.
Pálsson, S., Johansson, B., Berg, S., & Skoog, I. (2000). A populationstudy on the influence of depression on neuropsychologicalfunctioning in 85-year-olds. Acta Psychiatrica Scandinavica, 101(3), 185–193.
Peretti, S., Judge, R., & Hindmarch, I. (2000). Safety and tolerabilityconsiderations: tricyclic antidepressants vs. selective serotoninreuptake inhibitors. Acta Psychiatrica Scandinavica Supplementum,403, 17–25.
Philippot, P., & Brutoux, F. (2008). Induced rumination dampensexecutive processes in dysphoric young adults. Journal of Behav-ioural Therapy and Experimental Psychiatry, 39(3), 219–227.
Phillips, M. L., Ladouceur, C. D., & Drevets, W. C. (2008). Aneural model of voluntary and automatic emotion regulation:implications for understanding the pathophysiology and neuro-development of bipolar disorder. Molecular Psychiatry, 13(829), 833–857.
Porter, R. J., Bourke, C., & Gallagher, P. (2007). Neuropsychologicalimpairment in major depression: its nature, origin and clinicalsignificance. The Australian and New Zealand Journal ofPsychiatry, 41(2), 115–128.
Porterfield, T., Cook, M., Deary, I. J., & Ebmeier, K. P. (1997).Neuropsychological function and diurnal variation in depression.Journal of Clinical and Experimental Neuropsychology, 19(6),906–913.
Post, R. M. (1992). Transduction of psychosocial stress into theneurobiology of recurrent affective disorder. The AmericanJournal of Psychiatry, 149(8), 999–1010.
Raes, F., Watkins, E. R., Williams, J. M., & Hermans, D. (2008). Non-ruminative processing reduces overgeneral autobiographicalmemory retrieval in students. Behaviour Research and Therapy,46(6), 748–756.
Raichle, M. E., MacLeod, A. M., Snyder, A. Z., Powers, W. J.,Gusnard, D. A., & Shulman, G. L. (2001). A default mode ofbrain function. Proceedings of the National Academy of Sciencesof the United States of America, 98(2), 676–682.
Ramel, W., Goldin, P. R., Carmona, P. E., & McQuaid, J. R. (2004).The effects of mindfulness meditation on cognitive processes andaffect in patients with past depression. Cognitive Therapy andResearch, 28(4), 435–455.
Rapp, M. A., Dahlman, K., Sano, M., Grossman, H. T., Haroutunian,V., & Gorman, J. M. (2005). Neuropsychological differencesbetween late-onset and recurrent geriatric major depression. TheAmerican Journal of Psychiatry, 162(4), 691–698.
Rathgeber, K., & Gauggel, S. (2006). Neuropsychology of bipolardisorders. Psychiatrische Praxis, 33(Suppl 1), S60–S70.
Reppermund, S., Ising, M., Lucae, S., & Zihl, J. (2009). Cognitiveimpairment in unipolar depression is persistent and non-specific:further evidence for the final common pathway disorderhypothesis. Psychological Medicine, 39(4), 603–614.
Richards, P. M., & Ruff, R. M. (1989). Motivational effects onneuropsychological functioning: comparison of depressed versus
Neuropsychol Rev
nondepressed individuals. Journal of Consulting and ClinicalPsychology, 57, 396–402.
Rinck, M., & Becker, E. S. (2005). A comparison of attentional biasesand memory biases in women with social phobia and majordepression. Journal of Abnormal Psychology, 114(1), 62–74.
Ringen, P. A., Vaskinn, A., Sundet, K., Engh, J. A., Jonsdottir, H.,Simonsen, C., et al. (2010). Opposite relationships betweencannabis use and neurocognitive functioning in bipolar disorderand schizophrenia. Psychological Medicine, 40(8), 1337–1347.
Rogers, M. A., Kasai, K., Koji, M., Fukuda, R., Iwanami, A.,Nakagome, K., et al. (2004). Executive and prefrontal dysfunc-tion in unipolar depression: a review of neuropsychological andimaging evidence. Neuroscience Research, 50(1), 1–11.
Rose, E. J., Simonotto, E., & Ebmeier, K. P. (2006). Limbic over-activity in depression during preserved performance on then-back task. NeuroImage, 29, 203–215.
