spatial working memory in individuals at high risk for psychosis: longitudinal fmri study
TRANSCRIPT

Schizophrenia Research 123 (2010) 45–52
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r.com/ locate /schres
Spatial working memory in individuals at high risk for psychosis:Longitudinal fMRI study
P. Fusar-Poli a,b,⁎, M.R. Broome a,c, P. Matthiasson a, J.B. Woolley a, L.C. Johns a, P. Tabraham a,E. Bramon a, L. Valmaggia a, S.C. Williams d, P. McGuire a
a Psychosis Clinical Academic Group, Institute of Psychiatry, King’s Health Partners, King’s College London, UKb Section of Psychiatry, Department of Behavioural Sciences, University of Pavia, Italyc Health Sciences Research Institute, Warwick Medical School, University of Warwick, Coventry, UKd Brain Image Analysis Unit, Department of Biostatistics and Computing, Institute of Psychiatry, King's College London, UK
a r t i c l e i n f o
⁎ Corresponding author. Neuroimaging Section, DivMedicine PO67, Institute of Psychiatry, De CrespigLondon, UK. Tel.: +44 77 8666 6570; fax: +44 20 78
E-mail address: [email protected] (P. Fusar-Poli).
0920-9964/$ – see front matter © 2010 Elsevier B.V.doi:10.1016/j.schres.2010.06.008
a b s t r a c t
Article history:Received 13 August 2009Received in revised form 25 May 2010Accepted 12 June 2010Available online 4 August 2010
Background: Neurocognitive impairments in executive and mnemonic domains are alreadyevident in the pre-psychotic phases. The longitudinal dynamic course of the neurofunctionalabnormalities underlying liability to psychosis and their relation to clinical outcomes is unknown.Methods: In this study we used functional magnetic resonance imaging (fMRI) in a cohort ofsubjects at ultra high clinical risk for psychosis (with an “At Risk Mental State”, ARMS) and inhealthy controls. Images were acquired at baseline and again after one year on a 1.5 Tesla Signa,while patients were performing a visuospatial working memory task. Psychopathologicalassessment of the prodromal symptoms was conducted at the same time points by using theCAARMS and the PANSS instruments.Results: There were no significant differences between the ARMS and control groups with respectto age or IQ. Although both groups performed the PAL task with a high degree of accuracy, theARMS showed an increased latency in answers during the most demanding level of the task. Atbaseline, such cognitive impairmentwas associatedwith reduced activation in the left precuneus,left superior parietal lobule, right middle temporal gyrus in the ARMS as compared to controls. Inaddition, the ARMS failed to activate parietal areas with increasing difficulty of the task. Betweenpresentation and follow-up the overall clinical status of the ARMS sample improved, despite 2 outof the 15 subjects having developed a full-blown psychosis: the CAARMS (perceptual disorder andthought disorder subscales) and the PANNS general scores decreased, while the GAF scoreincreased. Such clinical ameliorationwas associatedwith a longitudinal compensatory increase inoccipitoparietal regions.Conclusions: The prodromal phase of psychosis is associatedwith functional alterations in parietaland temporal networks subserving visuospatial working memory which are more evident underhigh cognitive loads. The clinical improvement at one year is associated with a compensatoryincrease in occipitoparietal regions.
© 2010 Elsevier B.V. All rights reserved.
Keywords:Prodromal psychosisfMRIWorking memoryARMSCognition
ision of Psychologicalny Park 16, SE58AF48 0976.
All rights reserved.
1. Introduction
Subjects with an “At RiskMental State, ARMS” (Yung et al.,2005) present with attenuated psychotic symptoms whichare associated with an increased risk of developing a psy-chotic disorder within the following months (Cannon et al.,2007). The prodromal state for psychosis is characterized bypsychosocial impairment and neurocognitive deficits (Brewer

46 P. Fusar-Poli et al. / Schizophrenia Research 123 (2010) 45–52
et al., 2005; Lencz et al., 2006; Eastvold et al., 2007; Nieman etal., 2007), in particular in working memory domains (East-stvold et al., 2007). ARMS subjects can be distinguished fromhealthy controls specifically on the basis of working memoryperformance (Smith et al., 2006; Pflueger et al., 2007) andtheir baseline working memory functioning can predict thelongitudinal development of psychosis (Pukrop et al., 2007).Workingmemory encompasses twounimodal storage systems:a phonological loop and a visuospatial sketchpad. The latter iscapable of maintaining and manipulating visual and spatialinformation, a process that is crucial for performing a range ofcognitive tasks (Repovs and Baddeley, 2006). There is evidencesuggesting a relationship between spatial working memoryimpairments and the predisposition towards schizophrenia(Wood et al., 2003). In fact, the pattern of spatial workingmemory performance in relatives of schizophrenic reflect themodel of latent genetic liability upholding spatial workingmemory as a reliable cognitive endophenotype (Saperstein etal., 2006).
In the present study we sought to investigate cross-sectionally and longitudinally the neurofunctional correlatesof spatial working memory in the prodromal phases of psy-chosis. On the basis of previous evidence (Wood et al., 2002,2003; Smith et al., 2006; Vance et al., 2006; Fusar-Poli et al.,2007), we predicted that at baseline, ARMS subjects wouldshow altered cortical activation during the task relative tocontrols. The second hypothesis was that these differenceswould become more apparent as the mnemonic demands ofthe task were increased (Gould et al., 2003). We then testedthe hypothesis that over the subsequent follow-up period,baseline alterations in cortical function would changelongitudinally in parallel with changes in the clinical statusof the ARMS group.
