slide fibrous displasia
DESCRIPTION
fibrous displasiaTRANSCRIPT
CASE REPORT
FIBROUS DYSPLASIA OF SINONASAL ON CHILD
Hanski R.P Legrans
Scientific Supervisor
Dr. I Gde Ardika Nuaba,Sp.THT-KL(K) 1

INTRODUCTION
First described by Lichtenstein in1938
Characterized by progressive replacement of normal bone elements by fibrous tissue
Even benignpotential to cause functional & cosmetical damagecraniofacial bones
Most common site:Maxilla,mandible, frontal,sphenoid, & temporal bone
2
INTRODUCTION
The etiology is unknown, but is associated with mutations in the Gsα gene located on chromosome 20q13.2-13.3
First identified in patients with the syndrome McCune - Albright, but later occured in one form of fibrous dysplasia which are monostotic or polyostotic
3

INTRODUCTION
4
Clinical Features
Depends on the size, duration and extension of the natural
course of the disease.
Localized swelling and mild with or without pain until the derformity occured with complications such as proptosis, visual
disturbances, and sensorineural deafness
INTRODUCTION
5
• History,clinical examination,radiology, histopathology
Diagnosis
• Surgery:place & location,growth rate,aesthetic,function impairment,surgeon skill
• Medical: role of steroid & biphosponate
Management
INTRODUCTION
6
Reported a case of fibrous dysplasia of the
sinonasal on a child which performed tumour
resection with lateral rhinotomy approaching
LITERATURE REVIEW
7
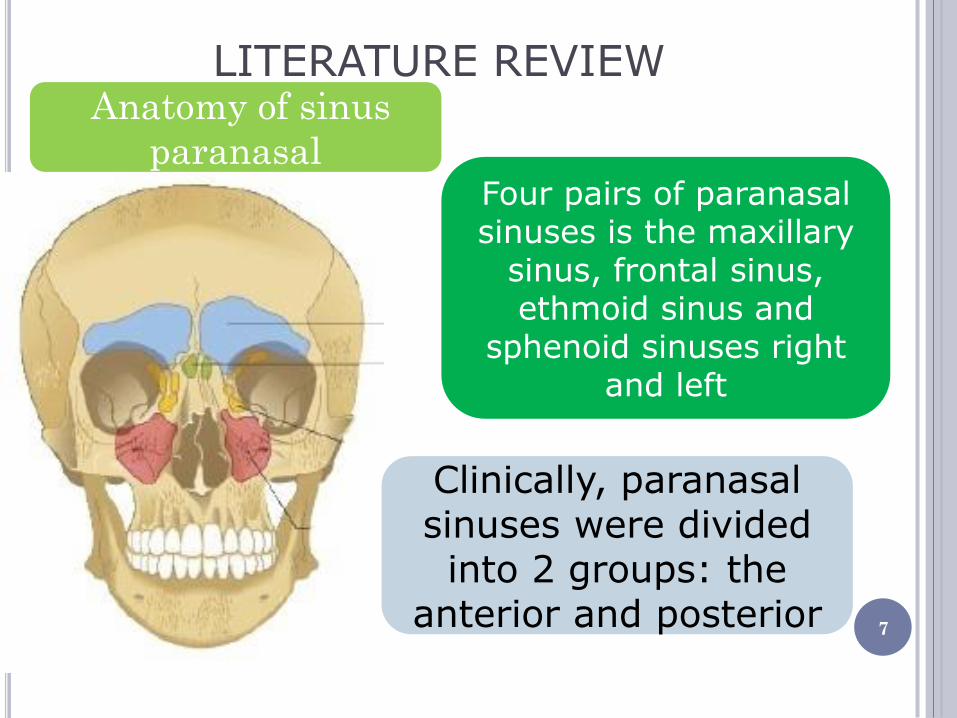
Anatomy of sinus
paranasal Four pairs of paranasal sinuses is the maxillary
sinus, frontal sinus, ethmoid sinus and
sphenoid sinuses right and left
Clinically, paranasal sinuses were divided into 2 groups: the
anterior and posterior

