skin & its appendages chapter 6. integumentary system skin and its appendages (attachments)...
TRANSCRIPT
Skin & its Appendages
Chapter 6
Integumentary System
• Skin and its appendages (attachments)
• Body’s thinnest, largest, most important organ
• Appendages = hair, nails, skin glands• Integument = “skin”• Relatively flat organ; classified as
cutaneous membrane
Structure of the Skin• Two main layers:1. Outer, thinner layer (or strata) –
epidermis– Composed of epithelial tissue
2. Inner, thicker layer of vascular connective tissue – dermis
• Dermal-epidermal junction – where epidermis and dermis meet
• Hypodermis – lies beneath the dermis (subcutaneous tissue)
– Rich in fat and areolar tissue – Fat content varies with state of nutrition
Structure of the Skin• Thin and thick skin – refers to epidermis
ONLY• Thin skin – covers most of body surface• Thick skin – palms of hands, soles of
feet, finger tips– All 5 layers of epidermis present– Raised dermal papillae (fingerprints or
footprints)– No hair is present in thick skin
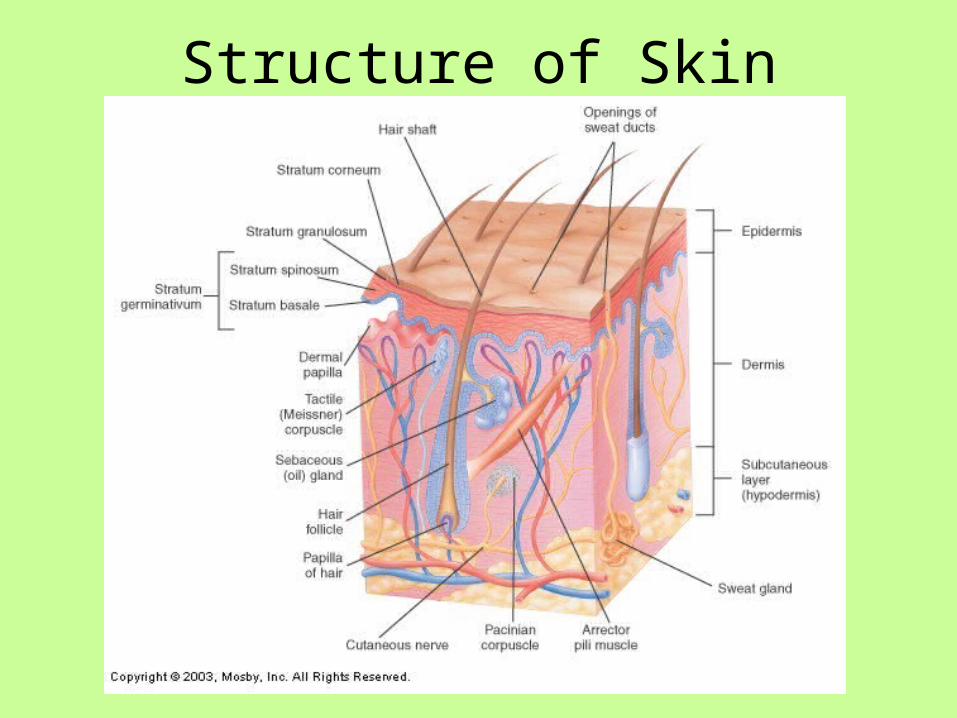
Structure of Skin
Epidermis – Cell Types3 cell types1. Keratinocytes: synthesize keratin
– Keratin: tough, fibrous protein found in hair, nails and outer skin
– Keratinocytes make up 90% of epidermal cells– Principal structural element of outer skin
2. Melanocytes: synthesize melanin (brown pigment – gives skin color)
– Melanin: protects deeper layers from ultraviolet light
3. Langerhan cells (immune cells)– Provide defense mechanism for the body– Arise from bone marrow & migrate to the
epidermis

Epidermis – Cell Layers
5 strata (cell layers)1. Stratum corneum (horny layer)
– Most superficial layer– Shingle-like dead cells– Cell shape = squamous– Cytoplasm replaced by keratin– Keratinization – process of cells formed
from deeper layers, fill with keratin and push to the surface
Epidermis – Cell Layers
2. Stratum lucidum (clear layer)– Keratinocytes are anucleated and clear– Cytoplasm filled with Eleidin – a protein-
