skeletal system€¦ · chapter 7 skeletal system 1. 7.1 introduction a. bones are very active,...
TRANSCRIPT
Chapter 7
Skeletal System
1
7.1 Introduction
A. Bones are very active, living tissues
B. Each bone is made up of several types of tissues (bone,
cartilage, dense connective tissue, blood, and nervous tissue)
and so is an organ.
C. Bone functions include: muscle attachment, protection and
support of soft tissues, blood cell production, and storage of
inorganic salts.
2
7.2 Bone Structure
A. Classification of bones according to shape
1. Long – Ex. – arm and leg bones
2. Short – Ex. – bones of the wrist and ankles
a. Sesamoid (round) bones – Ex. – patella
3. Flat – Ex. – ribs, scapula, skull bones
4. Irregular – Ex. – vertebrae, facial bones
3
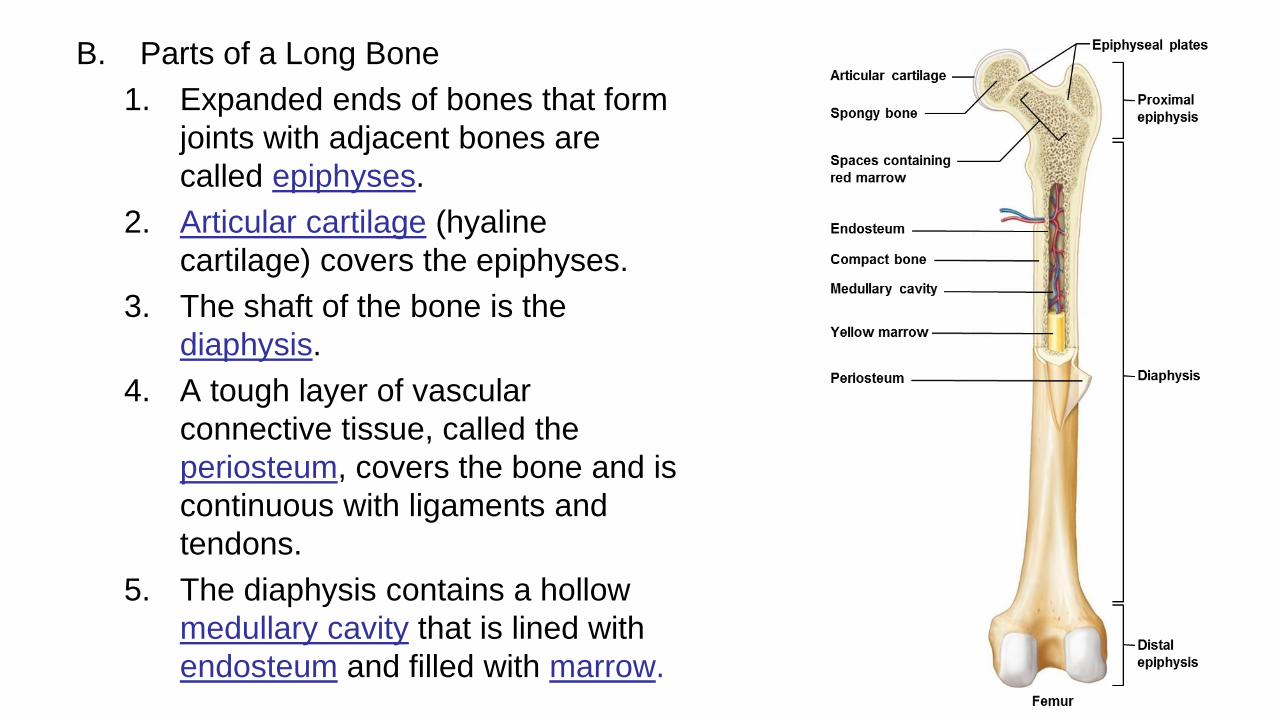
B. Parts of a Long Bone
1. Expanded ends of bones that form
joints with adjacent bones are
called epiphyses.
2. Articular cartilage (hyaline
cartilage) covers the epiphyses.
3. The shaft of the bone is the
diaphysis.
4. A tough layer of vascular
connective tissue, called the
periosteum, covers the bone and is
continuous with ligaments and
tendons.
5. The diaphysis contains a hollow
medullary cavity that is lined with
endosteum and filled with marrow. 4
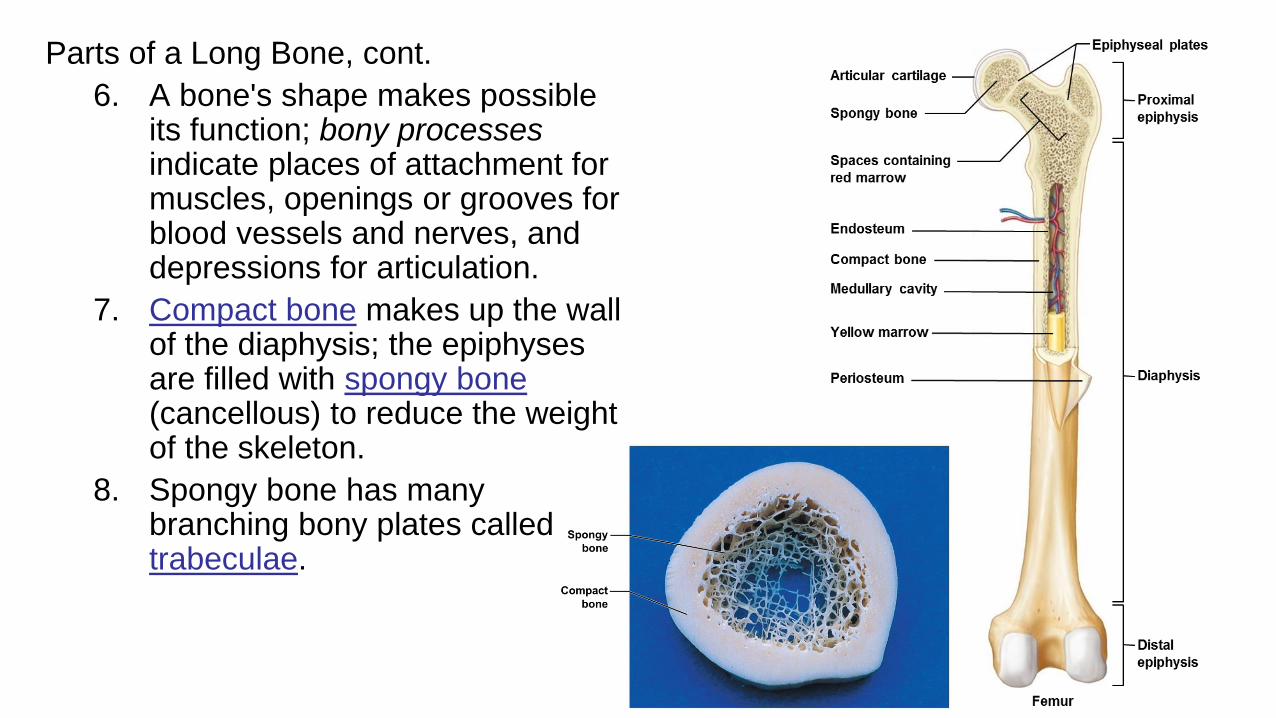
Parts of a Long Bone, cont.
6. A bone's shape makes possible its function; bony processesindicate places of attachment for muscles, openings or grooves for blood vessels and nerves, and depressions for articulation.
7. Compact bone makes up the wall of the diaphysis; the epiphyses are filled with spongy bone(cancellous) to reduce the weight of the skeleton.
8. Spongy bone has many branching bony plates called trabeculae.
5
C. Microscopic structure
1. Bone cells (osteocytes) are located within lacunae that lie in concentric circles around central (Haversian) canals.
2. Osteocytes pass nutrients and gasses in the matrix via canaliculi.
3. Extracellular matrix of bone consists mainly of collagen and inorganic salts.
a. Collagen provides strength and resilience
b. Inorganic salts provides hardness and resistance to crushing
6
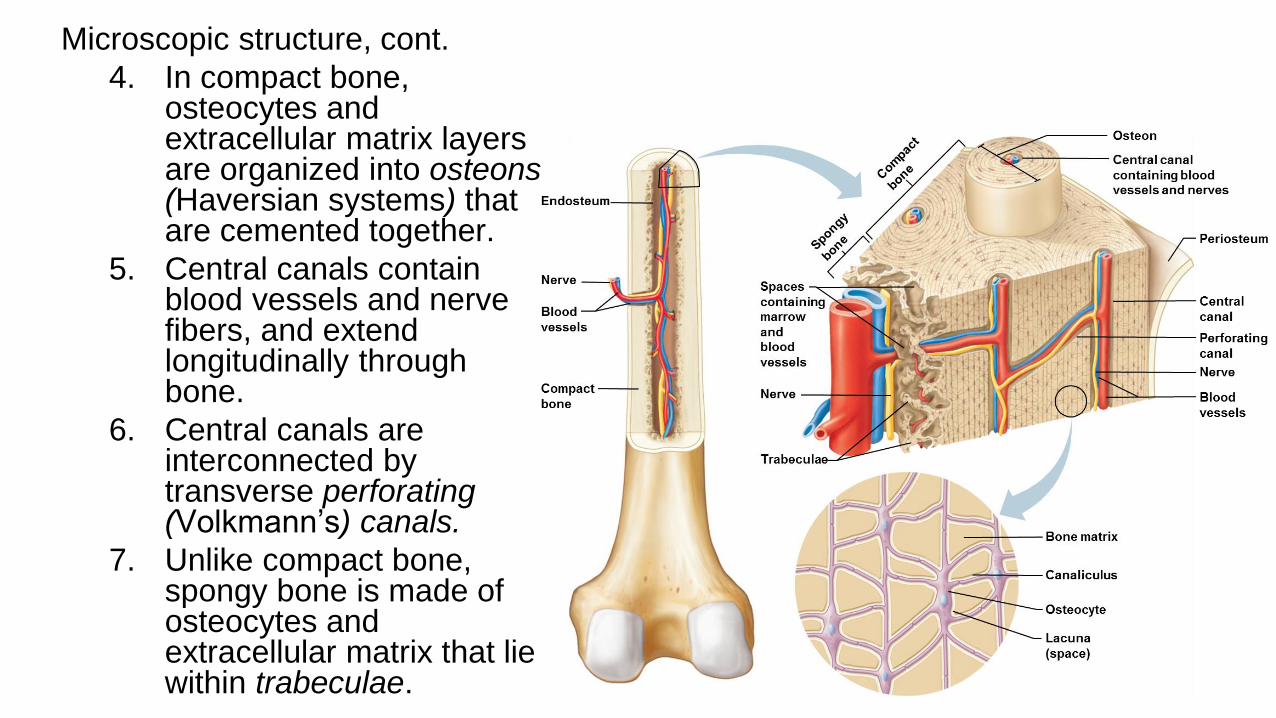
Microscopic structure, cont.
4. In compact bone, osteocytes and extracellular matrix layers are organized into osteons (Haversian systems) that are cemented together.
5. Central canals contain blood vessels and nerve fibers, and extend longitudinally through bone.
6. Central canals are interconnected by transverse perforating (Volkmann’s) canals.
7. Unlike compact bone, spongy bone is made of osteocytes and extracellular matrix that lie within trabeculae. 7
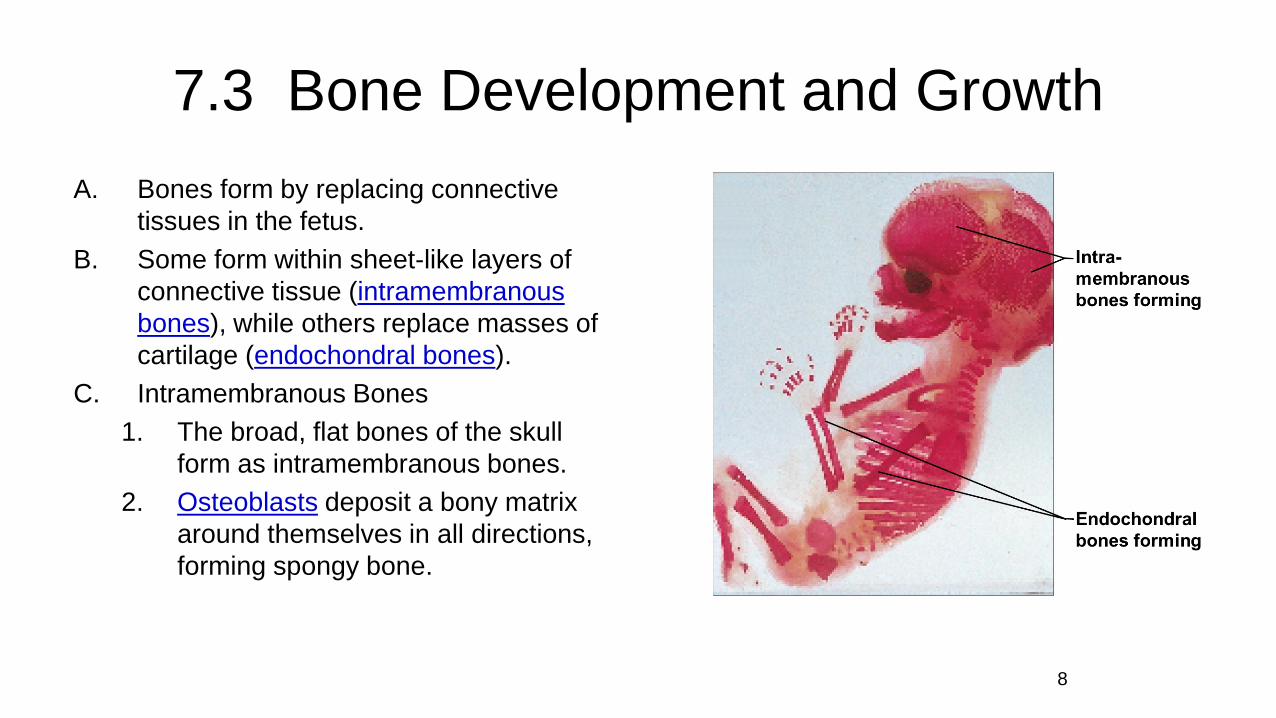
7.3 Bone Development and Growth
A. Bones form by replacing connective
tissues in the fetus.
B. Some form within sheet-like layers of
connective tissue (intramembranous
bones), while others replace masses of
cartilage (endochondral bones).
C. Intramembranous Bones
1. The broad, flat bones of the skull
form as intramembranous bones.
2. Osteoblasts deposit a bony matrix
around themselves in all directions,
forming spongy bone.
8

Intramembranous bones, cont.
3. Once the deposited bony matrix completely
surrounds the osteoblasts, they are then called
osteocytes.
4. Cells of the membranous tissue that lie outside
the developing bone give rise to the
periosteum.
5. Osteoblasts on the inside of the periosteum
form a layer of compact bone over the spongy
bone.
6. The formation of bone is referred to as
ossification.
9
D. Endochondral bones
1. Most of the bones of the skeleton fall into this category.
2. They first develop as hyaline cartilage models shaped like the future bones and are then replaced with bone.
3. Cartilage is broken down in the diaphysis and progressively replaced with bone while the periosteum develops on the outside.
4. Disintegrating cartilage is invaded by blood vessels and osteoblasts that first form spongy bone at the primary ossification center in the diaphysis.
10
Endochondral bones, cont.
5. Osteoblasts from the periosteum lay down
compact bone around the primary ossification
center.
6. Secondary ossification centers appear later in
the epiphyses.
7. A band of hyaline cartilage, the epiphyseal
plate, remains between the two ossification
centers.
8. Layers of cartilage cells undergoing mitosis
make up the epiphyseal plate.
11
Endochondral bones, cont.
9. Osteoclasts break down the calcified matrix and are replaced with
bone-building osteoblasts that deposit bone in place of calcified
cartilage.
10.A long bone continues to lengthen while the cartilaginous cells of
the epiphyseal plate are active. Once the plate ossifies, the bone
is done growing in length.
11.The medullary cavity forms in the diaphysis due to the activity of
osteoclasts.
12. Increases in thickness are due to ossification underneath the
periosteum, while epiphyseal plates are responsible for
lengthening bones.
12
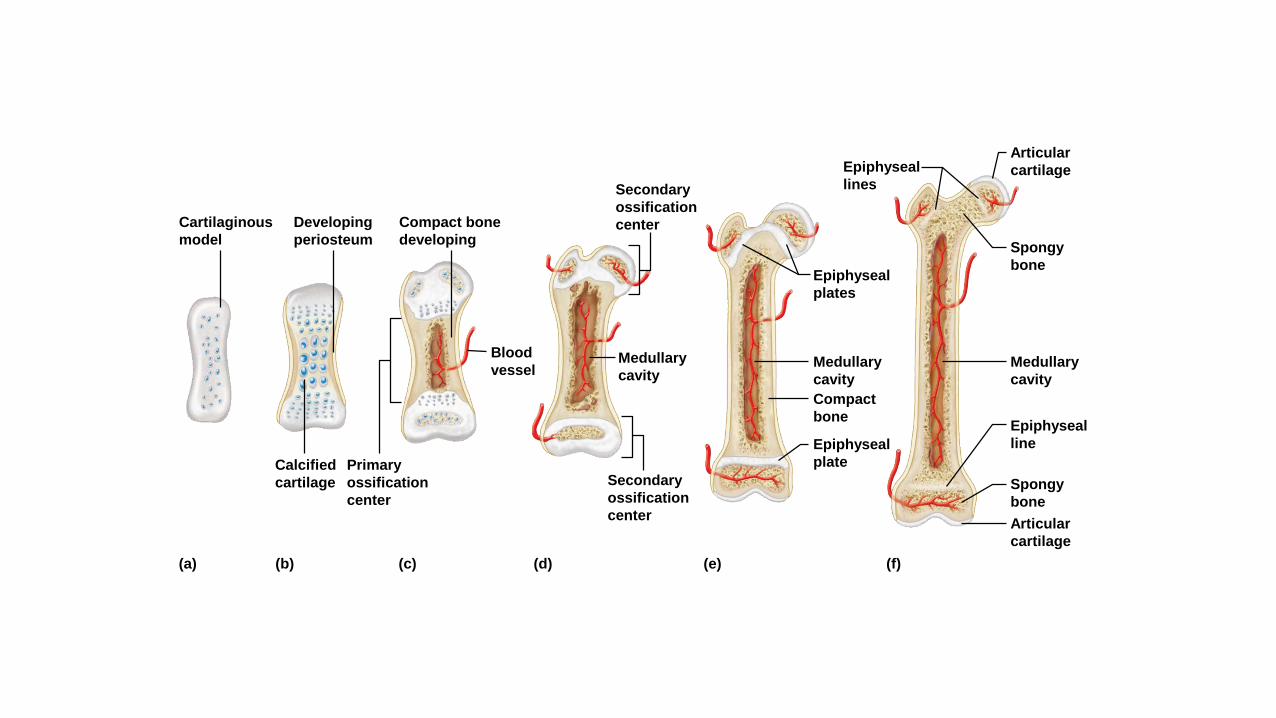
(b) (c) (d) (e) (f)(a)
Compact bone
developing
Developing
periosteum
Cartilaginous
model
Blood
vesselMedullary
cavityMedullary
cavity
Compact
bone
Epiphyseal
plate
Epiphyseal
plates
Medullary
cavity
Epiphyseal
line
Spongy
bone
Articular
cartilage
Spongy
bone
Articular
cartilage
Secondary
ossification
center
Secondary
ossification
center
Epiphyseal
lines
Calcified
cartilage
Primary
ossification
center
E. Homeostasis of bone tissue
1. Osteoclasts tear down and osteoblasts build
bone throughout the lifespan with the
processes of resorption and deposition, with
an average of 3% to 5% of bone calcium
exchanged each year.
2. This remodeling process is controlled by
hormones that regulate blood calcium levels.
3. Physical exercise with muscles pulling on
bones will stress the bones, which will increase
in thickness and strength.
14
F. Factors affecting bone development, growth, and
repair
1. Nutrition – vitamin D is needed for calcium
absorption
2. Hormonal secretions
a. Growth hormone – stimulates division of
cartilage cells of the epiphyseal plate
b. Sex hormones – stimulate ossification of the
epiphyseal plates to end growth in height
15