LITERATURE REVIEW Maxillary sinus:Largest sinus, irregular inverted
pyramid,ostium is placed on superior of maxillary sinus wall
Frontal Sinus:Located in os frontal,insulated and notched in the edge
Ethmoid Sinus: based on locationetmoid
anterior & posterior Pyramid shaped with basic on posterior
Sphenoid sinus:Located in os sphenoid,In developmentblood vessels & nerves are very
close to the cavity
8
EPIDEMIOLOGY
9
Certain prevalence is
unknown
Equal between male
& female
Younger age often in male than female
Jaw: often in maxilla than
mandible
can occur on femur, skull &
costae
ETIOLOGY
10
Unclear etiology but associated with mutation of gene GNAS I coding the
subunit α from Gs-α
Increased the production c-AMP affect proliferation & differentiation osteoblast
First identification on Mc Cune-Albright syndromeone form of fibrous dysplasia(polyostotic monoostotic)

PATHOGENESIS
11
Bone formation (endochondral & intramembran)
Long bones (endochondral)
Flat bones (intramembran)
Blood vesselcental
bone (absorption of
cartilage & bone
formation)
condensation of mesechymal cell
in stroma fibrousosteoblat immatureextrac
ellular matrix
PATHOGENESIS
12
FIBROUS
DYSPLASIA
Mutation after zygotic,the
bond of membrane to G-
protein coupled receptor
abnormal osteoblast
differentation abnormal
bone(immature)
Increasing IL-6activation
of osteoclastextent of
lession
CLINICAL FEATURES
13
Can be mild to severe
Local swelling with/without pain,
asymetrical face,deformity
Blocking nose, skin lession(café
au lait)
CHLEAC constriction
SNHLobstrucion of inner ear
structure,otic capsule & IAC
CLINICAL FEATURES
Clinical symptomslocation, onset,
expansion & the course of the disease
Each sinus has its own clinical symptoms
Ethmoid & sphenoid sinuseyeball
displacement, decreased of visual due to compression of fibrous dysplasia in optic nerve
Maxilla sinusfullness & swelling to the cheeks & oral cavity
14

DIAGNOSIS
15
Diagnosis estabilished:
history, physical
examination,
radiology,histopathology
A
B A. Homogenous Lession B. Ground Glass
Appearence
DIAGNOSIS
16
A
CT-Scan
Better to asses tumor
expansion
Not enough to estabilsh diagnosis
Ground glass 56%,
homogenous lession 23%, cystic pattern
21%
Radiology
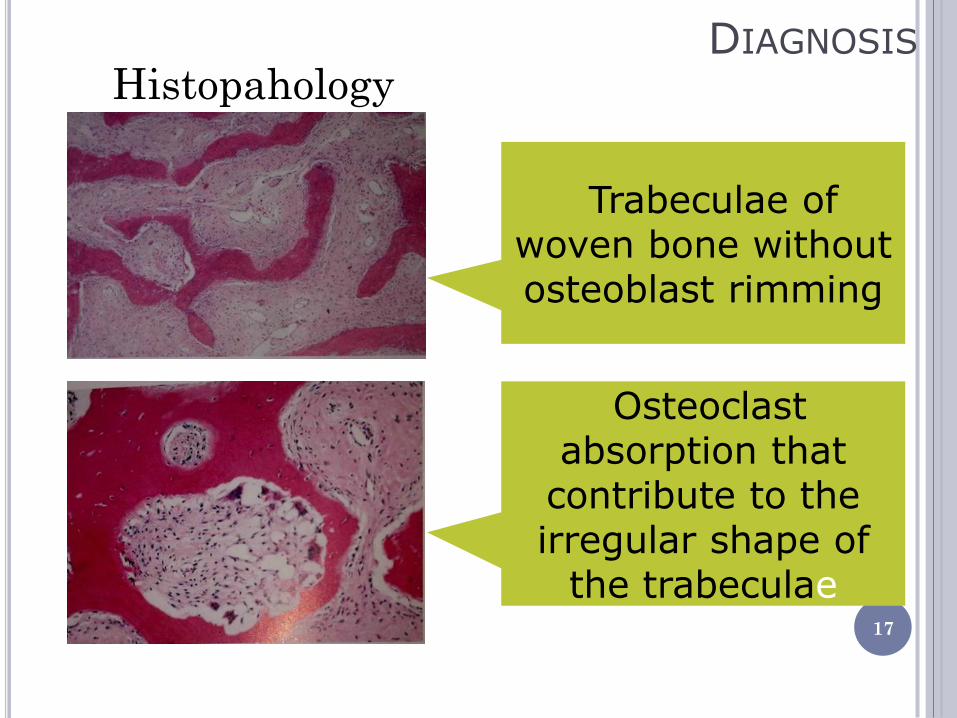
DIAGNOSIS
17
A Histopahology
Trabeculae of woven bone without osteoblast rimming
Osteoclast absorption that
contribute to the irregular shape of
the trabeculae
DIFFERENTIAL DIAGNOSIS
Fibrous osseus, Paget’s dissease, aneurismal osseus cyst, cystic Cristeller syndrome, amelobastoma, osteochondroma hypothyroid, malicnancy such as sarcoma, osteoblast metastatic lession
18
MANAGEMENT
19
Surgery & Medication
Surgery
invoving area,tumor growth rate, aesthetic, functional impairment, patient condition,skill
& multidiciplin availbility
Surgical Approaching: lateral rhinotomy, midfacial degloving
Medication
•Steroiddecompression •Biphosponate inhibits
osteoclast activity

