skin tumors
TRANSCRIPT
Skin tumors
Seborrhoeic keratosis (basal cell papilloma, seborrhoeic wart)
• This is a common benign epidermal tumour, unrelated to sebaceous glands.
CauseUsually unexplained but:• multiple lesions may be inherited (autosomal
dominant)• occasionally follow an inflammatory dermatosis• very rarely, the sudden eruption of hundreds of
itchy lesions is associated with an internal neoplasm (Leser–Trélat sign).
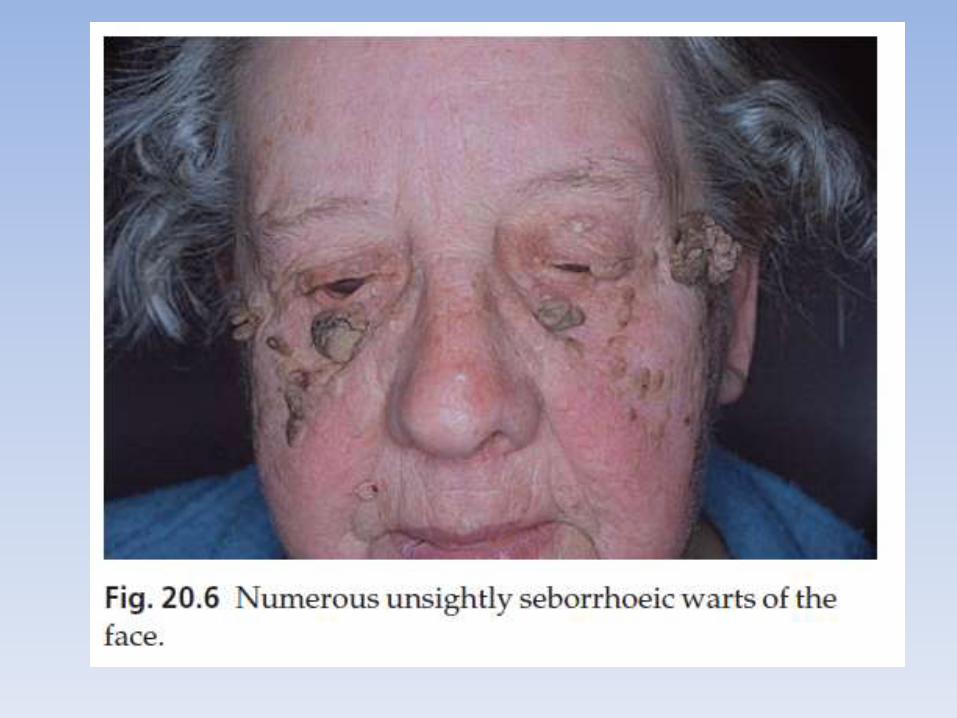
Presentation• usually arise after the age of 50 years, but flat
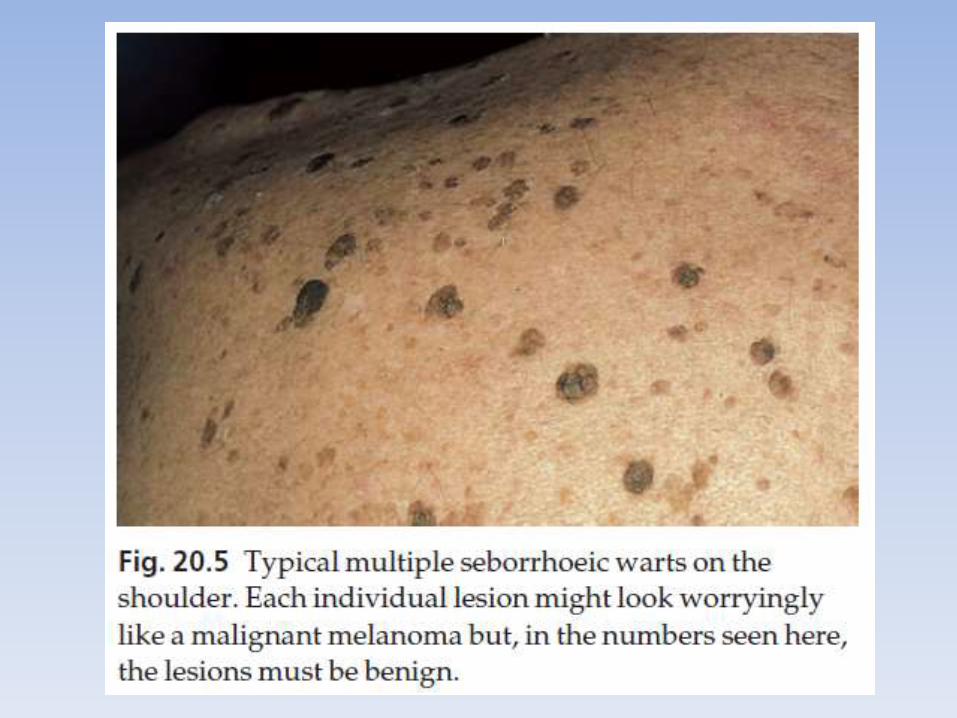
inconspicuous lesions are often visible earlier. • They are often multiple but may be single. • Lesions are most common on the face and trunk. Physical signs• A distinctive ‘stuck-on’ appearance due to ‘tucked under’
shoulders, as chewed chewing gum might appear.• May be flat, raised, filiform or pedunculated.• Surface may be smooth or verrucous.• Colour varies from yellow–white to dark brown–black.• Surface may have greasy scaling and scattered keratin plugs
(‘currant bun’ appearance).• If oval, long axis parallels skin lines.
Clinical course
• benign.
Differential diagnosis
• a pigmented basal cell carcinoma
• a malignant melanoma.
Treatment
• Seborrhoeic keratoses can safely be left alone, but ugly or easily traumatized ones can be removed with a curette under local anaesthetic (this has the advantage of providing histology)
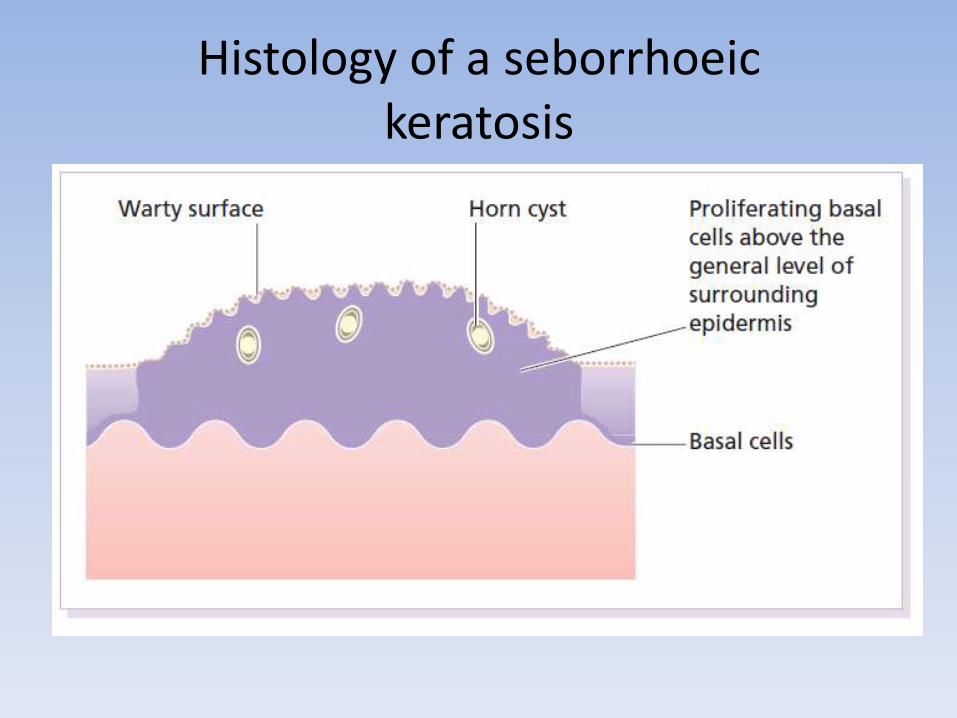
Histology of a seborrhoeickeratosis
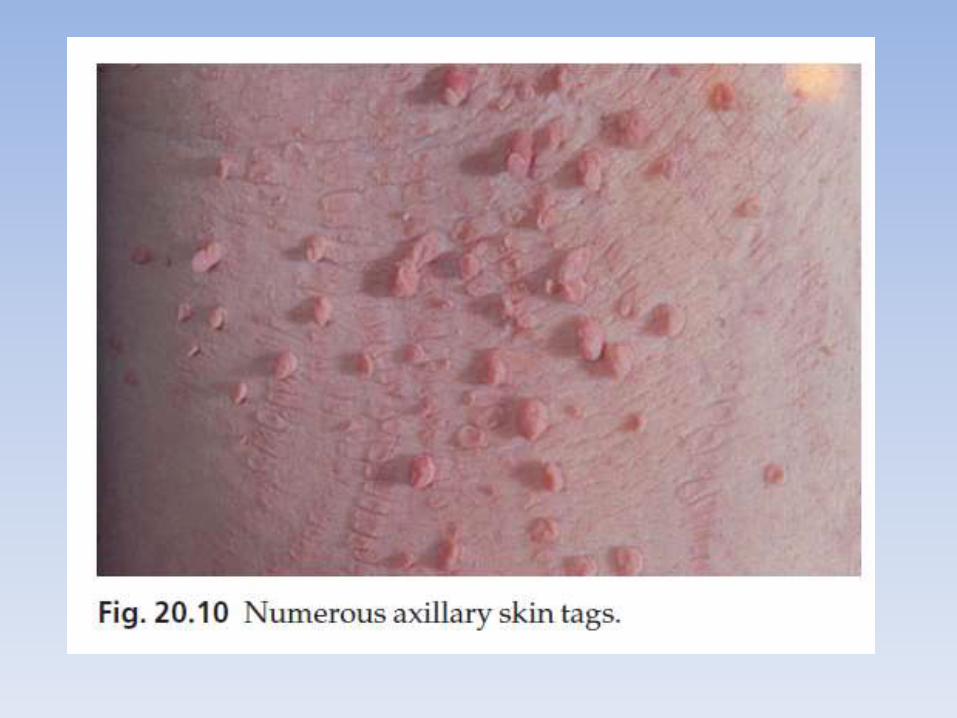
Skin tags (acrochordon)
• These common benign outgrowths of skin affect mainly the middle-aged and elderly.