7.4 Bone Function
A. Support and protection
1. Bones give shape to the head, face, thorax, and limbs.
2. Bones such as the pelvis and lower limbs provide support for
the body’s weight.
3. Bones of the skull protect the eyes, ears, and brain.
4. Bones of the rib cage and shoulder girdle protect the heart
and lungs.
5. Bones of the pelvic girdle protect lower abdominal and
reproductive organs.
16
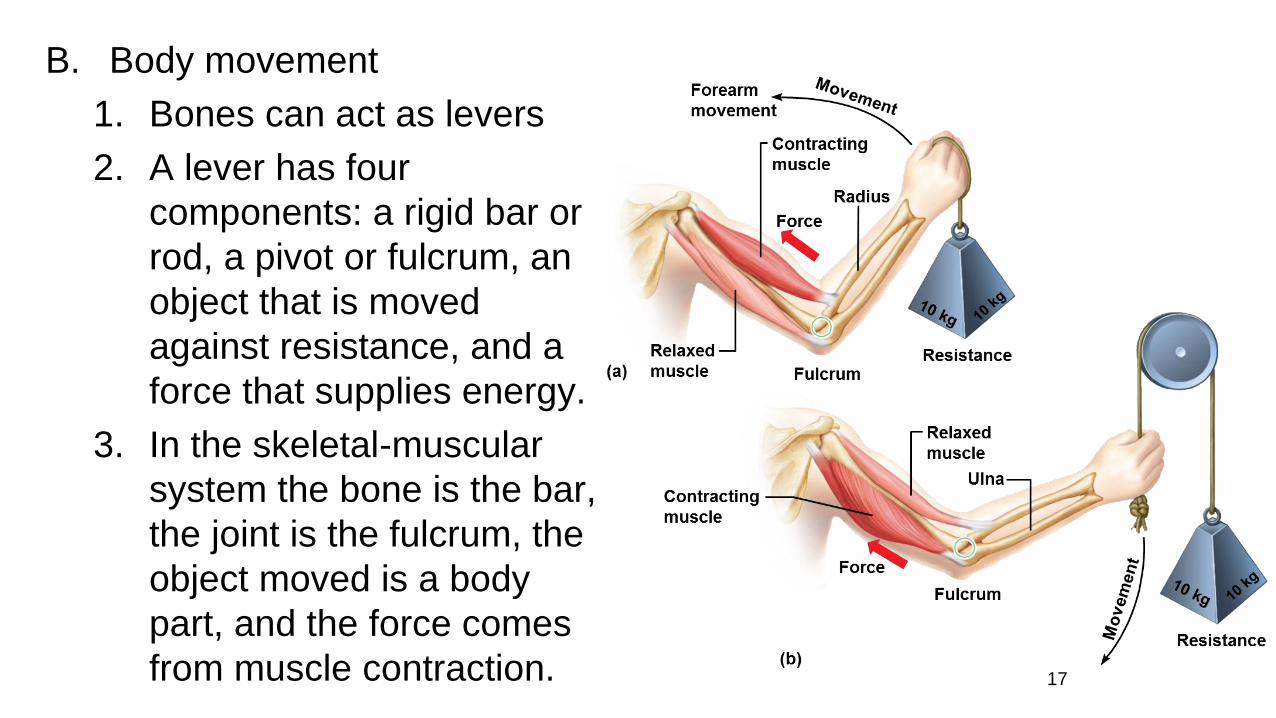
B. Body movement
1. Bones can act as levers
2. A lever has four
components: a rigid bar or
rod, a pivot or fulcrum, an
object that is moved
against resistance, and a
force that supplies energy.
3. In the skeletal-muscular
system the bone is the bar,
the joint is the fulcrum, the
object moved is a body
part, and the force comes
from muscle contraction. 17
C. Blood cell formation
1. Blood cells begin to form through hematopoiesis in the yolk sac
2. They are later manufactured in the liver and spleen and then
finally formed in the bone marrow.
3. Two kinds of marrow occupy the medullary cavities and the
larger central canals of bone.
a. Red marrow occupies the spongy bone of the skull, ribs, sternum,
clavicles, vertebrae, and pelvis in adults. It functions in the formation
of red blood cells, white blood cells, and platelets. Its color comes
from the O2 carrying pigment hemoglobin.
b. Yellow marrow stores fat and occupies most cavities of bone in
adults.
18
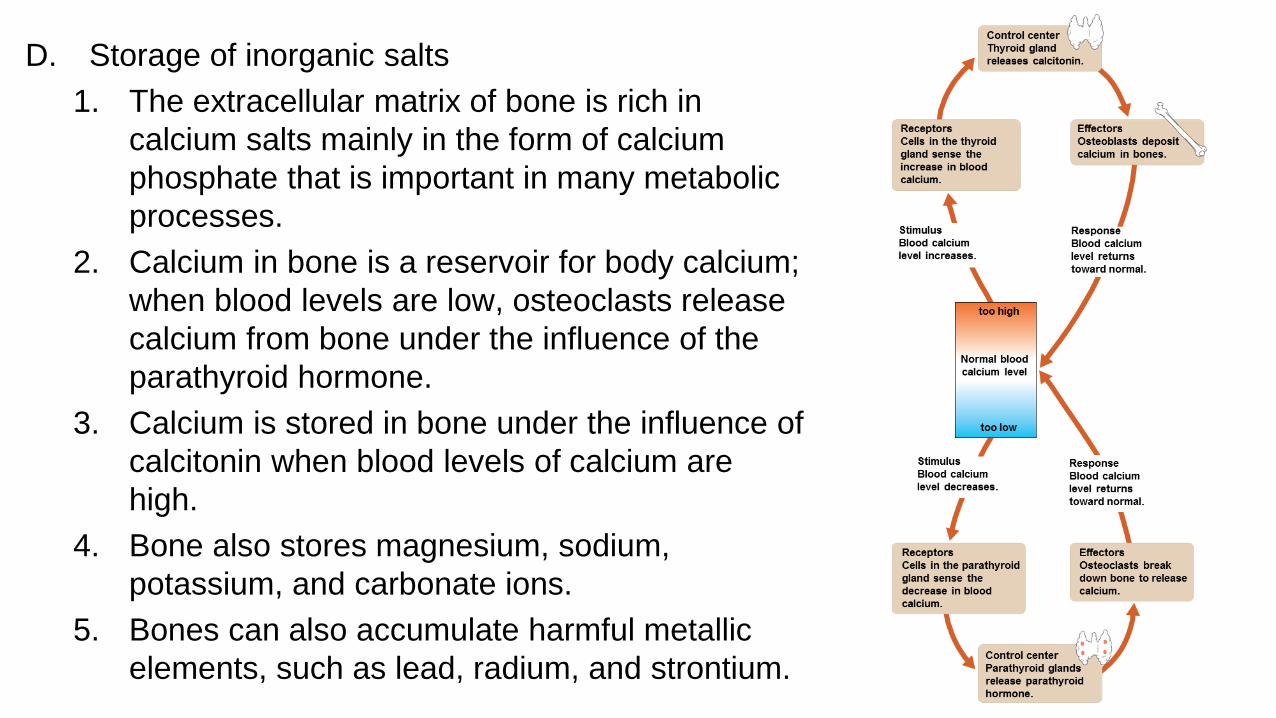
D. Storage of inorganic salts
1. The extracellular matrix of bone is rich in
calcium salts mainly in the form of calcium
phosphate that is important in many metabolic
processes.
2. Calcium in bone is a reservoir for body calcium;
when blood levels are low, osteoclasts release
calcium from bone under the influence of the
parathyroid hormone.
3. Calcium is stored in bone under the influence of
calcitonin when blood levels of calcium are
high.
4. Bone also stores magnesium, sodium,
potassium, and carbonate ions.
5. Bones can also accumulate harmful metallic
elements, such as lead, radium, and strontium. 19
7.5 Skeletal Organization
A. The axial skeleton consists of the bony and cartilaginous parts
that support the and protect the head, neck and trunk. Includes
the:
1. Skull – cranium and facial bones
2. Hyoid bone – supports the tongue and aids in swallowing
3. Vertebral column
4. Thoracic cage – ribs and sternum
20
B. The appendicular skeleton consists of the bones
of the upper and lower limbs and the bones that
anchor the limbs to the axial skeleton. Includes
the:
1. Pectoral girdle – clavicle and scapula
2. Upper limbs – humerus, ulna, radius, carpals,
metacarpals, and phalanges
3. Pelvic girdle – 2 hip bones
4. Lower limbs – femur, patella, tibia, fibula,
tarsals, metatarsals, and phalanges
21

22
23

24
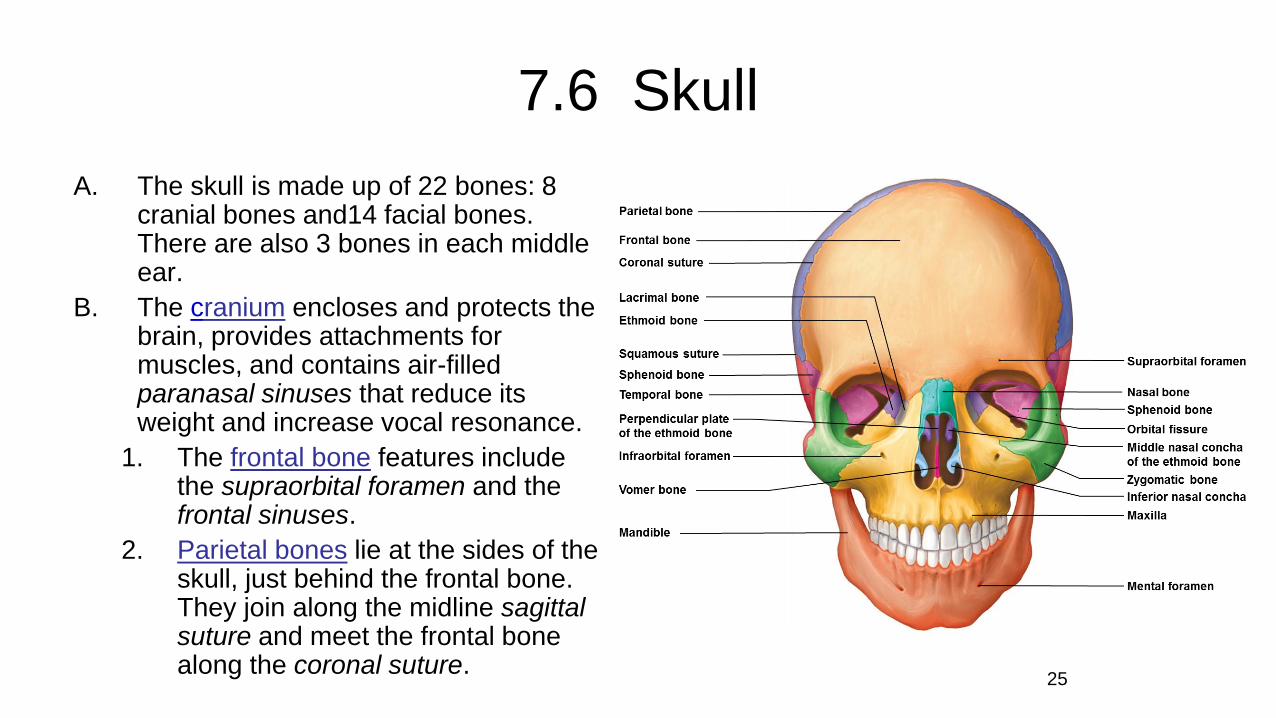
7.6 Skull
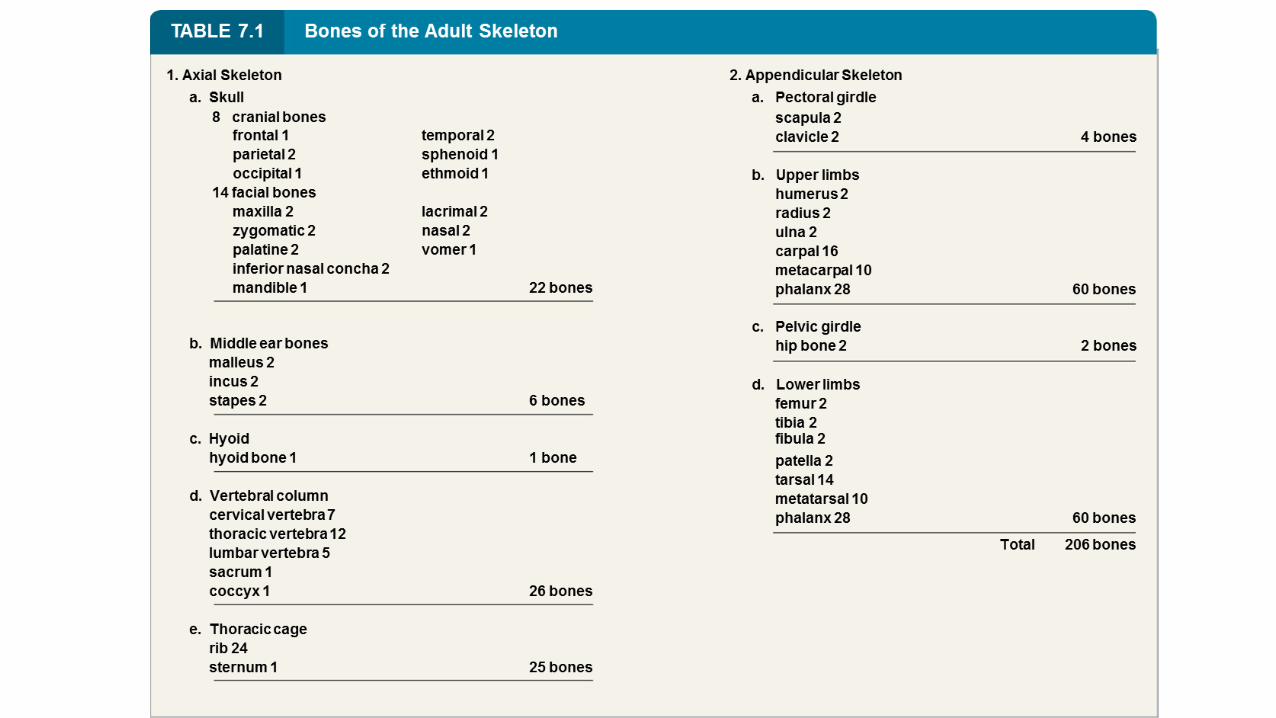
A. The skull is made up of 22 bones: 8 cranial bones and14 facial bones. There are also 3 bones in each middle ear.
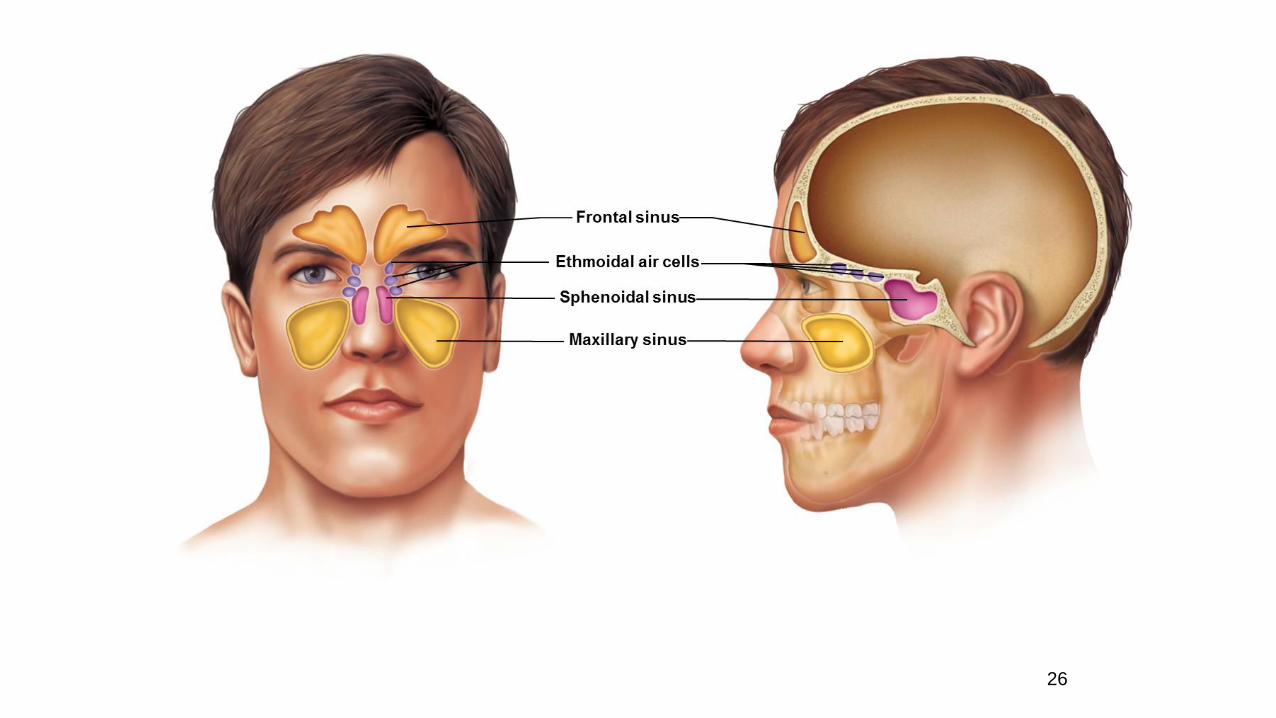
B. The cranium encloses and protects the brain, provides attachments for muscles, and contains air-filled paranasal sinuses that reduce its weight and increase vocal resonance.
1. The frontal bone features include the supraorbital foramen and the frontal sinuses.
2. Parietal bones lie at the sides of the skull, just behind the frontal bone. They join along the midline sagittal suture and meet the frontal bone along the coronal suture.
25
26
Cranium, cont.
3. The occipital bone forms the back of the skull
and the base of the cranium. Features include
the lambdoid suture, foramen magnum, and
occipital condyles.
4. The temporal bones form parts of the sides
and base of the cranium. Features include the
squamous suture, external acoustic meatus,
mandibular fossae, mastoid process, styloid
process, and zygomatic process.
27
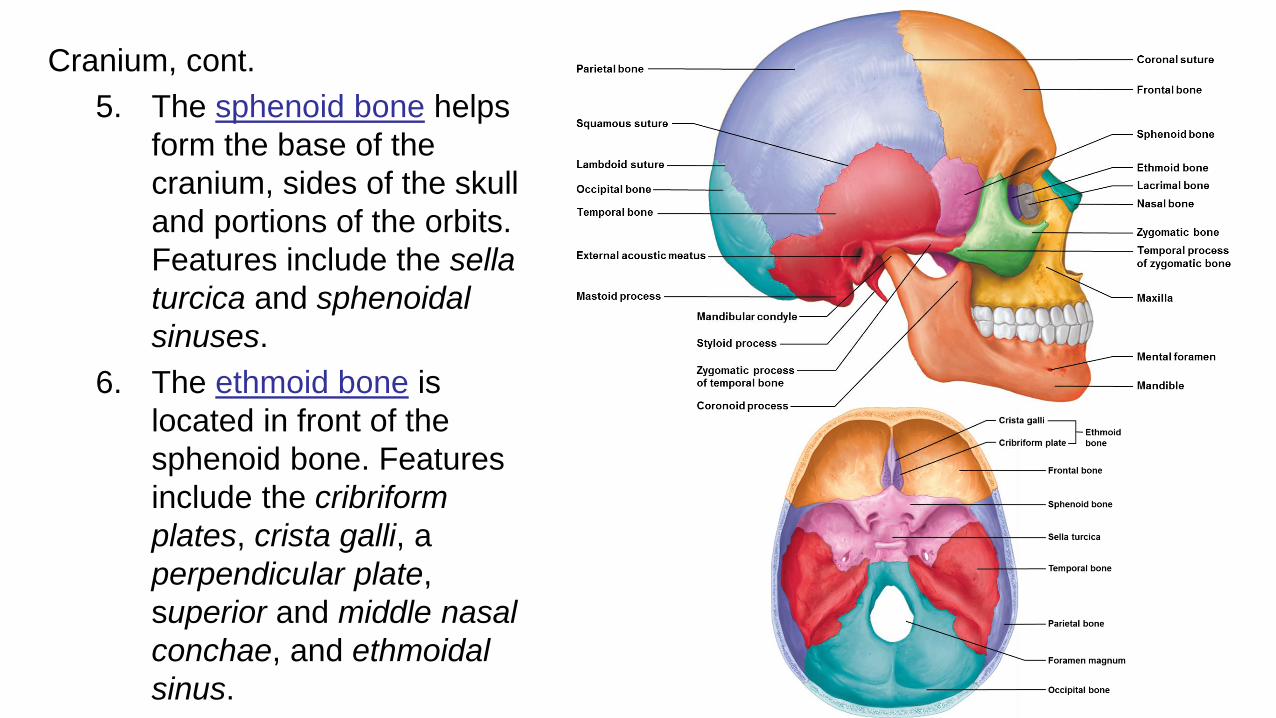
Cranium, cont.
5. The sphenoid bone helps
form the base of the
cranium, sides of the skull
and portions of the orbits.
Features include the sella
turcica and sphenoidal
sinuses.
6. The ethmoid bone is
located in front of the
sphenoid bone. Features
include the cribriform
plates, crista galli, a
perpendicular plate,
superior and middle nasal
conchae, and ethmoidal
sinus.
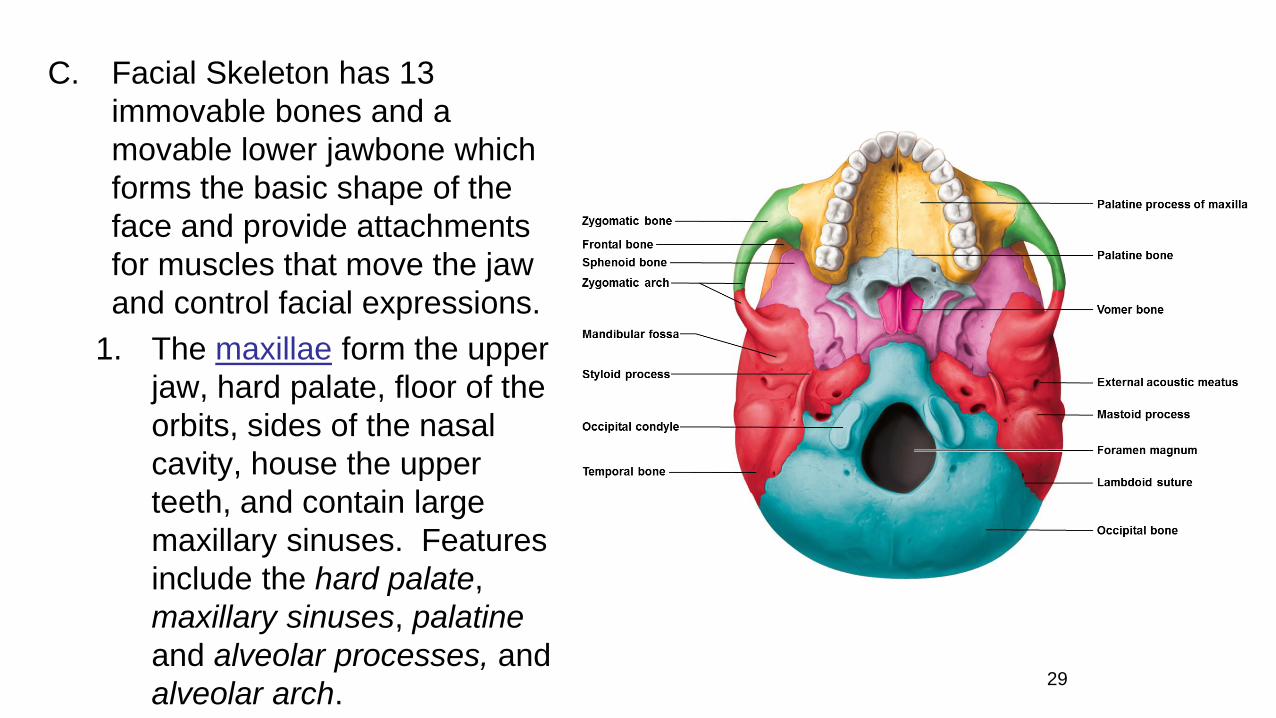
C. Facial Skeleton has 13
immovable bones and a
movable lower jawbone which
forms the basic shape of the
face and provide attachments
for muscles that move the jaw
and control facial expressions.
1. The maxillae form the upper
jaw, hard palate, floor of the
orbits, sides of the nasal
cavity, house the upper
teeth, and contain large
maxillary sinuses. Features
include the hard palate,
maxillary sinuses, palatine
and alveolar processes, and
alveolar arch.29
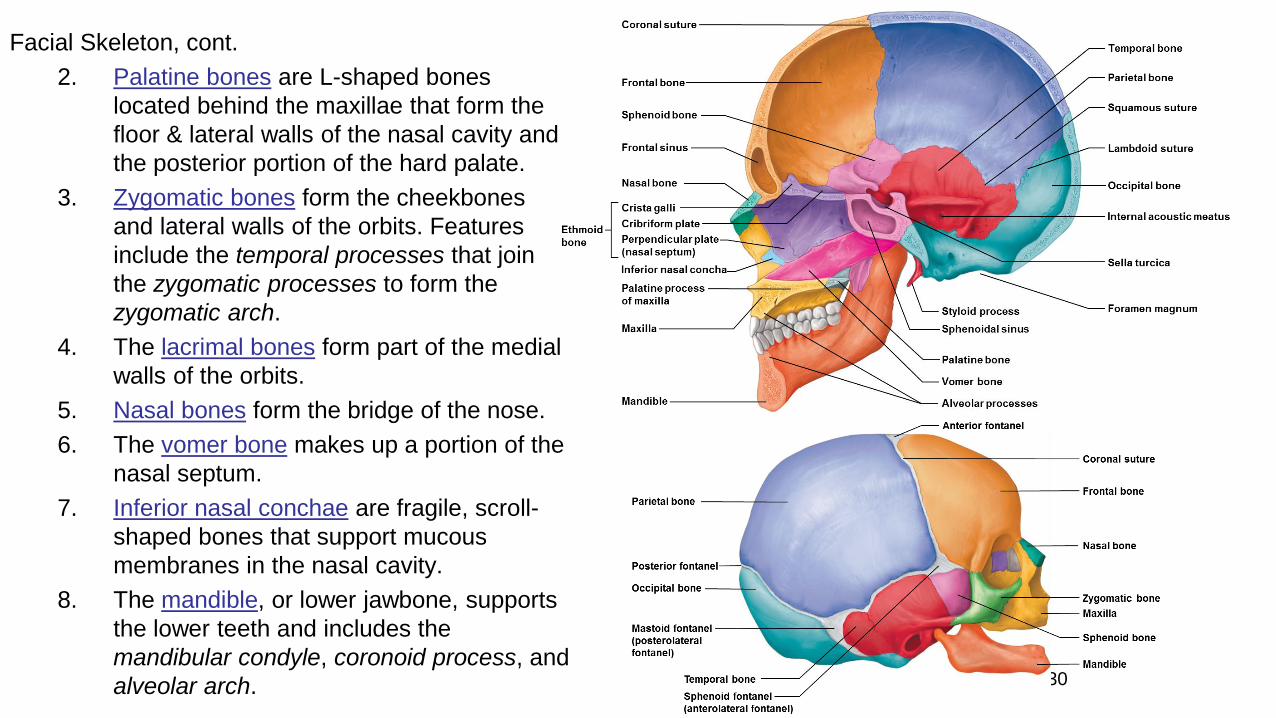
Facial Skeleton, cont.
2. Palatine bones are L-shaped bones
located behind the maxillae that form the
floor & lateral walls of the nasal cavity and
the posterior portion of the hard palate.
3. Zygomatic bones form the cheekbones
and lateral walls of the orbits. Features
include the temporal processes that join
the zygomatic processes to form the
zygomatic arch.
4. The lacrimal bones form part of the medial
walls of the orbits.
5. Nasal bones form the bridge of the nose.
6. The vomer bone makes up a portion of the
nasal septum.
7. Inferior nasal conchae are fragile, scroll-
shaped bones that support mucous
membranes in the nasal cavity.
8. The mandible, or lower jawbone, supports
the lower teeth and includes the
mandibular condyle, coronoid process, and
alveolar arch. 30
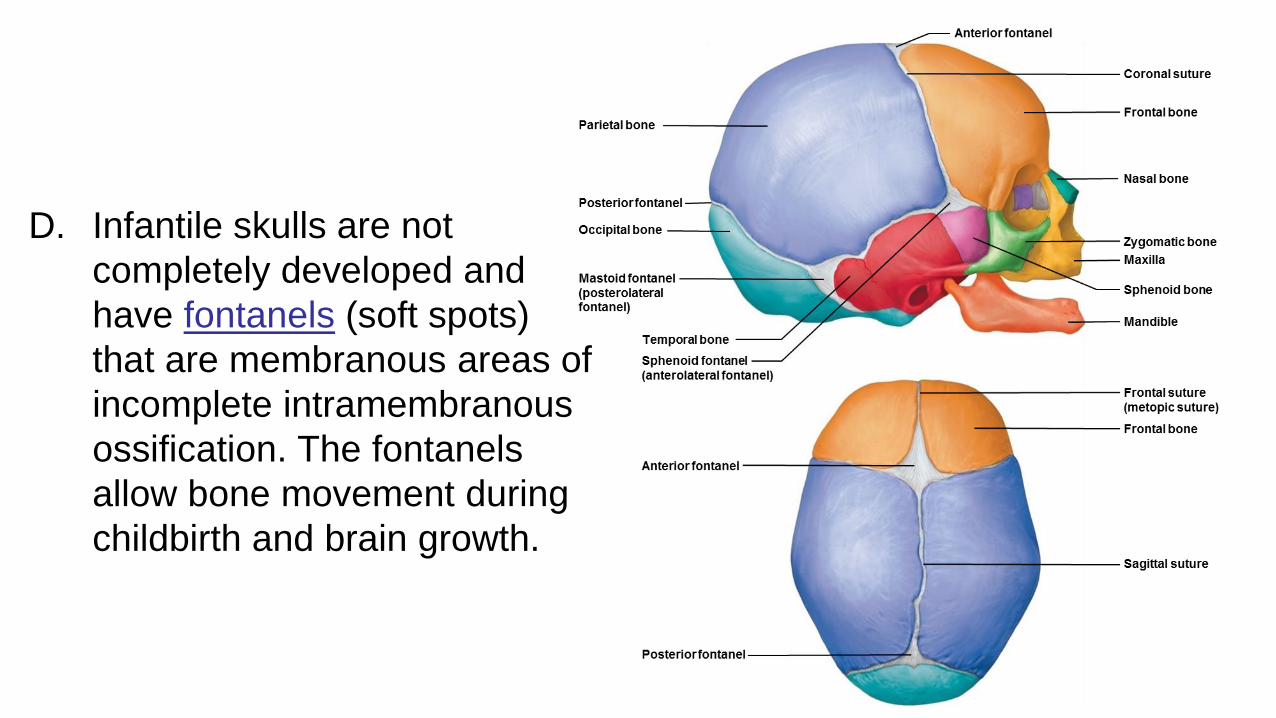
D. Infantile skulls are not
completely developed and
have fontanels (soft spots)
that are membranous areas of
incomplete intramembranous
ossification. The fontanels
allow bone movement during
childbirth and brain growth.
31
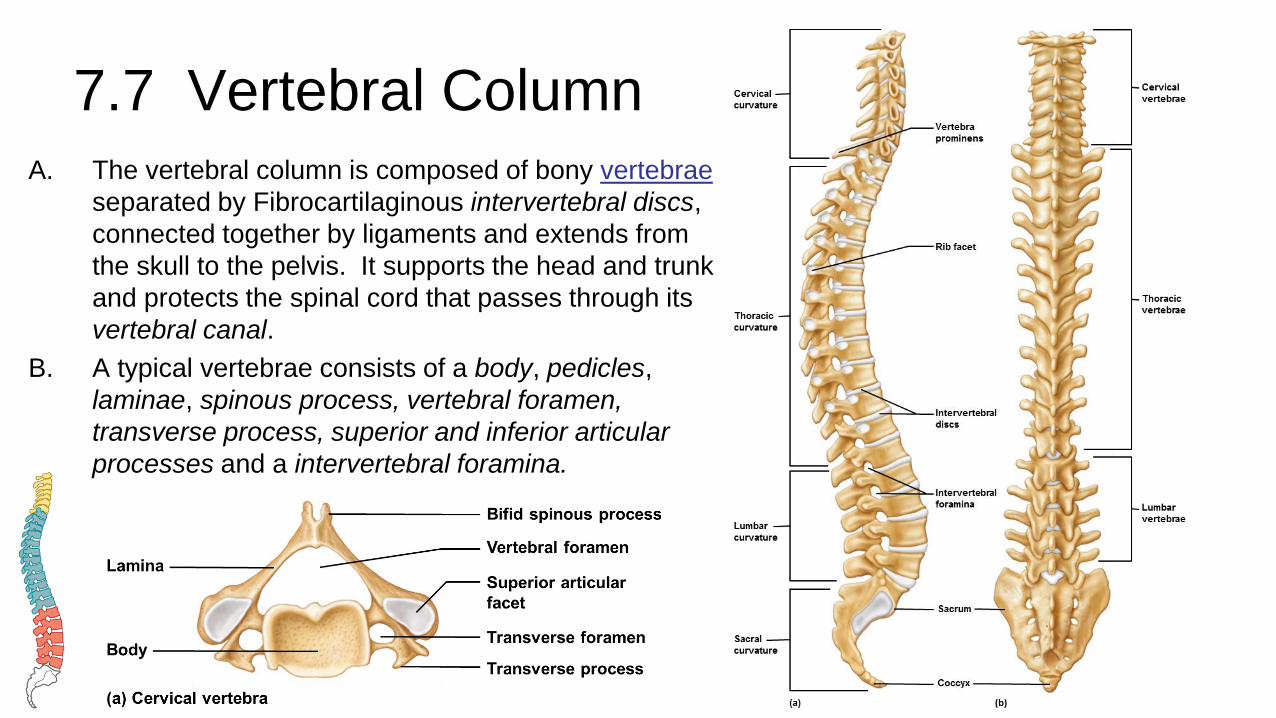
7.7 Vertebral ColumnA. The vertebral column is composed of bony vertebrae
separated by Fibrocartilaginous intervertebral discs,
connected together by ligaments and extends from
the skull to the pelvis. It supports the head and trunk
and protects the spinal cord that passes through its
vertebral canal.
B. A typical vertebrae consists of a body, pedicles,
laminae, spinous process, vertebral foramen,
transverse process, superior and inferior articular
processes and a intervertebral foramina.
32