2. Materials and method
2.1. Subjects
2.1.1. ARMS group (n=15)Individuals meeting PACE criteria for the At Risk Mental
State (ARMS (Yung et al., 1998)) were recruited fromOutreach and Support in South London (OASIS (Broomeet al., 2005)). The diagnosis was based on assessment by twoexperienced clinicians using the Comprehensive Assessmentfor the ARMS (CAARMS (Yung et al., 2005)), and a consensusmeeting with the clinical team. An individual meets PACEcriteria for the ARMS if they display one or more of thefollowing: ‘attenuated’ positive symptoms; frank psychoticsymptoms that last less than one week and resolve withouttreatment; a recent decline in function coupled with eitherschizotypal personality disorder or a first-degree relativewith psychosis. The subjects recruited were antipsychoticnaïve and were representative of the local population ofpeople presenting with an ARMS in terms of age, gender,ethnicity, and duration and intensity of symptoms (Broomeet al., 2005). They underwent a baseline scanning and asecond scan after one year. During the follow-up period,all ARMS subjects were received case management (whichincluded psycho education, crisis intervention, familycounseling and assistance with education or work-relateddifficulties, according to need) and Cognitive Behavioural
Therapy (CBT); in addition seven of them gave their consentto psychopharmacological treatment with low dosages ofantipsychotics (Quetiapine, dosage range 25 mg–150 mg/day, mean dosage 100 mg/day).
2.1.2. ControlsHealthy volunteers (n=15) were recruited via advertise-
ments in the local media. In order to match the ARMS subjectson sociodemographical variables, all control subjects wererecruited in the same borough of London as the clinicalsubjects (Lambeth), were native speakers of English andwereright-handed. Subjects and controls accepted to participate inthe study after they wrote written informed consent.
2.2. Clinical measures
Subjects were excluded if there was a history of neu-rological disorder or they met DSM-IV criteria for a substancemisuse disorder. Estimated IQ was assessed by using theNational Adult Reading Test (NART) (Nelson and Willison,1991). The severity of symptoms in the clinical groupswas assessed at the time of scanning using the followinginstruments: the Positive and Negative Symptom Scale(PANSS) (Kay, 1990), the Comprehensive Assessment of AtRiskMental States (CAARMS (Yung et al., 2005)). Handednesswas evaluated with the Lateral Preferences Inventory (Coren,1993). Consumption of illicit substances, tobacco and coffee/tea was evaluated using a modified version of the CannabisExperience Questionnaire (CEQ)(Barkus et al., 2006).
2.3. Experimental task
Stimuli were presented in 22.5 s epochs, alternating with34.5 s epochs of crosshair fixation; this cycle was repeatedtwelve times (for a total of 24 epochs) so the total duration ofthe experiment was 686 s or 343 images (TR=2 s). Cognitiveload was manipulated by presenting trials at one of threepossible levels of difficulty (easy, intermediate, and hard) in ablock design, with four blocks of each level of difficulty. Therewere thus a total of 12 blocks of trials alternating with12 blocks of crosshair fixation. The blocks of trials werealways presented in the same sequence with respect to levelof difficulty: easy, intermediate, and then hard. Each blockcomprised seven trials. Further details of the experimentaltasks are presented in Fig. 1.
2.4. fMRI scanning
2.4.1. Image acquisitionImages were acquired on a 1.5 Tesla Signa (GE) system at
the Maudsley Hospital, London. T2*-weighted images wereacquired in 38×3 mm slices, with a 0.3 mm gap in 14 axialplanes, and a TR of 2 s, TE 40 ms, flip angle 90. To facilitateanatomical localisation of activation, a high resolutioninversion recovery image dataset was also acquired, with3 mm contiguous slices and an in plane resolution of 3 mm(TR 1600 ms, TI 180 ms, TE 80 ms).
2.4.1.1. Image analysis. Functional MRI data were analyzedusing Statistical Parametric Mapping (SPM5; Wellcome De-partment of Cognitive Neurology, London, United Kingdom)

Fig. 1. Paired Associate Learning task. In an easy trial, two stimuli (highlydiscriminable coloured shapes) were shown either side (left and right) of acentral crosshair, followed by central crosshair alone, then the centralpresentation of one of the two original stimuli. Subjects had been trained tomove a joystick with their right hand in the direction of the locationoriginally occupied by the central stimulus. Intermediate and hard trialswere exactly the same except that four and eight stimuli were presentedaround the central crosshair, respectively. The speed and accuracy of thejoystick movements were recorded during scanning. In order to avoidhabituation of the subject, every stimulus had a randomly varied time ofpresentation, either between stimuli or before the presentation of the probe.
Table 1Longitudinal changes in the “at risk symptoms”.
