skim the surface - c.ymcdn.com · skim the surface: subcutaneous abdominal masses a quiz-based...
TRANSCRIPT

Skim the Surface: Subcutaneous Abdominal Masses A Quiz-Based Review
1
Nicole Kurzbard-Roach, MD1; Monica Deshmukh, MD2; Cecilia M. Jude, MD2; Barbara Kadell, MD1; Shaden Mohammad, MD2; Maitraya Patel, MD1,2
1Department of Radiology, Ronald Reagan UCLA Medical Center, 2Department of Radiology, Olive View-UCLA Medical Center

BACKGROUND Subcutaneous abdominal masses are encountered during routine imaging, either as incidental findings or in the evaluation of a palpable abnormality. Subcutaneous masses arise from multiple disease processes, including neoplastic and iatrogenic etiologies. Understanding and recognizing these entities will assist in the interpretation of these masses.
EDUCATIONAL GOALS After reviewing this quiz-based presentation, participants will be able to: • Understand the anatomy of the abdominal wall. • Identify common and uncommon abdominal wall masses and mass-like conditions. • Provide clinical management or follow up considerations where appropriate.
TARGET AUDIENCE Residents, fellows, general radiologists, abdominal radiologists
2
BACKGROUND | EDUCATIONAL GOALS
DISCLOSURES The authors have no relevant disclosures to report.

OVERVIEW
ABDOMINAL WALL ANATOMY
BENIGN NEOPLASM Fibromatosis (abdominal wall desmoid); Endometriosis; Varices; Neurofibroma; Rosai-Dorfman; Benign lipomatous tumor (lipoma) b
MALIGNANT NEOPLASM Liposarcoma; Cutaneous lymphoma; Metastases b
IATROGENIC/TRAUMA Liposuction/Abdominoplasty; Injection granuloma; Foreign body
CONGENITAL Undescended testis; Urachal remnant
3

4
ABDOMINAL WALL ANATOMY
• (A) Above the umbilicus, the muscular fascia/aponeuroses surround the rectus abdominus to form the linea alba
• (B) Below the umbilicus, the muscular fascia remains anterior to the rectus abdominus; only the transversalis fascia and peritoneum are posterior to the rectus muscles
• Abdominal wall is composed of multiple muscle and fascial layers:
Fascial planes outlined as follows: external oblique muscle; internal oblique muscle; transversus abdominus muscle; transversalis fascia; peritoneum; linea alba.
rectus abdominus
linea alba
A B
5
Which of the following is true regarding abdominal wall fibromatosis:
A. Does not enhance
B. Extends along the orientation of the involved muscle aponeurosis
C. Rarely recurs after surgical resection
D. The “fascial tail sign” refers to malignant transformation
QUESTION

6
BENIGN NEOPLASM
FIBROMATOSIS (DESMOID)
• Abdominal wall desmoids arise from proliferating fibroblastic cells in the fascia along the fascial plane of the involved aponeurosis
• Benign, though can be locally aggressive and recur following resection • Risk factors: female, post-partum, prior abdominal surgery
IMAGING CHARACTERISTICS CT: variable attenuation, post-contrast enhancement US: hypoechoic mass without vascularity MRI: heterogeneity reflects cellular and fibrous components - Generally T1 isointense to muscle; post-contrast enhancement - T2W: Cellular components hyperintense, fibrous components hypointense - “Fascial tail” sign describes linear extension of the mass along fascial plane
(A) Axial T2W, (B) T1W, and (C) T1W contrast-enhanced MRI demonstrate a T2 heterogeneous, T1 isointense mass in the right rectus abdominus muscle with post-contrast enhancement.
A
B
C
Answer: B. Extends along the orientation of the involved muscle aponeurosis

7
The major risk factor for abdominal wall endometriosis is: A. Cesarean section
B. Total abdominal hysterectomy
C. Laparoscopic hysterectomy
D. Laparoscopic myomectomy
QUESTION
Sagittal contrast-enhanced CT (CECT) demonstrates enhancing ill-defined soft tissue in the abdominal wall.