Cause• Unknown, sometimes familial.• Skin tags are most common in obese women, and rarely are
associated with tuberous sclerosis, acanthosis nigricans or acromegaly, and diabetes.
Presentation• Skin tags occur around the neck and within the major flexures. • They are soft skin-coloured or pigmented pedunculated papules.Treatment• Small lesions can be snipped off with fine scissors, frozen with liquid
nitrogen or destroyed with a hyfrecator without local anaesthesia. • There is no way of preventing new ones from developing.
Epidermoid and pilar cysts
• Often incorrectly called ‘sebaceous cysts’
• these are common and can occur on the scalp, face, behind the ears and on the trunk.
• They often have a central punctum
• when they rupture or are squeezed, foulsmellingcheesy material comes out
• Treatment is by excision, or by incision followed by expression of the contents and removal of the cyst wall.
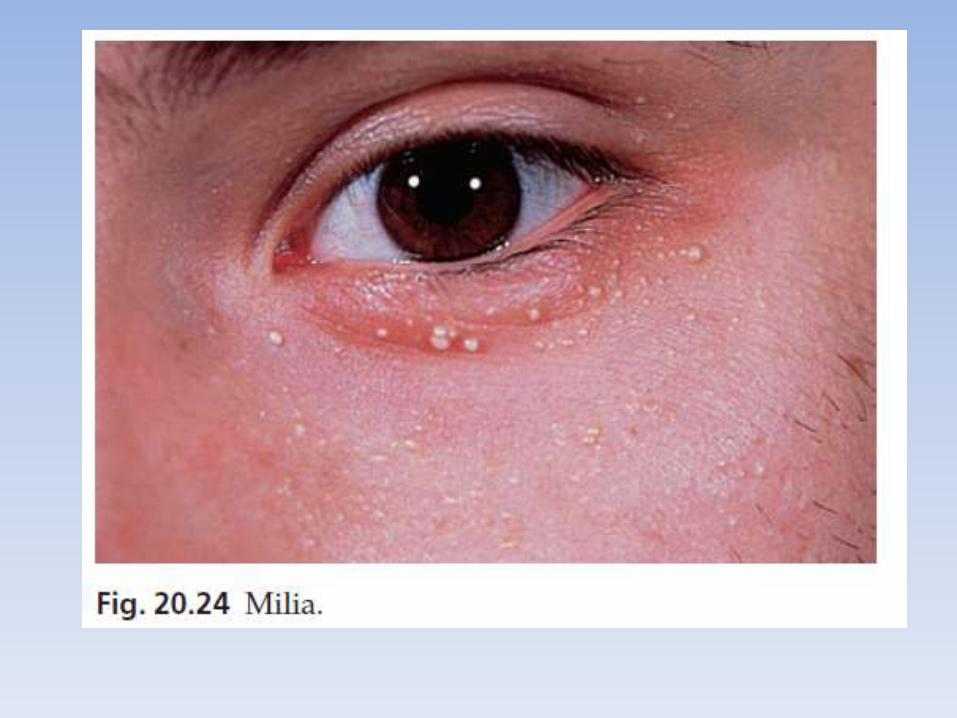
Milia
• Milia are small subepidermal keratin cysts • They are common on the face in all age groups
and appear as tiny white millet seed-like papules of 0.5–2 mm in diameter.
• They are occasionally seen at the site of a previous subepidermal blister (e.g. in epidermolysis bullosa and porphyria cutaneatarda).
• The contents of milia can be picked out with a sterile needle or pointed scalpel blade without local anaesthesia.
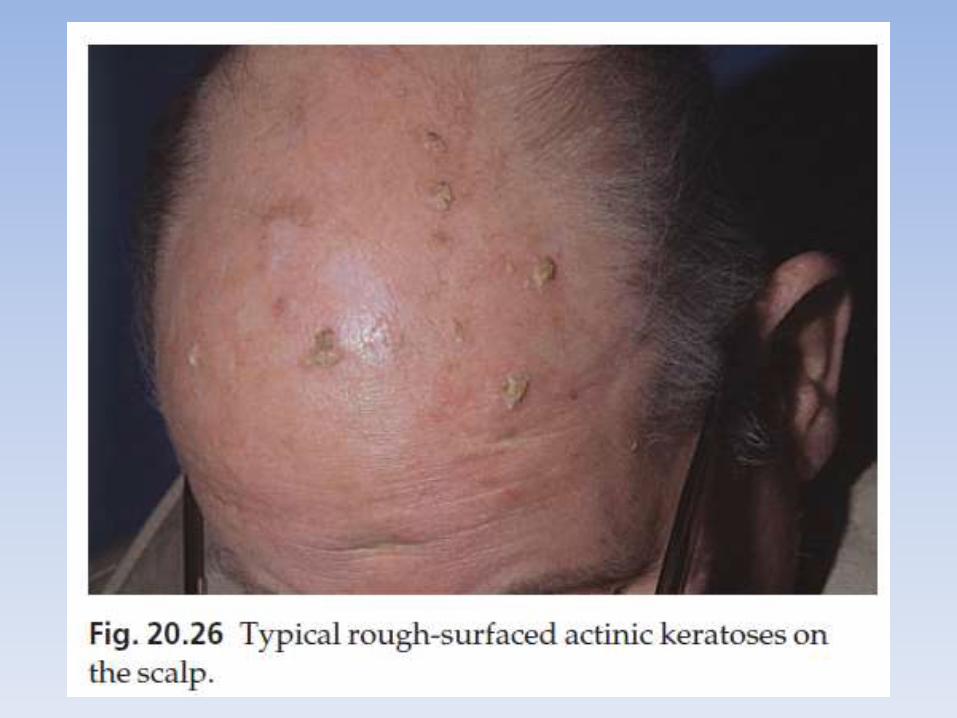
Actinic keratoses
• Is discrete rough-surfaced lesions crop up on sun-damaged skin.
• premalignant• Pathologically there is a case for classifying them as
squamous cell carcinomas in situ but very few progress to invasive squamous cell carcinomas.
Cause• The effects of sun exposure are cumulative. • Those with fair complexions living near the equator are
most at risk• Melanin protects, and actinic keratoses are not seen in
black skin. Conversely, albinos are especially prone to develop them.
Presentation
• They affect the middle-aged and elderly in temperate climates, but younger people in the tropics.
• The pink or grey rough scaling macules or papules seldom exceed 1 cm in diameter
• Their rough surface is sometimes better felt than seen.
Complications
• Transition to an invasive squamous cell carcinoma, although rare, should be suspected if a lesion enlarges, becomes nodular, ulcerates or bleeds. Luckily, such tumours seldom metastasize.
