souvenir - iscasouvenir of cme workshop on autoimmunity & autoimmune diseases (10 th & 11th...
TRANSCRIPT
SOUVENIR of
CME Workshop on
Autoimmunity & Autoimmune Diseases
(10th & 11th April, 2015)
Edited by
Dr. Gyanendra Awasthi
Reader and Head, Department of Biochemistry
Dolphin (PG) Institute of Bio medical & Natural Sciences, Dehradun
Organized by
Department of Biochemistry & pathology
Dolphin (PG) Institute of Biomedical & Natural Sciences, Dehradun
in collaboration with
Indian Immunology society
New Delhi, India
2016
International E - Publication www.isca.me , www.isca.co.in
International E - Publication 427, Palhar Nagar, RAPTC, VIP-Road, Indore-452005 (MP) INDIA
Phone: +91-731-2616100, Mobile: +91-80570-83382
E-mail: [email protected] , Website: www.isca.me , www.isca.co.in
© Copyright Reserved
2016
All rights reserved. No part of this publication may be reproduced, stored, in
a retrieval system or transmitted, in any form or by any means, electronic,
mechanical, photocopying, reordering or otherwise, without the prior
permission of the publisher.
ISBN: 978-93-84659-48-6
CME Workshop
on
Autoimmunity & Autoimmune Diseases
(10th
& 11th April, 2015)
Organized by
DEPARTMENT OF BIOCHEMISTRY
&
DEPARTMENT OF PATHOLOGY
DOLPHIN (PG) INSTITUTE OF BIOMEDICAL &
NATURAL SCIENCES DEHRA DUN
(UTTARAKHAND), INDIA
In Collaboration With
INDIAN IMMUNOLOGY SOCIETY
NEW DELHI, INDIA
CME Workshop on Autoimmunity & Autoimmune Diseases
(10th & 11th April 2015)
PATRONS
Shri Ramesh Garg Shri Arvind Gupta
President Chairman
Dolphin Educational Society of India Dolphin (PG) Institute of Biomedical &
New Delhi Natural Sciences, Dehra Dun
Dr. Vinod Mittal
Secretary & Director Academics
Dolphin Educational Society of India, New Delhi
ADVISORY COMMITTEE
Chairman
Dr. D.N. Rao
Professor & Head, Department of Biochemistry
All India Institute of Medical Sciences (AIIMS), New Delhi
Dr. Seema K. Avtar
Director
Synergy Institute of Medical Sciences
Dehradun
Dr. R.K. Singh
Professor & Gead
Department of Biochemistry
SGRR Medical College & Hospital,
Dehra Dun
Dr. Vineet Malhotra
Professor
Department of Biochemistry
HIHT University, Dehra Dun
Dr. Alpana Sharma
Addi. Professor
Department of Biochemistry
AIIMS, New Delhi
Dr. Nibhriti Das
Secretary, Indian Immunology Society
AIIMS, New Delhi
Dr. Abbas Ahmed Mehdi
Professor & Head
Department of Biochemistry
KGMU, Lucknow
CME Workshop on Autoimmunity & Autoimmune Diseases
(10th & 11th April 2015)
ORGANIZING COMMITTEE
Dolphin (PG) Institute of Biomedical & Natural Sciences
Dehra Dun
Convener
Dr. Shailja Pant
Principal
Co-Convener
Dr. Arun Kumàr
Director
Organizing Secretary
Dr. Gyanendra Awasthi
Reader and Head, Department of Biochemistry
Co-Organizing Secretary
Mr. Aditya Swamp
Lecturer, Department of Pathology
Joint Organizing Secretaries
Dr. Santosh Kumar
Lecturer, Department of Biochemistry
Dr. Ashwini Sanghi
Lecturer
Department of Biochemistry
Dr. Shiv Saran Singh
Lecturer
Department of Biochemistry
Mrs. Rashmi Chauhan
Lecturer
Department of Pathology
Mr. Ankit John
Lecturer
Department of Pathology
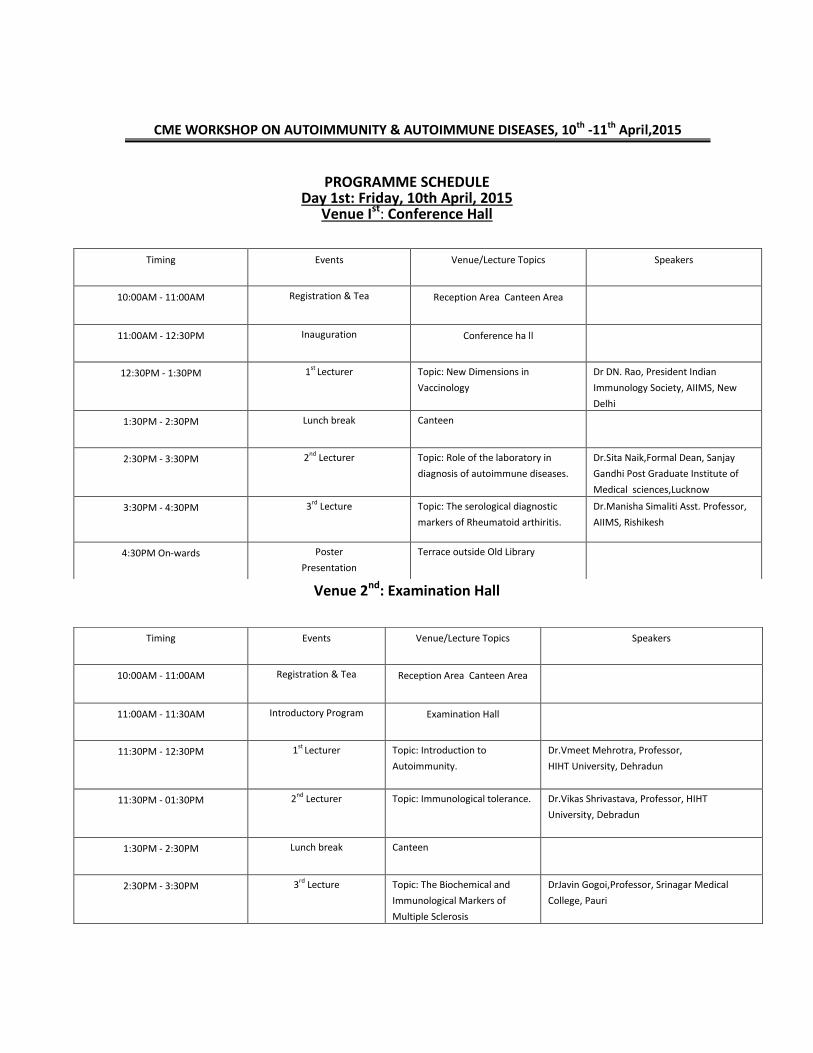
PROGRAMME SCHEDULE Day 1st: Friday, 10th April, 2015
Venue Ist: Conference Hall
Venue 2nd: Examination Hall
Timing Events Venue/Lecture Topics Speakers
10:00AM - 11:00AM Registration & Tea Reception Area Canteen Area
11:00AM - 12:30PM Inauguration Conference ha ll
12:30PM - 1:30PM 1st Lecturer Topic: New Dimensions in
Vaccinology
Dr DN. Rao, President Indian
Immunology Society, AIIMS, New
Delhi
1:30PM - 2:30PM Lunch break Canteen
2:30PM - 3:30PM 2nd Lecturer Topic: Role of the laboratory in
diagnosis of autoimmune diseases.
Dr.Sita Naik,Formal Dean, Sanjay
Gandhi Post Graduate Institute of
Medical sciences,Lucknow
3:30PM - 4:30PM 3rd Lecture Topic: The serological diagnostic
markers of Rheumatoid arthiritis.
Dr.Manisha Simaliti Asst. Professor,
AIIMS, Rishikesh
4:30PM On-wards Poster
Presentation
Terrace outside Old Library
Timing Events Venue/Lecture Topics Speakers
10:00AM - 11:00AM Registration & Tea Reception Area Canteen Area
11:00AM - 11:30AM Introductory Program Examination Hall
11:30PM - 12:30PM 1st Lecturer Topic: Introduction to
Autoimmunity.
Dr.Vmeet Mehrotra, Professor,
HIHT University, Dehradun
11:30PM - 01:30PM 2nd Lecturer Topic: Immunological tolerance.
Dr.Vikas Shrivastava, Professor, HIHT
University, Debradun
1:30PM - 2:30PM Lunch break Canteen
2:30PM - 3:30PM 3rd Lecture Topic: The Biochemical and
Immunological Markers of
Multiple Sclerosis
DrJavin Gogoi,Professor, Srinagar Medical
College, Pauri
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
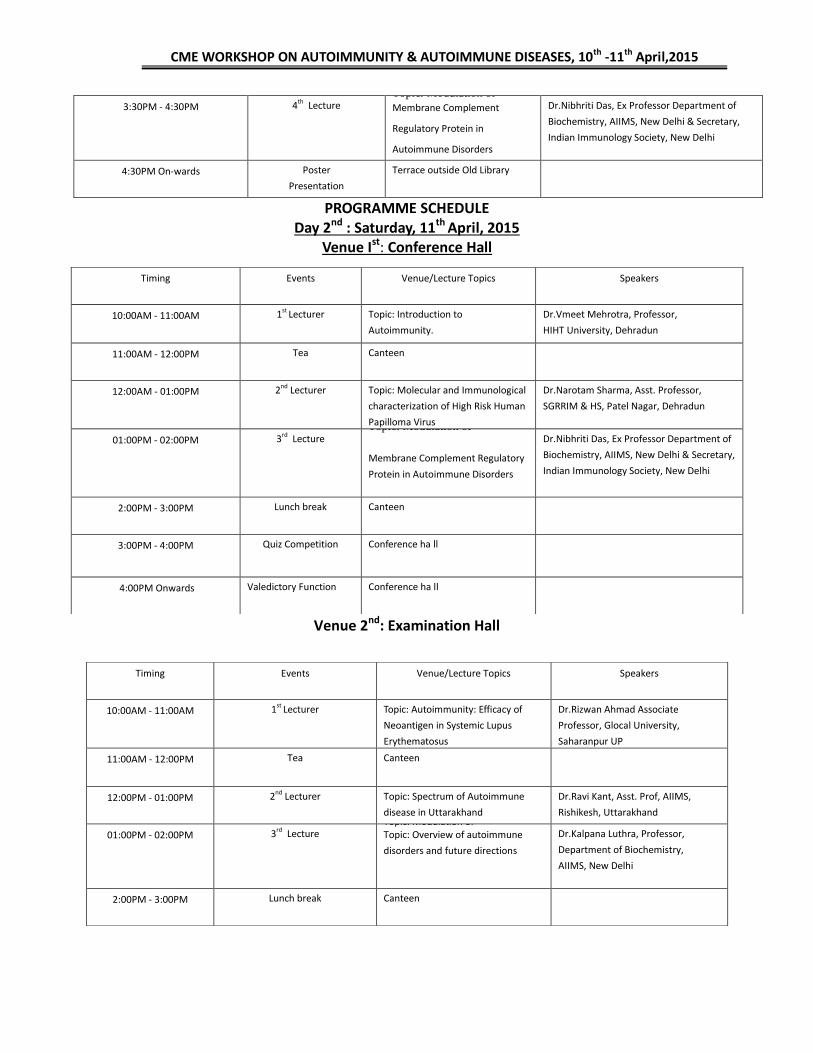
PROGRAMME SCHEDULE Day 2nd : Saturday, 11th April, 2015
Venue Ist: Conference Hall
Venue 2nd: Examination Hall
3:30PM - 4:30PM 4th Lecture Topic: Modulation of Membrane Complement
Regulatory Protein in
Autoimmune Disorders
Dr.Nibhriti Das, Ex Professor Department of
Biochemistry, AIIMS, New Delhi & Secretary,
Indian Immunology Society, New Delhi
4:30PM On-wards Poster
Presentation
Terrace outside Old Library
Timing Events Venue/Lecture Topics Speakers
10:00AM - 11:00AM 1st Lecturer Topic: Introduction to
Autoimmunity.