Baseline Follow-up
Mean SD Mean SD t p
GAF 59.57 6.59 71.07 17.45 −2.307 0.029CAARMS perceptualdisorders
3.50 1.34 2.00 2.00 2.329 0.028
CAARMS thoughtdisorders
3.71 0.83 2.21 1.85 2.774 0.010
CAARMS speechdisorder
1.86 1.56 0.93 1.33 1.695 0.102
PANNS positive 10.14 3.75 13.14 7.84 −1.291 0.208PANSS negative 10.93 3.97 11.50 6.77 −0.272 0.787PANSS general 25.57 9.85 17.93 5.57 2.526 0.018PANSS total 46.57 12.09 42.86 15.29 0.713 0.482
47P. Fusar-Poli et al. / Schizophrenia Research 123 (2010) 45–52
running in MATLAB7.1. All volumes were realigned to thefirst volume, corrected for motion artifacts, mean adjusted byproportional scaling, normalized into standard stereotacticspace (template provided by the Montreal NeurologicalInstitute), and smoothed using a 6 mm full-width-at half-maximum Gaussian kernel. The time series were high passfiltered to eliminate low-frequency components (filter width128 s) and adjusted for systematic differences across trials. Inthefirst level analysis the onset times (in seconds) for each trialwas convolved with a canonical haemodynamic responsefunction. The analysis was restricted to images associatedwith correct responses. Each task condition (easy, intermediate,and hard) was then contrasted against the baseline condition(cross hair fixation) in each subject. To test the main effect ofthe cognitive load, main effect of the group, group by loadinteraction and the hypothesis that there were between groupdifferences in activation, we performed a second level analysisby using a full factorial model. To explore the longitudinalchanges in brain structure pairwise T-tests between the twoscans were employed. The whole brain voxel-wise thresholdwas set at pb .05, FWE corrected.
3. Results
3.1. Clinical and demographic characteristics of the sample
There were no significant differences between the ARMSand Control groups with respect to age (control mean=25.18 years SD=5.07, ARMS mean=24.36 years, SD=4.48;F=0.026, p=0.873), IQ (control mean=102.6 SD=9.2,ARMSmean=101.7 SD=12.3; F=1.733, p=0.204) or gender(ARMS females n=7, control females n=6, X2=1.502,
p=0.220). All controls and ARMS were right-handed. Only aminority of the ARMS and control subjects used illicitsubstances, and this was mainly occasional use of cannabis.There was no significant difference between the groupsin cannabis or alcohol use (pN0.05). The PANSS and CAARMSgeneral scores and the GAF scores at baseline and follow-upare shown in Table 1. After one year, the overall psychopath-ological and functional status of the ARMS sample hadsignificantly improved, despite 2 out of the 15 subjects havingdeveloped a full-blown psychosis. Thus, between presentationand follow-up, the CAARMS (perceptual disorder and thoughtdisorder subscales) and PANSS general scores decreased, whilethe GAF score increased (pb0.05) (Table 1). When the twosubjects who made transition to psychosis were excluded, asignificant longitudinal improvement was observed in someadditional psychopathological domains (PANSS positive, neg-ative, general, CAARMS speech disorders). No significantcorrelations between changes on the PANSS or changes onthe CAARMS and clinical interventions (antipsychotics/casemanagement) were observed (pN0.05).
3.2. Behavioural results
Repeated measures ANCOVA showed a main effect fortask difficulty with respect to accuracy (F=151.46, pb .001)and latency (F=419.93, pb .001). As the mnemonic loadincreased, response latency increased and response accura-cy decreased in an approximately linear fashion (Fig. 2). Nomain effect for group was observed with respect to accuracy(F=2.01 p=.181). Conversely, a main effect for group wasfound with respect to latency (F=7.798, p=.016). Post-hocanalysis revealed that, compared to controls, ARMS subjectsshowed higher latency in responses during the hardest levelof the task (t=2.529, p=.018). No significant group by taskload interactions were observed with respect to accuracy(F=.028, p=.972) or latency (F=.887, p=.439) (Fig 2).Over the follow-up period no significant changes in taskperformance were observed within the ARMS (pN0.05).
3.3. fMRI results
3.3.1. Cross sectional results
3.3.1.1. Main effect of task. Across all subjects and levels of taskdemand, the task was associated with activation in a wide
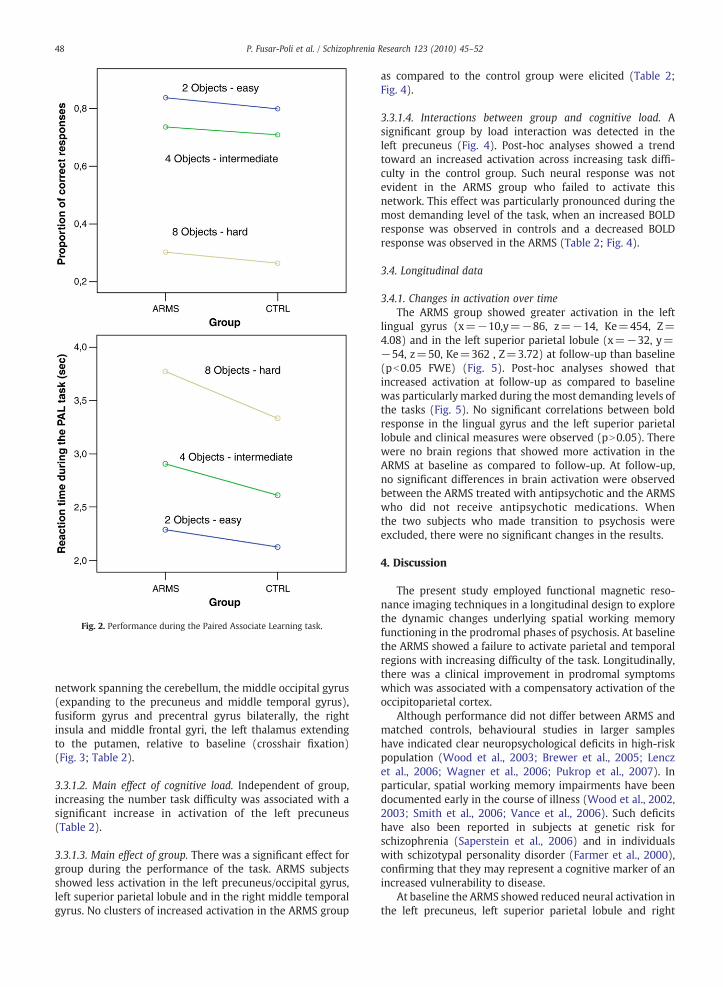
Fig. 2. Performance during the Paired Associate Learning task.