C. Cervical vertebrae
1. These seven bones comprise the neck and support the head and have distinctive transverse foramina.
2. The first vertebra is the atlas, supports the head. It has two facetsthat articulate with the occipital condyles and has no body or spinous process.
3. The second vertebra is the axis, with its tooth-like dens that pivots within the atlas.
4. Features that separate cervical vertebrae from the rest are the bifid spinous processes and transverse foramina.

D. Thoracic vertebrae
1. Twelve thoracic vertebrae
articulate with the ribs and
are larger and stronger than
the cervical vertebrae.
2. Features include a long,
pointed spinous process and
facets on the side of the
body to articular with the
ribs.
34

E. Lumbar vertebrae
1. The five massive lumbar
vertebrae support the weight of
the body and are located in the
small of the back.
35

F. Sacrum
1. The sacrum is a triangular structure at the base of the vertebral column made up of five
vertebrae fused together into one bone.
2. Features include a ridge of tubercles, posterior sacral foramina, sacral canal, sacral hiatus
and four pairs of anterior sacral foramina.
G. Coccyx
1. The coccyx, tailbone, is the lowest part of the vertebral column and is typically composed
of four fused vertebrae.
36
7.8 Thoracic Cage
A. The thoracic cage includes the ribs, thoracic vertebrae, sternum,
and costal cartilages.
B. It supports the pectoral girdle and upper limbs, protects the
viscera in the thoracic and upper abdominal cavities, and plays
a role in breathing.
37
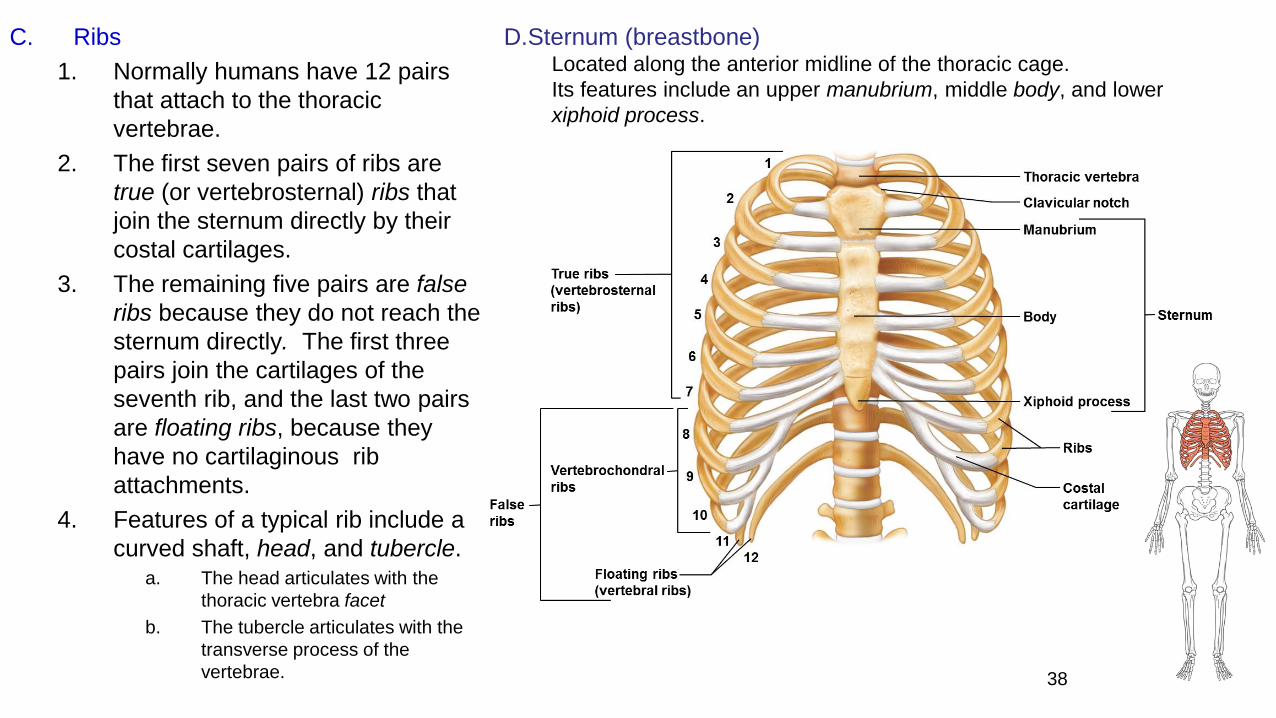
C. Ribs
1. Normally humans have 12 pairs
that attach to the thoracic
vertebrae.
2. The first seven pairs of ribs are
true (or vertebrosternal) ribs that
join the sternum directly by their
costal cartilages.
3. The remaining five pairs are false
ribs because they do not reach the
sternum directly. The first three
pairs join the cartilages of the
seventh rib, and the last two pairs
are floating ribs, because they
have no cartilaginous rib
attachments.
4. Features of a typical rib include a
curved shaft, head, and tubercle.a. The head articulates with the
thoracic vertebra facet
b. The tubercle articulates with the
transverse process of the
vertebrae. 38
D.Sternum (breastbone)Located along the anterior midline of the thoracic cage.
Its features include an upper manubrium, middle body, and lower
xiphoid process.
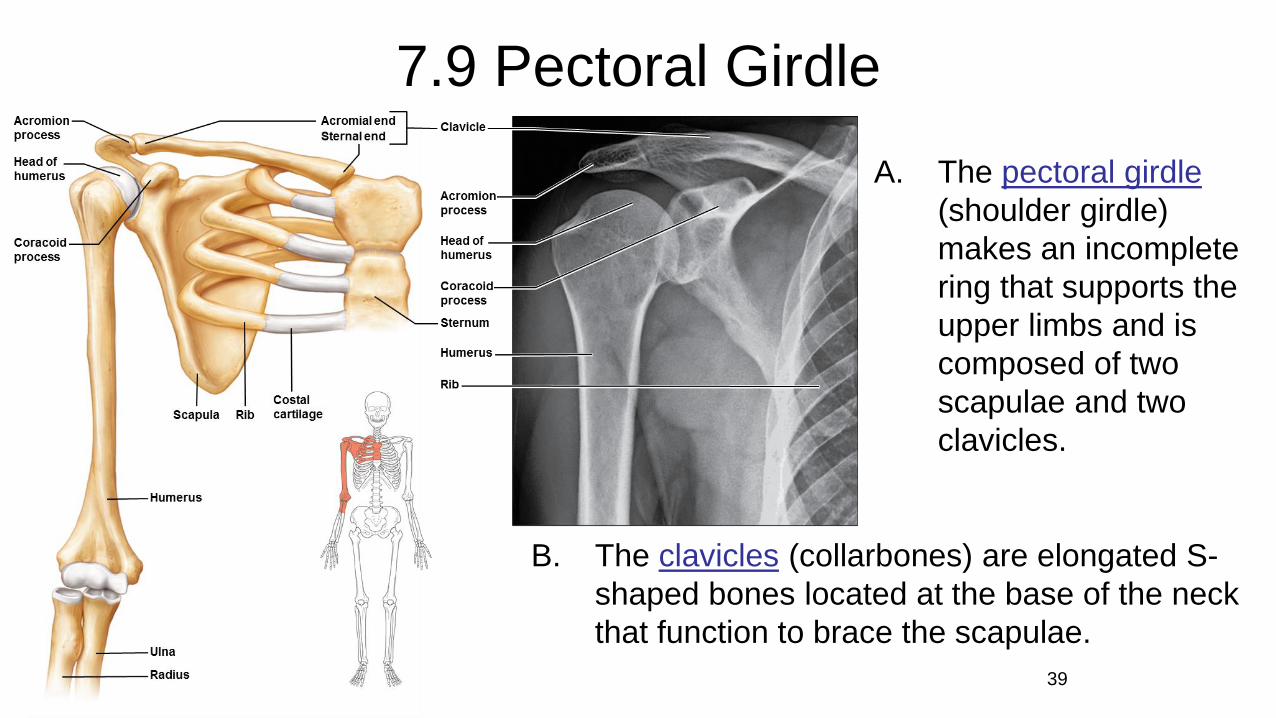
7.9 Pectoral Girdle
A. The pectoral girdle
(shoulder girdle)
makes an incomplete
ring that supports the
upper limbs and is
composed of two
scapulae and two
clavicles.
39
B. The clavicles (collarbones) are elongated S-
shaped bones located at the base of the neck
that function to brace the scapulae.
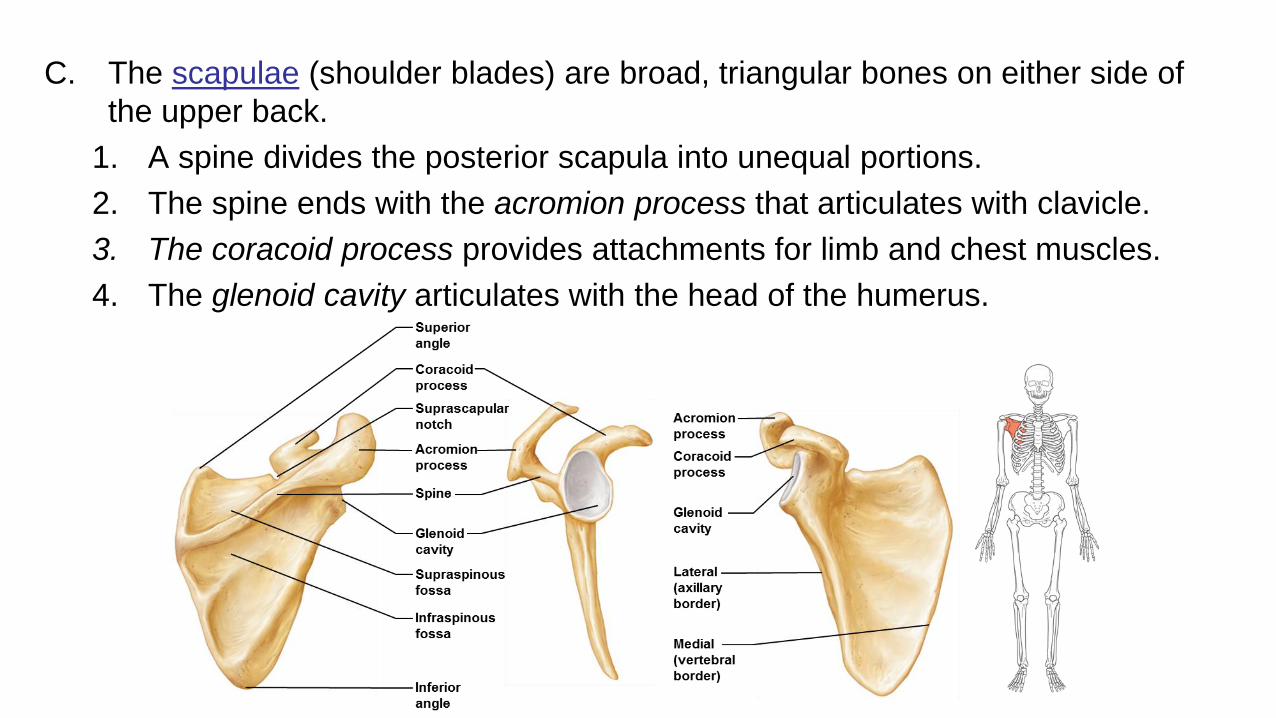
C. The scapulae (shoulder blades) are broad, triangular bones on either side of
the upper back.
1. A spine divides the posterior scapula into unequal portions.
2. The spine ends with the acromion process that articulates with clavicle.
3. The coracoid process provides attachments for limb and chest muscles.
4. The glenoid cavity articulates with the head of the humerus.
7.10 Upper Limb
A. Bones of the upper limb form the framework for the arm,
forearm, and hand. They also provide for muscle attachments
and they function as levers to move limb parts.
41
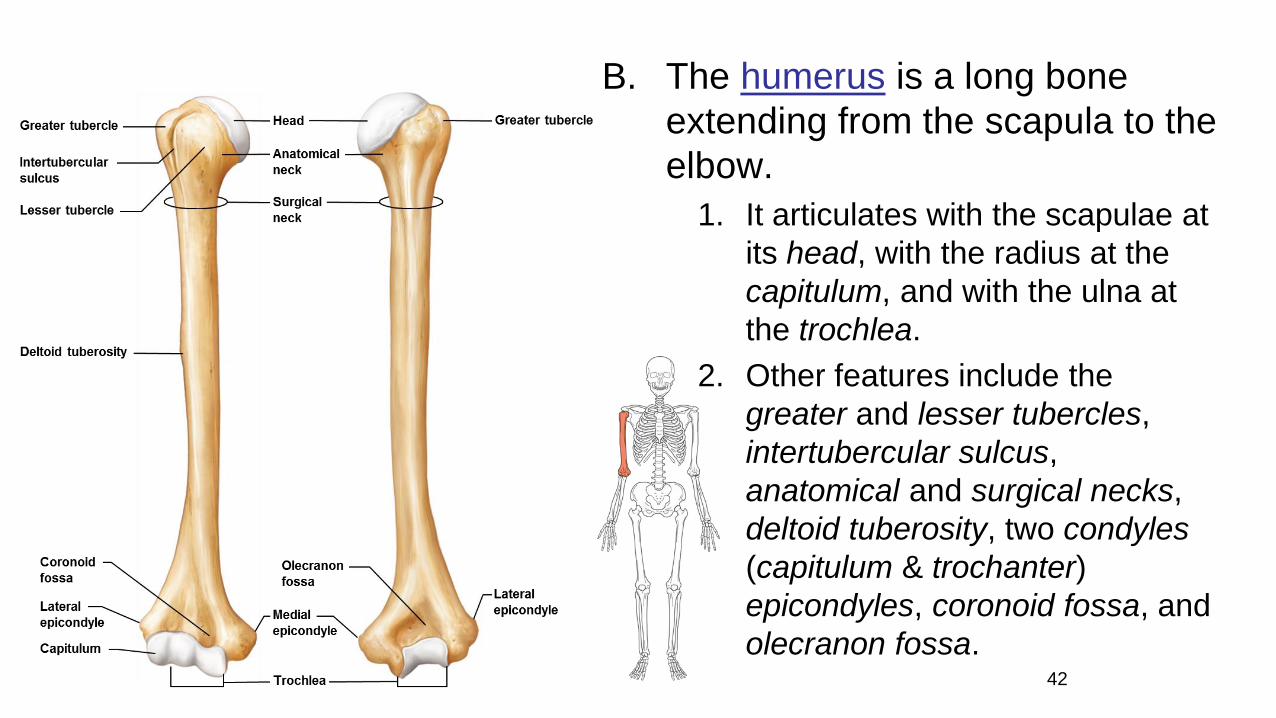
B. The humerus is a long bone
extending from the scapula to the
elbow.
1. It articulates with the scapulae at
its head, with the radius at the
capitulum, and with the ulna at
the trochlea.
2. Other features include the
greater and lesser tubercles,
intertubercular sulcus,
anatomical and surgical necks,
deltoid tuberosity, two condyles
(capitulum & trochanter)
epicondyles, coronoid fossa, and
olecranon fossa.42
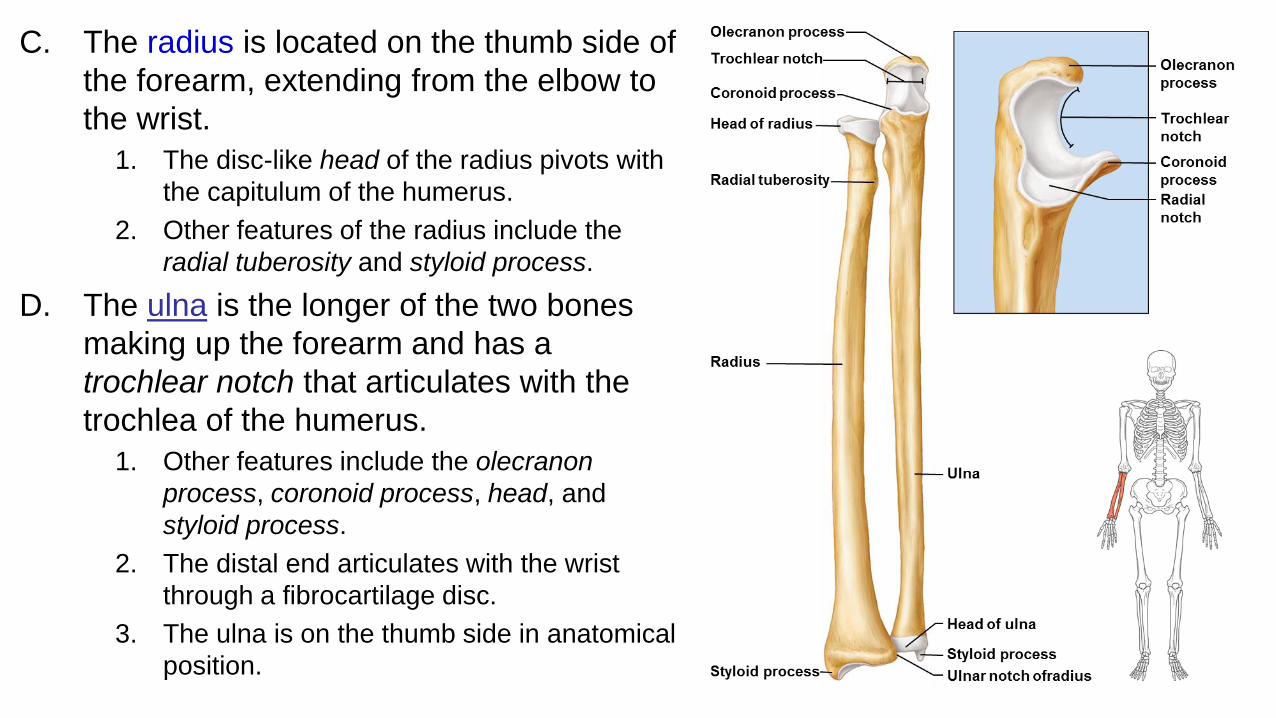
C. The radius is located on the thumb side of
the forearm, extending from the elbow to
the wrist.
1. The disc-like head of the radius pivots with
the capitulum of the humerus.
2. Other features of the radius include the
radial tuberosity and styloid process.
D. The ulna is the longer of the two bones
making up the forearm and has a
trochlear notch that articulates with the
trochlea of the humerus.
1. Other features include the olecranon
process, coronoid process, head, and
styloid process.
2. The distal end articulates with the wrist
through a fibrocartilage disc.
3. The ulna is on the thumb side in anatomical
position.