Dr.Vmeet Mehrotra, Professor,
HIHT University, Dehradun
11:00AM - 12:00PM Tea Canteen
12:00AM - 01:00PM 2nd Lecturer Topic: Molecular and Immunological
characterization of High Risk Human
Papilloma Virus
Dr.Narotam Sharma, Asst. Professor,
SGRRIM & HS, Patel Nagar, Dehradun
01:00PM - 02:00PM 3rd Lecture Topic: Modulation of
Membrane Complement Regulatory
Protein in Autoimmune Disorders
Dr.Nibhriti Das, Ex Professor Department of
Biochemistry, AIIMS, New Delhi & Secretary,
Indian Immunology Society, New Delhi
2:00PM - 3:00PM Lunch break Canteen
3:00PM - 4:00PM Quiz Competition Conference ha ll
4:00PM Onwards Valedictory Function Conference ha ll
Timing Events Venue/Lecture Topics Speakers
10:00AM - 11:00AM 1st Lecturer Topic: Autoimmunity: Efficacy of
Neoantigen in Systemic Lupus
Erythematosus
Dr.Rizwan Ahmad Associate
Professor, Glocal University,
Saharanpur UP
11:00AM - 12:00PM Tea Canteen
12:00PM - 01:00PM 2nd Lecturer Topic: Spectrum of Autoimmune
disease in Uttarakhand
Dr.Ravi Kant, Asst. Prof, AIIMS,
Rishikesh, Uttarakhand
01:00PM - 02:00PM 3rd Lecture Topic: Modulation of Topic: Overview of autoimmune
disorders and future directions
Dr.Kalpana Luthra, Professor,
Department of Biochemistry,
AIIMS, New Delhi
2:00PM - 3:00PM Lunch break Canteen
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
TABLE OF CONTENTS
SECTION —A (Guest speakers)
1.
Multiple Antigenic Peptides (MAP) Based on B and T Cell Epitopes of E2 Glycoprotein of Chikungunya Virus Showed Enhanced Immunogenicity and Induced Neutralizing Antibodies in Mice
Dr D.N.Rao 02
2. Role of the Laboratory in Diagnosis of Autoimmune Diseases
Dr. Sita Naik 03
3. The Serological Diagnosis of Rheumatoid Arthritis Dr.Manisha Simaliti 04 4. Autoimmunity Dr.Vineet Mehrotra 05- - 11 5. Immune system: How Not to Kill Your Own Kind Dr Vikas Shrivastava 12
6. The Biochemical & Immunological Markers of Multiple Sclerosis
Dr.Javin Gogoi 12
7. Modulation of Membrane Complement Regulatory Protein in Autoimmune Disorders
Dr.Nibhriti Das 13 — 14
8. Molecular & Immunological characterization of High Risk Human Papilloma Virus
Dr. Narotam Sharma 15
9. Spectrum of Autoimmune Disease in Uttarakhand Dr.Ravi Kant 15
10. Overview of Autoimmune Disorders & Future Directions
Dr.Kalpana Luthra 16
3:00PM - 4:00PM Quiz Competition Conference ha ll
4:00PM Onwards Valedictory Function Conference ha ll
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by:DIBNS,Dehradun & Indian Immunology Society,New Delhi
SECTION —B (Presentations)
S.No Topic Name of Author Page No.
1. Autoimmune Diseases Tyagi, Manjusha & Juyal, Preeti 18 - 20 2. Autoimmunity & Liver G.Awasthi & Aditya Swarup 21 3. Autoimmune Hepatitis Ashwani Sanghi 22 4. Hashimoto’s Thyroiditis Ankit Johari 23 5. Multiple Sclerosis Aditya Swamp 24 6. Myasthenia Gravis Aditya Swamp 25 7. Rheumatoid arthritis Rashmi Chouhan 26 8.
Autoimmune Disorders During Pregnancy G.Awasthi, Shiv Sharan Singh & Aditya Swarup
27 -28
9. Auto-Antibodies in Heart Diseases G.Awasthi & Aditya swamp 29
10. Advanced Glycation End Products (AGEs) Lokendra Kumar & Zafar asheed 30
11. MWCNT/Gold Nanoparticle Based Genosensor for Early Detection of Rheumatic Heart Disease
Ankur Kaushal, Dinesh Kumar, Deepak Kala, Shashi Khare & Ashok Kumar
31
12. Antibiotic Induced Alterations in the Commensal Microbiome
Prabhanshu Tripathi, & rew Stefka, Taylor Feehley, Tiffany Patton, Eugene Chang, Dionysios Antonopoulos, Zhiheng Pei & Cathryn Nagler
32
13. Electrochemical Detection of Cellac Disease Related Anti-Glia
upta Ankur Kaushal, Rupak Na ala & Dinesh Kumar
33
14. Increased Production of Autofñtibodies in Physically Active Older Individuals After Vaccination
Shiv Sharan Smgh 34
15. Diagnosis of Autoimmune Diseases Santosh Kumar 35 - 36
16.
Diseases & Role of Biomarkers
Santosh Kumar 37 - 38
17. Prevention of Autoimmune Diseases Santosh Kumar 39
18. Vaccines to Autoimmune Disorders: Safe or Harmful
Ashwani Sanghi 40
19. Treatment of Autoimmune Diseases Santosh Kumar 41 - 42 20. Advances in the Treatment of Myasthenia Gravis Rashmi Chouhan 43
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
1
SECTION -A
(Guest speakers)

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
2
Multiple Antigenic Peptides (MAP) Based on B and T Cell Epitopes of E2 Glycoprotein of Chikungunya Virus Showed Enhanced Immunogenicity
and Induced Neutralizing Antibodies in Mice
D.N. Rao, Dept. of Biochemistry, AIIMS, New Delhi (India)
Chikungunya is a viral disease caused by positive sense single stranded RNA virus. This virus transmitted to human by Aedes misquotes. High fever, myaligia, Joint swelling, body rashes are characteristic features of Chikungunya. Earlier studied demonstrated that dominant epitopes of envelope E2 protein can be used for diagnostic/vaccine design. In the present study we constructed Multiple Antigenic Peptide (MAP) based on in house established immunodominant B and T cell epitopes of E2 protein. Three MAPs (MAP-i, MAP-2, MAP-3) were constructed on lysine back bone and characterized by SDS-PAGE, immunoblot and immunoreactivity with E2 antisera. Humoral and cell mediated responses were studied in outbred and inbred mice. Mice were immunized intramuscularly with different formulations with/lwithout adjuvants (CpG ODN and Murabitide) in microspheres. MAP in microspheres with CpG ODN showed highest IgG peak titer (3,00,000) with IgG subclass mostly IgG2a/2b distribution compared to other formulations. Individual epitopes of MAPs showed immunoreactivity with MAPs antisera and a few epitopes showed dominance. In T cell mediated response, all the MAPs showed high stimulated index. Cytokine profile showed significant higher levels of mostly TH-l & TH17 vis IL-lβ, 1L2, IL-12, IL-17, TNF -α. All the MAP antibodies involved in virus neutralization. This is an alternative approach for vaccine design for Chikungunya.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
3
Role of the Laboratory in Diagnosis of Autoimmune Diseases
Sita Naik, Retired Professor and Head, Department of Immunology, SGPGIMS,
Lucknow and Advisor, Apollo Hospitals Education &Research Foundation (AHERF)
Few ares of medicine are so crucially dependent on laboratory diagnosis as the autoimmune
diseases. These diseases fall into two major groups, organ specific and systemic.
The organ specific autoimmune diseases predominantly affect organs of the endocrine systems
and various blood elements, but can also be the cause of infertility, renal disease and a host of
other conditions. . Diabetes, thyroid diseases and hemolytic anemia would be examples of this
group. The pathogenesis of these conditions is reasonably well established and diagnosis is
crucially dependent on the demonstration of the specific antibody.
The systemic autoimmune diseases on the other hand have complex multi-factorial etiologies,
which may not be directly linked to the detectable antibodies. Rheumatoid arthritis, systemic
lupus erythematosus (SLE) and Wegenr’s granulomatosus would be examples of this group.
The pattern of antibodies provides important diagnostic support and sometimes provides leads
to the diagnosis. In many instances the antibody titers also are useful markers for treatment
response and follow up. They form an essential part of the management of these conditions.
Historically, the earliest tests for autoantibodies was the LE test for SLE and Rose-Waaler test for
Rheumatoid arthritis. We have come a long way from that to the present third generation ELISA
tests which use recombinant proteins as antigens. This has made the tests more widely available
and results more standardized. However, their interpretation can be difficult in the absence of
the appropriate clinical support.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
4
The Serological Diagnosis of Rheumatoid Arthritis
Dr. Manisha Naithani, M.D. Assistant professor, Department of Biochemistry, All
India Institute of Medical Sciences, Rishikesh, Uttarakhand
Rheumatoid arthritis (RA) is a symmetric, inflammatory, peripheral polyarthritis of unknown
etiology. It typically leads to deformity through the stretching of tendons and ligaments and
destruction of joints through the erosion of cartilage and bone. The diagnosis of rheumatoid
arthritis can be made when symptoms of Inflammatory arthritis involving three or more joints
occur along with positive rheumatoid factor (RF) and/or anticitrullinated peptide/protein
antibody (such as anti-cyclic citrullinated peptide [CCP]) testing. Elevated levels of C-reactive
protein (CRP) or the erythrocyte sedimentation rate (ESR). Thus serologic parameters are of
paramount importance.
Rheumatoid factor is elevated in 70 to 80 percent of patients with RA. Their diagnostic utility is
limited by their relatively poor specificity; higher titers of RF (at least three times the upper limit
of normal) have somewhat greater specificity for RA. The prevalence of RF positivity in healthy
individuals rises with age. Anti-CCP antibodies have a similar sensitivity to RF for RA but have a
much higher specificity (95 to 98 percent). Recommendations are favouring sequential testing
for differential diagnosis, with a view towards improving early diagnosis, so that irreparable
joint damage can be avoided. The specificity is greater in patients with higher titers of anti-CCP
antibodies (at least three times the upper limit of normal). Another test, anti-mutated
citruilinated vimentin, gives similar results to anti-CCP and is used as an alternative in some
laboratories. Elevations of Acute phase reactants like the ESR and/or CRP level are consistent
with the presence of an inflammatory state, such as RA. The degree of elevation of these acute
phase reactants varies with the severity of inflammation. This talk would provide an overview of
modern serological diagnostic testing for rheumatoid arthritis.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
5
AUTOIMMUNITY
Shahla Shafiquea, Atiqur R Khanb, Vinit Mehrotrac
a Post Graduate Student, Department of Biochemistry, SRHU, Jollygrant, Dehradun
b Senior Resident, Department of Ophthalmology, SRHU, Jollygrant, Dehradun
c Professor, Department of Biochemistry, SRHU, Jollygrant, Dehradun
The immune system must distinguish self from harmful non-self to repel invaders and to
preserve the integrity of the host without inducing autoimmunity.