bound lipid that will eventually turn into keratin
– Blocks water penetration and loss– Present only in thick skin
Epidermis – Cell Layers3. Stratum Granulosum (granular layer)
– Keratinization begins in this layer– 2-4 layers of flattened cells– Cells in this strata are filled with granules
called keratohyalin
4. Stratum spinosum (spiny layer)– 8-10 layers of irregular shaped cells with
prominent intercellular bridges (connections)– Cells are rich with RNA for protein synthesis
required for the production of keratin
Epidermis – Cell Layers
5. Stratum basale (base layer)– Single layer of columnar cells– Mitosis only occurs here– Cells originate from here migrate to
superficial layers shed
Stratum germinativum (growth layer)– Used to describe the stratum spinosum
and the stratum basale together
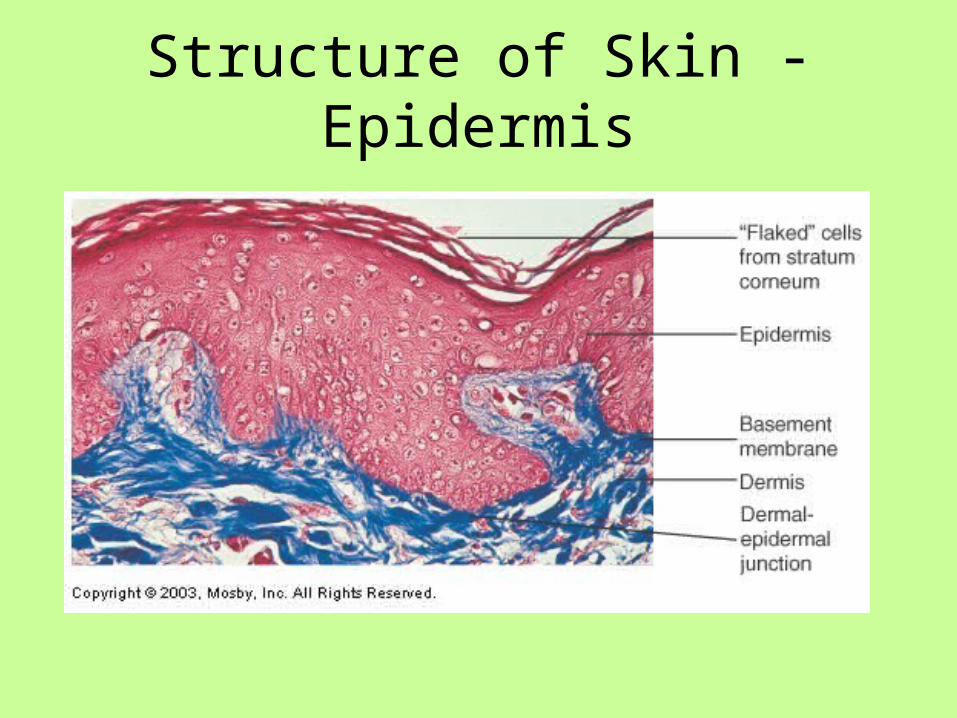
Structure of Skin - Epidermis
Epidermal Growth & Repair
• Regeneration time – time period required for population of cells to mature & reproduce
• Time for new cell formation = rate of old keratinized cells flaking off– Helps maintain constant thickness of epidermis
• Cells push upward into each layer die become keratinized desquamate (fall away/shed)
• Regeneration time is approximately 35 days
Dermal-Epidermal Junction
• Composed of basement membrane• Also contains specialized fibrous
elements & polysaccharide gel that cements epidermis to dermis
• Partial barrier to passage of some cells and large molecules
Dermis or corneum (“true skin”)
• Thicker than epidermis• Protective function against mechanical injury• Storage area for water and electrolytes• Contains somatic sensory receptors (nerves &
nerve endings)– Process information such as: pain, pressure, touch,
temperature
• Muscle fibers, hair follicles, sweat & sebaceous glands, blood vessels
• Rich vascular supply of the dermis plays a critical role in regulation of body temperature