48 P. Fusar-Poli et al. / Schizophrenia Research 123 (2010) 45–52
network spanning the cerebellum, the middle occipital gyrus(expanding to the precuneus and middle temporal gyrus),fusiform gyrus and precentral gyrus bilaterally, the rightinsula and middle frontal gyri, the left thalamus extendingto the putamen, relative to baseline (crosshair fixation)(Fig. 3; Table 2).
3.3.1.2. Main effect of cognitive load. Independent of group,increasing the number task difficulty was associated with asignificant increase in activation of the left precuneus(Table 2).
3.3.1.3. Main effect of group. There was a significant effect forgroup during the performance of the task. ARMS subjectsshowed less activation in the left precuneus/occipital gyrus,left superior parietal lobule and in the right middle temporalgyrus. No clusters of increased activation in the ARMS group
as compared to the control group were elicited (Table 2;Fig. 4).
3.3.1.4. Interactions between group and cognitive load. Asignificant group by load interaction was detected in theleft precuneus (Fig. 4). Post-hoc analyses showed a trendtoward an increased activation across increasing task diffi-culty in the control group. Such neural response was notevident in the ARMS group who failed to activate thisnetwork. This effect was particularly pronounced during themost demanding level of the task, when an increased BOLDresponse was observed in controls and a decreased BOLDresponse was observed in the ARMS (Table 2; Fig. 4).
3.4. Longitudinal data
3.4.1. Changes in activation over timeThe ARMS group showed greater activation in the left
lingual gyrus (x=−10,y=−86, z=−14, Ke=454, Z=4.08) and in the left superior parietal lobule (x=−32, y=−54, z=50, Ke=362 , Z=3.72) at follow-up than baseline(pb0.05 FWE) (Fig. 5). Post-hoc analyses showed thatincreased activation at follow-up as compared to baselinewas particularly marked during the most demanding levels ofthe tasks (Fig. 5). No significant correlations between boldresponse in the lingual gyrus and the left superior parietallobule and clinical measures were observed (pN0.05). Therewere no brain regions that showed more activation in theARMS at baseline as compared to follow-up. At follow-up,no significant differences in brain activation were observedbetween the ARMS treated with antipsychotic and the ARMSwho did not receive antipsychotic medications. Whenthe two subjects who made transition to psychosis wereexcluded, there were no significant changes in the results.
4. Discussion
The present study employed functional magnetic reso-nance imaging techniques in a longitudinal design to explorethe dynamic changes underlying spatial working memoryfunctioning in the prodromal phases of psychosis. At baselinethe ARMS showed a failure to activate parietal and temporalregions with increasing difficulty of the task. Longitudinally,there was a clinical improvement in prodromal symptomswhich was associated with a compensatory activation of theoccipitoparietal cortex.
Although performance did not differ between ARMS andmatched controls, behavioural studies in larger sampleshave indicated clear neuropsychological deficits in high-riskpopulation (Wood et al., 2003; Brewer et al., 2005; Lenczet al., 2006; Wagner et al., 2006; Pukrop et al., 2007). Inparticular, spatial working memory impairments have beendocumented early in the course of illness (Wood et al., 2002,2003; Smith et al., 2006; Vance et al., 2006). Such deficitshave also been reported in subjects at genetic risk forschizophrenia (Saperstein et al., 2006) and in individualswith schizotypal personality disorder (Farmer et al., 2000),confirming that they may represent a cognitive marker of anincreased vulnerability to disease.
At baseline the ARMS showed reduced neural activation inthe left precuneus, left superior parietal lobule and right
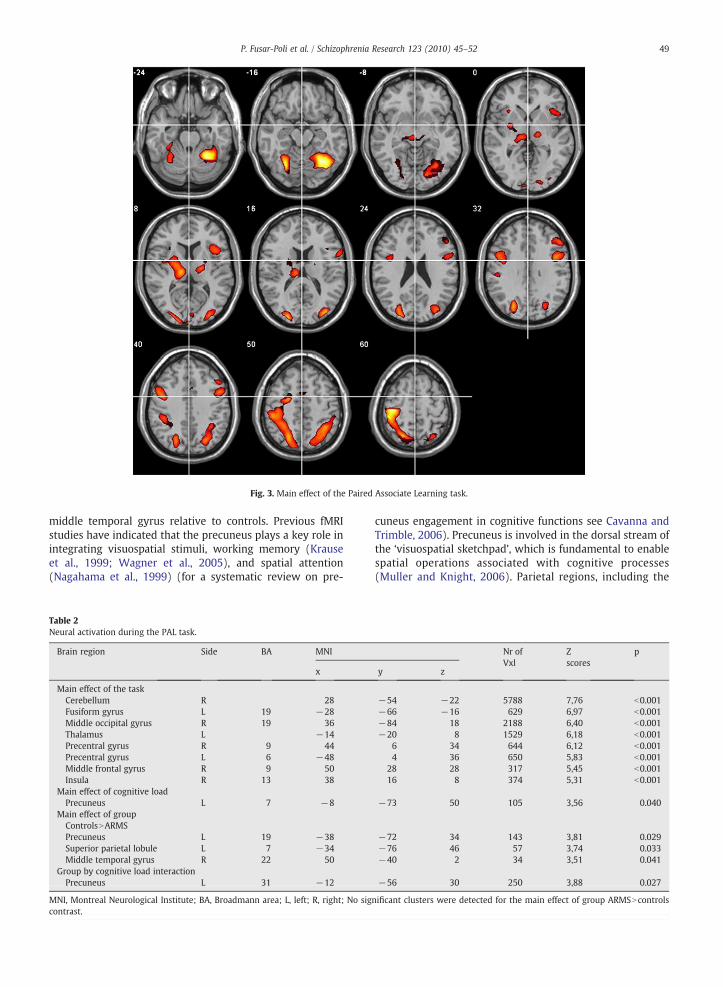
Fig. 3. Main effect of the Paired Associate Learning task.