One definition of the immune system is that it is an intricate set of cellular, chemical and soluble
protein mechanisms, intended to shield the body against alien substances such as infections and
tumor cells, without attacking self-molecules. Antigens are those molecules (self or alien
molecules) which evoke specific immune responses in the body. Immune cells are situated
throughout the entire body. Organs such as the spleen, thymus, skin and gut contain immune
cells tactically placed in order to screen the entry of alien substances. Optimum functioning of
the immune system occurs when the immune cells and cell products work together with each
other in a sequential and harmonious manner.
Any deficit in this function can result in susceptibility to infections, malignancies [1-3] or over-
reactivity to harmless antigens, leading to immunopathology and autoimmunity. Autoimmune
diseases are pathological conditions identified by abnormal autoimmune responses and
characterized by auto-antibodies and T-cell responses to self-molecules by immune system
reactivity. [4]
Autoimrnunity is defined as the development of immune system reactivity in the form of auto-
antibodies and T-celI responses to self-structures. The etiology of autoimmune diseases has
been difficult to elucidate. Several factors are thought to contribute to the development of
immune response to self, including genetics ad environment [5-7]
Occupational exposures such as silica or silicon dioxide (Si02); solvents such as vinyl chloride;
pesticides and ultraviolet radiation are also known to be associated with the development of
autoimmune disease. [4]
An individual’s immune system protects one from disease and infection. If a person has an
autoimmune disease, their immune system inaccurately attacks healthy cells in their body.
These diseases tend to be genetic. [8]
The role of T-Lymphocytes. T cells have a variety of effector and regulatory functions. Both T
and B cells are derived from stem cells within the bone marrow. Immature T lymphocytes travel
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
6
from the bone marrow to the thymus where they grow into mature T lymphocytes. This
development includes proliferation, rearrangement of TCR genes and acquisition of the surface
receptors and accessory molecules of mature T cells. T cells with the ability to react with self-
antigens are then removed by apoptosis, creating a state of self-tolerance. Mature T cells then
inhabit the secondary lymphoid tissues and from there constantly recirculate via the
bloodstream in the pursuit of antigens.
The role of B-lymphocytes. B lymphocytes originate in the bone marrow and also become fully
matured there. Stimulated B cells develop into plasma cells that synthesize significant amounts
of antibody (immunoglobulin). Immunoglobulins fall into five different basic classes, namely,
IgG, IgA, IgD, 1gM, and IgE, all of which are secreted and circulate in the blood. Surface
immunoglobulin is the antigen receptor for B lymphocytes and when it attaches to an antigen
the B cell is activated, usually with the help of a TH cell responding to the same antigen. Once
the B cell is activated, it undergoes mitotic division to manufacture a replica of cells which are
able to synthesize immunoglobulin of the same antigen specificity. Most of the B cells of such a
clone mature into plasma cells. When an antigen is encountered for the first time, this is
described as the primary immune response. A few cells from the same clone mature to become
memory B cells, which are circulating lymphocytes that are able to respond quickly to any
subsequent challenge with the same antigen. Antibody production during this secondary
immune response occurs much more rapidly, is of much greater magnitude and produces IgG.
This phenomenon explains the lifetime immunity that follows many common infections; it is
also the general principle on which vaccination is used. [9]
The function of Lymphocytes. The immune factor of the body’s defence system is embodied
in the lymphocytes, antibodies and lymphokines. The T lymphocytes have specific cell-
membrane-associated- antigen binding receptors. The direct T-cell receptor binding to target
antigens, results in two different types of effector actions. Cytotoxic killing of the target is one
type, the other type being the release of lymphokines that regulate the migration and useful
capabilities of other inflammatory cells. [10] The group of B-lymphocytes and plasma cells
produce immunoglobulin’s with a large variety of antibody-combining sites which interact
with a target. Complexes of antibodies with antigens attach preferentially to inflammatory cells
of the phagocytic system by the steady region sites of the immunoglobulin (Ig) molecules, and
they can activate the humoral complement system.[10]
Lymphocytes not only assemble the specific inflammatory reactions to the antigenic stimulus,
but also focus non-specific inflammatory responses on the target. This provides bodies with the
ability to adapt and enlarge reactions designed to get rid of deleterious causes with efficiency
and without delay. Immunity is a!so involved in the elimination of old or damaged cells within
the body and in the demolition of abnormal or mutant cells which occur within the body. This
last function is known as immune surveillance, and constitutes as a major defence against
cancer. It has, on the other hand, become apparent that immune responses are not always
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
7
advantageous and may result in severe damage to the body. [11]
The role of APC (Antigen presenting cells). Numerous parts of the immune system may be
involved in autoimmune pathology. Antigens are taken up by antigen-presenting cells (APCs)
such as dendritic cells (DCs) and processed into peptides which are loaded onto the major
histocompatibility complex (MHC) molecules for presentation to T cells via clonotypic T cell
receptors (TCRs). Cytolytic T cells (Tc, activated by MHC Class I on APC) can directly damage a
target, while T helper cells (Th, activated by MHC class II) release cytokines that can have direct
effects or can activate macrophages, monocytes and B cells. B cells themselves have surface
receptors that can bind to surface antigens. Upon receiving signals from Th cells, the B cell
secretes antibodies specific for the antigens. An antibody may bind to its specific target alone or
may bind to and activate macrophages simultaneously via the Fc receptor. [12]
There are more than eighty identified autoimmune diseases [13]. Multiple arms of the immune
system may be involved in autoimmune pathology. Antigens are taken up by antigen presenting
cells (APC) such as dendritic cells (DC) and processed into peptides which are loaded onto MHC
molecules for presentation to T cells via clonotypic T cell receptors (TCR). Cytolytic T cells (Tc,
activated by MHC class I on APC) can directly lyse a target, while T helper cells (Th, activated by
MHC class II) release cytokines that can have direct effects or can activate macrophages,
monocytes and B cells. B cells themselves have surface receptors that can bind surface antigens.
Upon receiving signals from Th cells, B cells secrete antibodies specific for the antigens.
Antibody may bind its specific target alone or may bind to and activate macrophages
simultaneously via the Fc receptor.
Multiple mechanisms have been described to explain how pathogens might induce activation
and critical expansion of autoreactive T cells and start autoimmune disease [14-19]. A microbial
antigen can include an epitope that is structurally similar to an autoantigen epitope, providing
the basic element of the mechanism referred to as molecular mimicry [18-23]. Another
mechanism would imply that the inflammatory setting and the paracrine secretion of T cell
growth factors induce the expansion of activated autoreactive T cells, whose small number was
previously insufficient to drive an autoimmune disease. Such a mechanism is referred to as
bystander activation [26]. Pathogen-induced tissue inflammation may result in local activation
of APC and enhanced processing/presentation of self-antigens that causes T cell priming,
followed by T cell activation and expansion of additional specificities (epitope spreading)
[25,26]. Activation of resting autoreactive T cells may be achieved by viral and bacterial
superantigens that bind a variety of MHC class II molecules and activate large numbers of T
cells, irrespective of their specificity [27].
a) Molecular mimicry describes the activation of crossreactive T cells that recognize both the
pathogen-derived epitopes and the self-derived epitopes. Pathogen-derived epitops are taken
up by APC and presented to T cells. Activation of T cells results in the direct lysis of self- tissue
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
8
or release of cytokines and chemokines that activate macrophages, which mediate self- tissue
damage, and provide help to pathogen-specific B cells. The subsequent release of self- tissue
antigens and their uptake by APC perpetuates the autoimmune disease.
b) Bystander activation is the nonspecific activation of self-reactive T cells. Activation of
pathogen-specific T cells leads to inflammation that damages self-tissue in an antigen
nonspecific manner, and triggers activation of self-reactive T cells.
c) Epitope spreading involves a persistent pathogen infection that causes damage to self-
tissue. This results in the release of self-peptides, which are engulfed by APC and presented to
self-reactive T cells. Continual damage and release of self-peptides results in the spread of the
self-reactive immune response to multiple seif-epitopes.
Traditional therapies for autoimmune disease have relied on immunosuppressive medications
that globally dampen immune responses.These agents are highly effective for many patients
and thus remain the current “gold standard” of care [28].
However, long-term treatments with high doses are often ne.eded to maintain disease control,
leaving the patient susceptible to life-threatening opportunistic infections and long-term risk of
malignancy. In addition, the benefits of many of these drugs are counterbalanced by toxicity
and serious side effect profiles.
Thus, there has been a push for the development of more specific strategies that lower the risk
of systemic immune suppression and improve tolerability. The optimal therapy for
autoimmunity would be one that achieves four main goals:
(i) Specifically targets the pathogenic cells and leaves the remainder of the immune system
functioning normally;
(ii) Reestablishes immune tolerance that is sable over time, such that continuous or long- term
therapy is not needed;
(iii) Has low toxicity and few side effects; and
(iv) Is overall cost-effective when compared to alternative approaches. The new wave of
treatments for autoimmune disease strives to achieve these goals. Mechanistically, these
approaches either focus on inhibiting the activation of pathogenic cells or are aimed at
augmenting the pathways that naturally suppress these cells.
In conclusion, there is cause for optimism that the days of nonspecific immunosuppressive
medications with limited efficacy, high toxicity, and life-threatening side effects might end as
the new generation of immunotherapy pushes forward. Certainly, we are making strides
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
9
toward achieving the perfect treatment for autoimmunity. Thus, it may no longer be prudent to
ask if we will ever get there, but instead, it may now be just a question of when we reach.
References:
1. Samaras V, Rafailidis PT, Mourtzoukou EG, Peppas G, Falagas ME (2010) Chronic bacterial
and parasitic infections and cancer: a review. J Infect Dev Ctries 4: 267-281.
2. Bouvard V, Baan R, Straif K, Grosse Y, Secretan B, El Ghissassi F, Benbrahim-Tallaa L, Guha
N, Freeman C, Galichet L, Cogliano V (2009) A review of human carcinogens--Part
B:biological agents. WHO International Agency for Research on Cancer Monograph
Working Group. Lancet Oncol 10: 32 1-322.
3. zur Hausen H (2006) Streptococcus bovis: causal or incidental involvement in cancer of the
eolon?Int J Cancer 119: xi-xii.
4. Invernizzi, P., Gershwin, M.E. 2009. The Genetics of human autoimmune disease. Journal of
Autoimmunity. 33:303-308.
5. Rioux JD and Abbas AK (2005) Paths to understanding the genetic basis of autoimmune
disease. Nature 435: 584-589.
6. Bjorses P, Aaltonen J, Horelli-Kuitunen N, Yaspo ML, Peltonen L (1998) Gene defect behind
APECED: a new ëlue to autoimmunity. Hum Mol Genet 7: 1547-1553.
7. Walker LS and Abbas AK (2002) The enemy within: keeping self-reactive T cells at bay in the
periphery. Nat Rev Immunol 2: 11-19.
8. Medical Encyclopedia. [15 May 2011]. Autoinimune Diseases.
(http:/Jwww.nlm.nih.gov/medliflePlUS/aUtoimmUnediseases.html). (16 August 2011).
9. Young, B., Lowe, J.S., Stevens, A., Heath, J.W. 2006. Wheather’s Functional Histology. A
Text and Colour Atlas. 5th Edition. Page 65, 66, 208, 209.
10. Oppenheim, J.J., Rosenstreich, D.L., Potter, M. 1981. Cellular Functions in Immunity and
Inflammation. Immunity and Inflammation. Page 13-14.