Differential diagnosis
• seborrhoeic wart
• viral wart
• a keratoacanthoma
• an intra-epidermal carcinoma or an invasive squamous cell carcinoma.
Investigations
• A biopsy is needed if there is concern over invasive change.
Treatment
• Freezing with liquid nitrogen or carbon dioxide snow
• Shave removal or curettage is best for large lesions and cutaneous horns.
• Multiple lesions, including subclinical ones, can be treated with 5-fluorouracil cream
• Healing is rapid
• 3% Sodium diclofenac
• Photo-dynamic therapy
Malignant skin tumors
Basal cell carcinoma (rodent ulcer)
• the most common form of skin cancer. • most commonly on the faces of the middle aged or elderly. • Lesions invade locally but, for practical purposes, never
metastasize.Cause• Prolonged sun exposure is the main factor so these
tumours are most common in white people who have lived in sunny areas, high latitudes, or near the equator.
• occur in scars caused by X-rays, vaccination or trauma. • Photosensitizing pitch, tar and oils can act as cocarcinogens
with ultraviolet radiation. • Arsenic predisposes to multiple basal cell carcinomas
Presentation
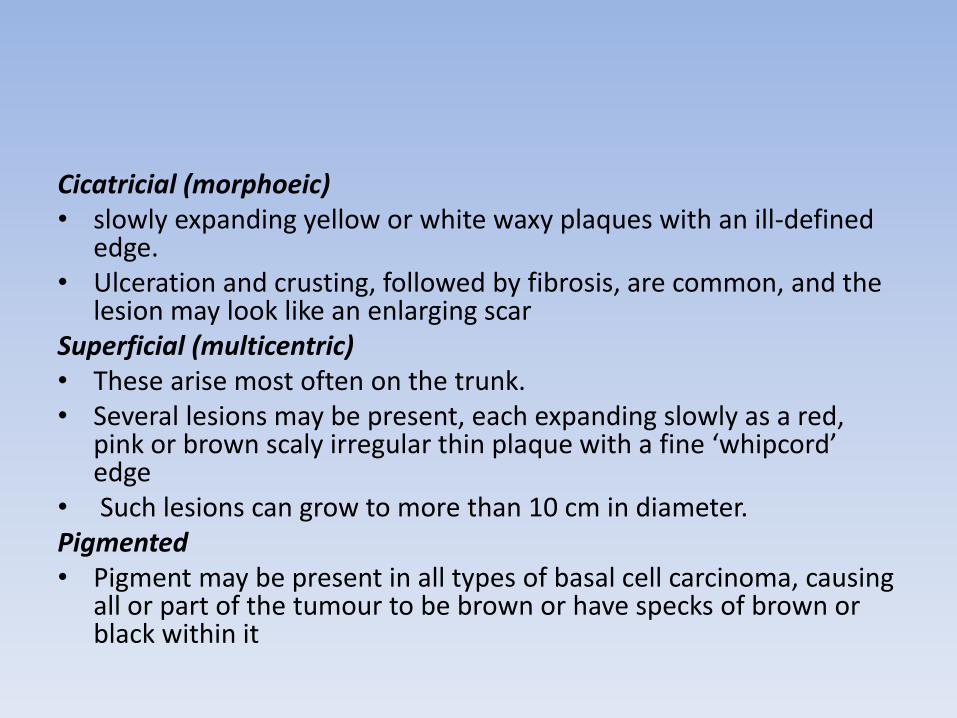
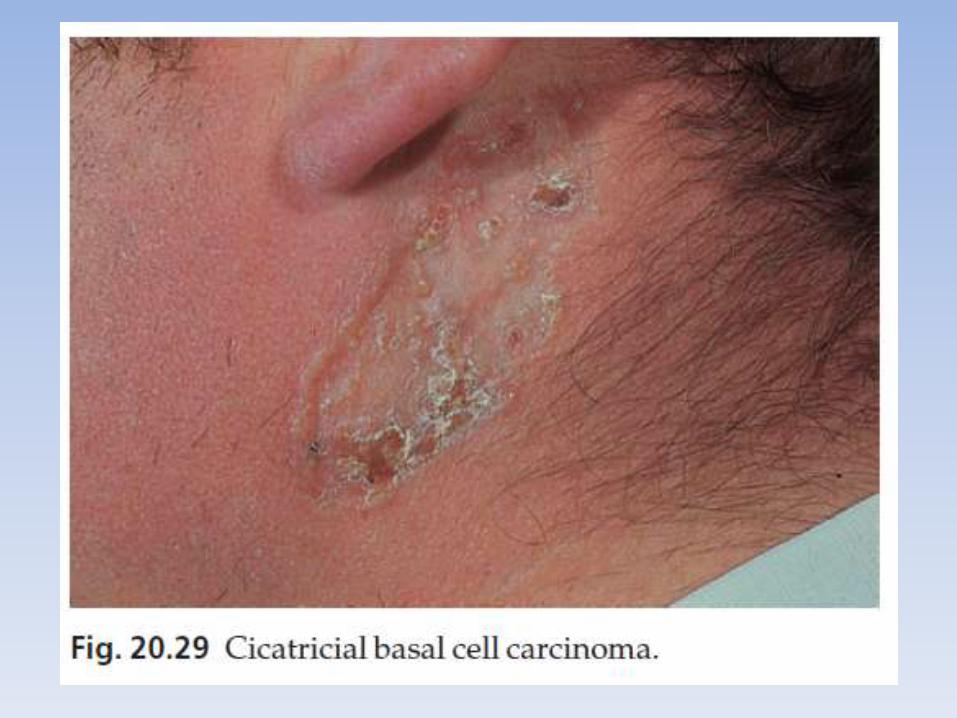
Nodulo-ulcerative • This is the most common type. • An early lesion is a small glistening translucent, sometimes
umbilicated, skin-coloured papule that slowly enlarges. • Central necrosis, although not invariable, leaves an ulcer with an
adherent crust and a rolled pearly edge• Coarse telangiectatic vessels often run across the tumour’s surface• Without treatment such lesions may reach 1–2 cm in diameter in 5–
10 yearsCystic • The lesion is at first like the nodular type, but later cystic changes
predominate and the nodule becomes tense and more translucent, with marked telangiectasia.