Papillary Layer of Dermis
• Thin layer• Loose connective tissue with elastic and
collagenous fibers• Dermal papillae – bumps that project into
epidermis– Creates distinct ridges on epidermal surface of
fingers & toes (finger/footprints); unique for every person
– Creates a gripping surface
Reticular Layer of Dermis• Thick layer• Dense irregular connective tissue• Network of fibers – collagenous & elastic• Contains muscle – skeletal & smooth (allows
for point of attachment for movement)• Skeletal muscle – scalp movement & facial
expressions• Arrector pili muscles: small bundles of
smooth muscle that causes hair to “stand on end” – which causes the skin around it to raise = “goosebumps”
• Somatic sensory receptors for pain, pressure, touch and temperature– Ex: tactile (Meissner) corpuscle senses light touch
& pressure
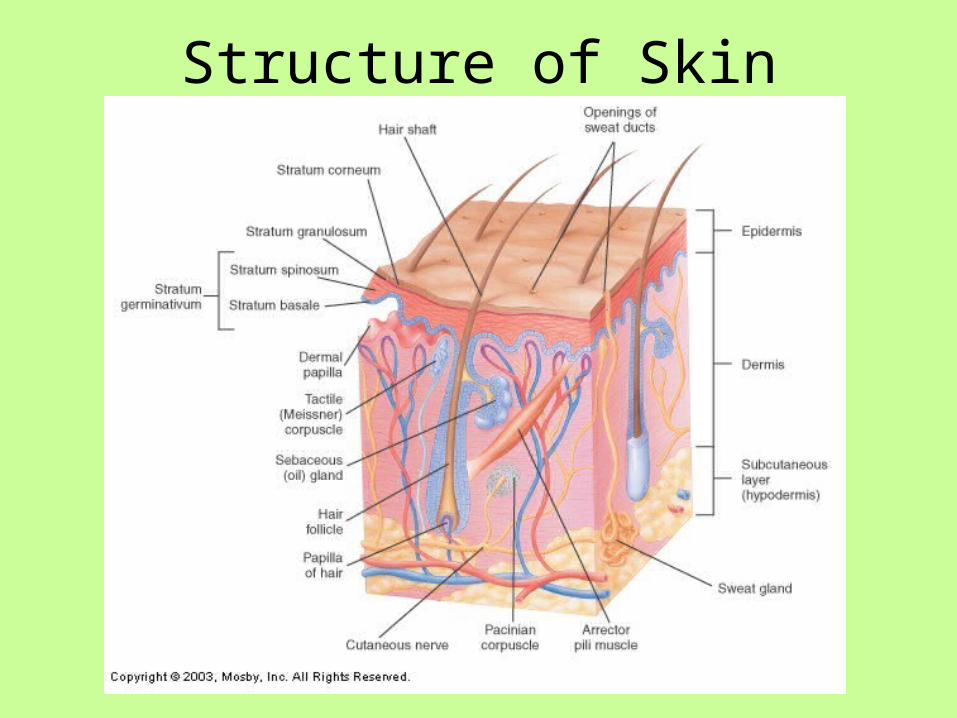
Structure of Skin
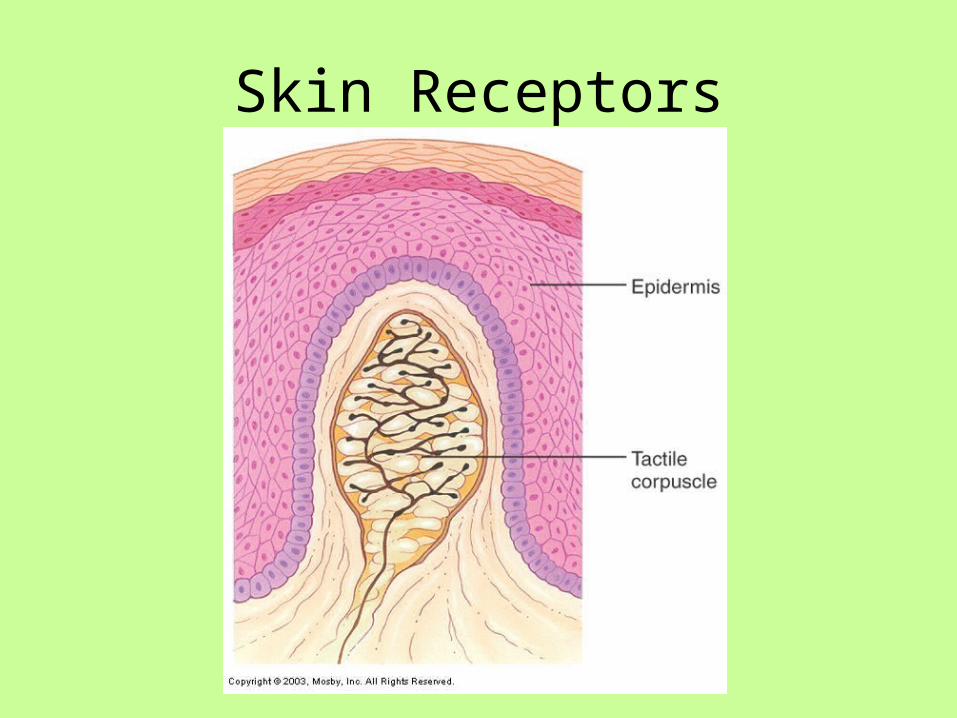
Skin Receptors

Dermal Growth & Repair • Does not shed & regenerate like the
epidermis– Rapid regeneration only occurs during
wound healing
• Dense fibrous connective tissue fills wound/incision/injury site to form a scar
• Langer’s Cleavage lines: collagenous fibers in dermal layer tend to orient themselves in patterns that differ from one body part to another
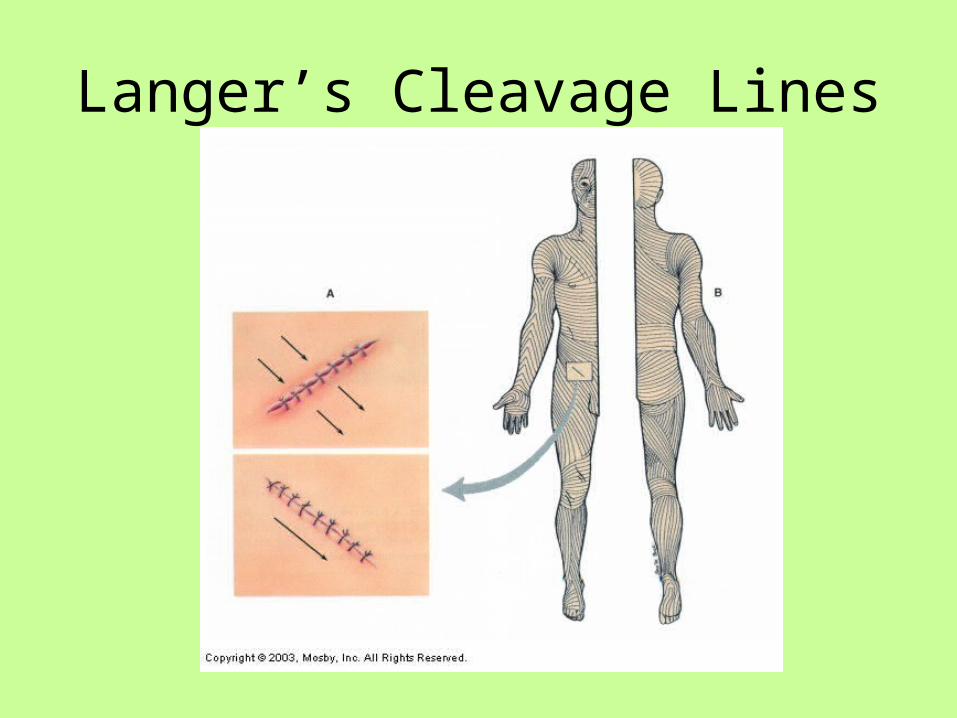
Langer’s Cleavage Lines
Dermal Growth & Repair
• Stretch marks – due to dermal tearing heal results in tiny scars– Ex: pregnancy, rapid weight gain/growth
Questions – Answer in complete sentences
1. Identify the two main or primary layers of skin. What tissue type dominates each layer?
2. The terms thin and thick refer to which primary layer of skin? How do thick and thin skin differ?
3. Identify the three cell types found in the epidermis. Give a description of all three.
4. List the five layers (or strata) of the epidermis. Give a brief description of each layer. Is each layer found in both thin and thick skin?