11. Vander, A.J., Sherman, J.H., Luciano, D.S. 1987. Defence mechanisms of the body:
Immunology, foreign chemicals, and stress. Human Physiology: The Mechanisms of Body
Function. 5:600.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
10
12. Journal of Translational Immunology. [January 2009]. The role of infections in Autoimmune
Disease. A M Ercolini and S D Miller.
(http://www.ncbi.nlm.nih.gOV/pmc/artiCleS/PMC26656731. (25 August 2011).
13. Seigrade MK, Cooper GS, Germolec DR, Heindel JJ (1999) Linking environmental agents and
autoimmune disease: an agenda for future research. Environ Health Perspect; 107
(Suppl.5): 811-813.
14. Rose NR and Bona C (1993) Defining criteria for autoimmune diseases (Witebsky’ S
postulates revisited). Immunol Today 14: 426-430.
15. Oldstone MBA (1998) Molecular mimicry and immune mediated diseases. FASEB J 12:
1255-1265.
16. Theofilopoulos AN, and Kono DH (1998) Mechanisms and genetics of autoimmunity.
AnnNYAcadSci 841: 225-235.
17. Lori JA and Inman RD (1999) Molecular mimicry and autoimmunity. N Engi 3 Med 341:
2068-2074.
18. Benoist C and Mathis D (2001) Autoimmunity provoked by infection: how good is the case
for T cell epitope mimicry? Nat Irmnunol 2: 797-80 1.
19. Wucherpfennig KW (2001) Mechanisms for the induction of autoimmunity by infectious
agents. 3 Clin Invest 108: 1097-1 104.
20. Bachmaier K, Neu N, de la Maza LM, Pal S, Hessel A, Penninger JM (1999) Chlamydia
infections and heart disease linked through antigenic mimicry. Science 283: 1335-1339.
21. Rose NR and Mackay JR (2000) Molecular mimicry: a critical look at exemplary instances in
human diseases. Cell Mol Life Sci 57: 542-551.
22. Hemmer B, Gran B, Zhao Y, Marques A, Pascal J, Tzou A, Kondo T, Cortese I, Bielekova B,
Straus SE, McFarland HF, Houghten R, Simon R, Pinilla C, Martin R (1999)
23. Identification of candidate T-cell epitopes and molecular mimics in chronic Lyme disease.
Nat Med 5: 1375-1382.
24. Martin R, Gran B, Zhao Y, Markovic-Plese S, Bielekova, B, Marques A, Sung MH,Hemmer B,
Simon R, McFarland HF, Pmilla C (2001) Molecular mimicry and antigen- specific T cell
responses in multiple sclerosis and chronic CNS Lyme disease. J Autoimmun16: 187-192.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
11
25. Murali-Krishna K, Altman JD, Suresh M, Sourdive DJ, Zajac Al, Miller ID, Slansky J,Abmed R
(1998) Counting antigen-specific CD8 T cells: a reevaluation of bystander activation during
viral infection. Immunity 8: 177-187.
26. Lehmann PV, Forsthuber T, Miller A, Sercarz EE (1992) Spreading of T-cell autoimmunity to
cryptic detenninants of an autoantigen. Nature 358: 155-157.
27. Miller SD, Vanderlugt CL, Begolka WS, Pao W, Yauch RL, Neville KL, Katz-Levy Y, Carrizosa A,
Kim BS (1997) Persistent infection with Theiler’s virus leads to CNS autoimmunity via
epitope spreading. Nat Med 3: 1133-1 136.
28. Schrer MT, Ignatowicz L, Winslow GM, Kappler JW, Marrack P (1993) Superantigens:
bacterial and viral proteins that manipulate the immune system. Annu Rev Cell Biol. 9: 101-
128.
29. Rosenblum, M.D., Gratz, I.K., Paw, J.S. et al, Treating human autoimmunity: current
practice and future prospects.Sci Transi Med. 2012;4 (125sr1).
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
12
Immune system: How Not to Kill Your Own Kind
Dr Vikas Shrivastava, Assistant Professor, Department of Pathology, SRHU, Jollygrant,
Dehradun
Immune system is a double edged sword which protects us from infections on one hand but
induces cell injury in case of excessive activation. Spectrum of presentations of immune
disorder may span from too little immunity (immunodeficiency disorders) to too much
immunological reactivity (hyper-sensitivity and auto-immune diseases).
To understand the pathogenesis of autoimmune disorders, it is imperative to understand the
physiology of immune system. Immune system has to learn to live with the cells and antigens of
own body. This self-tolerance can be broadly classified into two groups: central tolerance and
peripheral tolerance.
In this review I will attempt to highlight the mechanism of immune tolerance to the self
antigens and how this system may break down and lead to development of autoimmune
diseases.
The Biochemical and Immunological Markers of Multiple Sclerosis (MS)
Dr. J.B. Gogoi, Professor & Head, Department of Biochemistry, VCSGGIMS & R,
Srinagar, Garhwal, Uttarakhand
Multiple sclerosis (MS) is one of the common chronic, progressive and degenerative
autoimmune disease in young adults characterized by recurrent relapses and/or progression
within the central nervous system. It is a complex disease in which several pathophysiological
mechanisms such as axonal/neuronal damage, demyelination, inflammation, gliosis,
remyelination and repair, alteration of the immune system, etc are involved.
Biological markers reflect the immunopathological changes that occur in MS. These markers
indicate the responses to therapeutic intervations and optimizing therapy. They help in
development of progress-specific therapies and the prevention of disability.
Key Words: Multiple sclerosis, biological marker, immunological marker, inflammation,
demyelination, immune system.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
13
“Modulation of Membrane complement regulatory proteins in Autoimmune disorders"
Nibhriti Das, Former Professor,Department of Biochemistry, All India Institute of Medical
Sciences, New Delhi
Complement is a proinflammatory system of the innate immunity comprising of about 30
soluble and cell surface proteins . The system consists of zymogens, receptors and regulatory
proteins. On activation of the proenzymes by antibody dependent and antibody independent
mechanisms, chemotaxins, anaphylotoxins, opsonins and membrane attack comlex are
generated which facilitate phagocytic killing of pathogens and also cause effect direct cellular
lysis to clear the danger signals but simultaneously produce inflammatory reactions.
Exaggerated complement activation by the immune complexes and autoantigens is a key
mechanism in the pathogenesis and organ damage in autoimmune disorders. In normal health,
complement activation is tightly under control of a large number of complement regulatory
proteins, most of them are membrane –bound and are encoded by a gene cluster known as
regulator of complement activation (RCA).
For last two decades there had been remarkable advancement in understanding the role of
complement regulatory proteins In autoimmune disorders Recent studies with gene knockout
mice have suggested that membrane-bound complement regulatory proteins may critically
determine the sensitivity of host tissues to complement injury in autoimmune and
inflammatory disorders .
In this context, studies by several investigators on animal models and, by us on human subjects
for last several years suggest disease related modulation of CR1, a key complement regulatory
protein in SLE and RA. It had earlier been documented that complement receptor 1 on
erythrocytes (ECR1) is less expressed in the patients with SLE and in RA. This led to the
exploration of E-CR1 as a disease activity marker by us and other investigators. While we
elucidated the mechanism involved in disease acquired modulation of cell surface CR1 using
leucocyte CR1 as the test model, we expanded the investigation to explore the significance of
leucocyte CR1(L-CR1) in the pathophysiology , diagnosis and prognosis SLE and ,more recently,
to explore the same for RA. Strategy had been to study the expression of membrane
complement proteins in patients and controls, elucidate their correlations with complement
peptides and immune complexes and correlate the same with disease activity parameters,
DAS28 for RA and SLEDAI scores for SLE.
The levels of L-CR1 protein and CR1 transcript declined markedly in patients with SLE. CR1
transcript could be shown as a marker to discriminate between the patients with and without
lupus nephritis and also proved to be a prognostic marker through follow up studies as patients
who did not show any improvement in the levels of LCR1 had bad prognosis.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
14
Like CR1, MCP, DAF and CD59 are trans-membrane complement regulatory proteins with major
functional implications. While in human, expression of CR1 is limited primarily to glomerular
podocytes and blood cells excepting platelets, MCP, DAF and CD59 are expressed on all
nucleated cells. DAF and CD59 are also expressed on erythrocytes.
Since leucocyte CRPs are also involved in immune cell signaling and regulation of immune
responses, over the last few years our study got extended and focussed to leucocyte CRPs.
Our studies suggested disease related modulation of leucocyte MCP, DAF and CD59 transcript
expression in SLE and RA. Cytokines and immune complexes were found to alter the expression
of these cell surface complement proteins. Thus our findings suggest collaborative role of
cytokines, complement peptides and membrane complement regulatory proteins in modulating
the disease activity of systemic autoimmune disorders
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
15
Molecular and Immunological characterization of High Risk Human Papilloma Virus Types-Clinical Relevance w.r.t to Uttarakhand Females
Narotam Sharma, Assistant Professor, Department of Biochemistry, SGRRIMSH,
Dehradun, Uttarakhand
Human Papilloma Virus (HPV) also known as shy virus is an etiological agent for cervical cancer
along with the cause for genitial and cutaneous warts and lesions. Human Papilloma Virus (HPV)
is a necessary causative agent for the cause and progression of cervical cancer. Diagnosis is
difficult as HPV cannot be propagated in tissue culture, and therefore, in most cases its accurate
identification relies on molecular biology techniques. With the advent of Nucleic Acid
Amplification Techniques (NAATs) and other molecular diagnostics tools, have markedly
increased essential parameters like sensitivity and specificity for the detection of HPV. There are
about 120-130 HPV types! Genotypes known but 13-16 types are under High risk category
responsible for the cancer whereas about 10-12 HPV types are categorized in Low risk group
causing different lesions and warts. Thus molecular and Immunological characterization of
clinically relevant HPVs are of utmost significance for the proper management of the patients.
Spectrum of Autoimmune Diseases in Uttarakhand Dr.Ravi Kant, Assistant Professor, Department of Internal Medicine, AIIMS, Rishikesh
(Uttrakhand)
Uttarakhand and adjoining states has a high burden of autoimmune diseases .The majority of
autoimmune diseases are either undiagnosed , underdiagnosed or under-treated .At AIIMS
Rishikesh the data collected shows a very high incidence of rheumatoid artrithis .The patients at
presentation are having high disease activity score and majority of them have deformity . The
patients with rheumatoid arthritis has high incidence of seronegativity .The incidence of
ankylosing spondilitis is next to rheumatoid arthritis followed by systemic sclerosis and other
connective tissue disorders.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
16
Overview of autoimmune disorders and future directions
Dr.Kalpana Luthra, Professor, Department of Biochemistry, AIIMS, New Delhi
Autoimmune disorders include organ specific diseases such as Hashimoto’s thyroiditis, in which
the damage caused by the autoantibodies or self reactive lymphocytes is confined to the
specific organ; while in systemic autoimmune disorders, eg. Rheumatoid arthritis (RA) and
Systemic Lupus erythematosus (SLE), immune response is directed against most of the tissue
antigens throughout the body. Individuals mostly in early- to mid-adulthood are affected by
these diseases, and the associated morbidity imposes a considerable economic burden and
diminishes quality of life over decades. Moreover, both RA and SLE are associated with early
death. Although the prognosis for these diseases has improved substantially over the years,
overall outcome remains inadequate. The patients continue to be symptomatic even after
initiation of therapy, and the existing treatment strategies lead to immunosuppression.