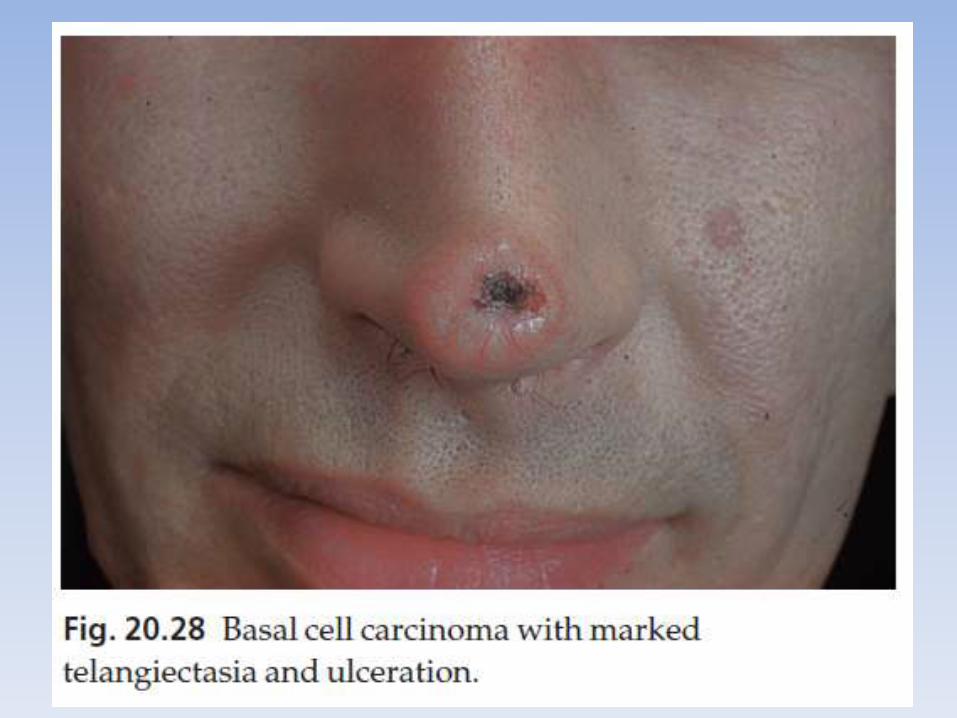
Cicatricial (morphoeic) • slowly expanding yellow or white waxy plaques with an ill-defined
edge. • Ulceration and crusting, followed by fibrosis, are common, and the
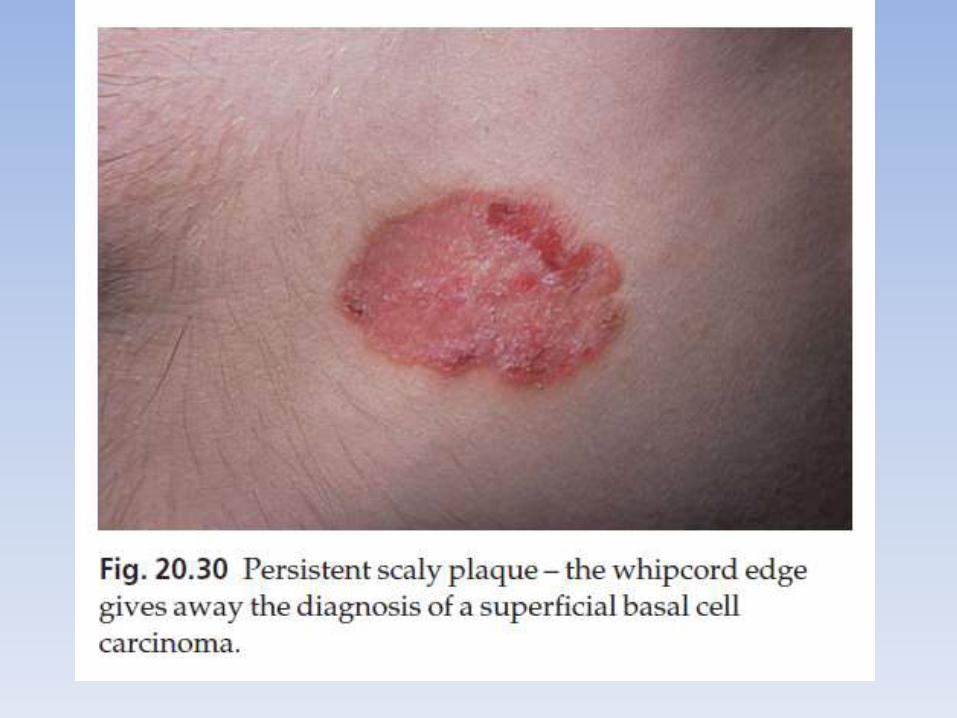
lesion may look like an enlarging scar Superficial (multicentric) • These arise most often on the trunk. • Several lesions may be present, each expanding slowly as a red,
pink or brown scaly irregular thin plaque with a fine ‘whipcord’ edge
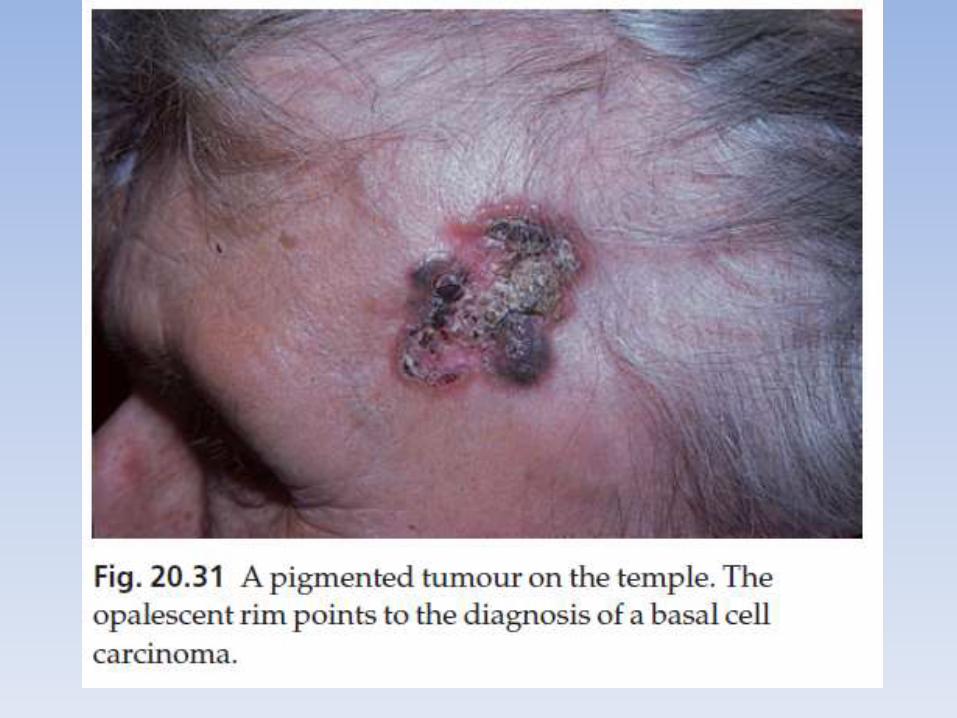
• Such lesions can grow to more than 10 cm in diameter.Pigmented • Pigment may be present in all types of basal cell carcinoma, causing
all or part of the tumour to be brown or have specks of brown or black within it
Clinical course
• The slow but relentless growth destroys tissue locally, invading underlying cartilage or bone or damage important structures such as the tear ducts.
Histology
• Small, darkly blue staining basal cells grow in well-defined aggregates which invade the dermis
• The outer layer of cells is arranged in a palisade.
• Numerous mitoses and apoptotic bodies are seen.
• In the cicatricial type, the islands of tumourare surrounded by fibrous tissue.
Differential diagnosis
• A nodular basal cell carcinoma may be confused with 1. an intradermal melanocytic naevus2. a squamous cell carcinoma 3. a giant molluscum contagiosum4. a traumatized benign papule 5. a keratoacanthomatous squamous cell carcinoma. • Pigmented basal cell carcinomas should be distinguished from
seborrhoeic warts and malignant melanomas. • A cicatricial basal cell carcinoma may mimic morphoea or a scar. • A superficial basal cell carcinoma may be confused with an intra-
epidermal carcinoma, with psoriasis or with nummular eczema
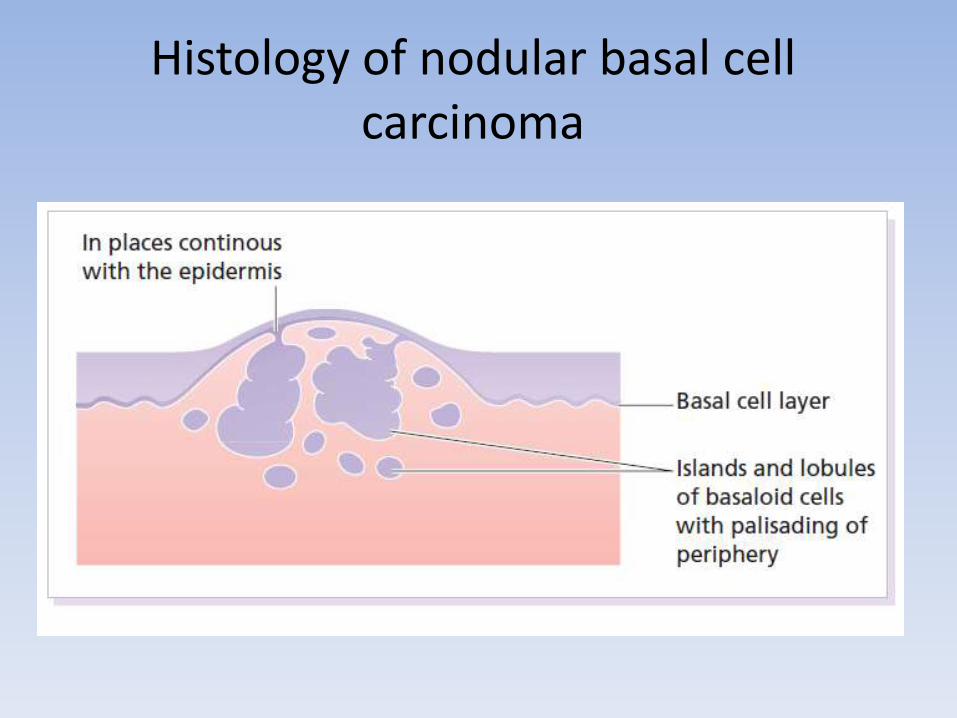
Histology of nodular basal cell carcinoma
Treatment
• There is no single treatment of choice for all basal cell carcinomas. • Treatment should be tailored to the type of tumour, its site and the
age and general health of the patient. • Excision, with 0.5 cm of surrounding normal skin, is the treatment
of choice for discrete nodular and cystic tumours in patients under 60 years.