E. The hand is made up of the
wrist, palm, and fingers.
1. The wrist of the hand is
made up of eight carpal
bones bound into a
carpus.
2. The framework of the
hand is made up of five
metacarpal bones.
3. The fingers are composed
of three phalanges in each
finger except the thumb,
which lacks the middle
phalanx. 44
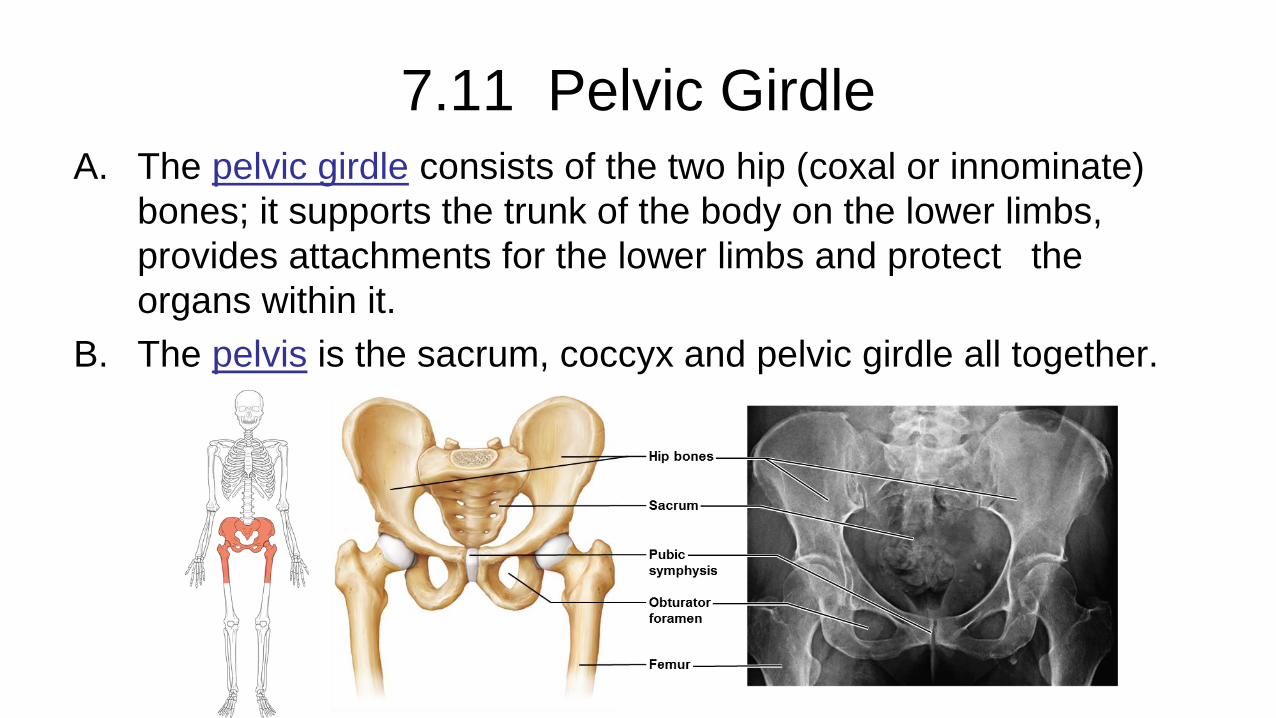
7.11 Pelvic GirdleA. The pelvic girdle consists of the two hip (coxal or innominate)
bones; it supports the trunk of the body on the lower limbs,
provides attachments for the lower limbs and protect the
organs within it.
B. The pelvis is the sacrum, coccyx and pelvic girdle all together.
45
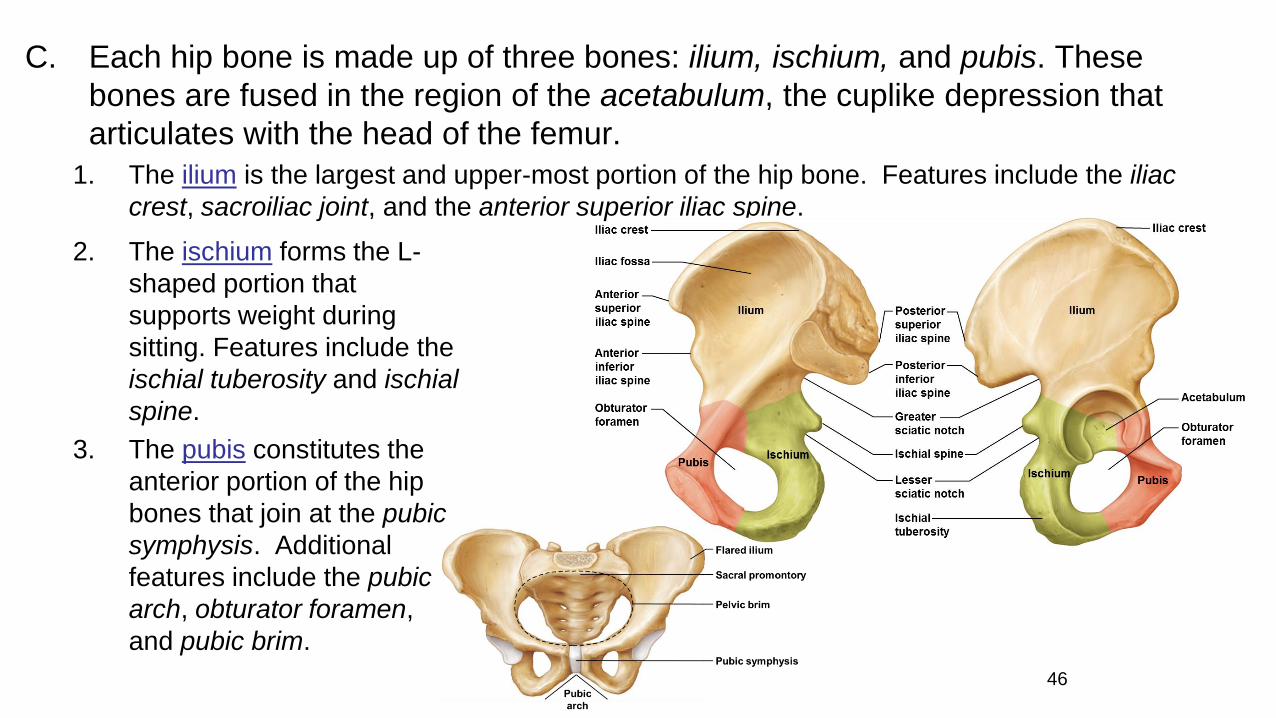
C. Each hip bone is made up of three bones: ilium, ischium, and pubis. These
bones are fused in the region of the acetabulum, the cuplike depression that
articulates with the head of the femur.
1. The ilium is the largest and upper-most portion of the hip bone. Features include the iliac
crest, sacroiliac joint, and the anterior superior iliac spine.
46
2. The ischium forms the L-
shaped portion that
supports weight during
sitting. Features include the
ischial tuberosity and ischial
spine.
3. The pubis constitutes the
anterior portion of the hip
bones that join at the pubic
symphysis. Additional
features include the pubic
arch, obturator foramen,
and pubic brim.
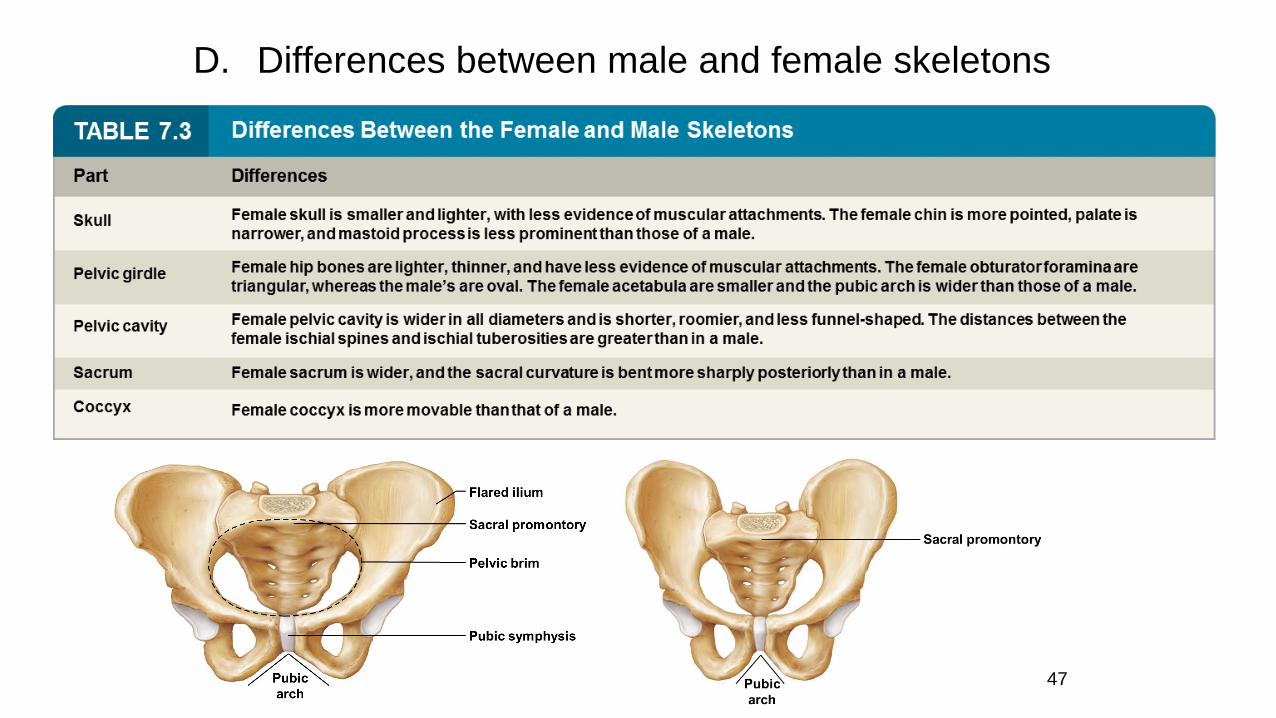
D. Differences between male and female skeletons
47

7.12 Lower Limb
A. The bones of the lower limb provide the
framework for the thigh, lower leg, and foot.
B. The femur, or thighbone, extends from the hip to
the knee and is the longest bone in the body.
1. Its head joins with the acetabulum; it also joins
with the tibia at the medial and lateral
condyles.
2. Other features of the femur include the fovea
capitis, neck, and greater and lesser
trochanters.
C. The patella (kneecap) is located in the tendon
that passes anteriorly over the knee.