ABDOMINAL WALL ENDOMETRIOMA BENIGN NEOPLASM
IMAGING CHARACTERISTICS CT: nodules isodense to muscle, mild post-contrast enhancement US: hypoehoic mass with mild peripheral vascularity MRI: T1 isointense to muscle; post-contrast enhancement; T2 hyperintense (unlike ovarian endometriomas, which show T2 shading)
• Endometriosis: functioning endometrial tissue outside the uterine cavity
• Most commonly within the pelvis • Endometrial tissue can seed the abdominal
wall following Cesarean section delivery even in patients without pelvic endometriosis
• Clinical symptoms: cyclic or non-cyclic pain associated with a mass
• Differential diagnosis: desmoid, metastasis, sarcoma, granuloma
8
(A) Axial CECT demonstrates ill-defined mildly enhancing soft tissue at Cesarean scar. (B) Ultrasound shows a hypoechoic mass with mild peripheral vascularity.
A B
Answer: A. Cesarean section The risk of abdominal wall scar endometriosis is highest following Cesarean section, though prevalence remains <1%. No increased risk in patients with history of intra-pelvic endometriosis has been reported. The abdominal wall is the most common site of extra-pelvic endometriosis.

9
Vulvoperineal varicosities are most often seen in the presence of: A. Portal hypertension
B. Lower extremity deep venous thrombosis
C. Congestive heart failure
D. Pelvic congestion syndrome
QUESTION

10
VARICES BENIGN NEOPLASM
Coronal CECT demonstrates labial mass composed of tubular structures.
• Abdominal wall varices serve as a porto-systemic collateral pathway in portal hypertension • Vulvoperineal varicosities are generally NOT seen in portal hypertension; they are associated
with pelvic congestion syndrome and may be related to ovarian venous incompetence • First presentation is usually during pregnancy
• Best visualized on CT venography, ultrasound, or MRI • Treatment for symptomatic lesions involves removing retrograde flow from ovarian veins: coil
embolization, sclerotherapy, surgical ligation
T2W fat-suppressed MRI demonstrates tortuous/serpiginous high signal structures consistent with a large vulvoperineal varix.
Answer: D. Pelvic congestion syndrome

11
Regarding neurofibromatosis:
A. Plexiform neurofibroma is sensitive but not specific for neurofibromatosis type 1 (NF1)
B. Neurofibromas are hypervascular and avidly enhancing
C. Neurofibromatosis is the second most common neurocutaneous syndrome
D. Neurofibromas are generally hypoattenuating on CT
QUESTION
Axial CECT demonstrates a cutaneous neurofibroma within the skin of the anterior abdomen in this patient with NF1.

12
NEUROFIBROMA BENIGN NEOPLASM
• Neurofibroma: a benign nerve sheath tumor which is inseparable from the parent nerve; associated with neurofibromatosis type 1 (NF1), the most common neurocutaneous syndrome (phakomatosis)
• NF1 is characterized by abnormal tumor suppression and multiple benign and malignant neoplasms throughout the body • Clinical manifestations also include skin pigmentation abnormalities (café au lait spots, axillary/groin freckles), Lisch
nodules (benign hamartomas of the iris), neurofibromas (cutaneous and intra-abdominal), optic gliomas
IMAGING CHARACTERISTICS Neurofibroma = fusiform, tapering mass CT: nodules mildly hypodense to muscle, mild post-contrast enhancement US: echogenic mass MRI: T1 hypointense; T2 “target sign” of central low intensity (fibrous stroma) and peripheral hyperintensity (myxoid matrix)
A B
(A) Axial CECT demonstrates a low density nodule within the skin of the right thigh in this patient with NF1. (B) Axial CECT shows a much larger, heterogeneous mass distally within the right thigh musculature is a malignant peripheral nerve sheath tumor. The heterogeneity reflects internal necrosis.
B
• Cutaneous neurofibromas usually appear during adolescence
• Plexiform neurofibromas extend throughout a nerve plexus; these are pathognomonic for NF1
• Malignant neoplasms include malignant peripheral nerve sheath tumor (MPNST), neuroendocrine tumors, sarcoma
Answer: D. Neurofibromas are generally hypoattenuating on CT

13
A. Cystic retroperitoneal mass
B. Retroperitoneal lymphadenopathy
C. Fat-containing subcutaneous mass
D. Perineural soft tissue mass
QUESTION
Axial CECT demonstrates ill-defined confluent soft tissue density within the subcutaneous fat and skin thickening in this patient with biopsy-proven Rosai-Dorfman disease.
Rosai-Dorfman disease can be included in the differential diagnosis of which finding?