• Mohs’ micrographic surgery is highly effective and becoming the treatment of choice for large (greater than 1 cm) tumours, and for tumours on cosmetically important sites such as the nose, and for tumours in certain anatomical areas such as the inner canthus or the nasolabial folds.
• Radiotherapy is helpful when surgery is contraindicated.• Cryotherapy, curettage and cautery and photodynamic therapy • The 5-year cure rate for all types of basal cell carcinoma is over 95%
but regular follow-up is advisable to detect local recurrences when they are small and remediable.
Squamous cell carcinoma
• This is a common tumor Cause• These tumors often arise in skin damaged by ultraviolet
radiation and also by X-rays and chronic inflammation. • ultraviolet-induced mutations in the p53 tumour
suppressor gene plays in the development of this cancer.
• Tar, mineral oils and inorganic arsenic• xeroderma pigmentosum, lead to multiple squamous
and basal cell carcinomas, and to malignant melanoma.• human papilloma virus
Presentation and course
• Tumours may arise as thickenings in an actinic keratosis or, de novo small scaling nodules
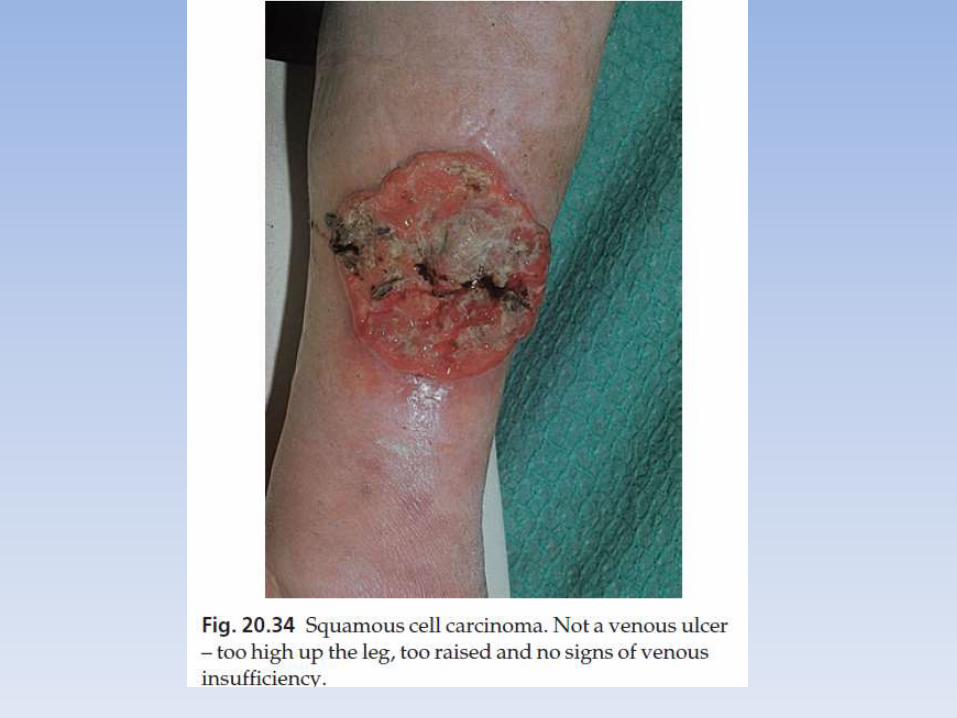
• rapidly growing lesions may start as ulcers with a granulating base and an induratededge.
• Squamous cell carcinomas are common on the lower lip and in the mouth.
Metastasis
• Tumours arising in non-exposed sites, such as the perineum and sole of foot and on the ear and lip may metastasize.
• Tumours arising in sun-exposed areas and in actinic keratosesseldom metastasize except in immunosuppressed patients.
Tumours are the most likely to metastasize if:• arising in chronic draining sinuses, chronic ulcers, areas of previous
X-radiation or thermal injury, or chronic inflammation. • Tumours more than 2 cm in diameter are twice as likely to recur
and metastasize compared with smaller tumours. tumours greater than 4 mm in depth or invading to the subcutaneous tissue
• in poorly differentiated tumours• in tumours with perineural involvement• those arising in the immunosuppressed.
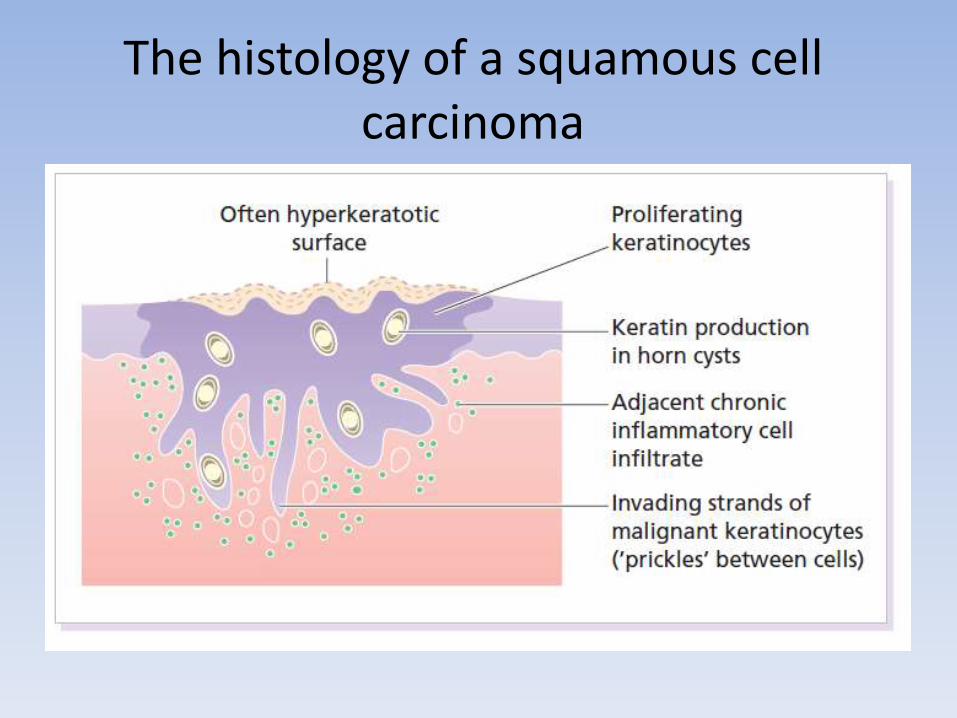
Histology• Keratinocytes disrupt the dermo-epidermal junction and
proliferate irregularly into the dermis. • Malignant cells usually retain the capacity to produce
keratinTreatment• low-risk tumours be excised with a 0.5-cm border of normal
skin. • high-risk tumours should have wider excision (6 mm or
more) or Mohs’ micrographic surgery • palpation of regional nodes is important in work-up and
follow-up. • Radiotherapy is effective but should be reserved for the
frail and elderly and special situations.• Follow-up for up to 5 years is recommended for patients
with recurrent disease and for those with high-risk tumours.
The histology of a squamous cell carcinoma
Malignant melanoma
Incidence
• females being affected more often than males.
• There is a higher incidence in white people living near the equator than in temperate zones and there the female preponderance is lost.
• The tumour is rare before puberty and in black people, Asians and Orientals and when it does occur in these races it is most often on the palms, soles or mucous membranes.
Cause
GeneticSusceptibility genes • Rarely (around 6%), melanomas are familial, occurring in
families where two or more first-degree relatives have a melanoma.
• Molecular defects in both tumour suppressor genes and oncogenes have been linked to these melanomas
• Mutations in CDKN2A confer on carriers a risk of melanoma of 20% by the age of 40 years and 40% by 60 years.
• Other high-risk susceptibility genes include CDK4
Cause
Susceptible phenotypes• white people with blond or red hair, many freckles and
a fair skin that tans poorly.• Those of Celtic origin are especially susceptible.• Melanoma can affect several members of a single
family in association with atypical (dysplastic) naeviSunlight• Both the incidence and mortality increase with
decreasing latitude. • Tumours occur most often, but not exclusively, on
exposed skin. • For melanomas, the number of sunburns seems more
relevant than cumulative ultraviolet radiation dose.
Cause
Pre-existing melanocytic naevi
• The risk of developing a malignant melanoma is highest in those with atypical naevi, congenital melanocytic naevi or many banal melanocytic naevi.
• A pre-existing naevus is seen histologically in about 30% of malignant melanomas.