PROGNOSIS
20
Better though poor outcome on younger patient or polyostotic
form
Frame time diagnosis to malignancy is 13,5
years
Risk of the pateint who didn’t receive
therapy: 0,4%
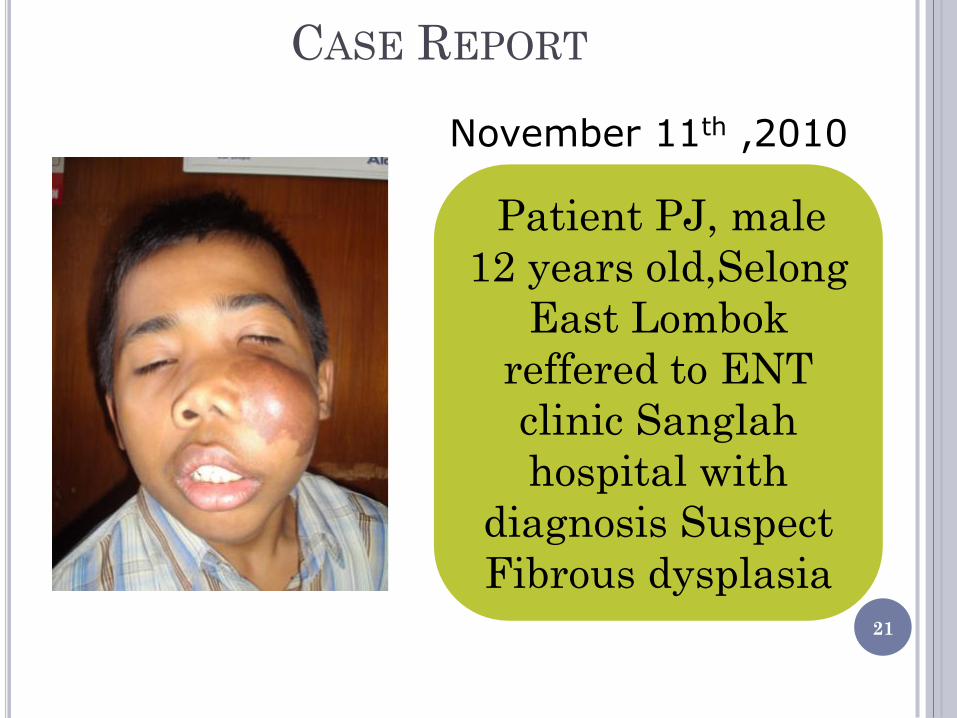
CASE REPORT
21
November 11th ,2010
Patient PJ, male
12 years old,Selong
East Lombok
reffered to ENT
clinic Sanglah
hospital with
diagnosis Suspect
Fibrous dysplasia

CASE REPORT
22
Chief Complaint
Lump in left cheek since 5 years ago
History of disease
Initially small and growing, sometimes
accompanied by pain. In addition nasal
congestion complaint on left nose, sometimes with discharge mixed with blood. No lumps elsewhere,no vision
complaint

CASE REPORT
23
Patient went to Mataram hospital on October 28th ,2010 and performed CT-scanlytic
lession resemble of ground glass,can be a fibrous dysplasia