D. The tibia (shinbone) supports the weight of
the body and articulates with the femur
(medial and lateral condyles) and with the
talus of the ankle.
1. Its anterior tibial tuberosity is the point of
attachment for the patellar ligament.
2. Other features include the medial
malleolus (inner ankle).
E. The fibula is a slender bone lying lateral to
the tibia.
1. It does not bear body weight.
2. Features include the head and a distal
lateral malleolus (outer ankle).
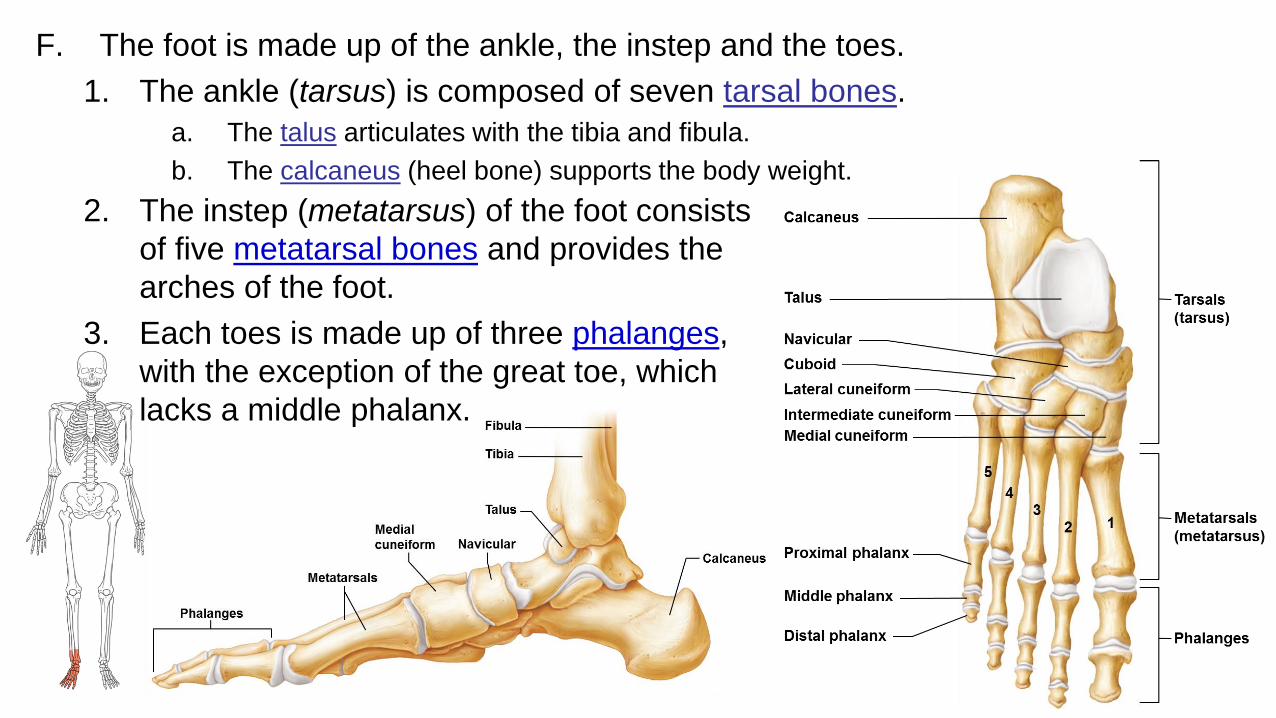
F. The foot is made up of the ankle, the instep and the toes.
1. The ankle (tarsus) is composed of seven tarsal bones.
a. The talus articulates with the tibia and fibula.
b. The calcaneus (heel bone) supports the body weight.
50
2. The instep (metatarsus) of the foot consists
of five metatarsal bones and provides the
arches of the foot.
3. Each toes is made up of three phalanges,
with the exception of the great toe, which
lacks a middle phalanx.
7.13 JointsA. Joints (articulations) are the functional junctions between bones.
1. Joints enable a wide variety of body movements, bond parts of the body together, make bone growth possible, and permit shape changes during childbirth.
2. Joints can be classified according to the degree of movement possible and can be immovable (synarthrotic), slightly movable (amphiarthrotic), or freely movable (diarthrotic).
3. Joints can also classified according to the type of tissue that binds them together – fibrous, cartilaginous, or synovial. (more commonly used today)
51
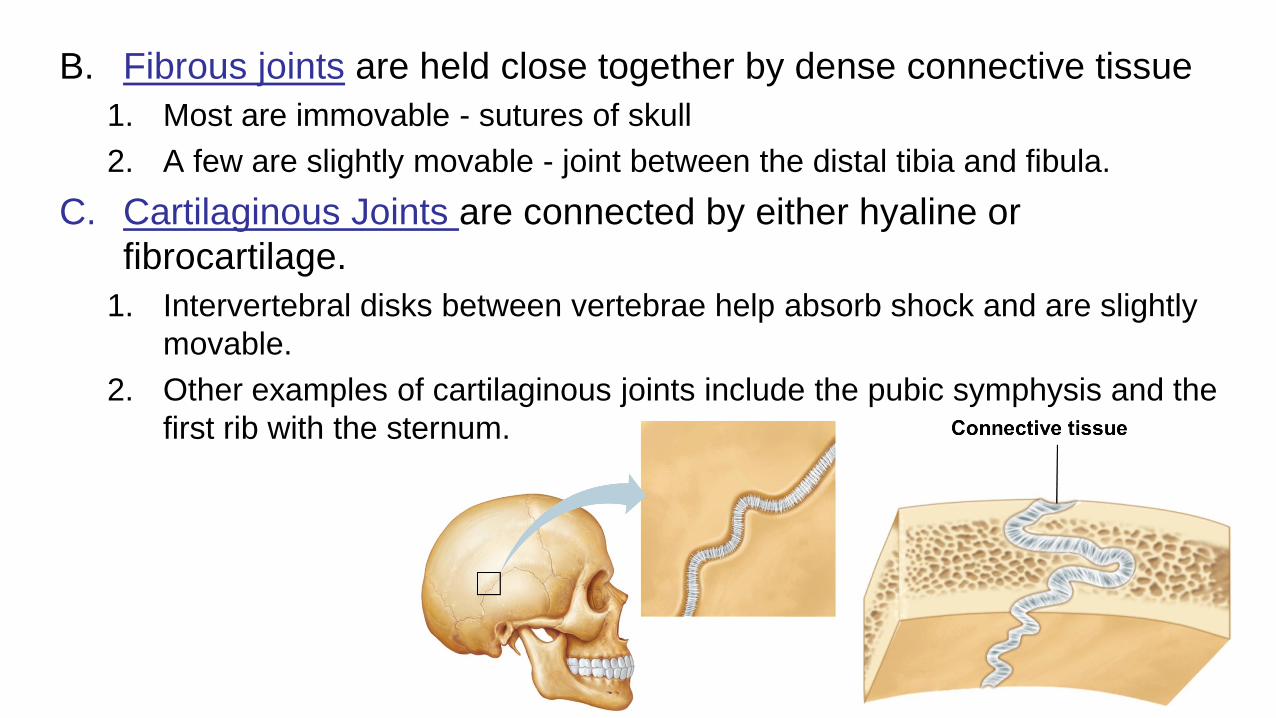
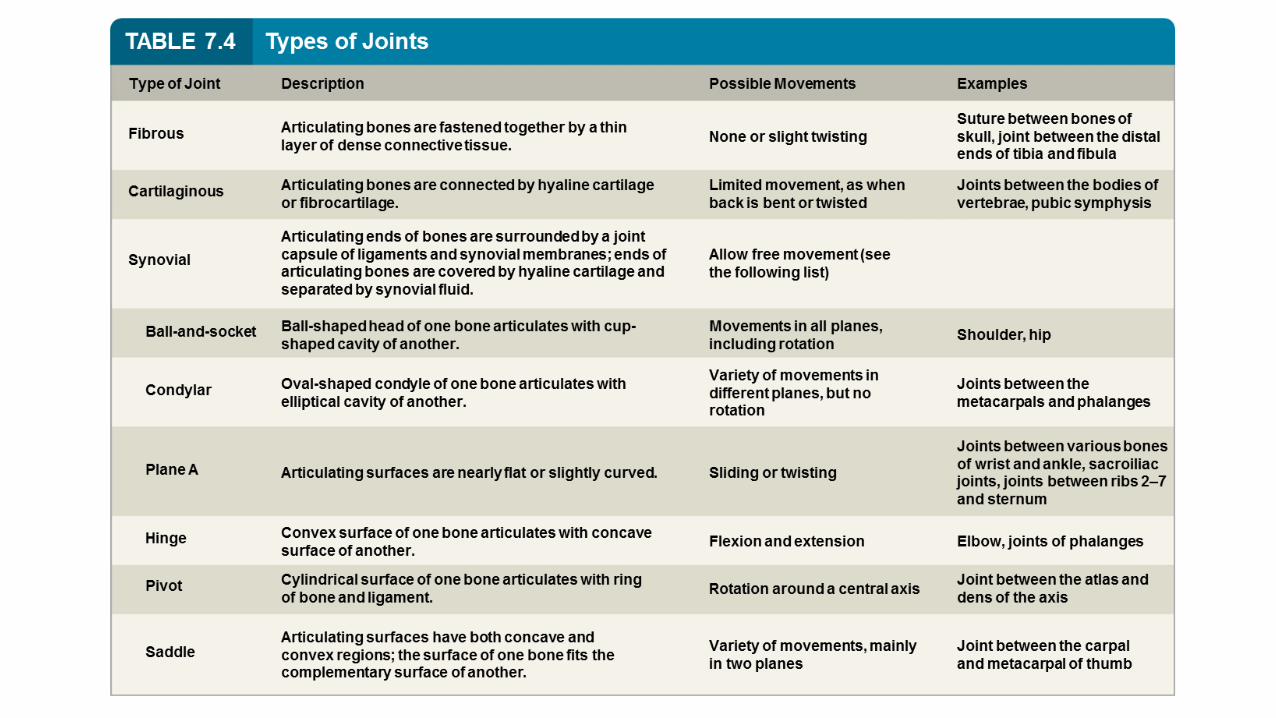
B. Fibrous joints are held close together by dense connective tissue
1. Most are immovable - sutures of skull
2. A few are slightly movable - joint between the distal tibia and fibula.
C. Cartilaginous Joints are connected by either hyaline or
fibrocartilage.
1. Intervertebral disks between vertebrae help absorb shock and are slightly
movable.
2. Other examples of cartilaginous joints include the pubic symphysis and the
first rib with the sternum.
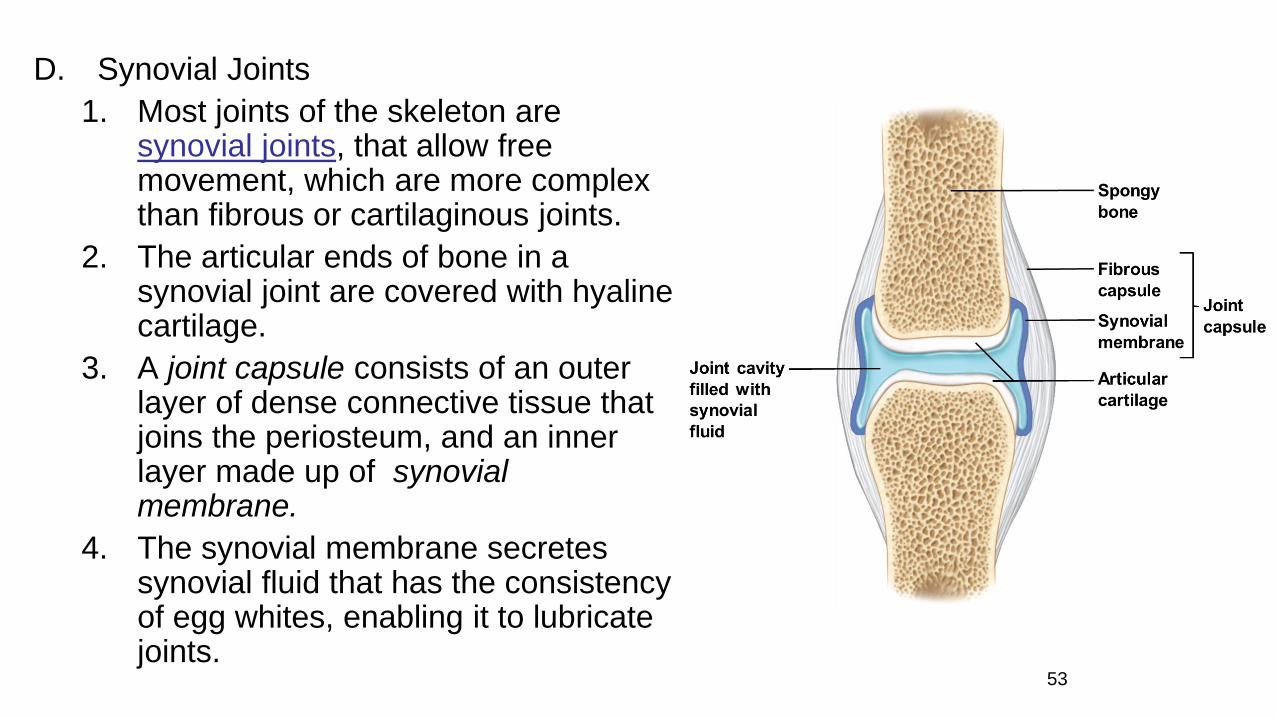
D. Synovial Joints
1. Most joints of the skeleton are synovial joints, that allow free movement, which are more complex than fibrous or cartilaginous joints.
2. The articular ends of bone in a synovial joint are covered with hyaline cartilage.
3. A joint capsule consists of an outer layer of dense connective tissue that joins the periosteum, and an inner layer made up of synovial membrane.
4. The synovial membrane secretes synovial fluid that has the consistency of egg whites, enabling it to lubricate joints.
53
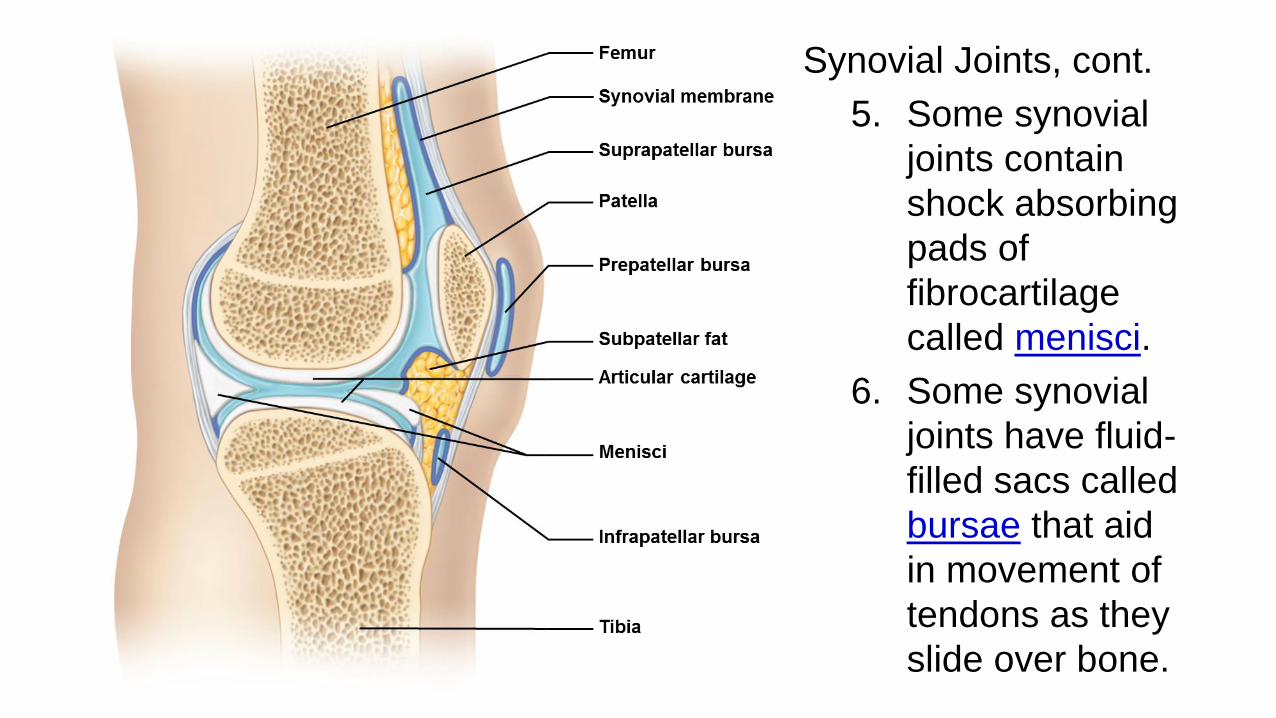
Synovial Joints, cont.
5. Some synovial
joints contain
shock absorbing
pads of
fibrocartilage
called menisci.
6. Some synovial
joints have fluid-
filled sacs called
bursae that aid
in movement of
tendons as they
slide over bone.
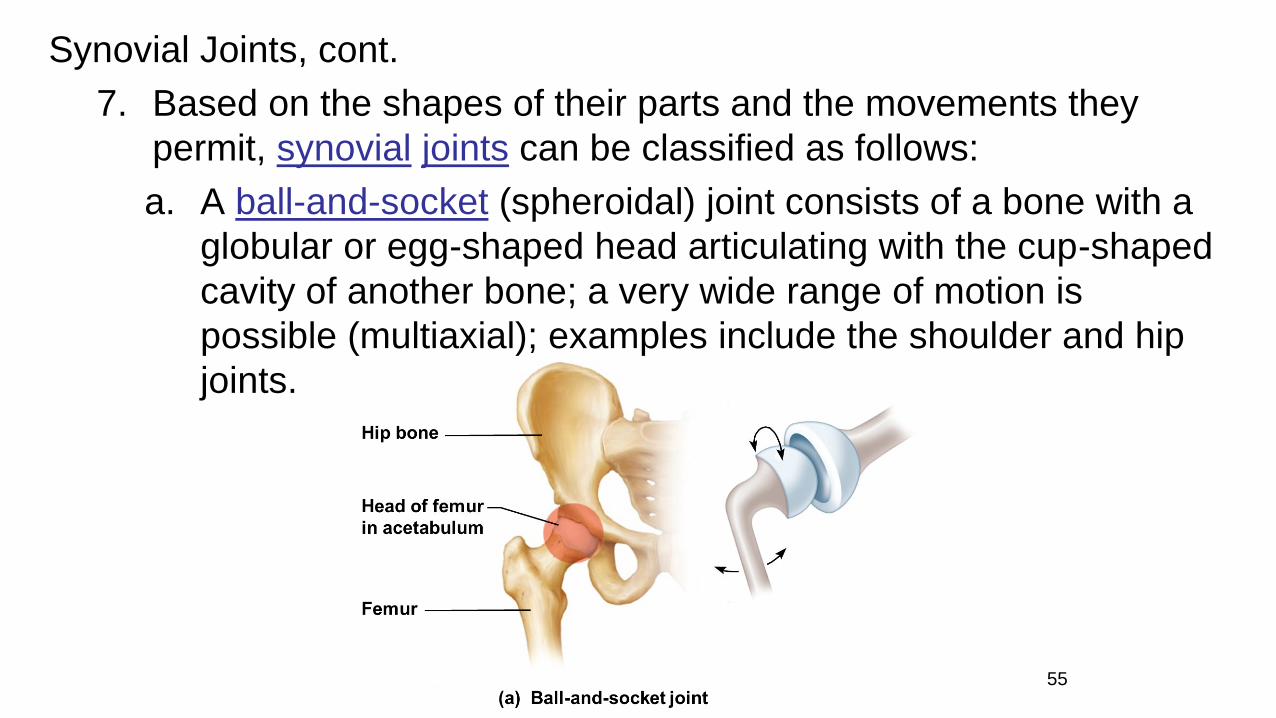
Synovial Joints, cont.
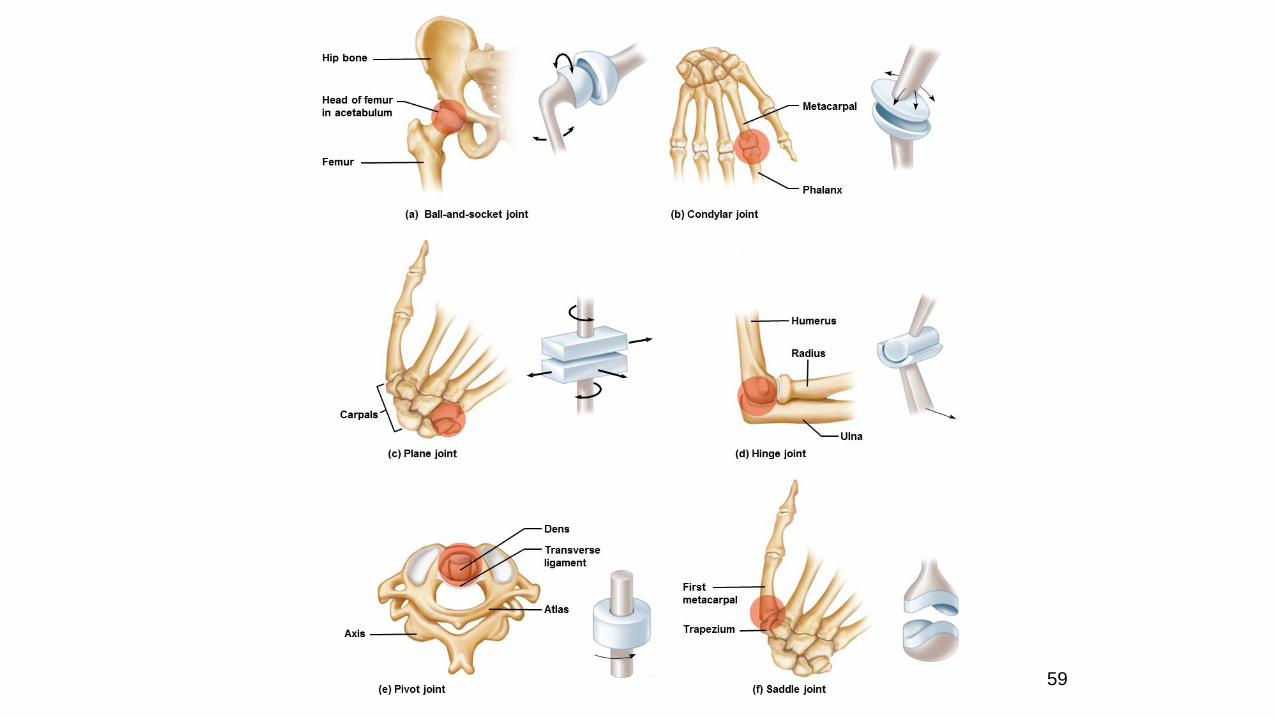
7. Based on the shapes of their parts and the movements they
permit, synovial joints can be classified as follows:
a. A ball-and-socket (spheroidal) joint consists of a bone with a
globular or egg-shaped head articulating with the cup-shaped
cavity of another bone; a very wide range of motion is
possible (multiaxial); examples include the shoulder and hip
joints.
55
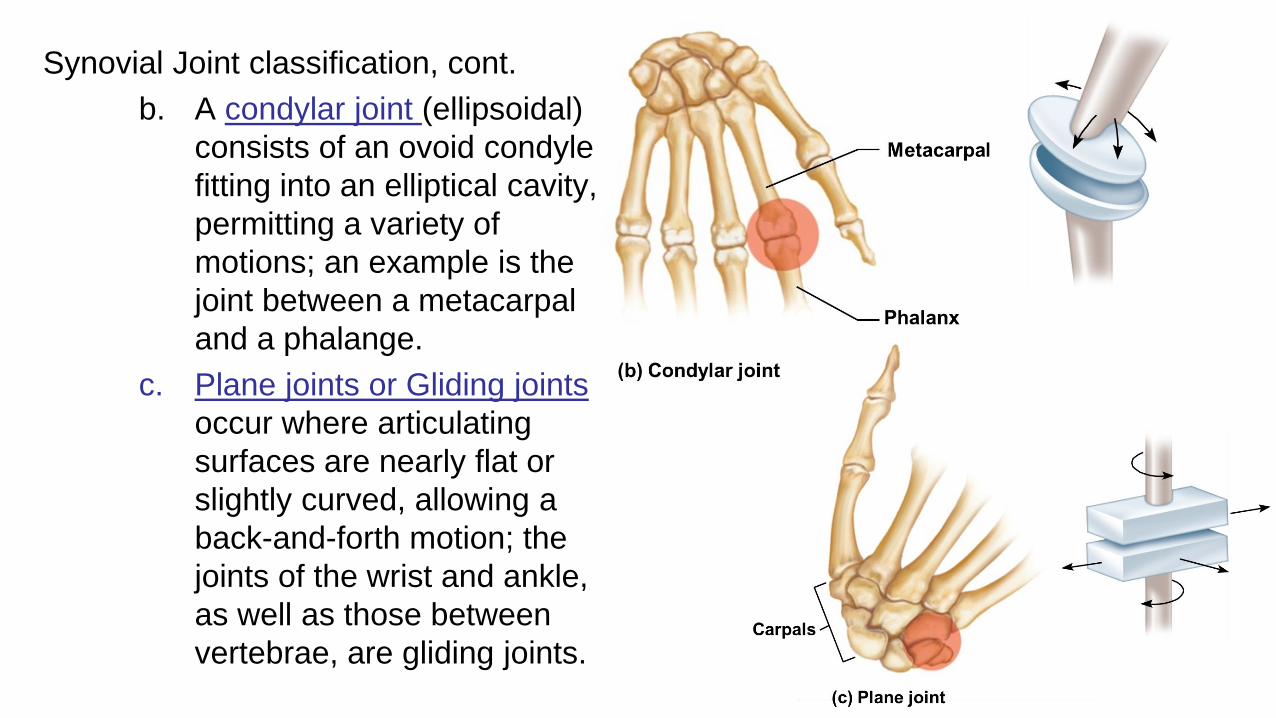
Synovial Joint classification, cont.
b. A condylar joint (ellipsoidal)
consists of an ovoid condyle
fitting into an elliptical cavity,
permitting a variety of
motions; an example is the
joint between a metacarpal
and a phalange.
c. Plane joints or Gliding joints
occur where articulating
surfaces are nearly flat or
slightly curved, allowing a
back-and-forth motion; the
joints of the wrist and ankle,
as well as those between
vertebrae, are gliding joints.56
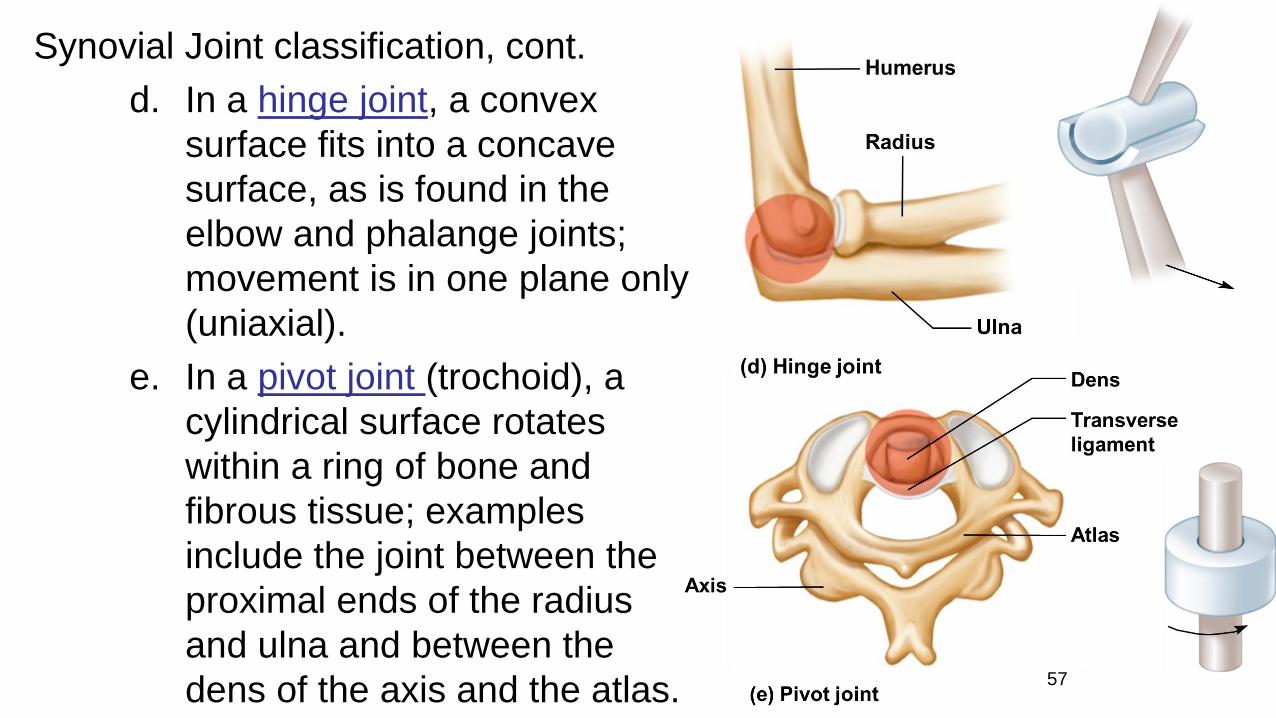
Synovial Joint classification, cont.
d. In a hinge joint, a convex
surface fits into a concave
surface, as is found in the
elbow and phalange joints;
movement is in one plane only
(uniaxial).
e. In a pivot joint (trochoid), a
cylindrical surface rotates
within a ring of bone and
fibrous tissue; examples
include the joint between the
proximal ends of the radius
and ulna and between the
dens of the axis and the atlas. 57