Prevention and early diagnosis
• This is best done by avoiding exposure of skin to sunlight and tanning booths.
• Dermatologists joke that the best sunscreen is a house.
• a sunscreen of SPF 15 or more should be used and reapplied after 20 min to add a second coat and to catch missed areas.
• Regular self-examination and the education
Clinical features
• 80 % of invasive melanomas are preceded by a superficial and radial growth phase, shown clinically as the expansion of an irregularly pigmented macule or plaque.
• Most are multicoloured mixtures of black, brown, blue, tan and pink.
• Their margins are irregular with reniformprojections and notches
• There are four main types of malignant melanoma.
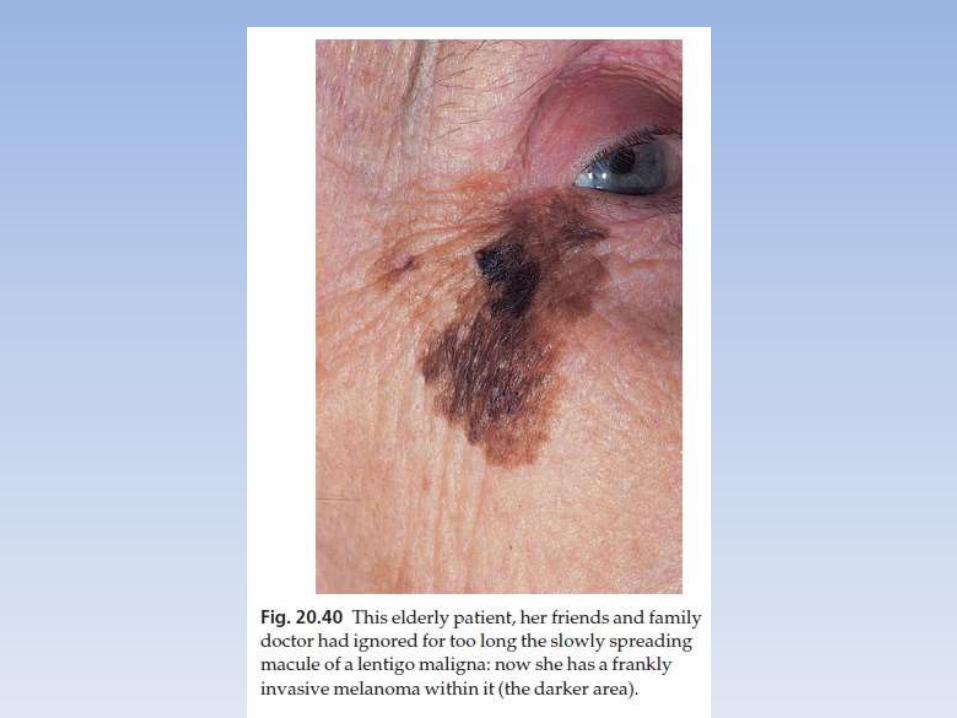
1. Lentigo maligna melanoma• occurs on the exposed skin of the elderly. • An irregularly pigmented, irregularly shaped macule (a
lentigo maligna) may have been enlarging slowly for many years as an in situ melanoma before an invasive nodule (the lentigo maligna melanoma) appears
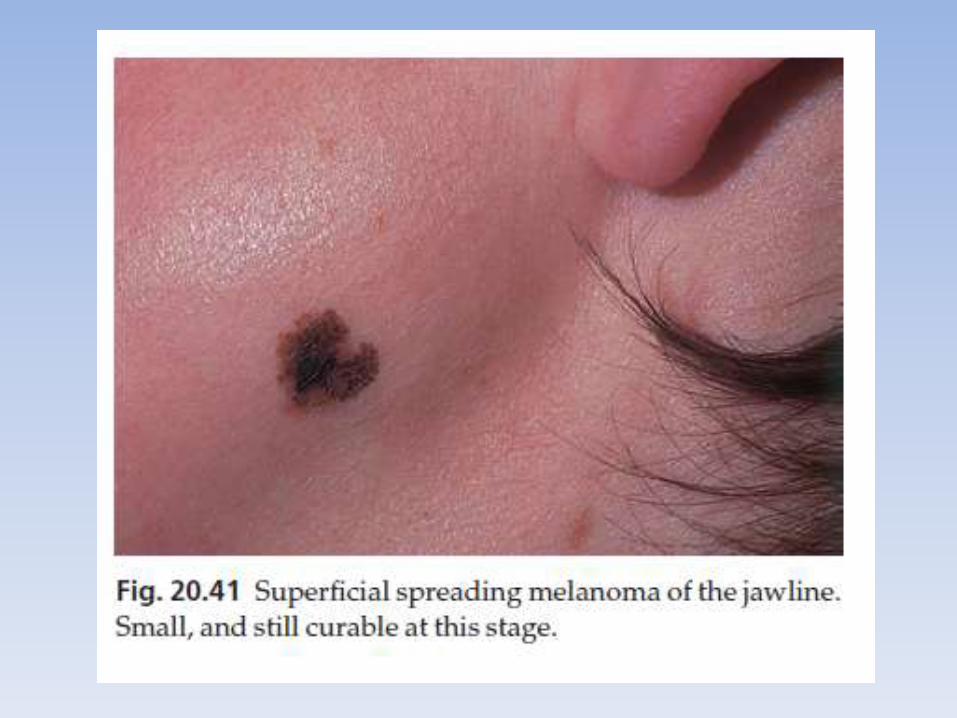
2. Superficial spreading melanoma • is the most common type in Caucasoids. • Its radial growth phase shows varied colours and is often
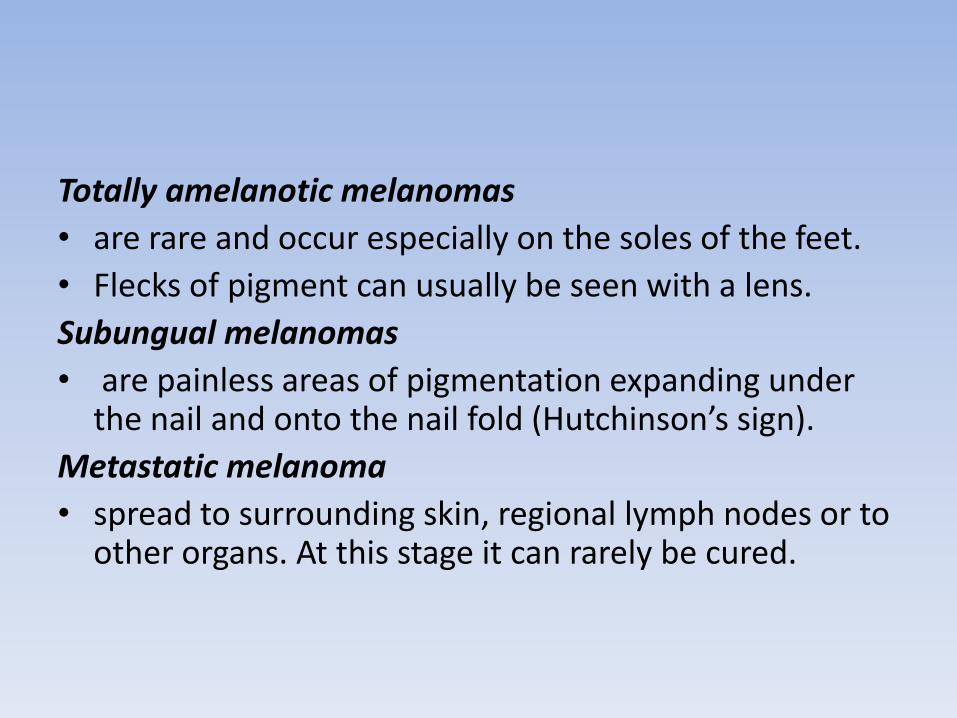
palpable• A nodule coming up within such a plaque signifies deep
dermal invasion and a poor prognosis
3. Acral lentiginous melanoma• occurs on the palms and soles and, although rare in
Caucasoids• is the most common type in Chinese and Japanese people. • The invasive phase is again signalled by a nodule coming up
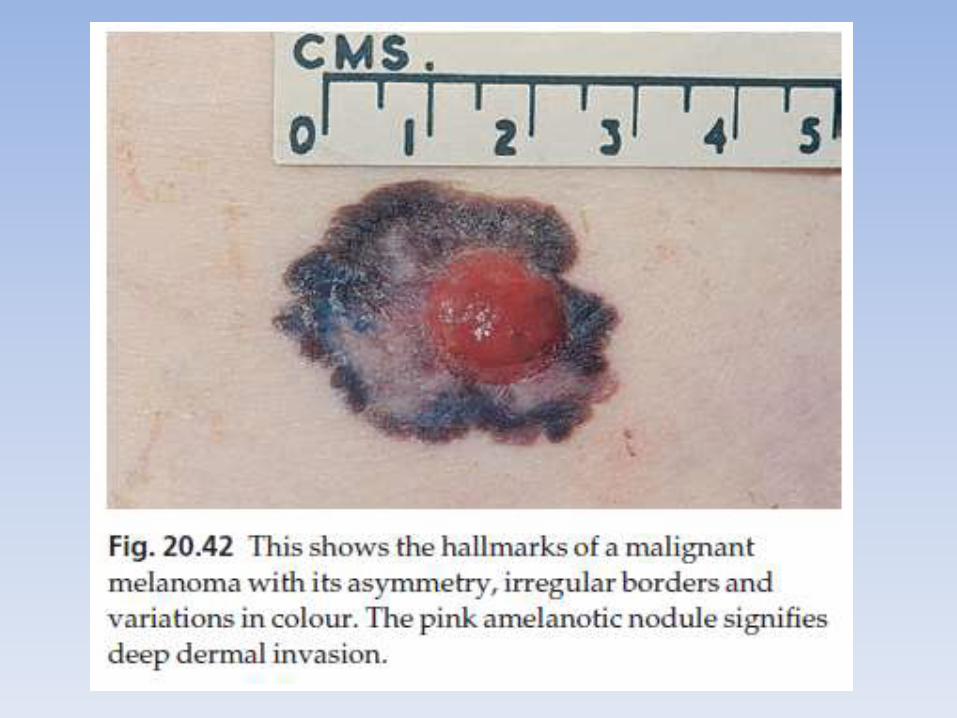
within an irregularly pigmented macule or patch.4. Nodular melanoma• appears as a pigmented nodule with no preceding in situ
phase. • It is the most rapidly growing and aggressive type. • Melanomas can also described by their colour, site and
degree of spread.