To successfully modulate immune responses in SLE and RA, we must understand which cellular
interactions or molecular pathways are aberrantly regulated in these diseases. Gene expression
analyses based on genome-wide association studies (GWAS) suggest that dendritic cell (DC)–and
B cell–intrinsic pathways may be dysregulated in SLE and T cell intrinsic pathways dysregulated
in RA. Nonetheless, each disease is promoted by an aberrant repertoire of adaptive immune
cells, triggered, plausibly by altered antigen presentation and abnormal B cell selection in the
germinal center (GC).
Several novel therapeutics are currently being explored. An ideal therapy would be to provide
sufficient immunomodulation so that the patients experience a prolonged disease-free, drug-
free existence, despite their genetic predisposition to disease, if any. Some of the recent
approaches addressed for accomplishing this goal are to modulate antigen presentation to the
adaptive immune system; to alter B cell selection in the germinal center, and to use decoy
antigens to prevent the formation of pro-inflammatory immune complexes. Disease activity is
sustained in part by the pro-inflammatory properties of the disease specifc immune complexes.
The pathways of disease initiation and propagation are potential targets of the next generation
therapies.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
17
SECTION -B (Presentations)
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
18
Autoimmune Diseases
ManjushaTyagi & Preeti Juyal,Assistant .Professor Dept of Microbiology
SGRR (PG) College,Dehradun
Autoimmune diseases are disorders in which the body’s immune system attacks the body’s
own cells and organs with proteins called autoantibodies; this process is called autoimmunity.
The body’s immune system normally makes large numbers of proteins called antibodies to help
the body fight off infections. In some cases, however, the body makes autoantibodies. Certain
environmental triggers can lead to autoimmunity. Environmental triggers are things originating
outside the body, such as bacteria, viruses, toxins, and medications. A combination of
autoimmunity, environmental triggers, and a genetic predisposition can lead to autoimmune
hepatitis. Autoimmune disorders are conditions in which a person's immune system attacks the
body's own cells, causing tissue destruction. Autoimmune diseases are classified as either
general, in which the autoimmune reaction takes place simultaneously in a number of tissues,
or organ specific, in which the autoimmune reaction targets a single organ. Autoimmune
disorders include the following:
Systemic lupus erythematosus: A general autoimmune disease in which antibodies attack a
number of different tissues. The disease recurs periodically and is seen mainly in young and
middle-aged women.
Rheumatoid arthritis : It occurs when the immune system attacks and destroys the tissues that
line bone joints and cartilage. The disease occurs throughout the body, although some joints
may be more affected than others.
Goodpasture's syndrome: It occurs when antibodies are deposited in the membranes of both
the lung and kidneys, causing both inflammation of kidney glomerulus (glomerulonephritis ) and
lung bleeding. It is typically a disease of young males.
Grave's disease: It is caused by an antibody that binds to specific cells in the thyroid gland,
causing them to make excessive amounts of thyroid hormone.
Hashimoto's thyroiditis It is Caused by an antibody that binds to cells in the thyroid gland.
Unlike in Grave's disease, however, this antibody's action results in less thyroid hormone being
made.
Pemphigus vulgaris: A group of autoimmune disorders that affect the skin.
Myasthenia gravis: A condition in which the immune system attacks a receptor on the surface
of muscle cells, preventing the muscle from receiving nerve impulses and resulting in severe
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
19
muscle weakness.
Scleroderma:It is also called CREST syndrome or progressive systemic sclerosis, scleroderma
affects the connective tissue.
Autoimmune hemolytic anemia: It occurs when the body produces antibodies that coat red
blood cells.
Autoimmune thrombocytopenic purpura: The disorder in which the immune system targets
and destroys blood platelets.
Polymyositis and Dermatomyositis: The Immune disorders that affect the neuromuscular
system.
Pernicious anemia:The Disorder in which the immune system attacks the lining of the stomach
in such a way that the body cannot metabolize vitamin B12.
Sjögren's syndrome:It occurs when the exocrine glands are attacked by the immune system,
resulting in excessive dryness.
Ankylosing spondylitis: The Immune system induced degeneration of the joints and soft tissue
of the spine.
Vasculitis: A group of autoimmune disorders in which the immune system attacks and destroys
blood vessels.
Type I diabetes mellitus: It may be caused by an antibody that attacks and destroys the islet
cells of the pancreas, which produce insulin.
Amyotrophic lateral schlerosis: It is also called Lou Gehrig's disease. An immune disorder that
causes the death of neurons which leads to progressive loss of muscular control.
Guillain-Barre syndrome:It is also called infectious polyneuritis. Often occurring after an
infection or an immunization (specifically Swine flu), the disease affects the myelin sheath,
which coats nerve cells. It causes progressive muscle weakness and paralysis.
Multiple sclerosis: An autoimmune disorder that may involve a virus affects the central nervous
system, causing loss of coordination and muscle control.
Scientists have made an important breakthrough in the fight against debilitating autoimmune
diseases scientists were able to selectively target the cells that cause autoimmune disease by
dampening down their aggression against the body's own tissues while converting them into
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
20
cells capable of protecting against disease. This type of conversion has been previously applied
to allergies, known as 'allergic desensitisation', but its application to autoimmune diseases has
only been appreciated recently. Investigators with the National Institutes of Health have
discovered the genomic switches of a blood cell key to regulating the human immune system.
Now today, open the door to new research and development in drugs and personalized
medicine to help those with autoimmune disorders such as inflammatory bowel disease or
rheumatoid arthritis. Identifying autoimmune disease susceptibility genes can be a challenge
because in most cases a complex mix of genetic and environmental factors is involved. Genetic
studies have shown that people with autoimmune diseases possess unique genetic variants, but
most of the alterations are found in regions of the DNA that do not carry genes. Scientists have
suspected that the variants are in DNA elements called enhancers, which act like switches to
control gene activities. Using genomic techniques, the researchers combed the T cell genome
for regions that are particularly accessible to proteins, a hallmark of DNA segments that carry
SEs. They identified several hundred, and further analysis showed that they largely control the
activities of genes that encode cytokine and cytokine receptors. These types of molecules are
important for T cell function because they enable them to communicate with other cells and to
mount an immune response. macrophages is their ability to change state depending on
environmental factors. Passing the activation process, macrophages can perform dramatically
different functions in the human body as pro-inflammatory or anti-inflammatory. The study of
these processes is important for the understanding of the human immune system and curing
autoimmune diseases. Benaroya Research Institute at Virginia Mason (BRI) is one of the
research institutes in the world dedicated to discovering causes and cures to eliminate
autoimmune diseases. BRI’s work in the laboratory to investigate diseases at a genetic and
molecular level is being translated into understanding how these approaches can be applied to
patients and at-risk individuals. Indeed, BRI is now using these therapies and discoveries in
clinical research to bring new medical advances to people at the earliest opportunity.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
21
Autoimmunity and Liver
G.Awasthi1 and Aditya swarup2
1 :Department of Biochemistry, Dolphin (P.G.) Institute, Dehradun
2:Department of Pathology, Dolphin (P.G.) Institute, Dehradun
Autoimmune hepatitis is a chronic or long lasting disease in which the body’s immune system
attacks the normal components, or cells, of the liver and causes inflammation and liver damage.
A combination of autoimmunity, environmental triggers, and a genetic predisposition can lead
to autoimmune hepatitis.
It is more common in females. The disease can occur at any age and affects all ethnic groups.
Autoimmune hepatitis is classified into two types. Type I autoimmune hepatitis is the most
common form in North America. Type 1 can occur at any age; however, it most often starts in
adolescence or young adulthood. About 70 percent of people with type 1 autoimmune hepatitis
are female. Type 2 autoimmune hepatitis is less common and occurs more often in children
than adults. People with type 2 can also have any of the above autoimmune disorders.
The most common symptoms of autoimmune hepatitis are fatigue, joint pain, nausea, loss of
appetite, pain or discomfort over the liver, skin rashes, dark yellow urine, light-colored stools,
jaundice, or yellowing of the skin and whites of the eyes. Symptoms of autoimmune hepatitis
range from mild to severe. Some people may feel as if they have a mild case of the flu.
Treatment works best when autoimmune hepatitis is diagnosed early. People with autoimmune
hepatitis generally respond to standard treatment and the disease can be controlled in most
cases. Long-term response to treatment can stop the disease from getting worse and may even
reverse some damage to the liver.
People with autoimmune hepatitis who have no symptoms or a mild form of the disease may or
may not need to take medication. In some people with mild autoimmune hepatitis, the disease
may go into remission. Corticosteroids (prednisone) are used for the treatment. Treatment may
begin with a high dose that is gradually lowered as the disease is controlled. The treatment goal
is to find the lowest possible dose that helps control the disease. Immune system suppressors
such as azathioprine are also be used. In some people, autoimmune hepatitis progresses to
cirrhosis and end-stage liver failure, and a liver transplant may be necessary.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
22
Autoimmune Hepatitis
Ashwani Sanghi, Department of Biochemistry, Dolphin (P.G) Institute , Dehradun
Autoimmune hepatitis (ATH) is one type of liver disease that occurs when immune system mistakes liver
cells for foreign aggressors and creates antibodies to attack them. Autoinimune hepatitis (AIH) is a
chronic condition and can result in cirrhosis (scarring) of the liver and (ultimately) liver failure. There are
two types of AIH: Type I Autoimmune hepatitis and Type II Autoimmune hepatitis. Type I is more
common and tends to affect young women, and is associated with other autoimmune diseases. This is
the most common form of all in North America. Type II primarily affects girls between the ages of 2 and
14. While A11T generally occurs in adolescence or early adulthood, it can develop at any age. Grave’s
disease, thyroiditis, ulcerative colitis, type I diabetes, rheumatoid arthritis, scleroderma, inflammatory
bowel disease (IBD), systemic lupus erythematosus are autoimmune conditions that can cause
symptoms of liver disease and are also associated with the development of AIH. Enlarged liver, abnormal
blood vessels on the skin, abdominal distention, dark urine, pale- colored stools, loss of appetite, nausea,
vomiting, joint pain, abdominal discomfort are common symptoms of Autoimmune Hepatitis. Symptoms
of Autoimmune Hepatitis are very similar to those of viral hepatitis
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
23
Hashimoto’s Thyroiditis
Ankit Johari , Department of Pathology, Dolphin Institute Sciences, Dehradun
Hashimoto’s thyroiditis is the most prevalent autoimmune thyroid gland disease. It is now
over a century since the first description of the disease by the Japanese doctor Hakaru
Hashimoto in 1912, yet the etiopathogenesis of the disease is still discussed. At present it is
thought that Hashimoto’s disease is provoked in genetically susceptible individuals by both
environmental and endogenous triggers. Genetic predisposition to development of the
autoimmune thyroid diseases was established on the basis of the epidemiologic studies
indicating increased prevalence of such diseases in some families, especially in twins. According
to current knowledge appearance of Hashimoto’s disease in Caucasians is associated with some
gene alleles: human leukocyte antigens (HLAs), mainly class II HLA DR3 and DR5, cytotoxic T
lymphocyte antigen-4 (CTLA-4), protein tyrosine phosphatase nonreceptor — type 22 (PTPN22),
thyroglobulin (Tg), vitamin D receptor (VDR) and cytokines. Among environmental factors
triggering the thyroid autoimmunity the following should be mentioned: excessive iodine intake,
treatment with certain drugs (interferon x, IL- 2, lithium, amiodarone), infections, mainly viral
and exposure to many chemicals such as polyaromatic hydrocarbons and phenyls. Female sex,
rebound phenomenon in postpartum period and fetal microchimerism are essential
endogenous factors in the etiopathogenesis of Hashimoto’s disease. Above mentioned factors
are responsible for the development of autoimmune response in thyroid gland. It leads to
increased antigen presentation by antigen presenting cells (APC), inappropriate presentation of
HLA antigens class II by thyroid follicular cells and reduced immune tolerance. Developing
autoimmune process, predominantly Th1-type, is responsible for the increased production of
TNF-α, IFN-γ and IL-1 cytokines. Destruction of thyroid tissue with subsequent development of
fibrous tissue is mediated by apoptosis process, CD8+ cytotoxicity, change of cell junctions and
complement activation. On clinical examination Hashimoto’s disease may present as classical,
atrophic, focal or juvenile form. Additionally, there are two variants of Hashimoto’s disease:
silent, painless thyroiditis and postpartum thyroiditis. Natural course of Hashimoto’s disease
leads to hypothyroid state. High antiperoxidase and antithyroglobulin antibodies concentrations
and hypoechogenic structure of thyroid gland on ultrasonographic examination confirm the
diagnosis of Hashimoto’s disease. Fine-needle aspiration biopsy is rarely needed to confirm
the diagnosis. The treatment of Hashimoto’s disease includes an administration of substitutive
doses of levothyroxine, but the time of treatment beginning is still the matter of discussion.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
24
Multiple Sclerosis
Aditya Swarup, Department of Pathology, Dolphin (P.G) Institute, Dehradun
The name multiple sclerosis refers to scars (sclerae—better known as plaques or lesions) in particular in
the white matter of the brain and spinal cord. MS was first described in 1868 by Jean-Martin Charcot.