Synovial Joint classification, cont.
f. A saddle joint (sellar) forms where articulating
surfaces have both concave and convex areas,
permits movements in two planes (biaxial); the joint
between the trapezium and the metacarpal of the
thumb is of this type.
59
60
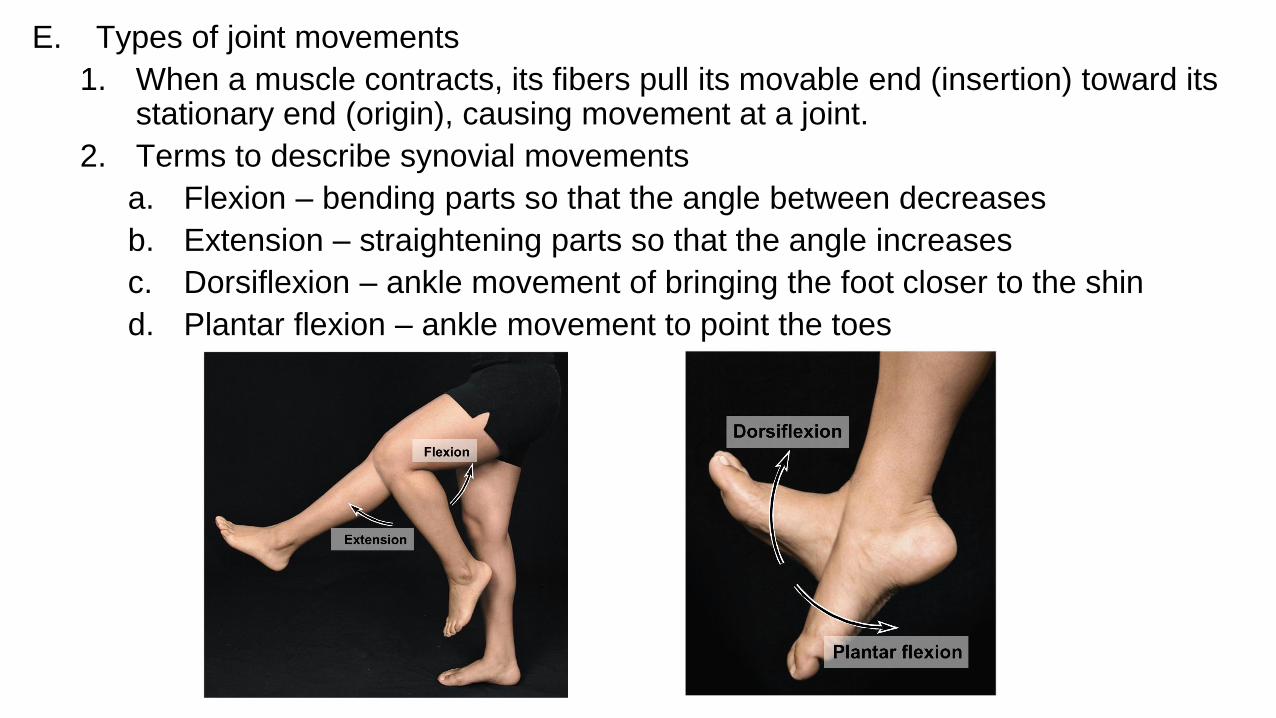
E. Types of joint movements
1. When a muscle contracts, its fibers pull its movable end (insertion) toward its stationary end (origin), causing movement at a joint.
2. Terms to describe synovial movements
a. Flexion – bending parts so that the angle between decreases
b. Extension – straightening parts so that the angle increases
c. Dorsiflexion – ankle movement of bringing the foot closer to the shin
d. Plantar flexion – ankle movement to point the toes
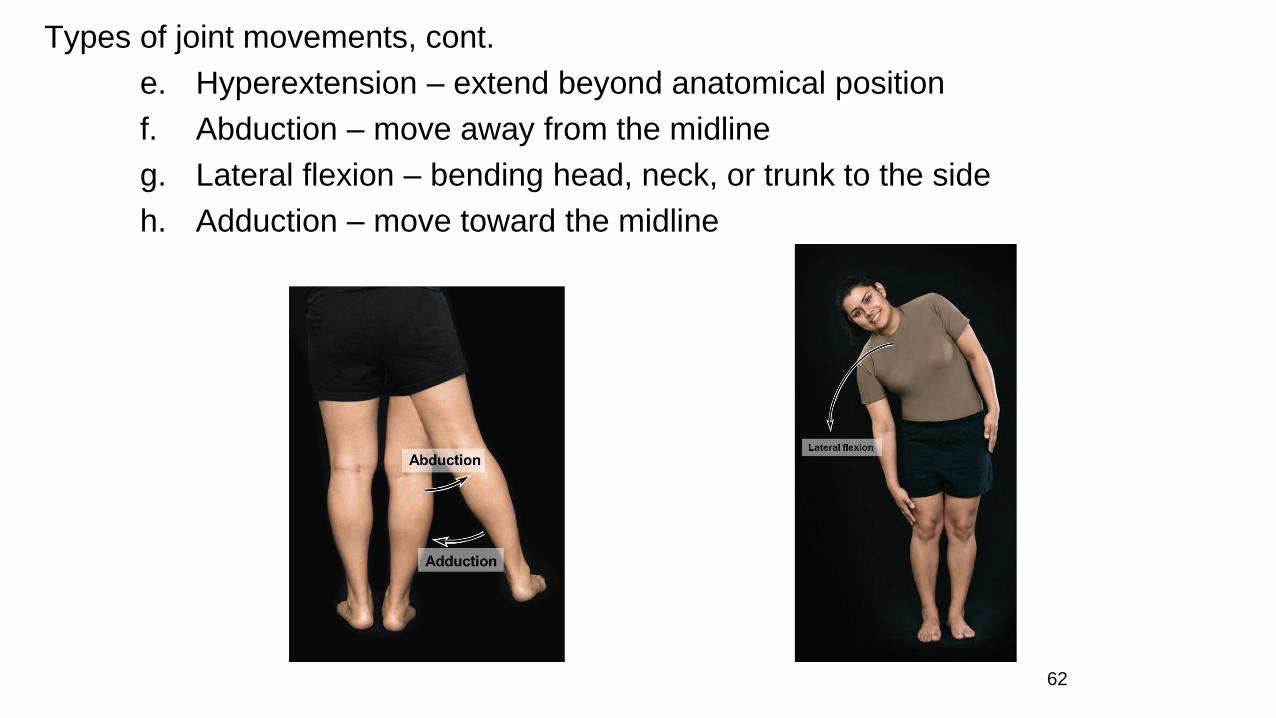
Types of joint movements, cont.
e. Hyperextension – extend beyond anatomical position
f. Abduction – move away from the midline
g. Lateral flexion – bending head, neck, or trunk to the side
h. Adduction – move toward the midline
62
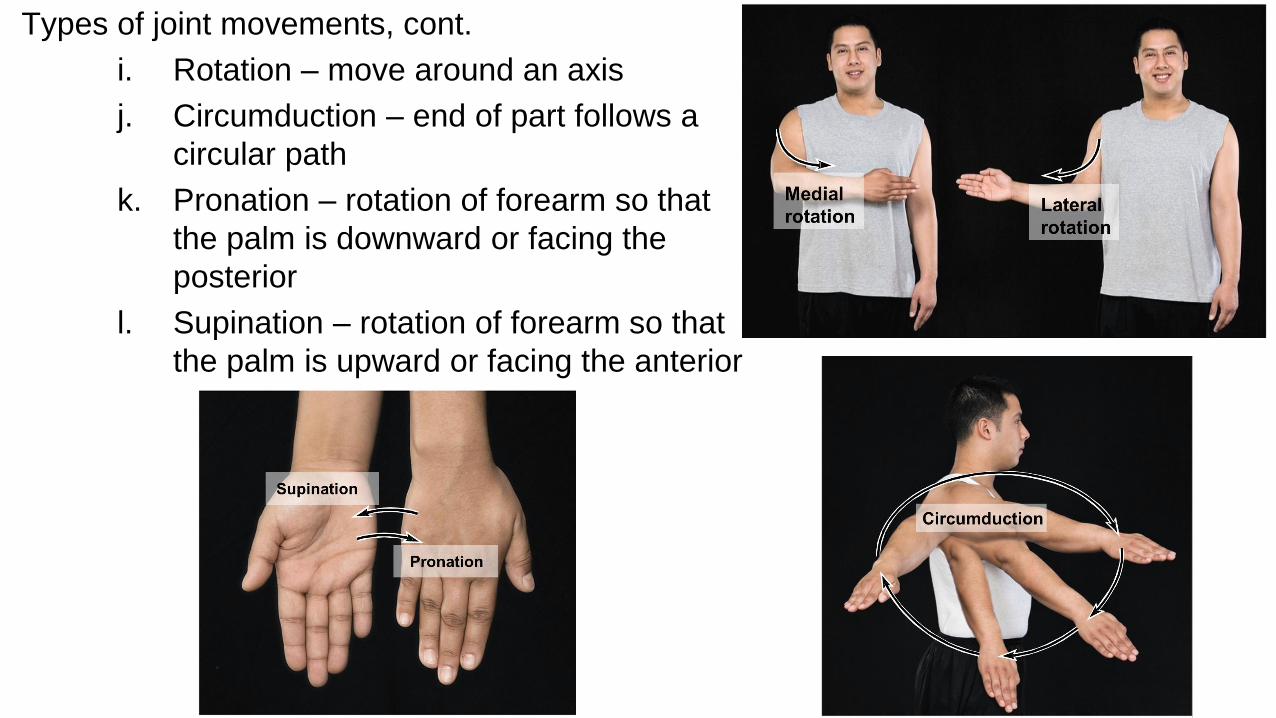
Types of joint movements, cont.
i. Rotation – move around an axis
j. Circumduction – end of part follows a
circular path
k. Pronation – rotation of forearm so that
the palm is downward or facing the
posterior
l. Supination – rotation of forearm so that
the palm is upward or facing the anterior
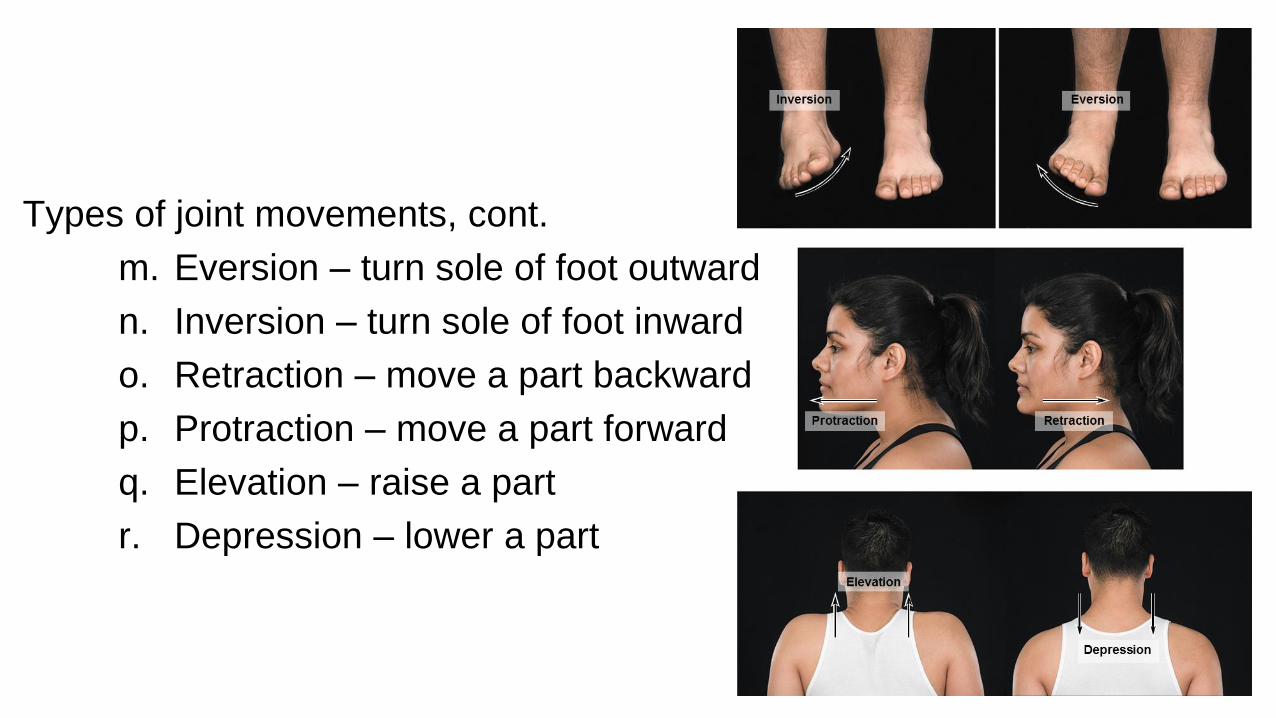
Types of joint movements, cont.
m. Eversion – turn sole of foot outward
n. Inversion – turn sole of foot inward
o. Retraction – move a part backward
p. Protraction – move a part forward
q. Elevation – raise a part
r. Depression – lower a part
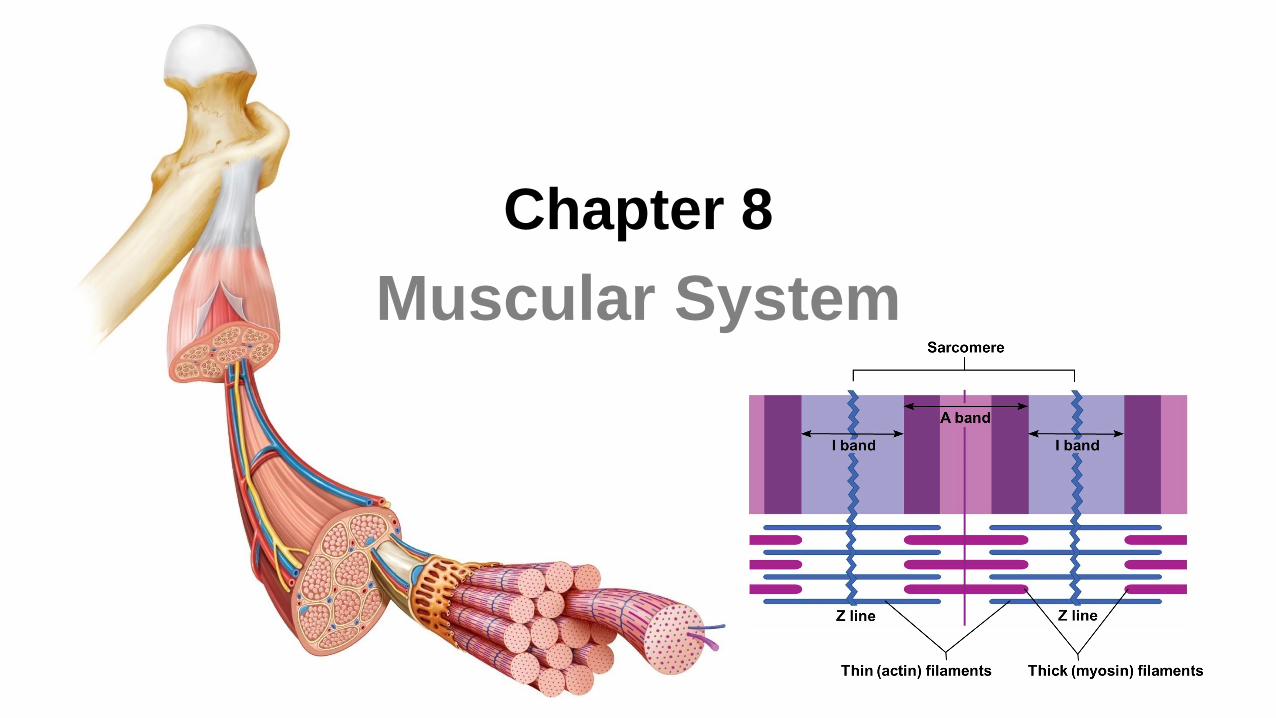
Chapter 8
Muscular System
8.1 Introduction
A. All movements require muscles which are organs using
chemical energy to contract, provide muscle tone, propel body
fluids and food, generate the heartbeat, and generate heat.
B. The three types of muscle in the body are skeletal, smooth, and
cardiac muscle.
66
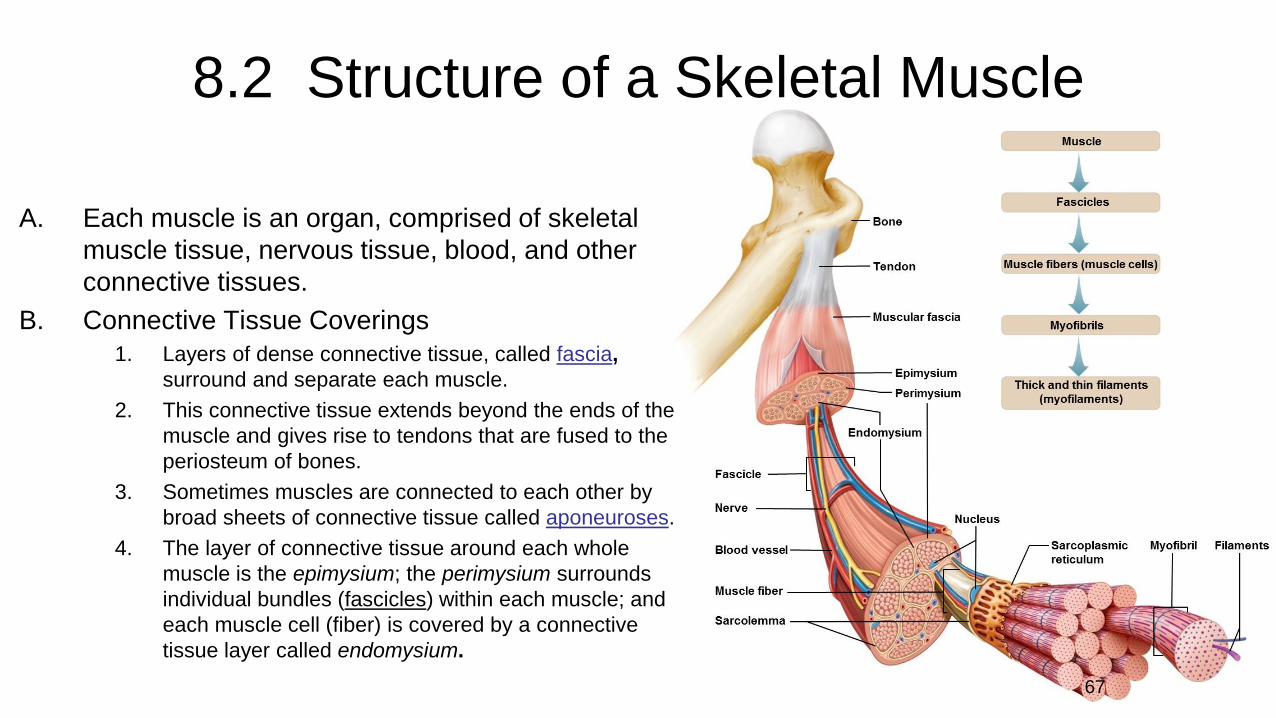
8.2 Structure of a Skeletal Muscle
A. Each muscle is an organ, comprised of skeletal
muscle tissue, nervous tissue, blood, and other
connective tissues.
B. Connective Tissue Coverings
1. Layers of dense connective tissue, called fascia,
surround and separate each muscle.
2. This connective tissue extends beyond the ends of the
muscle and gives rise to tendons that are fused to the
periosteum of bones.
3. Sometimes muscles are connected to each other by
broad sheets of connective tissue called aponeuroses.
4. The layer of connective tissue around each whole
muscle is the epimysium; the perimysium surrounds
individual bundles (fascicles) within each muscle; and
each muscle cell (fiber) is covered by a connective
tissue layer called endomysium.
67
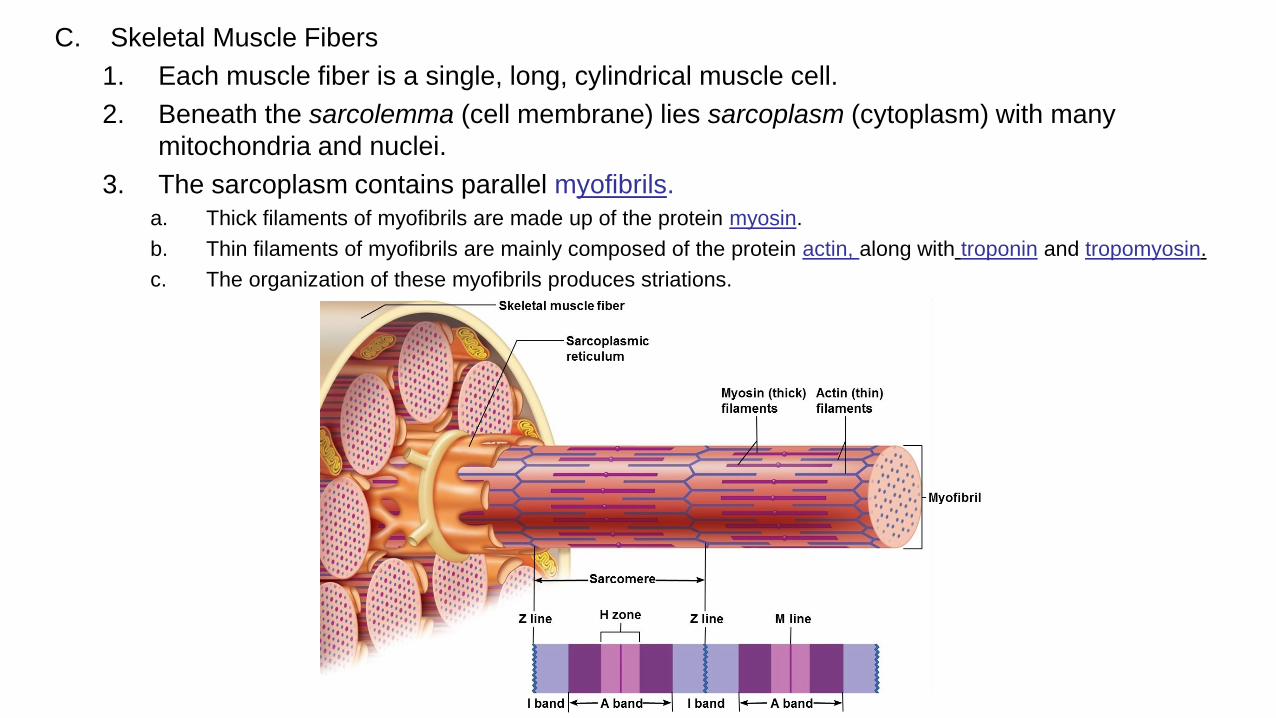
C. Skeletal Muscle Fibers
1. Each muscle fiber is a single, long, cylindrical muscle cell.
2. Beneath the sarcolemma (cell membrane) lies sarcoplasm (cytoplasm) with many
mitochondria and nuclei.
3. The sarcoplasm contains parallel myofibrils.
a. Thick filaments of myofibrils are made up of the protein myosin.
b. Thin filaments of myofibrils are mainly composed of the protein actin, along with troponin and tropomyosin.
c. The organization of these myofibrils produces striations.
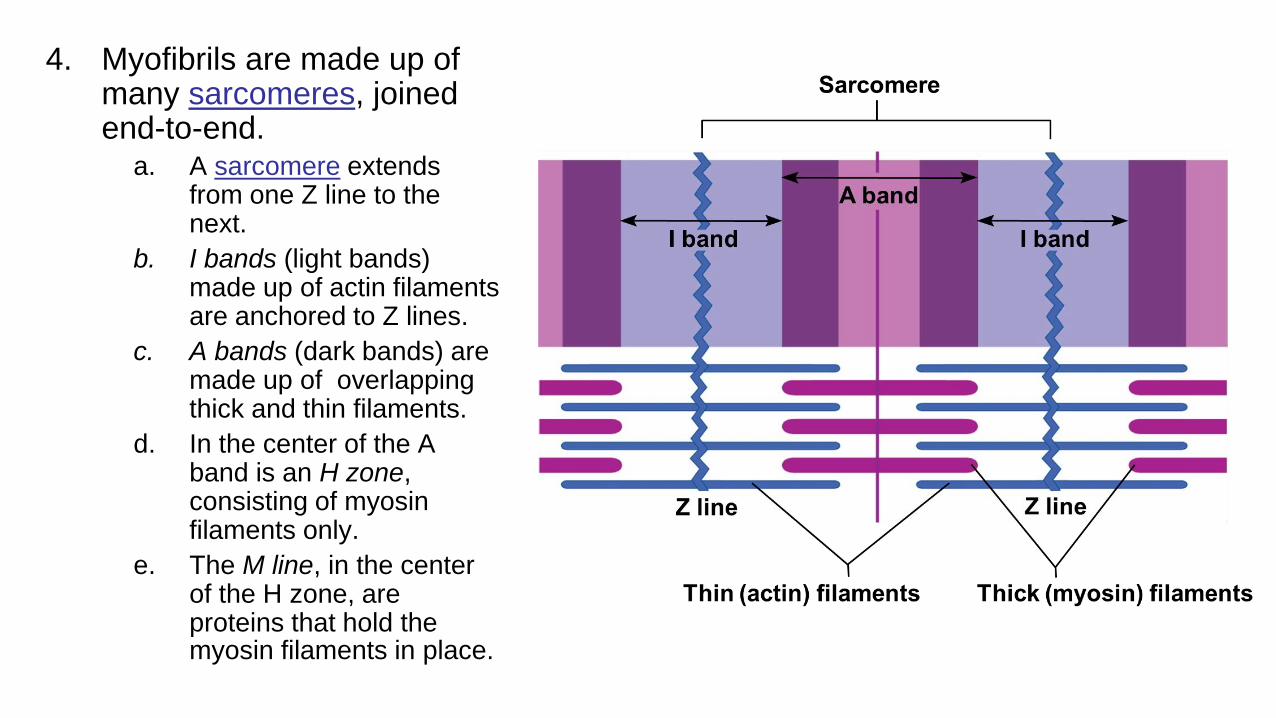
4. Myofibrils are made up of many sarcomeres, joined end-to-end.
a. A sarcomere extends from one Z line to the next.
b. I bands (light bands) made up of actin filaments are anchored to Z lines.
c. A bands (dark bands) are made up of overlapping thick and thin filaments.
d. In the center of the A band is an H zone, consisting of myosin filaments only.
e. The M line, in the center of the H zone, are proteins that hold the myosin filaments in place.