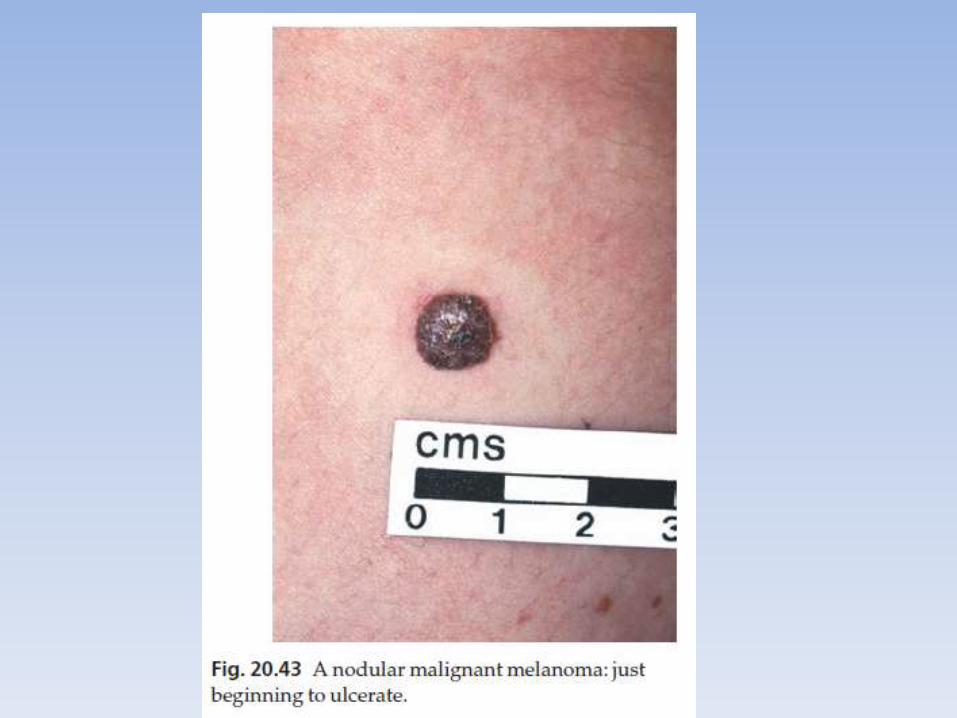
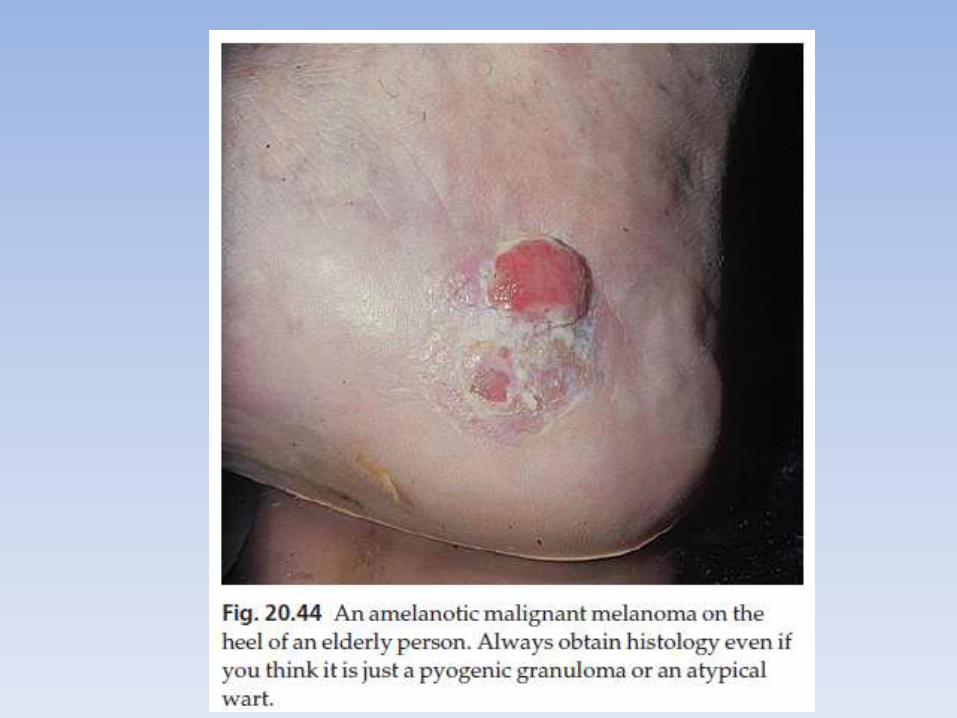
Totally amelanotic melanomas
• are rare and occur especially on the soles of the feet.
• Flecks of pigment can usually be seen with a lens.
Subungual melanomas
• are painless areas of pigmentation expanding under the nail and onto the nail fold (Hutchinson’s sign).
Metastatic melanoma
• spread to surrounding skin, regional lymph nodes or to other organs. At this stage it can rarely be cured.
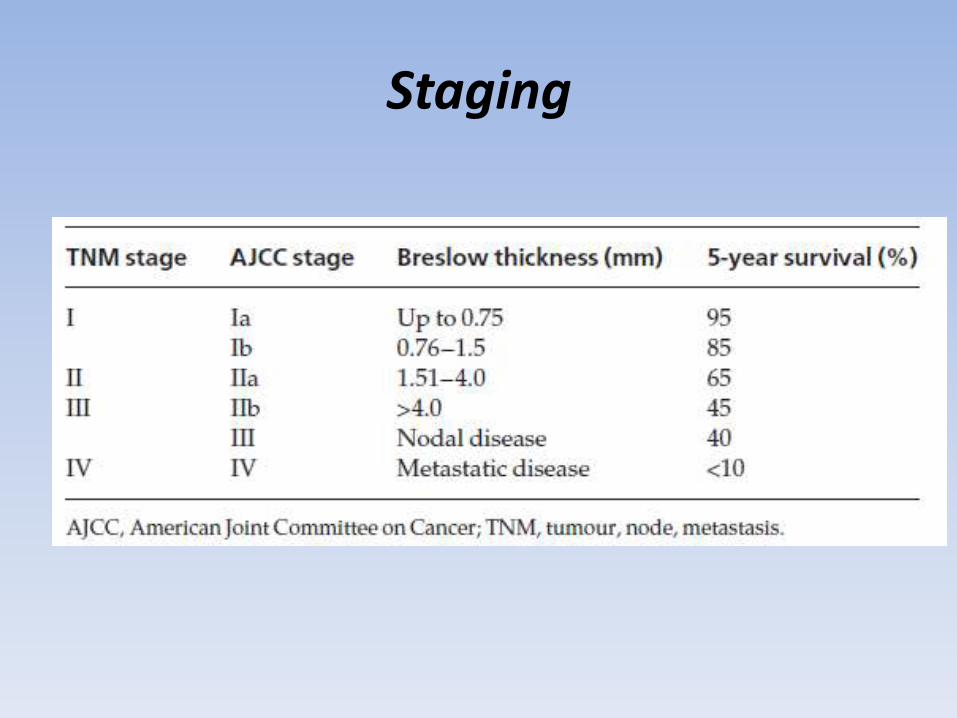
Staging
Histology
Lentigo maligna• Numerous atypical melanocytes, many in groups, are seen
along the basal layer extending downwards in the walls of hair follicles.