5. What is the name of the glue-like layer separating the dermis from the epidermis?
6. What structure forms the bumps that produce ridges on the palms and soles? Which layer of the dermis is this structure located in?
7. Which layer is vascular: the epidermis or dermis? What important role does the dermal vasculature play?
What Determines Our Skin Color?
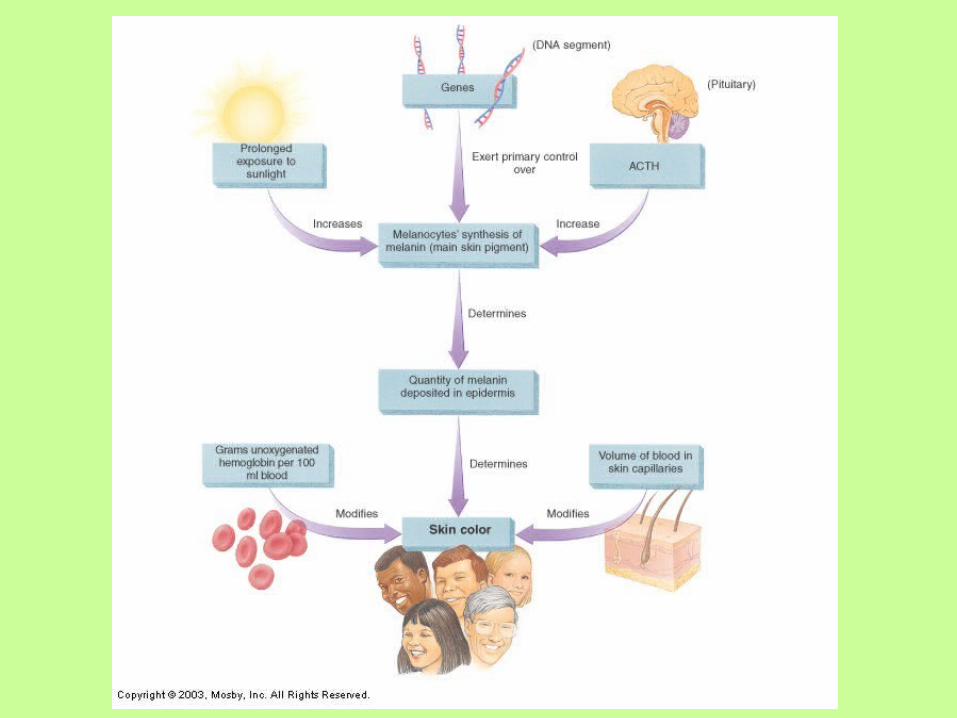
Skin Pigments – 2 types1. Melanin – brown pigment
– Skin color determined by quantity of melanin– Melanocytes convert the amino acid tyrosine
to melanin; process catalyzed with tyrosinase– Majority of melanocytes found in stratum
basale– Amount of melanin produced depends on
genetics, sun exposure, age and hormones ACTH)
– Ex: Albinism (albino individuals) – tryrosinase is absent from birth; melanin cannot be synthesized
Skin Color2. Carotene – yellow pigment
– Pigment found in food– Can deposit in stratum corneum of thick
skin (palms & soles of feet)
Other determinants of skin color:• Changes in the vasculature
– Blood vessels constrict = pale– Blood vessels dilate = blush
• Poorly oxygenated hemoglobin (low oxygen saturation) causes cyanosis (bluish color to skin)
Functions of the Skin
1. Protection2. Sensation3. Movement without injury4. Excretion5. Endocrine functions (vitamin D)6. Immunity7. Temperature regulation
Protection• Surface film – thin film of emulsified
materials spread over the skin’s surface– Produced from the mixture of residue/secretions
from sweat & sebaceous glands with epithelial cells constantly being shed
– Function of the surface film:• Antibacterial & antifungal activity, lubrication, hydration
of the skin surface, buffering of caustic irritants, blockage of toxic agents
• Keratin protects against dehydration, microorganisms, chemical/mechanical damage
• Melanin – protects against ultraviolet radiation
Sensation
• Sensory receptors serve as antennas that detect stimuli– Pressure, pain, temperature, touch– Ex: tactile corpuscle