• Rosai-Dorfman disease describes the clinical entity of sinus histiocytosis with massive lymphadenopathy (SHML)
• Benign progressive histiocytic proliferative disorder characterized by lymphadenopathy, usually cervical, though cases of massive retroperitoneal lymphadenopathy have been reported
• Extra-nodal manifestations (soft tissue thickening and nodules) are present in up to 43% patients
• Most common extra-nodal site: skin - usually head/neck, though can develop throughout the body
14
ROSAI-DORFMAN
Axial contrast-enhanced CT demonstrates soft tissue density nodules within the subcutaneous fat and skin in this patient with biopsy-proven Rosai-Dorfman disease.
BENIGN NEOPLASM
Answer: B. Retroperitoneal lymphadenopathy
• Extra-nodal manifestations can also include the gastrointestinal and genitourinary tracts
• Age of presentation usually < 20 years
• Etiology unknown, may represent autoimmune/inflammatory or post-infectious process

(A) Axial and (B) coronal CECT show a small non-enhancing fat-density lesion within the left external oblique muscle consistent with a superficial lipoma.
15
BENIGN LIPOMATOUS TUMOR BENIGN NEOPLASM
• Lipoma = most common benign soft tissue tumor • Represents up to 50% soft tissue neoplasms
• Common cause of palpable mass & referral for imaging • Multiple lesions in 5-15% patients • Superficial lipoma: subcutaneous, more common • Deep lipoma: retroperitoneal, intramuscular
• Difficult to distinguish from well-differentiated liposarcoma
A
B IMAGING CHARACTERISTICS May have thin capsule; should NOT enhance CT: fat attenuation, may have thin septations US: echogenic MRI: fat signal on all sequences

16
A fluid-signal intensity mass with fat-containing septations and post-contrast enhancement is incidentally noted in the paraspinal musculature on an abdominal MRI. This finding should prompt consideration of which primary tumor:
QUESTION QUESTION
A. Well-differentiated liposarcoma
B. De-differentiated liposarcoma
C. Myxoid/round cell liposarcoma
D. Pleomorphic liposarcoma

17
LIPOSARCOMA
Liposarcoma (LPS) type
Demographics Imaging
Atypical lipomatous tumor (ALT), well-differentiated LPS, de-differentiated LPS
- Most common LPS type (50%)
- Sites: Extremities (ALT); Inguinal/paratesticular; retroperitoneum
- Metastases: lung, liver
- Mostly fat - Septations > 2 mm - Nodules/masses: - < 1 cm well-
differentiated; - > 1 cm de-differentiated
Myxoid/round cell LPS
- Young adults - Sites: lower extremities -
intramuscular - Metastases: paraspinal, bone,
contralateral extremity, retroperitoneum
- Multi-loculated fluid-containing mass
- Fat-containing septations; overall <25% fat
- Diffuse enhancement
Pleomorphic LPS - Older adults (mean age 65) - Sites: extremities – deep soft
tissues - Metastases: lung, liver
- Solid mass with minimal fat
- May have internal hemorrhage/necrosis
Sagittal CECT demonstrating a fat-containing mass with enhancing septations and nodules in the left inguinal region. Biopsy confirmed well-differentiated liposarcoma.
MALIGNANT NEOPLASM
Answer: C. Myxoid/round cell liposarcoma May appear cystic on MRI - contrast is essential to differentiate from a cyst.