49P. Fusar-Poli et al. / Schizophrenia Research 123 (2010) 45–52
middle temporal gyrus relative to controls. Previous fMRIstudies have indicated that the precuneus plays a key role inintegrating visuospatial stimuli, working memory (Krauseet al., 1999; Wagner et al., 2005), and spatial attention(Nagahama et al., 1999) (for a systematic review on pre-
Table 2Neural activation during the PAL task.
Brain region Side BA MNI
x
Main effect of the taskCerebellum R 28Fusiform gyrus L 19 −28Middle occipital gyrus R 19 36Thalamus L −14Precentral gyrus R 9 44Precentral gyrus L 6 −48Middle frontal gyrus R 9 50Insula R 13 38
Main effect of cognitive loadPrecuneus L 7 −8
Main effect of groupControlsNARMSPrecuneus L 19 −38Superior parietal lobule L 7 −34Middle temporal gyrus R 22 50
Group by cognitive load interactionPrecuneus L 31 −12
MNI, Montreal Neurological Institute; BA, Broadmann area; L, left; R, right; No sigcontrast.
cuneus engagement in cognitive functions see Cavanna andTrimble, 2006). Precuneus is involved in the dorsal stream ofthe ‘visuospatial sketchpad’, which is fundamental to enablespatial operations associated with cognitive processes(Muller and Knight, 2006). Parietal regions, including the
Nr ofVxl
Zscores
p
y z
−54 −22 5788 7,76 b0.001−66 −16 629 6,97 b0.001−84 18 2188 6,40 b0.001−20 8 1529 6,18 b0.001
6 34 644 6,12 b0.0014 36 650 5,83 b0.001
28 28 317 5,45 b0.00116 8 374 5,31 b0.001
−73 50 105 3,56 0.040
−72 34 143 3,81 0.029−76 46 57 3,74 0.033−40 2 34 3,51 0.041
−56 30 250 3,88 0.027
nificant clusters were detected for the main effect of group ARMSNcontrols
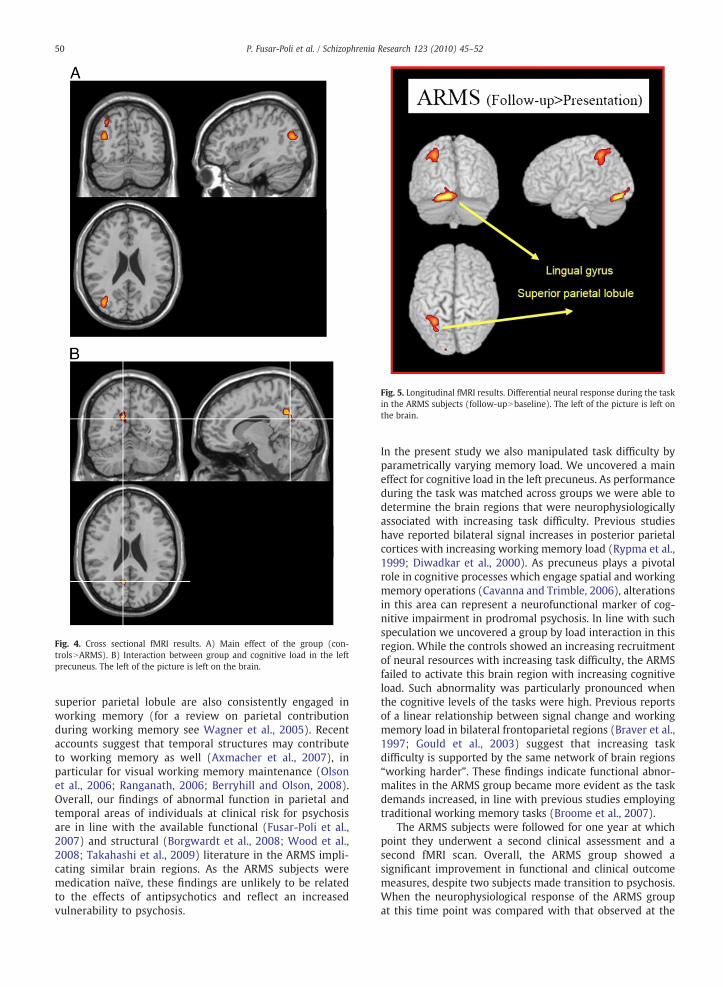
Fig. 4. Cross sectional fMRI results. A) Main effect of the group (con-trolsNARMS). B) Interaction between group and cognitive load in the lefprecuneus. The left of the picture is left on the brain.