Movement & Growth
• Movement and growth of the body as a whole can occur due to the presence of elastic fibers in the skin
Excretion
• Body regulates volume and chemical composition of sweat through functions of the skin
• Skin influences fluid volumes in the body & waste products excreted from the skin– Ex: uric acid, ammonia, urea
Vitamin D Production
• Endocrine process• First steps of vitamin D production
occurs in the skin when exposed to ultraviolet light
• Vitamin D synthesis is completed in the kidneys & liver
Immunity
• Specialized cells are present in the skin– Ex: langerhan cells with help from
helper T cells trigger immune reactions
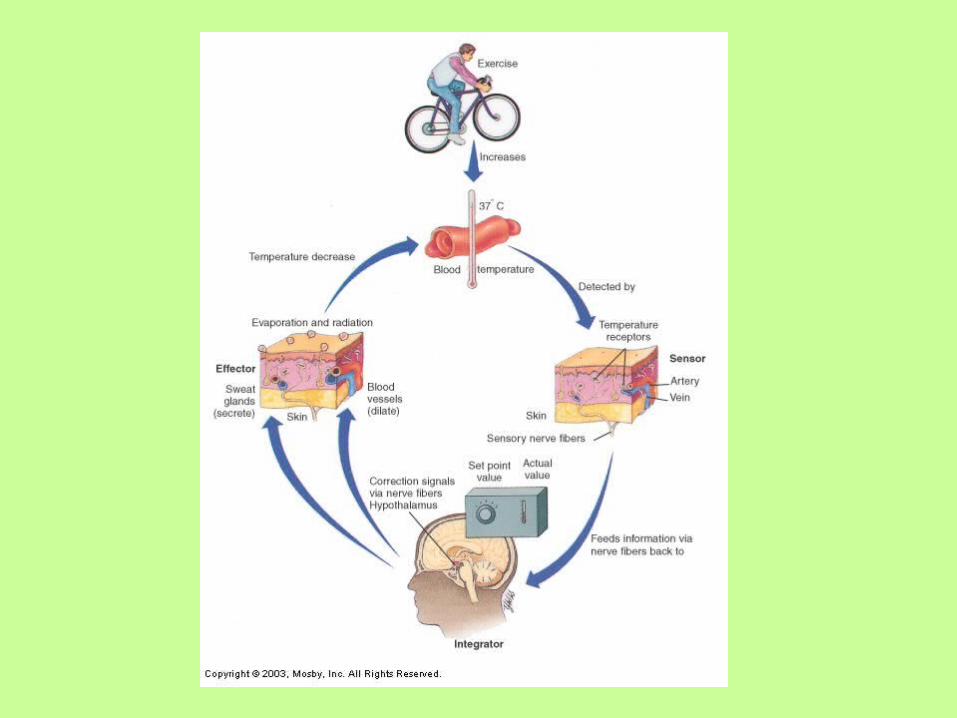
Regulation of Body Temperature
• Majority of heat production is the result of food metabolism and activity of muscles and glands (esp the liver)
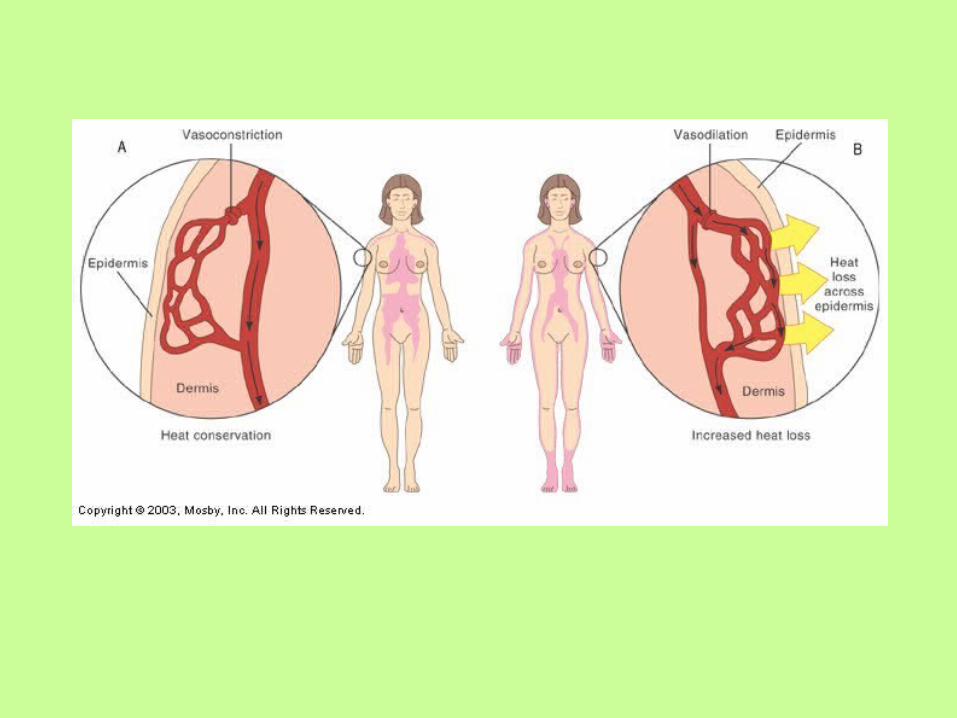
• Vasocontriction: prevents heat loss warm blood circulating deeper within the body
• Vasodilation: increases heat loss increases skin’s blood supply heat lost to the external environment– Evaporation, radiation, conduction and convection
• Homeostasis of body temperature controlled by negative feedback mechanism
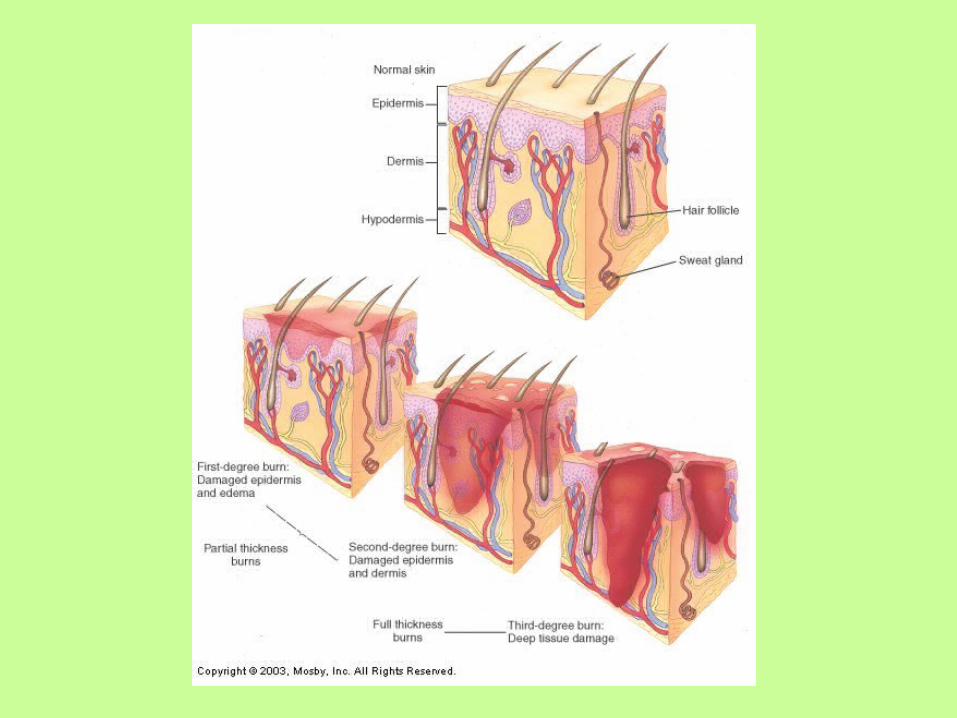
Burns
• Tissue injury or skin cell death that results from heat/fire, overexposure to ultraviolet light, contact with electrical current, corrosive chemicals
Burns – Estimating Affected Body Surface
• Treatment & prognosis of a burn depends largely on the amount of skin surface affected
• “Rule of palms” – the size of the patient’s palm is approximately 1% of their body surface
• “Rule of nines”– Body surface divided into 11 areas
(anterior and posterior) of 9%– Perineum (genital area) accounts for 1 %

Severity of Burns• First degree burns – usually caused by a sunburn
– only epidermis is damaged– skin is red and swollen, no blistering