18
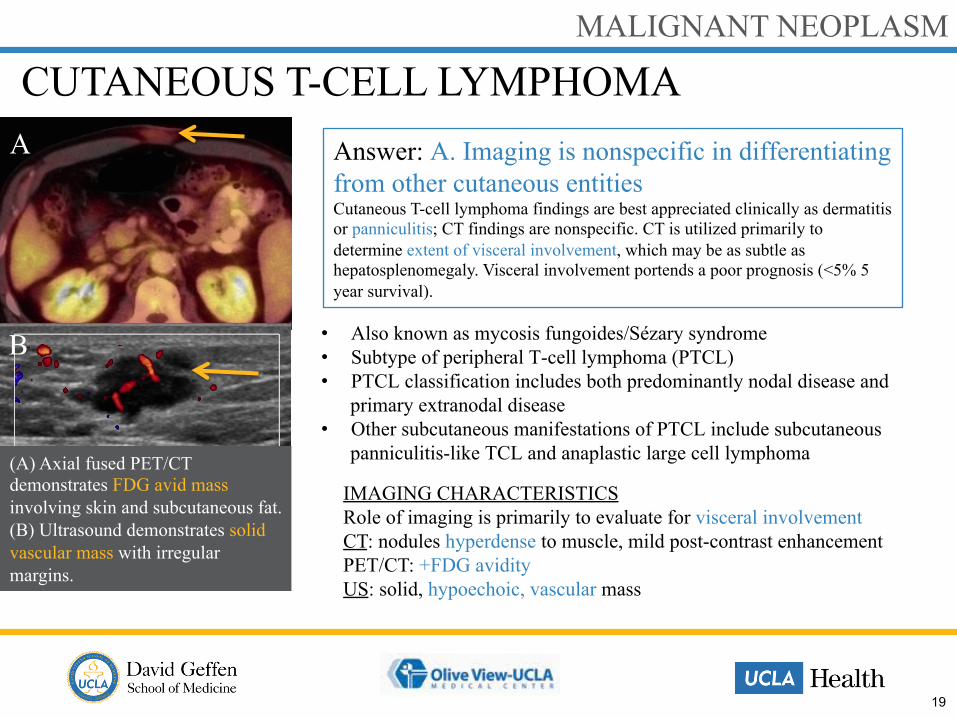
Regarding cutaneous T-cell lymphoma: A. Imaging is nonspecific in differentiating from other cutaneous entities
B. Patients typically have no clinical skin findings
C. Skin lesions usually show no FDG avidity
D. Visceral and nodal involvement has >75% 5 year survival rate
QUESTION
19
CUTANEOUS T-CELL LYMPHOMA MALIGNANT NEOPLASM
• Also known as mycosis fungoides/Sézary syndrome • Subtype of peripheral T-cell lymphoma (PTCL) • PTCL classification includes both predominantly nodal disease and
primary extranodal disease • Other subcutaneous manifestations of PTCL include subcutaneous
panniculitis-like TCL and anaplastic large cell lymphoma
IMAGING CHARACTERISTICS Role of imaging is primarily to evaluate for visceral involvement CT: nodules hyperdense to muscle, mild post-contrast enhancement PET/CT: +FDG avidity US: solid, hypoechoic, vascular mass
(A) Axial fused PET/CT demonstrates FDG avid mass involving skin and subcutaneous fat. (B) Ultrasound demonstrates solid vascular mass with irregular margins.
Answer: A. Imaging is nonspecific in differentiating from other cutaneous entities Cutaneous T-cell lymphoma findings are best appreciated clinically as dermatitis or panniculitis; CT findings are nonspecific. CT is utilized primarily to determine extent of visceral involvement, which may be as subtle as hepatosplenomegaly. Visceral involvement portends a poor prognosis (<5% 5 year survival).
A
B

20
METASTASES MALIGNANT NEOPLASM
(A) Axial CECT demonstrates a hypoenhancing subcutaneous nodule in the anterior abdominal wall. Biopsy confirmed metastatic pancreatic adenocarcinoma.
(B) Axial CECT demonstrates hyperenhancing subcutaneous nodules in the lateral anterior wall. Biopsy confirmed metastatic cervical squamous cell carcinoma.
(C) Axial CECT demonstrating isodense subcutaneous nodules in the left rectus and left gluteal regions. Biopsy confirmed lymphoma.
• Primary epithelial tumors are the most common skin malignancies (basal cell carcinoma, squamous cell carcinoma, melanoma)
• Cutaneous metastases from internal/visceral malignancies are rare, occurring in less than 10% cases• Spread is from direct invasion (including at surgical sites), hematogenous, and/or lymphatic spread
• Breast and colon cancer are the most common cutaneous metastases in women; lung and colon cancer are the most common in men
A B C

21
A. Seroma
B. Hematoma
C. Bunched rectus abdominus musculature
D. Flap necrosis
QUESTION
What complication of abdominoplasty is shown?