Multiple sclerosis is the most common autoimmune disorder affecting the central nervous system. As of
2008, between 2 and 2.5 million people are affected globally with rates varying widely in different
regions of the world and among different populations. In 2013 20,000 people died from MS up from
12,000 in 1990. The disease usually begins between the ages of 20 and 50 and is twice as common in
women as in men.
Multiple sclerosis (MS) is also known as disseminated sclerosis or encephalomyelitis disseminate and is
an inflammatory disease in which the insulating covers of nerve cells in the brain and spinal cord are
damaged. This damage disrupts the ability of parts of the nervous system to communicate, resulting in a
wide range of signs and symptoms including physical, mental and sometimes psychiatric problems. MS
takes several forms, with new symptoms either occurring in isolated attacks (relapsing forms) or building
up over time (progressive forms).
While the cause is not clear, the underlying mechanism is thought to be either destruction by the
immune system or failure of the myelin-producing cells. Proposed causes for this include genetics and
environmental factors such as infections.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
25
Myasthenia gravis
Aditya Swarup, Department of Pathology, Dolphin (PG) Institute, Dehradun
Myasthenia gravis is a chronic autoimmune neuromuscular disease characterized by varying
degrees of weakness of the skeletal (voluntary) muscles of the body. Myasthenia gravis is caused
by a defect in the transmission of nerve impulses to muscles. The voluntary muscles of the
entire body are controlled by nerve impulses that arise in the brain. These nerve impulses travel
down the nerves to the place where the nerves meet the muscle fibers. Nerve fibers do not
actually connect with muscle fibers. There is a space between the nerve ending and muscle
fiber; this space is called the neuromuscular junction. When the nerve impulse originating in the
brain arrives at the nerve ending, it releases a chemical called acetylcholine. Acetyicholine
travels across the space to the muscle fiber side of the neuromuscular junction where it
attaches to many receptor sites. The muscle contracts when enough of the receptor sites have
been activated by the acetyicholine In MG, there can be as much as an 80% reduction in the
number of these receptor sites. The reduction in the number of receptor sites is caused by an
antibody that destroys or blocks the receptor site.
Antibodies are proteins that play an important role in the immune system. They are normally
directed at foreign proteins called antigens that attack the body. Such foreign proteins include
bacteria and viruses. Antibodies help the body to protect itself from these foreign proteins. For
reasons not well understood, the immune system of the person with MG makes antibodies
against the receptor sites of the neuromuscular junction. Abnormal antibodies can be measured
in the blood of many people with MG. The antibodies destroy the receptor sites more rapidly
than the body can replace them. Muscle weakness occurs when acetyicholine cannot activate
enough receptor sites at the neuromuscular junction
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
26
Rheumatoid arthritis
Rashmi Chouhan, Department of Pathology, Dolphin (P.G) Institute , Dehradun
RA affects between 0.5 and 1% of adults in the developed world with between 5 and 50 per
100,000 peop1e newly developing the condition each year. Onset is most frequent during
middle age, but people of any age can be affected. In 2013 it resulted in 38,000 deaths up from
28,000 deaths in 1990.. The first recognized description of RA was made in 1800 by Dr. Augustin
Jacob Landré-Beauvais (1772—1840) of Paris.
Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the
joints. Autoinimune diseases are illnesses that occur when the body’s tissues are mistakenly
attacked by their own immune system. The immune system contains a complex organization of
cells and antibodies designed normally to “seek and destroy” invaders of the body,
particularly infections. Patients with autoimmune diseases have antibodies and immune cells in
their blood that target their own body tissues, where they can be associated with inflammation.
While inflammation of the tissue around the joints and inflammatory arthritis are characteristic
features of rheumatoid arthritis, the disease can also cause inflammation and injury in other
organs in the body. Because it can affect multiple other organs of the body, rheumatoid
arthritis is referred to as a systemic illness and is sometimes called rheumatoid disease.
Rheumatoid arthritis that begins in people under 16 years of age is referred to as juvenile
idiopathic arthritis (formerly juvenile rheumatoid arthritis).
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
27
Autoimmune Disorders During Pregnancy
G.Awasthi1,Shivsharan Singh1 and Aditya swarup2
1:Department of Biochemistry,Dolphin (P.G.) Institute , Dehradun
2:Department of Pathology, Dolphin (P.G.) Institute,, Dehradun
Autoimmune disorders, including Graves disease are more common among women, particularly
pregnant women. The abnormal antibodies produced in autoimmune disorders can cross the
placenta and cause problems in the fetus. Pregnancy affects different autoimmune disorders in
different ways.
Antiphospholipid syndrome:Antiphospholipid syndrome, which causes blood clots to form too
easily or excessively, can cause a miscarriage or stillbirth. Pregnant women may develop high
blood pressure or preeclampsia The fetus may not grow as expected.If a woman has
antiphospholipid syndrome, she is usually treated with anticoagulants and with low-dose aspirin
during pregnancy and for 6 wk postpartum. Such treatment can prevent blood clots and
pregnancy complications from developing.
Systemic lupus erythematosus (lupus): It may appear for the first time, worsen, or become less
severe during pregnancy. How a pregnancy affects the course of lupus cannot be predicted, but
the most common time for flare-ups is immediately after delivery.Women who develop lupus
often have a history of repeated miscarriages, fetuses that do not grow as much as expected,
and preterm delivery. If women have complications due to lupus (such as kidney damage or
high blood pressure), the risk of death for the fetus or newborn and for the woman is
increased.
In pregnant women, lupus antibodies may cross the placenta to the fetus. As a result, the fetus
may have a very slow heart rate, anemia, a low platelet count, or a low white blood cell count.
However, these antibodies gradually disappear over several weeks after the baby is born, and
the problems they cause resolve except for the slow heart rate.If women with lupus were
taking hydroxychloroquine before they became pregnant, they may take it throughout
pregnancy. If flare-ups occur, women may need to take a low dose of prednisone (a
corticosteroid) by mouth, another corticosteroid such as methylprednisolone , or a drug that
suppresses the immune system (immunosuppressant) such as azathioprine
Myasthenia gravis: This disorder, which causes muscle weakness, does not usually cause
serious or permanent complications during pregnancy. However, women may need to take
higher doses of drugs (such as neostigmine ) used to treat the disorder or may need to take
corticosteroids or drugs that suppress the immune system (immunosuppressants).Some drugs
that are commonly used during pregnancy, such as magnesium and oxytocin, can make the
weakness caused by myasthenia gravis worse. So women who have myasthenia gravis must
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
28
make sure their doctors know they have it. Very rarely during labor, women who have
myasthenia gravis need help with breathing (assisted ventilation).
The antibodies that cause this disorder can cross the placenta. So about one of five babies born
to women with myasthenia gravis is born with the disorder. However, the resulting muscle
weakness in the baby is usually temporary because the antibodies from the mother gradually
disappear and the baby does not produce antibodies of this type.
Immune thrombocytopenia (ITP): In ITP, antibodies decrease the number of platelets (also
called thrombocytes) in the bloodstream. Too few platelets (thrombocytopenia) can cause
excessive bleeding in pregnant women and their babies. If not treated during pregnancy, the
disorder tends to become more severe. Corticosteroids, usually prednisone given by mouth,
can increase the number (count) of platelets and thus improve blood clotting in pregnant
women with this disorder. However, this improvement lasts in only about half of women. Also,
prednisone increases the risk that the fetus will not grow as much as expected or will be born
prematurely. Women who have a dangerously low platelet count may be given high doses of
immune globulin intravenously shortly before delivery. This treatment temporarily increases
the platelet count and improves blood clotting. As a result, labor can proceed safely, and
women can have a vaginal delivery without uncontrolled bleeding.Pregnant women are given
platelet transfusions only when a cesarean delivery is needed and when the platelet count is so
low that severe bleeding may occur.Rarely, when the platelet count remains dangerously low
despite treatment, the spleen, which normally traps and destroys old blood cells and platelets,
is removed. The best time for this surgery is during the 2nd trimester.The antibodies that cause
the disorder may cross the placenta to the fetus. However, they rarely affect the platelet count
in the fetus.
Rheumatoid arthritis: Rheumatoid arthritis may develop during pregnancy or, even more often,
shortly after delivery. If arthritis has damaged the hip joints or lower (lumbar) spine, delivery
may be difficult for the woman, but this disorder does not affect the fetus. The symptoms of
rheumatoid arthritis may lessen during pregnancy, but they usually return to their original level
after pregnancy.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
29
Auto-Antibodies in Heart Diseases
G.Awasthi1 and Aditya swarup2
1Department of Biochemistry, Dolphin (P.G.) Institute , Dehradun
2Department of Pathology, Dolphin (P.G.) Institute ,Dehradun
Heart failure is the final clinical entity of many diverse disease causes and mechanisms. Among
the modulators of disease progression a dysregulation in the immune system of yet unknown
reasons is believed to play a central role in disease progression. Circulating autoantibodies have
been critically linked to heart failure. These autoantibodies are targeted against diverse self-
antigens, which often are not restricted in their exposition to cardiac muscle. Their prevalence,
mode of action, and potential therapeutic modulation are intensively investigated. Although a
triggering injury to myocardium is believed to be the crucial initiating event, the genetic
predisposition, environmental and epigenetic modulators, and other still unknown mechanisms
are critical for development of the pathological antibody titers observed in peripheral blood and
the intensity of inflammation in myocardial structures. In some studies it was found that
circulating anti-heart autoantibodies may precede disease manifestation and are independent
predictors of disease development. Clinical observations on a prognostic relevance of
autoantibodies have prompted therapeutic trials focused on nonspecific removal of
autoantibodies from the circulation via immune-adsorption. There are first reports on a
beneficial outcome in patients treated by immune-adsorption. However, the presence of anti-
heart specific autoantibodies may not always be harmful because some antibodies seem to be
protective in chronic heart failure.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
30
Advanced glycation end products (AGEs) modified immunoglobulin G (IgG) presents unique epitopes for type 1 diabetes autoantibodies
Lokendra Kumar1,3 and1, 2Zafar Rasheed
1Department of Biochemistry, SBSPGI, Balawala, Dehradun, UK, India.