5. Beneath the sarcolemma of a muscle fiber lies the sarcoplasmicreticulum (endoplasmic reticulum), which is associated with transverse (T) tubules (invaginations of the sarcolemma).
a. Each T tubule lies between two cisternae of the sarcoplasmic reticulum and is open to the outside of the muscle fiber.
b. The sarcoplasmic reticulum and transverse tubules activate the muscle contraction mechanism when the fiber is stimulated.
70
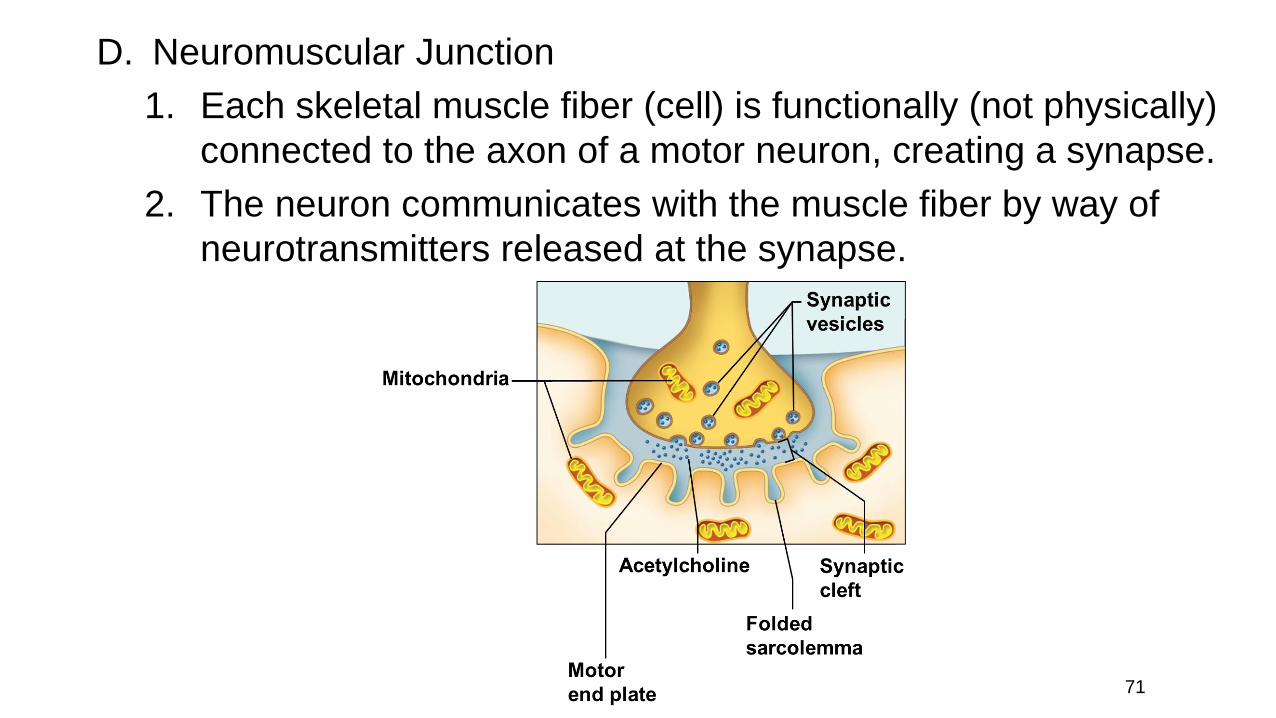
D. Neuromuscular Junction
1. Each skeletal muscle fiber (cell) is functionally (not physically)
connected to the axon of a motor neuron, creating a synapse.
2. The neuron communicates with the muscle fiber by way of
neurotransmitters released at the synapse.
71

Neuromuscular Junction, cont.
3. The site where the motor neuron and muscle fiber meet is the neuromuscularjunction.
a. The muscle fiber membrane forms a motor end plate in which the sarcolemma is tightly folded and where nuclei and mitochondria are abundant.
b. The cytoplasm of the motor neuron contains numerous mitochondria and synaptic vesicles storing neurotransmitters.
c. When an electrical impulse reaches the end of the motor neuron axon, vesicles release neurotransmitter into the synaptic cleft and will stimulate the muscle fiber to contract.
8.3 Skeletal Muscle Contraction
A. Muscle contraction involves several components that result in
the shortening of sarcomeres, and the pulling of the muscle against its attachments.
73

B. Role of Myosin and Actin 1. Myosin consists of two twisted strands with globular heads projected outward
along the strands.
2. Actin is a globular protein put together in twisted filaments, with myosin binding sites; tropomyosin and troponin are two proteins associated with the surface of the actin filaments.
74
Role of myosin and actin, cont.
3. According to the sliding filament model of muscle contraction, a myosin head cross-bridge attaches to a binding site on the actin filament and bends, pulling on the actin filament; it then releases and attaches to the next binding site on the actin, pulling again.
4. Energy from the conversion of ATP to ADP is provided to the cross-bridges from the enzyme ATPase, causing them to be in a “cocked” position.
75
C. Stimulus for Contraction
1. The motor neuron must release the neurotransmitter acetylcholine from its synaptic vesicles into the synaptic cleft in order to initiate a muscle contraction.
2. Protein receptors in the motor end plate bind to the neurotransmitters, which increases the membrane permeability to sodium ions. The entry of these charged particles creates a muscle impulse that spreads over the surface of the sarcolemma and into the T tubules, where it reaches the sarcoplasmic reticulum.
76

Stimulus for contraction, cont.
3. Upon receipt of the muscle impulse, the sarcoplasmic reticulum releases its stored calcium to the sarcoplasm of the muscle fiber.
4. The high concentration of calcium in the sarcoplasm interacts with the troponin and tropomyosin molecules, which move aside, exposing the myosin binding sites on the actin filaments.
5. Myosin cross-bridges now bind and pull on the actin filaments, and using ATP, causes the sarcomere to shorten.
77
Stimulus for contraction, cont.
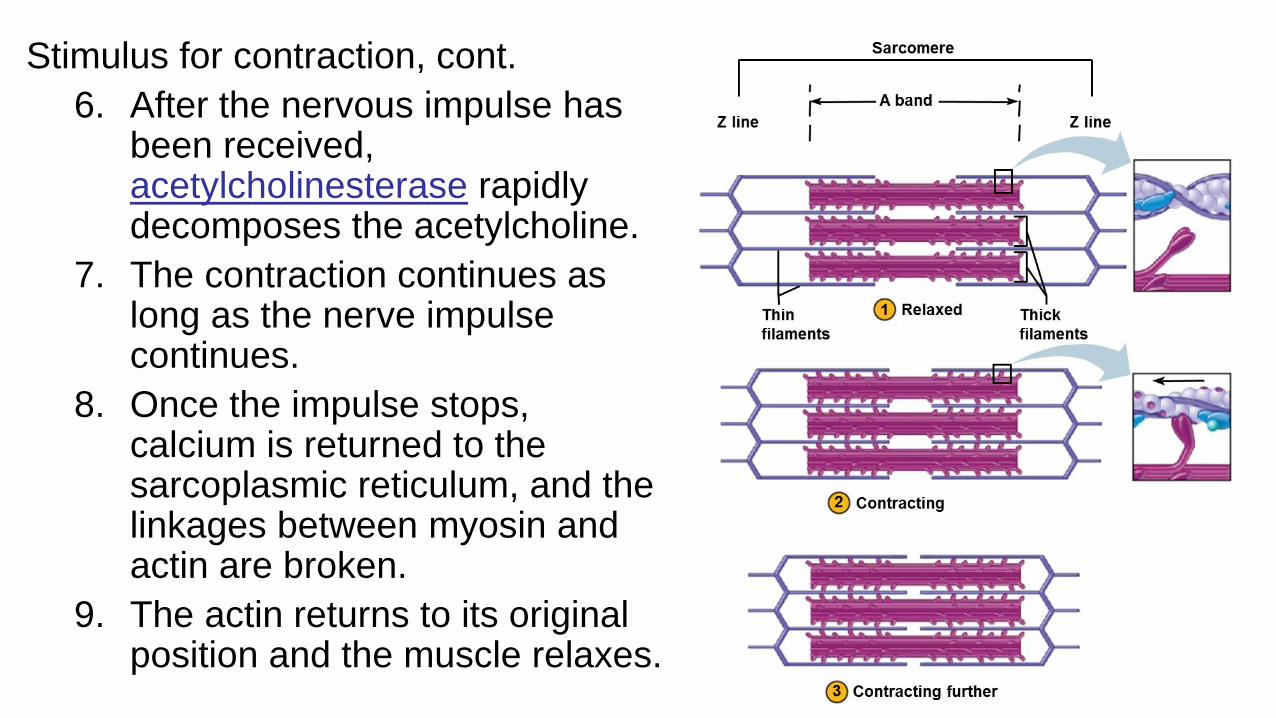
6. After the nervous impulse has been received, acetylcholinesterase rapidly decomposes the acetylcholine.
7. The contraction continues as long as the nerve impulse continues.
8. Once the impulse stops, calcium is returned to the sarcoplasmic reticulum, and the linkages between myosin and actin are broken.
9. The actin returns to its original position and the muscle relaxes.
78

Troponin
Tropomyosin
Myosin
filament
Muscle contraction
Release of Ca+2 from
sarcoplasmic reticulum
exposes binding sites
on thin filament:
Muscle relaxation
Active transport of Ca+2 into
sarcoplasmic reticulum, which
requires ATP, makes myosin
binding sites unavailable.
Continued contraction
If the stimulus for contraction is
maintained, Ca+2 continues to bind
to troponin.
Ca+2 binds
to troponin
Binding sites on
actin filament
exposed
ATP
Contraction cycle
PADP +
PADP +PADP +
Ca+2Relaxed muscle
PADP + PADP +
PADP + PADP +
P
ADP
P
ADP
ATP ATP ATP
PADP + PADP +
ATP
1
2
3
4
5
6
P
Actin
molecules
Actin
filament
ATP splits, which provides power to “cock” the
myosin heads and store energy for the next power
stroke
Ca+2
Ca+2 Ca+2 Ca+2
Tropomyosin
pulled aside
Exposed binding sites on actin allow the muscle
contraction cycle to occur
Myosin heads bind to actin, forming cross-bridges,
connecting myosin to actin
ADP and release from myosin and cross-
bridge pulls actin filament (power stroke)
New ATP binds to myosin, breaking the
connection to actin


D. Energy Sources for Contraction
1. Energy for contraction comes from molecules of ATP. This chemical is in limited supply and so
must be regenerated
2. The initial source of energy for muscle contraction is ATP that is stored in the muscle.
3. Creatine phosphate, which stores excess energy released by the mitochondria, is present to
regenerate ATP from ADP and phosphate.
a. Whenever the supply of ATP is sufficient, creatine phosphokinase promotes the synthesis of
creatine phosphate.
b. As ATP decomposes, the energy from creatine phosphate can be transferred to ADP molecules,
converting them back to ATP.
4. As the supply of creatine phosphate declines, the cell must rely on cellular respiration to
generate ATP.
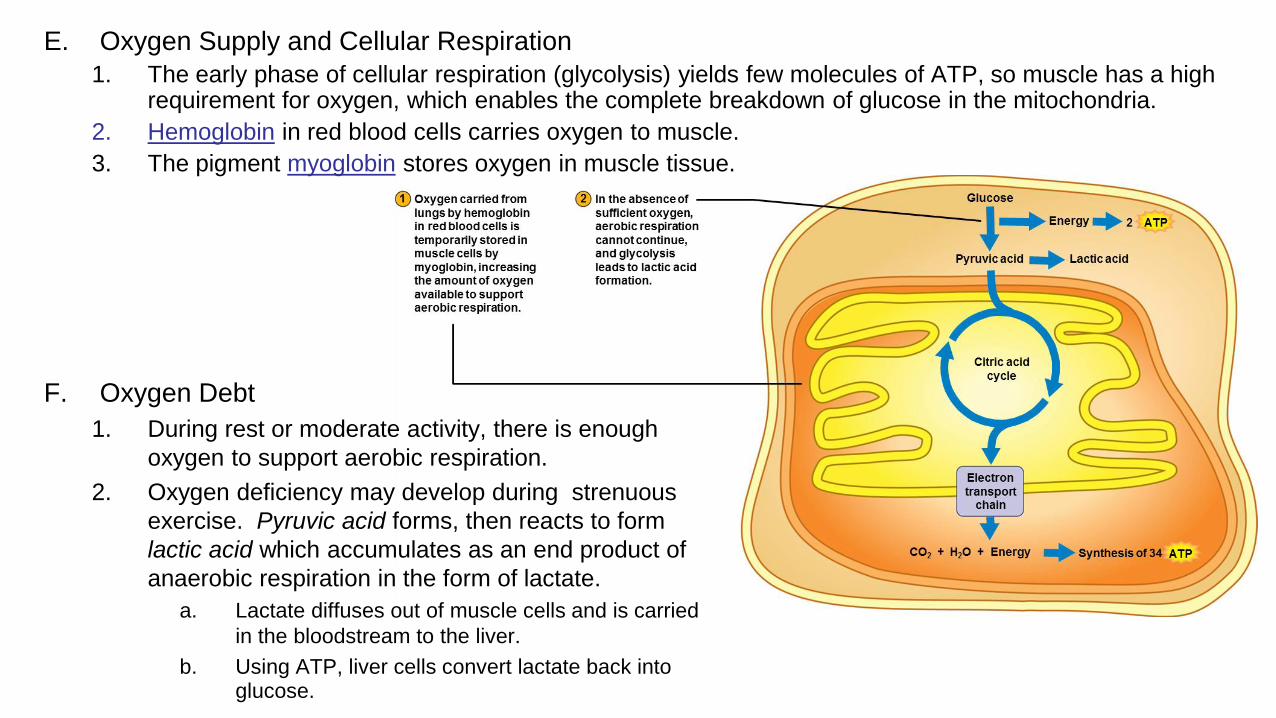
E. Oxygen Supply and Cellular Respiration
1. The early phase of cellular respiration (glycolysis) yields few molecules of ATP, so muscle has a high requirement for oxygen, which enables the complete breakdown of glucose in the mitochondria.
2. Hemoglobin in red blood cells carries oxygen to muscle.
3. The pigment myoglobin stores oxygen in muscle tissue.
F. Oxygen Debt
1. During rest or moderate activity, there is enough
oxygen to support aerobic respiration.
2. Oxygen deficiency may develop during strenuous
exercise. Pyruvic acid forms, then reacts to form
lactic acid which accumulates as an end product of
anaerobic respiration in the form of lactate.
a. Lactate diffuses out of muscle cells and is carried
in the bloodstream to the liver.
b. Using ATP, liver cells convert lactate back into glucose.
Oxygen debt, cont.
3. Oxygen debt refers to the amount of oxygen
that liver cells require to convert the
accumulated lactate back into glucose, plus the
amount that muscle cells need to resynthesize
ATP and creatine phosphate to their original
concentrations.
4. Repaying an oxygen debt may take several
hours.
5. Physical training helps to increase muscle’s
capacity to improve energy production.
83


G. Muscle Fatigue
1. When a muscle loses its ability to contract during strenuous exercise, it is referred to as fatigue.
2. Muscle fatigue usually arises from electrolyte imbalances and decreased ATP levels.
3. A muscle cramp occurs due to a lack of ATP required to return calcium ions back to the sarcoplasmic reticulum so muscle fibers can relax.
85
H. Heat Production
1. Contraction of skeletal muscle represents an
important source of heat for the body.
2. Much of the energy produced through the
reactions of cellular respiration is lost as heat
(another source of heat for the body).
86

8.4 Muscular Responses
A. One method of studying muscle function is to remove a single
fiber and connect it to a device that records its responses to
electrical stimulation.
B. Threshold Stimulus – the minimum stimulus required to generate
a impulse through the muscle, release calcium ions, activate
cross-bridges, and contract the muscle.
87

C. Recording a Muscular Contraction
1. The response of a single muscle fiber to
a single impulse is referred to as a
twitch.
2. A myogram is the recording of an
electrically-stimulated muscle
contraction.
3. A latent period is a brief delay between
the stimulation and beginning of the
contraction
4. The latent period is followed by a period
of contraction and a period of relaxation.
5. When a muscle fiber contracts, it
contracts to its full extent (all-or-none
response).
6. Muscle fibers vary in the speed of
contraction
a. Fatigue-resistant slow twitch fibers
b. Fatigable fast twitch fibers 88

D. Summation
1. A muscle fiber receiving a
series of stimuli of increasing
frequency reaches a point
when it is unable to relax
completely and the force of
individual twitches combine
by the process of summation.
2. If the sustained contraction
lacks any relaxation, it is
called a tetanic contraction.
3. This increases the force of
contraction for a single
muscle fiber.
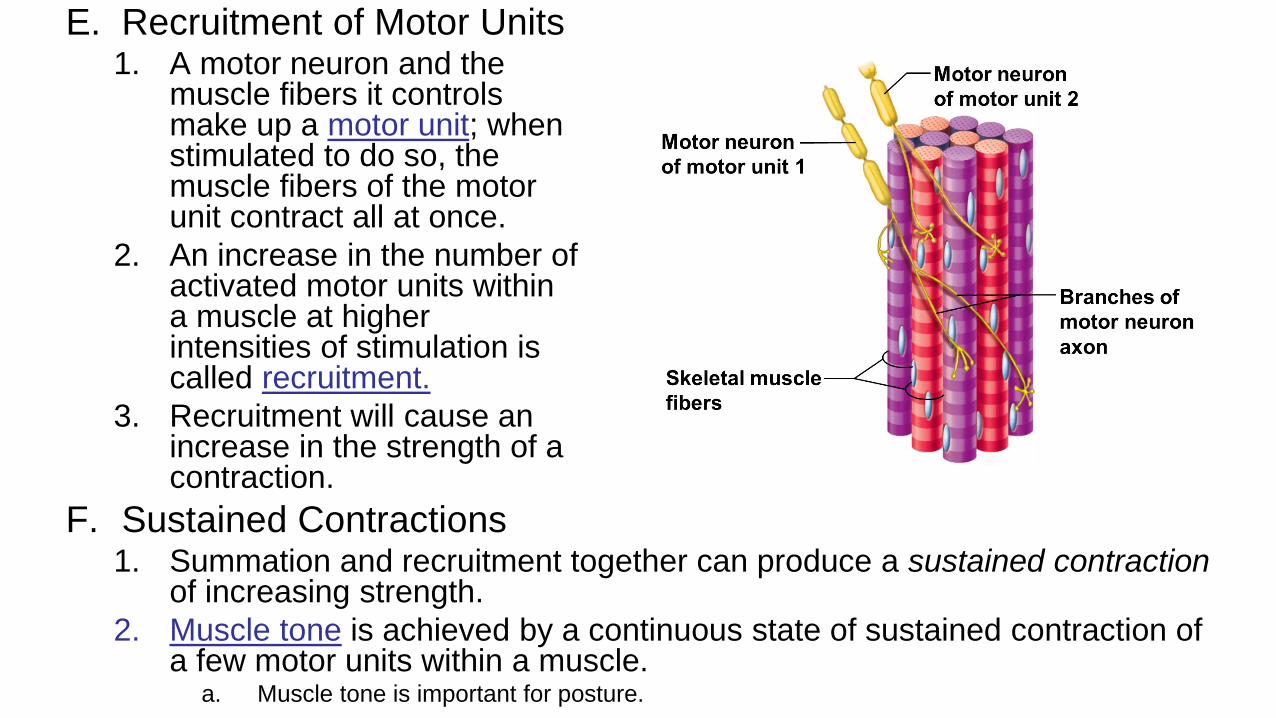
E. Recruitment of Motor Units1. A motor neuron and the
muscle fibers it controls make up a motor unit; when stimulated to do so, the muscle fibers of the motor unit contract all at once.
2. An increase in the number of activated motor units within a muscle at higher intensities of stimulation is called recruitment.
3. Recruitment will cause an increase in the strength of a contraction.
F. Sustained Contractions 1. Summation and recruitment together can produce a sustained contraction
of increasing strength.
2. Muscle tone is achieved by a continuous state of sustained contraction of a few motor units within a muscle.
a. Muscle tone is important for posture.
8.5 Smooth Muscles
A. Smooth Muscle Fibers
1. Smooth muscle cells are elongated with tapered ends, lack
striations and have a relatively undeveloped sarcoplasmic
reticulum.
2. The actin and myosin molecules extend the length of the cell
and are organized differently from skeletal muscle, causing no
striations.
91
3. Multiunit smooth muscle and visceral muscle are two types
of smooth muscles.
a. In multiunit smooth muscle, such as in the blood vessels
and iris of the eye, fibers occur separately rather than as
sheets.
b. Visceral smooth muscle occurs in sheets and is found in
the walls of hollow organs; these fibers can stimulate one
another and display rhythmicity, and are thus responsible
for peristalsis in hollow organs and tubes.
92
B. Smooth Muscle Contraction
1. The myosin-binding-to-actin mechanism is similar for smooth muscles and skeletal muscles.
2. Both acetylcholine and norepinephrine stimulate and inhibit smooth muscle contraction, depending on the target muscle.
3. Hormones can also stimulate or inhibit contraction.
4. Smooth muscle is slower to contract and relax than is skeletal
muscle, but can contract longer using the same amount of ATP.
5. Smooth muscle can also change its length without changing
tautness which is important in the filling of organs such as the
stomach.
93

8.6 Cardiac MuscleA. Cardiac muscle consists of branching, striated cells that
interconnect in three-dimensional networks.
B. The mechanism of contraction in cardiac muscle is essentially
the same as that for skeletal and smooth muscle, but with some
differences.
1. Cardiac muscle has transverse tubules that supply extra calcium, and
can thus contract for longer periods.
2. Cardiac muscle is self-exciting and rhythmic, creating a pattern of
contraction and relaxation.
C. Complex membrane junctions, called intercalated discs, join
cells and transmit the force of contraction from one cell to the
next, as well as aid in the rapid transmission of impulses
throughout the heart. 94

8.7 Skeletal Muscle Actions
A. Origin and Insertion
1. The immovable end of a muscle is the origin, while the movable end is the insertion; contraction pulls the insertion toward the origin.
2. Some muscles have more than one insertion or origin.

B. Interaction of Skeletal Muscles
1. Of a group of muscles, the one doing the majority of the work
is the agonist (prime mover).
2. Helper muscles are called synergists
3. Opposing muscles are called antagonists.
4. The relationships between muscles depends on the action –
role can and do change.
96
8.8 Major Skeletal Muscles
A. Muscles are named according to any of these: size, shape,
location, action, number of attachments, direction of its fibers, or
combinations of the above.
1. Pectoralis major – size and location
2. Deltoid – shape
3. Extensor digitorum – action
4. Biceps brachii – number of attachments and location
5. Sternocleidomastoid – attachments
6. External oblique – location and direction of fibers
97