Fig. 5. Longitudinal fMRI results. Differential neural response during the taskin the ARMS subjects (follow-upNbaseline). The left of the picture is left onthe brain.
50 P. Fusar-Poli et al. / Schizophrenia Research 123 (2010) 45–52
t
superior parietal lobule are also consistently engaged inworking memory (for a review on parietal contributionduring working memory see Wagner et al., 2005). Recentaccounts suggest that temporal structures may contributeto working memory as well (Axmacher et al., 2007), inparticular for visual working memory maintenance (Olsonet al., 2006; Ranganath, 2006; Berryhill and Olson, 2008).Overall, our findings of abnormal function in parietal andtemporal areas of individuals at clinical risk for psychosisare in line with the available functional (Fusar-Poli et al.,2007) and structural (Borgwardt et al., 2008; Wood et al.,2008; Takahashi et al., 2009) literature in the ARMS impli-cating similar brain regions. As the ARMS subjects weremedication naïve, these findings are unlikely to be relatedto the effects of antipsychotics and reflect an increasedvulnerability to psychosis.
In the present study we also manipulated task difficulty byparametrically varying memory load. We uncovered a maineffect for cognitive load in the left precuneus. As performanceduring the task was matched across groups we were able todetermine the brain regions that were neurophysiologicallyassociated with increasing task difficulty. Previous studieshave reported bilateral signal increases in posterior parietalcortices with increasing working memory load (Rypma et al.,1999; Diwadkar et al., 2000). As precuneus plays a pivotalrole in cognitive processes which engage spatial and workingmemory operations (Cavanna and Trimble, 2006), alterationsin this area can represent a neurofunctional marker of cog-nitive impairment in prodromal psychosis. In line with suchspeculation we uncovered a group by load interaction in thisregion. While the controls showed an increasing recruitmentof neural resources with increasing task difficulty, the ARMSfailed to activate this brain region with increasing cognitiveload. Such abnormality was particularly pronounced whenthe cognitive levels of the tasks were high. Previous reportsof a linear relationship between signal change and workingmemory load in bilateral frontoparietal regions (Braver et al.,1997; Gould et al., 2003) suggest that increasing taskdifficulty is supported by the same network of brain regions“working harder”. These findings indicate functional abnor-malites in the ARMS group became more evident as the taskdemands increased, in line with previous studies employingtraditional working memory tasks (Broome et al., 2007).
The ARMS subjects were followed for one year at whichpoint they underwent a second clinical assessment and asecond fMRI scan. Overall, the ARMS group showed asignificant improvement in functional and clinical outcomemeasures, despite two subjects made transition to psychosis.When the neurophysiological response of the ARMS groupat this time point was compared with that observed at the

51P. Fusar-Poli et al. / Schizophrenia Research 123 (2010) 45–52
baseline, we found relatively increased activation in theleft lingual gyrus and in the left superior parietal lobule.Engagement of posterior parietal and occipital cortices hasbeen consistently reported in visuospatial working memorytasks (Belger et al., 1998). In particular, activation in theoccipitotemporal (ventral visual) pathway was related toobject working memory while activation in the occipitopar-ietal (dorsal visual) pathway was related to spatial workingmemory (Muller and Knight, 2006). Other authors haveconfirmed that occipitoparietal areas play a crucial role inlinking an object to a certain spatial location (Sommer et al.,2005). In terms of cognitive function, activations in parietalregions are usually attributed to information storage pro-cesses in working memory or to processes of spatial per-ception, computation and attention (Gould et al., 2003).Activity in the occipital cortex, though common in workingmemory tasks, has also been related to processes ofvisuospatial perception or recognition (Gould et al., 2003).Consequently, the increased occipitoparietal activation maybe interpreted to represent a compensatory cortical responseto the neurofunctional deficits observed at baseline.
Limitations of the study are well acknowledged. Althoughwe uncovered no significant correlations with antipsychotictreatment or case management, the sample was too small topermit a powerful analysis of the potential impact of anyspecific clinical measure. Similarly, although two of the ARMSgroup went on to develop a first episode of frank psychosis,the small sample size precluded comparisons between thefunctional findings in these subjects and the remainder whodid not. The extent to which the present findings vary withinthe ARMS group with clinical outcome and with clinicalinterventionwill require further studies in larger samples andthe randomization of subjects according to the form of clinicalintervention.
5. Conclusion
The prodromal phase of psychosis is associated withfunctional alterations in parietal and temporal networkssubserving visuospatial working memory which are moreevident with high cognitive loads. The clinical improvementat one year is associated with a compensatory increase inparietal regions.
Role of funding sourceThe sponsor had no role in designing or implementing the study.
ContributorsPaolo Fusar-Poli collected the data, wrote the draft of themanuscript and
conducted data analysis. Matthew Broome, Pall Matthiasson, James Woolley,Paul Tabraham, Louise Johns, Lucia Valmaggia collected the data andcontributed to their interpretation. Elvira Bramon, Steve Willams and PhilipMcGuire supervised statistical analysis and interpretation of results andassisted with the draft of the manuscript.
Conflict of interestThe authors have no disclosures to report.
AcknowledgementsNone.
References
Axmacher, N., Mormann, F., Fernandez, G., Cohen, M.X., Elger, C.E., Fell, J.,2007. Sustained neural activity patterns during working memory in thehuman medial temporal lobe. J. Neurosci. 27 (29), 7807–7816.
Barkus, E.J., Stirling, J., Hopkins, R.S., Lewis, S., 2006. Cannabis-inducedpsychosis-like experiences are associated with high schizotypy. Psycho-pathology 39 (4), 175–178.