Rosenbloom, M. J., O'Reilly, A., Sassoon, S. A., Sullivan, E. V., &Pfefferbaum, A. (2005). Persistent cognitive deficits incommunity-treated alcoholic men and women volunteering forresearch: limited contribution from psychiatric comorbidity.Journal of Studies on Alcohol and Drugs, 66(2), 254–265.
Roskar, S., Zorko, M., Bucik, V., & Marusic, A. (2007). Problemsolving for depressed suicide attempters and depressedindividuals without suicide attempt. Psychiatria Danubia, 19(4), 296–302.
Rucklidge, J. J. (2006). Impact of ADHD on the neurocognitivefunctioning of adolescents with bipolar disorder. BiologicalPsychiatry, 60(9), 921–928.
Sanchez-Moreno, J., Martinez-Aran, A., Colom, F., Scott, J., Tabares-Seisdedos, R., Sugranyes, G., et al. (2009). Neurocognitivedysfunctions in euthymic bipolar patients with and without priorhistory of alcohol use. The Journal of Clinical Psychiatry, 70(8),1120–1127.
Sapolsky, R. M. (1996). Why stress is bad for your brain. Science, 273(9), 749–750.
Savard, R. J., Rey, A. C., & Post, R. M. (1980). Halstead-ReitanCategory Test in bipolar and unipolar affective disorders. TheJournal of Nervous and Mental Disease, 5, 297–304.
Savitz, J. B., van der Merwe, L., Stein, D. J., Solms, M., & Ramesar,R. S. (2008). Neuropsychological task performance in bipolarspectrum illness: genetics, alcohol abuse, medication andchildhood trauma. Bipolar Disorders, 10(4), 479–494.
Schatzberg, A. F., Posener, J. A., DeBattista, C., Kalehzan, B. M.,Rothschild, A. J., & Shear, P. K. (2000). Neuropsychologicaldeficits in psychotic versus nonpsychotic major depression andno mental illness. The American Journal of Psychiatry, 157(7),1095–1100.
Scheurich, A., Fellgiebel, A., Schermuly, I., Bauer, S., Wolfges, R., &Muller, M. J. (2008). Experimental evidence for a motivationalorigin of cognitive impairment in major depression. PsychologicalMedicine, 38(2), 237–246.
Schlosser, N., Wolf, O. T., & Wingenfeld, K. (2011). Cognitivecorrelates of hypothalamic–pituitary–adrenal axis in majordepression. Expert Review of Endocrinology and Metabolism, 6(1), 109–126.
Secora, A. M., Eddie, D., Wyman, B. J., Brooks, D. J., Mariani, J. J.,& Levin, F. R. (2010). A comparison of psychosocial andcognitive functioning between depressed and non-depressedpatients with cannabis dependence. Journal of AddictiveDiseases, 29(3), 325–337.
Semkovska, M., & McLoughlin, D. M. (2010). Objective cognitiveperformance associated with electroconvulsive therapy fordepression: a systematic review and meta-analysis. BiologicalPsychiatry, 68(6), 568–577.
Shamay-Tsoory, S., Harari, H., Szepsenwol, O., & Levkovitz, Y.(2009). Neuropsychological evidence of impaired cognitive
empathy in euthymic bipolar disorder. The Journal of Neuropsy-chiatry and Clinical Neurosciences, 21(1), 59–67.
Sheline, Y. I., Wang, P. W., Gado, M. H., Csernansky, J. G., & Vannier,M. W. (1996). Hippocampal atrophy in recurrent major depres-sion. Proceedings of the National Academy of Sciences of theUnited States of America, 93(9), 3908–3913.
Sheline, Y. I., Barch, D. M., Price, J. L., Rundle, M. M., Vaishnavi, S.N., Snyder, A. Z., et al. (2009). The default mode network andself-referential processes in depression. Proceedings of theNational Academy of Sciences of the United States of America,106(6), 1942–1947.
Siegle, G. J., Steinhauer, S. R., Thase, M. E., Stenger, V. A., & Carter,C. S. (2002). Can’t shake that feeling: event-related fMRIassessment of sustained amygdala activity in response toemotional information in depressed individuals. BiologicalPsychiatry, 51, 693–707.