• Second degree burns – Epidermis and dermis are damaged– damage to sweat glands, hair follicles, and sebaceous glands– Blisters, severe pain, swelling and scarring are common
• Third degree burns (full thickness burns)– destruction of epidermis and dermis– tissue death extends below sweat glands and hair follicles– burning may involve fascia, muscle, and bone– Patient may be insensitive to pain immediately after due to
destruction of nerve endings– Severe scarring
Hair
• Hairless areas: palms, soles of feet, lips, nipples, some parts of genitalia
• At approximately 6 months gestation – fetus is covered with lanugo
• After birth vellus hair replaces lanugo• At puberty – terminal hair replaces
vellus hair

Hair Growth• Growth begins when epidermal cells spread
down into dermis to form a follicle• Follicle consists of 2 layers
– Outer dermal root sheath– Epithelial root sheath (external & internal parts)
• Follicle’s inner layer formed by stratum germinativum– Germinal matrix: a cap-shaped cluster of cells
at the bottom of the follicle
• It is the cells of the germinal matrix that are responsible for forming hair/hair growth

Hair Anatomy
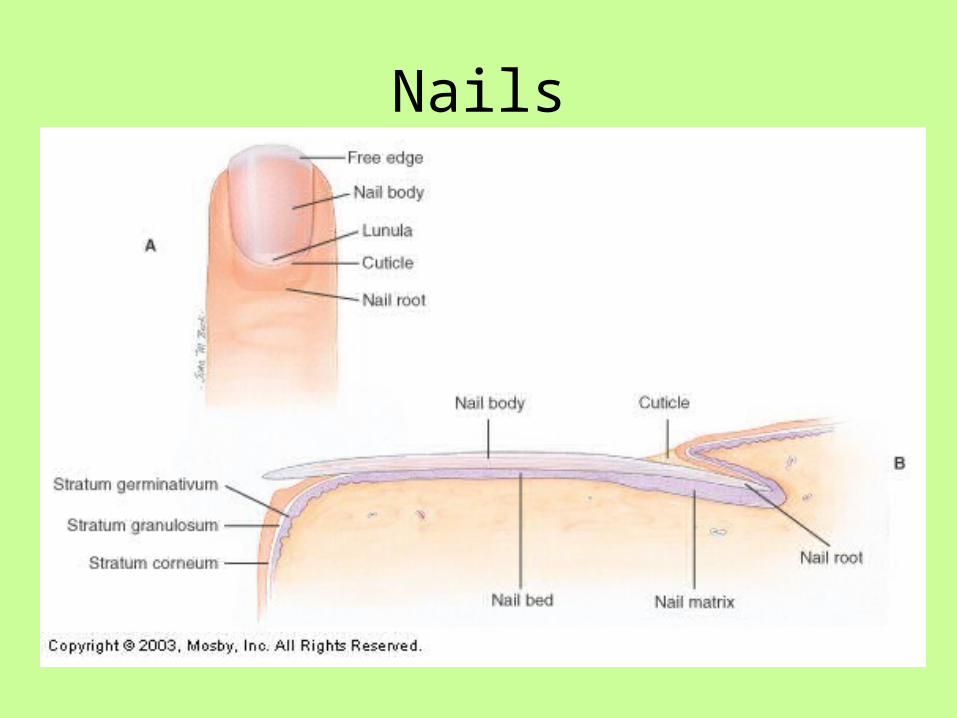
Nails
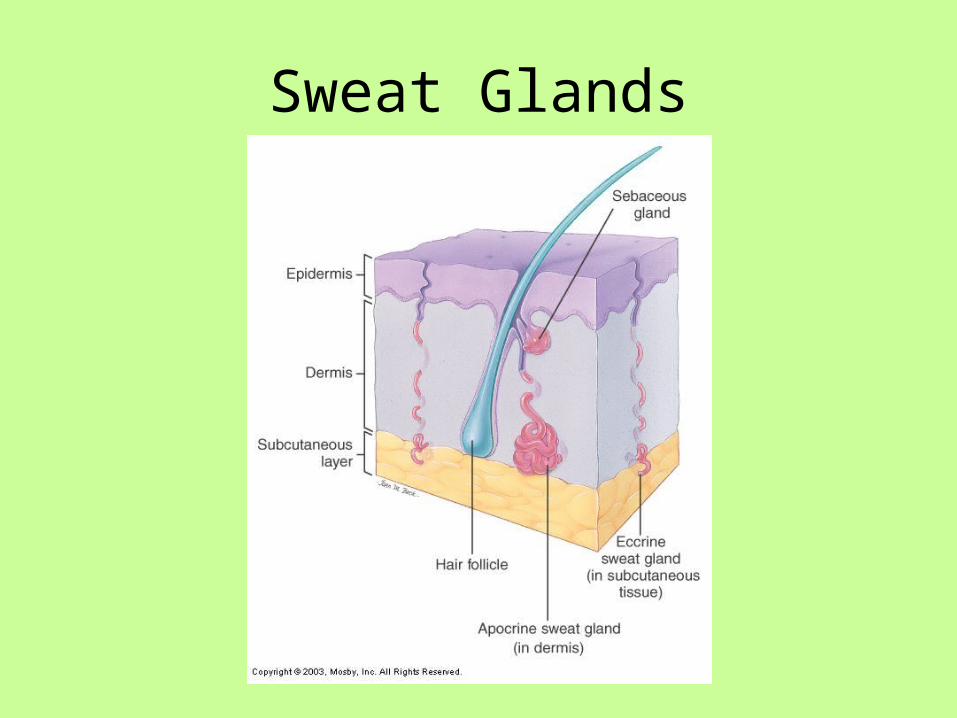
Skin GlandsSweat glands - most common
– Two types: Eccrine & apocrine– Based on location, secretion & nervous system connections
1. Eccrine sweat glands - most numerous and wide spread– simple, coiled, tubular gland– Produces sweat or perspiration - a watery liquid rich in salts,
ammonia, uric acid, urea and other wastes– Sweat also plays an important role in maintaining constant
body temperature– Majority found on soles of feet, palms, forehead and upper
torso 2. Apocrine sweat glands - larger than eccrine glands
– located deep in the subcutaneous layer of the skin– Ex: armpit (axilla), areola of breast, pigmented skin around
anus– Ducts are connected to and secrete into hair follicles– Classified as simple, branched tubular glands– Function of apocrine glands begins at puberty– Odor is from skin bacteria, not secretions