2Department of Pathology, Microbiology, & Immunology, School of Medicine,
University of South Carolina, Columbia, SC, USA 3Department of Microbiology, P M College of Education Aligarh, UP, India
Non-enzymatic glycation of protein in serum and tissues is a pathphysiological consequence of
hyperglycemia in diabetes mellitus (DM) and also correlates with aging. Advanced glycation end
products (AGEs)–damaged IgG (AGE-IgG) occurs as a result of hyperglycemia. AGE-IgG is of
special interest due to its possible influence on the functionality of immunoglobulins and overall
immune-competence. The role of AGE damaged IgG in type 1 DM has been investigated in the
present study.
IgG was isolated from the normal humans and was subjected to in vitro glycation with glucose.
Formation of AGEs induced modification on IgG has been studied by physico-chemical
techniques. Immunogenicity of native and AGE-modified IgG was probed by inducing polyclonal
antibodies in experimental animals. The binding characteristics of circulating antibodies in DM
patients against native and AGE-IgG were assessed. Type 1 DM patients (n=31) were examined
by ELISA and their results were compared with healthy age-matched human controls (n=22).
The AGEs caused extensive damaged to IgG. The AGE-IgG was found to be highly immunogenic
in rabbits as comparison to native IgG. High degree of specific binding by 61.3 % of DM sera
autoantibodies towards AGE-IgG was observed, in comparison to its native analogue (p< 0.05).
Sera from those type 1 DM patients having smoking history, high aging with high degree of
disease showed substantially stronger binding to AGE-IgG over native IgG in particular. IgG from
type 1 DM patients (DM-IgG) contained higher levels of carbonyls than from IgG of normal
human subjects (normal-IgG) (p<0.001).
The AGEs modification of IgG causes perturbations, resulting in the generation of neo-epitopes,
and making it a potential immunogen. The IgG modified with AGEs may be one of the factors for
the induction of circulating type 1 DM autoantibodies.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
31
MWCNT/Gold nanoparticle based Genosensor for early Detection of Rheumatic Heart Disease
Ankur Kaushalab, Dinesh Kumara, Deepak Kalaa, Shashi Kharec and Ashok Kumar*ab
aShoolini University of Biotechnology and Management Science, Solan-173212, India bCSIR-Institute of Genomics and Integrative Biology, Mall Road, Delhi-110007, India
cNational Centre for Disease Control, Sham Nath Marg, Delhi-110054, India
RHD sensor based on DNA probe of Streptococcus pyogenes has been developed by the
immobilization of 5´-NH2 labeled single stranded DNA probe on to a MWCNT/gold nanoparticle
based screen printed carbon electrode. The immobilized single stranded DNA probe was further
hybridized with isolated genomic DNA of S. pyogenes. The carbon electrode surface
characterization, before and after hybridization, was carried out by scanning electron
microscopy (SEM) and Fourier transform infrared spectroscopy (FTIR). The change in current
after hybridization was measured by cyclic voltammetry (CV), differential pulse voltammetry
(DPV) and impedance based studies using redox indicator. The immobilized probe can detect up
to 0.5-100 ng/6µl of genomic DNA. The available detection method for diagnosis of RHD is
bacterial culture, β-hemolysis, bacitracin sensitivity, hippurate test, phadebact test, CRP (C-
reactive protein), ESR and PCR. All these methods are either time consuming or have some
limitations. DNA biosensor is specific, quick (30 min) and reliable method for early detection of
S. pyogenes infection causing pharyngitis. Specificity was further determined by hybridization
with different bacterial strains. Electrode was found stable for 6 months on storage at 4 °C with
5–6 % loss in initial DPV current.
.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
32
Antibiotic induced alterations in the commensal microbiome reduce CD4+Foxp3+ Tregs in the colonic lamina propria and increase allergic responses to food
Prabhanshu Tripathi1,2, Andrew Stefka1, Taylor Feehley1, Tiffany Patton1, Eugene Chang1,
Dionysios Antonopoulos1, Zhiheng Pei3 and Cathryn Nagler1 1University of Chicago, Chicago, IL, USA, 2University of Gothenburg, Gothenburg, Sweden and
3NYU School of Medicine, New York, NY
Antibiotic (Abx) use in early life has been implicated in the increasing prevalence of food allergy,
presumably due to its effects on the commensal bacterial microbiome. To gain insight into the
mechanisms by which commensal bacteria regulate allergic responses to food, C57Bl/6 mice
were treated with a cocktail of Abx, beginning by gavage at two weeks of age and continuing in
the drinking water after weaning. 16S rDNA based pyrosequence analysis demonstrated that
Abx treatment significantly altered the composition and diversity of the fecal microbiota;
Lachnospiraceae (Clostridia) were significantly reduced and Bacteroidaceae were enriched in
fecal samples obtained from Abx treated mice. Reduced Clostridia abundance correlated with
significantly decreased proportions of CD4+Foxp3+ Tregs in the colonic lamina propria, but not
the spleen or mesenteric lymph node, of Abx treated mice compared to untreated controls.
Elevated allergen specific IgE and IgG1 responses were induced in Abx treated (but not
untreated) mice sensitized with purified peanut extract plus cholera toxin. Transfer of
CD4+Foxp3+Tregs from untreated mice, prior to sensitization, blocked the allergen specific IgE
response induced by Abx treatment. Our data supports the hypothesis that bacteria (Clostridia)
induce CD4+Foxp3+ Tregs in the colonic mucosa. These Tregs are depleted (and protection
against an allergic response to food is reduced) in Abx treated mice.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
33
Detection of Celiac disease related anti-gliadin antibodies using carbon based surface chemistry
Shagun Gupta, Ankur Kaushal, Rupak Nagraik, Deepak Kala, Dinesh Kumar*
Shoolini University of Biotechnology and Management Sciences, Solan-173212
Celiac Disease (CD) is an autoimmune disorder, characterized by the ingestion of gliadin protein,
a component of wheat gluten. CD is closely associated with genes that code HLA-II antigens,
mainly of DQ2 and DQ8 classes. Small intestinal biopsy is considered the main approach for
diagnosis of classical celiac disease. In addition, IgA and IgG antibodies against gliadin are
valuable tools for the detection of patients with celiac disease and for therapy control. In the
present work, an electrochemical biosensor for the diagnosis of Celiac disease related anti-
gliadin antibodies using Differential pulse voltammetric study is compared with ELISA. The
working electrode of immunosensor consists of gliadin (Ag)/antigliadin Ab/ Alkaline Phosphatase
(AP) labeled antibody immobilized on carbidimide-functionalized multiwalled carbon nanotube
(cf-MWCNT) electrode. The Indoxyl phosphate/silver nitrate substrate was used for detection of
immune complex formed on electrode surface to monitor the direct Ag-Ab interaction on
electrode surface. It was observed that the sensitivity of immunosensor was high compared to
ELISA.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
34
Increased Production of Autoantibodies in Physically Active Older
Individuals After Vaccination Shiv Sharan Singh, Department of Biochemistry, Dolphin (P.G) Institute , Dehradun
The process of immunosenescence causes both morphological and functional changes in the
immune system.One of the main features of immunosenescence in the elderly is the loss of the
ability to recognize foreign antigens and the body’s own antigens, leading to an increase in
autoantibody levels. Other characteristics of immunosenescence include a reduction in naive T-
cells, an accumulation of memory cells and a change in cytokine profile from Th1 to Th2.
Immunosenescence is associated to aging and among many changes in immune response is
reported a reduced response to vaccination and an increase in the number of cases of
autoimmunity, caused by autoantibodies known as natural antibodies whose function,
according to reports, would be protection against infection and inflammation. Although
immunosenescence is an irreversible process, regular moderate exercise can attenuate some
aspects of the decline in the immune system. Practically it is found that the serum Ig M and IgG
levels after vaccination were higher in the group that exercised regularly than in the sedentary
group. We were also able o demonstrate a significant correlation between levels of natural
autoantibodies and response to vaccination
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
35
Diagnosis of Autoimmune Diseases
Santosh Kumar, Department of Biochemistry, Dolphin (PG.) Institute , Dehradun
The first step in managing patients with any disorder is proper diagnosis. Diagnosing
autoimmune diseases can be particularly difficult, however, because these disorders can affect
any organ or tissue in the body, and produce highly diverse clinical manifestations, depending
on the site of autoimmune attack. Moreover, disease symptoms are often not apparent until the
disease has reached a relatively advanced stage.
Diagnosis of an autoimmune disease typically begins with a careful health history, including
assessment of possible occupational and environmental exposures. Many of the early symptoms
of these disorders, such as fatigue, joint and muscle pain, fever, or weight changes are
nonspecific. While these symptoms alone may not point to a particular autoimmune disease,
when considered in retrospect they can help to pinpoint when the disease process began.
Added diagnostic clues may be revealed through family history, as the presence of autoimmune
disease in a patient’s family further suggests that an autoiinmune disease should be
considered among the diagnostic possibilities. Similarly, a social and occupational history may
identify exposures associated with a particular autoimmune disorder.
Laboratory testing helps to establish the location and extent of disease. Such testing can reveal
the presence of specific autoantibodies, which can be a strong indicator of an autoimmune
disorder. Although laboratory testing has limitations, it is currently the cornerstone of diagnosis.
Some immunologic tests are difficult to interpret, however, and must always be considered
along with clinical findings.
Recent studies suggest that autoantibody detection may be valuable in earlier diagnosis of
autoimmune diseases, thereby allowing treatment to be initiated sooner. Research has shown
that individuals who go on to develop clinical manifestations of type 1 diabetes, for example,
often have had multiple antibodies to the insulin-producing islet cells for some time before
disease is evident. The presence of such antibodies, especially if coupled with a family history
and genetic factors associated with the disease, increases the likelihood that symptoms will
appear in the future. In some instances it may be possible to use antibodies to monitor
response to treatment or to forecast an exacerbation of a disease in remission. However,
because some autoimmune diseases are caused by infiltrating cells rather than autoantibodies,
practical tests for cell-mediated autoimmune reactions are a high priority need.
Imaging technology can also be a valuable diagnostic tool. For example, imaging tests that
reveal areas of demyelinization in the brain (plaques) have been useful for diagnosing and
staging multiple sclerosis and for monitoring responses to therapy. Other specialized imaging
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
36
technologies are of increasing value in following the course of several autoimmune disorders.
The absence of diagnostic standards has hampered efforts of researchers aid clinician to identify
autoimmune diseases at early stages. For a few diseases, including lupus, multiple sclerosis, and
rheumatoid arthritis, professional groups have developed diagnostic criteria. These criteria are
essential for epidemiologic studies, but may not always be valid for clinical diagnosis in
individual cases. Because so many early symptoms of autoimmune disease are relatively non-
specific, years may go by before a definitive diagnosis can be reached and treatment initiated.
These long delays represent a particular hardship for patients, who too often go from one
physician to another seeking a cause of their illness. These problems have stimulated recent
investigations seeking better objective indicators of disease called biomarkers. Often based on a
particular pattern of biochemical and immunologic data linked to a specific disease or disease
risk, biomarkers have the potential to considerably improve our ability to diagnose autoimmune
disorders earlier in the disease process.