CASE REPORT
24
Physical examination
Compos mentis, vital
sign within normal limit
ENT examination: a Lump on left cheek with size
15cm x 10cm,skin lession café au lait,deformity,
tumor on left nasal cavity,with mucoid
discharge
CASE REPORT
25
Working diagnosis:
susp.fibrous dyplasia
Planned for left lateral rhinotomy
Thorax Rontgen, blood test & hemostasis
function
November 13th ,2010
pediatrician & anestesiology
Scheduled for resection with rhinotomy lateral approaching on
Novenber 22nd ,2010
CASE REPORT
26
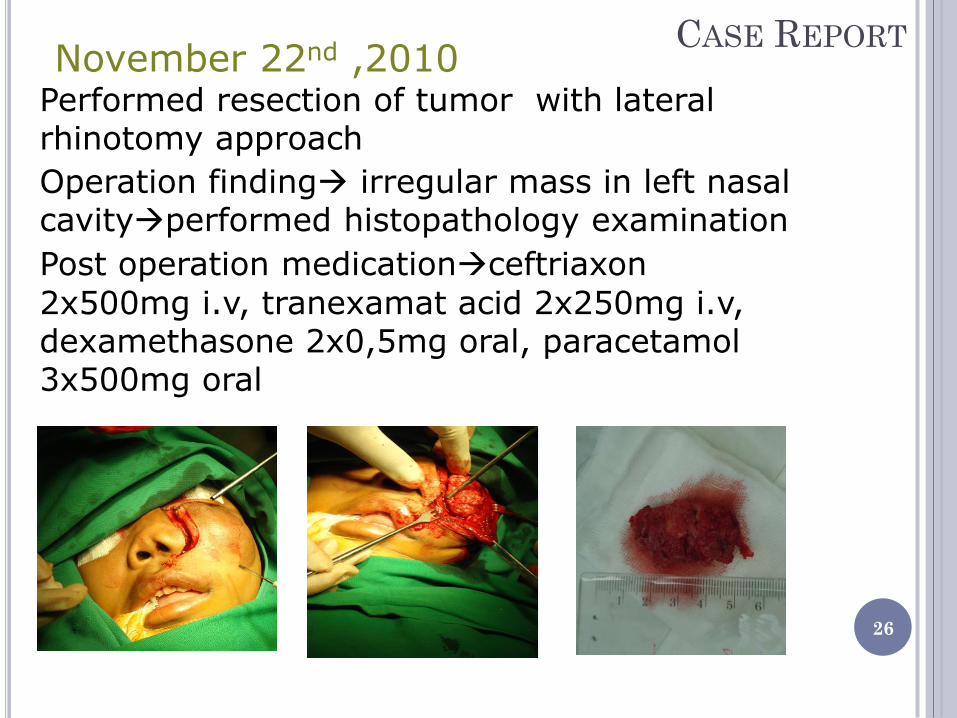
November 22nd ,2010 Performed resection of tumor with lateral rhinotomy approach
Operation finding irregular mass in left nasal cavityperformed histopathology examination
Post operation medicationceftriaxon
2x500mg i.v, tranexamat acid 2x250mg i.v, dexamethasone 2x0,5mg oral, paracetamol 3x500mg oral
CASE REPORT
27
1st day:November 23rd 2010
No complaint, swelling on left cheek, packing on left nasal cavity, no active bleeding on posterior wall of pharyng
Incision wound care
Continuing medication theraphy
2nd day:November 24th 2010
No complaint, swelling on the left cheek, remove the anterior & sinus packing, no active bleeding
Patient discharged with medication cefadroxil 2x500mg oral, paracetamol 3x500mg,& dexamethasone 3x05mg
Post Operation Follow Up
CASE REPORT
28
Post Operation Follow Up
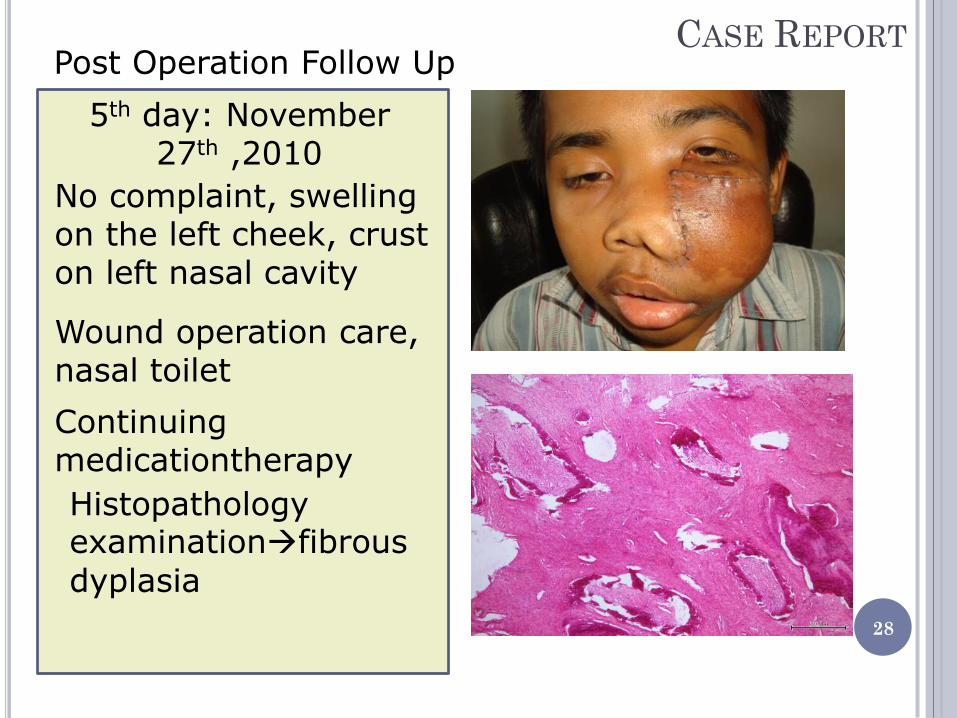
5th day: November 27th ,2010
No complaint, swelling on the left cheek, crust on left nasal cavity
Wound operation care, nasal toilet
Continuing medicationtherapy
Histopathology examinationfibrous
dyplasia