22
LIPOSUCTION/ABDOMINOPLASTY IATROGENIC
IMAGING CHARACTERISTICS Liposuction: (A) linear densities radiating from skin surface (cannula tracts); overlying skin thickening Abdominoplasty: (B) bunching together of rectus abdominus muscles (due to surgical plication) is an expected post-operative appearance
A B
Answer: B. Hematoma Active contrast extravasation is present in the left gluteal soft tissues. Management included embolization of the bleeding vessel (pre-embolization angiogram shown). Seroma is the most common early post-operative complication, though is not seen in this case.

23
INJECTION GRANULOMA IATROGENIC
• Silicone injection for aesthetic gluteal augmentation is not FDA-approved in the USA; presumably patients with this finding were treated outside the USA (or illegally)
• Imaging appearance of injected silicone is varied, as demonstrated above.
(A) Coronal CT shows ill-defined nodular and confluent soft tissue density within the gluteal subcutaneous fat, with scattered foci of air. Occasional calcifications suggest granulomatous reaction. (B) Axial CECT of a different patient demonstrates innumerable round and oval hyperdense nodules in the gluteal fat.
BA
Not all gluteal injections are silicone. (A) Coronal T2W MRI shows intramuscular and subcutaneous hyperintense nodules. This patient acknowledged receiving steroid injections. (B) Axial T1W contrast-enhanced MRI in arterial phase and (C) portal venous phase show an arterially enhancing lesion with washout. Biopsy confirmed adenoma.
A
B
C

24
Subcutaneous foreign bodies are generally visible on radiographs except which of the following:
A. Plastic
B. Glass
C. Gold
D. Wood
QUESTION
Ultrasound demonstrates a fragment of a palm frond in the subcutaneous tissues. The fragment is echogenic with surrounding hypoechoic “halo” of edema.

25
IATROGENIC/TRAUMA
• Subcutaneous foreign objects may be known at the time of imaging or may be discovered incidentally • Imaging must include evaluation for complications, including abscess formation, proximity to vital vascular
structures/organs, and/or underlying osteomyelitis
FOREIGN BODY
(A) Axial CT and (B) associated topogram image show scattered areas of punctate metallic densities, reported to be buckshot following an assault. The topogram better demonstrates the overall distribution of involvement. (C) Coronal CT of a different patient performed for malignancy follow up demonstrates multiple linear hyperdensities representing tips of acupuncture needles from the practice of Hari acupuncture. A B C
Answer: D. Wood Organic materials such as plants and wood are initially radio-lucent and may be difficult to visualize on radiographs if no overlying skin change or subcutaneous gas is present. ALL subcutaneous foreign bodies are echogenic on ultrasound.

A. Laparoscopy
B. Ultrasound
C. CT
D. MRI
26
The initial imaging modality to evaluate for unknown location of undescended testis is:
QUESTION

27
UNDESCENDED TESTIS CONGENITAL
• Undescended (cryptorchid) testes increase risk for infertility, torsion, inguinal hernia, and malignant degeneration • Risk of malignancy is increased 5-10x regardless of whether early orchiopexy (recommended by age 6-12
months) is performed • Malignancy risk is also increased in the contralateral testis
A
(C) Axial CECT in a different patient shows absent right spermatic cord in this patient with known cryptorchidism. (D) Coronal CECT reveals a large heterogeneous mass arising from the undescended right testis, which is seen in the inguinal canal. Biopsy confirmed germ cell tumor.
C D(A) Scrotal ultrasound with normal right testis; left testis not identified in scrotum or inguinal canal. (B) Coronal T2W MRI shows the left testis in the pelvis adjacent to external iliac vessels.
A B
Answer: B. Ultrasound Ultrasound remains the initial modality of choice to evaluate the scrotum and inguinal canal in the setting of non-palpable testis. MRI is more sensitive and specific for evaluating the position of intra-abdominal testes. Laparoscopy can be performed if the testis is not visualized on MRI.