Sweat Glands
Sebaceous Glands• Secrete oil for hair & skin• Simple alveolar gland; found in dermal layer• Oil = sebum
– Lubricates skin– Antifungal property – kills fungus & bacterial
• Increases effectiveness of surface film
• Mostly associated with hair follicles• Glands activated at puberty
– Stimulated by sex hormones
• Accumulation of sebum in ducts = white pimple• Oxidation causes sebum to darken = blackhead
Ceruminous Glands
• Modified apocrine sweat gland• Open into the skin of the external ear
cannal• Brown waxy substance = cerumen• Provides protection from dehydration
– Risk for blockage and hearing loss
Mechanisms of Disease – Skin Disorders
• Skin Infections• Vascular & Inflammatory Disorders• Abnormal Body Temperature • Skin Cancers
Skin Infections• Impetigo
– Bacterial infection caused by either staphylococcus or streptococcus that usually occurs in young children
– Reddish discoloration that develops into vesicles (blisters) and yellowish crusts
– Can become systemic
• Tinea – fungal infection (ex: ringworm, jock itch, athlete’s foot)– s/sx: erythema (redness), scaling, crusting– Tx: antifungal medications
Skin Infections
• Warts – caused by papillomaviruses– Usually benign, but can be malignant– Transmitted through direct contact– Tx: freezing, drying, laser therapy
• Boils (furuncles) – local staphylococcus infections– Infection of hair follicles– Large, inflamed pus-filled lesions
Vascular & Inflammatory Skin Disorders
• Decubitus ulcers (bedsores)– Lesions caused by decreased blood flow to skin
area; usually on boney prominences – Tx: changing position, soft surfaces
• Urticaria (hives) – raised red lesions (aka wheals)– Caused by leakage of fluid from blood vessels in
skin– Causes severe itching– Usually due to allergic reaction, physical irritant or
systematic disease• Scleroderma – autoimmune disease affecting