CASE REPORT
29
Post Operation Follow Up
7th Day: November 29th 2010
No complaint, swelling on left
cheek, no discharge & crust
Suture removal & wound care
Follow up within 6 monthsCT-
scan
DISCUSSION
Fibrous dysplasia
Progressive replacement of normal bone elements by fibrous tissue
Benign but potentially cause functional damage
Monostotic lession & polyostotic lession
Unknown etiology, but related to the Gsα gen
mutation located on chromosom 20q13.2-13.3 30

DISCUSSION
31
Literature
Case
Ratio of gender equal Younger age male Cholakova et al
range of age 5-67 year old
Male 12 years old
Monostotic>polyostotic Most common site of monostotic fibrous dysplasia(Lee et al):regio zygoma-maxilla
Fibrous dyplasia type monostotic On Sinus maxillaris

DISCUSSION
32
Literature
Case
Clinical symptoms: deformity, asymetrical face, pain, nasal obstruction, skin lession café au lait
Patient complaint of sweeling on left cheek which since 5 years ago, pain(+), nasal obstruction(+), mucoid disharge mixed with blood Examination:asymetrical face, deformity, café au lait,tumor fullfil the left nasal cavity, mucoid discharge

DISCUSSION
33
Diagnosis of fibrous dyplasia
Lee et al
Anamnesis & clinical
examinationto determine
whether it is monostotic or polyostotic
Chan et al
Difficult to estabilished the diagnosis solely based on
anamnesis or physical examination or radiology
Tsai et al
Usually asymptomatic until the tumor compress the
adjacent structure & presents symptoms such
pain & proptosis
DISCUSSION
34
Literature
Case
Histopathology: fibrous tissue with spindle cell shape & do not mature, the presence of trabecular-isolated trabeculae of woven bone without rimming osteoblasts
proliferation of benign fibroblast, monotonous spindle core, fine chromatin, extensive eosinophilic cytoplasm forming files, immersed in a collagen matrix. Among fibrous tissue appeared the lamellar bones & calcification without osteoblast rimming

DISCUSSION
35
Literature
Case
CT-scan: 3 variations description: ground glass (56%), homogenous (23%) and cyctic (21%)
CT-scan: tumor mass with ground glass appearence on the left maxillary sinus pushes the septum to the right
Management:Surgery (lateral rhinotomy, midfacial degloving, FESS) & medication(biphosponate,NSAID & steroid)
Surgery: rhinotomy lateralis Medication:corticosteroid(dexamethasone 2x0,5mg)
DISCUSSION
36
Literature
Case
Hullar & Lustig: regular control for patients who underwent surgery DiCaprio & Enneking: CT-scan prefeably every 6 months to determine the reccurence
Patient was advised for follow up on the next 6 month to performed CT-Scan

CONCLUSION
37
Reported a case of fibrous dysplasia on the left sinonasal
which performed tumor resection with lateral rhinotomy approach
•Replacement of the normal bone elements with fibrous tissue •Unknown etiology,often associated with mutation gene •Variety of clinical symptoms •Diagnosis esatbilished: anamnesis, physical examination, supporting examination(CT-Scan) •Management: Surgery & medication