Smith, G. E., Rasmussen, K. G., Jr., Cullum, C. M., Felmlee-Devine,M. D., Petrides, G., Rummans, T. A., et al. (2010). A randomizedcontrolled trial comparing the memory effects of continuationelectroconvulsive therapy versus continuation pharmacotherapy:results from the Consortium for Research in ECT (CORE) study.The Journal of Clinical Psychiatry, 71(2), 185–193.
Sotiropoulos, I., Cerqueira, J. J., Catania, C., Takashima, A., Sousa,N., & Almeida, O. F. (2008). Stress and glucocorticoid footprintsin the brain-the path from depression to Alzheimer’s disease.Neuroscience & Biobehavioural Reviews, 32(6), 1161–1173.
Steele, J. D., Meyer, M., & Ebmeier, K. P. (2004). Neural predictiveerror signal correlates with depressive illness severity in a gameparadigm. NeuroImage, 23, 269–280.
Strakowski, S. M., Adler, C. M., & DelBello, M. P. (2002). VolumetricMRI studies of mood disorders: do they distinguish unipolar andbipolar disorder? Bipolar Disorders, 4, 80–88.
Swerdlow, N. R., & Koob, G. F. (1987). Dopamine, schizophrenia,mania, and depression: toward a unified hypothesis in cortico-striato-pallido-thalamic function. The Behavioral and BrainSciences, 10, 197–245.
Taylor Tavares, J. V., Clark, L., Cannon, D. M., Erickson, K., Drevets,W. C., & Sahakian, B. J. (2007). Distinct profiles of neuro-cognitive function in unmedicated unipolar depression andbipolar II depression. Biological Psychiatry, 62(8), 917–924.
Taylor, W. D., Steffens, D. C., McQuoid, D. R., Payne, M. E., Lee, S.H., Lai, T. J., et al. (2003). Smaller orbital frontal cortex volumesassociated with functional disability in depressed elders. BiologicalPsychiatry, 53(2), 144–149.
Thomas, A. J., Gallagher, P., Robinson, L. J., Porter, R. J., Young, A.H., Ferrier, I. N., et al. (2009). A comparison of neurocognitiveimpairment in younger and older adults with major depression.Psychological Medicine, 39(5), 725–733.
Torrent, C., Martinez-Aran, A., Daban, C., Sanchez-Moreno, J.,Comes, M., Goikolea, J. M., et al. (2006). Cognitive impairmentin bipolar II disorder. The British Journal of Psychiatry, 189,254–259.
Trebo, E., Holzner, B., Pircher, M., Prunnlechner, R., & Gunther, V.(2007). The effects of a computer assisted cognitive trainingon neuropsychological parameters, mood and dysfunctionalcognitions in depressive patients. Neuropsychiatrie, 21(3),207–215.
Uekermann, J., Daum, I., Schlebusch, P., Wiebel, B., & Trenckmann,U. (2003). Depression and cognitive functioning in alcoholism.Addiction, 98(11), 1521–1529.
van den Heuvel, N., Smits, C. H., Deeg, D. J., & Beekman, A. T.(1996). Personality: a moderator of the relation betweencognitive functioning and depression in adults aged 55-85?Journal of Affective Disorders, 41(3), 229–240.
van Gorp, W. G., Altshuler, L., Theberge, D. C., Wilkins, J., & Dixon,W. (1998). Cognitive impairment in euthymic bipolar patients
Neuropsychol Rev

with and without prior alcohol dependence. A preliminary study.Archives of General Psychiatry, 55(1), 41–46.
Veiel, H. O. F. (1997). A preliminary profile of neuropsychologicaldeficits associated with major depression. Journal of Clinical andExperimental Neuropsychology, 19, 587–603.
Videbech, P., Ravnkilde, B., Kristensen, S., Egander, A., Clemmensen,K., Rasmussen, N. A., et al. (2003). The Danish PET/depressionproject: poor verbal fluency performance despite normal prefrontalactivation in patients with major depression. Psychiatry Research,123(1), 49–63.
Vythilingam, M., Heim, C., Newport, J., Miller, A. H., Anderson, E.,Bronen, R., et al. (2002). Childhood trauma associated withsmaller hippocampal volume in women with major depression.The American Journal of Psychiatry, 159(12), 2072–2080.