A. Squamous cell carcinoma
B. Adenocarcinoma
C. Transitional cell carcinoma
D. Undifferentiated carcinoma
28
The most common malignancy to develop in a urachal remnant is:
QUESTION

29
URACHAL REMNANT CONGENITAL
• Congenital abnormalities of the urachus are due to incomplete resorption of the allantois • Spectrum of anomalies includes
• Patent urachus (50%) – diagnosed neonatally • Urachal cyst (30%) – often infected at time of diagnosis • Urachal sinus (15%) – dilatation at umbilical aspect • Urachal diverticulum (5%) – dilatation at vesicular aspect
• Complications: infection, calculus formation, adenocarcinoma
(A) Axial CECT demonstrates midline rim-enhancing fluid collections involving the rectus musculature. (B) Sagittal CECT shows the collection contiguous with the dome of the bladder extending toward the umbilicus. The appearance is most suggestive of an infected urachal remnant, likely a urachal diverticulum. A B
Answer: B. Adenocarcinoma Adenocarcinoma is the most common malignancy of the urachus, though it is a very rare primary bladder neoplasm (<2% primary bladder tumors). Up to 34% of bladder adenocarcinomas are urachal. Development of adenocarcinoma is thought to be secondary to epithelial metaplasia followed by malignant degeneration.

Familiarity with the spectrum of subcutaneous abdominal masses and mass-like pathology will enable the radiologist to provide more accurate interpretation of these lesions and direct further evaluation and management.
30
CONCLUSION
Beaman FD, Kransdorf MJ, Andrews TR, et al. Superficial soft-tissue masses: analysis, diagnosis, and differential considerations. Radiographics 2007;27:509-523. Casillas J, Sais GJ, Greve JL, Iparraguirre MC, Morillo G. Imaging of intra- and extraabdominal desmoid tumors. Radiographics 1991;11:959-968. de Heredia LL, hauptfleisch J, Hughes R, et al,. Magnetic resonance imaging of pressure sores in spinal cord injured patients: accuracy in predicting osteomyelitis. Top Spinal Cord Inj Rehabil 2012;18:146-148 Frank SJ, Flusberg M, Friedman S, et al. Aesthetic surgery of the buttocks: imaging appearance. Skel Radiol 2014;43:133-139. Gidawney R, Badler RL, Yam BL, et al. Endometriosis of abdominal and pelvic wall scars: multimodality imaging findings, pathologic correlation, and radiologic mimics. Radiographics 2012;32:2031-2043. Jarraya M, Hayashi D, de Villiers RV, et al. Multimodality imaging of foreign bodies of the musculoskeletal system. AJR 2014;203:W92-W102. Juan YH, Saboo SS, Tirumani SH, et al. Malignant skin and subcutaneous neoplasms in adults: multimodality imaging with CT, MRI, and 18F-FDG PET/CT. AJR 2014;202:W422-W438. Jung SC, Chung JW, Jae HJ, et al. Unusual causes of varicose veins in the lower extremities: CT venographic and doppler US findings. Radiographics 2009;29:525-536. Koster IM, Cleyndert P, Giard RWM. Urachal carcinoma. Radiographics 2009;29:939-942 La Barge DV, Salzman KL, Harnsberger HR, et al. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): imaging manifestations in the head and neck. AJR 2008;191:W299-W306. Levy AD, Patel N, Dow N, Abbott RM, Miettinen M, Sobin LH. Abdominal neoplasms in patients with neurofibromatosis type 1: radiologic-pathologic correlation. Radiographics 2005;25:455-480. Murphey MD, Carroll JF, Flemming DJ, et al. Benign musculoskeletal lipomatous lesions. Radiographics 2004; 24:1433-1466 Murphey MD, Ruble CM, Tyszko SM, et al. Musculoskeletal fibromatoses: radiologic-pathologic correlation. Radiographics 2009; 29:2143-2176. Rimola J, Perendreu J, Falco J. Percutaneous arterial embolization in the management of rectus sheath hematoma. AJR 2007;188:W497-502.
REFERENCES
Contact: [email protected]