Belger, A., Puce, A., Krystal, J.H., Gore, J.C., Goldman-Rakic, P., McCarthy, G.,1998. Dissociation of mnemonic and perceptual processes during spatialand nonspatial working memory using fMRI. Hum. Brain Mapp. 6 (1),14–32.
Berryhill, M.E., Olson, I.R., 2008. The right parietal lobe is critical for visualworking memory. Neuropsychologia 46 (7), 1767–1774.
Borgwardt, S.J., McGuire, P.K., Aston, J., Gschwandtner, U., Pfluger, M.O.,Stieglitz, R.D., Radue, E.W., Riecher-Rossler, A., 2008. Reductions infrontal, temporal and parietal volume associated with the onset ofpsychosis. Schizophr. Res. 106 (2–3), 108–114.
Braver, T.S., Cohen, J.D., Nystrom, L.E., Jonides, J., Smith, E.E., Noll, D.C., 1997. Aparametric study of prefrontal cortex involvement in human workingmemory. Neuroimage 5 (1), 49–62.
Brewer, W.J., Francey, S.M., Wood, S.J., Jackson, H.J., Pantelis, C., Phillips, L.J.,Yung, A.R., Anderson, V.A., McGorry, P.D., 2005. Memory impairmentsidentified in people at ultra-high risk for psychosis who later developfirst-episode psychosis. Am. J. Psychiatry 162 (1), 71–78.
Broome, M., Woolley, J., Tabraham, P., Johns, L., Bramon, E., Murray, G.,Pariante, C., McGuire, P.K., Murray, R., 2005. What causes the onset ofpsychosis? Schizophr. Res. 79 (1), 23–34.
Broome, M.R., Johns, L.C., Valli, I., Woolley, J.B., Tabraham, P., Brett, C.,Valmaggia, L., Peters, E., Garety, P.A., McGuire, P.K., 2007. Delusionformation and reasoning biases in those at clinical high risk forpsychosis. Br. J. Psychiatry 191, s38–s42.
Cannon, T.D., Cornblatt, B., McGorry, P., 2007. The empirical status of the ultrahigh-risk (prodromal) research paradigm. Schizophr. Bull. 33 (3),661–664.
Cavanna, A.E., Trimble, M.R., 2006. The precuneus: a review of its functionalanatomy and behavioural correlates. Brain 129 (Pt 3), 564–583.
Coren, S., 1993. Measurement of handedness via self-report: the relationshipbetween brief and extended inventories. Percept. Mot. Skills 76 (3 Pt 1),1035–1042.
Diwadkar, V.A., Carpenter, P.A., Just, M.A., 2000. Collaborative activitybetween parietal and dorso-lateral prefrontal cortex in dynamic spatialworking memory revealed by fMRI. Neuroimage 12 (1), 85–99.
Eastvold, A.D., Heaton, R.K., Cadenhead, K.S., 2007. Neurocognitive deficitsin the (putative) prodrome and first episode of psychosis. Schizophr. Res.93 (1–3), 266–277.
Farmer, C.M., O'Donnell, B.F., Niznikiewicz, M.A., Voglmaier, M.M., McCarley,R.W., Shenton, M.E., 2000. Visual perception and working memory inschizotypal personality disorder. Am. J. Psychiatry 157 (5), 781–788.
Fusar-Poli, P., Perez, J., Broome, M., Borgwardt, S., Placentino, A., Caverzasi, E.,Cortesi, M., Veggiotti, P., Politi, P., Barale, F., McGuire, P., 2007.Neurofunctional correlates of vulnerability to psychosis: a systematicreview and meta-analysis. Neurosci. Biobehav. Rev. 31 (4), 465–484.
Gould, R.L., Brown, R.G., Owen, A.M., ffytche, D.H., Howard, R.J., 2003. fMRIBOLD response to increasing task difficulty during successful pairedassociates learning. Neuroimage 20 (2), 1006–1019.
Kay, S.R., 1990. Positive–negative symptom assessment in schizophrenia:psychometric issues and scale comparison. Psychiatr. Q. 61 (3), 163–178.
Krause, B.J., Schmidt, D., Mottaghy, F.M., Taylor, J., Halsband, U., Herzog, H.,Tellmann, L., Muller-Gartner, H.W., 1999. Episodic retrieval activates theprecuneus irrespective of the imagery content of word pair associates. APET study. Brain 122 (Pt 2), 255–263.
Lencz, T., Smith, C.W., McLaughlin, D., Auther, A., Nakayama, E., Hovey, L.,Cornblatt, B.A., 2006. Generalized and specific neurocognitive deficits inprodromal schizophrenia. Biol. Psychiatry 59 (9), 863–871.
Muller, N.G., Knight, R.T., 2006. The functional neuroanatomy of workingmemory: contributions of human brain lesion studies. Neuroscience 139(1), 51–58.
Nagahama, Y., Okada, T., Katsumi, Y., Hayashi, T., Yamauchi, H., Sawamoto, N.,Toma, K., Nakamura, K., Hanakawa, T., Konishi, J., Fukuyama, H.,Shibasaki, H., 1999. Transient neural activity in the medial superiorfrontal gyrus and precuneus time locked with attention shift betweenobject features. Neuroimage 10 (2), 193–199.
Nelson, H.E., Willison, J.R., 1991. National Adult Reading Test (NART): TestManual2nd ed. NFER-Nelson, Windsor, England.