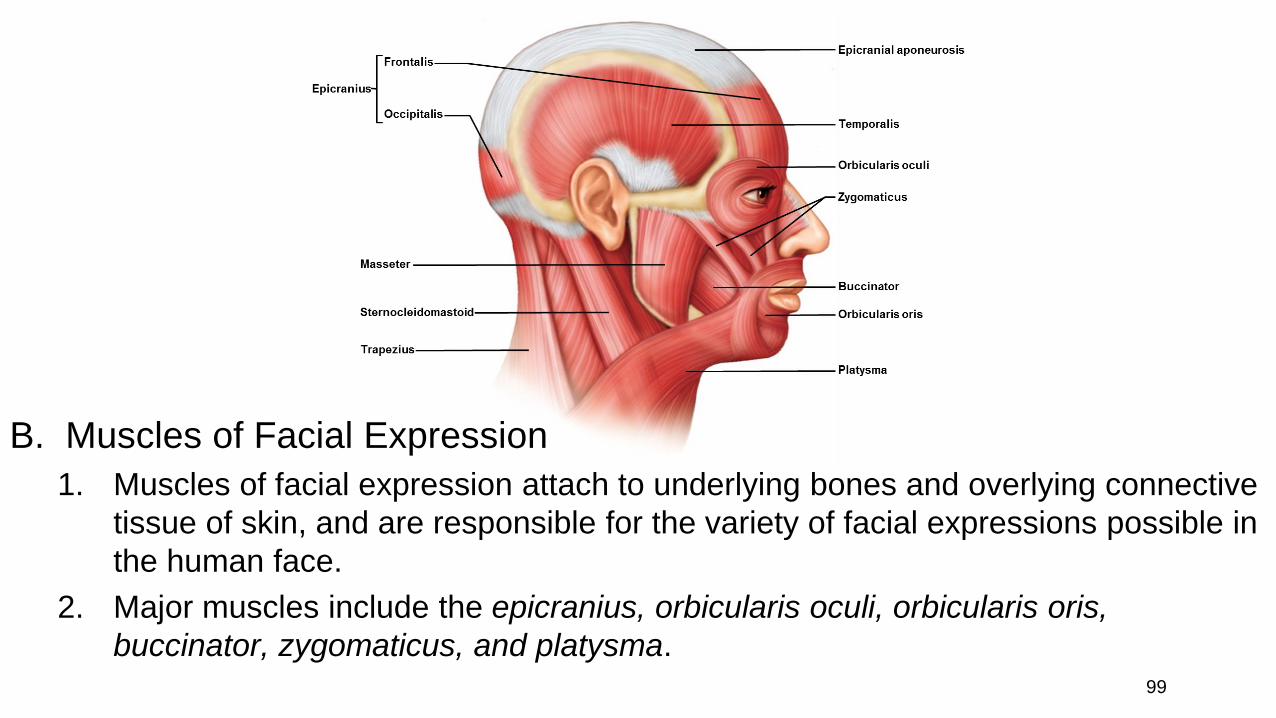
B. Muscles of Facial Expression
1. Muscles of facial expression attach to underlying bones and overlying connective
tissue of skin, and are responsible for the variety of facial expressions possible in
the human face.
2. Major muscles include the epicranius, orbicularis oculi, orbicularis oris,
buccinator, zygomaticus, and platysma.99
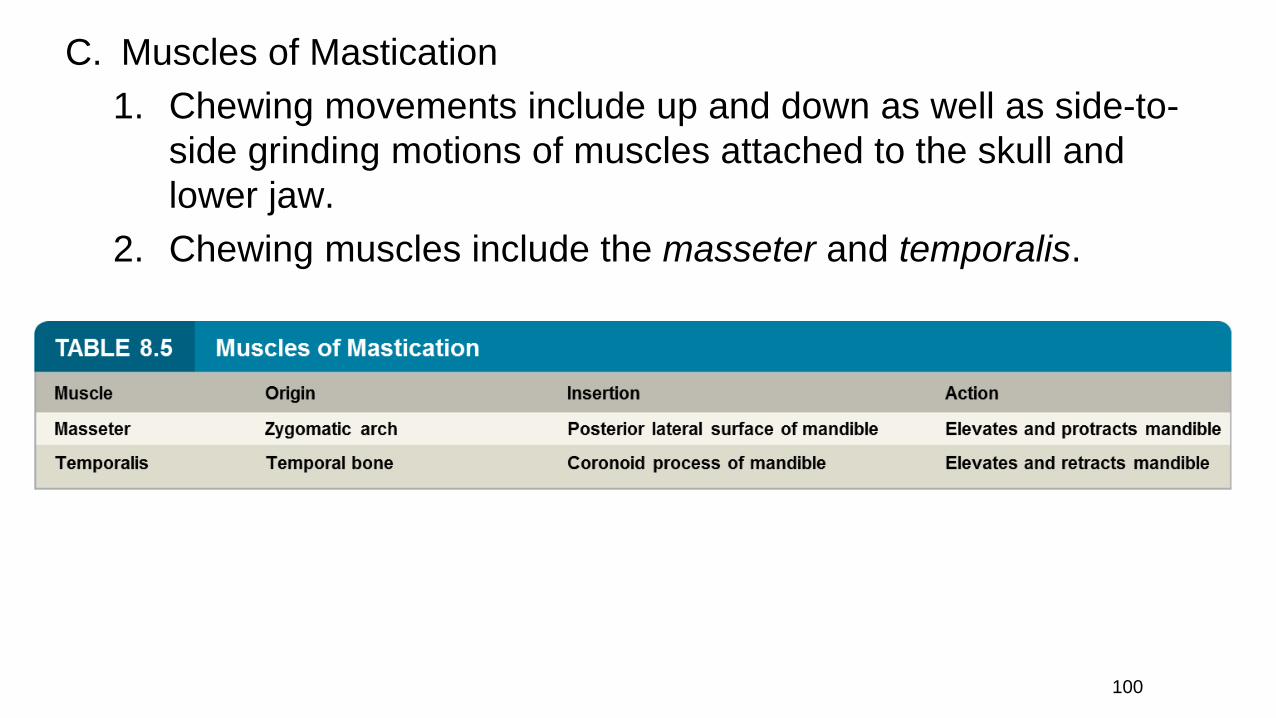
C. Muscles of Mastication
1. Chewing movements include up and down as well as side-to-
side grinding motions of muscles attached to the skull and
lower jaw.
2. Chewing muscles include the masseter and temporalis.
100
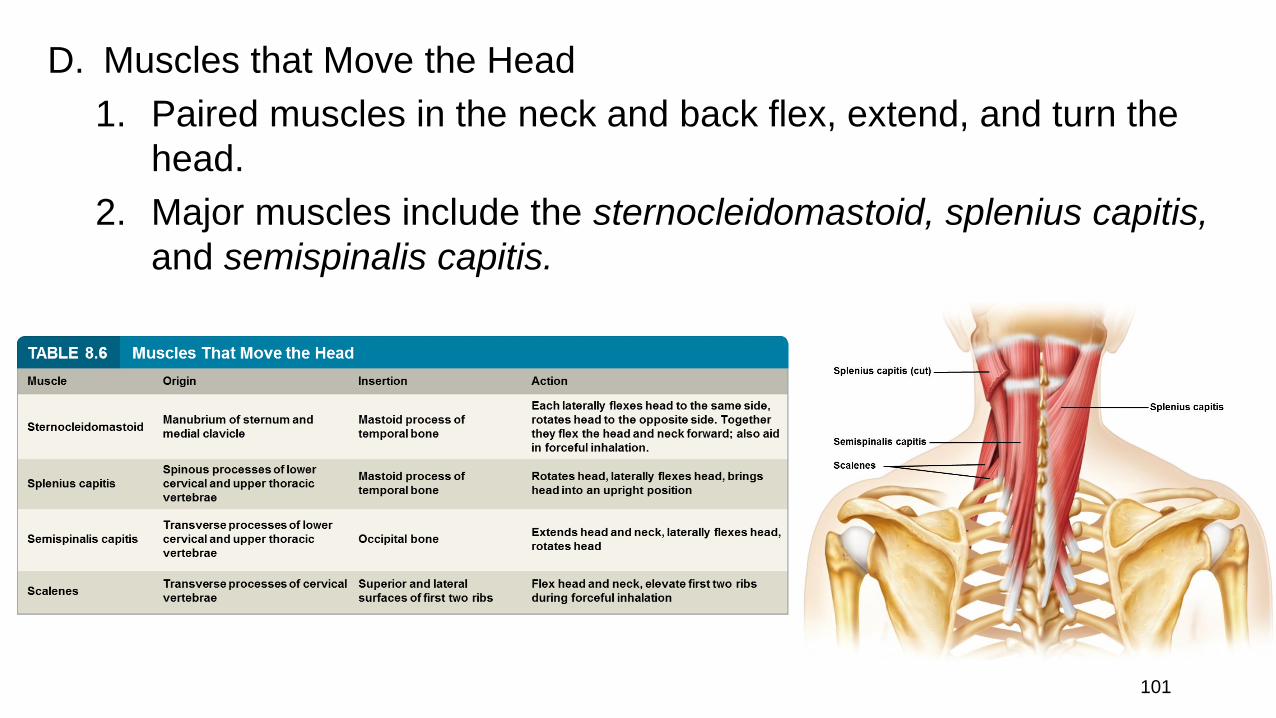
D. Muscles that Move the Head
1. Paired muscles in the neck and back flex, extend, and turn the
head.
2. Major muscles include the sternocleidomastoid, splenius capitis,
and semispinalis capitis.
101
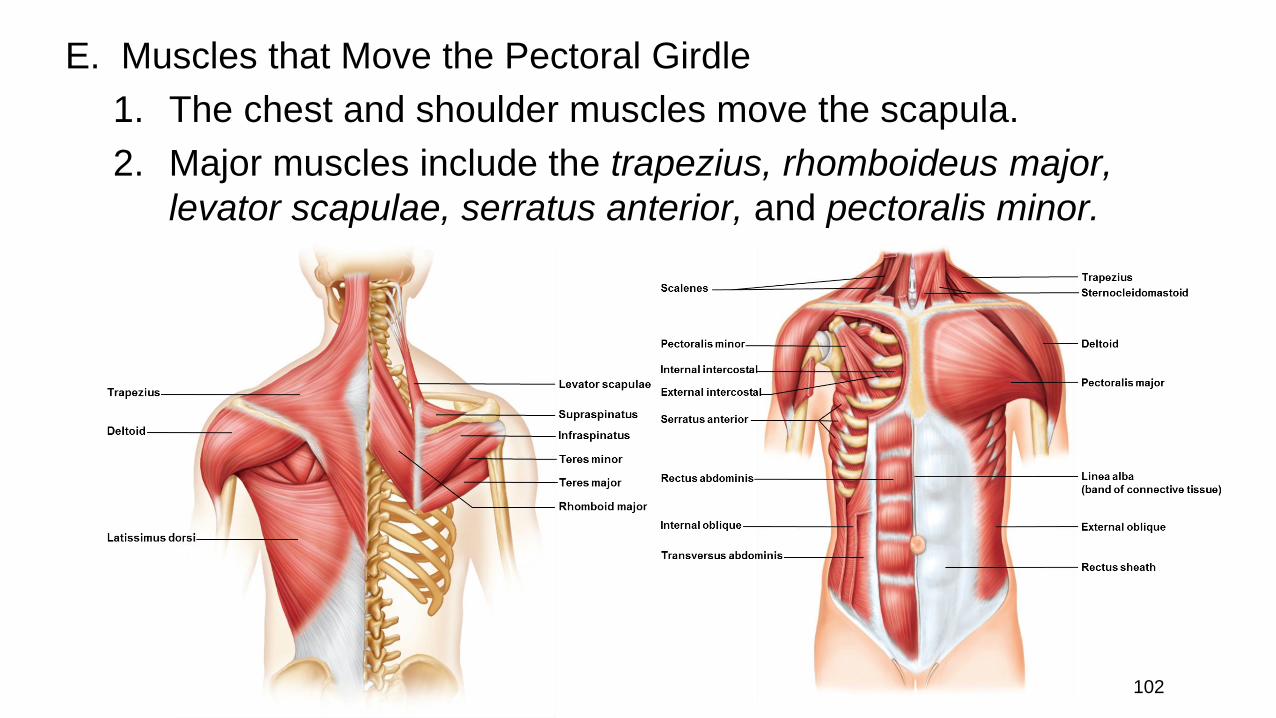
E. Muscles that Move the Pectoral Girdle
1. The chest and shoulder muscles move the scapula.
2. Major muscles include the trapezius, rhomboideus major,
levator scapulae, serratus anterior, and pectoralis minor.
102
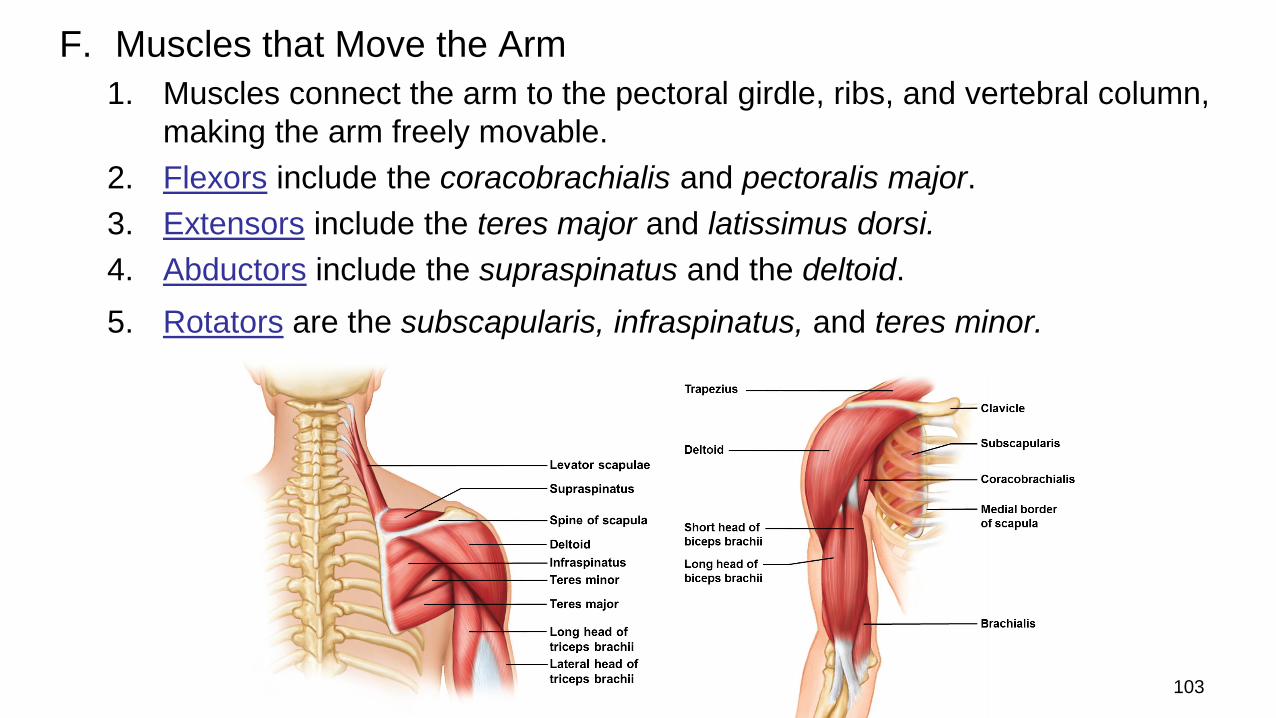
F. Muscles that Move the Arm
1. Muscles connect the arm to the pectoral girdle, ribs, and vertebral column,
making the arm freely movable.
2. Flexors include the coracobrachialis and pectoralis major.
3. Extensors include the teres major and latissimus dorsi.
4. Abductors include the supraspinatus and the deltoid.
5. Rotators are the subscapularis, infraspinatus, and teres minor.
103

G. Muscles that Move the
Forearm
1. These muscles arise from
the humerus or pectoral
girdle and connect to the
ulna and radius.
2. Flexors are the biceps
brachii, brachialis, and
brachioradialis.
3. An extensor is the triceps
brachii muscle.
4. Rotators include the
supinator, pronator teres,
and pronator quadratus.
104

H. Muscles that Move the Hand
1. Movements of the hand are caused by muscles originating from the distal
humerus, and the radius and ulna.
2. Flexors (on the anterior side) include the flexor carpi radialis, flexor carpi
ulnaris, palmaris longus, and flexor digitorum profundus.
3. Extensors (on the posterior side )include the extensor carpi radialis longus,
extensor carpi radialis brevis, extensor carpi ulnaris, and extensor
digitorum.
105
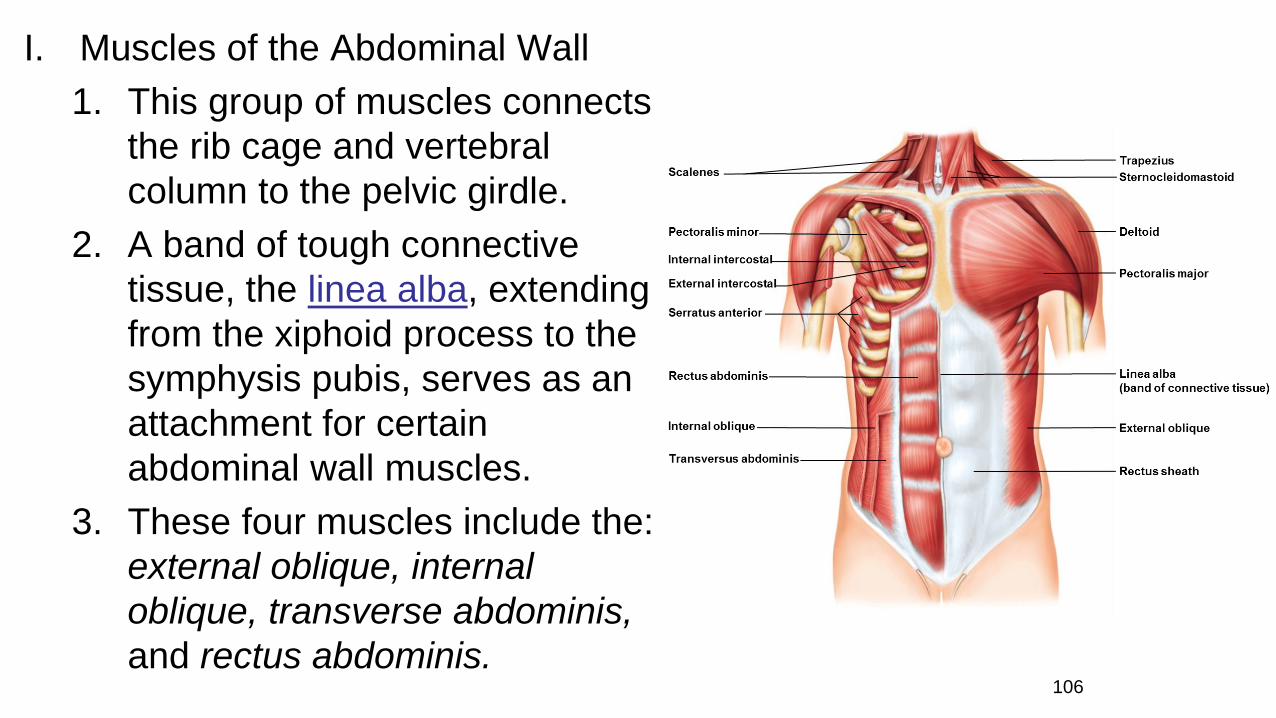
I. Muscles of the Abdominal Wall
1. This group of muscles connects
the rib cage and vertebral
column to the pelvic girdle.
2. A band of tough connective
tissue, the linea alba, extending
from the xiphoid process to the
symphysis pubis, serves as an
attachment for certain
abdominal wall muscles.
3. These four muscles include the:
external oblique, internal
oblique, transverse abdominis,
and rectus abdominis.106
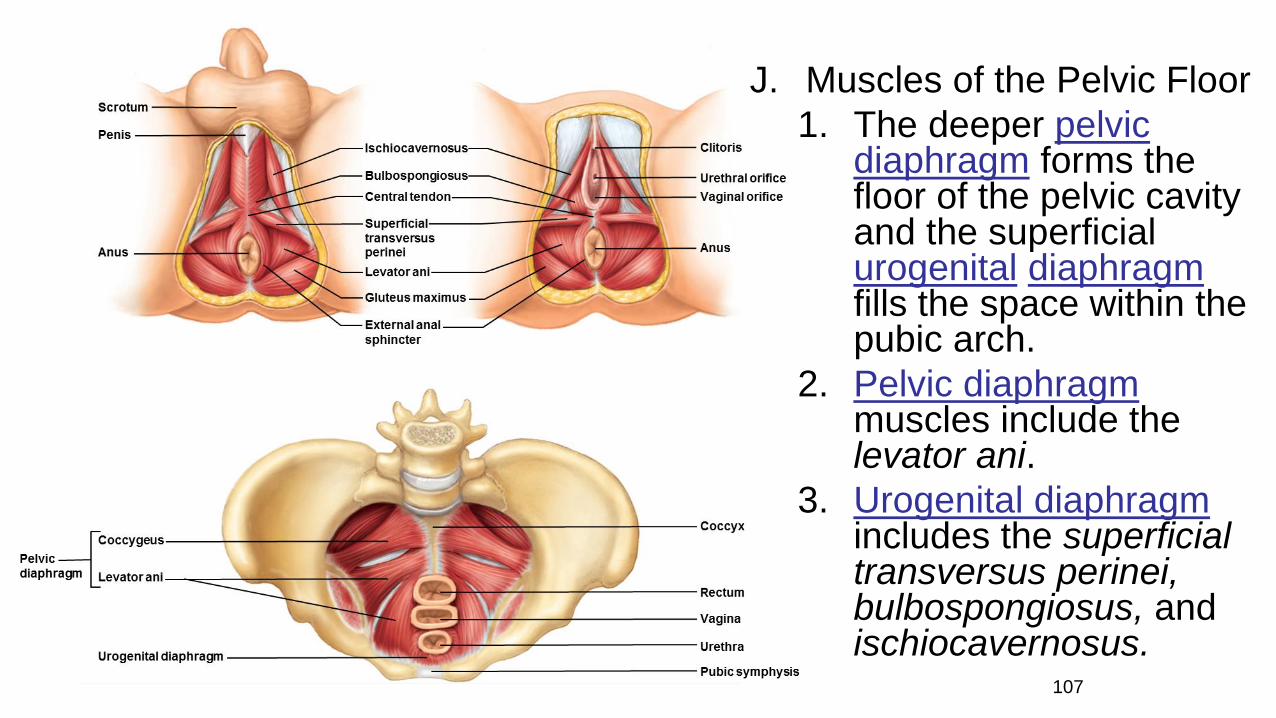
J. Muscles of the Pelvic Floor
1. The deeper pelvic diaphragm forms the floor of the pelvic cavity and the superficial urogenital diaphragmfills the space within the pubic arch.
2. Pelvic diaphragm muscles include the levator ani.
3. Urogenital diaphragmincludes the superficial transversus perinei, bulbospongiosus, and ischiocavernosus.
107

K. Muscles that Move the Thigh1. The muscles that move
the thigh are attached to the femur and to the pelvic girdle.
2. Anterior group muscles include the psoas major and iliacus.
3. Posterior group muscles include the gluteus maximus, gluteus medius, gluteus minimus, andtensor fasciae latae.
4. Thigh adductors include the adductor longus, adductor magnus, andgracilis. 108
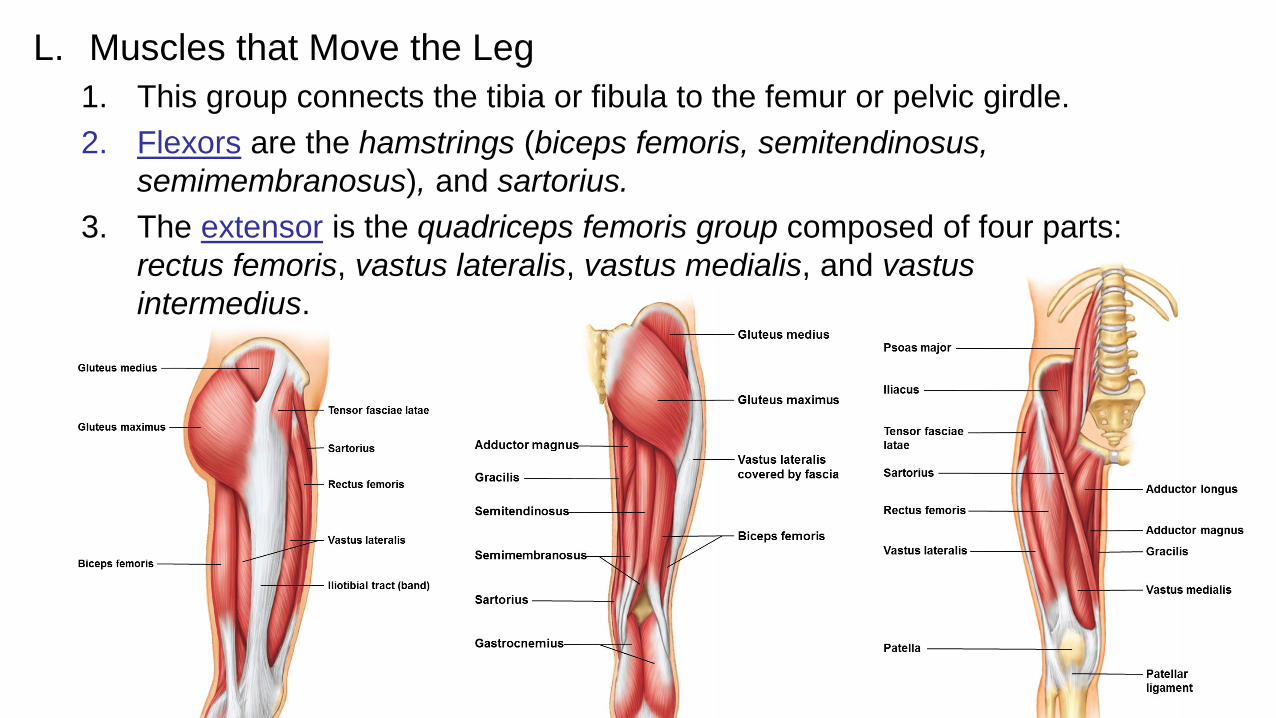
L. Muscles that Move the Leg
1. This group connects the tibia or fibula to the femur or pelvic girdle.
2. Flexors are the hamstrings (biceps femoris, semitendinosus,
semimembranosus), and sartorius.
3. The extensor is the quadriceps femoris group composed of four parts:
rectus femoris, vastus lateralis, vastus medialis, and vastus
intermedius.
109

M. Muscles that Move the Foot1. Muscles that move the foot are attached to the femur, fibula, or tibia, and move the foot
upward, downward, or in a turning motion.
2. Dorsal flexors include the tibialis anterior, fibularis (peroneus) tertius, and extensor digitorum
longus.
3. Plantar flexors are the gastrocnemius, soleus, and flexor digitorum longus.
4. An invertor is the tibialis posterior.
5. An evertor is the fibularis (peroneus) longus.
110