Reference: Progress in Autoimmune Diseases Research, National Institutes of Health, The
Autoimmune Disease Coordinating Committee, U.S. Department Of Health And Human Services,
National Institutes of Health, National Institute of Allergy and Infectious Diseases,
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
37
Recent Advances in Diagnosis of Autoimmune Diseases & Role of Biomarkers
Santosh Kumar, Department of Biochemistry, Dolphin (PG.) Institute , Dehradun
The investigation of autoiminunity provides an interest challenge in “omics” research and,
particularly, proteome research, as autoimmunc diseases are common disorders of unsolved
etiology that occur in a wide range of manifestations, in all of which tissues and organs are
attacked by the body’s own immune system. Autoantibodies are a hallmark of many
autoimmune diseases and the presence of autoantibodies is a distinctive and key characteristic
of autoimmune diseases. Conventionally, the study of autoimmune response has always been
conducted by analyzing the presence and/or concentration of individual antibodies in biological
fluids. New proteomic techniques allow the simultaneous identification/measurement of
different autoantibodies in sera of patients suffering from autoimmune diseases. The possibility
of simultaneously measuring a number of correlated analytes appears to be very interesting for
analytical reasons (reduced volumes of biological samples, reagents and low costs),
logistical/managerial reasons, and pathophysiological reasons (combination of markers in
disease-oriented or organ-oriented profiling). While recently collected data demonstrate
satisfactory analytical sensitivity and reproducibility, some issues such as standardization and
data interpretati6n have to be solved before the introduction of these new and promising
techniques into clinical practice.
Biomarkers are physiologic characteristics that indicate the presence of either specific biologic
processes or specific responses to pharmacologic agents. To be useful, a biomarker must be
objectively and reliably measurable. Researchers and clinicians in autoimmune disease
prevention and treatment are investing great effort to identify and validate biomarkers that can
reveal increased disease risk, disease initiation and progression, response to treatment,
environmental influences, and other important information.
Autoimmune disease biomarkers have the potential to enable diagnosis before the onset of
symptoms, predict specific organ involvement and disease flares, identify clinically meaningful
disease subsets, predict and monitor response to therapy, and describe organ or tissue
damage. Biomarkers might also be very useful in preclinical studies to identify genetic
predisposition to disease or environmental triggers, and they may provide early information
about the potential efficacy of experimental agents or mechanisms underlying drug activity.
Biomarkers will also enhance the conduct of clinical trials, because they can serve as surrogate
endpoints that substitute for traditional clinical endpoints and therefore help predict the effect
of a therapeutic intervention. With an adequate arsenal of biomarkers, it will likely become
possible to conduct shorter clinical trials involving fewer patients. Prevention trials in particular,
which tend to be lengthy and expensive, may benefit from the availability of validated
surrogate endpoints.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
38
Biomarker development and validation is complex and many biomarkers are needed, since
those that are iefiuI at oi ag of disease may not be useful at other Stages. Research to date
suggests that some biomarkers may be common to a variety of autoinimune diseases, although
others are disease-specific. Currently, many biomarker candidates have been identified, but
few, if any have been confirmed conclusively enough to enable their routine use in clinical and
epidemiologic studies or patient care.
References:
Mario Plebani, Marina Pittoni, Marilena Celadin, Daniela Bernardi, Monica Maria Mion; “Recent
advances in diagnostic technologies for autoimmune diseases”; Autoimmunity Reviews 8
(2009) 238—243. Progress in Autoimmune Diseases Research, National Institutes of Health, The
Autoimmune Disease Coordinating Committee, U.S. Department Of Health And Human
Services, National Institutes of Health, National Institute of Allergy and Infectious Diseases,
(2005) 54.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April, 2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
39
Prevention of Autoimmune Diseases
Santosh Kumar, Department of Biochemistry, Dolphin (P.G) Institute , Dehradun
Prevention — arresting the autoimmune process at its outset before irreversible tissue injury occurs —
remains the long-range goal of much autoimmune disease research. Yet to effectively develop and
implement prevention strategies, scientists must first be able to identify individuals or populations at risk
for developing an autoimmune disorder. Since about one-third of autoimmune disease risk is inherited, it
will, be important to define the genetic make-up of the most susceptible individuals in order to target
prevention efforts. This effort has been aided by our increasing knowledge of the human genome and the
genes that contribute to autoimmune susceptibility. As with prevention research in other diseases such as
cancer, efforts to learn about a disease in highly affected families often lead to the design of prevention
strategies that are effective in populations with no known genetic vulnerability.
Many autoimmune disorders involve environmental factors, and identifying these is a major focus of
prevention research. Environmental triggers may include infectious agents, normal dietary components
(e.g., celiac disease symptoms can be avoided by eliminating gluten in the diet), supplements and food
contaminants such as mercury, or occupational or other environmental exposures. As we learn more about
environmental influences in autoimmune disease, it may be possible to prevent the onset of disease even
in the most vulnerable individuals. For example, identifying those at high risk for type 1 diabetes depends
on a combination of genetic factors and the appearance of islet autoantibodies. The presence of these
autoantibodies precedes clinical symptoms, but is a strong indicator of relatively rapid progression to
frank diabetes.
The third essential step in a prevention program is to develop preventive interventions that can be safely
and ethically implemented before disease is evident. Such measures, when they become available, can be
coupled with public screening programs designed to identify individuals at risk.
Reference: Progress in Autoimmune Diseases Research, National Institutes of Health, The Autoimmune
Disease Coordinating Committee, U.S. Department Of Health And Human Services, National Institutes
of Health, National Institute of Allergy and Infectious Diseases, (2005) 56-57.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April, 2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
40
Vaccine to Autoimmune disorders : Safe or Harmful
Ashwani Sanghi, Department of Biochemistry, Dolphin (P.G) Institute, Dehradun
Some research suggests that vaccines are safe, effective, and do not increase the risk of
autoimmune disorders. Various researches are going on about that they are safe for the general
public or have a different effect on people who are already genetically inclined to develop
autoimmune disorders.
“Autoimmune diseases generally involve difficulties with the immune system turning itself off,
so any stimulation of the immune system can sometimes lead to a flare of disease. Vaccines
may cause transient flares of disease in some patients,” says immunologist Julian Ambrus,
MD, an associate professor of medicine at Buffalo General Hospital in New York.
The increasing prevalence of autoimmune disorders occurring over a period in which there has
been an increase in the use of vaccines has led to various assumptions in linking specific
vaccines to specific autoimmune disorders. A symptom of autoimmune disorder occasionally
occurs soon after a vaccination, which can lead to the perception that the both are linked like
Hepatitis B vaccine increases risk of multiple sclerosis, influenza vaccine increases risk of
Guillain-Barré syndrome and use of many more pediatric vaccines has caused an increased risk
of type 1 diabetes.
There are several other ways in which a vaccine could theoretically cause an autoimmune
disorder. An ingredient in the vaccine or its chemical structure or body’s immune response
may trigger the autoimmune disorder. “There is no evidence that vaccines cause autoimmune
disorders,” says Dr. Arnbrus.
One of the challenges in researching this controversy is dividing the people involved into
meaningful smaller groups based on risk. Overall, the data suggests that there is no increased
risk of developing an autoimmune disorder as a result of vaccination, but whether that is true
for very small groups of vulnerable people is not yet fully understood.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
41
Treatment of Autoimmune Diseases
Santosh Kumar, Department of Biochemistry, Dolphin (P.G) Institute , Dehradun
Treatments to reduce the symptoms of most autoimmune diseases are available, but definitive
cures have yet to be developed. In general, two approaches to treatment are currently
available. The first involves replacing or repairing impaired function. For example, patients with
type 1 diabetes mellitus can take insulin to replace the hormone that is not produced by their
damaged pancreatic islet cells. Similarly, patients with autoimmune thyroiditis can be treated
with thyroid hormones. These methods do not arrest the autoimmune process, although the
patient may undergo remission while receiving symptom based treatment. In most cases,
however, the patient must depend on replacement therapy throughout his or her lifetime.
Sometimes a damaged organ can be replaced by transplantation. For example, scientists are
now testing the effectiveness of islet cell transplant as a treatment for diabetes. Patients with
end-stage renal disease or dilated cardiomyopathy may be candidates for a kidney or heart
transplant. In the future, stem cell therapies might allow replacement or repair of damaged
organs. Replacement therapy is most likely to be successful if the impaired function is localized
to a single organ system.
The second treatment approach centers on suppressing the destructive autoimmune response.
Systemic autoimmune diseases often require general suppression of the immune response.
Immunosuppressive drugs reduce the overall immune response and thereby ameliorate the
manifestations of the disease. However, because these drugs also reduce the individual’s
resistance to infection, they must be used with great caution. In addition, they often have
adverse side effects. Such treatments are most often used in debilitating diseases such as lupus
and rheumatoid arthritis.
Much effort has been devoted in recent years to developing more focused therapies than
global immunosuppression, most of which target a specific step in the tissue-damaging
inflammatory response. A number of promising new biologic agents that produce more
targeted immunosuppression are already in advanced clinical trials. They include monoclonal
antibodies that decrease T cells or B cells specifically, act on only activated T cells, inhibit
particular cytokine mediators of inflammation, or block the recruitment and localization of
lymphocytes to the target organ. Although these targeted approaches usually have fewer side
effects, they may increase the patient’s vulnerability to infection, and therefore also must be
used with caution. Moreover, a therapy that benefits one autoimmune disease will sometimes
make another disorder worse.
An even more refined treatment approach is to arrest the harmful autoimmune response —
usually at the point of lymphocyte recognition — without dampening the immune response
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
42
overall. This approach usually involves identifying the precise antigen responsible for initiating
the pathogenic autoimmune response, and blocking it at the point of lymphocyte recognition.
While successful in animal studies, this approach has thus far been problematic in humans. By
the time most patients are treated, their disease has usually advanced to a point where the
immune response has encompassed multiple epitopes on the same antigen or even other
molecules of the affected organ. Blocking a single epitope at this stage is unlikely to be
effective. Earlier diagnosis, however, would make this treatment approach more feasible in
humans.
Researchers are using our growing knowledge of the biology of immune response to develop
innovative new intervention strategies. These include bone marrow transplantation and
strategies to enhance a naturally-occurring regulatory mechanism (e.g., shifting immune
response from a damaging T cell subpopulation to a less injurious one, or increasing the
number of regulatory cells produced by the thymus). Other interventions may include new
therapies and counseling about avoiding exacerbating factors (e.g., certain infections,
environmental agents).
Reference: Progress in Autoimmune Diseases Research, National institutes of Health, The
Autoimmune Disease Coordinating Committee, U.S. Department Of Health And Human
Services, National Institutes of Health, National Institute of Allergy and Infectious Diseases,
(2005) 55-56.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015

Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
43
Advances in the Treatment of Myasthenia Gravis
Rashmi chouhan, Department of Pathology, Dolphin Institute , Dehradun.
Myasthenia gravis (MG) should be classified according to antibody status (acetyicholine, MuSK, LRP4,
titin), thymus (hyperplasia, neoplasia, atrophy), age at debut (< or >50 years), symptom localization
(generalized, ocular) and severity. With optimal treatment, the prognosis is good in terms of daily
functions, quality of life and survival. Symptomatic treatment with acetylcholine esterase is usually
combined with immunosuppression. A combination of prednisolone and azathioprine remains the first
choice alternative, whereas rituximab is a promising second choice drug for severe generalized MG.
Thymectomy is recommended for early-onset, generalized MG and for thymoma MG. In acute
exacerbations including MG crisis, intravenous immunoglobulin and plasma exchange have good and
similar effects. MG in young females needs therapeutic considerations regarding potential pregnancy.
CME WORKSHOP ON AUTOIMMUNITY & AUTOIMMUNE DISEASES, 10th -11th April,2015
Organized by: DIBNS, Dehradun & Indian Immunology Society, New Delhi
44