Lentigo maligna melanoma • Dermal invasion occurs, with a breach of the basement
membrane region. In situ changes are seen in the adjacent epidermis.
Superficial spreading melanoma in situ • Large epithelioid melanoma cells permeate the epidermis.Superficial spreading melanoma• The dermal nodule may be composed of epithelioid cells,
spindle cells or naevus-like cells. In situ changes are seen in the adjacent epidermis.
Histology
Acral lentiginous melanoma in situ • Atypical melanocytes are seen in the base of the epidermis
and permeating the mid epidermis.Acral lentiginous melanoma • Melanoma cells invade the dermis. In situ changes are seen
in the adjacent epidermis.Nodular melanoma • tumour comprises epithelioid, spindle and naevoid cells
and there is no in situ melanoma in the adjacent epidermis.Desmoplastic melanoma • Melanoma cells are seen amongst a dense fibrous stroma.
The overlying epidermis may show signs of a preceding lentigo maligna or acral lentiginous melanoma in situ
Microstaging
Breslow’s method • is to measure, with an ocular micrometer, the
vertical distance from the granular cell layer to the deepest part of the tumour.
Clark’s method• used less frequently nowadays, is to assess the
depth of penetration of the melanoma in relation to the different layers of the dermis
• The thicker and more penetrating a lesion, the worse is its prognosis.
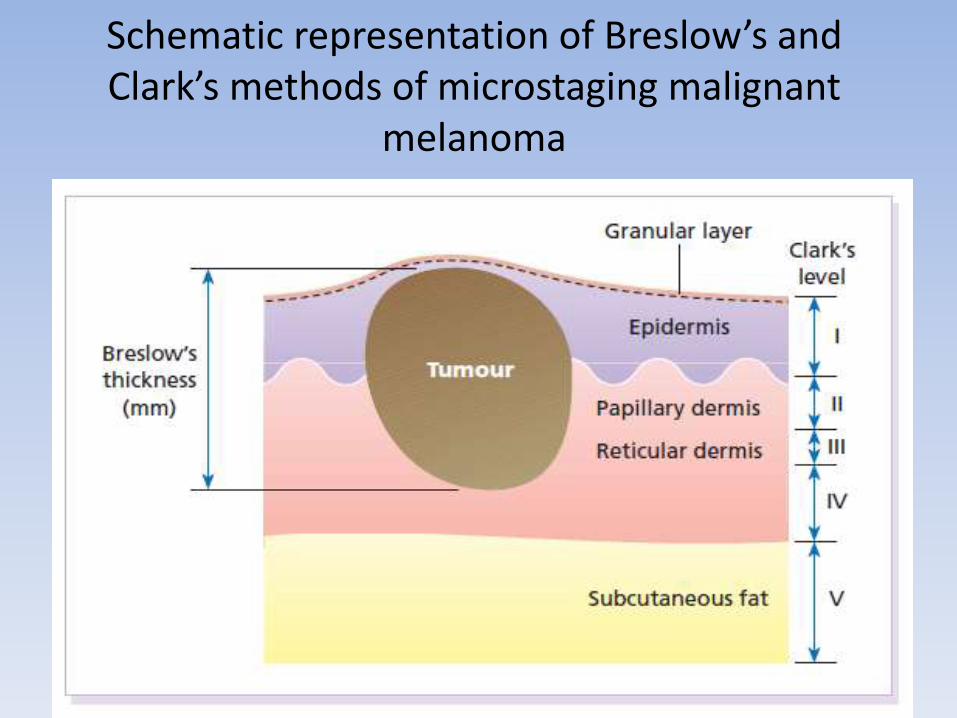
Schematic representation of Breslow’s and Clark’s methods of microstaging malignant
melanoma
Differential diagnosis
1. melanocytic naevus2. seborrhoeic keratosis3. pigmented actinic keratosis4. lentigo5. pigmented basal cell carcinoma6. sclerosing haemangioma7. subungual or periungual haematoma8. An amelanotic melanoma is most often
confused with a pyogenic granuloma and with a squamous cell carcinoma.
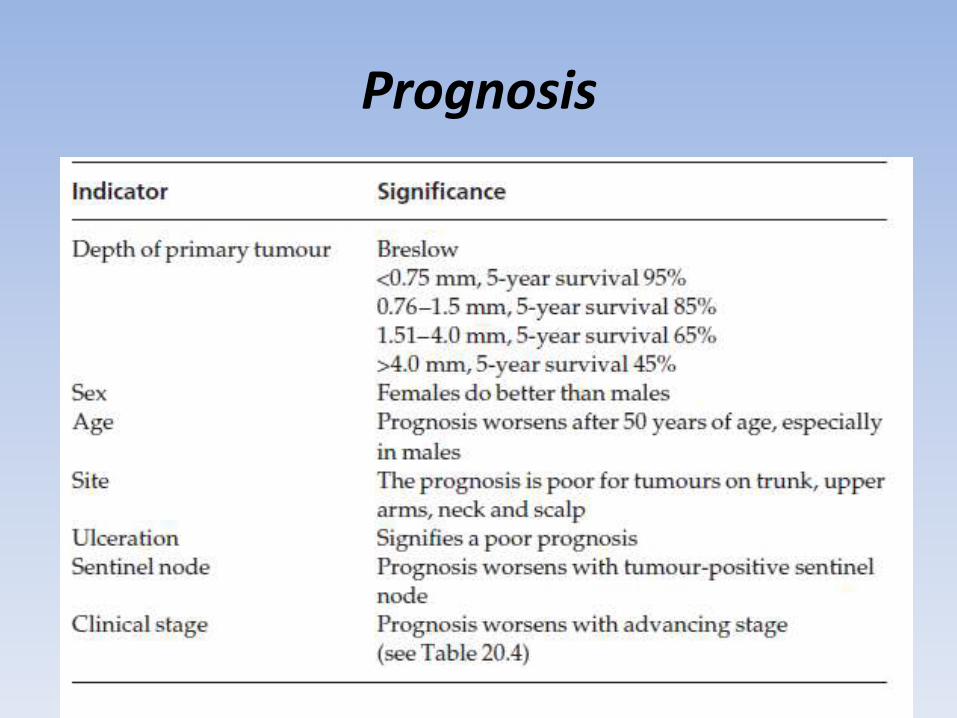
Prognosis
Treatment
Surgery• Surgical excision, with minimal delay, is required. • An excision biopsy, with a 2–5 mm margin of clearance
laterally and down to the subcutaneous fat, is recommended for all suspicious lesions.
• Shave and punch biopsies are not recommended, but can be performed if the lesion is in a cosmetically sensitive site.
• Shave biopsies may not include the deep margin, making it difficult to gauge prognosis, and superficial shave biopsies may be misdiagnosed.
• Punch biopies can lead to a sampling error
Treatment
• If the histology confirms the diagnosis of malignant melanoma then wider excision, including the wound of the excision biopsy, with a minimum of 0.5 cm clearance for melanomas in situ and 1 cm clearance is required for all invasive melanomas.
• Nowadays many surgeons excise 1 cm of normal skin around the tumour (or wound) for every millimetre of tumour thickness, up to 3 mm
• fine needle aspiration if lymph node involvement is suspected clinically. If involvement is confirmed then formal block dissection of the involved group of nodes should be carried out.
Follow-up care
• Patients who have had melanoma should be screened for recurrence and for metastases. Recurrence usually appears as a growth or pigmentation at the original site.
• In transit melanomas are satellite nodulesnnearby but not connected to the original tumour.
• The regional nodal basins should be palpated• 80 % of recurrent and/or metastatic melanomas
occur within 3 years of definitive surgery. • A second primary melanoma is not unusual
TheEnd