blood vessels and connective tissue of skin– Results in patches of yellowish, hardened skin
Vascular & Inflammatory Skin Disorders
• Psoriasis – chronic inflammatory disease– Genetic basis– Cutaneous inflammation, followed by scaly
lesions– Results from excessive rate of epithelial cell
growth
• Eczema – most common inflammatory skin disorder– Inflammation, papules (bumps), vesicles
(blisters), crusts– Usually s/sx of underlying condition
• Ex: allergic reaction or poison ivy

Abnormal Body Temperature
• Fever– Associated with systemic inflammatory release
• Malignant hyperthermia – Abnormal rise in body temperature & muscle rigidity when
exposed to anesthetics or muscle relaxants
• Heat exhaustion– Caused by fluid loss
• Heat stroke– Inability to maintain normal body temp (>105) in warm
environments
• Hypothermia– Inability to maintain normal body temp (<95) in cold
environments
• Frostbite– Local damage to tissues from very low temperatures
Skin Cancer
Basal Cell Carcinoma• Most common type of skin cancer• Arises from stratum basale• Most common areas – nose & face• Usually occurs in patients > 40 y/o• Rarely metastasizes
Skin Cancer
Squamous cell carcinoma• Slow growing; arises from epidermis• Occurs in middle-aged & elderly• Affects sun-exposed areas (scalp,
forehead, backs of hands)• Some forms may metastasize

Skin CancerMalignant Melanoma• Most deadly of all skin cancers• Affects older individuals with light skin, eyes
& hair; usually have poor ability to tan• May develop from pigmented mole• Use ABCD rule for detection:
– Asymmetrical• Benign moles = symmetrical; malignant moles =
asymmetrical – Border
• Benign moles have distinct border; malignant = irregular/indistinct border
– Color• Benign = even color of brown; malignant = unevenly
colored, mixture of shades– Diameter
• Malignant = diameter usually > 6mm
Anthony’s Textbook of Anatomy and Physiology 17th Edition. Thibodeau, Gary A. PhD and Patton, Kevin T. PhD. Mosby, Inc.