Nieman, D., Becker, H., van de Fliert, R., Plat, N., Bour, L., Koelman, H.,Klaassen, M., Dingemans, P., Niessen, M., Linszen, D., 2007. Antisaccadetask performance in patients at ultra high risk for developing psychosis.Schizophr. Res. 95 (1–3), 54–60.

52 P. Fusar-Poli et al. / Schizophrenia Research 123 (2010) 45–52
Olson, I.R., Moore, K.S., Stark, M., Chatterjee, A., 2006. Visual workingmemory is impaired when the medial temporal lobe is damaged. J. Cogn.Neurosci. 18 (7), 1087–1097.
Pflueger, M.O., Gschwandtner, U., Stieglitz, R.D., Riecher-Rossler, A., 2007.Neuropsychological deficits in individuals with an at riskmental state forpsychosis—working memory as a potential trait marker. Schizophr. Res.97 (1–3), 14–24.
Pukrop, R., Ruhrmann, S., Schultze-Lutter, F., Bechdolf, A., Brockhaus-Dumke,A., Klosterkotter, J., 2007. Neurocognitive indicators for a conversion topsychosis: comparison of patients in a potentially initial prodromal statewho did or did not convert to a psychosis. Schizophr. Res. 92 (1–3),116–125.
Ranganath, C., 2006. Working memory for visual objects: complementaryroles of inferior temporal, medial temporal, and prefrontal cortex.Neuroscience 139 (1), 277–289.
Repovs, G., Baddeley, A., 2006. The multi-component model of workingmemory: explorations in experimental cognitive psychology. Neurosci-ence 139 (1), 5–21.
Rypma, B., Prabhakaran, V., Desmond, J.E., Glover, G.H., Gabrieli, J.D., 1999.Load-dependent roles of frontal brain regions in the maintenance ofworking memory. Neuroimage 9 (2), 216–226.
Saperstein, A.M., Fuller, R.L., Avila, M.T., Adami, H., McMahon, R.P., Thaker, G.K.,Gold, J.M., 2006. Spatial working memory as a cognitive endophenotypeof schizophrenia: assessing risk for pathophysiological dysfunction.Schizophr. Bull. 32 (3), 498–506.
Smith, C.W., Park, S., Cornblatt, B., 2006. Spatial working memory deficitsin adolescents at clinical high risk for schizophrenia. Schizophr. Res. 81(2–3), 211–215.
Sommer, T., Rose, M., Weiller, C., Buchel, C., 2005. Contributions of occipital,parietal and parahippocampal cortex to encoding of object–locationassociations. Neuropsychologia 43 (5), 732–743.
Takahashi, T., Wood, S.J., Yung, A.R., Soulsby, B., McGorry, P.D., Suzuki, M.,Kawasaki, Y., Phillips, L.J., Velakoulis, D., Pantelis, C., 2009. Progressive
graymatter reduction of the superior temporal gyrus during transition topsychosis. Arch. Gen. Psychiatry 66 (4), 366–376.
Vance, A., Hall, N., Bellgrove, M.A., Casey, M., Karsz, F., Maruff, P., 2006.Visuospatial workingmemory deficits in adolescent onset schizophrenia.Schizophr. Res.
Wagner, A.D., Shannon, B.J., Kahn, I., Buckner, R.L., 2005. Parietal lobecontributions to episodic memory retrieval. Trends Cogn. Sci. 9 (9),445–453.
Wagner, M., Frommann, I., Jessen, F., Pukrop, R., Bechdolf, A., Ruhrmann, S.,Klosterkotter, J., Brinkmeyer, J., Woelwer, W., Decker, P., Maier, W., 2006.Cognitive and neurolobiological risk indicators in early and lateprodromal stages. Schizophr. Res. 86 (Supplement), S35–S36.
Wood, S.J., Proffitt, T., Mahony, K., Smith, D.J., Buchanan, J.A., Brewer, W.,Stuart, G.W., Velakoulis, D., McGorry, P.D., Pantelis, C., 2002. Visuospatialmemory and learning in first-episode schizophreniform psychosis andestablished schizophrenia: a functional correlate of hippocampalpathology? Psychol. Med. 32 (3), 429–438.
Wood, S.J., Pantelis, C., Proffitt, T., Phillips, L.J., Stuart, G.W., Buchanan, J.A.,Mahony, K., Brewer, W., Smith, D.J., McGorry, P.D., 2003. Spatial workingmemory ability is a marker of risk-for-psychosis. Psychol. Med. 33 (7),1239–1247.
Wood, S.J., Pantelis, C., Velakoulis, D., Yucel, M., Fornito, A., McGorry, P.D.,2008. Progressive changes in the development toward schizophrenia:studies in subjects at increased symptomatic risk. Schizophr. Bull. 34 (2),322–329.
Yung, A.R., Phillips, L.J., McGorry, P.D., McFarlane, C.A., Francey, S., Harrigan, S.,Patton, G.C., Jackson, H.J., 1998. Prediction of psychosis—a step towardsindicated prevention of schizophrenia. Br. J. Psychiatry 172, 14–20.
Yung, A.R., Yuen, H.P., McGorry, P.D., Phillips, L.J., Kelly, D., Dell'Olio, M.,Francey, S.M., Cosgrave, E.M., Killackey, E., Stanford, C., Godfrey, K.,Buckby, J., 2005. Mapping the onset of psychosis: the ComprehensiveAssessment of At-Risk Mental States. Aust. N. Z. J. Psychiatry 39 (11–12),964–971.