Wagner, G., Sinsel, E., Sobanski, T., Kohler, S., Marinou, V., Mentzel,H. J., et al. (2006). Cortical inefficiency in patients with unipolardepression: an event-related FMRI study with the Stroop task.Biological Psychiatry, 59, 958–965.
Wagner, G., Koch, K., Schachtzabel, C., Reichenbach, J. R., Sauer, H.,& Schlosser Md, R. G. (2008). Enhanced rostral anteriorcingulate cortex activation during cognitive control is related toorbitofrontal volume reduction in unipolar depression. Journal ofPsychiatry & Neuroscience, 33(3), 199–208.
Wang, S. H., Zhang, Z. J., Guo, Y. J., Teng, G. J., & Chen, B. A.(2008). Hippocampal neurogenesis and behavioural studies onadult ischemic rat response to chronic mild stress. BehaviouralBrain Research, 189(1), 9–16.
Watkins, E., & Brown, R. G. (2002). Rumination and executivefunction in depression: an experimental study. Journal ofNeurology, Neurosurgery, and Psychiatry, 72(3), 400–402.
Weber, B., Fritze, J., Schneider, B., Kuhner, T., & Maurer, K. (2002).Bias in computerized neuropsychological assessment of depres-sive disorders caused by computer attitude. Acta PsychiatricaScandinavica, 105(2), 126–130.
Werner, N. S., Meindl, T., Materne, J., Engel, R. R., Huber, D., Riedel,M., et al. (2009). Functional MRI study of memory-related brainregions in patients with depressive disorder. Journal of AffectiveDisorders, 119, 124–131.
Westheide, J., Quednow, B. B., Kuhn, K. U., Hoppe, C., Cooper-Mahkorn, D., Hawellek, B., et al. (2008). Executive performanceof depressed suicide attempters: the role of suicidal ideation.European Archives of Psychiatry and Clinical Neuroscience, 258(7), 414–421.
Whalley, H. C., McKirdy, J., Romaniuk, L., Sussmann, J., Johnstone,E. C., Wan, H. I., et al. (2009). Functional imaging ofemotional memory in bipolar disorder and schizophrenia.Bipolar Disorders, 11, 840–856.
WHO. (1991). ICD-10 classification of mental and behavioraldisorders with glossary and diagnostic criteria for researchICD-10: DCR-10. Edinburgh: Churchchill Livingstone.
Wingo, A. P., Harvey, P. D., & Baldessarini, R. J. (2009). Neuro-cognitive impairment in bipolar disorder patients: functionalimplications. Bipolar Disorders, 11(2), 113–125.
Wingo, A. P., Wingo, T. S., Harvey, P. D., & Baldessarini, R. J. (2009).Effects of lithium on cognitive performance: a meta-analysis. TheJournal of Clinical Psychiatry, 70(11), 1588–1597.
Withall, A., Harris, L. M., & Cumming, S. R. (2010). A longitudinalstudy of cognitive function in melancholic and non-melancholicsubtypes of major depressive disorder. Journal of AffectiveDisorders, 123(1–3), 150–157.
Wittchen, H. U. (1994). Wie häufig sind depressive Erkrankungen? InM. Hautzinger (Ed.), Verhaltenstherapie bei depressionen (pp.10–24). Baltmannsweiler: Röttger-Schneider.
Yuan, Y., Zhu, W., Zhang, Z., Bai, F., Yu, H., Shi, Y., et al. (2008).Regional gray matter changes are associated with cognitivedeficits in remitted geriatric depression: an optimized voxel-based morphometry study. Biological Psychiatry, 64(6), 541–544.
Zihl, J., & Münzel, K. (2004). Der Beitrag der Neuropschologie fürdie Psychiatrie. In S. Lautenbacher & S. Gauggel (Eds.),Neuropsychologie psychischer Störungen (pp. 28–41). Berlin:Springer.
Zylowska, L., Ackerman, D. L., Yang, M. H., Futrell, J. L., Horton, N.L., Hale, T. S., et al. (2008). Mindfulness meditation training inadults and adolescents with ADHD: a feasibility study. Journal ofAttention Disorders, 11(6), 737–746.
Neuropsychol Rev